Update on pharmacological treatment of heart failure
32
Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy
Transcript of Update on pharmacological treatment of heart failure

Update on pharmacological treatment of heart failure
Aldo Pietro Maggioni, MD, FESC
ANMCO Research Center
Firenze, Italy
Presenter Disclosures
Dr. Maggioni :
• Serving in Committees of studies sponsored by: Amgen, Bayer, Abbott Vascular, Johnson & Johnson, Novartis Pharma AG
Agenda
• Systolic heart failure (NYHA class II-IV)
• treatment options
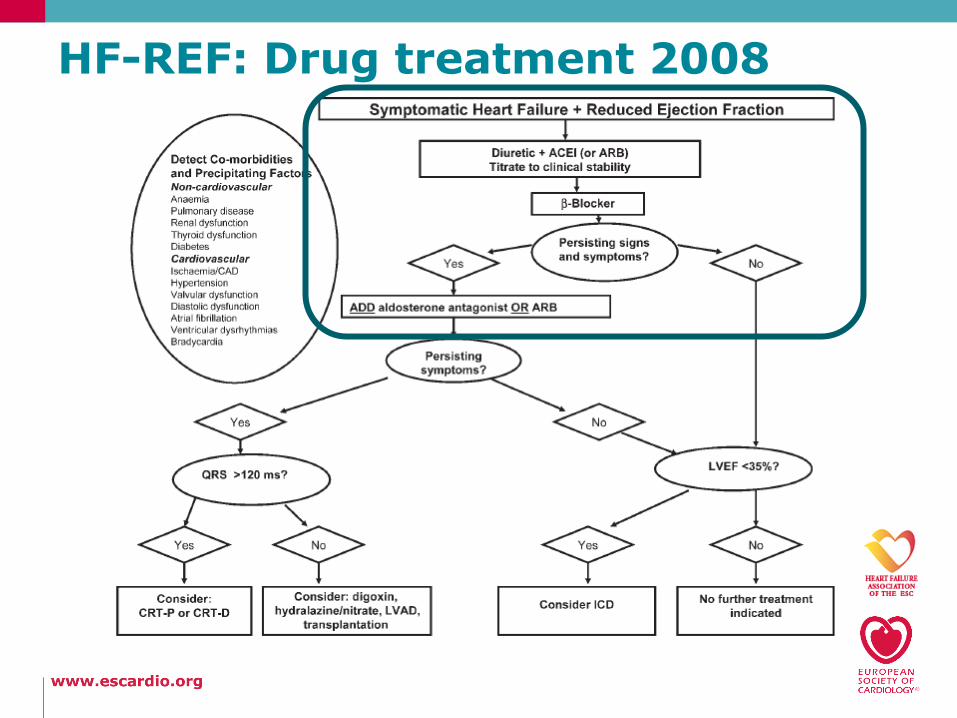
HF-REF: Drug treatment 2008
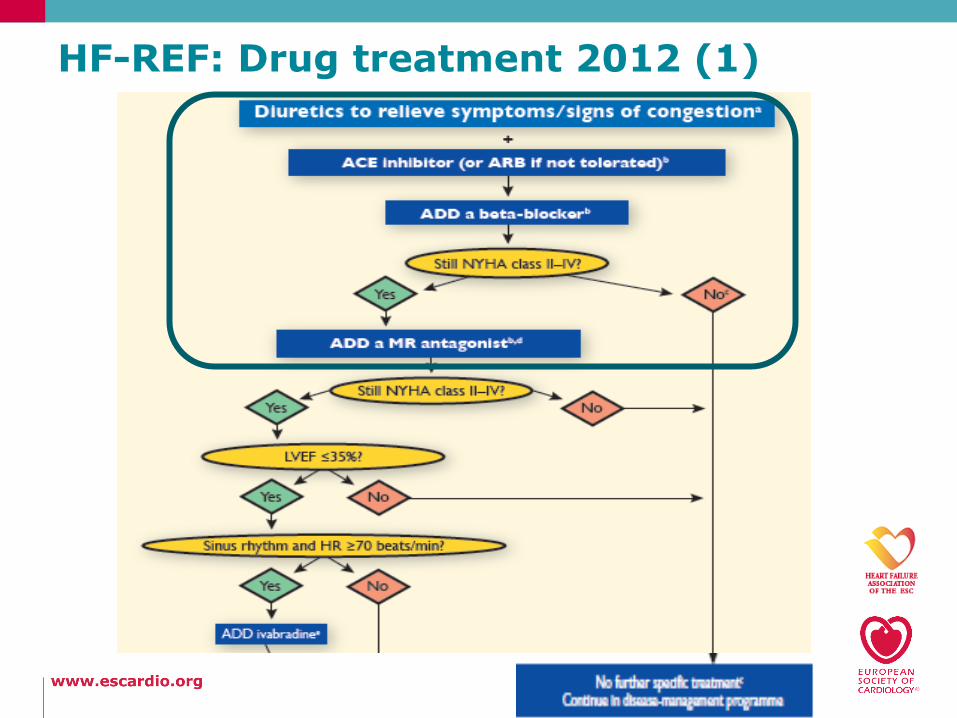
HF-REF: Drug treatment 2012 (1)
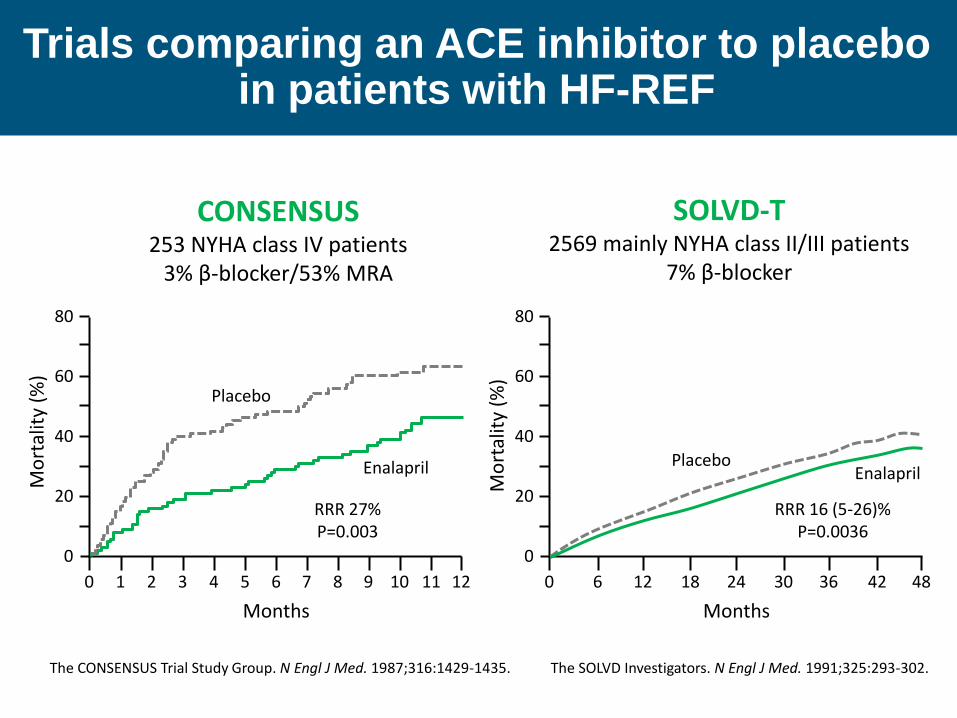
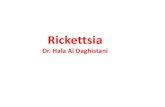
CONSENSUS 253 NYHA class IV patients
3% β-blocker/53% MRA
SOLVD-T 2569 mainly NYHA class II/III patients
7% β-blocker
Placebo
Enalapril
RRR 27% P=0.003
Mo
rtal
ity
(%)
Months
0 1 2 3 4 5 6 7 8 9 10 11 12
20
40
60
80
0
Placebo Enalapril
RRR 16 (5-26)% P=0.0036
Mo
rtal
ity
(%)
Months
0 6 12 18 24 30 36 42 48
20
40
60
80
0
The CONSENSUS Trial Study Group. N Engl J Med. 1987;316:1429-1435. The SOLVD Investigators. N Engl J Med. 1991;325:293-302.
