Fotosintesis - Wikipedia Bahasa Indonesia, Ensiklopedia Bebas
Upload
ezra-dizon-manzanoCategory
view
40download
0description

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 1/22
AsthmaClassification and external resources
Peak flow meters are used to measure the peak expiratory flow rate,important in both monitoring and diagnosing asthma.[1]
ICD-10 J45(http://apps.who.int/classifications/icd10/browse/2010/en#/J45)
ICD-9 493 (http://www.icd9data.com/getICD9Code.ashx?icd9=493)
OMIM 600807 (http://omim.org/entry/600807)
DiseasesDB 1006 (http://www.diseasesdatabase.com/ddb1006.htm)
MedlinePlus 000141(http://www.nlm.nih.gov/medlineplus/ency/article/000141.htm)
eMedicine article/806890 (http://emedicine.medscape.com/article/806890-overview)
MeSH D001249 (http://www.nlm.nih.gov/cgi/mesh/2013/MB_cgi?field=uid&term=D001249)
AsthmaFrom Wikipedia, the free encyclopedia
Asthma (from the Greek ἅσθμα,ásthma, "panting") is a commonchronic inflammatory disease of theairways characterized by variableand recurring symptoms, reversibleairflow obstruction, andbronchospasm.[2] Commonsymptoms include wheezing,coughing, chest tightness, andshortness of breath.[3]
Asthma is thought to be caused bya combination of genetic andenvironmental factors.[4] Itsdiagnosis is usually based on thepattern of symptoms, response totherapy over time, andspirometry.[5] It is clinicallyclassified according to thefrequency of symptoms, forcedexpiratory volume in one second(FEV1), and peak expiratory flowrate.[6] Asthma may also beclassified as atopic (extrinsic) ornon-atopic (intrinsic)[7] whereatopy refers to a predispositiontoward developing type 1hypersensitivity reactions.[8]
Treatment of acute symptoms isusually with an inhaled short-actingbeta-2 agonist (such as salbutamol)and oral corticosteroids.[9] In very severe cases intravenous corticosteroids, magnesium sulfate andhospitalization maybe required.[10] Symptoms can be prevented by avoiding triggers, such as allergens[11] andirritants, and by the use of inhaled corticosteroids.[12] Long-acting beta agonists (LABA) or leukotrieneantagonists may be used in addition to inhaled corticosteroids if asthma symptoms remain uncontrolled.[13]
The prevalence of asthma has increased significantly since the 1970s. As of 2011, 235–300 million peoplewere affected globally,[14][15] including about 250,000 deaths.[15]
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 2/22
Contents1 Signs and symptoms
1.1 Associated conditions2 Causes
2.1 Environmental2.2 Genetic2.3 Medical conditions2.4 Exacerbation
3 Pathophysiology4 Diagnosis
4.1 Spirometry4.2 Others4.3 Classification4.4 Differential diagnosis
5 Prevention6 Management
6.1 Lifestyle modification6.2 Medications6.3 Others6.4 Alternative medicine
7 Prognosis8 Epidemiology9 History10 Notes11 External links
Signs and symptomsAsthma is characterized by recurrent episodes of wheezing, shortness of breath, chest tightness, andcoughing.[16] Sputum may be produced from the lung by coughing but is often hard to bring up.[17] Duringrecovery from an attack it may appear pus like due to high levels of white blood cells called eosinophils.[18]
Symptoms are usually worse at night and in the early morning or in response to exercise or cold air.[19] Somepeople with asthma rarely experience symptoms, usually in response to triggers, whereas others may havemarked and persistent symptoms.[20]
Associated conditions
A number of other health conditions occur more frequently in those with asthma including: gastro-esophagealreflux disease (GERD), rhinosinusitis, and obstructive sleep apnea.[21] Psychological disorders are also morecommon[22] with anxiety disorders occurring in between 16–52% and mood disorders in 14–41%.[23] Ithowever is not known if asthma causes psychological problems or if psychological problems lead toasthma.[24]

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 3/22
CausesAsthma is caused by a combination of complex and incompletely understood environmental and geneticinteractions.[4][25] These factors influence both its severity and its responsiveness to treatment.[26] It isbelieved that the recent increased rates of asthma are due to changing epigenetics (heritable factors other thanthose related to the DNA sequence) and a changing living environment.[27]
Environmental
Many environmental factors have been associated with asthma's development and exacerbation including:allergens, air pollution, and other environmental chemicals.[28] Smoking during pregnancy and after deliveryis associated with a greater risk of asthma-like symptoms.[29] Low air quality, from traffic pollution or highozone levels,[30] has been associated with both asthma development and increased asthma severity.[31]
Exposure to indoor volatile organic compounds may be a trigger for asthma; formaldehyde exposure, forexample, has a positive association.[32] Also, phthalates in PVC are associated with asthma in children andadults[33][34] as are high levels of endotoxin exposure.[35]
Asthma is associated with exposure to indoor allergens.[36] Common indoor allergens include: dust mites,cockroaches, animal dander, and mold.[37][38] Efforts to decrease dust mites have been found to beineffective.[39] Certain viral respiratory infections may increase the risk of developing asthma when acquiredas young children such as:[40] respiratory syncytial virus and rhinovirus.[41] Certain other infections howevermay decrease the risk.[41]
Hygiene hypothesis
The hygiene hypothesis is a theory which attempts to explain the increased rates of asthma worldwide as adirect and unintended result of reduced exposure, during childhood, to non–pathogenic bacteria andviruses.[42][43] It has been proposed that the reduced exposure to bacteria and viruses is due, in part, toincreased cleanliness and decreased family size in modern societies.[44] Evidence supporting the hygienehypothesis includes lower rates of asthma on farms and in households with pets.[44]
Use of antibiotics in early life has been linked to the development of asthma.[45] Also, delivery via caesareansection is associated with an increased risk (estimated at 20–80%) of asthma—this increased risk is attributedto the lack of healthy bacterial colonization that the newborn would have acquired from passage through thebirth canal.[46][47] There is a link between asthma and the degree of affluence.[48]
Genetic
Family history is a risk factor for asthma with many different genes being implicated.[50] If one identical twinis affected, the probability of the other having the disease is approximately 25%.[50] By the end of 2005, 25genes had been associated with asthma in six or more separate populations including:GSTM1, IL10, CTLA-4,SPINK5,LTC4S, IL4R and ADAM33 among others.[51] Many of these genes are related to the immune system

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 4/22
CD14-endotoxin interaction based on CD14SNP C-159T[49]
Endotoxin levels CC genotype TT genotypeHigh exposure Low risk High risk
Low exposure High risk Low risk
or modulating inflammation. Even among this list of genessupported by highly replicated studies, results have notbeen consistent among all populations tested.[51] In 2006over 100 genes were associated with asthma in one geneticassociation study alone;[51] more continue to be found.[52]
Some genetic variants may only cause asthma when theyare combined with specific environmental exposures.[4]
An example is a specific single nucleotide polymorphismin the CD14 region and exposure to endotoxin (a bacterial product). Endotoxin exposure can come fromseveral environmental sources including tobacco smoke, dogs, and farms. Risk for asthma, then, is determinedby both a person's genetics and the level of endotoxin exposure.[49]
Medical conditions
A triad of atopic eczema, allergic rhinitis and asthma is called atopy.[53] The strongest risk factor fordeveloping asthma is a history of atopic disease;[40] with asthma occurring at a much greater rate in those whohave either eczema or hay fever.[54] Asthma has been associated with Churg–Strauss syndrome, anautoimmune disease and vasculitis. Individuals with certain types of urticaria may also experience symptomsof asthma.[53]
There is a correlation between obesity and the risk of asthma with both having increased in recentyears.[55][56] Several factors may be at play including decreased respiratory function due to a buildup of fatand the fact that adipose tissue leads to a pro-inflammatory state.[57]
Beta blocker medications such as propranolol can trigger asthma in those who are susceptible.[58]
Cardioselective beta-blockers, however, appear safe in those with mild or moderate disease.[59] Othermedications that can cause problems are ASA, NSAIDs, and angiotensin-converting enzyme inhibitors.[60]
Exacerbation
Some individuals will have stable asthma for weeks or months and then suddenly develop an episode of acuteasthma. Different individuals react differently to various factors.[61] Most individuals can develop severeexacerbation from a number of triggering agents.[61]
Home factors that can lead to exacerbation of asthma include dust, animal dander (especially cat and dog hair),cockroach allergens and mold.[61] Perfumes are a common cause of acute attacks in women and children.Both viral and bacterial infections of the upper respiratory tract can worsen the disease.[61] Psychologicalstress may worsen symptoms—it is thought that stress alters the immune system and thus increases the airwayinflammatory response to allergens and irritants.[31][62]
Pathophysiology

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 5/22
Obstruction of the lumen of abronchiole by mucoid exudate, gobletcell metaplasia, and epithelialbasement membrane thickening in aperson with asthma.
