ΘΒΔΒΑ ΔΔΓΑ Η ΔΘ - medicalmate.grmedicalmate.gr/img/cms/Vivliothiki Gia Epaggelmaties...
85
ΘΡΟΜΒΟΔΜΒΟΛΙΚΑ ΔΠΔΙΟΓΙΑ ΣΗ ΜΔΘ ΓΙΑΝΝΗ ΚΑΨΟΚΑΛΤΒΑ ΔΙΓΙΚΔΤΟΜΔΝΟ ΑΝΑΙΘΗΙΟΛΟΓΙΑ Α.Ν.Θ. „ΘΔΑΓΔΝΔΙΟ‟
Transcript of ΘΒΔΒΑ ΔΔΓΑ Η ΔΘ - medicalmate.grmedicalmate.gr/img/cms/Vivliothiki Gia Epaggelmaties...

ΘΡΟΜΒΟΔΜΒΟΛΙΚΑ ΔΠΔΙΟΓΙΑ ΣΗ
ΜΔΘ
ΓΙΑΝΝΗ ΚΑΨΟΚΑΛΤΒΑ
ΔΙΓΙΚΔΤΟΜΔΝΟ ΑΝΑΙΘΗΙΟΛΟΓΙΑ Α.Ν.Θ.
„ΘΔΑΓΔΝΔΙΟ‟

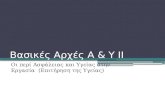
Virchow's triad.
Kyrle P A , Eichinger S Blood 2009;114:1138-1139
©2009 by American Society of Hematology

Biomaterials Research - Manfred Maitz
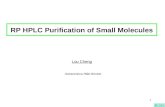
The Blood Clotting Cascade
•Manfred Maitz
FZ-Rossendorf
•www.manfred.maitz-online.de

Biomaterials Research - Manfred Maitz
The Clotting Cascade
FibrinogenFibrin
monomers
Fibrin
polymers
Thrombin

Biomaterials Research - Manfred Maitz
Factor F X
F IXaF IX
F XIaF XI
Surface Contact
Collagen
FXII activator
F XIIaF XII
Intrinsic Pathway
Ca2+
Ca2+
Ca2+
The Clotting Cascade
Factor F X
F VIIF VIIa
F III (Tissue
Thromboplastin)
Tissue/Cell Defect
Extrinsic Pathway
Ca2+
Ca2+
FibrinogenFibrin
monomers
Fibrin
polymers
ThrombinProthrombin I
Factor F Xa
Ca2+
Platelet Factor 3
Crosslinked
Fibrin Meshwork
F XIIIa F XIII
F VF Va
F VIIIaF VIII

Biomaterials Research - Manfred Maitz
Ser:O
H
RN
CO
HN
RC
Serine Proteases
H2O
O
RN
CO-
HN
RC
Ser
HTetraedric
Transition State
RN
C
O OH :O
HSer
Release of the
N-terminal peptide
HN H
RC
O
RN
CO Ser
Break of the
Peptide Bonding
Enzyme-acetyl-
transition-state

Biomaterials Research - Manfred Maitz
The Fibrinolytic System
Fibrin
degradation productsFibrinogen Fibrin-clot
PlasminPlasminogen
T-PA
F XIIa
HMWK
Kallikrein
Urokinase
Streptokinase
Clotting
Cascade

LIFEBLOOD
THE
ThrombosisCHARITY
Venous thromboembolism –
Definition, epidemiology,
aetiology and pathogenesis
These slides were kindly provided by AstraZeneca

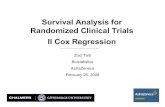
Ulcus crurisChronic PE
PE
Venous thromboembolism
DVT
Post-thromboticsyndrome
Death
Deep vein insufficiency
Pulmonaryhypertension

Deep vein thrombosis
Veins of the leg
Common femoral vein
Thrombus
KneeProximal
Distal

Symptoms of post-thrombotic syndrome – long
“lag-phase” (years)
Pain
Oedema
Discoloration
Varices
Ulceration
Post-thrombotic syndrome

Post-thrombotic syndrome

Ulcus cruris venosum

Severe stasis and ulceration

Embolus
Pulmonaryartery
Pulmonaryvein
Leftatrium
Rightatrium
Rightventricle
Leftventricle