Trials comparing an ACE inhibitor to placebo in patients with HF-REF
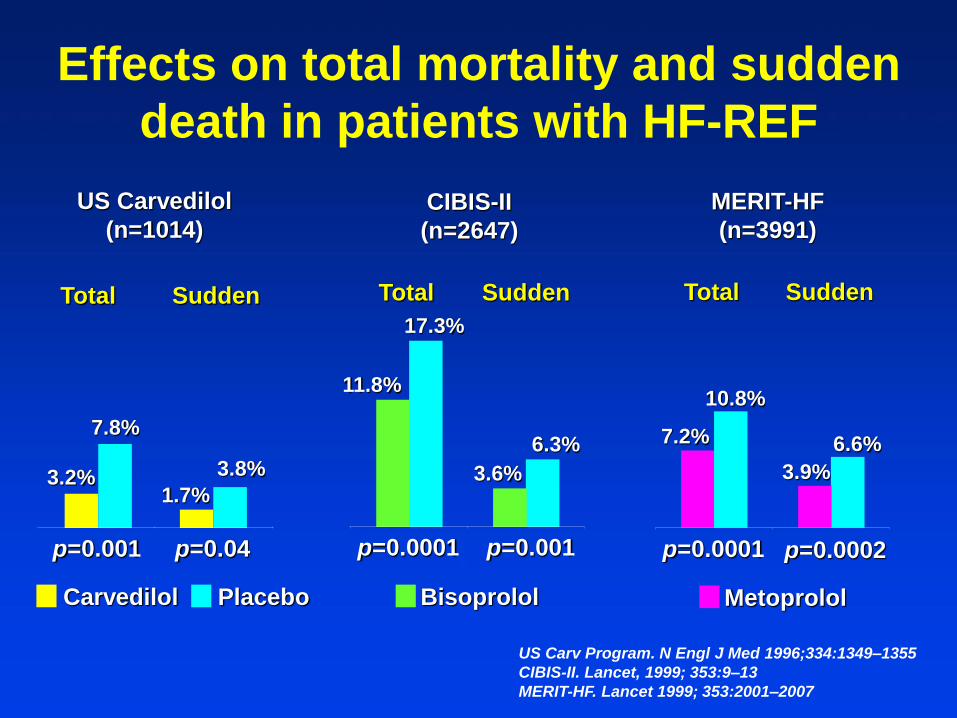
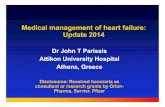
Total Sudden
p=0.001 p=0.04
US Carvedilol
(n=1014)
Total Sudden
CIBIS-II
(n=2647)
p=0.0001 p=0.001
Total Sudden
MERIT-HF
(n=3991)
p=0.0001 p=0.0002
3.2% 1.7%
7.8%
3.8%
7.2%
10.8%
3.9%
6.6%
11.8%
17.3%
3.6%
6.3%
Effects on total mortality and sudden
death in patients with HF-REF
Carvedilol Placebo Bisoprolol Metoprolol
US Carv Program. N Engl J Med 1996;334:1349–1355
CIBIS-II. Lancet, 1999; 353:9–13
MERIT-HF. Lancet 1999; 353:2001–2007
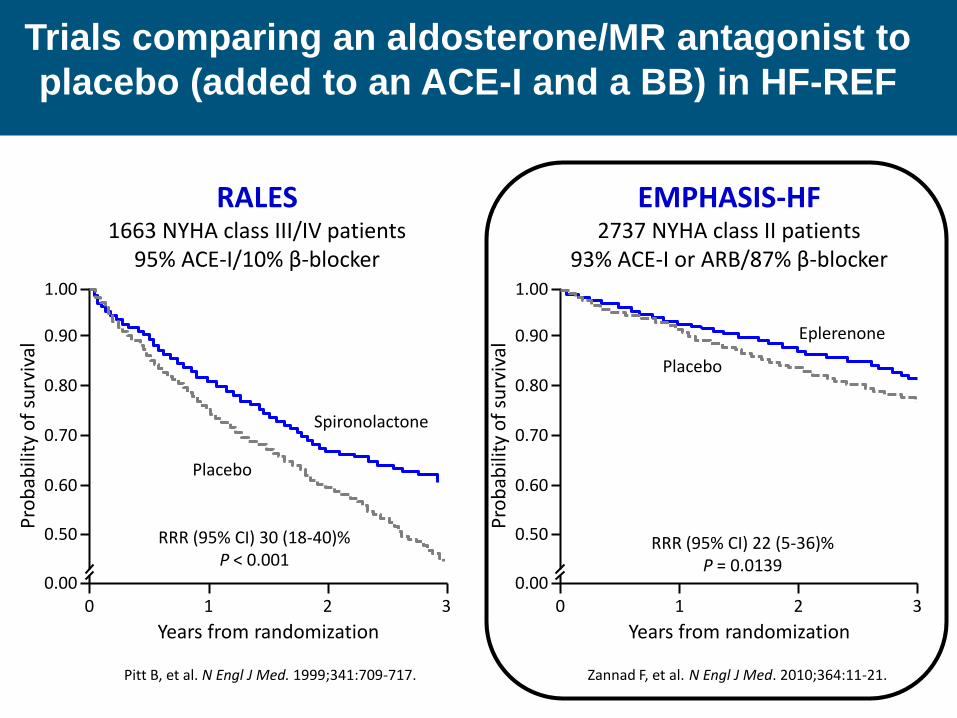
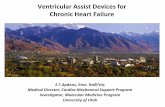
RALES 1663 NYHA class III/IV patients
95% ACE-I/10% β-blocker
EMPHASIS-HF 2737 NYHA class II patients
93% ACE-I or ARB/87% β-blocker
RRR (95% CI) 22 (5-36)% P = 0.0139
Eplerenone
Placebo
Placebo
Spironolactone
RRR (95% CI) 30 (18-40)% P < 0.001
Pro
bab
ility
of
surv
ival
Years from randomization 0 1 2 3
0.50
0.70
0.80
0.90
0.00
1.00
0.60 P
rob
abili
ty o
f su
rviv
al
Years from randomization 0 1 2 3
0.50
0.70
0.80
0.90
0.00
1.00
0.60
Pitt B, et al. N Engl J Med. 1999;341:709-717. Zannad F, et al. N Engl J Med. 2010;364:11-21.