Main article: Pathophysiology of asthma
Asthma is the result of chronic inflammation of the airways whichsubsequently results in increased contractability of the surroundingsmooth muscles. This among other factors leads to bouts of narrowingof the airway and the classic symptoms of wheezing. The narrowingis typically reversible with or without treatment. Occasionally theairways themselves change.[16] Typical changes in the airwaysinclude an increase in eosinophils and thickening of the laminareticularis. Chronically the airways' smooth muscle may increase insize along with an increase in the numbers of mucous glands. Othercell types involved include: T lymphocytes, macrophages, andneutrophils. There may also be involvement of other components ofthe immune system including: cytokines, chemokines, histamine, andleukotrienes among others.[41]
Diagnosis
While asthma is a well recognized condition, there is not one universal agreed upon definition.[41] It is definedby the Global Initiative for Asthma as "a chronic inflammatory disorder of the airways in which many cellsand cellular elements play a role. The chronic inflammation is associated with airway hyper-responsivenessthat leads to recurrent episodes of wheezing, breathlessness, chest tightness and coughing particularly at nightor in the early morning. These episodes are usually associated with widespread but variable airflowobstruction within the lung that is often reversible either spontaneously or with treatment".[16]
There is currently no precise test with the diagnosis typically based on the pattern of symptoms and responseto therapy over time.[5][41] A diagnosis of asthma should be suspected if there is a history of: recurrentwheezing, coughing or difficulty breathing and these symptoms occur or worsen due to exercise, viralinfections, allergens or air pollution.[63] Spirometry is then used to confirm the diagnosis.[63] In children underthe age of six the diagnosis is more difficult as they are too young for spirometry.[64]
Spirometry
Spirometry is recommended to aid in diagnosis and management.[65][66] It is the single best test for asthma. Ifthe FEV1 measured by this technique improves more than 12% following administration of a bronchodilatorsuch as salbutamol, this is supportive of the diagnosis.[67] It however may be normal in those with a history ofmild asthma, not currently acting up. Single-breath diffusing capacity can help differentiate asthma fromCOPD.[41] It is reasonable to perform spirometry every one or two years to follow how well a person's asthmais controlled.[68]
Others

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 6/22
Clinical classification (≥ 12 years old)[6]
Severity Symptomfrequency
Night timesymptoms
%FEV1 ofpredicted
FEV1Variability SABA use
Intermittent ≤2/week ≤2/month ≥80% <20% ≤2 days/weekMild persistent >2/week 3–4/month ≥80% 20–30% >2 days/week
Moderatepersistent Daily >1/week 60–80% >30% daily
Severe persistent Continuously Frequent(7×/week) <60% >30% ≥twice/day
The methacholine challenge involves the inhalation of increasing concentrations of a substance that causesairway narrowing in those predisposed. If negative it means that a person does not have asthma; if positive,however, it is not specific for the disease.[41]
Other supportive evidence includes: a ≥20% difference in peak expiratory flow rate on at least three days in aweek for at least two weeks, a ≥20% improvement of peak flow following treatment with either salbutamol,inhaled corticosteroids or prednisone, or a ≥20% decrease in peak flow following exposure to a trigger.[69]
Testing peak expiratory flow is more variable than spirometry, however, and thus not recommended forroutine diagnosis. It may be useful for daily self-monitoring in those with moderate to severe disease and forchecking the effectiveness of new medications. It may also be helpful in guiding treatment in those with acuteexacerbations.[70]
Classification
Asthma isclinicallyclassifiedaccordingto thefrequencyof
symptoms, forced expiratory volume in one second (FEV1), and peak expiratory flow rate.[6] Asthma mayalso be classified as atopic (extrinsic) or non-atopic (intrinsic), based on whether symptoms are precipitated byallergens (atopic) or not (non-atopic).[7] While asthma is classified based on severity, at the moment there is noclear method for classifying different subgroups of asthma beyond this system.[71] Finding ways to identifysubgroups that respond well to different types of treatments is a current critical goal of asthma research.[71]
Although asthma is a chronic obstructive condition, it is not considered as a part of chronic obstructivepulmonary disease as this term refers specifically to combinations of disease that are irreversible such asbronchiectasis, chronic bronchitis, and emphysema.[72] Unlike these diseases, the airway obstruction in asthmais usually reversible; however, if left untreated, the chronic inflammation from asthma can lead the lungs tobecome irreversibly obstructed due to airway remodeling.[73] In contrast to emphysema, asthma affects thebronchi, not the alveoli.[74]
Asthma exacerbation
An acute asthma exacerbation is commonly referred to as an asthma attack. The classic symptoms areshortness of breath, wheezing, and chest tightness.[41] While these are the primary symptoms of asthma,[76]
some people present primarily with coughing, and in severe cases, air motion may be significantly impaired

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 7/22
Severity of an acute exacerbation[75]
Near-fatal High PaCO2 and/or requiring mechanical ventilation
Life threatening(any one of)
Clinical signs MeasurementsAltered level of consciousness Peak flow < 33%
Exhaustion Oxygen saturation < 92%Arrhythmia PaO2 < 8 kPa
Low blood pressure "Normal" PaCO2
CyanosisSilent chest
Poor respiratory effort
Acute severe(any one of)
Peak flow 33–50%Respiratory rate ≥ 25 breaths per minute
Heart rate ≥ 110 beats per minuteUnable to complete sentences in one breath
ModerateWorsening symptoms
Peak flow 50–80% best or predictedNo features of acute severe asthma
such that no wheezing isheard.[75]
Signs which occur during anasthma attack include the useof accessory muscles ofrespiration(sternocleidomastoid andscalene muscles of the neck),there may be a paradoxicalpulse (a pulse that is weakerduring inhalation and strongerduring exhalation), and over-inflation of the chest.[77] Ablue color of the skin and nailsmay occur from lack ofoxygen.[78]
In a mild exacerbation the peakexpiratory flow rate (PEFR) is≥200 L/min or ≥50% of thepredicted best.[79] Moderate isdefined as between 80 and200 L/min or 25% and 50% ofthe predicted best while severeis defined as ≤ 80 L/min or≤25% of the predicted best.[79]
Acute severe asthma, previously known as status asthmaticus, is an acute exacerbation of asthma that does notrespond to standard treatments of bronchodilators and corticosteroids.[80] Half of cases are due to infectionswith others caused by allergen, air pollution, or insufficient or inappropriate medication use.[80]
Brittle asthma is a kind of asthma distinguishable by recurrent, severe attacks.[75] Type 1 brittle asthma is adisease with wide peak flow variability, despite intense medication. Type 2 brittle asthma is background well-controlled asthma with sudden severe exacerbations.[75]
Exercise-induced
Main article: Exercise-induced bronchoconstriction
Exercise can trigger bronchoconstriction in both people with and without asthma.[81] It occurs in most peoplewith asthma and up to 20% of people without asthma.[81] In athletes it occurs more common in elite athletes,with rates varying from 3% for bobsled racers to 50% for cycling and 60% for cross-country skiing.[81] While

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 8/22
it may occur with any weather conditions it is more common when it is dry and cold.[82] Inhaled beta2-agonists do not appear to improve athletic performance among those without asthma[83] however oral dosesmay improve endurance and strength.[84][85]
Occupational
Main article: Occupational asthma
Asthma as a result of (or worsened by) workplace exposures, is a commonly reported occupational disease.[86]
Many cases however are not reported or recognized as such.[87][88] It is estimated that 5–25% of asthma casesin adults are work–related. A few hundred different agents have been implicated with the most common being:isocyanates, grain and wood dust, colophony, soldering flux, latex, animals, and aldehydes. The employmentassociated with the highest risk of problems include: those who spray paint, bakers and those who processfood, nurses, chemical workers, those who work with animals, welders, hairdressers and timber workers.[86]
Differential diagnosis
Many other conditions can cause symptoms similar to those of asthma. In children, other upper airwaydiseases such as allergic rhinitis and sinusitis should be considered as well as other causes of airwayobstruction including: foreign body aspiration, tracheal stenosis or laryngotracheomalacia, vascular rings,enlarged lymph nodes or neck masses. In adults, COPD, congestive heart failure, airway masses, as well asdrug-induced coughing due to ACE inhibitors should be considered. In both populations vocal corddysfunction may present similarly.[89]
Chronic obstructive pulmonary disease can coexist with asthma and can occur as a complication of chronicasthma. After the age of 65 most people with obstructive airway disease will have asthma and COPD. In thissetting, COPD can be differentiated by increased airway neutrophils, abnormally increased wall thickness, andincreased smooth muscle in the bronchi. However, this level of investigation is not performed due to COPDand asthma sharing similar principles of management: corticosteroids, long acting beta agonists, and smokingcessation.[90] It closely resembles asthma in symptoms, is correlated with more exposure to cigarette smoke, anolder age, less symptom reversibility after bronchodilator administration, and decreased likelihood of familyhistory of atopy.[91][92]
