β 2 -microglobulin amyloidosis
25
Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997) Review p2 -microglobulin amyloidosis Jonathan Kay, M.D. Department of Internal Medicine, Lahey Hitchcock Medical Center, Burlington, MA, and the Department of Medicine, Harvard Medical School, Boston, MA, USA Kf.1 If OKIK P,-microglobulin amyloidosis, dialysis-related amyloidosis, hemodialysis, uremia, advanced gl-vcosylation end products, carpal tunnel syndrome, shoulder periarthritis, bone cysts, destructive spondyloarthropathy, renal transplantation, aminoguanidine .~HHXI.I 7qr~lhs: AP = amyloid-P peptide, AGE = advancedglycosylation endproducts, AGE-P2M = advancedglycosylation endproduct- modijied P2-microglobulin, P2M = p, microglobulin, CAPD = continuous ambulatoty peritoneal dialysis, CT = computed tomography, 30G = 3-deoxyglucosone, DRAQ = dialysis-related amyloidosis questionnaire, HLA = human leukocyte antigen; IGF I = ins1llln-fike grodijhctor I, IL-1 = interleukin-I, IL-6 = interleukin-6, LF-L = lactoferrin-likepolypeptide, MMP = matrix metalloproternase, ,24RI = magnerrc resonance imaging, PMMA = polymethylmethaciylate; RACE = receptor for advancedg1,vcosylation endproducts. .CAP =serum am),loid P component, TGF-p = transforming growjth factor fi TIMP = tissue inhibitor of metalloproteinuse, TNFa = tumor necrosis factor a Abstract @microglobulin (P2M) amyloidosis is a disabling dis- ease that aflects patients with long-term chronic renalfail- ure but not individuals with normal renal function. It is an ideal model for study of the amyloid diseases because a de$ned population is at risk for the development of this condition, its clinical manlfesfations evolve predictably over time, and it ultimately occurs in the majority of patients who have received long-term dialysis therapy. The clinical features ofP2M amyloidosis are reviewed, high- lighting the systemic nature of this disease. The various techniques available to diagnose this condition are described. The pathogenesis of P2M amyloidosis is recon- sidered in light of recently published data regarding advanced glycation end products (AGE). Available and potential treatments for this condition are also discussed. occurring in patients undergoing hemodialysis in 1975, 15 years after Scribner2first treated a patient with chronic ure- mia with intermittent hemodialysis. Amyloid was frst identi- fied in a carpal tunnel biopsy specimen from a patient undergoing hemodialysis by Kenzora’ in 1978. Assenat and colleagues4 reported an association between the carpal tun- nel syndrome and a scapulohumeral periarthritis in 1980. In 1985, Gejyo and colleagues5identified P2M as the protein precursor of the amyloid associated with chronic hemodi- alysis. Subsequently, a variety of syndromes predominantly involving the musculoskeletal system and occurring in patients with chronic renal failure have been shown to be caused by P2M amyloid deposition. Following the identifi- cation of AGE in P2M amyloid deposits by Miyata and co-workers in 19936, a new direction to elucidate the patho- genesis of this condition has been pursued. Clinical features Historical background he current understanding of dialysis-associated amy- loidosis has evolved over the past two decades. War- T ren and Otieno’ described carpal tunnel syndrome Patients with P2M amyloidosis commonly display mus- culoskeletal signs and symptoms. In contrast, although gas- trointestinal tract complications have been reported, visceral (32M amyloid deposits usually do not cause symptoms. Sys- Correspondence Dr Jonathan Kay, Section of Rheumatologq Lahey Hitchcock Medical Center. 41 Mall Road, Burlington, MA 01805 USA Tel 6 17-273-8857 Fax 6 17-273-5249 E-mail Jonathan Kay2 Lahey Hitchcock org Submitted March 6. 1997 Revision Accepted Ma) 30, 1997 187 Amyloid Downloaded from informahealthcare.com by University of Bath on 11/02/14 For personal use only.
Transcript of β 2 -microglobulin amyloidosis

Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997)
Review
p 2 -microglobulin amyloidosis Jonathan Kay, M.D.
Department of Internal Medicine, Lahey Hitchcock Medical Center, Burlington, MA, and the Department of Medicine, Harvard Medical School, Boston, MA, USA
Kf.1 I f OKIK P,-microglobulin amyloidosis, dialysis-related amyloidosis, hemodialysis, uremia, advanced gl-vcosylation end products, carpal tunnel syndrome, shoulder periarthritis, bone cysts, destructive spondyloarthropathy, renal transplantation, aminoguanidine
. ~ H H X I . I 7qr~lhs: AP = amyloid-P peptide, AGE = advancedglycosylation endproducts, AGE-P2M = advancedglycosylation endproduct- modijied P2-microglobulin, P2M = p, microglobulin, CAPD = continuous ambulatoty peritoneal dialysis, CT = computed tomography, 30G = 3-deoxyglucosone, DRAQ = dialysis-related amyloidosis questionnaire, HLA = human leukocyte antigen; IGF I = ins1llln-fike grod i jhc tor I, IL-1 = interleukin-I, IL-6 = interleukin-6, LF-L = lactoferrin-like polypeptide, MMP = matrix metalloproternase, ,24RI =
magnerrc resonance imaging, PMMA = polymethylmethaciylate; RACE = receptor fo r advancedg1,vcosylation endproducts. .CAP =serum am),loid P component, TGF-p = transforming growjth factor f i TIMP = tissue inhibitor of metalloproteinuse, TNFa = tumor necrosis factor a
Abstract
@microglobulin (P2M) amyloidosis is a disabling dis- ease that aflects patients with long-term chronic renalfail- ure but not individuals with normal renal function. It is an ideal model for study of the amyloid diseases because a de$ned population is at risk for the development of this condition, its clinical manlfes fations evolve predictably over time, and it ultimately occurs in the majority of patients who have received long-term dialysis therapy. The clinical features ofP2M amyloidosis are reviewed, high- lighting the systemic nature of this disease. The various techniques available to diagnose this condition are described. The pathogenesis of P2M amyloidosis is recon- sidered in light of recently published data regarding advanced glycation end products (AGE). Available and potential treatments for this condition are also discussed.
occurring in patients undergoing hemodialysis in 1975, 15 years after Scribner2 first treated a patient with chronic ure- mia with intermittent hemodialysis. Amyloid was frst identi- fied in a carpal tunnel biopsy specimen from a patient undergoing hemodialysis by Kenzora’ in 1978. Assenat and colleagues4 reported an association between the carpal tun- nel syndrome and a scapulohumeral periarthritis in 1980. In 1985, Gejyo and colleagues5 identified P2M as the protein precursor of the amyloid associated with chronic hemodi- alysis. Subsequently, a variety of syndromes predominantly involving the musculoskeletal system and occurring in patients with chronic renal failure have been shown to be caused by P2M amyloid deposition. Following the identifi- cation of AGE in P2M amyloid deposits by Miyata and co-workers in 19936, a new direction to elucidate the patho- genesis of this condition has been pursued.
Clinical features Historical background
he current understanding of dialysis-associated amy- loidosis has evolved over the past two decades. War- T ren and Otieno’ described carpal tunnel syndrome
Patients with P2M amyloidosis commonly display mus- culoskeletal signs and symptoms. In contrast, although gas- trointestinal tract complications have been reported, visceral (32M amyloid deposits usually do not cause symptoms. Sys-
Correspondence Dr Jonathan Kay, Section of Rheumatologq Lahey Hitchcock Medical Center. 41 Mall Road, Burlington, MA 01805 USA Tel 6 17-273-8857 Fax 6 17-273-5249 E-mail Jonathan K a y 2 Lahey Hitchcock org
Submitted March 6. 1997 Revision Accepted Ma) 30, 1997
187
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Kay
temic involvement by P2M amyloidosis seems to occur less commonly than musculoskeletal involvement. However, the only available data describing the prevalence of signs and symptoms of P2M amyloidosis are derived from several major cross-sectional cohort studies. The true prevalence of P2M amyloidosis has not been established because biop- sies have not systematically been performed on sufficient patients undergoing dialysis to determine the actual frequency of musculoskeletal and systemic P2M amyloid deposition.
Musculoskeletal involvement P2M amyloid deposits preferentially in bone, articular
cartilage, synovium, muscle, and ligaments'. Patients with P2M amyloidosis often have a characteristic triad of shoul- der pain, carpal tunnel syndrome, and flexor tendon depos- its in the hands on presentation. This clinical syndrome is similar to the musculoskeletal complications seen in patients with long-standing diabetes mellitus, including shoulder periarthritis, carpal tunnel syndrome, flexor tenosynovitis, and Dupuytren's contracture of the hands', and suggests the possibility of a common pathogenetic mechanism, such as modification of proteins with AGE9. The clinical and radiographic appearance of amyloid deposits in patients undergoing hemodialysis also resembles many of the find- ings seen in patients with rheumatoid arthritis, sometimes leading to the misdiagnosis of dialysis-related amyloidosis as rheumatoid arthritis (Table 1).
Laurent and colleaguesI0 described the prevalence of musculoskeletal symptoms associated with dialysis-related amyloidosis in 256 patients on long term hemodialysis. Shoul- der pain developed, in most patients, after 5 years of hemo- dialysis treatment and occurred more often in patients with carpal tunnel syndrome. As many as 95% of patients with amyloid deposits demonstrated in tissue removed at the time of carpal tunnel release also had shoulder pain. The inci- dence of carpal tunnel syndrome and shoulder pain increases with longer duration of hemodialysis'0-'2; both are present in most patients who have undergone hemodialysis for longer than 12 years". Among patients receiving hemodi- alysis for 10 years or longer, the prevalence of shoulder pain, often bilateral, has ranged from 34% to 84%'?-''; the
Table 1. Musculoskeletal manifestations of P2M amyloidosis.
Scapulohumeral periarthritis Carpal tunnel syndrome Flexor tenosynovitis Destructive spondyloarthropathy Cervico-occipital pseudotumor Bone cysts Pathologic fractures
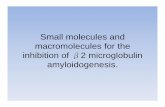
FIGURE 1. Shoulder pad sign in a patient with !32M amyloidosis.
prevalence of carpal tunnel syndrome, also often bilateral, has ranged from 9% to 73%12-''. The wide variation in preva- lence observed among these studies probably reflects the heterogeneity of the patient populations examined.
Shoulder periartliritis P2M amyloid deposition in the shoulders of patients
undergoing chronic hemodialysis may produce a scapulohumeral periarthriti~l~. The rotator cuff muscles may be thickened or amyloid may deposit between the muscles and tendons of the rotator cuffz', causing the shoulders to appear hypertrophied with shoulder pads (Figure 1). Depos- its of P2M amyloid in the biceps and supraspinatus tendons and tendon sheaths may predispose these tendons to rup- ture". The subacromial bursa may be thickened and an inflammatory infiltrate may be present within the synovium'3.
Patients receiving long-term hemodialysis often report anterolateral shoulder pain that is worse when they are in a supine position, especially during dialysis treatments and at night, and may improve when they assume a sitting or stand- ing position''. The coracoacromial ligament and sometimes the bicipital groove are tender to palpation. Impingement of the thickened subacromial bursa beneath the acromial pro- cess may induce pain and limit range of shoulder motion, especially in abduction. Adhesive capsulitis of the shoulder may be present.
Carpal tunnel syndrome Hand pain and numbness and dysesthesias in the dis-
tribution of the median nerve may occur in chronic hemodi- alysis as a result of P2M amyloid deposits in the carpal
188
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin Invest. 3, 187-211 (1997)
tunnel?. Symptoms of carpal tunnel syndrome occur more frequently on the side of the longest functioning vascular accessz4. However, bilateral carpal tunnel syndrome has occurred even in patients whose vascular access site is on one side only. Exacerbation of carpal tunnel syndrome symp- toms during hemodialysis may result from a fistula-induced arterial steal phenomenon causing ischemia to the median nerve in the narrowed carpal tunnel3.
Flexor tenosynovitis Irreducible flexion contractures of the fingers fi-equently
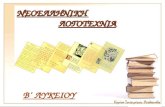
develop in individuals on hemodialysis when P2M amyloid is deposited along the flexor tendons of the handL3, causing the digital flexor tendons of the hand to adhere to one another?’. These deposits may create a subcutaneous soft tissue mass in the palm (Figure 2). The flexor tendons become prominent when the fmgers are extended. This “gui- tar string sign” in a patient on dialysis with shoulder pain or carpal tunnel syndrome or both is highly suggestive of 132M am? Ioidosisz6.
Spine The axial skeleton is affected less frequently than the
upper extremities. Maruyama and colleagues” found radio- graphic features characteristic of the destructive spondyloarthropathy associated with dialysis-related amy- loidosis in 9. I % of 405 patients. The prevalence ofthis con- dition is also higher the longer the duration ofhemodialysis28: destructive spondyloarthropathy was present in 13.4% of the I57 patients who had been receiving hemodialysis for longer than 10 years. Kessler and colleague^'^ found a simi- lar prevalence of 14.0% in a cohort of 171 patients from 19 centers in northeastern France who had been receiving hemodialysis for longer than 10 years.
Radiographic features of the destructive spondyloarthropathy2’ that occurs in patients receiving long- term hemodialysis are similar to those seen in infection of the disk space, including narrowing ofthe intervertebral disk spaces and erosions of the vertebral end-plates without appreciable formation of osteophyte. These erosions occur most frequently at the anterosuperior or anteroinferior mar- gins ofthe vertebral bodies, similar to the Romanus lesion of ankylosing spondylitisjO.
The cervical spine is most often affected by destructive spondyloarthropathy; however, similar changes may also occur in the dorsal and lumbar spine”. Radiographic changes of the destructive spondyloarthropathy are usually noted in the lower cervical spine’’. ?’. z9: the disk spaces between the fourth and fifth cervical vertebrae and between the fifth and sixth cervical vertebrae are most frequently involved” (Fig- ure 3). Ohashi and colleagues2* hypothesized that P2M amy- loid deposition in intervertebral disks is accelerated by mechanical stress due to the motion of daily life: P2M amy-
loid deposits appear first in the disk spaces between the fourth and fifth cervical vertebrae, between the fifth and sixth cervical vertebrae. and between the sixth and seventh cervical vertebrae where the range of motion is greatest.
Involvement of the upper cervical spine has also been demonstrated3’. Cystic radiolucencies of the first and sec- ond cervical vertebral bodies or the odontoid process are the most common radiographic changes seen31. Periodontoid soft tissue masses of 132M amyloid, termed pseudotumors, may occur with destructive changes of the cervico-occipital hinge joint3z. Such a pseudotumor has been reported in a patient on hemodialysis for only 4 yearsi3.
Radiographic changes of the cervico-occipital hinge joint were found in 9 of 23 patients (39%) on hemodialysis for 8 years or longer’l. Periodontoid pseudotumors were identified3‘ by magnetic resonance imaging (MRI) in 7 of 25 patients (28%) treated for 10 years or longer. However, the prevalence of upper cervical spine involvement may be over- estimated because of the small number of patients included in the studies describing these changes. Kessler and col- leagues1’ observed spondyloarthropathy affecting the cervico-occipital hinge joint in only 2 of 171 patients ( 1 YO) receiving hemodialysis for longer than 10 years.
Deposits of 132M amyloid have been demonstrated in paravertebral ligaments and intervertebral disks”, even in the absence of radiographic changes of destructive spondyloarthropathyz8. Postmortem examination of the intervertebral disks of patients who received dialysis for fewer than 5 years revealed small deposits of P2M amyloid almost exclusively in the annulus fibrosus of cervical disks as early as 1 year and 7 months after the initiation of hemo- dialysis28. Patients who underwent dialysis for longer t h s n 5 years had P2M amyloid deposits in lumbar and upper tho- racic disks as well as in cervical disks.
FIGURE 2. Amyloid deposits in the wrist and palm, with irreducible flexion contractures of the fingers, in a patient with P 2 M arnyloidosis. The thenar atrophy reflects the presence of long-standing carpal tunnel syndrome.
189
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

The initial symptom of destructive spondyloarthropathy is pain, typically in the neck when the cervical spine is involved36. However, most patients who have radiographic abnormalities in the cervical spine have no neck pain". Although neurologic compromise occurs infrequently, sig- nificant myelopathy has been reported to result from P2M amyloid deposits in the cervical and lumbar spinal canal. Thickening of the dorsal ligaments and ligamentum flavum of the cervical spine has resulted in obstruction of the sub- arachnoid space and spinal cord compressioni7. In three patients who had received long-term hemodialysis, spastic quadriparesis resulted from extradural P2M amyloid depos- its compressing the lower cervical spinal Compres- sion of the upper cervical spinal cord by a periodontoid pseudotumor resulted in quadriparesis and death of a 5 1 - year-old woman who had received hemodialysis for 17 years39. P2M amyloid deposition in the intervertebral disks and ligamentum flavum of the lumbar spine has also resulted in compression of the thecal sac and cauda equina".
Bone cysts Cystic bone lesions also develop in patients with P2M
amyloidosis. Subchondral amyloid cysts, most commonly found in the carpal bones", may also occur in the acetabu- lum and in long bones, such as the femoral head or neck, the
FIGURE 3. Lateral cervical spine radiograph of a patient with p2M amyloidosis showing changes characteristic of destructive spondyloarthropathy. The intervertebral disk spaces between the third and fourth cervical vertebrae and between the fifth and sixth cervical vertebrae are narrowed and the vertebral end-plates are eroded without appreciable formation of osteophyte.
humeral head, the distal radius, and the tibia1 plateau. Unlike brown tumors of hyperparathyroidism, these bone cysts typically occur adjacent to joints". On plain radiographs, they appear as well-defined radiolucencies with occasional disruption of the bony cortex but no periosteal reaction" 13.