Thrombus formation in a deep vein

A fragment of a thrombus travelling
towards the lungs

Pulmonary embolism
Dyspnea, syncope, hypotension,
cyanosis
Embolus

Pulmonary embolism kills

Pulmonary embolism
Pleuritic pain, cough, haemoptysis
Symptoms may be vague or absent
Embolus

Pulmonary embolismDeep vein thrombosis
Venous thromboembolism (VTE)

Normal PA chest radiograph

Pulmonary hypertension PA chest
radiograph
Prominent pulmonary
artery segmentEnlarged, but “pruned” proximal
pulmonary artery

Venous thromboembolism is a
major problem
DVT
2 million
Pulmonary hypertension
30,000
Silent PE1 million
PE
600,000
Death
100,000
Post-thrombotic syndrome800,000
Hirsh J & Hoak J. Circulation 1996; 93:2212–45
Estimated annual incidence rates in the USA

Classification of level of VTE risk
Surgery in
patients with
multiple risk factors
(age >40, cancer,
prior VTE)
Hip or knee
arthroplasty, hip
fracture surgery
Major trauma,
spinal cord injury
Surgery in
patients 40-60
years with no
additional risk
factors
Minor surgery
in patients with
additional risk
factors
Minor surgery in
patients <40
years with no
additional risk
factors
Surgery in
patients >60
years, or age
40-60 with
additional
risk factors
(prior VTE,
cancer,
molecular
hyper-
coagulability)
Geerts WH et al. Chest 2004;126:338S–400S
Low risk High risk Highest riskModerate risk

Thromboembolic risk categories
Geerts WH et al. Chest 2004;126:338S–400S
Frequency of
fatal PE (%)
Frequency of
calf DVT (%)Category
Frequency of
proximal DVT (%)
Highest risk 40-80 10-20 0.2-5
High risk 20-40 4-8 0.4-1.0
Moderate risk 10-20 2-4 0.1-0.4
Low risk 2 0.4 <0.01

Pregnancy
Oral contraceptives
Hormone replacement
therapy
Immobilisation
Surgery
Persistent Transient
Acquired
Age
History of VTE
Malignancy
Antiphospholipid antibody syndrome
Genetic
Thrombophilia
VTE – risk factors

Thrombophilia and risk of recurrence
Antithrombin deficiency
Homozygous factor VLeiden
Combined defects
Antiphospholipid antibodies (LA/ACA)
Protein C deficiency
Protein S deficiency
Heterozygous factor VLeiden
Heterozygous prothrombin gene mutation
Risk
Risk importance

Pathogenesis of VTE
Virchow´s triad
Stasis Injury to the vessel wall
Hypercoagulability
Rudolf Virchow

Pathogenesis of VTE
Virchow´s triad
Injury to the vessel wall
Damage to the vessel wall can be
produced by direct trauma such as
major hip or knee surgery, stab
wounds or insertion of venous
catheters, by direct invasion from
cancer cells, or as a consequence of
age. Support structures in vessel
walls deteriorate with age, leading to
weakness and a predisposition to
damage from distension.
Stasis
Hypercoagulability

Pathogenesis of VTE
Virchow´s triad
Injury to the
vessel wall
Hypercoagulability
Stasis
Stasis describes the slowing or even
cessation of blood flow. This
commonly occurs in veins as a result
of immobility or paralysis and can
lead to concentration and subsequent
activation of coagulation factors.
Stasis can also cause the vessel walls
to become distended, resulting in
endothelial damage.

Pathogenesis of VTE
Virchow´s triad
Stasis Injury to the vessel wall
Hypercoagulability
The term hypercoagulability means an increased propensity to
clot. Hypercoagulability can occur as a result of a genetic
defect, stasis, malignancy or hormone changes such as
during pregnancy, during administration of oral contraceptives
or hormone replacement therapy.

6. Vessel wall with activated endothelium
(colour-enhanced scanning electron micrograph)
This scanning electron micrograph shows how the
endothelium has reacted to compression and damage during
surgery. The endothelial cells are activated and the clotting
cascade has started. The formation of thrombin is the pivotal
step in fibrin formation and thrombus development.