Prevention
The evidence for the effectiveness of measures to prevent the development of asthma is weak.[93] Some showpromise including: limiting smoke exposure both in utero and after delivery, breastfeeding, and increasedexposure to daycare or large families but none are well supported enough to be recommended for thisindication.[93] Early pet exposure may be useful.[94] Results from exposure to pets at other times areinconclusive[95] and it is only recommended that pets be removed from the home if a person has allergicsymptoms to said pet.[96] Dietary restrictions during pregnancy or when breast feeding have not been found tobe effective and thus are not recommended.[96] Reducing or eliminating compounds known to sensitivepeople from the work place may be effective.[86]

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 9/22
Management
While there is no cure for asthma, symptoms can typically be improved.[97] A specific, customized plan forproactively monitoring and managing symptoms should be created. This plan should include the reduction ofexposure to allergens, testing to assess the severity of symptoms, and the usage of medications. The treatmentplan should be written down and advise adjustments to treament according to changes in symptoms.[98]
The most effective treatment for asthma is identifying triggers, such as cigarette smoke, pets, or aspirin, andeliminating exposure to them. If trigger avoidance is insufficient, the use of medication is recommended.Pharmaceutical drugs are selected based on, among other things, the severity of illness and the frequency ofsymptoms. Specific medications for asthma are broadly classified into fast-acting and long-actingcategories.[99][100]
Bronchodilators are recommended for short-term relief of symptoms. In those with occasional attacks, no othermedication is needed. If mild persistent disease is present (more than two attacks a week), low-dose inhaledcorticosteroids or alternatively, an oral leukotriene antagonist or a mast cell stabilizer is recommended. Forthose who have daily attacks, a higher dose of inhaled corticosteroids is used. In a moderate or severeexacerbation, oral corticosteroids are added to these treatments.[9]
Lifestyle modification
Avoidance of triggers is a key component of improving control and preventing attacks. The most commontriggers include allergens, smoke (tobacco and other), air pollution, non selective beta-blockers, and sulfite-containing foods.[101][102] Cigarette smoking and second-hand smoke (passive smoke) may reduce theeffectiveness of medications such as corticosteroids.[103] Dust mite control measures, including air filtration,chemicals to kill mites, vacuuming, mattress covers and others methods had no effect on asthma symptoms.[39]
Medications
Medications used to treat asthma are divided into two general classes: quick-relief medications used to treatacute symptoms; and long-term control medications used to prevent further exacerbation.[99]
Fast–acting
Short-acting beta2-adrenoceptor agonists (SABA), such as salbutamol (albuterol USAN) are the firstline treatment for asthma symptoms.[9]
Anticholinergic medications, such as ipratropium bromide, provide additional benefit when used incombination with SABA in those with moderate or severe symptoms.[9] Anticholinergicbronchodilators can also be used if a person cannot tolerate a SABA.[72]
Older, less selective adrenergic agonists, such as inhaled epinephrine, have similar efficacy toSABAs.[104] They are however not recommended due to concerns regarding excessive cardiacstimulation.[105]
Long–term control
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 10/22
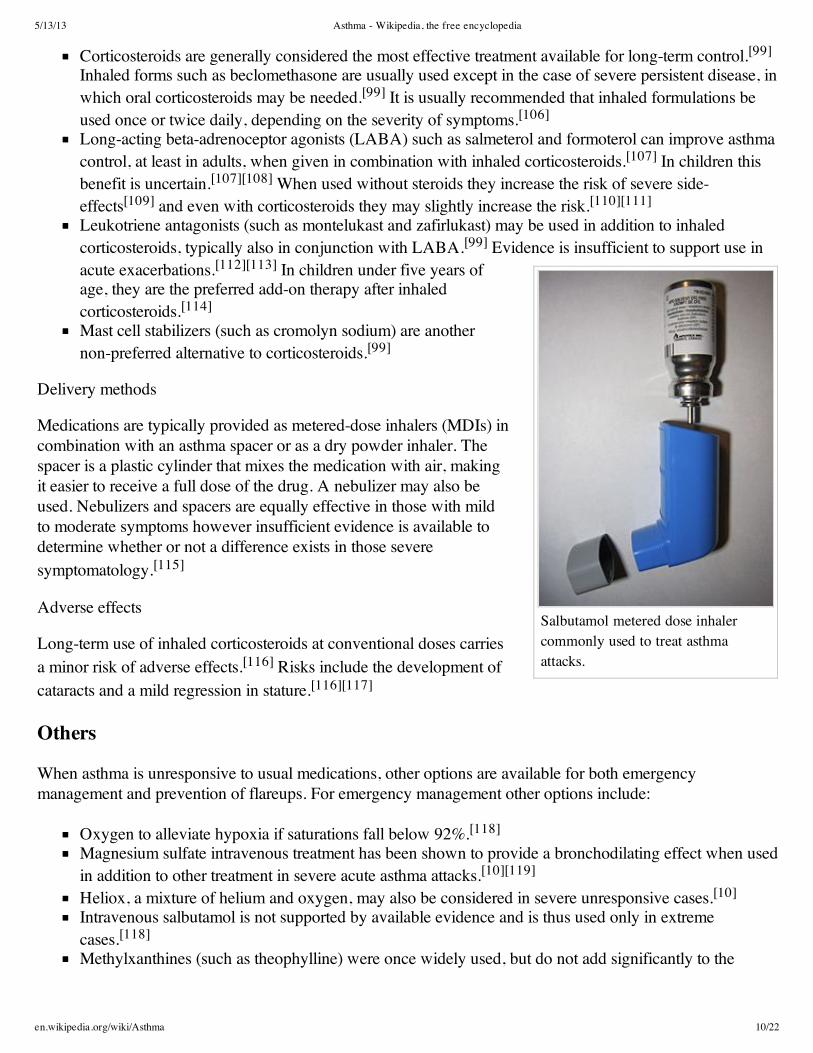
Salbutamol metered dose inhalercommonly used to treat asthmaattacks.
Corticosteroids are generally considered the most effective treatment available for long-term control.[99]
Inhaled forms such as beclomethasone are usually used except in the case of severe persistent disease, inwhich oral corticosteroids may be needed.[99] It is usually recommended that inhaled formulations beused once or twice daily, depending on the severity of symptoms.[106]
Long-acting beta-adrenoceptor agonists (LABA) such as salmeterol and formoterol can improve asthmacontrol, at least in adults, when given in combination with inhaled corticosteroids.[107] In children thisbenefit is uncertain.[107][108] When used without steroids they increase the risk of severe side-effects[109] and even with corticosteroids they may slightly increase the risk.[110][111]
Leukotriene antagonists (such as montelukast and zafirlukast) may be used in addition to inhaledcorticosteroids, typically also in conjunction with LABA.[99] Evidence is insufficient to support use inacute exacerbations.[112][113] In children under five years ofage, they are the preferred add-on therapy after inhaledcorticosteroids.[114]
Mast cell stabilizers (such as cromolyn sodium) are anothernon-preferred alternative to corticosteroids.[99]
Delivery methods
Medications are typically provided as metered-dose inhalers (MDIs) incombination with an asthma spacer or as a dry powder inhaler. Thespacer is a plastic cylinder that mixes the medication with air, makingit easier to receive a full dose of the drug. A nebulizer may also beused. Nebulizers and spacers are equally effective in those with mildto moderate symptoms however insufficient evidence is available todetermine whether or not a difference exists in those severesymptomatology.[115]
Adverse effects
Long-term use of inhaled corticosteroids at conventional doses carriesa minor risk of adverse effects.[116] Risks include the development ofcataracts and a mild regression in stature.[116][117]
Others
When asthma is unresponsive to usual medications, other options are available for both emergencymanagement and prevention of flareups. For emergency management other options include:
Oxygen to alleviate hypoxia if saturations fall below 92%.[118]
Magnesium sulfate intravenous treatment has been shown to provide a bronchodilating effect when usedin addition to other treatment in severe acute asthma attacks.[10][119]
Heliox, a mixture of helium and oxygen, may also be considered in severe unresponsive cases.[10]
Intravenous salbutamol is not supported by available evidence and is thus used only in extremecases.[118]
Methylxanthines (such as theophylline) were once widely used, but do not add significantly to the
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 11/22
Fluticasone propionate metered doseinhaler commonly used for long-termcontrol.
effects of inhaled beta-agonists.[118] Their use in acute exacerbations is controversial.[120]
The dissociative anesthetic ketamine is theoretically useful if intubation and mechanical ventilation isneeded in people who are approaching respiratory arrest; however, there is no evidence from clinicaltrials to support this.[121]
For those with severe persistent asthma not controlled by inhaled corticosteroids and LABAs bronchialthermoplasty may be an option.[122] It involves the delivery of controlled thermal energy to the airway wallduring a series of bronchoscopies.[122] While it may increase exacerbation frequency in the first few months itappears to decrease the subsequent rate. Effects beyond one year are unknown.[123] Evidence suggests thatsublingual immunotherapy in those with both allergic rhinitis and asthma improve outcomes.[124]
Alternative medicine
Many people with asthma, like those with other chronic disorders, usealternative treatments; surveys show that roughly 50% use some formof unconventional therapy.[125][126] There is little data to support theeffectiveness of most of these therapies. Evidence is insufficient tosupport the usage of Vitamin C.[127] Acupuncture is notrecommended for the treatment as there is insufficient evidence tosupport its use.[128][129] Air ionisers show no evidence that theyimprove asthma symptoms or benefit lung function; this appliedequally to positive and negative ion generators.[130]
"Manual therapies", including osteopathic, chiropractic,physiotherapeutic and respiratory therapeutic maneuvers, haveinsufficient evidence to support their use in treating asthma.[131] TheButeyko breathing technique for controlling hyperventilation mayresult in a reduction in medications use however does not have anyeffect on lung function.[100] Thus an expert panel felt that evidencewas insufficient to support its use.[128]
Prognosis
The prognosis for asthma is generally good, especially for children with mild disease.[133] Mortality hasdecreased over the last few decades due to better recognition and improvement in care.[134] Globally it causesmoderate or severe disability in 19.4 million people as of 2004 (16 million of which are in low and middleincome countries).[135] Of asthma diagnosed during childhood, half of cases will no longer carry the diagnosisafter a decade.[50] Airway remodeling is observed, but it is unknown whether these represent harmful orbeneficial changes.[136] Early treatment with corticosteroids seems to prevent or ameliorates a decline in lungfunction.[137]
Epidemiology

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 12/22
Disability-adjusted life year forasthma per 100,000 inhabitants in2004.[132]
no data
<100
100–150
150–200
200–250
250–300
300–350
350–400
400–450
450–500
500–550
550–600
>600
Rates of asthma in different countriesof the world as of 2004.