Cysts vary in size, ranging from 2 to 3 mm diameter in the carpal bones to as large as 40 mm in the a c e t a b u l ~ m ~ ~ . Even in the absence of radiographic features of hyperparathy- roidism, these cysts increase in number and enlarge with timeu.
Pathologic fractures Pathologic fractures, especially of the femoral neck, may
occur through areas of bone weakened by amyloid depos- itS45.47 . Patients with femoral neck fractures may experience the sudden onset of intense leg pain, especially when walk- ing48. The prevalence of femoral neck fracture associated with long-term hemodialysis is significantly higher in patients with periosteal P2M deposition on iliac crest bone biopsy specimens than in patients without P2M depositioni9.
Systemic involvement Although P2M amyloid deposits predominantly in
osteoarticular tissue, visceral deposits of P2M amyloid have been identified. Most patients with visceral deposits have undergone hemodialysis for 10 years or longer and also have either carpal tunnel syndrome or arthropathysO. The amount of visceral P2M amyloid deposition increases with longer duration of dialysis50, however, the extent of systemic involvement remains controversial.
Most of the information available about systemic involvement by P2M amyloid is derived from postmortem examination of patients receiving long-term hemodialysis, whereas during life, histologic evidence is acquired only when the clinical consequences of the amyloid deposits require surgical intervention. Thus, the actual extent of asymptomatic visceral P2M amyloid deposition is poorly understood, especially in patients who have undergone dialysis for less than 10 years.
The prevalence of visceral P2M amyloid deposition iden- tified on postmortem examination varies among published reports. In a study of 19 patients, all of whom had osteoarticular P2M amyloid deposits, four also had visceral P2M amyloid deposits that were small and localized to blood vessel walls of heart, lung, liver, duodenum, tongue, pros- tate, and adrenal glands'. Patients with visceral deposits had received hemodialysis for longer than 13 years. Another study demonstrated visceral P2M amyloid depos- its on postmortem examination of 7 patients who had received hemodialysis for 10 years or longer but not in any of 13 patients who had undergone hemodialysis for less than 10 years". Visceral P2M amyloid was deposited mainly
190
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J Exp. Clin. Invest. 4, 187-211 (1997)
in blood vessel walls; the heart, gastrointestinal tract, and lungs were most frequently involved. In autopsy material from 6 patients with osteoarticular P2M amyloid deposits. visceral P2M amyloid deposits were found only in a 70-year- old woman who had received hemodialysis for 10 years; no visceral P2M amyloid deposits were found in the other 5 patients, although one 58-year-old man had received hemodialysis for longer than 14 years”. Thus, other factors in addition to the duration of dialysis determine the extent of visceral P2M amyloid deposition.
Two types of visceral P2M amyloid deposits have been identified: vascular deposits and interstitial deposits5? (Table 2). In contrast to osteoarticular P2M amyloid, which is deposited predominantly in the interstitium, visceral P2M amyloid is deposited predominantly in blood vessels’O. Vas- cular deposits may be linear, replacing the muscular layer around the circumference of small vessels, or nodular, located beneath the vascular endothelium and protruding into the vessel lumen50. Linear deposits of P2M amyloid in blood vessel walls may result in vascular fragility and bleed-
ischemia of the tissues supplied by those vesselss4 and occasionally result in perforation of viscera52. Interstitial de- posits may be focal or difhse (“plate-like”) and can infiltrate visceral smooth m ~ s c l e ~ ’ ~ ~ ~ . Diffuse interstitial P2M amyloid deposits may cause m a l a b ~ o r p t i o n ~ ~ or disturbances of smooth muscle h n c t i ~ n ~ ~ .
inoi l . , nodular deposits occluding vessel lumens may lead to
Gastrointestinal tract Most of the visceral P2M amyloid deposits reported to
cause symptoms during life have been in the gastrointesti- nal tract. Subepithelial P2M amyloid deposits have caused nodular enlargement of the tongue and difficulty in swal-
caused macroglossia and ~ d y n o p h a g i a ~ ~ . Gastric ulceration has been associated with extensive P2M amyloid deposi- tion in the lamina submucosa and lamina muscularis propria ofthe stomach5‘. P2M amyloid deposition in the lamina mus- cularis mucosae of the stomach and the walls of small sub- mucosal vessels has resulted in intestinal pseudo-obstruction with gastric dilations7. Hemorrhage has occurred at sites of P2M amyloid deposition in submucosal blood vessels of the duodenum53 and jejunums6. P2M amy- loid deposition in small- and medium-sized blood vessels and in the lamina muscularis propia ofthe small intestine has also resulted in small bowel ischemia and perforation’O. c 4 .
Extensive deposition of P2M amyloid in submucosal blood vessels and the lamina muscularis propria of the small and large intestines has resulted in malabsorption and diarrhea’6 and in intestinal pseudo-obstruction6’. P2M amyloid depo- sition in submucosal blood vessel walls and the muscle layer of the large intestine has resulted in intestinal in far~ t ion~‘ ,~’ -
and p e r f ~ r a t i o n ~ ? . ~ ~ . P2M amyloid deposition in the walls
lowing% 59. , diffuse submucosal P2M amyloid deposits have
of small submucosal blood vessels of the colon has also been associated with intestinal pseudo-obstruction64, 66. 67 .
Thus, systemic deposition of P2M amyloid may result in significant morbidity.
P2M amyloid deposits not causing signs or symptoms have been detected within the walls of small submucosal blood vessels in the rectum of patients undergoing long- term hemodia ly~ i s~~ , 68-70. Rectal biopsy may demonstrate systemic involvement of P2M amyloidosis if the sample includes submucosal tissue55, but it may not yield diagnos- tic findings, even from patients in whom visceral P2M amy- loid deposition subsequently has been demonstrated on postmortem examination, because of sampling error7I.
In the liver, small P2M amyloid deposits have also been observed in the walls of arterioles, small arteries, and veins7.
tion caused by P2M amyloid deposition has not been reported.
47. 50, 5 5 , 56, 71-75 . H owever, clinically evident hepatic dysfunc-
Heart and lungs P2M amyloid deposits have been identified in the myo-
cardium52. 5 3 . 5 5 . 7 1 . 7 5 , endocardiums3, cardiac valves and valve rings7’. 7 6 , and within blood vessel walls in the heart7, 46.47. (O.
T2. 55, 56. 72-74. 76-78 . Campistol and reported two- dimensional echocardiographic evidence of amyloidosis in 12 of 23 patients (52%) who had undergone hemodialysis for 6 years or longer. P2M amyloid deposited in the myocar- dium and mitral valve ring of a patient who had received long-term hemodialysis caused “difficulty seating” a pros- thetic valve in the valve ring during mitral valve replacement surgery7‘.
P2M amyloid deposits have also been described in the walls of small pulmonary blood vessels7. 47 76.
Although most P2M amyloid deposits in the heart and lungs are asymptomatic, severe pulmonary hypertension, right ventricular failure, and low cardiac output developed as a result of P2M amyloid deposited predominantly in the walls of small arteries, arterioles and venules supplying the myo- cardium and of small peripheral pulmonary arteries and veins in a 6 1 -year-old woman who had received hemodialysis for 13 years76.
52. 55. 56,
Genitourinary tract Small deposits of P2M amyloid in the genitourinary tract
have been observed in the kidney5’ 5? 56 71 75 and the urinary bladder52, 7 3 . 79 of patients who had undergone long-term hemodialysis. Two patients, each of whom received a renal allograft from the same donor after having undergone hemo- dialysis for only 10 and 25 months, had nodular deposits of 132M amyloid within the walls of the transplanted ureters that caused ureteral obstruction 3 months after transplanta- tion*’. Neither of the recipients nor the donor had other evi- dence of P2M amyloidosis.
191
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Kav
Urinary matrix calculi, which are found in 5% to 7.5% of patients receiving chronic hemodialysis, contain P2M, serum amyloid P component (SAP), and lysozyrne". Congo red-stained sections of these stones reveal the apple-green birefringence that is characteristic of amyloids2.
In the male reproductive tract, both vascular and inter- stitial deposits have been noted in the prostate7. ' 5 73. 75 and testissz, 5 5 , 7s. In the female reproductive tract, large paren- chymal deposits of P2M amyloid, some with areas of acute and granulomatous inflammation, have been observed in the uterine broad ligament, within blood vessel walls in the broad ligament, and in the myometrium8*.
Nervous system P2M amyloid deposits have been identified in the en-
doneurium, perineurium, and around blood vessels in the epineurium on biopsy of a sural nerve from a 55-year-old woman receiving hemodialysis for 10 yearsg3. She had symp- toms of peripheral neuropathy but did not have either carpal tunnel syndrome or arthropathy. P2M amyloid deposits have been found in the walls of blood vessels in the brain of a 59- year-old man who had undergone hemodialysis for 15 years7s.
Endocrine system On postmortem examination of patients who had
received long-term hemodialysis, P2M amyloid deposits have been found in blood vessel walls of the thyroid gland56, 71,
pancreas7', 7 3 , and adrenal glands7. s*. 5 5 . 56. 7s. Diffuse intersti- tial P2M amyloid deposits also have been found in the par- athyroid glands of a 60-year-old man who had received hemodialysis for 11 years5' and in the enlarged left lobe of
the thyroid gland of a 5 1 -year-old man who had undergone hemodialysis for 13 yearss9. However, during life, none of these patients manifested clinical evidence of decreased glan- dular hnction related to the presence of these deposits.
Skin Cutaneous manifestations of P2M amyloidosis occur
infrequently in patients receiving chronic hemodialysis. Biopsies of clinically uninvolved skin from patients under- going long-term hemodialysis have demonstrated no P2M amyloid deposition, even in patients with amyloid arthropa- thy and carpal tunnel syndromeS1~ss.72. However, biopsies of hyperpigmented skin lesions from 37 patients who had been receiving hemodialysis for longer than 10 years revealed cutaneous P2M amyloid in 3 patients (8.1%) by light rnicros- copy; amyloid fibrils were detected in skin biopsies from 17 of 30 of these patients (56.7%) using electron microscopy8'. Cutaneous P2M amyloid deposits have also been found on biopsy of lichenoid-appearing papules that developed on the arms and trunk of a 40-year-old man with musculoskel- etal manifestations who had undergone hemodialysis for more than 15 yearsg5. Arnyloid was deposited in the dermal papillae, along the dermal-epidermal junction. and around the eccrine ducts and hair follicles.
Subcutaneous amyloidomas also occur in patients with P2M amyloidosis. Large subcutaneous P2M amyloid deposits, occasionally bilateral, have been observed in the gluteal regions of five patientss8, 79. 86-88 and the popliteal fossae of two patient^^^,^^. Each of the patients, who ranged in age from 40 to 76 years and had received hemodialysis for 10 to 18 years, also had carpal tunnel syndrome or arthropathy.
Table 2. Visceral P2M amyloid deposition.
Vascular deposits Interstitial deposits
Tongue Esophagus Stomach Intestine Rectum Liver Spleen Pancreas Brain Heart Lung Thyroid Adrenal glands Kidney Testes Prostate Urinary bladder Uterine broad ligament
Tongue Stomach Intestine Rectum Heart Thyroid Parathyroid gland Kidney Prostate Testes Uterine broad ligament Peripheral nerve Skin
192
In summary, P2M amyloid deposits not only in osteoarticular tissue but also in viscera and skin of patients receiving long-term dialysis treatment for chronic renal fail- ure. Deposits of P2M arnyloid outside the musculoskeletal system may also result in significant morbidity, as has been observed in the gastrointestinal tract. Systemic involvement by P2M amyloidosis appears to occur predominantly in patients who have undergone hemodialysis for longer than 10 years. However, systematic postmortem examination of a large number of patients with chronic renal failure will be necessary to determine the actual extent of systemic P2M amyloid deposition.
Effect of age Dialysis arthropathy occurs more commonly in older
patients. Gaucher and colleagues9' reported that most of their patients with dialysis arthropathy were between the ages of 50 and 70 years; most of the patients who were younger than SO years were without clinical evidence of dialysis arthropathy. A European multicenter study" dern- onstrated that advanced age at onset of dialysis correlates
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997)
with the development of carpal tunnel syndrome and radio- graphic evidence of amyloid bone cysts. The destructive spondyloarthropathy is also more likely to be present in individuals who were older at the onset of h e m ~ d i a l y s i s ” ~ ~ ~ . Signs of dialysis-related amyloidosis appear sooner in patients who are older at the initiation of hemodialysis therapy93.
P,-microglobulin amyloidosis occurring before dialysis
Three cases have been reported in which P2M amyloi- dosis developed in patients with chronic renal failure who had not yet received dialysis treatment, although almost all of the patients in whom P2M amyloidosis has been demon- strated had undergone hemodialysis or continuous ambula- tory peritoneal dialysis (CAPD). Thus, because P2M amyloidosis occurs in individuals with chronic renal disease who have not yet received dialysis therapy, it is a conse- quence of the duration of uremia and not of the dialysis treatment alone. However, factors related to the dialysis prescription may contribute to the development of P2M amyloidosis.
P2M amyloid was demonstrated in the stemoclavicular joint of a 69-year-old woman with “long-standing renal insufficiency” who also had radiographic evidence of cysts in the carpal bones and knees and of lumbar ~pondyloarthropathy~“. P2M amyloid was also demonstrated in the intervertebral disk between the fifth and sixth cervical vertebrae of a 5 1 -year-old woman in whom renal insufficiency had been present for 17 yearsgs. Radiographs revealed ero- sive spondyloarthropathy involving the intervertebral disks between the fifth and seventh cervical vertebrae, erosive arthropathy of the right acromioclavicular joint, and cysts in the hands and left femoral neck.
A third case of P2M amyloidosis, developing before chronic hemodialysis, has been reported in a 65-year old man with noninsulin-dependent diabetes mellitus of 30 years’ duration and severe uremia of 1 year’s duration96. Radio- graphs obtained at the onset of hemodialysis demonstrated cystic radiolucencies in the left wrist and erosive spondyloarthropathy involving the intervertebral disks between the fifth and eighth cervical vertebrae. The patient had received only four hemodialysis treatments when he underwent surgical decompression of the left carpal tunnel: P2M amyloid deposits were present in the excised trans- verse carpal ligament and tenosynovium. The presence of long-standing diabetes mellitus with microvascular compli- cations, in the setting of advanced age, may have acceler- ated the development of P2M amyloidosis before dialysis treatment in this patient, despite his relatively brief duration of uremia. Advanced glycation end products (AGE), which have been implicated both in the development of diabetic
complications and the aging process9’, may have contrib- uted to the rapid development of P2M amyloidosis in this patient.
P,-microglobulin amyloidosis and diabetes mellitus
If AGE are involved in the pathogenesis of both dia- betic complications and P2M amyloidosis, diabetic patients with nephropathy might be expected to experience the mani- festations of P2M amyloidosis earlier than nondiabetic patients with renal failure. Because the 5-year survival rate for diabetics with end-stage renal disease (20%) is only half that for nondiabetics (39%), diabetic patients receiving hemodialysis may not live sufficiently long for clinically evi- dent P2M amyloidosis to develop98.
A recent cross-sectional case-control study of diabetic and nondiabetic patients who had undergone hemodialysis for longer than 5 years described the prevalence of radiolu- cent cysts in the carpal bones and of carpal tunnel syn- drome to be similar in both groups99. However, each ofthese clinical manifestations may occur in conditions other than P2M amyloidosis, and tissue was not examined for P2M amyloid deposition. Thus, further investigation of the occurrence of P2M amyloidosis in diabetic patients with chronic renal failure is necessary. Additional studies com- paring the prevalence of both periarthritis of the shoulder and flexor tenosynovitis of the hand in diabetic and nondia- betic patients receiving hemodialysis, with histologic con- firmation of P2M amyloid deposition, are needed to elucidate the relationship between these two conditions.
Diagnosis
The diagnosis of dialysis-related amyloidosis is sug- gested primarily by its clinical appearance. Radiographic find- ings, such as bone cysts, narrowing of the intervertebral disk space, and vertebral end-plate erosion, serve to cor- roborate the diagnosis. However, histologic identification of P2M amyloid by Congo red and immunohistochemical staining in biopsy specimenP9 or in centrifuged synovial fluid sedimentsIoo remains the gold standard for diagnosis. As with AA amyloid, potassium permanganate pretreatment of tissue sections decreases Congo red
Computed tomography (CT) and MRI Amyloid deposits have distinct MRl characteristics: the
relatively long T1 and short T2 relaxation times result in a low to intermediate signal intensity, between that of fibro- cartilage and that of muscle, on both T1- and T2-weighted images. These signal characteristics distinguish amyloid
193
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

deposits from inflammatory or fluid-filled lesions, which dis- play low signal intensity on TI-weighted images and high signal intensity on T2-weighted imageslO'. On CT scanning, these amyloid deposits have intermediate internal attenua- tion values between 0 and 30 Hounsfield
P2M amyloid deposits that are too small to be seen on conventional radiographs may be evident by CT or MRIIo2. These imaging modalities may demonstrate soft-tissue masses, such as cervico-occipital p~eudotumors~', 34 that are not apparent on plain radiographs. CT or MRI may also show communication of intraosseous amyloid deposits with the joint space'02.
