





γλώσσες
Σελίδες
Νομικός


Μedical management of heart failure: Update 2014
Dr John T ParissisDr John T Parissis
Attikon University Hospital
Athens, Greece
Disclosures: Received honoraria as consultant or research grants by Orion-
Pharma, Servier, Pfizer

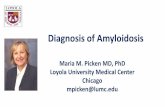
Evidence-Based Treatment for Heart Failure with Reduced LVEF
Control VolumeReduce Mortality
Sodium Restriction*
Diuretics*
β-Blocker
ivabradine
ACEI
or ARB
Aldosterone
Antagonist
Treat Residual Symptoms
Digoxin*
Treat Residual SymptomsCRT ±
an ICD*Hyd/ISDN*
*For select indicated patients.
ICD*
Treat Comorbidities
Aspirin*
Warfarin*
Statin*
Enhance Adherence
Education
Disease Management
Performance Improvement Systems18

ESC 2012

Hospitalization
free survival
1.0
0.9
0.8 High (100%)
Adherence to HF guidelines predicts HF
hospitalizations
0.7
0.6
0.5
0 20 60 100 120
Log rank test p = 0.002
Low (0-33%)
Moderate (50-67%)
days
40 80 140 160 180
Komajda M et al. Eur Heart J 2005.

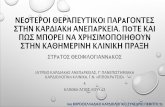
Heart Failure Guidelines and Clinical Practice
(Please mind the gap)

Overall, only 25% of patients are discharged from hospital receiving ACE/ARB + BB + diuretic oral combination therapy, suggesting poor compliance with guidelines (ALARM REGISTRY)
20%16%
31%16%
5%
Mexico
Brazil
Australia
Turkey
Oral heart failure medications on discharge
All patients receiving BB + ACE and/or ARB + DIUR
19%60%
25%20%
38%20%
0% 10% 20% 30% 40% 50% 60% 70%
Greece
UK
Spain
Italy
Germany
France
Sample =All discharged/surviving AHF patients, 4491
Follath F, Yilmaz B, Parissis J, et al. Intensive Care Med 2011 Sept;38(1):170-177

Maggioni A P et al. Eur J Heart Fail 2010;12:1076-1084

Impact of Discharge Use of Beta Blocker on Early Clinical Outcomes in Heart Failure
Survival Probability
1.00
0.95
0.90
0.85
P=0.0003
30 day Survival
P<0.01
*Only subset of patients with 60- to 90-day follow-up are included. Patients with beta-blocker contraindications are excluded.
Survival Probability
0.85
0.80
0.75
0.700 10 20 30 40 50 60 70 80 90 100 110 120 130
Patients at Risk
Beta-blocker 1,946 1,855 1,649 333 68
No Beta-blocker 362 337 304 60 7
Days After Hospital Discharge
Beta-Blocker No Beta-Blocker
Fonarow et al. J Am Coll Cardiol. 2008;52:190-199.27

ESC HF LONG TERM REGISTRY


Patient education and support reduces HF hospitalization rates and cost
Krumholz et al. J Am Coll Cardiol 2002;39:83–9

A Maisel JACC 2013

Primary Results of the HABIT Trial(Heart Failure Assessment With BNP in the Home)
Maisel et al. J Am Coll Cardiol 2013;61:1726–35

ESC guidelines 2012

Conventional Treatments of Acute Heart Failure
Diuretics
Reduce
fluid
Vasodilators
Decrease
preload
Inotropes
Augment
contrac-
Fonarow GC. Rev Cardiovasc Med. 2001;2(suppl 2):S7–S12.
fluid
volume
preload
and/or
afterload
contrac-
tility

Patients with EF<40%Whole cohort of ALARM
Impact of high vs low dose of diuretics on short term
mortality of AHF patients using propensity matched scores
A. Mebazaa and J. Parissis on behalf of ALARM investigators EJHF 2012

Role of Congestion and Its Interaction With Renal Function in Advanced HF
Metra M et al. Circ Heart Fail 2012

Short-term Survival by Treatment Among Patients Hospitalized with Acute Heart Failure: The Global ALARM-HF Registry Using Propensity Scoring Methods
0.2
0.3
0.4In-hospital mortality
Inotropes
0 5 10 15 20 25 30
0.0
0.1
0.2
Days
In-hospital mortality
Whole cohort
Diuretics
Vasodilators
Mebazaa A, Parissis J, Porcher R, et al. Intensive Care Med 2011 Feb;37(2):290-301

Dobutamine: cl IIa, Level evidence C
PDEIs: cl III, Level evidence B
Available inotropic agents
Dopamine: cl IIb, Level evidence C
Levosimendan: cl IIb,Level evidence C
for patients on beta-blocker
ESC Guidelines 2012.