no data
<1%
1-2%
2-3%
3-4%
4-5%
5-6%
6-7%
7-8%
8-10%
10-12.5%
12.5–15%
>15%
Main article: Epidemiology of asthma
As of 2011, 235–300 millionpeople worldwide are affectedby asthma,[14][15] andapproximately 250,000people die per year from thedisease.[16] Rates varybetween countries withprevalences between 1 and18%.[16] It is more commonin developed than developingcountries.[16] One thus seeslower rates in Asia, EasternEurope and Africa.[41] Withindeveloped countries it is morecommon in those who areeconomically disadvantagedwhile in contrast indeveloping countries it is
more common in the affluent.[16] The reason for these differences is not well known.[16] Low and middleincome countries make up more than 80% of the mortality.[138]
While asthma is twice as common in boys as girls,[16] severe asthma occurs at equal rates.[139] In contrastadult women have a higher rate of asthma than men[16] and it is more common in the young than the old.[41]
Global rates of asthma have increased significantly between the 1960s and 2008[140][141] with it beingrecognized as a major public health problem since the 1970s.[41] Rates of asthma have plateaued in thedeveloped world since the mid-1990s with recent increases primarily in the developing world.[142] Asthmaaffects approximately 7% of the population of the United States[109] and 5% of people in the UnitedKingdom.[143] Canada, Australia and New Zealand have rates of about 14–15%.[144]
HistoryAsthma was recognized in Ancient Egypt and was treated by drinking an incense mixture known askyphi.[145] It was officially named as a specific respiratory problem by Hippocrates circa 450 BC, with theGreek word for "panting" forming the basis of our modern name.[41] In 200 BC it was believed to be at leastpartly related to the emotions.[23]
In 1873, one of the first papers in modern medicine on the subject tried to explain the pathophysiology of thedisease while one in 1872, concluded that asthma can be cured by rubbing the chest with chloroformliniment.[146][147] Medical treatment in 1880, included the use of intravenous doses of a drug calledpilocarpin.[148] In 1886, F.H. Bosworth theorized a connection between asthma and hay fever.[149]

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 13/22
Epinephrine was first referred to in the treatment of asthma in 1905.[150] Oral corticosteroids began to be usedfor this condition in the 1950s while inhaled corticosteroids and selective short acting beta agonist came intowide use in the 1960s.[151][152]
During the 1930s–1950s, asthma was known as one of the "holy seven" psychosomatic illnesses. Its causewas considered to be psychological, with treatment often based on psychoanalysis and other talking cures.[153]
As these psychoanalysts interpreted the asthmatic wheeze as the suppressed cry of the child for its mother,they considered the treatment of depression to be especially important for individuals with asthma.[153]
Notes
1. ^ GINA 2011, p. 182. ^ NHLBI Guideline 2007, pp. 11–123. ^ British Guideline 2009, p. 44. ^ a b c Martinez FD (2007). "Genes, environments, development and asthma: a reappraisal". Eur Respir J 29 (1):
179–84. doi:10.1183/09031936.00087906 (http://dx.doi.org/10.1183%2F09031936.00087906). PMID 17197483(//www.ncbi.nlm.nih.gov/pubmed/17197483).
5. ^ a b Lemanske RF, Busse WW (February 2010). "Asthma: clinical expression and molecular mechanisms"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2853245). J. Allergy Clin. Immunol. 125 (2 Suppl 2): S95–102.doi:10.1016/j.jaci.2009.10.047 (http://dx.doi.org/10.1016%2Fj.jaci.2009.10.047). PMC 2853245(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2853245). PMID 20176271(//www.ncbi.nlm.nih.gov/pubmed/20176271).
6. ^ a b c Yawn BP (September 2008). "Factors accounting for asthma variability: achieving optimal symptom controlfor individual patients" (http://www.webcitation.org/5nySCf5x8). Primary Care Respiratory Journal 17 (3): 138–147. doi:10.3132/pcrj.2008.00004 (http://dx.doi.org/10.3132%2Fpcrj.2008.00004). PMID 18264646(//www.ncbi.nlm.nih.gov/pubmed/18264646). Archived from the original(http://www.thepcrj.org/journ/vol17/17_3_138_147.pdf) on 2010-03-04.
7. ^ a b Kumar, Vinay; Abbas, Abul K; Fausto, Nelson et al., eds. (2010). Robbins and Cotran pathologic basis ofdisease (8th ed.). Saunders. p. 688. ISBN 978-1-4160-3121-5. OCLC 643462931(//www.worldcat.org/oclc/643462931).
8. ^ Stedman's Medical Dictionary (28 ed.). Lippincott Williams and Wilkins. 2005. ISBN 0-7817-3390-1.9. ^ a b c d NHLBI Guideline 2007, p. 214
10. ^ a b c NHLBI Guideline 2007, pp. 373–37511. ^ NHLBI Guideline 2007, pp. 169–17212. ^ GINA 2011, p. 7113. ^ GINA 2011, p. 3314. ^ a b "World Health Organization Fact Sheet Fact sheet No 307: Asthma"
(http://web.archive.org/web/20110629035454/http://www.who.int/mediacentre/factsheets/fs307/en/). 2011.Retrieved Jan 17th,2013.
15. ^ a b c GINA 2011, p. 316. ^ a b c d e f g h i j GINA 2011, pp. 2–517. ^ Jindal, editor-in-chief SK. Textbook of pulmonary and critical care medicine (http://books.google.ca/books?
id=EvGTw3wn-zEC&pg=PA242). New Delhi: Jaypee Brothers Medical Publishers. p. 242. ISBN 978-93-5025-073-0.
18. ^ George, Ronald B. (2005). Chest medicine : essentials of pulmonary and critical care medicine(http://books.google.ca/books?id=ZzlX2zJMbdgC&pg=PA62) (5th ed. ed.). Philadelphia, PA: Lippincott Williams& Wilkins. p. 62. ISBN 978-0-7817-5273-2.
19. ^ British Guideline 2009, p. 14

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 14/22
20. ^ GINA 2011, pp. 8–921. ^ Boulet LP (April 2009). "Influence of comorbid conditions on asthma". Eur Respir J 33 (4): 897–906.
doi:10.1183/09031936.00121308 (http://dx.doi.org/10.1183%2F09031936.00121308). PMID 19336592(//www.ncbi.nlm.nih.gov/pubmed/19336592).
22. ^ Boulet, LP; Boulay, MÈ (2011 Jun). "Asthma-related comorbidities.". Expert review of respiratory medicine 5(3): 377–93. PMID 21702660 (//www.ncbi.nlm.nih.gov/pubmed/21702660).
23. ^ a b editors, Andrew Harver, Harry Kotses, (2010). Asthma, health and society a public health perspective(http://books.google.ca/books?id=nkP8_h_ewLMC&pg=PA315). New York: Springer. p. 315. ISBN 978-0-387-78285-0.
24. ^ Thomas, M; Bruton, A; Moffat, M; Cleland, J (2011 Sep). "Asthma and psychological dysfunction.". Primarycare respiratory journal : journal of the General Practice Airways Group 20 (3): 250–6. PMID 21674122(//www.ncbi.nlm.nih.gov/pubmed/21674122).
25. ^ Miller, RL; Ho SM (March 2008). "Environmental epigenetics and asthma: current concepts and call for studies"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2267336). American Journal of Respiratory and Critical CareMedicine 177 (6): 567–573. doi:10.1164/rccm.200710-1511PP (http://dx.doi.org/10.1164%2Frccm.200710-1511PP). PMC 2267336 (//www.ncbi.nlm.nih.gov/pmc/articles/PMC2267336). PMID 18187692(//www.ncbi.nlm.nih.gov/pubmed/18187692).
26. ^ Choudhry S, Seibold MA, Borrell LN "et al." (2007). "Dissecting complex diseases in complex populations:asthma in latino americans" (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2647623). Proc Am Thorac Soc 4 (3):226–33. doi:10.1513/pats.200701-029AW (http://dx.doi.org/10.1513%2Fpats.200701-029AW). PMC 2647623(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2647623). PMID 17607004(//www.ncbi.nlm.nih.gov/pubmed/17607004).
27. ^ Dietert, RR (2011 Sep). "Maternal and childhood asthma: risk factors, interactions, and ramifications.".Reproductive toxicology (Elmsford, N.Y.) 32 (2): 198–204. PMID 21575714(//www.ncbi.nlm.nih.gov/pubmed/21575714).
28. ^ Kelly, FJ; Fussell, JC (2011 Aug). "Air pollution and airway disease.". Clinical and experimental allergy :journal of the British Society for Allergy and Clinical Immunology 41 (8): 1059–71. PMID 21623970(//www.ncbi.nlm.nih.gov/pubmed/21623970).
29. ^ GINA 2011, p. 630. ^ GINA 2011, p. 6131. ^ a b Gold DR, Wright R (2005). "Population disparities in asthma". Annu Rev Public Health 26: 89–113.
doi:10.1146/annurev.publhealth.26.021304.144528(http://dx.doi.org/10.1146%2Fannurev.publhealth.26.021304.144528). PMID 15760282(//www.ncbi.nlm.nih.gov/pubmed/15760282).
32. ^ McGwin, G; Lienert, J; Kennedy, JI (2010 Mar). "Formaldehyde exposure and asthma in children: a systematicreview.". Environmental health perspectives 118 (3): 313–7. PMID 20064771(//www.ncbi.nlm.nih.gov/pubmed/20064771).