MRI of the spine may differentiate destructive spondyloarthropathy from infectious diskitis and from ver- tebral osteomyelitis. MRI o f destructive spon- dyloarthropathy demonstrates low to intermediate signal intensity in the intervertebral disk and adjacent vertebral end plates on both T 1 - and T2-weighted images. These MRI characteristics differ from those observed in infectious diskitis, where there is low signal intensity on T1 -weighted images and high signal intensity on T2-weighted images, and from those seen in vertebral osteomyelitis, where a prevertebral soft tissue mass is often visiblelo3.
Scintigraphic imaging Scintigraphic imaging has been tested as a noninvasive
technique to identify P2M amyloid deposits in patients receiving hemodialysis. Scintigraphy with 99mTc-methylene dip hosp honat e ( 99mTc-MD P) demonstrates increased radiotracer uptake by articular bone and soft tissue around large joints affected by P2M a m y l o i d o ~ i s ~ ~ ~ . Increased ra- diotracer uptake has been observed at the sites of cystic bone lesions, which are presumed to correlate with intraosseous P2M amyloid depo~its'~'. However, in a study of 17 patients with dialysis arthropathy, 99"'Tc-MDP uptake was not detected in 7 of 16 clinically affected shoulders'04. In another series of 7 patients with P2M amyloidosis who had undergone hemodialysis for 10 years or longer, radiotracer uptake was also increased diffusely throughout the skeleton in 3 patients with marked hyperparathyroidism and in the small joints of the hands in 3 patients at sites of erosive azotemic ~steoarthropathy~~~, which is a complica- tion of long-term hemodialysis that is not associated with P2M amyloid deposition'06. Thus, scintigraphy with 99mT~- MDP in patients receiving hemodialysis is not specific for the diagnosis of P2M amyloidosis.
Whole-body scintigraphic imaging with Iz3I-SAP, which has been used to identify, quantify, and monitor amyloid deposits in patients with AL, AA, and hereditary forms of systemic amylo id~s i s '~~ , has also been used to localize amy- loid deposits in patients undergoing hemodialysislo8. Radiotracer uptake was observed in joints in which P2M
amyloid had been demonstrated by biopsy. Although radiotracer uptake was detected in all symptomatic wrists and in 9 of 10 symptomatic knees, it was detected in only 7 of 19 (37%) symptomatic shoulders. The lower sensitivity of 1231-SAP scintigraphy in the shoulder, which is a joint often affected by P2M amyloidosis early in its clinical course, lim- its the utility of this investigational imaging modality as a screening test for this condition.
Scintigraphy with ')'I-P2M, another investigational imaging technique, has detected P2M amyloid deposits in patients receiving long-term hemodialysi~'~~. This radiotracer accumulates in osteoarticular structures, including the shoul- ders, that are clinically symptomatic and/or demonstrate radiographic changes characteristic of P2M amyloidosis; it does not accumulate in structures where both symptoms and radiographic changes are absent. Histologic examina- tion of tissue obtained from a patient who had been injected with '"I-P2M demonstrated concentration ofthe radioactiv- ity in P2M amyloid deposits and not in surrounding tissues. Further study of this imaging technique is necessary to determine whether it is a sensitive and specific method for detecting P2M amyloid deposits. However, the risks of radiation exposure and of blood-borne infections will limit its use in screening patients for P2M amyloidosis.
Ultrasonography Diagnostic ultrasonography, a noninvasive imaging mo-
dality that involves no exposure to radiation or to blood products, detects changes that are characteristic of P2M amyloidosis in patients undergoing chronic hemodialysis. We have used real-time, high-resolution ultrasonography to evaluate the shoulders of patients chronically hemodialyzed against cuprophane membranes. In comparison to 13 patients with normal renal fimction and no evidence of amy- loid, at least one of two ultrasonographic findings was selectively observed in 1 1 of 14 (79%) patients undergoing hemodialysis with clinical and histologic evidence of P2M amyloid: rotator cuffs greater than 8 mm in thickness and echogenic pads between muscle groups of the rotator cuff. These findings were not observed in any patient with nor- mal renal function or in 19 of 20 (95%) patients undergoing hemodialysis without clinical or histologic evidence of P2M amyloidosis. Thus, the presence of at least one of these two findings on ultrasonography of the shoulder provides a rela- tively sensitive and highly specific noninvasive adjunct to the clinical diagnosis of P2M amyloidosis in the patient undergoing long-term hemodialysisZ1.
Thickening of synovial tissue has also been demon- strated by ultrasonography in the knees of 11 patients receiving hemodialysis. The mean total synovial thickness was 4.7 mm in the 19 knees with suprapatellar effusions com- pared with 0.3 mm in 18 knees of 9 individuals without knee
194
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J Exp. Clin. Invest. 4, 187-211 (1997)
symptoms or joint effusions. Patients with amyloid demon- strated in synovial fluid aspirated from the knee had thicker knee joint synovium than the patient without amyloid in synovial fluid, suggesting that increased knee joint syn- ovial thickness correlates with the presence of P2M amyloid in patients undergoing long-term hemodialysis44. Further study is necessary to confirm this observation.
Screening questionnaire We developed a 19-item self-administered questionnaire
to evaluate the effects of dialysis-related amyloidosis on functional status'''. This dialysis-related amyloidosis ques- tionnaire (DRAQ) is a reliable, internally consistent, and valid instrument to assess symptoms and disability associated with P2M amyloidosis. When the DRAQ was administered to 15 patients with dialysis-related amyloidosis and 15 age- matched control subjects who had been on hemodialysis for less than 24 months, a DRAQ score of 30 or more indicated the presence of dialysis-related amyloidosis with a sensitiv- ity of 93% and specificity of 80%. The positive predictive value of a DRAQ score of 30 or more ranged from 2% when the prevalence of P2M amyloidosis was estimated to be 0.5% to 54% when the disease prevalence was estimated to be 20%. The negative predictive value of a DRAQ score of 30 or more was greater than 98% when the disease prevalence was estimated to be 20% or less, suggesting that symptom- atic and disabling P2M amyloidosis would be unlikely in individuals with low total DRAQ scores. The DRAQ is sen- sitive and specific enough to be useful and cost effective in population screening, particularly as the first test in a two- part case-finding strategy utilizing either shoulder ultra- sonography or another radiographic technique to further evaluate patients with elevated DRAQ scores.
Abdominal fat pad aspiration Abdominal fat pad aspiration is a sensitive and specific
screening test to diagnosis AL"' and AA amyloidosis and familial amyloid polyneuropathy'I2, but it has not proven to be as useful in screening for P2M amyloidosis. Although Campistol and colleagues" found amyloid deposits by Congo red staining in abdominal fat pad aspirates from 9 of 25 patients (36%) who had received hemodialysis for 6 years or longer, Varga and colleague^"^ found no amyloid depos- its in abdominal fat pad aspirates obtained from 30 patients who had undergone hemodialysis for 2 years or longer. Although the patients in both studies were of similar age. only 37% of the patients studied by Varga and associates had carpal tunnel syndrome, whereas 84% of the patients studied by Campistol and colleagues had carpal tunnel syn- drome. This suggests that a lower prevalence of P2M amy-
loidosis among the patients studied by Varga and colleagues could have accounted for the absence of amyloid deposits in the abdominal fat pad aspirates obtained from their population.
Constituents of P,-microglobulin amyloid deposits
P2M amyloid deposits contain various macromolecular and cellular constituents. Besides the subunit protein P2M, proteases and protease inhibitors have been demonstrated in and around P2M amyloid deposits. Proteoglycans, gly- cosaminoglycans, and other proteins that are also present may affect the formation or deposition of P2M amyloid fibrils. The predominant cells infiltrating P2M amyloid deposits are macrophages2*.
P ,-microglobulin P2M was frst described in 1968 by Berggkd and Beam
as a low molecular weight P,-globulin isolated from urine of patients with tubular proteinuria caused by Wilson's dis- ease or chronic cadmium poisoning'I4. In 1985, Gejyo and colleagues identified P2M as the subunit protein in the amy- loid associated with chronic hemodialysis'. This nonglycosylated 1 1,800 dalton protein is homologous in sequence"', 'I6 and to the constant (C) region domains of immunoglobulin (Ig) K and h light chains and the y 1 heavy chain of IgG. It is found on the plasma membrane of all nucleated mammalian cells, where it is noncovalently associated with human leukocyte antigen (HLA) Class I molecules118. It is normally present in most biological fluids, including serum, urine, and synovial fluid'19. Serum concen- trations range up to 2.7 pg/ml in healthy individuals with normal renal function. P2M is filtered by glomeruli and catabo- lized after proximal tubular reabsorption'20. Serum levels of P2M correlate with serum creatinine levels, and patients undergoing hemodialysis have an 8- to 60-fold elevation in their serum P2M levels1".
Intact monomeric P2M is present in amyloid deposits of patients receiving chronic hemodialysis'. Aggregates of intact P2M, consisting of dimers and tetramers, have also been isolated from amyloid deposits of patients undergoing chronic hemodialysis". I ? ? . The prominent P-pleated sheet structure of P2M permits it to adopt the fibrillar configura- tion of amyloidh8~77. ] I 7 . By electron microscopy, P2M amy- loid deposits as nodules composed of short, tightly packed bundles of parallel aggregated fibrils with a curvilinear configurationh8 "
Several modified forms of P2M have also been identi- tied in some amyloid specimens. Sera, plasma ultrafiltrate,
195
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

and amyloid deposits contain isoforms of P2M that migrate to a more acidic position than normal P2M on isoelectric focusing124. Although deamidation of Asn to Asp at resi- dues 17 and 42 has been identified in one such isoform of P2M purified from plasma ultrafiltrate of a patient with carpal tunnel syndrome who had undergone hemodialysis for longer than 15 amino terminal amino acid sequencing of six other such P2M isoforms extracted from amyloid depos- its has not demonstrated deamidation of Asn to Asp at resi- due 1 7Iz6. AGE-modified P2M (AGE-P2M), which constitutes about 10% of the total P2M in the sera and urine of patients receiving long-term hemodialysis, also migrates to a more acidic position than normal P2M on isoelectric focusing and has been demonstrated in P2M amyloid deposits6. P2M that is truncated after the amino terminal Lys-6 has also been identified in amyloid deposits from bone and carpal tunnel synovium and P2M truncated after Lys-19 has been found in amyloid kidney stones but not in osteoarticular amyloid deposit~'~' . While this pattern of fragmentation could repre- sent an artifact generated ex vivo during extraction and iso- lation of the amyloid fibrils, it might be produced in vivo by limited proteolysis of P2M at the amino terminus by lysine- specific proteases.
Proteases and protease inhibitors By immunostaining, the human neutrophil proteases
elastase and cathepsin GI2* and matrix metalloproteinases (MMP)129 have been demonstrated in and adjacent to P2M amyloid deposits. The MMP that is expressed most promi- nently in P2M amyloid deposits is MMP-I, which can degrade types I, 11, 111, and X In carpal tunnel synovium, MMP-1 is found in hyperplastic synovial lining cells, in fibroblasts beneath the proliferating synovial lining cells, in mesenchymal cells with chondroid metaplasia, and in granulation tissue. MMP- 1 expression correlates with the degree of macrophage infiltration and synovial proliferation but not with the amount of amyloid deposition or duration of hemodialysis. To a lesser degree, MMP-2 is also present in fibroblasts beneath the synovial lining cells and MMP-9 is present in capillary endothelial cells in areas of neovascularization. In the hip joint, MMP-I is expressed by chondrocytes beneath P2M amyloid deposits in articular cartilage, by mesenchymal cells in and around amyloid deposits, and by periosseous fibroblasts and osteoclasts at the interface between subchondral bone and amyloid. These osteoclasts also express MMP-9129. However, although enzymatic activity characteristic of elastase and cathepsin G is associated with fibrils isolated from deposits of P2M amy- loid, collagenolytic activity is notlz8.
The presence of protease inhibitors in P2M amyloid deposits may account for the absent collagenolytic activity ofthese MMP. Tissue inhibitors ofmetalloproteinase (TIMP)
have been identified around deposits of P2M a m y l ~ i d ' ~ ~ , I".
TIMP-1 is found in synovial lining cells and in capillary endothelial cells in areas of neovascularization; TIMP-2 is present in fibroblasts beneath the synovial lining cells129. Amyloid P component, which has been reported to inhibit the proteolytic activity of elastase in v i r r ~ ~ ~ l , is found in the interstitial space between P2M amyloid fibrils12'. Anti- thrombin 111, a,-proteinase inhibitor130, and a,-macroglobu- lin130, 132 , are also present in P2M amyloid deposits as well as in surrounding tissue. These molecules may inhibit proteoly- sis or permit limited proteolysis of P2M at the site of fibril deposition.
Other macromolecules Deposits of dialysis-related amyloid contain macromol-
ecules other than P2M, proteases, and protease inhibitors, which may influence the formation or deposition of P2M amyloid fibrils Ubiquitin, an 8,600 dalton protein that has amyloid enhancing factor activity in a murine model of AA amylo id~s i s l~~ , deposits with P2M amyloid in '35.
Compared with healthy individuals with normal renal hnc- tion, plasma levels of ubiquitin measured by radioimmunoas- say are elevated both in patients with chronic renal failure who have not yet received dialysis therapy and in those who have undergone hemodialysis. This elevation may result from decreased renal clearance of ubiquitin. Plasma ubiquitin concentrations increase with longer duration of hemodialysis and are significantly higher in patients with carpal tunnel syndrome than in those without carpal tunnel syndrome, despite the two groups having similar serum con- centrations of P2M13'. Thus, could ubiquitin promote the formation of P2M amyloid in patients with chronic renal failure?
An 85,000 dalton heterodimer protein, with subunit molecular weights ofapproximately 55,000 and 30,000 daltons, has been purified from sera of patients undergoing hemodi- alysis and identified in P2M amyloid This heterodimer binds the fluorescent dye, thioflavin T. Whereas the 85,000 dalton protein has a novel amino terminal amino acid sequence, the smaller subunit chain of the heterodimer has been identified as the K light chain137. Although the function of the 85,000 dalton heterodimer protein or of K
light chains in P2M amyloid deposits is not known, electron microscopy with double label immunogold staining demon- strates colocalization of amyloid filament immunoreactivity with antibodies to P2M and K light chains137, 13*. The 14,000 dalton human globin P-chain is also associated with P2M amyloid fibrils139.
Proteoglycans and glycosaminoglycans surround the nodules and bundles of P2M amyloid but are not present on the amyloid fibrils t h e m ~ e l v e s ' ~ ~ . Chondroitin sulfate is the major glycosaminoglycan that surrounds P2M amyloid
196
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin. Invest. I, 187-211 (1997)
fibrils1", I d ' ; in contrast, dermatan sulfate and heparan sul- fate are the major glycosaminoglycans surrounding AL and AA amyloid fibrilslJO. Nishi and colleagues12' suggested that the proteoglycans and glycosaminoglycans may have a regu- latory effect on the distribution and arrangement of P2M amyloid fibrils.
Cellular constituents Macrophages are the predominant cell type infiltrating
P2M amyloid deposits28, in contrast to AL or AA amyloido- sis, where little inflammatory cell infiltration is observed around amyloid In tenosynovial tissue, the macrophage infiltration occurs mainly around blood ves- sels"'. Immunohistochemical staining reveals these mac- rophages to express HLA-DR and the CDI 3, CD14, CD33'", and CD68 antigens on their surfaces and to contain 1L-1 P, TNFa'*, and IL-6Id3. Many of these macrophages also ex- press the adhesion molecules LFA-1 (CDl IdCDI S), Mac- 1 (CD 1 1 b/CDl S), and VLA-4 (CD49dlCD29) on their sur- faces"'. The degree of inflammatory cell infiltration corre- lates with the extent of P2M amyloid deposition, with little cellular infiltration around small deposits of P2M amyloid. Electron microscopy provides evidence of phagocytosis of P2M amyloid fibrils by macrophages, with protruded cyto- plasmic processes engulfing amyloid fibrils and phagolysosome-like vacuoles containing amyloid fibrils6*
Multinucleated giant cells, some of which have phago- cytosed amyloid, may be present in areas with significant P2M amyloid depositionz8. Lymphocytes are infrequently detected around P2M amyloid deposits'44.
At the edges of bone cysts containing P2M amyloid, trabecular bone appears eroded with scalloped margins145. Osteoclast activity is slightly increased, whereas no signs of bone regeneration by osteoblasts are evident. Electron microscopy of mesenchymal cells and osteolining cells that have engulfed P2M amyloid fibrils from bone cysts reveals degeneration of the cell membranes and intracellular organs'23. This may represent the rnorphologic correlate of the observation that P2M inhibits calcification of cultured murine os t e~b las t s l~~ .
Pathogenesis
Various factors have been implicated in the pathogen- esis of P2M amyloidosis. Retention of the subunit protein P2M by patients with chronic renal failureI2' is presumed to be the basic requirement for the initiation of P2M amyloid deposition. Poor biocompatibility of dialysis membranes has been suggested as a cause of P2M amyloidosis, although it does not completely account for the development of this
condition. AGE-modification of proteins, elevated levels of cytokines, and impaired bone metabolism may promote P2M amyloid deposition.
Elevated concentrations of 0,-microglobulin Because P2M forms amyloid fibrils at high concentra-
t i on~ '~ ' , it has been proposed that the dialysis-related amy- loidosis is due to the elevated P2M levels seen among patients undergoing hemodialysis. Levels of P2M in syn- ovial fluid, where P2M amyloid deposition is most promi- nent, are similar to those in serum148. However, serum levels of P2M in patients with carpal tunnel syndrome caused by amyloidosis are not appreciably higher than levels of P2M in patients without carpal tunnel syndrome who have un- dergone hemodialysis for an equivalent durationlJ9. Serum P2M levels are comparable for patients of different ages, despite the increased prevalence of dialysis arthropathy among older patientsIs0. Thus, dialysis-related amyloidosis cannot be explained solely on the basis of chronically elevated levels of 132M.