Trials comparing an aldosterone/MR antagonist to
placebo (added to an ACE-I and a BB) in HF-REF
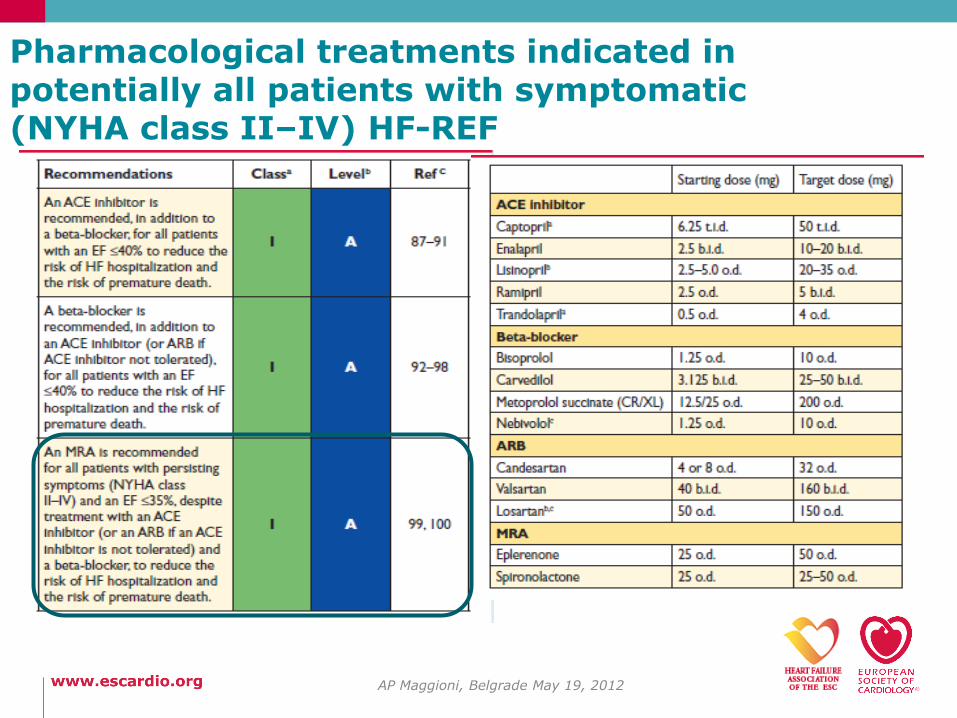
Pharmacological treatments indicated in potentially all patients with symptomatic (NYHA class II–IV) HF-REF
AP Maggioni, Belgrade May 19, 2012
Agenda
• Systolic heart failure (NYHA class II-IV)
• treatment options
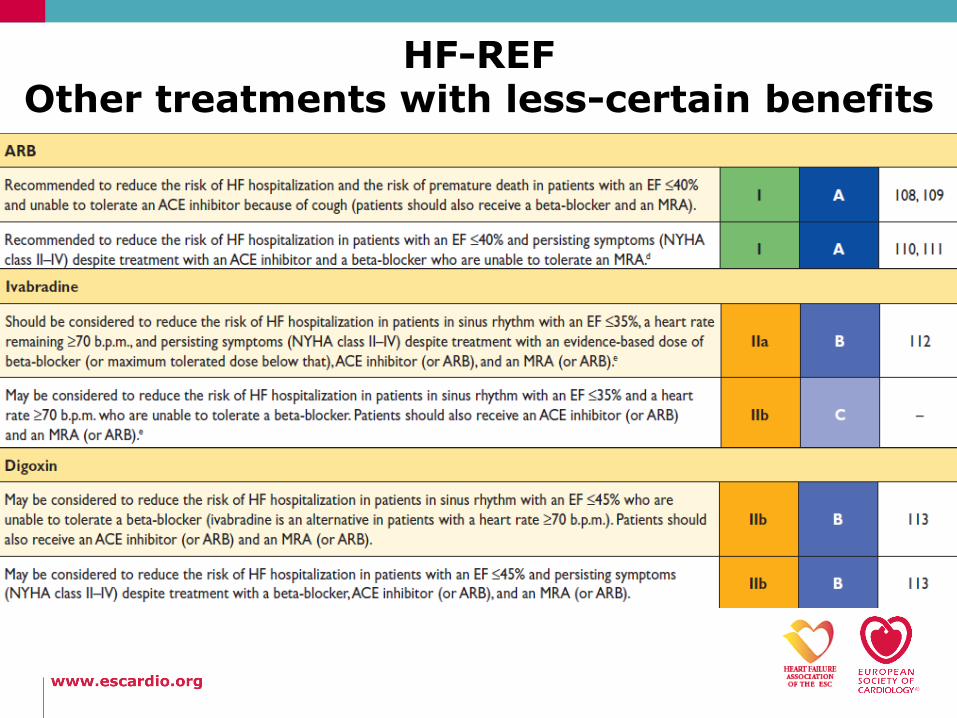
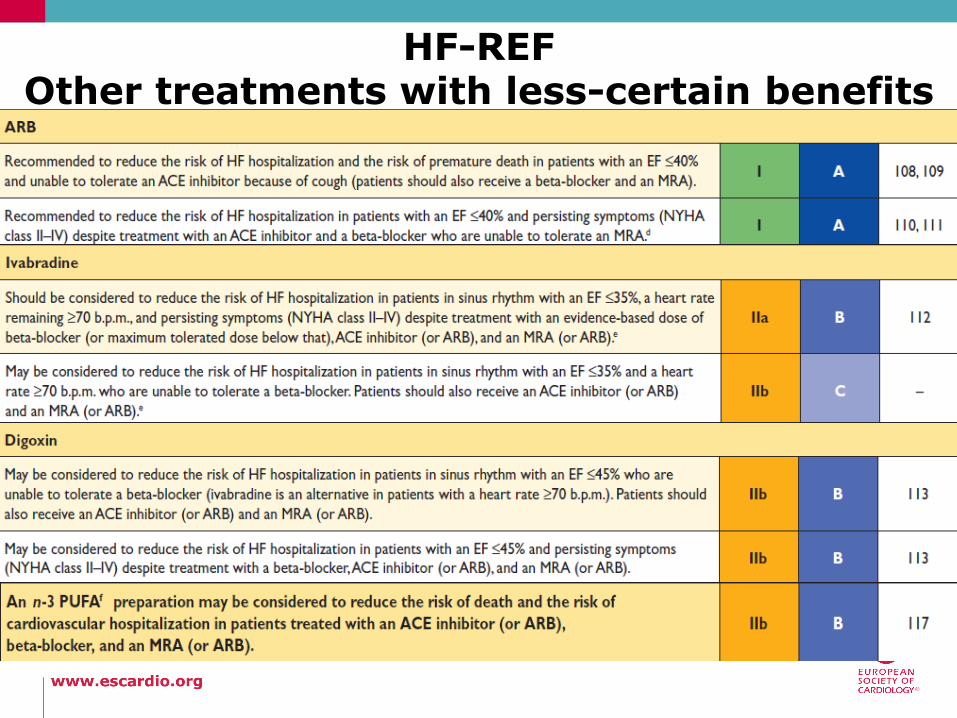
• other treatments with less-certain benefits
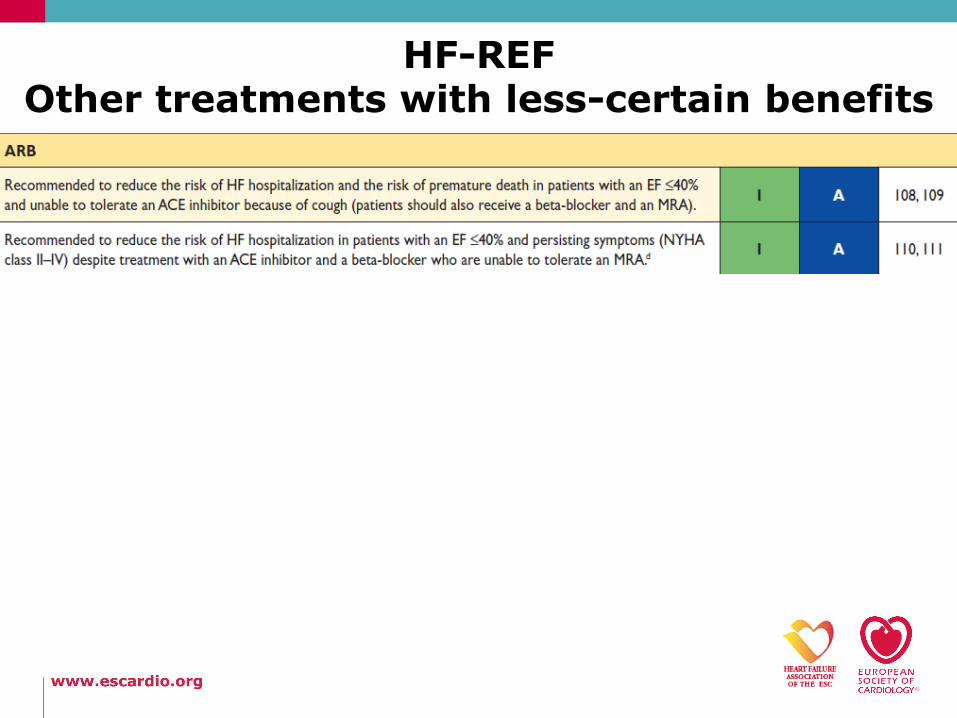
HF-REF Other treatments with less-certain benefits
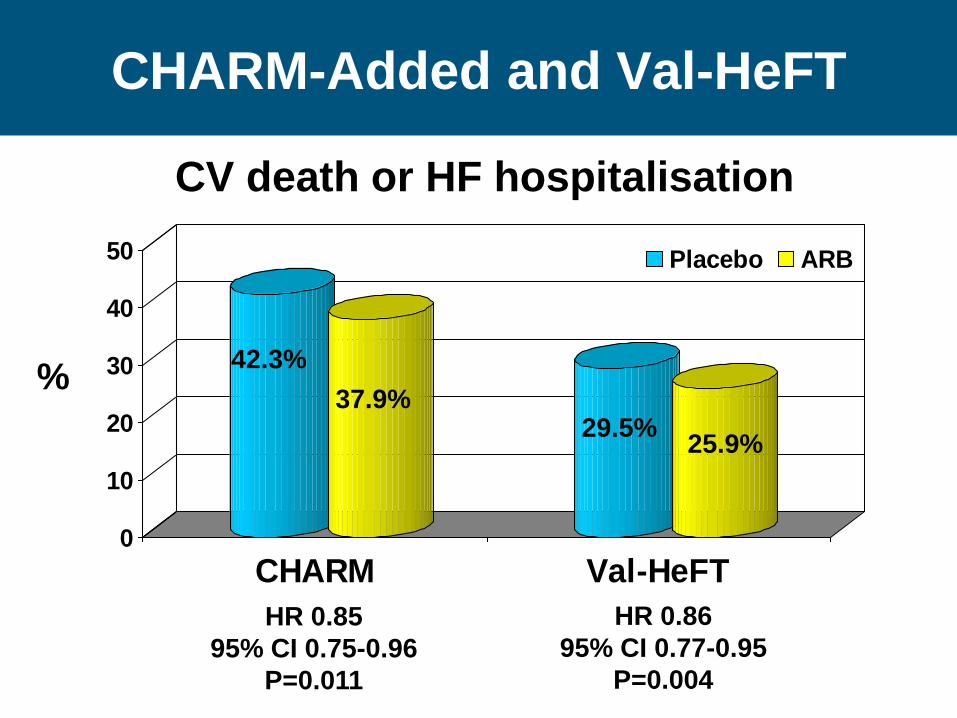
CHARM-Added and Val-HeFT
0
10
20
30
40
50
CHARM Val-HeFT
Placebo ARB
42.3%
37.9% 29.5%
25.9%
HR 0.85
95% CI 0.75-0.96
P=0.011
HR 0.86
95% CI 0.77-0.95
P=0.004
%
CV death or HF hospitalisation