33. ^ Jaakkola JJ, Knight TL. (July 2008). "The role of exposure to phthalates from polyvinyl chloride products in thedevelopment of asthma and allergies: a systematic review and meta-analysis"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2453150). Environ Health Perspect 116 (7): 845–53.doi:10.1289/ehp.10846 (http://dx.doi.org/10.1289%2Fehp.10846). PMC 2453150(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2453150). PMID 18629304(//www.ncbi.nlm.nih.gov/pubmed/18629304).
34. ^ Bornehag, CG; Nanberg, E (2010 Apr). "Phthalate exposure and asthma in children.". International journal ofandrology 33 (2): 333–45. PMID 20059582 (//www.ncbi.nlm.nih.gov/pubmed/20059582).
35. ^ Liu AH (2004). "Something old, something new: indoor endotoxin, allergens and asthma". Paediatr Respir Rev5 (Suppl A): S65–71. doi:10.1016/S1526-0542(04)90013-9 (http://dx.doi.org/10.1016%2FS1526-0542%2804%2990013-9). PMID 14980246 (//www.ncbi.nlm.nih.gov/pubmed/14980246).
36. ^ Ahluwalia, SK; Matsui, EC (April 2011). "The indoor environment and its effects on childhood asthma.".Current opinion in allergy and clinical immunology 11 (2): 137–43. PMID 21301330(//www.ncbi.nlm.nih.gov/pubmed/21301330).
37. ^ Arshad, SH (January 2010). "Does exposure to indoor allergens contribute to the development of asthma and
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 15/22
37. ^ Arshad, SH (January 2010). "Does exposure to indoor allergens contribute to the development of asthma andallergy?". Current allergy and asthma reports 10 (1): 49–55. PMID 20425514(//www.ncbi.nlm.nih.gov/pubmed/20425514).
38. ^ Custovic, A; Simpson, A (2012). "The role of inhalant allergens in allergic airways disease.". Journal ofinvestigational allergology & clinical immunology : official organ of the International Association of Asthmology(INTERASMA) and Sociedad Latinoamericana de Alergia e Inmunologia 22 (6): 393–401; qiuz follow 401.PMID 23101182 (//www.ncbi.nlm.nih.gov/pubmed/23101182).
39. ^ a b PC Gøtzsche, HK Johansen (2008). "House dust mite control measures for asthma". In Gøtzsche, Peter C.Cochrane Database Syst Rev (2): CD001187. doi:10.1002/14651858.CD001187.pub3(http://dx.doi.org/10.1002%2F14651858.CD001187.pub3). PMID 18425868(//www.ncbi.nlm.nih.gov/pubmed/18425868).
40. ^ a b NHLBI Guideline 2007, p. 1141. ^ a b c d e f g h i j k l Murray and Nadel's textbook of respiratory medicine. (5th ed. ed.). Philadelphia, PA:
Saunders/Elsevier. 2010. pp. Chapter 38. ISBN 1-4160-4710-7.42. ^ Ramsey, CD; Celedón JC (January 2005). "The hygiene hypothesis and asthma". Current Opinion in Pulmonary
Medicine 11 (1): 14–20. doi:10.1097/01.mcp.0000145791.13714.ae(http://dx.doi.org/10.1097%2F01.mcp.0000145791.13714.ae). PMID 15591883(//www.ncbi.nlm.nih.gov/pubmed/15591883).
43. ^ Bufford, JD; Gern JE (May 2005). "The hygiene hypothesis revisited". Immunology and Allergy Clinics of NorthAmerica 25 (2): 247–262. doi:10.1016/j.iac.2005.03.005 (http://dx.doi.org/10.1016%2Fj.iac.2005.03.005).PMID 15878454 (//www.ncbi.nlm.nih.gov/pubmed/15878454).
44. ^ a b Brooks, C; Pearce, N; Douwes, J (2013 Feb). "The hygiene hypothesis in allergy and asthma: an update.".Current opinion in allergy and clinical immunology 13 (1): 70–7. PMID 23103806(//www.ncbi.nlm.nih.gov/pubmed/23103806).
45. ^ Murk, W; Risnes, KR, Bracken, MB (2011 Jun). "Prenatal or early-life exposure to antibiotics and risk ofchildhood asthma: a systematic review.". Pediatrics 127 (6): 1125–38. doi:10.1542/peds.2010-2092(http://dx.doi.org/10.1542%2Fpeds.2010-2092). PMID 21606151 (//www.ncbi.nlm.nih.gov/pubmed/21606151).
46. ^ British Guideline 2009, p. 7247. ^ Neu, J; Rushing, J (2011 Jun). "Cesarean versus vaginal delivery: long-term infant outcomes and the hygiene
hypothesis.". Clinics in perinatology 38 (2): 321–31. PMID 21645799(//www.ncbi.nlm.nih.gov/pubmed/21645799).
48. ^ Von Hertzen, LC; Haahtela, T (2004 Feb). "Asthma and atopy -the price of affluence?". Allergy 59 (2): 124–37.PMID 14763924 (//www.ncbi.nlm.nih.gov/pubmed/14763924).
49. ^ a b Martinez FD (2007). "CD14, endotoxin, and asthma risk: actions and interactions"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2647622). Proc Am Thorac Soc 4 (3): 221–5.doi:10.1513/pats.200702-035AW (http://dx.doi.org/10.1513%2Fpats.200702-035AW). PMC 2647622(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2647622). PMID 17607003(//www.ncbi.nlm.nih.gov/pubmed/17607003).
50. ^ a b c Elward, Graham Douglas, Kurtis S. (2010). Asthma (http://books.google.ca/books?id=gS4BsugTBvoC&pg=PA27). London: Manson Pub. pp. 27–29. ISBN 978-1-84076-513-7.
51. ^ a b c Ober C, Hoffjan S (2006). "Asthma genetics 2006: the long and winding road to gene discovery". GenesImmun 7 (2): 95–100. doi:10.1038/sj.gene.6364284 (http://dx.doi.org/10.1038%2Fsj.gene.6364284).PMID 16395390 (//www.ncbi.nlm.nih.gov/pubmed/16395390).
52. ^ Halapi, E; Bjornsdottir, US (2009 Jan). "Overview on the current status of asthma genetics.". The clinicalrespiratory journal 3 (1): 2–7. PMID 20298365 (//www.ncbi.nlm.nih.gov/pubmed/20298365).
53. ^ a b Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis:Mosby. ISBN 1-4160-2999-0.
54. ^ GINA 2011, p. 455. ^ Beuther DA (January 2010). "Recent insight into obesity and asthma". Curr Opin Pulm Med 16 (1): 64–70.
doi:10.1097/MCP.0b013e3283338fa7 (http://dx.doi.org/10.1097%2FMCP.0b013e3283338fa7). PMID 19844182(//www.ncbi.nlm.nih.gov/pubmed/19844182).
56. ^ Holguin F, Fitzpatrick A (March 2010). "Obesity, asthma, and oxidative stress". J. Appl. Physiol. 108 (3): 754–9. doi:10.1152/japplphysiol.00702.2009 (http://dx.doi.org/10.1152%2Fjapplphysiol.00702.2009). PMID 19926826
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 16/22
9. doi:10.1152/japplphysiol.00702.2009 (http://dx.doi.org/10.1152%2Fjapplphysiol.00702.2009). PMID 19926826(//www.ncbi.nlm.nih.gov/pubmed/19926826).
57. ^ Wood LG, Gibson PG (July 2009). "Dietary factors lead to innate immune activation in asthma". Pharmacol.Ther. 123 (1): 37–53. doi:10.1016/j.pharmthera.2009.03.015(http://dx.doi.org/10.1016%2Fj.pharmthera.2009.03.015). PMID 19375453(//www.ncbi.nlm.nih.gov/pubmed/19375453).
58. ^ O'Rourke ST (October 2007). "Antianginal actions of beta-adrenoceptor antagonists"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2064893). Am J Pharm Educ 71 (5): 95. PMC 2064893(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2064893). PMID 17998992(//www.ncbi.nlm.nih.gov/pubmed/17998992).
59. ^ Salpeter, S; Ormiston, T; Salpeter, E (2001). "Cardioselective beta-blocker use in patients with reversible airwaydisease.". Cochrane database of systematic reviews (Online) (2): CD002992. PMID 11406056(//www.ncbi.nlm.nih.gov/pubmed/11406056).
60. ^ Covar, RA; Macomber, BA; Szefler, SJ (2005 Feb). "Medications as asthma trigers.". Immunology and allergyclinics of North America 25 (1): 169–90. PMID 15579370 (//www.ncbi.nlm.nih.gov/pubmed/15579370).
61. ^ a b c d Baxi SN, Phipatanakul W (April 2010). "The role of allergen exposure and avoidance in asthma"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2975603). Adolesc Med State Art Rev 21 (1): 57–71, viii–ix.PMC 2975603 (//www.ncbi.nlm.nih.gov/pmc/articles/PMC2975603). PMID 20568555(//www.ncbi.nlm.nih.gov/pubmed/20568555).
62. ^ Chen E, Miller GE (2007). "Stress and inflammation in exacerbations of asthma"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2077080). Brain Behav Immun. 21 (8): 993–9.doi:10.1016/j.bbi.2007.03.009 (http://dx.doi.org/10.1016%2Fj.bbi.2007.03.009). PMC 2077080(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2077080). PMID 17493786(//www.ncbi.nlm.nih.gov/pubmed/17493786).