Dialysis membranes The role of the dialysis membrane in the pathogenesis
ofP2M amyloidosis is uncertain. The epidemiologic studies published are limited by small numbers of patients dialyzed exclusively on the newer membranes. In one study, the inci- dence of carpal tunnel syndrome was greater among pa- tients who had been dialyzed against cellulose-based cuprophane membranes than among those dialyzed exclu- sively against the polyacrylonitrile membrane AN69I5'. In a larger European multicenter bone cysts, but not carpal tunnel syndrome, were observed more frequently among patients dialyzed against cuprophane membranes than among those dialyzed against AN69. Polyacrylonitrile membranes are considered to be more biocompatible than cuprophane membranes because they induce less intradialytic leukopenia and hypotension and do not acti- vate complement by the alternative pathway to generate the anaphylatoxin C5a1". Thus, it has been proposed that P2M amyloidosis may be caused by dialysis with less biocompatible membranes.
Contact with dialyzer membranes may enhance P2M production by cells. Transcription of P2M mRNA in lym- phocytes is stimulated by contact with cuprophane dialyzer membranes; this transcription is stereospecifically inhibited by the soluble carbohydrate L-fucose"'. These lymphocytes express increased amounts of P2M and HLA Class I antigen on their surface. P2M production by peripheral blood mono- nuclear cells cultured inside hollow fiber dialyzer membranes is higher when cells are incubated with cuprophane mem-
197
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

brane than when cells are incubated with either of the more biocompatible polymethylmethacrylate (PMMA) or AN69 membrane^'^^. P2M production by peripheral blood mono- nuclear cells in vitro is also increased in cells isolated from patients receiving intermittent hemodialysis with a new cuprophane membrane but not in cells isolated from patients receiving hemodialysis with the more biocompatible PMMA membrane. Incubation of these mononuclear cells with IL- 1 P or C5a further increases P2M produ~ t ion l~~ .
However, P2M amyloidosis is not completely explained by poor biocompatibility of membranes. In a French multicenter study17, the prevalence of dialysis-related arthr- opathy was similar among patients undergoing dialysis for more than 10 years regardless of whether they had been dialyzed against cuprophane or the more biocompatible AN69 membranes. P2M is not generated during hemodialysis with cuprophane membranes; when corrected for the decrement in extracellular volume (instead ofplasma volume), P2M lev- els do not increase’55. Serum P2M levels ofpatients on CAPD are comparable to levels of patients on hemodialy~is l~~. Finally, hemodialysis is not necessary for the deposition of P2M amyloid: deposits have been reported in patients with chronic renal failure who had never undergone d i a l y ~ i s ~ ~ - ~ ~ and in patients who had been treated exclusively with CAPD’57.
Advanced glycation end products The predominant form of P2M in amyloid fibrils extracted
from carpal tunnel tissue specimens of patients undergoing hemodialysis is modified with AGE6. AGE have several char- acteristic properties: they are yellow-brown in color, fluo- resce with emission at 440 nm upon excitation at 370 nm, and covalently crosslink macromolecule^^^^. AGE-modified pro- teins exhibit enhanced binding to collagen and trap nonglycosylated serum proteins, such as immunoglobulin, albumin, and low-density lipoprotein. AGE-modified proteins are less susceptible to degradation by proteases than are unmodified proteins9, 159. AGE generate reactive oxygen intermediatesI6O. These properties of AGE-modified proteins are presumed to contribute to the development of athero- sclerosis and various complications of diabetes mellitus, in- cluding nephropathy, neuropathy, retinopathy, and cataracts9, I 6 I .
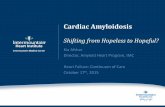
Post-translational modification of proteins with AGE results from nonenzymatic glycosylation by the Maillard reaction between reducing sugars and free amino groups on proteins (Figure 4). In the first step ofthe Maillard reaction, an a-amino group of the N-terminal amino acid or the E- amino group of lysine reacts with the carbonyl group of a reducing sugar to form a Schiff base. This step is reversible and reaches equilibrium over several hours’62. The Schiff base then undergoes intramolecular rearrangement to form
the more stable Amadori product, reaching equilibrium over 28 days. This second step is also reversible but the Keg is 8.4, favoring Amadori product f ~ r m a t i o n ’ ~ ~ . The Amadori products subsequently undergo a series of irreversible chemical reactions, including dehydration and rearrange- ment, to form highly reactive carbonyl compounds, such as 3-deoxyglucosone [3-deoxy-D-erythro-hexos-2-ulose] (3- DG)164. Over weeks to years, Amadori products undergo condensation with these carbonyl compounds, with other Amadori products, and with additional reactive amino groups to form AGEI6*.
Glucose concentration and protein half-life, among other variables, determine the extent of Amadori product and, con- sequently, ofAGE formation165. Thus, AGE and their precur- sors accumulate in diabetes mellitus and aging because of increased production. Patients with diabetes mellitus and hyperglycemia have higher concentrations than healthy euglycemic individuals of 3-DG166, AGE-modified plasma
and Amadori products, such as hemoglobin
AGE irreversibly bound to long-lived proteins, such as collagen158 and lens ~ rys t a l l i n l~~ , accumulate with age. Pro- teins with long half-lives, such as amyloid fibril subunit pro- teins6. I7O, are more susceptible to AGE-modification. The accumulation of AGE-modified proteins with age corresponds with the observations that P2M amyloidosis occurs earlier93 and is more prevalentg2 among older patients with chronic renal failure.
The functioning kidney clears AGE-modified proteins better than do dialysis modalities. Thus, AGE accumulate in uremia because of decreased removal. Serum concentrations of AGE-modified low molecular weight (2,000 to 6,000 dalton) proteins are 2 or 3 times lower in nondiabetic individuals with normal renal h c t i o n or with functioning renal allografts than in nondiabetic patients receiving conventional or high- flux hemodialysis or CAPD17’. Additionally, serum levels of the AGE precursor 3-DG are 5 or 6 times lower in nondiabetic individuals with normal renal function than in nondiabetic patients receiving conventional hemodialysis or CAPD1”. The presence of elevated serum levels of 3-DG and AGE- modified low molecular weight proteins in patients with chronic renal failure undergoing hemodialysis or CAPD par- allels the occurrence of P2M amyloidosis in these popula- tions. The absence of elevated serum levels of 3-DG and AGE-modified low molecular weight proteins in nondiabetic patients with hnctioning renal allografts is consistent with the observation that P2M amyloid deposits do not progress, and may even regress, in patients who have undergone suc- cessful renal tran~plantationl~~.
AGE-modified proteins are specifically recognized by a receptor present on the surface of mononuclear phagocytes and endothelial cells. This 35,000 dalton receptor for AGE (RAGE) is a member of the immunoglobulin ~ u p e r f a m i l y ~ ~ ~ .
Alc168.
198
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amvloid: Int. J. EXD. Clin. Invest. 4. 187-211 (1997)
On mononuclear phagocytes and endothelial cells, a 30,000 dalton lactoferrin-like polypeptide (LF-L) binds noncovalently to the extracellular domain of RAGE, forming a RAGE/LF-L complex that also binds AGE'75.
Binding of AGE-modified proteins to the RAGEILF-L complex on mononuclear phagocytes results in various cel- lular responses. Cells exposed to AGE-modified proteins may exhibit signs of oxidant The concentrations of reactive oxygen intermediates generated by AGE-modified proteins can activate the transcription factor NF-KB in the promotor of genes encoding cytokines, resulting in enhanced cytokine gene e x p r e ~ s i o n ' ~ ~ . AGE-modified proteins induce the secretion of proinflammatory cytokines, such as interleukin- 1 (IL- l), tumor necrosis factor-a ( T N F c ~ ) ' ~ ~ , and interleukin-6 (IL-6)I8". Binding of soluble AGE-modified pro- teins to the RAGE/LF-L complex on mononuclear phago- cytes initiates monocyte chemotaxis; binding of immobilized AGE to this complex slows the migration of mononuclear phagocytes and may lead to the concentration of mono-
nuclear phagocytes in tissue deposits, such as P2M amy- loid deposits, which contain AGE-modified
AGE-modified P2M (AGE- P2M) is present in the sera and urine of patients receiving long-term hemodialysis but not of healthy individuals with normal renal functionb. Pentosidine'* ' , NE-(carboxymethyl)lysine18?, and i rn idaz~ lone '~~ are AGE structures present on AGE-P2M in amyloid deposits of patients who had received long-term hemodialysis. The a-amino group ofthe amino-terminal iso- leucine residue is the primary glycated site on AGE-P2M purified from the urine of patients undergoing hemodialy- sis; the &-amino groups of lysine residues in at least six positions are additional sites of gIycationlE4.
AGE formation in types I, 11, and I11 collagens (the pre- dominant collagens in osteoarticular tissue) is increased com- pared with type IV collagen (a collagen found in basement membranes) when each is incubated for 30 days with glu- cose under identical conditionsIs5. P2M binds readily to immobilized types I, 11,111, and IV collagen in vitro whether
pi + L 'y H \ ,o
1 CH C
CH,OH ,!&- Microglo bulin CH20H
7
( y w 4 NHZ I (CHOHh
Glucose Schiff Base
NH
y 2
'F '
(YHOH), ( y w ,
-I- !H2 -- C = O NH2
CH,OH CH,OH
3-Deoxyglucasone Amadori Product (Carbonyl Compound)
AGE-P,-Microg lo bul in
m
FIGURE 4. Post-translational modification of (12M with AGE. In the first step of the Maillard reaction, an amino group reacts with the carbonyl group of a reducing sugar to form a Schiff base. The Schiff base then undergoes intramolecular rearrangement to form the more stable Amadori product. The Amadori products subsequently undergo a series of irreversible chemical reactions, including dehydration and rearrangement, to form highly reactive carbonyl compounds, such as 3-deoxyglucosone [3-deoxy-D- erythro-hexos-2-ulose] (3-DG). Amadori products ultimately undergo condensation with these carbonyl compounds, with other Amadori products, and with additional reactive amino groups to form AGE, such as pentosidine, Nr-(carboxyrnethy1)lysine (CML), and imidazolone.
lrnidazalone Ho
199
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

the collagen is modified with AGE or unmodifiedlB5. The amount of P2M that binds collagen is dependent on the concentration of either collagen or P2MIa6. However, signifi- cantly more P2M binds to immobilized AGE-modified type I collagen than to unmodified type I collagen18s. At the same concentration, more normal (unmodified) P2M binds to immobilized AGE-modified type I collagen than does AGE- P2M. Once bound to AGE-modified type I collagen, normal P2M undergoes AGE modification in sitdX5. These data sup- port the hypothesis that normal P2M binds to AGE-modi- fied collagen, which is probably more abundant in osteoarticular tissue than in visceral basement membranes of older patients with chronic renal failure and that AGE formation subsequently occurs in the bound P2M. Once modified, the AGE-P2M may form cross links with the AGE- modified collagen. These cross-linked AGE-P2M collagens may ultimately be incorporated into deposits of P2M amyloid.
Of the different isoforms of P2M purified from the sera and urine of patients receiving long-term hemodialysis, AGE- P2M appears to be responsible for the observed biologic activity. AGE-P2M, but not normal P2M, enhances both chemotaxis (directed migration) and chemokinesis (random migration) of human monocyteslS7. AGE-P2M, but not nor- mal P2M, induces enhanced oxidant stress and the elabora- tion of reactive oxygen intermediates by monocytesLsx. AGE-P2M might also contribute to the elevation of TNFaIa9, IL-1 IS9, and IL-61y0 levels observed in patients undergoing long-term hemodialysis. AGE-P2M induces synthesis and secretion of TNF-a187,18s, IL-1 P I x 7 , and IL-6Iy1 by macroph- ages, whereas macrophages incubated with normal P2M secrete much lower amounts of TNF-alS7, IL-1 PlS7, and IL- 6I9l. Neither deamidated P2M nor P2M modified with Amadori products elicits monocyte chemotaxis or induces secretion of TNF-a, 1L- 1 P, or IL-6 significantly more than does normal p2MIy2. The amounts of TNF-a and 1L-lP secreted by macrophages incubated with AGE-P2M are suf- ficient to induce transcription of collagenase mRNA by cul- tured human synovial cells and morphologic changes, with the synovial cells becoming dendritic in shapeIs7. Both chemotaxis and synthesis and secretion of TNF-a by mono- cytes are mediated by interaction between AGE-P2M and RAGEIa8. AGE-P2M-induced secretion of TNF-a by mono- cytes involves oxidant stress, since release of this cytokine is inhibited in the presence of the antioxidant N - acetylcysteineLa8.
AGE modification of proteins and binding of amyloid precursor proteins to RAGE may also be involved in the pathogenesis of amyloid diseases besides P2M amyloido- sis. Immunostaining of hippocampal tissue from patients with Alzheimer’s disease has demonstrated the AGE pyrroline and pentosidine to be associated with amyloid-P peptide (AD) and tau protein in neurofibrillary tangles and senile
plaqueslg3. AGE-modified recombinant human tau protein, when introduced into cultured neuroblastoma cells. results in more synthesis of AP precursor and release of AP by these cells than when they are loaded with nonglycated recombinant human tau RAGE mediates the spe- cific binding of AP to the surface of mouse brain endothelial cells, rat cortical neurons, and the mouse microglial cell line BV-2, although through structural determinants distinct from AGEIy4. RAGE expression is increased on neurons close to AP deposits, and RAGE levels are increased about 2.5-fold in brain of patients with Alzheimer’s disease compared with age-matched Interaction of AP with RAGE induces migration of microglia and accumulation of micro- glia at deposits of AS, as well as transcription, translation, and secretion of TNFa by m i ~ r o g l i a ’ ~ ~ . The similarity be- tween the RAGE-mediated effects of AGE-P2M and of AP on mononuclear phagocytes suggests that analogous inter- actions between amyloid precursor proteins and RAGE might also occur in other amyloid diseases.
Cytokines The “interleukin hypothesis,” which was proposed by
Henderson and colleagues19s in 1983, states that the recur- rent induction of cytokines during the hemodialysis proce- dure causes the chronic complications seen among patients undergoing long-term hemodialysis. Elevated levels of cytokines, including IL-1, TNFa, and IL-6, are observed in patients with chronic renal failure receiving hemodia lys i~ ’~~ lye. In addition, TNFa levelsLs9 and IL-6 activityLg0 are elevated in the plasma of uremic patients who have not yet undergone dialysis. P2M amyloidosis, which occurs both in patients undergoing hemodialysis and in individuals not yet exposed to dialysis membranes, may be a complication of chronic renal failure that develops, in part, as a conse- quence of these elevated plasma levels of cytokines.
Various substances to which patients are exposed dur- ing the hemodialysis procedure stimulate mononuclear leu- kocytes to produce cytokines, such as TNFa and IL-1. These substances include acetate in the dialysateLy6, lipopolysac- charide (endotoxin) contaminating the dialy~ate’~’, mem- brane-derived carbohydratesLy8, and C5a generated by membrane-induced complement activationly9 2oo. In addition. AGE-P2M stimulates mononuclear leukocytes to produce TNFa, IL-1 lSs, and IL-6I9’. Mononuclear cells obtained from carpal tunnel tenosynovium of patients undergoing long-term hemodialysis have spontaneously produced IL- 1 P and IL-6 in tissue culture”’, perhaps in response to stimu- lation by AGE-P2M.
The elevated levels of cytokines in the plasma of patients with chronic renal failure may induce P2M produc- tion. Cytokines, such as interferon-y (IFN y). TNFa, and IL- 1, as well as lipopolysaccharide, stimulate the synthesis and
200
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997)
release of P2M by macrophages in vitro202. TNFaZo3 and IL- lZo4 each augment the expression of HLA Class I antigens, with a concomitant increase in P2M expression, on the sur- face of nucleated cells. TNF-a and IL-1 P each may also act synergistically with interferon-y (IFN-y) to increase cell sur- face expression of HLA Class I antigens on nucleated cells beyond that induced by IFN-)I alone205. Although IL-6, ei- ther alone or in combination with IFN-y, has no effect on HLA Class I antigen expression on the surface of nucleated cells’05, IL-6 induces P2M secretion by human hepatoblastoma and hepatoma cells in vitro and may stimu- late P2M production by hepatocytes in vivo206.
Hypothetical mechanism for the formation of P2M amyloid deposits
Noncovalently bound P2M is released from the surface of cells that shrink and swell in response to changes in osmotic pressure that occur during hernodialy~is’~~. Because of renal failure, decreased catabolism and decreased excre- tion of P2M result in increased serum levels of free P2M. Circulating P2M then can bind to AGE-modified collagen: the affinity of P2M for types I, 11, and I11 collagens, which occur in osteoarticular tissue, is greater than that for type IV collagen, which is present in basement Once bound to AGE-modified collagen, P2M itself may be modi- fied with AGE in situ. The AGE-P2M then can form crosslinks with the AGE-modified collagen.
The cross-linked AGE-P2M and AGE-modified collagen could trap other constituents of the P2M amyloid deposits, such as amyloid P component and ubiquitin. Ubiquitin may promote the formation of amyloid. Limited proteolysis of the P2M. perhaps regulated by the protease inhibitors that are found in P2M amyloid deposits, might also contribute to the formation of amyloid fibrils. Proteoglycans andor glycosami- noglycans, such as chondroitin sulfate, may regulate the distribution and arrangement ofthese P2M amyloid fibril^'?^.