Classical therapies are insufficient to protect peripheral organs
ESC HF pilot, ALARM-HF, ADHERE, SURVIVE demonstrated:
� Worsening of renal function (30-45%)
� Hepatic dysfunction (20-30%)
� Ongoing myocardial injury (Tn release) (30%)
� Hyponatremia, CNS abnormalities ( 12-20%)

Investigational pharmacotherapies for the management of ADHF
INOTROPES
- Myocin activators
- SERCA enhancers
and Na/K-ATPase
inhibitors
- Ryanodine receptor stabilizers
METABOLIC
MODULATORS
DeComa et al. JACC 2006;48:2397
MODULATORS
- CPT-1 inhibitors
DIURETICS
- Adenosine antagonists
- Vasopressin antagonists
- Natriuretic peptides (ularitide)
VASODILATORS
- Relaxin

The challenge of cardiac myocin activation
- Target the force
generating enzyme cardiac
myosin ATPase, accelerating
its activity.
- Increase fractional
shortening of cardiac shortening of cardiac
myocytes without
altering intracellular
calcium levels in
experimental models.
-An IV formulation of
CK1827452 is currently in
phase I clinical development.
Malic et al. AHA Scientific Sessions 2005 Dallas TX

HFSA 2006

Circ Heart Fail 2010;3:522-527

Istaroxime: a Na/K-ATPase inhibitor with positive lusitropic properties
Sabbah et al. Am J Cardiol 2007;99:41A
Adamson et al. J Cardiovasc Pharmacol 2003;42:169

Changes in hemodynamic and other measures in the HORIZON-HF trial, three dosages of IV istaroxime vs placebo
µg/kg/minParameter 0.5,
n=291.0, n=30
1.5, n=30
Placebo, n=31
PCWPa (mm Hg) -3.2b -3.3c -4.7d 0.0
Systolic BP (mm Hg) +4.9 +8.3b +15.6d +1.3
MAP (mm Hg) +2.2 +3.3 +7.5c +0.9
Gheorghiade M et al. J Am Coll Cardiol 2008; 51:2276-2285.
MAP (mm Hg) +2.2 +3.3 +7.5c +0.9
LVEDV (mL) +2.9 -6.4 -14.1b +3.9
QTc (ms) -25.7e -38.0e -49.2e -2.4
a. Primary end pointb. p<0.05c. p<0.01 d. p<0.001e. p=0.0001PCWP=pulmonary capillary wedge pressureMAP=mean arterial pressureLVEDV=left ventricular end-diastolic volume; QTc=corrected QT interval

Treatment of SR Ca2+ leak in HF with ryanodine receptor stabilizers
Masafumi Yano et al. Circulation. 2003;107:477-484

CURRENT VASOPRESSIN ANTAGONISTS
G. Filippatos and J. Parissis, J Card Fail 2008;14:648-650

60-Day All-cause Mortality
8.7
18.7 2017.8
13.2
9.1
20
Percent (%)
P<0.05P <0.05
Placebo
Tolvaptan
Vasopressin Antagonist for Heart Failure:ACTIV in CHF Trial
* Edema, Dyspnea, and JVD at baseline
Overall Hyponatremia (Na+ <136 mEq/L)
BUN
(> 29 mg/dL)Congestion*
8.7
5.4
9.1
5.5
0
10
Percent (%)
N = 80 239 16 53 30 110 41 163
(20%) (22%) (37%) (46%) (51%) (68%)
Gheorghiade M. JAMA. 2004;291:1963-1971.

Proportion Surviving
0,6
0,8
1
Tolvaptan
Placebo
Kaplan-Meier analysis of all-cause mortality in the EVEREST trial
Months in Study
Proportion Surviving
Log-Rank Test: P=.76
0
0,2
0,4
0 3 6 9 12 15 18 21 24
Konstam et al. JAMA 2007;297:1319-31.