63. ^ a b NHLBI Guideline 2007, p. 4264. ^ GINA 2011, p. 2065. ^ American Academy of Allergy, Asthma, and Immunology, "Five things physicians and patients should question"
(http://choosingwisely.org/wp-content/uploads/2012/04/5things_12_factsheet_AAAAI.pdf), Choosing wisely: aninitiative of the ABIM Foundation (American Academy of Allergy, Asthma, and Immunology), retrieved August14, 2012
66. ^ Third Expert Panel on the Diagnosis and Management of Asthma (2007). Guidelines for the diagnosis andmanagement of asthma (http://www.ncbi.nlm.nih.gov/books/NBK7232/). National Heart, Lung, and Blood Institute(US).
67. ^ Perez, LL (March–April 2013). "Office spirometry". Osteopathic Family Physician 5 (2): 65–69.doi:10.1016/j.osfp.2012.09.003 (http://dx.doi.org/10.1016%2Fj.osfp.2012.09.003).
68. ^ NHLBI Guideline 2007, p. 5869. ^ Pinnock H, Shah R (2007). "Asthma" (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1853223). BMJ 334
(7598): 847–50. doi:10.1136/bmj.39140.634896.BE (http://dx.doi.org/10.1136%2Fbmj.39140.634896.BE).PMC 1853223 (//www.ncbi.nlm.nih.gov/pmc/articles/PMC1853223). PMID 17446617(//www.ncbi.nlm.nih.gov/pubmed/17446617).
70. ^ NHLBI Guideline 2007, p. 5971. ^ a b Moore WC, Pascual RM (June 2010). "Update in asthma 2009". American Journal of Respiratory and Critical
Care Medicine 181 (11): 1181–7. doi:10.1164/rccm.201003-0321UP (http://dx.doi.org/10.1164%2Frccm.201003-0321UP). PMID 20516492 (//www.ncbi.nlm.nih.gov/pubmed/20516492).
72. ^ a b Self, Timothy; Chrisman, Cary; Finch, Christopher (2009). "22. Asthma". In Mary Anne Koda-Kimble,Brian K Alldredge, et al. Applied therapeutics: the clinical use of drugs (9th ed.). Philadelphia: LippincottWilliams & Wilkins. OCLC 230848069 (//www.worldcat.org/oclc/230848069).
73. ^ Delacourt, C (June 2004). "Conséquences bronchiques de l'asthme non traité" [Bronchial changes in untreatedasthma]. Archives de Pédiatrie 11 (Suppl. 2): 71s–73s. PMID 15301800(//www.ncbi.nlm.nih.gov/pubmed/15301800).
74. ^ Schiffman, George (18 December 2009). "Chronic obstructive pulmonary disease"(http://www.medicinenet.com/chronic_obstructive_pulmonary_disease_copd/article.htm). MedicineNet. Archived
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 17/22
(http://www.medicinenet.com/chronic_obstructive_pulmonary_disease_copd/article.htm). MedicineNet. Archived(http://web.archive.org/web/20100828011049/http://www.medicinenet.com/chronic_obstructive_pulmonary_disease_copd/article.htm) from the original on 28 August 2010. Retrieved 2 September 2010.
75. ^ a b c d British Guideline 2009, p. 5476. ^ Barnes, PJ (2008). "Asthma". In Fauci, Anthony S; Braunwald, E,; Kasper, DL. Harrison's Principles of Internal
Medicine (17th ed.). New York: McGraw-Hill. pp. 1596–1607. ISBN 978-0-07-146633-2.77. ^ Maitre B, Similowski T, Derenne JP (September 1995). "Physical examination of the adult patient with
respiratory diseases: inspection and palpation" (http://erj.ersjournals.com/content/8/9/1584.long). Eur. Respir. J. 8(9): 1584–93. PMID 8575588 (//www.ncbi.nlm.nih.gov/pubmed/8575588).
78. ^ Werner, HA (June 2001). "Status asthmaticus in children: a review". Chest 119 (6): 1596–1607.doi:10.1378/chest.119.6.1913 (http://dx.doi.org/10.1378%2Fchest.119.6.1913). PMID 11399724(//www.ncbi.nlm.nih.gov/pubmed/11399724).
79. ^ a b Shiber JR, Santana J (May 2006). "Dyspnea". Med. Clin. North Am. 90 (3): 453–79.doi:10.1016/j.mcna.2005.11.006 (http://dx.doi.org/10.1016%2Fj.mcna.2005.11.006). PMID 16473100(//www.ncbi.nlm.nih.gov/pubmed/16473100).
80. ^ a b Shah, R; Saltoun, CA (2012 May–Jun). "Chapter 14: Acute severe asthma (status asthmaticus).". Allergy andasthma proceedings : the official journal of regional and state allergy societies. 33 Suppl 1: S47–50.PMID 22794687 (//www.ncbi.nlm.nih.gov/pubmed/22794687).
81. ^ a b c Khan, DA (2012 Jan–Feb). "Exercise-induced bronchoconstriction: burden and prevalence.". Allergy andasthma proceedings : the official journal of regional and state allergy societies 33 (1): 1–6. PMID 22370526(//www.ncbi.nlm.nih.gov/pubmed/22370526).
82. ^ GINA 2011, p. 1783. ^ Carlsen, KH; Anderson, SD; Bjermer, L; Bonini, S; Brusasco, V; Canonica, W; Cummiskey, J; Delgado, L; Del
Giacco, SR; Drobnic, F; Haahtela, T; Larsson, K; Palange, P; Popov, T; van Cauwenberge, P; EuropeanRespiratory, Society; European Academy of Allergy and Clinical, Immunology; GA(2)LEN, (2008 May)."Treatment of exercise-induced asthma, respiratory and allergic disorders in sports and the relationship to doping:Part II of the report from the Joint Task Force of European Respiratory Society (ERS) and European Academy ofAllergy and Clinical Immunology (EAACI) in cooperation with GA(2)LEN.". Allergy 63 (5): 492–505.PMID 18394123 (//www.ncbi.nlm.nih.gov/pubmed/18394123).
84. ^ Kindermann, W (2007). "Do inhaled beta(2)-agonists have an ergogenic potential in non-asthmatic competitiveathletes?". Sports medicine (Auckland, N.Z.) 37 (2): 95–102. PMID 17241101(//www.ncbi.nlm.nih.gov/pubmed/17241101).
85. ^ Pluim, BM; de Hon, O; Staal, JB; Limpens, J; Kuipers, H; Overbeek, SE; Zwinderman, AH; Scholten, RJ (2011Jan 1). "β₂-Agonists and physical performance: a systematic review and meta-analysis of randomized controlledtrials.". Sports medicine (Auckland, N.Z.) 41 (1): 39–57. PMID 21142283(//www.ncbi.nlm.nih.gov/pubmed/21142283).
86. ^ a b c Baur, X; Aasen, TB; Burge, PS; Heederik, D; Henneberger, PK; Maestrelli, P; Schlünssen, V; Vandenplas,O; Wilken, D; ERS Task Force on the Management of Work-related, Asthma (2012 Jun 1). "The management ofwork-related asthma guidelines: a broader perspective.". European respiratory review : an official journal of theEuropean Respiratory Society 21 (124): 125–39. PMID 22654084 (//www.ncbi.nlm.nih.gov/pubmed/22654084).
87. ^ Kunnamo, ed.-in-chief: Ilkka (2005). Evidence-based medicine guidelines (http://books.google.ca/books?id=frYEiHYtOv0C&pg=PA214). Chichester: Wiley. p. 214. ISBN 978-0-470-01184-3.
88. ^ Kraft, editors, Mario Castro, Monica (2008). Clinical asthma (http://books.google.ca/books?id=y9WYwLVn7pgC&pg=PT1185). Philadelphia: Mosby / Elsevier. pp. Chapter 42. ISBN 978-0-323-07081-2.
89. ^ NHLBI Guideline 2007, p. 4690. ^ Gibson PG, McDonald VM, Marks GB (September 2010). "Asthma in older adults". Lancet 376 (9743): 803–13.
doi:10.1016/S0140-6736(10)61087-2 (http://dx.doi.org/10.1016%2FS0140-6736%2810%2961087-2).PMID 20816547 (//www.ncbi.nlm.nih.gov/pubmed/20816547).
91. ^ Hargreave FE; Parameswaran K (August 2006). "Asthma, COPD and bronchitis are just components of airwaydisease" (http://erj.ersjournals.com/content/28/2/264.full). European Respiratory Journal 28 (2): 264–267.doi:10.1183/09031936.06.00056106 (http://dx.doi.org/10.1183%2F09031936.06.00056106). PMID 16880365(//www.ncbi.nlm.nih.gov/pubmed/16880365).
92. ^ Diaz, P. Knoell (2009). "23. Chronic obstructive pulmonary disease". Applied therapeutics: the clinical use of
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 18/22
92. ^ Diaz, P. Knoell (2009). "23. Chronic obstructive pulmonary disease". Applied therapeutics: the clinical use ofdrugs (9th ed.). Philadelphia: Lippincott Williams & Wilkins.
93. ^ a b NHLBI Guideline 2007, pp. 184–594. ^ Lodge, CJ; Allen, KJ; Lowe, AJ; Hill, DJ; Hosking, CS; Abramson, MJ; Dharmage, SC (2012). "Perinatal cat
and dog exposure and the risk of asthma and allergy in the urban environment: a systematic review of longitudinalstudies.". Clinical & developmental immunology 2012: 176484. PMID 22235226(//www.ncbi.nlm.nih.gov/pubmed/22235226).
95. ^ Chen, CM; Tischer, C; Schnappinger, M; Heinrich, J (2010 Jan). "The role of cats and dogs in asthma andallergy—a systematic review.". International journal of hygiene and environmental health 213 (1): 1–31.PMID 20053584 (//www.ncbi.nlm.nih.gov/pubmed/20053584).