P,-microglobulin and bone metabolism The amyloid subunit protein P2M may also contribute
to the development of renal osteodystrophy. Various effects of human P2M on bone metabolism have been observed in wtro when physiologic concentrations of P2M have been studied in rodent models ofbone remodeling. P2M has growth factor-like activity and regulates bone formation, as do insu- lin-like growth factor I (IGF I) and transforming growth fac- tor P (TGF-P)208. P2M stimulates synthesis ofDNA, collagen, and noncollagen proteins by intact fetal rat calvariae and fetal rat osteoblast-enriched cellszoq. This growth-promot- ing activity of P2M is mediated, at least in part, through IGF I but not TGF-P. P2M enhances IGF I binding to fetal rat
osteoblast-enriched cells by increasing IGF I receptor num- ber and IGF I synthesis and secretion208.
The effect of human P2M on proliferation of osteoblasts, as assessed by DNA synthesis and collagen synthesis by cultured tissues, varies depending upon the source of P2M, the concentration of P2M, and the tissue examined. At con- centrations comparable to those found in plasma of patients receiving hemodialysis, human P2M stimulates cell prolif- eration in fetal rat calvarial organ culture, in isolated fetal rat osteoblast-enriched cell culture209, and in isolated human osteoblast-like bone cell culture2’0. However, even at con- centrations similar to those found in plasma of patients receiving hemodialysis, P2M purified from plasma of uremic individuals has no effect on cell proliferation in cultures of mouse calvaria-derived osteoblasts2’ I . Furthermore, at lower concentrations, human P2M does not stimulate DNA syn- thesis in neonatal mouse calvarial organ culture2I2 or in iso- lated human osteoblast-like bone cell Likewise, at concentrations comparable to those found in plasma of patients receiving hemodialysis, P2M purified from plasma of healthy individuals stimulates collagen synthesis both in fetal rat calvarial organ culture and in isolated fetal rat osteo- blast-enriched cell culture209, whereas P2M purified from plasma of uremic individuals has no effect on collagen syn- thesis in mouse calvaria-derived osteoblast cell culture2”. Based upon these in vitro data, the in V I V O effect of P2M on cell proliferation and collagen synthesis by osteoblasts in patients with chronic renal failure cannot be predicted.
P2M also impairs bone mineralization. P2M inhibits cal- cification, but not collagen synthesis, in cultures of mouse calvaria-derived osteoblasts2”. P2M also induces calcium efflux in cultures of neonatal mouse calvariae, probably by stimulating bone resorption and uncoupling bone formation from resorption or inhibiting bone formation2I2 2 1 1 . This cal- cium efflux, which may occur as a result ofthe interaction of P2M with other growth factors, such as IGF I , is directly mediated by IL-1 P but not by prostaglandins213. AGE-P2M induces more IL-1 P production by cultured neonatal mouse calvariae than does normal P2M; this increased IL- 1 p pro- duction augments calcium effluxZIJ. Thus, P2M and AGE- P2M may contribute to the development ofthe osteomalacia that is observed in patients with renal osteodystrophy by enhancing synthesis of bone matrix proteins and interfering with bone mineralization.
Additionally, P2M stimulates collagenase synthesis and secretion by rabbit synovial and human skin fibroblasts in vitro”’. IL-1 and TNFa, levels of which are elevated in the circulation of patients with chronic renal failure, also stimu- late collagenase production by synovial cells and skin fibro- blasts216. Breakdown of cartilage and bone caused by collagenase, the synthesis of which can be induced by P2M and cytokines, may contribute to the development of bone
20 1
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

cysts and of the destructive spondyloarthropathy observed in patients with P2M amyloidosis.
Treatment
Presently, no treatment is available to reverse P2M amy- loid deposition, Medical therapy of patients with 132M amy- loidosis is symptomatic. Surgery may be necessary for patients with large deposits of P2M amyloid. Successful renal transplantation can halt the progression of some mani- festations of P2M amyloidosi~l'~. However, in the future, medications that inhibit AGE formation might interfere with the pathogenesis of this condition.
Medical therapy Physical and occupational therapeutic modalities may
lessen the disability associated with musculoskeletal mani- festations of P2M amyloidosis. Wrist splints for carpal tun- nel syndrome and adaptive devices to assist with activities of daily living are useful. Heat and range-of-motion exer- cises for the shoulder increase mobility. Conservative treat- ment of cervical destructive spondyloarthropathy consists of immobilization of the neck in a cervical collar27. The intraarticular injection of corticosteroids or the application of 10% hydrocortisone cream to the shoulder using phonophoresis may greatly decrease the pain associated with the shoulder periarthritis of dialysis-related amyloido- sis and permit increased shoulder function.
Nonsteroidal anti-inflammatory drugs are usefid in treat- ing symptoms of pain involving multiple joints26. Because of the increased risk of bleeding in patients undergoing dialy- sis, consideration should be given to the concurrent use of a prostaglandin analogue, such as misoprostol. Joint pain and restriction of motion may improve in patients with P2M amyloidosis who are treated with oral prednisone, up to 8 mgiday, although symptoms recur within 48 hours upon the discontinuation of prednisone2I7. However, the potential risks of corticosteroid-induced bone loss and atherosclerosis limit the use of low-dose prednisone to patients whose P2M amy- loidosis has not responded to other forms of medical therapy.
Surgical intervention Carpal tunnel release is indicated for patients who have
symptoms unresponsive to conservative management; how- ever, symptoms may recur after surgery has been performed, requiring re-exploration of the carpal tunnel24. Arthroscopic release of the transverse carpal ligament, performed through a smaller skin incision on the forearm, may yield results simi- lar to those achieved with open carpal tunnel release21s.
Arthroscopic resection of the coracoacromial ligament may provide symptomatic relief of shoulder pain related to de- posits of P2M amyloid2'.
If the cervical spine is unstable and neurologic findings progress, surgical fusion of the cervical spine is indi~ated?~. When spinal cord compression is present, a decompressive laminectomy may permit recovery of neurologic function3*
Pathologic fractures through P2M amyloid deposits in the femoral neck should be treated by total hip arthroplasty with a cemented femoral component because of the compro- mised structural integrity of the involved bone2I9. Internal fixation of the femoral neck in patients with bone cysts or pathologic fractures due to P2M amyloid deposition fre- quently results in migration of the pin or screw and is not recommended220,221. Cystic lesions in the femoral neck of 2.5 cm or more in diameter, where at least half of the surrounding cortex is destroyed, or that cause pain on weight bearing should be treated prophylactically to prevent fracture, either by curettage and bone grafting222 or by total hip arthroplasty22'.
40. 4 1
Choice of dialysis modality The role of dialysis with less biocompatible membranes
in the pathogenesis of P2M amyloidosis is controversial. More biocompatible membranes, such as polyacrylonitrile (AN69), do not necessarily reduce the incidence of dialysis- related amyloidosi~'~. However, the greater reduction in cir- culating P2M levels achieved with high-flux hemodialysis using more biocompatible membranes, such as polysulfone, compared with conventional hemodialysis using less biocompatible membranes, such as c u ~ r o p h a n e ~ ~ , might lessen the degree to which renal osteodystrophy occurs.
Renal transplantation Serum levels of P2M fall rapidly following successful
renal transplantation224. Patients with P2M amyloidosis who undergo successful renal transplantation experience a marked reduction in joint pain and stiffness following transplanta- tion173, 225-229 . Symptoms usually resolve over a period of several days to 6 m ~ n t h ~ ~ ~ ~ - ~ ~ ~ . Joint pain recurs rapidly in patients who resume hemodialysis because of graft rejec- tionz2*, 229. Although prednisone and other immunosuppres- sive therapy may contribute to the reduction in joint pain following renal transplantation2I7, pain relief has been sus- tained despite reduction or complete withdrawal of corticos- t e r o i d ~ ' ~ ~ . This suggests that some factor other than immunosuppressive therapy results in the dramatic improve- ment in symptoms.
Although P2M amyloid deposits detected by Iz3I-la- beled SAP scintigraphy enlarge in patients undergoing he-
202
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997)
modialysis, these deposits do not progress and may regress in patients who have undergone successful renal transplan- t a t i ~ n ” ~ . Following renal transplantation, subchondral bone cysts do not increase in size or number’73. 226-229 . Although cyst size may decrease, bone cysts do not r e ~ o l v e ” ~ , and P2M amyloid has been detected in osteoarticular structures 10 years after successful renal t r ansp lan ta t i~n~~~ . In patients who resume hemodialysis after graft rejection, bone cysts subsequently increase in number229.
Thus, early renal transplantation in appropriate candi- dates, before significant deposition of P2M amyloid has occurred, may be the most effective preventive measure that is presently available for a condition without a definitive cure. However, although renal transplantation is accompa- nied by improvement in the symptoms of P2M amyloidosis and no further enlargement of P2M amyloid bone cysts, it does not stop the development of all manifestations of 132M amyloidosis. Despite successful renal transplantation, destructive cervical spondyloarthropathy progresses with further disk space narrowing and an increase in the size of vertebral end plate erosionszz8.
Aminoguanidine Although there is presently no effective therapy for
(32M amyloidosis other than symptomatic treatment of com- plications, future treatment strategies directed toward inhi- bition of AGE formation might interfere with the pathogenesis of this condition. The nucleophilic hydrazine derivative aminoguanidine hydrochloride reacts with Amadori products and Amadori-derived compounds, such as 3-DG, and inhibits formation of AGE before irreversible protein cross-linking occurs231. When administered to streptozotocin-induced diabetic rats, aminoguanidine pre- vents or delays the occurrence of r e t i n ~ p a t h y ~ ~ ~ , nephropa- thy’3’ ‘j4, and n e ~ r o p a t h y ~ ~ ~ . Additionally, it prevents the formation of AGE and hyperglycemia-induced collagen cross-linking in arterial wall connective tissue of alloxan- induced diabetic The ability of aminoguanidine to delay the development of nephropathy is being studied in phase 111 clinical trials in patients with type I and type I1 diabetes mellitus2-”.
Aminoguanidine is well absorbed from the gastrointes- tinal Approximately 80% of the orally administered dose is excreted in the urine by individuals with normal renal function; in individuals with impaired renal function, the clearance of aminoguanidine is directly proportional to the glomerular filtration rate. Patients undergoing chronic hemodialysis tolerate the oral administration of aminoguanidine with minimal, if any, side effects. Aminoguanidine may be administered orally three times weekly after hemodialysis and is effectively removed from plasma by hemodialysis. Clinical trials of aminoguanidine in
patients with chronic renal failure will be necessary to deter- mine whether this compound can halt or delay the develop- ment of P2M amyloidosis.
Future directions for study
Further study of the epidemiology of P2M amyloidosis is needed. The prevalence of P2M amyloidosis should be estimated in a large population ofpatients with chronic renal failure using reliable and specific noninvasive diagnostic methods. Although the musculoskeletal manifestations of p2M amyloidosis have been well characterized, additional investigation is necessary to determine the actual extent of visceral involvement by this condition. This information will help to predict which patients are at risk for the complica- tions associated with visceral P2M amyloid deposition.
The occurrence of P2M amyloidosis in diabetic patients with chronic renal failure also requires further investigation. Because diabetic patients receiving hemodialysis may not live long enough for clinically evident P2M amyloidosis to develop, shoulder ultrasonography or scintigraphic imag- ing with 1231-serum amyloid P component might be employed to detect the appearance of early, asymptomatic deposits of P2M amyloid.
Medical therapy must be developed to prevent the oc- currence of P2M amyloidosis and permit regression of amy- loid deposits. At present, no preventive intervention exists other than for renal transplantation, which only stabilizes many of the existing signs and symptoms of this disease and might delay further amyloid deposition. Because AGE appear to play a pivotal role in the development ofthis con- dition, a trial of aminoguanidine in patients with chronic renal failure is warranted to determine whether this drug can interfere with the clinical manifestations of this disease.
A predictive test would be useful to help decide which patients would benefit most from a treatment to prevent the development of P2M amyloid. It might be used to determine the optimal timing of renal transplantation. However, based upon the current understanding of the pathogenesis of P2M amyloidosis, neither the total serum P2M level nor the circu- lating AGE-P2M level is a promising candidate for such a test . Further investigation of the mechanism by which P2M amyloidosis develops is necessary and may also shed light upon the pathogenesis of the other amyloid disorders.
Summary
P2M amyloidosis is a complication ofchronic renal fail- ure that has been recognized mostly in patients receiving long-term hemodialysis. The clinical features of this condi-
203
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

tion are particularly evident in the musculoskeletal system: patients with P2M amyloidosis typically present with the triad of shoulder periarthritis, carpal tunnel syndrome, and flexor tenosynovitis of the hands. Other musculoskeletal manifestations of P2M amyloidosis include destructive spondyloarthropathy, cervico-occipital pseudotumors, bone cysts, and pathologic fractures. Visceral and cutaneous deposits of P2M also occur and may cause clinical symptoms.
The pathogenesis of P2M amyloidosis is not entirely understood. Important factors may include elevated levels of P2M, limitedproteolytic cleavage of P2M, modification of P2M and other proteins with AGE, and elevated circulating levels of proinflammatory cytokines. The type of dialysis membrane used may affect P2M production and clearance and, by generating C5a through activation of the alternative complement pathway, cytokine production.
At present, only renal transplantation may slow or halt the progression of P2M amyloidosis. Medical therapies may decrease pain associated with this condition but do not alter the disease course. Surgical procedures may be used to remove large deposits of P2M amyloid and to replace joints that have been damaged by these deposits. Future treat- ment strategies might address biologic processes involved in the pathogenesis of P2M amyloidosis, such as AGE modi- fication of proteins, to prevent progression and permit regression of this disabling complication that affects patients with chronic renal failure.
References
Warren DJ and Otieno LS (1975). Carpal tunnel syndrome in patients on intermittent haemodialysis. Postgrad Med J 51, 450-452 Scribner BH (1990). A personalized history ofchronic hemo- dialysis. Am JKidneyDis 16, 511-519 Kenzora JE (1978). Dialysis carpal tunnel syndrome. Ortho- pedics 1 I 195-203 Assenat H, Calemard E. Charra B. Laurent G, Terrat JC and Vanel T (1980). Hemodialyse: syndrome du canal carpien et substance amyloi'de [letter]. Nouvelle Presse Mid 9, 17 15 Gejyo F, Yamada T, Odani S, Nakagawa Y, Arawaka M, Kunimoto T, Kataoka H. Suzuki M. Hirasawa Y, Shirahama T. Cohen AS and Schmid K (1985). A new form of amyloid protein associated with chronic hemodialysis was identified as P2-microglobulin. Biochem Biophys Res Commun 129: 70 1 - 706 Miyata T, Oda 0, Inagi R, Iida Y. Araki N: YamadaN, Horiuchi S, Taniguchi N. Maeda K and Kinoshita T (1993). Dz- microglobulin modified with advanced glycation end prod- ucts is a major component of hemodialysis-associated amyloidosis. JClin Invest 92. 243-1252 Athanasou NA, Ayers D, Rainey AJ, Oliver DO and Duthie RB (1991). Joint and systemic distribution of dialysis amy-
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
loid. Quart JMed 78.205-2 14 Gray RG and Gottlieb NL (1976). Rheumatic disorders asso- ciated with diabetes mellitus: literature review. SeminArthri- tis Rheum 6,9-34 Brownlee M, Vlassara H and Cerami A (1984). Nonenq- matic glycosylation and the pathogenesis of diabetic compli- cations. Ann Intern .Wed 101, 527-531 Laurent G, Calemard E and Charra B (1988). Dialysis related amyloidosis. Kidney Int 33 (Suppl24) , S32-S34 Hazenberg BPC, Geerlings W, Grond J, van RijswijkMH and van der Hem GK ( 1 990). Clinical evaluation of osteoarthr- opathy in 43 patients on haemodialysis, using cuprophane membranes for 2 5 years. In Natvig JB: Fsrre 0. Husby G, Husebekk A, Skngen B, Sletten K and Westermark P (eds.) Amyloid and Amyloidosis 1990, pp. 373-376. (Dordrecht: Kluwer Academic Publishers) Kurer MHJ, Baillod RA and Madgwick JCA (1991). Muscu- loskeletal manifestations of amyloidosis: a review of 83 pa- tients on haemodialysis for at least 10 years. J Bone Joint Surg [Br] 73-B, 271 -216 Chattopadhyay C. Ackrill P and Clague RB (1987). The shoul- der pain syndrome and soft-tissue abnormalities in patients on long-term haemodialysis. Br JRheumatol26,18 1-1 87 Bardin T, Vasseur M. de Vernejoul MC: Raymond I? Laflorgue B, Judith C, Zingraff J and Kuntz D ( 1 988). Etude prospec- tive de l'atteinte articulaire des malades hemodialyses depuis plus de 10 ans. Rev Rheum 55, 131-134 Goldstein S, Winston E. Chung TJ. Chopra S and Pariser K (1985). Chronic arthropathy in long-term hemodialysis. A m J Med 78,82-86 Brown EA, Arnold IR and Cower PE (1986). Dialysis arthropathy: complication of long term treatment with haemodialysis. Br MedJ292. 163-1 66 Kessler M, Netter P, Azoulay E, Mayeux D, Pere P. Gaucher A and the Co-Operative Group on Dialysis-Associated Arthropathy ( 1992). Dialysis-associated arthropathy: a multicentre survey of 171 patients receiving haemodialysis for over 10 years. Br J Rheumatol31, 1 57- 162 Konishiike T, Hashizume H, Nishida K, Inoue H and Nagoshi M (1996). Shoulder pain in long-term haemodialysis patients. A clinical study of 166 patients. JBone Joint Surg [Br] 78-B.