Potentially Important Clinical Risk
Factors for VTE in Critically Ill
Patients
• Factors present before ICU admission
• Surgery
• Trauma
• Malignancy and its treatment
• Sepsis
• Immobilization
• Bedrest
• Stroke
• Spinal cord injury
• Increased age
• Pregnancy/puerperium
• Estrogens
•
Venous Thromboembolism and Its
Prevention in Critical Care
Journal of Critical Care, Vol 17, No 2
(June), 2002: pp 95-104

Potentially Important Clinical Risk
Factors for VTE in Critically ill
Patients
• Factors acquired in ICU
• Central venous lines
• Sepsis
• Pharmacologic sedation, paralysis
• Mechanical ventilation
Venous Thromboembolism
and Its Prevention in Critical
Care
Journal of Critical Care, Vol 17,
No 2 (June), 2002: pp 95-104

Incidence of DVT in Hospitalized
Patients
• Patient Group DVT Incidence
• Bedrest medical patients 10%–20%
• General abdominal surgery 15%–40%
• Neurosurgery 15%–40%
• Stroke 20%–50%
• Tibial fracture 20%–70%
• Hip or knee surgery 40%–60%
• Major trauma 40%–70%
• Spinal cord injury 60%–80%
• ICU 10%–80%
Venous
Thromboembolism and Its
Prevention in Critical
CareJournal of Critical
Care, Vol 17, No 2 (June),
2002: pp 95-104

Why ICU-specific studies addressing
VTE risks and prophylaxis are essential
• Symptoms or signs of possible VTE are much more common in critical
care patients; however,confirming (or excluding) this diagnosis is often
more difficult and is associated with greater risks for investigation among
these patients.
• • Many ICU patients have reduced cardiorespiratory reserve. Therefore,
small pulmonary emboli, well tolerated by non-ICU patients, may be
poorly tolerated by critically ill patients.
• • Critically ill patients have the highest morbidity and mortality of
hospitalized patients, and it is unclear whether the relative benefit of
different prophylaxis strategies are similar between these and other
patients.
• • Bleeding associated with anticoagulant prophylaxis may be more
frequent and associated with greater morbidity in ICU patients
Venous Thromboembolism and Its Prevention in Critical CareJournal of Critical Care, Vol 17, No 2 (June), 2002: pp 95

384/99 medslides.com38
Venous Thromboembolism
State of the Art
•American Journal of
•Respiratory and Critical Care
Medicine
•Vol 159, 1999

394/99 medslides.com39
Venous Thromboembolism
• Two major clinical manifestations
– deep venous thrombosis (DVT)
– pulmonary embolism (PE)
– 30% DVT pts develop symptomatic PE
50%-60% DVT pts develop asymptomatic
PE
• VTE affects 1/1000 persons yearly
• PE causes 50,000 death in the U.S.
yearly

404/99 medslides.com40
DVT - Risk factors and
Prevalence
• DVT most often originates in the
deep veins of the major calf muscles
• venous stasis
• trauma
• surgery
• childbirth
• increasing age
• all cancers

414/99 medslides.com41
Thrombophilia
• Definition
• recurrent venous or arterial
thrombosis from inherited or acquired
causes

424/99 medslides.com42
Inherited Thrombophilic States
•
Prevalence (%)
• Patients
with
VTE
1st
• Event
• Activated protein C resistance 3-4 20
50 3-7
• Hyperhomocysteinemia - 15 -
-
• Protein C deficiency 0.2-0.4 3 1-
9 5-12
• Protein S deficiency 0.1 2 1-
13 4-11
General
Population Recurrence RR*
* Relative Risk for recurrent VTE. Relative to an index case no inherited
thrombophillia.
Am J Respir Crit Care Med. Vol 159: 1-14; 1999

434/99 medslides.com43
Activated Protein C Resistance
• Inheritated abnormality known as factor V Leiden
• involves a point mutation (adenine for guanine)
that results in the substitution of glutamine for
arginine at position 506 on factor V
• activated protein-C becomes resistant to
degradation
• the heterozygous state (5% of Caucasians) carries
a 3 to 5 fold increased risk for VTE
• Factor V Leiden can be identified in 20% of
patients with one episode and 50% of those with
recurrent VTE