96. ^ a b Prescott, SL; Tang, ML; Australasian Society of Clinical Immunology and, Allergy (2005 May 2). "TheAustralasian Society of Clinical Immunology and Allergy position statement: Summary of allergy prevention inchildren.". The Medical journal of Australia 182 (9): 464–7. PMID 15865590(//www.ncbi.nlm.nih.gov/pubmed/15865590).
97. ^ Ripoll, Brian C. Leutholtz, Ignacio. Exercise and disease management (http://books.google.ch/books?id=eAn9-bm_pi8C&pg=PA100) (2nd ed. ed.). Boca Raton: CRC Press. p. 100. ISBN 978-1-4398-2759-8.
98. ^ GINA 2011, p. 5699. ^ a b c d e f NHLBI Guideline 2007, p. 213
100. ^ a b "British Guideline on the Management of Asthma" (http://www.sign.ac.uk/pdf/sign101.pdf) (PDF). ScottishIntercollegiate Guidelines Network. 2008. Archived(http://web.archive.org/web/20080819203455/http://www.sign.ac.uk/pdf/sign101.pdf) from the original on 19August 2008. Retrieved 2008-08-04.
101. ^ NHLBI Guideline 2007, p. 69102. ^ Thomson NC, Spears M (2005). "The influence of smoking on the treatment response in patients with asthma".
Curr Opin Allergy Clin Immunol 5 (1): 57–63. doi:10.1097/00130832-200502000-00011(http://dx.doi.org/10.1097%2F00130832-200502000-00011). PMID 15643345(//www.ncbi.nlm.nih.gov/pubmed/15643345).
103. ^ Stapleton M, Howard-Thompson A, George C, Hoover RM, Self TH (2011). "Smoking and asthma.". J AmBoard Fam Med 24 (3): 313–22. doi:10.3122/jabfm.2011.03.100180(http://dx.doi.org/10.3122%2Fjabfm.2011.03.100180). PMID 21551404(//www.ncbi.nlm.nih.gov/pubmed/21551404).
104. ^ Rodrigo GJ, Nannini LJ (2006). "Comparison between nebulized adrenaline and beta2 agonists for the treatmentof acute asthma. A meta-analysis of randomized trials". Am J Emerg Med 24 (2): 217–22.doi:10.1016/j.ajem.2005.10.008 (http://dx.doi.org/10.1016%2Fj.ajem.2005.10.008). PMID 16490653(//www.ncbi.nlm.nih.gov/pubmed/16490653).
105. ^ NHLBI Guideline 2007, p. 351106. ^ NHLBI Guideline 2007, p. 218107. ^ a b Ducharme, FM; Ni Chroinin, M; Greenstone, I; Lasserson, TJ (2010 May 12). "Addition of long-acting
beta2-agonists to inhaled corticosteroids versus same dose inhaled corticosteroids for chronic asthma in adults andchildren.". Cochrane database of systematic reviews (Online) (5): CD005535. PMID 20464739(//www.ncbi.nlm.nih.gov/pubmed/20464739).
108. ^ Ducharme, FM; Ni Chroinin, M; Greenstone, I; Lasserson, TJ (2010 Apr 14). "Addition of long-acting beta2-agonists to inhaled steroids versus higher dose inhaled corticosteroids in adults and children with persistentasthma.". Cochrane database of systematic reviews (Online) (4): CD005533. PMID 20393943(//www.ncbi.nlm.nih.gov/pubmed/20393943).
109. ^ a b Fanta CH (March 2009). "Asthma". New England Journal of Medicine 360 (10): 1002–14.doi:10.1056/NEJMra0804579 (http://dx.doi.org/10.1056%2FNEJMra0804579). PMID 19264689(//www.ncbi.nlm.nih.gov/pubmed/19264689).
110. ^ Cates, CJ; Cates, MJ (2012 Apr 18). "Regular treatment with formoterol for chronic asthma: serious adverseevents.". Cochrane database of systematic reviews (Online) 4: CD006923. PMID 22513944(//www.ncbi.nlm.nih.gov/pubmed/22513944).
111. ^ Cates, CJ; Cates, MJ (2008 Jul 16). "Regular treatment with salmeterol for chronic asthma: serious adverse

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 19/22
111. ^ Cates, CJ; Cates, MJ (2008 Jul 16). "Regular treatment with salmeterol for chronic asthma: serious adverseevents.". Cochrane database of systematic reviews (Online) (3): CD006363. PMID 18646149(//www.ncbi.nlm.nih.gov/pubmed/18646149).
112. ^ GINA 2011, p. 74113. ^ Watts, K; Chavasse, RJ (2012 May 16). "Leukotriene receptor antagonists in addition to usual care for acute
asthma in adults and children.". Cochrane database of systematic reviews (Online) 5: CD006100. PMID 22592708(//www.ncbi.nlm.nih.gov/pubmed/22592708).
114. ^ British Guideline 2009, p. 43115. ^ NHLBI Guideline 2007, p. 250116. ^ a b Rachelefsky, G (2009 Jan). "Inhaled corticosteroids and asthma control in children: assessing impairment and
risk.". Pediatrics 123 (1): 353–66. doi:10.1542/peds.2007-3273 (http://dx.doi.org/10.1542%2Fpeds.2007-3273).PMID 19117903 (//www.ncbi.nlm.nih.gov/pubmed/19117903).
117. ^ Dahl R (August 2006). "Systemic side effects of inhaled corticosteroids in patients with asthma". Respir Med 100(8): 1307–17. doi:10.1016/j.rmed.2005.11.020 (http://dx.doi.org/10.1016%2Fj.rmed.2005.11.020).PMID 16412623 (//www.ncbi.nlm.nih.gov/pubmed/16412623).
118. ^ a b c Rodrigo GJ, Rodrigo C, Hall JB (2004). "Acute asthma in adults: a review". Chest 125 (3): 1081–102.doi:10.1378/chest.125.3.1081 (http://dx.doi.org/10.1378%2Fchest.125.3.1081). PMID 15006973(//www.ncbi.nlm.nih.gov/pubmed/15006973).
119. ^ Noppen, M. (August 2002). "Magnesium Treatment for Asthma : Where Do We Stand?". Chest 122 (2): 396–8.doi:10.1378/chest.122.2.396 (http://dx.doi.org/10.1378%2Fchest.122.2.396). PMID 12171805(//www.ncbi.nlm.nih.gov/pubmed/12171805).
120. ^ GINA 2011, p. 37121. ^ NHLBI Guideline 2007, p. 399122. ^ a b Castro, M; Musani, AI, Mayse, ML, Shargill, NS (2010 Apr). "Bronchial thermoplasty: a novel technique in
the treatment of severe asthma.". Therapeutic advances in respiratory disease 4 (2): 101–16.doi:10.1177/1753465810367505 (http://dx.doi.org/10.1177%2F1753465810367505). PMID 20435668(//www.ncbi.nlm.nih.gov/pubmed/20435668).
123. ^ GINA 2011, p. 70124. ^ Lin, Sandra (27). "Sublingual Immunotherapy for the Treatment of Allergic Rhinoconjunctivitis and Asthma A
Systematic Review". JAMA 309 (12): 1278–1288. doi:10.1001/jama.2013.2049(http://dx.doi.org/10.1001%2Fjama.2013.2049).
125. ^ Blanc PD, Trupin L, Earnest G, Katz PP, Yelin EH, Eisner MD (2001). "Alternative therapies among adultswith a reported diagnosis of asthma or rhinosinusitis : data from a population-based survey". Chest 120 (5): 1461–7. doi:10.1378/chest.120.5.1461 (http://dx.doi.org/10.1378%2Fchest.120.5.1461). PMID 11713120(//www.ncbi.nlm.nih.gov/pubmed/11713120).
126. ^ Shenfield G, Lim E, Allen H (2002). "Survey of the use of complementary medicines and therapies in childrenwith asthma". J Paediatr Child Health 38 (3): 252–7. doi:10.1046/j.1440-1754.2002.00770.x(http://dx.doi.org/10.1046%2Fj.1440-1754.2002.00770.x). PMID 12047692(//www.ncbi.nlm.nih.gov/pubmed/12047692).
127. ^ Kaur, B; Rowe BH, Arnold E (2009). "Vitamin C supplementation for asthma". In Arnold, Elizabeth. CochraneDatabase Syst Rev (1): CD000993. doi:10.1002/14651858.CD000993.pub3(http://dx.doi.org/10.1002%2F14651858.CD000993.pub3). PMID 19160185(//www.ncbi.nlm.nih.gov/pubmed/19160185). Unknown parameter |unused_data= ignored (help)
128. ^ a b NHLBI Guideline 2007, p. 240129. ^ McCarney RW, Brinkhaus B, Lasserson TJ, Linde K (2004). "Acupuncture for chronic asthma". In McCarney,
Robert W. Cochrane Database Syst Rev (1): CD000008. doi:10.1002/14651858.CD000008.pub2(http://dx.doi.org/10.1002%2F14651858.CD000008.pub2). PMID 14973944(//www.ncbi.nlm.nih.gov/pubmed/14973944).
130. ^ Blackhall, K; Appleton, S; Cates, CJ (2012 Sep 12). "Ionisers for chronic asthma.". Cochrane database ofsystematic reviews (Online) 9: CD002986. PMID 22972060 (//www.ncbi.nlm.nih.gov/pubmed/22972060).