Murase T and Kawai H ( 1 993): Carpal-tunnel syndrome in hemodialysis: syndrome diagnosed in 8 of 60 patients. .4cta Orthop Scand 64,475-478 Hurst NP, van den Berg R, Disney A. Alcock M. A l b e q n L. Green M and Pascoe V (1989). 'Dialysis related arthropa- thy': a survey of 95 patients receiving chronic haemodialysis with special reference to P, microglobulin related amyloido- sis. Ann Rheum Dis 48,409-420 Kay J, Benson CB. Lester S. Corson JM, Pinkus GS. Lazarus. JM and Owen WF Jr ( 1 992). Utility of high resolution ultra- sound for the diagnosis of dialysis-related amyloidosis. 'Irthritis Rheum 35.926-932 Nakazawa R, Hamaguchi K. Hosaka E. Shishido H and Yokoyama T ( 1 987). Synovial amyloidosis of P2-microglobulin type in patients undergoing long-term hemodialysis [letter]. Nephron 44.379-380 Okutsu 1. Ninomiya S. Takatori Y. Hamanaka I. Takemura T
601-605
204
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: lnt. J. Exp. Clin. Invest. 4, 187-211 (1997)
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
and Otsubo K (1991). Endoscopic management of shoulder pain in long-term haemodialysis patients. Nephrol Dial Trans- plant6, 117-119 Gilbert MS, Robinson A: Baez A, Gupta S, Glabman S and Haimov M (1 988). Carpal tunnel syndrome in patients who are receiving long-term hemodialysis. JBone Joint Surg (Am]
Gejyo F, Homma N and Arakawa M (1988). Carpal tunnel syndrome and 0,-microglobulin-related amyloidosis in chronic hemodialysis patients. Blood Purif6, 125-13 1 Gravallese EM. Baker N, Lester S, Kay J and Owen WF Jr (1 992). Rheumatology Grand Rounds. Musculoskeletal mani- festations in mi micro globulin amyloidosis: case discussion. Arthritis Rheum 35,592-602 Maruyama H, Gejyo F and Arakawa M (1 992). Clinical stud- ies of destructive spondyloarthropathy in long-term hemodi- alysis patients. Nephron 61, 37-44 Ohashi K, Hara M, Kawai R, Ogura Y. Honda K; Nihei H and Mimura N (1 992). Cervical discs are most susceptible to beta,-microglobulin amyloid deposition in the vertebral col- umn. KidneyInt 41,1646-1652 Kuntz D, Naveau 9. Bardin T, Drueke T, Treves R and Dryll A ( 1984). Destructive spondyloarthropathy in hemodialyzed patients: a new syndrome. Arthritis Rheum 27, 369-375 Sundaram M, Seelig R and Pohl D (1987). Vertebral erosions in patients undergoing maintenance hemodialysis for chronic renal failure. AJR 149,323-327 Gerster JC, Carruzzo PA, Ginalski JM and Wauters JP ( 1 989). Cervicooccipital hinge changes during longterm hemodialysis. J Rheumatoll6, 1469- 1473 Kessler M, Netter P, Grignon B, Bertheau JM. Aymard B, Azoulay E and Gaucher A (1990). Destructive p,- microglobulin amyloid arthropathy of the cervico-occipital hinge in a hemodialyzed patient [letter]. Arthritis Rheum 33.
Paillaud E, Clerc D, Berge E, Durandin M and Bisson M (1993). Pseudotumor of the craniocervical hinge in a patient receiving hemodialysis for 4 years [letter]. J Rheumatol20.
Rousselin B, Helenon 0, Zingraff J, Delons S, Drueke T. Bardin T and Moreau JF (1990). Pseudotumor of the craniocervical junction during long-term hemodialysis. Arthritis Rheum 33,1567-1573 Fiocchi 0, Bedani PL, Orzincolo C, Storari A, Cavazzini PL, Malacarne F and Farinelli A (1 989). Radiological features of dialysis amyloid spondyloarthropathy. Int J Artificial Or- gans 12,2 16-222 Orzincolo C, Bedani PL, Scutellari PN, Cardona P. Trotta F and Gilli P ( 1990). Destructive spondyloarthropathy and ra- diographic follow-up in hemodialysis patients. Skeletal Radiol
Kroner G, Stabler A, Seiderer M, Moran JE and Gurland HJ ( 1 99 I). 0, microglobulin-related amyloidosis causing atlanto- axial spondylarthropathy with spinal-cord compression in haemodialysis patients: detection by MRI. Nephrol Dial Transplant 6(Suppl 2), 91-95 Allain TJ, Stevens PE, Bridges LR and Phillips ME (1988). Dialysis myelopathy: quadriparesis due to extradural amy- loid of !3, microglobulin origin. Br Med J296.752-753
70-A. 1145-1 153
602-604
1634-1 635
19.483-487
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
Allard JC, Artze ME, Porter G, Ghandur-Mnaymneh L. de Velasco R and Perez GO (1992) . Fatal destructive spondyloarthropathy in two patients on long-term hemodi- alysis. Am J Kidney Dis 19, 8 1-85 Sanchez R, Praga M, Rivas Salas JJ, Araque A. Mazuecos A, Andres A and Rodicio JL (1 993). Compressive myelopathy due to dialysis-associated amyloidosis. Nephron 65.463-465 Marcelli C, Perennou D. Cyteval C, Leray H, Lamarque J-L. Mion C and Simon L (1996). Amyloidosis-related caudaequina compression in long-term hemodialysis patients: three case reports. Spine 21, 381-385 Ross LV, Ross GJ: Mesgarzadeh M. Edmonds PR and Bonakdarpour A (1 99 I ) . Hemodialysis-related amyloidomas ofbone. Radiology 178.263-265 Sargent MA, Fleming SJ, Chattopadhyay C, Ackrill P and Sambrook P (1 989). Bone cysts and haemodialysis-related amyloidosis. Clin Radiol 40,277-28 1 Gielen JL, van Holsbeeck MT. Hauglustaine D. Verresen L. Verbeken E, Baert AL. Meeus L. Vandevoorde P. Michielsen P and Coral A ( 1 990). Growing bone cysts in long-term he- modialysis. Skeletal Radiol 19,43-49 Huaux JP, Noel H. Bastien P. Malghem J, Maldague 9. Devogelaer JP and Nagant de Deuxchaisnes C (1985). Amy- lose articulaire, fracture du col femoral et hemodial yse periodique chronique. Rev Rhum 52, 179-182 Casey TT, Stone WJ, DiRaimondo CR, Brantley BD. DiRaimondo CV, Gorevic PD and Page DL (1986). Tumoral amyloidosis of bone of beta,-microglobulin origin in associa- tion with long-term hemodialysis: a new type of amyloid disease. Hum Pathol17.73 1-738 Bardin T, Zingraff J. Shirahama T,Noel LH, Droz D. Voisin MC. Drueke T. Dryll A, Skinner M. Cohen AS and Kuntz D ( 1987). Hemodialysis-associated amyloidosis and beta-2 microglobulin: clinical and immunohistochemical study. Am J Med 8 3 , 4 19-424 Campistol JM, Sole M, MuAoz-Gomez J, Riba J. Ramon R and Revert L (1990). Pathological fractures in patients who have amyloidosis associated with dialysis. JBone Joint Surg LAm] 72-A, 568-574 Onishi S. Andress DL, Maloney NA, Cobum JW and Sherrard DJ (1991). Beta,-microglobulin deposition in bone in chronic renal failure. Kidney Int 39,990-995 Gal R, Korzets A, Schwartz A. Rath-Wolfson L and Gafter U (1994). Systemic distribution of 0,-microglobulin-derived amyloidosis in patients who undergo long-term hemodialy- sis: report of seven cases and review of the literature. Arch Path01 Lab Med 118,718-721 Hampl H. Lobeck H, Bartel-Schwarze S, Stein H, Eulitz M and Linke RP (1987). Clinical: morphologic, biochemical. and immunohistochemical aspects of dialysis-associated amyloi- dosis. Trans A m Soc Artlflntern Organs 33.250-259 Zhou H. Pfeifer U and Linke R (1991). Generalized amyloi- dosis from 0,-microglobulin, with caecal perforation after long- term haemodialysis. LFrchows Arcliiv A PatholAnat Histopathol
Fuchs A, Jagirdar J and Schwartz IS (1987). Beta 2- microglobulin amyloidosis (AB2M) in patients undergoing long-term hemodialysis. A new type of amyloid. Am J Clin
419.349-353
Pathol88.302-307
205
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
Choi HSH, Heller D. Picken MM, Sidhu GS and Kahn T (1 989). Infarction of intestine with massive amyloid deposi- tion in two patients on long-term hemodialysis. Gastroenter-
Campistol JM, Sole M, Mufloz-Gomez J. Lopez-Pedret J and Revert L (1990). Systemic involvement of dialysis-amy- loidosis. Am JNephrol 10,389-396 Maher ER, Hamilton Dutoit S, Baillod FL4, Sweny P and Moorhead JF (1 988). Gastrointestinal complications of di- alysis related amyloidosis. Br Med J297 , 265-266 Shinoda T, Komatsu M, Aizawa T, Shirota T, Yamada T, Ehara T and Mizukami E (1989). Intestinal pseudo-obstruc- tion due to dialysis amyloidosis. Clin Nephrol32, 284-289 Sethi D, Hutchison AJ, Cary NRB, Brown EA Jr. Curtis JR, Woodrow DF and Gower PE (1990). Macroglossia and amyloidoma of the buttock: evidence of systemic involve- ment in dialysis amyloid. Nephron 55. 3 12-3 15 Guccion JG, Redman RS and Winne CE (1989). Hemodialy- sis-associated amyloidosis presenting as lingual nodules. Oral Surg Oral Med Oral Pathol68, 6 18-623 Tada S, Iida M, Yao T, Kitamoto T, Yao T and Fujishima M (1 993). Intestinal pseudo-obstruction in patients with amy- loidosis: clinicopathologic differences between chemical types of amyloid protein. Gut 34, 1412-1417 Saguem MH and Widgren S (1990). Amylo’idose digestive avec ulctre ischemique du colon chez un hemodialyse chronique.AnnPathol10, 187-190 Picken MM and Shen S ( 1 994). P,-microglobulin amyloido- sis: illustrative cases. Ultrastruct Pathology 18, 133- 136 Wu TH, Tsai CY, Chiang SS, Wang JS, Huang TP and Yu CL (1994). Dialysis-related amyloidosis and acquired renal cys- tic disease with renal cell carcinoma in uremia [letter]. Neph- ron 67,129 Borczuk A, Mannion C, Dickson D and Alt E (1995). Intes- tinal pseudo-obstruction and ischemia secondary to both 0,- microglobulin and serum A amyloid deposition. Mod Pathol
Takahashi S, Morita T, Koda Y, Murayama H and Hirasawa Y (1988). Gastrointestinal involvement of dialysis-related amy- loidosis. Clin Nephrof 30, 168- 171 IkegayaN, Kobayashi S, Hishida A, Kaneko E, Furuhashi M and Maruyama Y (1995). Colonic dilitation due to dialysis- related amyloidosis. Am JKidney Dis 25, 807-809 Tiffet 0, Poulard G, Versini P, Baccot S, Boucheron S and Cuilleret J (1996). Pseudo-obstruction colique par amylose digestive chez I’hemodialysk chronique. A propos d’un cas. Ann Chir 50,279-282 Morita T, Suzuki M, Kamimura A and Hirasawa Y (1 985). Amyloidosis of a possible new type in patients receiving long-term hemodialysis. Arch Pathol Lab Med 109> 1029- 1032 Shirahama T, Skinner M, Cohen AS, Gejyo F, Arakawa M. Suzuki M and Hirasawa Y (1985). Histochemical and immu- nohistochemical characterization of amyloid associated with chronic hemodialysis as P,-microglobulin. Lab Invest 53,705- 709 Gejyo F, Odani S, Yamada T, Honma N, Saito H, Suzuki Y, Nakagawa Y, Kobayashi H, Maruyama Y, Hirasawa Y. Suzuki M and Arakawa M (1986). P,-microglobulin: a new form of
010gy96,230-234
8,577-582
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
amyloid protein associated with chronic hemodialysis. Kid- ney Int 30,385-390 Ullian ME, Hammond WS, Alfrey AC, Schultz A and Molitoris BA ( 1 989). Beta-2-microglobulin-associated amy- loidosis in chronic hemodialysis patients with carpal tunnel syndrome. Medicine (Baltimore) 68, 107-1 15 Noel LH, Zingraff J. Bardin T, Atienza C. Kuntz D and Driieke T (1987). Tissue distribution of dialysis amyloidosis. Clin Nephrol27,175- 178 Ogawa H, Saito A, Hirabayashi N and Hara K (1987). Amy- loid deposition in systemic organs in long-term hernodialysis patients. Clin Nephrol28, 199-204 Athanasou NA, Chaplin AJ and Oliver DO (1990). Subcuta- neous deposition of beta,-microglobulin amyloid in a long- term haemodialysis patient. Nephrol Dial Transplant 5:
Mazanec K, McClure J. Bartley CJ, Newbould MJ and Ackrill P (1992). Systemic amyloidosis of P, microglobulin type. J Clin Pathol 45,832-833 Lutz AE, Schneider U, Ehlerding G, Frenzel H, Koch KM and Kuhn K (1995). Right ventricular cardiac failure and pul- monary hypertension in a long-term dialysis patient - un- usual presentation of visceral b,-microglobulin amyloidosis. Nephrol Dial Transplant 10,555-558 Gorevic PD, Casey TT, Stone WJ, DiRaimondo CR, Prelli FC and Frangione B (1985). Beta-2 microglobulin is an amyloidogenic protein in man. J Clin Invest 76,2425-2429 Campistol JM, Cases A, Torras A,Soler M, Mufiomez J, Montoliu J, Lopez-Pedret J and Revert L (1987). Visceral involvement of dialysis amyloidosis. Am J Nephrol 7, 390- 393 Lipner HI, Minkowitz S, Neiderman G, Louis BM and Hoch BS (1995). Dialysis-related amyloidosis manifested as masses in the buttocks. South Med J 8 8 , 876-878 Buchholz N-P, Moch H, Gasser TC, Linke RP, Thiel GT and Mihatsch MJ (1995). Ureteral amyloid deposits of B2- microglobulin origin in both kidney receipients of 1 donor. J Urol153,399-401 Ozasa H, Suzuki T, Takahashi K and Ota K (1989). Protein components of amyloid-like kidney stones of chronic hemo- dialysis patients. Nephron 53, 257-260 Theaker JM, Raine AEG, Rainey AJ, Heryet A, Clark A and Oliver DO (1987). Systemic amyloidosis of P,-microglobulin type: a complication of long term haemodialysis. JClin Pathol
Ono S, Momose T, Arai T, Kaneko M, Koide K and Nagao K ( 1 994). Peripheral neuropathy associated with dialysis amy- loidosis [letter]. J Neurol Neurosurg Psychiatry 57, 1137- I138 Taira M, Ohashi M, Ito A and Masuko K (1988). Amyloid in the skin of patients undergoing long-term hemodialysis. In Isobe T, Araki S, Uchino F, Kit0 S and Tubura E (eds.) Amy- loid and Amyloidosis, pp. 727-730. (New York: Plenum Press) Sat0 KC, Kumakiri M, Koizumi H, Ando M, Ohkawara A, Fujioka Y and Kon T (1993). Lichenoid skin lesions as a sign of P,-microglobulin-induced amyloidosis in a long-term haemodialysis patient. Br J Dermatol 128,686-689 FIoege J, Brandis A, Nonnast-Daniel B, Westhoff-Bleck M, Tiedow G, Linke RP and Koch KM (1989). Subcutaneous
878-881
40,1247-1251
206
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997)
87
88
89
90
91
92
93
94
95
96
97
98
99
aniyloid-tumor of beta-2-microglobulin origin in a long-term hemodialysis patient. Nephron 53, 73-75 Fernandez-Alonso J , Rios-Camacho C, Valenzuela-Castafio A and Rocha-Castilla JL (1993). Pseudotumoral amyloidosis of (32-microglobulin origin in the buttock of a patient receiv- ing long term haemodialysis. JClin Pathol 46.77 1-772 Tom Y. Htwe M, Chandra R and Smith-Behn DJ (1994). Bilateral PI-microglobulin amyloidomas of the buttocks in a long-term hemodialysis patient. Arch Pathol Lab Med 118. 65 1-653 Brancaccio D. Gallieni M, Padovese P. Anelli A. Coggi G and Uslenghi C ( I 988). Dialysis amyloidosis with passive politeal deposition of (32-microglobulin amyloid [letter]. Lancet 2. 802 Feese W. Hopkovitz A and Lifschitz MD (1988). B,- microglobulin and associated amyloidosis presenting as bilat- eral popliteal tumors. Am JKidney Dis 12, 323-325 Gaucher A, Kessler M, Netter P. Azoulay E, Pere P and Mur JM (1988). Dialysis arthropathy: the effect of age [letter]. J Rheum 15,1880-1881 van Ypersele de Strihou C. Jadoul M, Malghem J, Maldague B, Jamart J and the Working Party on Dialysis Amyloidosis ( 1991). Effect of dialysis membrane and patient's age on signs of dialysis-related amyloidosis. Kidney Int 39. 101 2-101 9 Baldrati I, Docci D, Tomidei G, Capponcini C, Neri L and Feletti C (1994). Age and dialysis-related amyloidosis [let- ter]. Nephron 67, 120 Zingraff J, Noel LH, Bardin T, Atienza C, Zins B. Drueke TB and Kuntz D (1990). P,-microglobulin amyloidosis in chronic renal failure [letter]. NEnglJMed323. 1070-1071 bloriniere P, Marie A, el Esper N, Fardellone P, Deramond H, Remond A, Sebert J-L and Fournier A (1991). Destructive spondyloarthropathy with (3,-microglobulin amyloid depos- its in a uremic patient before chronic hemodialysis. h'ephron
Kessler M, Hestin D, Aymard B, Mainard D, Claudon M, Netter P and Gaucher A ( 1 995). Carpal-tunnel syndrome with P2-microglobulin amyloid deposits and erosive arthr- opathy of the wrist and spine in a uraemic patient before chronic haemodialysis [letter]. Nephrol Dial Transplant 10.