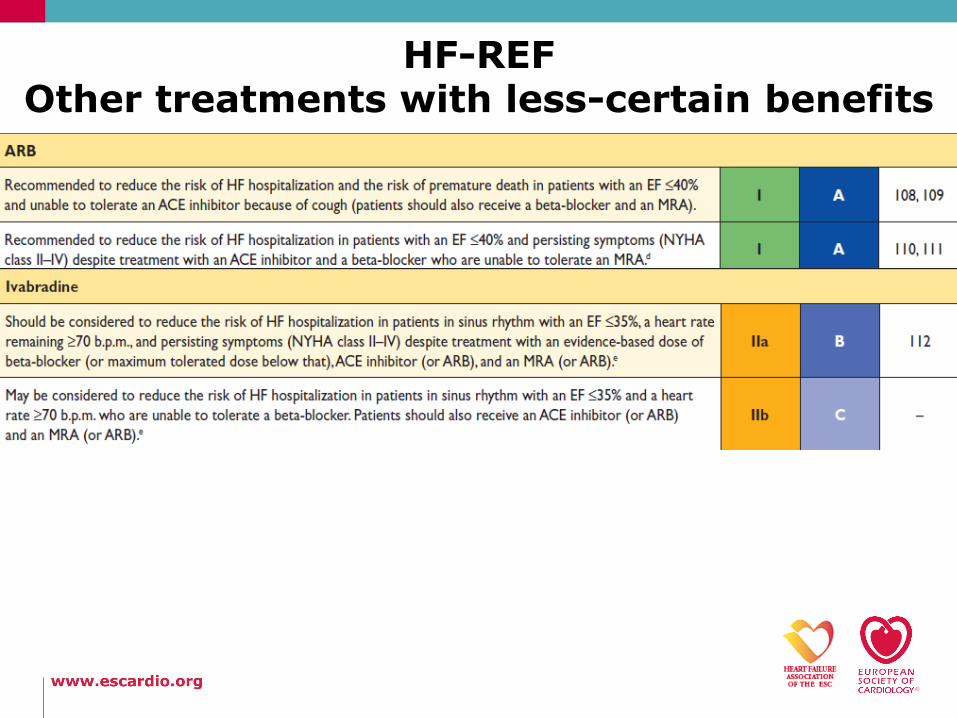
HF-REF Other treatments with less-certain benefits
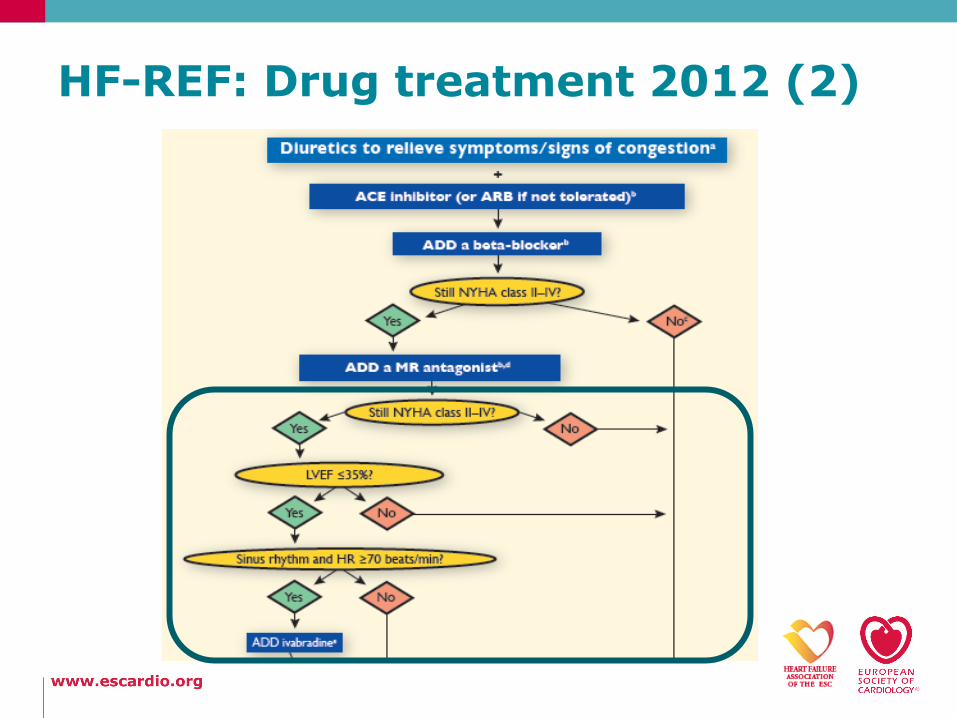
HF-REF: Drug treatment 2012 (2)
HF-REF Other treatments with less-certain benefits
HF-REF Other treatments with less-certain benefits
AP Maggioni, Belgrade May 19, 2012
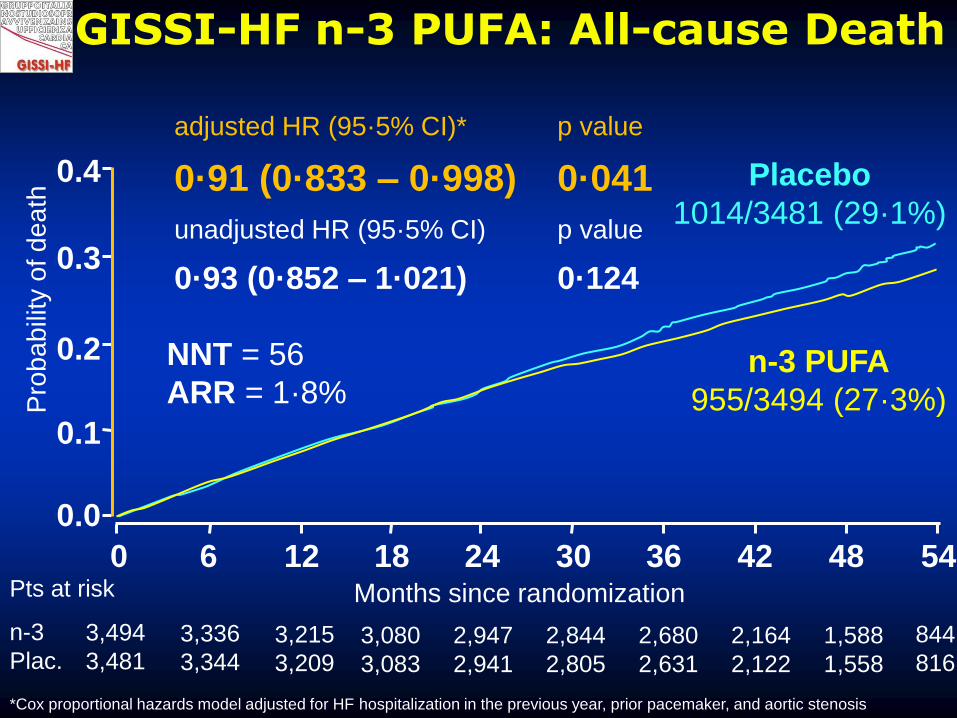
NNT = 56
ARR = 1·8%
adjusted HR (95·5% CI)* p value
0·91 (0·833 – 0·998) 0·041
unadjusted HR (95·5% CI) p value
0·93 (0·852 – 1·021) 0·124
0.4
0.3
0.2
0.1
0.0
0 6 12 18 24 30 36 42 48 54
Pro
ba
bili
ty o
f d
ea
th
Months since randomization
*Cox proportional hazards model adjusted for HF hospitalization in the previous year, prior pacemaker, and aortic stenosis
Pts at risk
n-3
Plac.
3,494
3,481 3,336
3,344 3,215
3,209 3,080
3,083
2,947