444/99 medslides.com44
Prevention of Venous
Thromboembolism• Without Prophylaxis
(%) Recommended With Prophylaxis (%)
• Risk Group Prox DVT Fatal PE Prophylaxis Prox DVT
Fatal PE
• Hip replacement 20-30 2-4 WAR, LMWH 5
0.1-0.2
• Knee replacement 20-30 2-4 WAR, LMWH, IPC 5
0.1-0.2
• Hip fracture 25-35 2-4 WAR, LMWH 10
0.2-0.4
• Major trauma 20 0.5-1.0 LMWH, IPC 10
<0.1
• Abdominal or pelvic
• cancer surgery 20 0.5-1.0
LMWH, IPC, WAR 10 <0.1
• Abdominal surgery,
• coronary artery 5-7 0.5
UF, LMWH, IPC <1 <0.1
• bypass graft WAR, ES
Am J Respir Crit Care Med. Vol 159: 1-14; 1999
ES = elastic stockings; IPC = intermittent pneumatic compression; UF = unfractionated heparin

454/99 medslides.com45
Prevention
• Anticoagulation and other antithrombotics form
the basis for prophylaxis
• Drugs are continued for 5-7 d for high-risk; 7-10
d for orthopedic procedure on the lower
extremity
• No prophylactic technique is completely
effective

464/99 medslides.com46
Vena Caval Filters
prophylactic device for pulmonary
embolism• patient with proximal DVT
– who cannot receive anticoagulants
– who has failed anticoagulants
• patient undergoing pulmonary embolectomy
• patient undergoing pulmonary endarterectomy
for chronic thromboembolic pulmonary
hypertension
• filters appear to prevent PE within the following
2 wks but did not affect short or long-term
mortality

474/99 medslides.com47
Diagnosis
• Of patients with suspected DVT, only one in four
will prove to have DVT
• Differential diagnosis:
– cellulitis, heart failure with edema, ruptured Baker‟s
cyst, chronic venous insufficiency
• Diagnostic tests:
– ultrasound with manual compression
– impedance plethysmography
– contrast venography
– fibrin degradation product D-dimer

484/99 medslides.com48
Diagnostic Approach to DVT
Am J Respir Crit Care Med. Vol 159: 1-14; 1999

494/99 medslides.com49
Natural History of DVT
• Untreated proximal DVT
– clinical PE occurs in 1/3 to 1/2 of patients
– sub-clinical PE occurs in another 1/3
– untreated PE tends to recur in days to weeks
• Post-phlebitic syndrome (10-30% of
DVT)
– pain, edema, skin discoloration, and
ulceration associated with chronic venous
insufficiency

504/99 medslides.com50
Pulmonary Embolism
• Three major clinical presentations:
• 1. dyspnea with or without pleuritic chest
pain and hemoptysis
• 2. hemodynamic instability and syncope
(usually associated with massive pulmonary
embolism)
• 3. mimicking indolent pneumonia or heart
failure, especially in the elderly

514/99 medslides.com51
Common symptoms of Acute
PE
• PIOPED study found
– Dyspnea
– Pleuritic chest pain
– Tachypnea (resp rate 20 / min)
• in 97% of patients with angiographic
proven PE
• The absence of this triad reduces the
clinical probability of PE

524/99 medslides.com52
Estimating Clinical Probability of
Pulmonary Embolism
• High Risk factor present
(80-100% probable) Otherwise unexplained dyspnea, tachypnea, or
pleuritic
chest pain
Otherwise unexplained radiographic or gas
exchange
abnormality
• Intermediate Neither high nor low clinical probability
(20-79% probable)
• Low Risk factor not present
(1-19% probable) Dyspnea, tachypnea, or pleuritic pain possibly
present
but unexplained by another condition
Radiographic or gas exchange abnormality
possibly
present but explainable by another condition
Am J Respir Crit Care Med. Vol 159: 1-14; 1999