Brownlee M (1995). Advanced protein glycosylation in dia- betes and aging. Annu Rev Med 46.223-234 United States Renal Data System (1995). USRDS 1995 An- nual Data Report, p. 67. (Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases) Lehnert H, Jacob C, Marzoll I, Schmidt-Gayk H, Stein G. Ritz E and the Diabetes Amyloid Study Group ( 1 996). Preva- lence of dialysis-related amyloidosis i n diabetic patients.
59,654-657
298-299
.Vephrol Dial Transplant 11; 2004-2007 100 Mufioz-Gomez J; Gomez-PCrez R. Sole-Arques M and
Llopart-Buisan E (1 987). Synovial fluid examination for the diagnosis of synovial amyloidosis in patients with chronic renal failure undergoing haemodialysis. ilnn Rhetrm Dis 46.
101 Cobby MJ, Adler RS. Swartz R and Martel W (1991). Dialy- sis-related amyloid arthropathy: MR findings in four patients.
324-326
.dJR 157,1023-1027
102 Claudon M. Regent D. Gaucher A. Kessler M, Fabre J-L. Grignon B and Netter P (1990). MR patterns of dialysis arthropathy. J Comput Assist Tomogr 14, 968-974
103 Rafto SE, Dalinka ME. Schiebler ML. Burk DL Jr and Kricun ML (1988). Spondyloarthropathy of the cervical spine in long-term hemodialysis. Radiology 166.201-204
104 Sethi D. Naunton Morgan TC, B r o w EA. Jewkes RF and Cower PE (1990). Technetium-99-labelled methylene diphosphonate uptake scans in patients with dialysis arthr- opathy. Nephron 54. 202-207
105 Grateau G, Zingraff J. Fauchet M. Mundler 0. Raymond P. Berthelot JM, Bardin T, Kuntz I> and Drueke T (1988). Ra- dionuclide exploration of dialysis amyloidosis: preliminary experience. Am JKidney Dis 11.23 1-237
106 Flipo R-MI Le Loet X. Siame J-L, Benoit J, Goutallier D, Duquesnoy B and Bardin T (1995). Destructive arthropathy of the hands in chronic hemodialysis patients: a report of seven cases with pathological documentation. Rev Rhum [Engl
107 Hawkins PN (1994). Studies with radiolabelled serum amy- loid P component provide evidence for turnover and regres- sion of amyloid deposits in vivo. Clin Sci 87, 289-295
108 Nelson SR, Hawkins PN, Richardson S. Lavender JP, Sethi D. Cower PE, Pugh CW, Winearls CG. Oliver DO and Pepys MB (1991). Imaging of haemodialysis-associated amyloido- sis with 'Z31-serum amyloid P component. Lancet 338. 335- 339
109 Floege J, Nonnast-Daniel B, Gielow P. Brandis A. Spindler E, Hundeshagen H, Koch KM and Shaldon S (1989). Specific imaging of dialysis-related amyloid deposits using I3'I-beta- 2-microglobulin. Nephron 51.444-447
1 10 Chertow GM, Trimbur T. Karlson EW. Lazarus JM and Kay J ( 1 996). Performance characteristics of a dialysis-related amyloidosis questionnaire. J A m Soc A'ephrol7. 1235-1240
11 1 Gertz MA, Li C-Y. ShirahamaT and Kyle RA (1988). Utility of subcutaneous fat aspiration for the diagnosis of systemic amyloidosis (immunoglobulin light chain). Arch Intern .Wed
I 12 Duston MA, Skinner M. Meenan RF and Cohen AS (1989). Sensitivity, specificity, and predictive value of abdominal fat aspiration for the diagnosis of amyloidosis. Arthritis Rheum
113 Varga J, Idelson BA, Felson D. Skinner M and Cohen AS (1987). Lack of amyloid in abdominal fat aspirates from pa- tients undergoing long-term hemodialysis. Arch Intern Med
1 14 Berggird I and Beam AG (1968). Isolation and properties of a low molecular weight (3,-globulin occurring in human bio- logical fluids. JBiol Chem 243.4095-4103
1 15 Peterson PA. Cunningham BA, Berggard I and Edelman GM (1972). (3, microglobulin - a free immunoglobulin domain. Proch'atlilcadSci LEA 69, 1697-1701
116 Smithies 0 and Poulik MD (1972). Initiation of protein syn- thesis at an unusual position in an immunoglobulin gene? Science 175.187- 189
117 Karlsson FA (1974). Physical-chemical properties of (3,- microglobulin. lmrnunochernistry 11. 11 1-1 14
118 Grey HM. Kubo RT. Colon SM, Poulik MD. Cresswell P. Springer T. Turner M and Strominger JL (1973). The small
Ed] 62.24 1-247
148,929-933
32,82-85
147,1455-1457
207
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

subunit of HL-A antigens is p2 microglobulin. JOrp Med 138, 1608-1 612
1 19 Karlsson FA, Wibell L and Evrin PE (1980). 02-microglobulin in clinical medicine. Scand JClin Lab lnvest 40 (Suppl), 27- 37
120 Katzmann JA, Greipp PR, O’Fallon WM and Kyle RA (1 986). Serum microglo globulin. Mayo Clin Proc 61,752-753
121 Vincent C, Revillard JP, Galland M and Traeger J (1978). Serum P,-microglobulin in hemodialized patients. Nephron
122 Gorevic PD, Munoz PC, Casey TT. DiRaimondo CR, Stone WJ, Prelli FC, Rodrigues MM, Poulik MD and Frangione B ( 1986). Polymerization of intact microglo globulin in tissues causes amyloidosis in patients on chronic hemodialysis. Proc Natl Acad Sci USA 83,7908-79 12
123 Nishi S, Ogino S, Maruyama Y, Honma N, Gejyo F, Morita T and Arakawa M (1990). Electron microscopic and immunhistochemical study of beta-2-microglobulin-related amyloidosis. Nephron 56,357-363
124 Ogawa H, Saito A, Oda 0, Nakajima M and Chung TG (1 988). Detection of novel 0,-microglobulin in the serum of hemodi- alysis patients and its amyloidogenic predisposition. Clin Nephrol30,158-163
125 Odani H, Oyama R, Titani K, Ogawa H and Saito A (1990). Purification and complete amino acid sequence of novel 0,- microglobulin. Biochem Siophys Res Commun 168, 1223-1229
126 Argiles A, Garcia-Garcia M: Derancourt J, Mourad G and Demaille JG (1995). Beta2 microglobulin isoforms in healthy individuals and in amyloid deposits. Kidney Int 48, 1397- 1405
127 Linke RP, Hampl H, Lobeck H. Ritz E, Bommer J, Waldherr R and Eulitz M (1989). Lysine-specific cleavage of p,- microglobulin in amyloid deposits associated with hemodi- alysis. Kidney Int 36, 675-681
128 Stone PJ, Campistol JM, Abraham CR, Rodgers OG, Shirahama T and Skinner M (1993). Neutrophil proteases associated with amyloid fibrils. Biochem Siophys Res Cornmun
129 Ohashi K, Kawai R, HaraM, OkadaY, Tachibana S and Ogura Y (1996). Increased matrix metalloproteinases as possible cause of osseoarticular tissue destruction in long-term haemodialysis and p,-microglobulin amyloidosis. Krchows Arch 428,37-46
130 Campistol JM, Shirahama T, Abraham CR, Rodgers OG, Sole M. Cohen AS and Skinner M (1 992). Demonstration ofplasma proteinase inhibitors in b,-microglobulin amyloid deposits. Kidney Int 42,9 15-923
13 1 Li JJ and McAdam KPWJ (1984). Human amyloid P compo- nent: an elastase inhibitor. Scand J Immunol 20.2 19-226
I32 Argiles A, Mourad G, Axelrud-Cavadore C, Watrin A, Mion C and Cavadore JC (1989). High-molecular mass proteins in haemodialysis-associated amyloidosis. C h Sci 73,547-552
133 Alizadeh-Khiavi K, Normand J, Chronopoulos S. Ali A and Ali-Khan Z (1992). Amyloid enhancing factor activity is as- sociated with ubiquitin. L’irchows Archiv A Pathol Anat 420.
134 Okada M, Miyazaki S and Hirasawa Y (1993). Increase in plasma concentration of ubiquitin in dialysis patients: pos- sible involvement in p, microglobulin amyloidosis. Clin Chim
21,260-268
197, 130-136
139-148
Acta 220, 135-144 135 Aruga E, Ozasa H, Teraoka S and Ota K (1993). Macromol-
ecules that are colocalized with deposits of p,-microglobulin in hemodialysis-associated amyloidosis. Lnb Invesr 69,223- 230
136 Brancaccio D, Ghiggeri GM, Carberi A, Anelli A, Ginevri F, Loggi G and Gusman R (1991). Purification and partial char- acterization of a new 85 Kda amyloidosis-related protein in chronic hemodialysis. Biochem Bioph,w Res Commun 176.
137 Brancaccio D, Ghiggeri GM, Braidotti P, Garberi A. Gallieni M, Bellotti V, Zoni U. Gusmano Rand Coggi G (1 995). Depo- sition of kappa and lambda light chains in amyloid filaments of dialysis-related amyloidosis. J Am Soc Nephrol 6, 1262- 1270
138 Takahashi M, Hoshii Y. Kawano H, Gondo T, Ishihara T and Isobe T (1996). Ultrastructural evidence for colocalization of k light chain- and (32-microglobulin-derived amyloids using double labelling immunogold electron microscopy. L’irchows Arch 429,383-388
139 Argiles A, Mourad G7 Axelrud-Cavadore C, Derancourt J. Jauregui Adell J , Mion C and Cavadore JC (1987). Haemodialysis-associated m y loidosis: P,-microglobulin alone or associated with globin chains? Clin Sci 73,5 15-518
140 Ohishi H, Skinner M, Sato-Araki N, Okuyama T, Gejyo F. Kimura A, Cohen AS and Schmid K ( 1990). Glycosaminogly- cans of the hemodialysis-associated carpal synovial amyloid and of amyloid-rich tissues and fibrils of heart, liver. and spleen. CIin Chem 36. 88-9 1
141 Ohashi K, HaraM. YanagishitaM, Kawai R. TachibanaS and Ogura Y ( 1995). Proteoglycans in haemodialysis-related amy- loidosis. C’irchows Arch 427,49-59
142 Kawai R; Oohashi K. Hara M, Ogura Y, Honda K. Nihei H and Mimura N (1992). lnframmatory [sic] cell infiltration around beta 2-microglobulin amyloid deposition: histologic comparison of with AA or AL amyloidosis. Nippon Jinzo Gakkai Shi 34,683-691
143 Inoue H, Saito I, Nakazawa R, Mukaida N: Matsushima K. Azuma N, Suzuki M and Miyasaka N (1 995). Expression of inflammatory cytokines and adhesion molecules in haemodialysis-associated amyloidosis. Nephrol Dial Trans- plant 10,2077-2082
144 Argiles A, Mourad G. Kerr PG, Garcia M, Collins B and Demaille JG (1994). Cells surrounding haemodialysis-associ- ated amyloid deposits are mainly macrophages. Nephrol Dial Transplant 9,662-667
145 Sol6 M, Mufioz-Gomez J and Campistol J (1990). Role of amyloid in dialysis-related arthropathies: a morphological analysis of 23 cases. l7rchows Archiv A Pathol Anat 417,523- 528
146 Kataoka H? Gejyo F. Yamada S. Kunimoto T and Arakawa M ( 1 986). Inhibitory effects of J3,-microglobulin on in vitro cal- cification of osteoblastic cells. Biochem Biophys Res Commun
147 Connors LH, Shirahama T, Skinner M, Fenves A and Cohen AS (1985). In vitro formation of amyloid fibrils from intact beta 2-microglobulin. Biochem Biophvs Res Commun 131.
148 Sethi D and Gower PE (1986). Synovial fluid ~2-microglobulin
1037- 1043
141.360-366
1063-1068
208
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997)
levels in dialysis arthropathy [letter]. N Engl J Med 315. 14 19-1420
149 Ge.jyo F, HommaN, Suzuki Y and ArakawaM (1986). Serum levels of O,-microglobulin as a new form of amyloid protein in patients undergoing long-term hemodialysis [letter]. NEnglJ Med314, 585-586
I50 Benzakour M. Charmes JP, Vincent D, Cogny van Weydevelt F. Lagarde CI Rince M and Leroux-Robert C (1987). Amylose 02m des dialyses: predisposition des sujets figes [letter]. Presse ,\fed 16. 133 1
15 1 Chanard J, Bindi P, Lavaud S, Toupance 0, Maheut H and Lacour F. Carpal tunnel syndrome and type of dialysis mem- brane. Br MedJ298, 867-868
152 Hakim RM. Fearon DT and Lazarus JM (1984). Biocompatibility of dialysis membranes: effect of chronic complement activation. Kidney Innt 26, 194-200
153 Jahn B, Betz M. Deppisch R, Janssen 0, Hansch GM and Ritz E (1991). Stimulation of beta,-microglobulin synthesis in lymphocytes after exposure to Cuprophan dialyzer mem- branes. Kidney Int 40,285-290
154 Zaoui PM, Stone WJ and Hakim RJ (1990). Effects of dialy- sis membranes on beta2-microglobulin production and cellular expression. Kidney Int 38,962-968
I55 Bergstrom J and Wehle B (1987). No change in corrected p,- microglobulin concentration after cuprophane haemodialysls [letter]. Lancet 1,628-629
156 Ballardie FW, Kerr DN, Tennent G and Pepys MB (1986). Haemodialysis versus CAPD: equal predisposition to amy- loidosis? [letter]. Lancet 1, 795-796
I57 Cornelis F, Bardin T, Faller B, Verger C. Allouache M, Raymond P, Rottembourg J, Tourliere D, Benhamou C. Noel LH and Kuntz D ( 1 989). Rheumatic syndromes and &- microglobulin amyloidosis in patients receiving long-term peritoneal dialysis. Arthritis Rheum 32; 785-788
158 Monnier VM, Kohn RR and Cerami A (1984). Accelerated age-related browning of human collagen in diabetes mellitus. Proc Nut1 Acad Aci USA 81,583-587
159 Vlassara H, Bucala Rand Striker L (1 994). Pathogenic effects of advanced glycosylation: biochemical. biologic. and clinical implications for diabetes and aging. Lab Invest 70, 138-1 5 1
160 Hunt JV and Wolff S P (1991). Oxidative glycation and free radical production: a causal mechanism of diabetic complica- tions. Free Radic Res Commun 12-13 (Pt I ) . 1 1 5 - 123
161 Brownlee M, Cerami A and Vlassara H (1988). Advanced glycosylation end products in tissue and the biochemical ba- sis ofdiabetic complications. h’EnglJMed318. 1315-1321
162 Bucala R, Vlassara H and Cerami A (1992). Advanced glycosylation endproducts. In Harding JJ. James M and Crabbe C (eds.). Post-translational modification ofproteins. Yo1 2, pp. 53-79. (Boca Raton, FL: CRC Press)
I63 hilortensen HB and Christophersen C (1 983). Glucosylation of haemoglobin a in red blood cells studied in vitro: kinetics of the formation and dissociation ofhaemoglobin A,c. Clin Chim Acta 134, 3 17-326
164 Shin DB, Hayase F and Kato H (1988). Polymerization of proteins caused by reaction with sugars and the formation of 3-deoxyglucosone under physiological conditions. Agric Biol Chem 52, 1451-3458
I65 Higgins PJ and Bunn HF (1981). Kinetic analysis ofthe non-
enzymatic glycosylation of hemoglobin. J Biol Chem 256.