2,941
2,844
2,805
2,680
2,631
2,164
2,122
1,588
1,558
844
816
Placebo
1014/3481 (29·1%)
GISSI-HF n-3 PUFA: All-cause Death
n-3 PUFA
955/3494 (27·3%)
Agenda
• Systolic heart failure (NYHA class II-IV)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Statins (neutral results of CORONA and GISSI-HF)
• Renin inhibitors (studies still ongoing)
• Oral anticoagulants other than in patients with AF
• Treatments that may cause harm
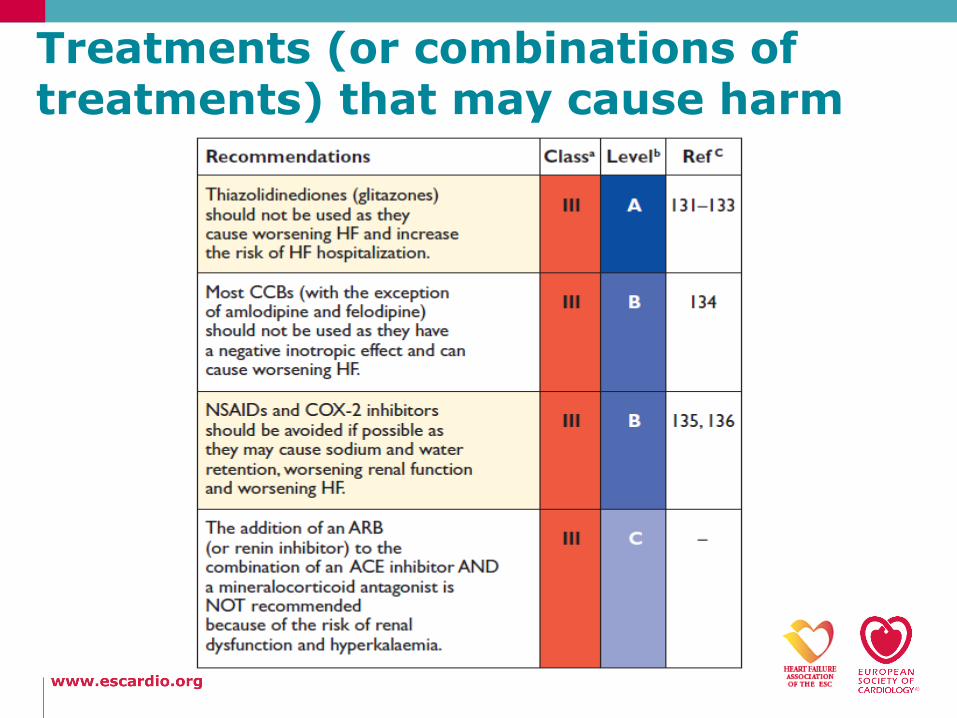
Treatments (or combinations of treatments) that may cause harm
Agenda
• Systolic heart failure (HF-REF)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Preserved ejection fraction (HF-PEF)
Pharmacological treatment of patients with HF-PEF (1)
• No treatment has yet been shown, convincingly, to reduce morbidity and mortality in these patients