Effects of adenosine antagonists on GFR and diuresis in ADHF
Gottlieb et al. Circulation 2002;105:1348

Primary Endpoint (PROTECT)Percent of Patients
Odds ratio (95% CI) vs Pbo: 0.92 (0.78, 1.09)
36.0 40.6
60
80
100
Percent of Patients
44.2
19.8
37.5
21.80
20
40
60
Placebo Ro 30 mg
Treatment Success Patient Unchanged Treatment Failure
p=0.348 for comparison of distribution using the van Elteren extension of Wilcoxon test

Time to Death or CV or Renal Rehospitalization - Day 60
0.4
0.3
0.2
0.1
Cumulative Risk
Hazard Ratio (95% CI) = 0.98 (0.83, 1.17)
P-value = 0.861
Placebo
Rolofylline 30 mg
0.0
0 5 10 15 20 25 30 35 40 45 50 55 60 65
Study Day
Death: Placebo 9.5% vs rolofylline 8.9%
Re-hospitalization: Placebo 25.6% vs rolofylline 25.7%

New natriuretic peptides: ularitide
� In 1988, Urodilatin, a renally synthesized isoform of ANP was isolated from human urine.
� Both experimental and early clinical trials demonstrated therapeutic effects of urodilatin (diuresis, natriuresis, vasodilation , reduction of PCWP) to a greater extent than ANP.ANP.
� In SIRIUS I (n=24 pts) and II (n=221pts) ularitide caused a greater improvement of CI and reduction of SVR and NT-proBNP than placebo persisting at 24 hours (neutral effect on 30-day mortality and renal function).
� Ularitide at 30 ng/Kg/min caused SBP reduction/ hypotension in 16% of pts.
(SBP< 80 mm Hg in 10.9% of pts)
Mitrovic et al. Am Heart J 2005;150:1239
Mitrovic et al. Eur Heart J 2006; 27:2823

Beneficial effects of ularitide on clinical status of decompensated HF patients: SIRIUS II
Mitrovic, V. et al. Eur Heart J 2006 27:2823-2832; doi:10.1093/eurheartj/ehl337
The Ularitide Global Evaluation in Acute Decompensated Heart Failure (URGENT), a
phase 3, randomized, double-blind, placebo-controlled study of ularitide in the treatment
of patients with AHFS is expected to begin soon.

Relaxin Mechanisms of Action
� Vasodilation
– NO, cGMP effectors
– Induction of NOS II/III
– Upregulation of endothelial endothelin type B receptor, which mediates vasodilation
� Preferential dilation of
Relaxin
� Preferential dilation of constricted vessels
– Relaxin-upregulated ETB receptors act as vasodilating ET-1 sink
� Anti-inflammatory
– Down-modulation of inflammatory cytokines linked to outcome in HF (TNF-α, TGF-β)
� Other: Anti-ischemic, Anti-apoptotic, Anti-fibrotic
Teichman, SL, et al. Heart Fail Rev 2009; Dschietzig, T, et al. Pharmacol Therap 2006


RELAX-AHFEffect of serelaxin on AHF symptoms
Serelaxin, recombinant
human relaxin-2, is a
vasoactive peptide hormone
with many biological and
haemodynamic effects
Inclusion criteria (1161pts)
Teerlink et al. Lancet 2013;381:29-39
Inclusion criteria (1161pts)
•dyspnoea
•congestion on Rx
•Increased BNP/NT-proBNP
•GFR: 30-75ml/min
•Systolic BP>125 mm Hg.
48-h i.v. serelaxin or placebo (30
μg/kg per day) within 16 h from
presentation

RELAX-AHFEffect of serelaxin on 180d mortality
Teerlink et al. Lancet 2013;381:29-39

Effect of Serelaxin on Cardiac, Renal, and Hepatic Biomarkers in RELAX-AHF
J Am Coll Cardiol 2013;61:196–206)

Serelaxin in AHF patients with preserved LVEF: RELAX-AHF sub-analysis
Filippatos et al Eur Heart J 2013 November 12

Etiology of Anemia inPatients With Advanced Heart Failure
37 advanced CHF pts; NYHA IV; mean LVEF: 37 advanced CHF pts; NYHA IV; mean LVEF: 22%.
Nanas J Nanas J ,,…, Anastasiou…, Anastasiou--Nana MNana M . . J Am Coll Cardiol 2006;48:2485–9

Ferric Carboxymaltose in Patients with HeartFailure and Iron Deficiency(Anker S, Colet C, Filippatos G, et al. NEJM 2009)

CONCLUSION
� Patient education and further implementation of treatment guidelines are essential approaches to improve outcomes in HF.
� There are still no Class I effective therapies in AHF in comparison to � There are still no Class I effective therapies in AHF in comparison to CHF.
� Investigational drugs targeting to novel pathophysiologic concepts are promising treatment approaches and ongoing trials will define their clinical efficacy and safety.
Top Related