534/99 medslides.com53
Diagnostic Test
• Ventilation-perfusion lung scan
– 2 moderate-to-large perfusion defects (>25% of a lung
segment) with intact ventilation in a clear chest x-ray in the
involved area
• Widened (A-a) O2 gradient
– low PO2, low PCO2
• Chest x-ray
– central pulmonary artery engorgement, paucity of peripheral
vessels (Westermark sign)
• Electrocardiogram
– nonspecific ST-T changes, right-axis, S1-Q3-T3, P-pulmonale

544/99 medslides.com54
Suspect Pulmonary Embolism ?
Give heparin IV and order V/Q scan
Low V/Q probability,
low clinical probability
High V/Q probability +
high clinical probability
Intermediate V/Q probability,
Low or high V/Q prob with
discordant clinical probability
Probability
V/Q Clinical
1. Low Mid
2. Mid Low
No treatment
Probability
V/Q Clinical
3. Low High
4. Mid Mid / High
5. High Low / Mid
Leg Ultrasound Treat
_
Pulmonary
Angiography
+
+
Am J Respir Crit Care Med. Vol 159: 1-14; 1999

554/99 medslides.com55
CTPHChronic Thromboembolic Pulmonary
Hypertension
• Result of recurrent or unresolved PE
• Occurs in 1% of patients with PE
• Sx: increasing dyspnea, exertion constant
• Diagnosis:
– diagnosis should be considered in any one with
unexplained dyspnea on exercise
– V/Q scan shows multiple large defects

564/99 medslides.com56
Treatment
• iv heparin until the diagnosis is ruled out
• heparin - UFH or LMWH
• warfarin / coumarin derivatives
• adjunctive recommendations:
– bed rest until heparin is therapeutic
– elastic stockings until patient becomes
ambulatory ( post-thrombotic syndrome)

574/99 medslides.com57
Body Weight-Based Dosing
of Intravenous Heparin• Initial dosing: Loading 80 U/kg 18 U/kg/hg (APTT in 6 hrs)
• APTT(s) Dose Change Additional Next APTT (h)
• (x normal) (U/kg/h) Action
• <35 (1.2 x) +4 Rebolus 80 U/kg 6
• 35-45 (1.2-1.5x) +2 Rebolus 40 U/kg 6
• 46-70 (1.5-2.3x) 0 0 6*
• 71-90 (2.3-3.0x) -2 0 6
• >90 (<3x) -3 Stop infusion 1 h 6* During first 24 h, thereafter, once / day
Am J Respir Crit Care Med. Vol 159: 1-14; 1999

584/99 medslides.com58
Low-Molecular-Weight Heparin
• Drug Prophylactic Indication Treatment Dose
• Ardeparin Knee arthroplasty 130 anti-Xa U/kg bid
(Normaiflo)
• Dalteparin Abdominal surgery 120 anti-Xa U/kg bid
(Fragmin)
• Enoxaparin Hip or knee arthroplasty, 1-1.5 mg/kg bid
(Lovenox) Abdominal surgery (1 mg 100 anti-Xa
units)
• Danaparoid Hip arthroplasty
(Orgaran)
* LMWH < 5.6 kD, lose anti-IIa activity, cannot be reliably monitored with APTT
Am J Respir Crit Care Med. Vol 159: 1-14; 1999

Incidence of DVT in Hospitalized
Patients
• Patient Group DVT Incidence
• Bedrest medical patients 10%–20%
• General abdominal surgery 15%–40%
• Neurosurgery 15%–40%
• Stroke 20%–50%
• Tibial fracture 20%–70%
• Hip or knee surgery 40%–60%
• Major trauma 40%–70%
• Spinal cord injury 60%–80%
• ICU 10%–80%
Venous
Thromboembolism and Its
Prevention in Critical
CareJournal of Critical
Care, Vol 17, No 2 (June),
2002: pp 95-104