• Diuretics are used to control sodium and water retention and relieve breathlessness and oedema
• Adequate treatment of hypertension and myocardial ischaemia is also considered to be important, as is control of the ventricular rate in patients with AF
• The drugs that should be avoided in HF-REF should also be avoided in HF-PEF, with the exception of CCBs
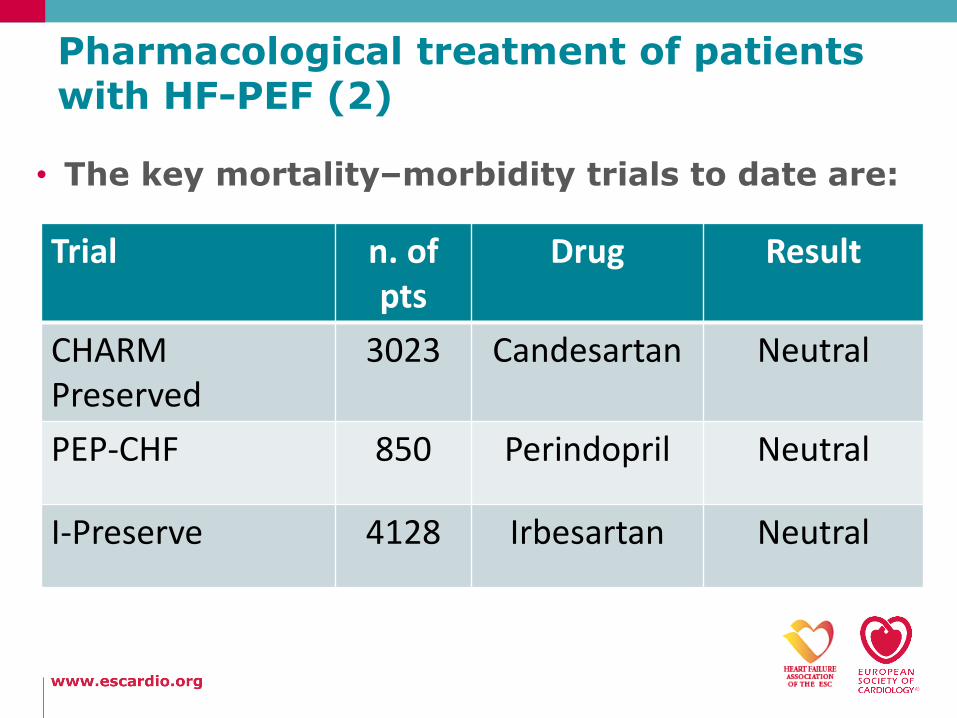
Pharmacological treatment of patients with HF-PEF (2)
• The key mortality–morbidity trials to date are:
Trial n. of
pts Drug Result
CHARM Preserved
3023 Candesartan Neutral
PEP-CHF 850 Perindopril Neutral
I-Preserve 4128 Irbesartan Neutral
Agenda
• Systolic heart failure (HF-REF)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Preserved ejection fraction (HF-PEF)