166 Niwa T. Takeda N, Yoshizumi H. Tatematsu A. Ohara M. Tomiyama S and Niimura K (1993). Presence of 3- deoxyglucosone, a potent protein crosslinking intermediate of Maillard reaction, in diabetic serum. Biochem Bioplzys Res Commun 196,837-843
167 Odetti P. Fogarty J. Sell DR and Monnier VM ( 1 992). Chro- matographic quantitation of plasma and erythrocyte pentosidine in diabetic and uremic subjects. Diabetes41, 153- I59
168 Trivelli LA, Ranney HM and Lai H-T (1971). Hemoglobin components in patients with diabetes mellitus. N Engl JA4ed 284,353-357
169 Araki N, Ueno N, Chakrabarti B. Morino Y and Horiuchi S ( 1 992). Immunochemical evidence for the presence of ad- vanced glycation end products in human lens proteins and its positive correlation with aging. JBiol Chem 267. 102 1 1 - I02 14
170 Vitek MP, Bhattacharya K, Glendening JM, Stopa E, Vlassara H. Bucala R, Manogue K and Cerami A (1994). Advanced glycation end products contribute to amyloidosis in Alzheimer disease. Proc Natl AcadSci USA 91,4766-4770
171 Makita Z. Bucala R, Rayfield EJ. Friedman EA. Kaufman AM. Korbet SM. Barth RH. Winston JA. Fuh H. Manogue KR, Cerami A and Vlassara H. Reactive glycosylation endproducts in diabetic uraemia and treatment of renal failure. Lancet 343, 15 19- 1522
172 Niwa T. Katsuzaki T, Momoi T. Miyazaki T, Ogawa H. Saito A. Miyazaki S, Maeda K. Taternichi N and Takei Y ( 1996). Modification of f3,m with advanced glycation end products as observed in dialysis-related amyloidosis by 3-DG accumu- lating in uremic serum. Kidneylnt49, 861-867
173 Tan SY, Irish A, Winearls CG. Brow,n EA, Gower PE, Clutterback EJ, Madhoo S , Lavender JP. Pepys MB and Hawkins PN (1996). Long term effect of renal transplanta- tion on dialysis-related amyloid deposits and symptomatol- ogy. Kidney Int 50,282-289
174 Neeper M, Schmidt AM, Brett J. Yan SD, Wang F. Pan Y-CE. Elliston K. Stern D and Shaw A (1992). Cloning and expres- sion of a cell surface receptor for advanced glycosylation end products of proteins. J Biol Chem 267, 14998- 15004
175 Schmidt A-M. Yan SD. Brett J. Mora R. Nowygrod R and Stern D (1993). Regulation ofhuman mononuclear phagocyte migration by cell surface-binding proteins for advanced glycation end products. JCl in Invest 92, 2 155-2 168
176 Schmidt AM. Mora R, Cao R, Yan SD. Brett J. Ramakrishnan R. Tsang TC. Simionescu M and Stern D (1994). The endot- helial cell binding site for advanced glycation end products consists of a complex: an integral membrane protein and a lactoferrin-like polypeptide. J Biol Chem 269.9882-9888
177 Yan SD. Chen X, Schmidt A-M. Brett J. Godman G. Zou Y- S. Scott CW. Caputo C. Frappier T. Smith MA. Perry G, Yen S-H and Stern D (1994). Glycated tau protein in Alzheimer‘s disease: a mechanism for induction of oxidant stress. Proc IvatldcadSci L:SA 91,7787-7791
178 Yan SD. Yan SF. Chen X, Fu J , Chen M, Kuppusamy P. Smith MA. Perry G. Godman GC. Nawroth P. Zweier JL and Stern D ( 1 995). Nonenzymatically glycated tau in Alzheimer’s disease induces neuronal oxidant stress resulting in cytokine
5204-5208
209
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

gene expression and release of amyloid P-peptide. Nature Medicine 1,693-698
179 Vlassara H, Brownlee M, Manogue KR, Dinarello CA and Pasagian A (1 988). CachectidTNF and IL-I induced by glu- cose-modified proteins: role in normal tissue remodeling. Sci- ence 240.1546- 1548
180 Morohoshi M, Fujisawa K. Uchimura I and Numano F (1 995). The effect of glucose and advanced glycosylation end prod- ucts on IL-6 production by human monocytes. Ann NY Acad Sci 748,562-570
181
182
183
I84
185
186
187
188
189
Miyata T, Taneda S, Kawai R, Ueda 1’. Horiuchi S, Hara M, Maeda K and Monnier VM (1996). Identification of pentosidine as a native structure for advanced glycation end products in (3,-microglobulin-containing amyloid fibrils in patients with dialysis-related amyloidosis. Proc Natl Acad Sci USA 93,2353-2358 Niwa T, Sato M, Katsuzaki T, Tomoo T, Miyazaki T, Tatemichi N, Takei Y and Kondo T (1 996). Amyloid in B,- microglobulin is modified with W-(carboxymethy1)lysine in dialysis-related amyloidosis. Kidney Int 50, 1303- 1309 Niwa T, Katsuzaki T, Miyazaki S, Momoi T, Akiba T, Miyazaki T, Nokura K. Hayase F, Tatemichi N and Takei Y (1 997). Amyloid !3,-microglobulin is modified with imidazolone, a novel advanced glycation end product, in di- alysis-related amyloidosis. Kidney Int 51, 187-194 Miyata T, Inagi R, Wada Y, Ueda Y, lida Y, Takahashi M, Taniguchi N and Maeda K (1994). Glycation of human !3,- microglobulin in patients with hemodialysis-associated amy- loidosis: identification of the glycated sites. Biochemistry 33. 1221 5-12221 Hou FF, Chertow GM, Kay J , Boyce J , Lazarus JM, Braatz JA and Owen WF Jr (1997). Interaction between p2- microglobulin and advanced glycation end products in the development of dialysis-related amyloidosis. Kidney Int 51, 15 14-1 5 19 Homma N, Gejyo F. Isemura M and Arakawa M (1 989). Collagen-binding affinity of beta-2-microglobulin, a preprotein of hemodialysis-associated amyloidosis. Nephron 53, 37-40 Miyata T. Inagi R, Iida Y. Sato M, Yamada N, Oda 0. Maeda K and Seo H (1994). Involvement of p,-microglobulin modi- fied with advanced glycation end products in the pathogen- esis of hemodialysis-associated amyloidosis: induction of human monocyte chemotaxis and macrophage secretion of tumor necrosis factor-a and interleukin- 1. J Clin Invest 93,
Miyata T, Hori 0. Zhang JH, Yan SD. Ferran L, Iida Y and Schmidt AM (1996). The receptor for advanced glycation end products (RAGE) is a central mediator of the interaction of AGE-P,-microglobulin with human mononuclear phago- cytes via an oxidant-sensitive pathway: implications for the pathogenesis of dialysis-related amyloidosis. J Clin lnvest
Herbelin A. Nguyen AT, Zingraff J, Ureiia P and Descamps- Latscha B (1990). Influence of uremia and hemodialysis on circulating interleukin-1 and tumor necrosis factor a. Kidney Int 37, 1 16- 125
52 1-528
98, 1088- 1094
190 Herbelin A, Ureiia P, Nguyen AT, Zingraff J and Descamps- Latscha B ( 1 991). Elevated circulating levels of interleukin-6 in patients with chronic renal failure. Kidney Int 39,954-960
191
192
193
194
195
196
197
198
199
200
20 1
202
203
204
205
206
Iida Y. Miyata T. Inagi R, Sugiyama S and Maeda K (1994). p,-microglobulin modified with advanced glycation end prod- ucts induces interleukin-6 from human macrophages: role in the pathogenesis of hemodialysis-associated amyloidosis. Biochem Biophys Res Comrnun 201,235-1241 Miyata T, Iida Y, Ueda Y, Shinzato T, Seo H, Monnier VM. Maeda K and Wada Y. Monocyte/macrophage response to p,-microglobulin modified with advanced glycation end prod- ucts. Kidney Int 49, 538-550 Smith MA, Taneda S, Richey PL, Miyata S, Yan SD, Stem D. Sayre LM. Monnier VM and Perry G (1994). Advanced Maillard reaction end products are associated with Alzheimer disease pathology. Proc NatlAcadSci USA 91. 5710-5714 Yan SD, Chen X, Fu J. Chen M, Zhu H, Roher A, Slattery T. Zhao L, Nagashima M, Morser J, Migheli A, Nawroth P, Stern D and Schmidt AM (1 996). RAGE and amyloid-P pep- tide neurotoxicity in Alzheimer’s disease. Nature 382, 685- 69 1 Henderson LW, Koch KM, Dinarello CA and Shaldon S (1 983). Hemodialysis hypotension: the interleukin hypoth- esis. BloodPurifl, 3-8 Bingel M, Lonnemann G, Koch KM, Dinarello CA and Shaldon S (1987). Enhancement of in-vitro human interleukin- 1 production by sodium acetate. Lancet I , 14-1 6 Lonnemann G (1990). The role of contaminated dialysate in hemodialysis-associated cytokine production. Contrib Nephrol86, 121-127 Abel G and Czop JK ( 1 992). Stimulation of human monocyte P-glucan receptors by glucan particles induces production of TNF-a and IL-I p. Int JImmunopharmacoll4. 1363-1373 Craddock PR, Fehr J, Dalmasso AP, Brigham KL and Jacob HS (1 977). Hemodialysis leukopenia: pulmonary vascular leukostasis resulting from complement activation by dialyser cellophane membranes. J Clin Invest 59,879-888 Cavaillon JM, Fitting C and Haeffner-Cavaillon N ( I 990). Recombinant C5a enhances interleukin 1 and tumor necrosis factor release by lipopolysaccharide-stimulated monocytes and macrophages. Eur JImmunol20, 253-257 Miyasaka N, Sato K. Kitano Y, Higaki M, Nishioka K and Ohta K (1992). Aberrant cytokine production from tenosynovium in dialysis associated amyloidosis. Ann Rheum Dis 51, 797-802 Knudsen PJ, Shaldon S. Floege J and Koch M. Hemodialysis- related induction of P,-microglobulin synthesis and release by mononuclear phagocytes. Int J ArtifOrgans 13.73-76 Collins T, Lapierre LA, Fiers W, Strominger JL and Pober JS (1 986). Recombinant human tumor necrosis factor increases mRNA levels and surface expression of HLA-A, B antigens in vascular endothelial cells and dermal fibroblasts in vitro. Proc Natl Acad Sci USA 83.446-450 Lovett D, Kozan B, Hadam M, Resch K and Gemsa D (1986). Macrophage cytotoxicity: interleukin 1 as a mediator of tu- mor cytostasis. J Immunol 136, 340-347 Migita K, Eguchi K, Otsubo T. Kawakami A, Nakao H, Ueki Y, Shimomura C, Kurata A, Fukuda T. Matsunaga M, Ishikawa N, Ito K and Nagataki S (1990). Cytokine regulation of HLA on thyroid epithelial cells. Clin Exp Immunol82, 548-552 Homma T, Tsujinaka T, Kido Y. Yasuda T, Murata A and Mori T (1992). Secretion of beta-2-microglobulin from hu-
210
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.

Amyloid: Int. J. Exp. Clin. Invest. 4, 187-211 (1997)
man hepatoblastoma and hepatoma cells on stimulation with interleukin-6. Eur Surg Res 24,204-2 10
207 Shaldon S. Koch KM. Dinarello CA, Colton CK. Knudsen PJ. Floege J and Granolleras C (1987). oz-microglobulin and haemodialysis [letter]. Lancet 1,925-926
208 Centrella M. McCarthy TL and Canalis E (1989). @,- microglobulin enhances insulin-like growth factor 1 receptor levels and synthesis in bone cell cultures. J Biol Chem 264.
209 Canalis E, McCarthy T and Centrella M (1987). A bone- derived growth factor isolated from rat calvariae is beta, microglobulin. Endocrinology 121, 1198-l200
21 0 Evans DB, Thavarajah M and Kanis JA ( I 991). Inimunoreac- tivity and proliferative actions of 0, microglobulin on human bone-derived cells in vitro. Biochem Biuphys Res Comtnrrn
2 I 1 Kataoka H, Gejyo F, Yamada S, Kunitomo T and Arakawa M ( 1 986). Inhibitory effects of p,-microglobulin on in vitro cal- cification of osteoblastic cells. Biochem Biophys Res Commzrn
212 Moe SM and Sprague SM (1992). !3,-microglobulin induces calcium efflux from cultured neonatal mouse calvariae. A m J Physiol263 (Renal Fluid Electrolyte Physiol32), F540-F545
213 Moe SM, Hack BK. Curnmings SA and Sprague SM (1995). Role of 1L- 1 I!, and prostaglandins in !3,-microglobulin-induced bone mineral dissolution. Kidney Int 47.587-591
2 I4 Miyata T and Sprague SM (1 996). Advanced glycation of !3,- microglobulin in the pathogenesis of bone lesions in dialysis- associated amyloidosis. Nephrol Dial Transplant I1 [Suppl
2 I5 Brinckerhoff CE. Mitchell TI. Karmilowicz ML,. Kluve- Beckerman B and Benson MD (1988). Autocrine induction ofcollagenase by serum arnyloid A-like and P,-rnicroglobulin- like proteins. Science 243,655-657
2 I6 Dayer JM. Beutler B and Cerami A ( 1 985). Cachectin/tumor necrosis factor stimulates collagenase and prostaglandin EL production by human synovial cells and dermal fibroblasts .I ExpMed162.2163-2168
217 Bardin T (1994). Low dose prednisone in dialysis-related amyloid arthropathy. Rev Rhum [Engl Ed] 61 (9 Suppl).
2 I8 Okutsu I, Hanianaka I. Ninomiya S. Takatori Y. Shimizu K and Ugawa Y (1993). Results of endoscopic management of carpal-tunnel syndrome in long-term haemodialysis versus idiopathic patients. 1Vephrol Dial Transplant 8. 1 110-1 114
2 19 Scheumann GFW. Holch M, Nerlich ML, Brandis A. Ostertag H and Tscherne H (1991). Pathological fractures and Iytic bone lesion of the femoral neck associated with D,- microglobulin amyloid deposition in long-term dialysis p i - tients. Arch Orthop Trauma Surg 110, 93-97
220 Lai KN. Chan KW. Siu DLS. Wong CC and Yeung D (1984). Pathologic hip fractures secondary to amyloidoma: case report and review of the literature. Am J M e d 77. 937-943
22 1 DiRaimondo CR. Casey TT, DiRaimondo CV and Stone WJ ( 1986). Pathologic fractures associated with idiopathic amy- loidosis of bone in chronic hemodialysis patients. ,\ephron
222 Naito M. Ogata K. Shiota E and Oyama M (1994). Amyloid bone cysts of the femoral neck: impending fractures treated
18268-18271
175,795-803
141.360-366
31.86-90
97s-100s
43.22-27
by curettage and bone grafting. J Bone Joint Surg [Br] 76-B, 922-925
223 DiRaimondo CR and Pollak VE (1989). P,-microglobulin ki- netics in maintenance hemodialysis: a comparison ofconven- tional and high-flux dialyszers and the effects of dialyzer reuse. Am J Kidney Dis 13,390-395
224 Edwards LC. Helderman JH. Hamm LL. Ludwin D. Gailiunas P J r and Hull AR (1983). Noninvasive monitoring of renal transplant function by analysis of beta,-rnicroglobulin. Kid- ne-v Int 23.767-770
225 Sethi D. Brown EA. Maini RN and Gower PE (1988). Renal transplantation for dialysis arthropathy [letter]. Lancet 2.
226 Jadoul M. Malghem J. Pirson Y, Maldague B and van Ypersele de Strihou C (1989). Effect of renal transplantation on the radiological signs of dialysis amyloid osteoarthropathy. CIin Yephrol32. 194- 197
227 Campistol JM, Ponz E, Mutioz-Gornez J. Oppenheimer F. Ricard MJ, Vilardell J and Andreu J (1992). Renal transplan- tation for dialysis amyloidosis. Transplant Proc 24. 1 18- 1 19
228 Bardin T. Lebail-Dame JL, Zingraff J. Laredo JD. Voisin MC. Kreis H and Kuntz D ( 1 995). Dialysis arthropathy: outcome after renal transplantation. Am J .Wed 99, 243-248
229 Mourad G and Argiles A (1996). Renal transplantation rc- lieves the symptoms but does not reverse P2-microglobulin amyloidosis. J Am Soc il’ephrol7.798-804
230 Kessler M. Aymard B and Pourel J (1994). Persistence of p,- microglobulin amyloid 10 years after renal transplantation [letter]. Nephrol Dial Transplant 9, 333-334
23 1 Edelstein D and Brownlee M (1992). Mechanistic studies of advanced glycosylation end product inhibition by aminoguanidine. Diabetes 41.26-29
232 Hammes HP. Martin S, Federlin K, Geisen K and Brownlee M (1991). Arninoguanidine treatment inhibits the develop- ment ofexperimental diabetic retinopathy. Proc #aatl.rlcadSci USA 88. 13555-1 1558
233 Itakura M. Yoshikawa H. Bannai C. Kato M, Kunika K. Kawkami Y. Yamaoka T and Yamashita K (1991). Aminoguanidine decreases urinary albumin and high-molecu- lar-weight proteins in diabetic rats. Life Sci 49; 889-897
234 Soulis-Liparota T, Cooper M. Papazoglou D. Clarke B and Jerums G (1991). Retardation by aminoguanidine ofdevelop- ment of albuminuria. rnesangial expansion. and tissue tluores- cence in streptozocin-induced diabetic rat. Diabetes 40.
235 Yagihashi S. Kamijo M, Baba M. Yagihashi N and Nagai K (1992). Effect ofaminoguanidine on functional and structural abnormalities in peripheral nerve of STZ-induced diabetic rats. Diabetes 41. 47-52
236 Brownlee M. Vlassara H. Kooney A. Ulrich P and Cerami A ( 1986). Aminoguanidine prevents diabetes-induced arterial \tall protein cross-linking. Science 232. 1629- 1632
237 Bucala R and Vlassara H (1995). Advanced glycosylation end products in diabetic renal and vascular disease. Am J Kidne)] Dls 26, 875-888
238 Foote EF, Look ZM. Giles P. Keane, WF and Halstenson. CE ( 1995). The pharmacokinetics ofaminoguanidine in end-stage renal disease patients on hemodialysis. Am J Kidney Dis 25. 420-425
448-449
1328-1334
21 1
Am
yloi
d D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Bat
h on
11/
02/1
4Fo
r pe
rson
al u
se o
nly.