Why ICU-specific studies addressing
VTE risks and prophylaxis are essential
• Symptoms or signs of possible VTE are much more common in critical
care patients; however,confirming (or excluding) this diagnosis is often
more difficult and is associated with greater risks for investigation among
these patients.
• • Many ICU patients have reduced cardiorespiratory reserve. Therefore,
small pulmonary emboli, well tolerated by non-ICU patients, may be
poorly tolerated by critically ill patients.
• • Critically ill patients have the highest morbidity and mortality of
hospitalized patients, and it is unclear whether the relative benefit of
different prophylaxis strategies are similar between these and other
patients.
• • Bleeding associated with anticoagulant prophylaxis may be more
frequent and associated with greater morbidity in ICU patients
Venous Thromboembolism and Its Prevention in Critical CareJournal of Critical Care, Vol 17, No 2 (June), 2002: pp 95






Biomaterials Research - Manfred Maitz
Effect of Antithrombin III/Heparin
FibrinogenFibrin
monomers
Prothrombin I Thrombin
Factor F XaFactor F X Factor F X
F VIIF VIIa
F IXaF IX
F XIaF XI
Surface Contact
Collagen
FXII activator
F XIIaF XII
F III (Tissue
Thromboplastin)
Tissue/Cell Defect
Intrinsic Pathway Extrinsic Pathway
Platelet Factor 3
Ca2+
Ca2+
Ca2+
Ca2+Ca2+
Fibrin
polymersCrosslinked
Fibrin Meshwork
F XIIIa F XIII
F VF Va
F VIIIaF VIII
Ca2+

Biomaterials Research - Manfred Maitz
Thrombin Time (TT)
FibrinogenFibrin
monomers
Prothrombin I Thrombin
Factor F XaFactor F X Factor F X
F VIIF VIIa
F IXaF IX
F XIaF XI
Surface Contact
Collagen
FXII activator
F XIIaF XII
F III (Tissue
Thromboplastin)
Tissue/Cell Defect
Intrinsic Pathway Extrinsic Pathway
Platelet Factor 3
Ca2+
Ca2+
Ca2+
Ca2+Ca2+
Fibrin
polymersCrosslinked
Fibrin Meshwork
F XIIIa F XIII
F VF Va
F VIIIaF VIII
Ca2+

Biomaterials Research - Manfred Maitz
The Quick (PT)-Test
FibrinogenFibrin
monomers
Prothrombin I Thrombin
Factor F XaFactor F X Factor F X
F VIIF VIIa
F IXaF IX
F XIaF XI
Surface Contact
Collagen
FXII activator
F XIIaF XII
F III (Tissue
Thromboplastin)
Tissue/Cell Defect
Intrinsic Pathway Extrinsic Pathway
Platelet Factor 3
Ca2+
Ca2+
Ca2+
Ca2+Ca2+
Fibrin
polymersCrosslinked
Fibrin Meshwork
F XIIIa F XIII
F VF Va
F VIIIaF VIII
Ca2+

Biomaterials Research - Manfred Maitz
Partial Thromboplastin Time [(a)PTT]
FibrinogenFibrin
monomers
Prothrombin I Thrombin
Factor F XaFactor F X Factor F X
F VIIF VIIa
F IXaF IX
F XIaF XI
Surface Contact
Collagen
FXII activator
F XIIaF XII
F III (Tissue
Thromboplastin)
Tissue/Cell Defect
Intrinsic Pathway Extrinsic Pathway
Platelet Factor 3
Ca2+
Ca2+
Ca2+
Ca2+Ca2+
Fibrin
polymersCrosslinked
Fibrin Meshwork
F XIIIa F XIII
F VF Va
F VIIIaF VIII
Ca2+

Biomaterials Research - Manfred Maitz
Surface Sensitive Steps
FibrinogenFibrin
monomers
Prothrombin I Thrombin
Factor F XaFactor F X Factor F X
F VIIF VIIa
F IXaF IX
F XIaF XI
Surface Contact
Collagen
FXII activator
F XIIaF XII
F III (Tissue
Thromboplastin)
Tissue/Cell Defect
Intrinsic Pathway Extrinsic Pathway
Platelet Factor 3
Ca2+
Ca2+
Ca2+
Ca2+Ca2+
Fibrin
polymersCrosslinked
Fibrin Meshwork
F XIIIa F XIII
F VF Va
F VIIIaF VIII
Ca2+










•Management of venous thromboembolism in the
intensive
•care unit
•Stephen M. Pastores MD, FACP, FCCP, FCCM⁎
•Journal of Critical Care (2009) 24, 185–191