• Update on pharmacological treatment of co-morbidities
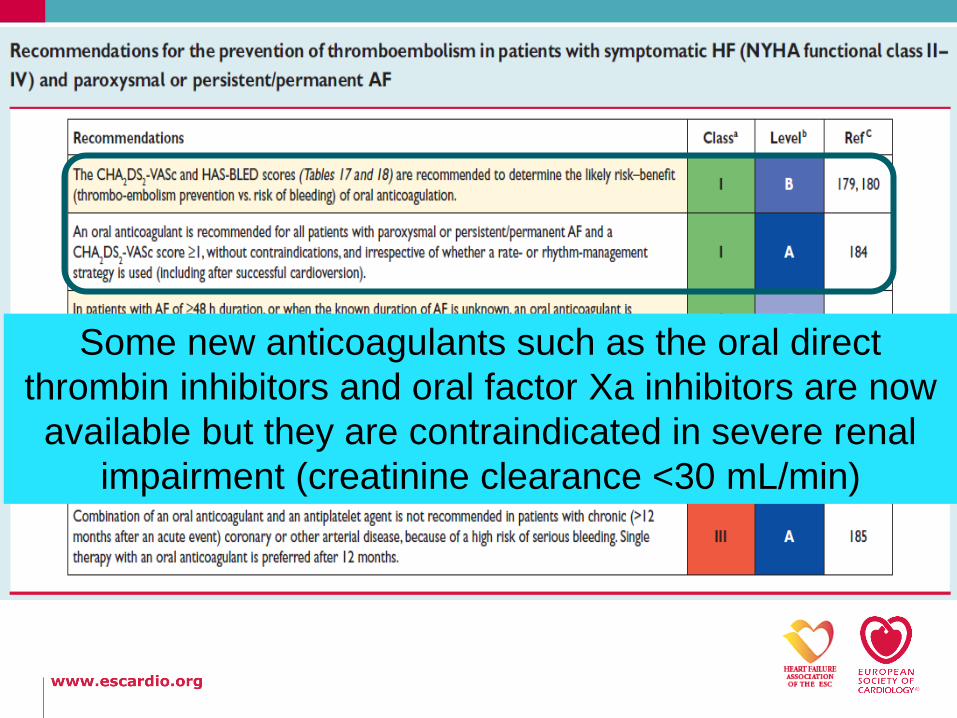
Some new anticoagulants such as the oral direct
thrombin inhibitors and oral factor Xa inhibitors are now
available but they are contraindicated in severe renal
impairment (creatinine clearance <30 mL/min)
Anaemia and iron deficiency
• Anaemia is associated with worse functional status, greater risk of HF hospitalization, and reduced survival
• Correctable causes should be treated in the usual way
• The value of erythropoietin-stimulating agents is unknown but is currently being tested in a large mortality–morbidity RCT (RED-HF)
• Iron deficiency may independently contribute to muscle dysfunction in HF and causes anaemia
• FAIR HF evaluated 459 HF-REF patients (NYHA class II-III), a haemoglobin level 9.5 to 13.5 g/dL, and iron deficiency