131. ^ Hondras MA, Linde K, Jones AP (2005). "Manual therapy for asthma". In Hondras, Maria A. CochraneDatabase Syst Rev (2): CD001002. doi:10.1002/14651858.CD001002.pub2(http://dx.doi.org/10.1002%2F14651858.CD001002.pub2). PMID 15846609

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 20/22
(http://dx.doi.org/10.1002%2F14651858.CD001002.pub2). PMID 15846609(//www.ncbi.nlm.nih.gov/pubmed/15846609).
132. ^ "WHO Disease and injury country estimates"(http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html). World HealthOrganization. 2009. Archived(http://web.archive.org/web/20091111101009/http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html) from the original on 11 November 2009. Retrieved November 11, 2009.
133. ^ Sergel, Michelle J.; Cydulka, Rita K. (September 2009). "Ch. 75: Asthma" (http://books.google.com/books?id=Idb0Z658lFQC&pg=PT465). In Wolfson, Allan B.; Harwood-Nuss, Ann. Harwood-Nuss' Clinical Practice ofEmergency Medicine (5th ed.). Lippincott Williams & Wilkins. pp. 432–. ISBN 978-0-7817-8943-1.
134. ^ NHLBI Guideline 2007, p. 1135. ^ Organization, World Health (2008). The global burden of disease : 2004 update. ([Online-Ausg.] ed.). Geneva,
Switzerland: World Health Organization. p. 35. ISBN 978-92-4-156371-0.136. ^ Maddox L, Schwartz DA (2002). "The pathophysiology of asthma". Annu. Rev. Med. 53: 477–98.
doi:10.1146/annurev.med.53.082901.103921 (http://dx.doi.org/10.1146%2Fannurev.med.53.082901.103921).PMID 11818486 (//www.ncbi.nlm.nih.gov/pubmed/11818486).
137. ^ Beckett PA, Howarth PH (2003). "Pharmacotherapy and airway remodelling in asthma?"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1746582). Thorax 58 (2): 163–74. doi:10.1136/thorax.58.2.163(http://dx.doi.org/10.1136%2Fthorax.58.2.163). PMC 1746582(//www.ncbi.nlm.nih.gov/pmc/articles/PMC1746582). PMID 12554904(//www.ncbi.nlm.nih.gov/pubmed/12554904).
138. ^ World Health Organization. "WHO: Asthma" (http://www.who.int/mediacentre/factsheets/fs307/en/). Archived(http://web.archive.org/web/20071215181927/http://www.who.int/mediacentre/factsheets/fs307/en/) from theoriginal on 15 December 2007. Retrieved 2007-12-29.
139. ^ Bush A, Menzies-Gow A (December 2009). "Phenotypic differences between pediatric and adult asthma". ProcAm Thorac Soc 6 (8): 712–9. doi:10.1513/pats.200906-046DP (http://dx.doi.org/10.1513%2Fpats.200906-046DP).PMID 20008882 (//www.ncbi.nlm.nih.gov/pubmed/20008882).
140. ^ Grant EN, Wagner R, Weiss KB (August 1999). "Observations on emerging patterns of asthma in our society". JAllergy Clin Immunol 104 (2 Pt 2): S1–S9. doi:10.1016/S0091-6749(99)70268-X(http://dx.doi.org/10.1016%2FS0091-6749%2899%2970268-X). PMID 10452783(//www.ncbi.nlm.nih.gov/pubmed/10452783).
141. ^ Anandan C, Nurmatov U, van Schayck OC, Sheikh A (February 2010). "Is the prevalence of asthma declining?Systematic review of epidemiological studies". Allergy 65 (2): 152–67. doi:10.1111/j.1398-9995.2009.02244.x(http://dx.doi.org/10.1111%2Fj.1398-9995.2009.02244.x). PMID 19912154(//www.ncbi.nlm.nih.gov/pubmed/19912154).
142. ^ Bousquet, J; Bousquet, PJ; Godard, P; Daures, JP (2005 Jul). "The public health implications of asthma.".Bulletin of the World Health Organization 83 (7): 548–54. PMID 16175830(//www.ncbi.nlm.nih.gov/pubmed/16175830).
143. ^ Anderson, HR; Gupta R, Strachan DP, Limb ES (January 2007). "50 years of asthma: UK trends from 1955 to2004" (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2111282). Thorax 62 (1): 85–90.doi:10.1136/thx.2006.066407 (http://dx.doi.org/10.1136%2Fthx.2006.066407). PMC 2111282(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2111282). PMID 17189533(//www.ncbi.nlm.nih.gov/pubmed/17189533).
144. ^ Masoli, Matthew (2004). Global Burden of Asthma (http://www.ginasthma.org/pdf/GINABurdenReport.pdf).p. 9.
145. ^ Manniche L (1999). Sacred luxuries: fragrance, aromatherapy, and cosmetics in ancient Egypt. CornellUniversity Press. pp. 49 (http://books.google.com/books?id=ZCgVdm7UKhIC&pg=PA49). ISBN 978-0-8014-3720-5.
146. ^ Thorowgood JC (November 1873). "On bronchial asthma"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2294647). British Medical Journal 2 (673): 600.doi:10.1136/bmj.2.673.600 (http://dx.doi.org/10.1136%2Fbmj.2.673.600). PMC 2294647(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2294647). PMID 20747287(//www.ncbi.nlm.nih.gov/pubmed/20747287).
5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 21/22
(//www.ncbi.nlm.nih.gov/pubmed/20747287).147. ^ Gaskoin G (March 1872). "On the treatment of asthma"
(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2297349). British Medical Journal 1 (587): 339.doi:10.1136/bmj.1.587.339 (http://dx.doi.org/10.1136%2Fbmj.1.587.339). PMC 2297349(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2297349). PMID 20746575(//www.ncbi.nlm.nih.gov/pubmed/20746575).
148. ^ Berkart JB (June 1880). "The treatment of asthma" (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2240555).British Medical Journal 1 (1016): 917–8. doi:10.1136/bmj.1.1016.917(http://dx.doi.org/10.1136%2Fbmj.1.1016.917). PMC 2240555(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2240555). PMID 20749537(//www.ncbi.nlm.nih.gov/pubmed/20749537).Berkart JB (June 1880). "The treatment of asthma" (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2240530).British Medical Journal 1 (1017): 960–2. doi:10.1136/bmj.1.1017.960(http://dx.doi.org/10.1136%2Fbmj.1.1017.960). PMC 2240530(//www.ncbi.nlm.nih.gov/pmc/articles/PMC2240530). PMID 20749546(//www.ncbi.nlm.nih.gov/pubmed/20749546).
149. ^ Bosworth FH (1886). "Hay fever, asthma, and allied affections"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2526599). Transactions of the Annual Meeting of the AmericanClimatological Association 2: 151–70. PMC 2526599 (//www.ncbi.nlm.nih.gov/pmc/articles/PMC2526599).PMID 21407325 (//www.ncbi.nlm.nih.gov/pubmed/21407325).
150. ^ Doig RL (February 1905). "Epinephrin; especially in asthma"(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1650334). California State Journal of Medicine 3 (2): 54–5.PMC 1650334 (//www.ncbi.nlm.nih.gov/pmc/articles/PMC1650334). PMID 18733372(//www.ncbi.nlm.nih.gov/pubmed/18733372).
151. ^ von Mutius, E; Drazen, JM (2012 Mar 1). "A patient with asthma seeks medical advice in 1828, 1928, and2012.". New England Journal of Medicine 366 (9): 827–34. PMID 22375974(//www.ncbi.nlm.nih.gov/pubmed/22375974).
152. ^ Crompton G (2006 Dec). "A brief history of inhaled asthma therapy over the last fifty years". Primary carerespiratory journal : journal of the General Practice Airways Group 15 (6): 326–31. PMID 17092772(//www.ncbi.nlm.nih.gov/pubmed/17092772).
153. ^ a b Opolski M, Wilson I (September 2005). "Asthma and depression: a pragmatic review of the literature andrecommendations for future research" (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1253523). Clin PractEpidemol Ment Health 1: 18. doi:10.1186/1745-0179-1-18 (http://dx.doi.org/10.1186%2F1745-0179-1-18).PMC 1253523 (//www.ncbi.nlm.nih.gov/pmc/articles/PMC1253523). PMID 16185365(//www.ncbi.nlm.nih.gov/pubmed/16185365).
References
National Asthma Education and Prevention Program (NAEPP) (2007). "Expert Panel Report 3: Guidelines for theDiagnosis and Management of Asthma" (http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf) (PDF).National Heart Lung and Blood Institute."British Guideline on the Management of Asthma" (http://www.sign.ac.uk/pdf/sign101.pdf) (PDF). BritishThoracic Society. 2008 (revised 2012)."Global Strategy for Asthma Management and Prevention"(http://www.ginasthma.org/uploads/users/files/GINA_Report2011_May4.pdf) (PDF). Global Initiative for Asthma.2011.
External linksAsthma (http://www.dmoz.org/Health/Conditions_and_Diseases/Respiratory_Disorders/Asthma//) at the OpenDirectory Project

5/13/13 Asthma - Wikipedia, the free encyclopedia
en.wikipedia.org/wiki/Asthma 22/22
Retrieved from "http://en.wikipedia.org/w/index.php?title=Asthma&oldid=550167655"Categories: Asthma Chronic lower respiratory diseases Respiratory therapy
This page was last modified on 13 April 2013 at 15:45.Text is available under the Creative Commons Attribution-ShareAlike License; additional terms mayapply. By using this site, you agree to the Terms of Use and Privacy Policy. Wikipedia® is a registered trademark of the Wikimedia Foundation, Inc., a non-profit organization.