• IV iron therapy improved self-reported patient global assessment
• IV iron may be considered as a treatment for these patients
Agenda
• Systolic heart failure (HF-REF)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Preserved ejection fraction (HF-PEF)
• Update on pharmacological treatment of co-morbidities
• Acute HF
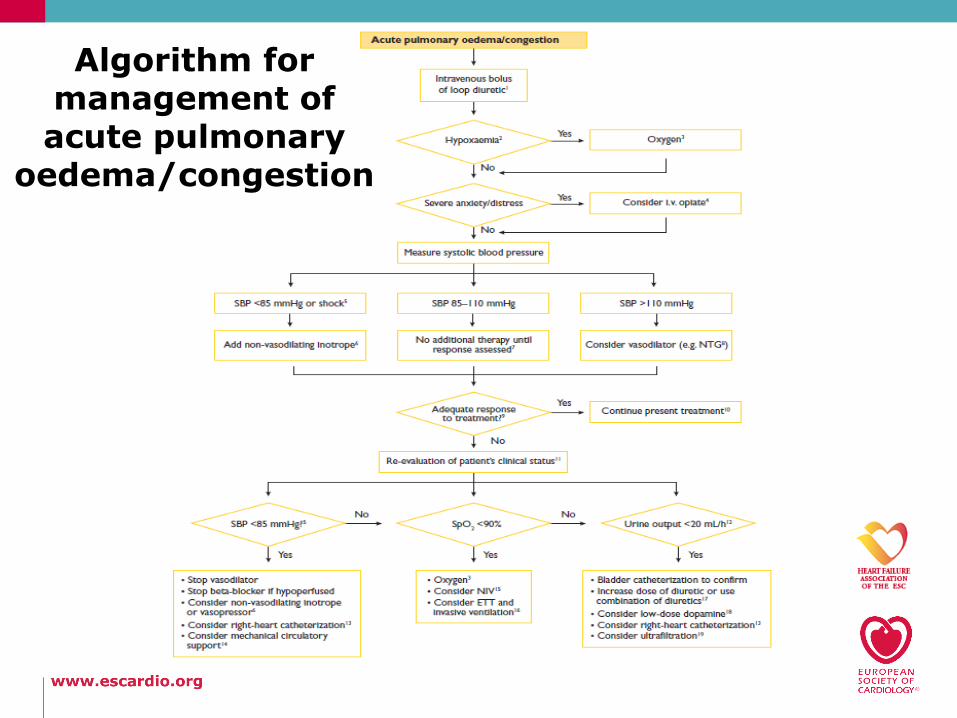
Algorithm for management of acute pulmonary
oedema/congestion
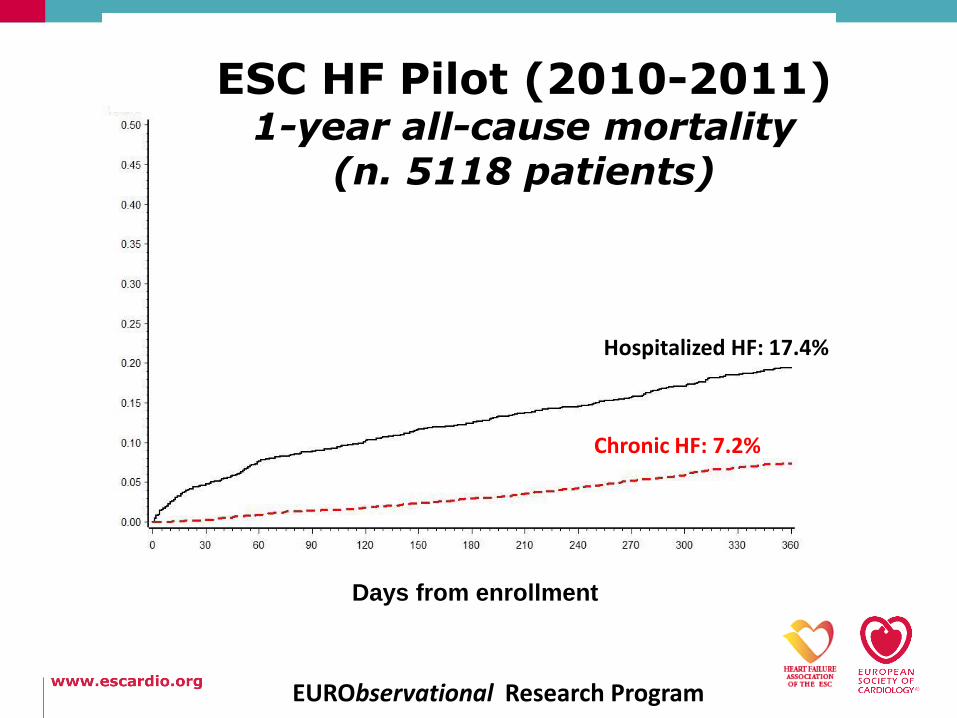
ESC HF Pilot (2010-2011) 1-year all-cause mortality
(n. 5118 patients)
Days from enrollment
Chronic HF: 7.2%
Hospitalized HF: 17.4%
EURObservational Research Program
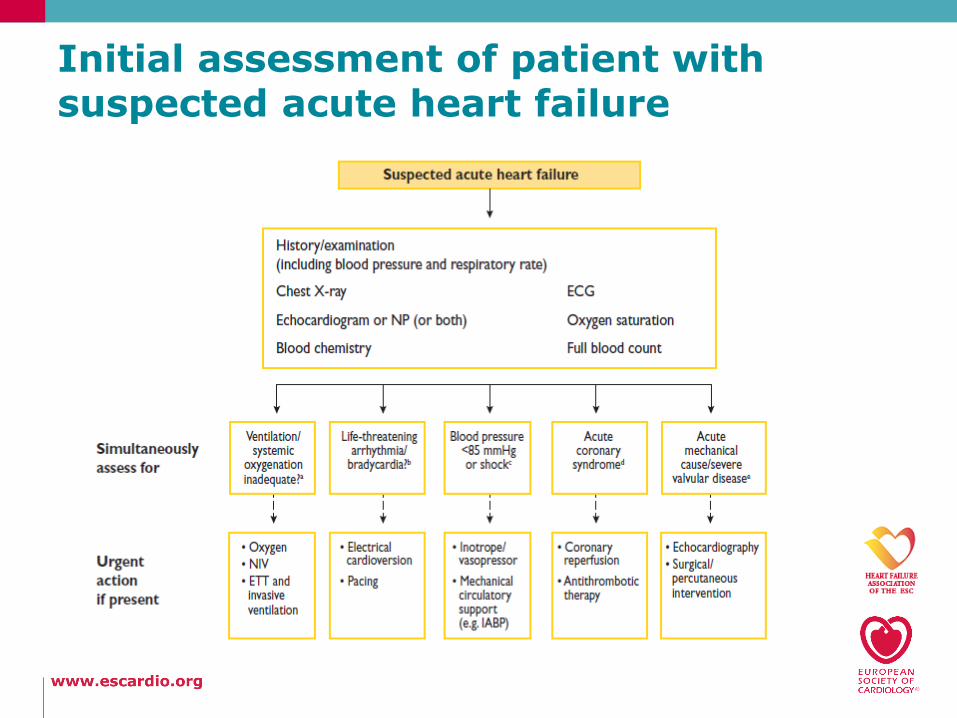
Initial assessment of patient with suspected acute heart failure