





γλώσσες
Σελίδες
Νομικός

Gastro-intestinal failureIntensive Care Training Program
Radboud University Medical Centre Nijmegen
Case history (1)
• Male, 47
• No previous medical history
• Mechanical ventilation for severe CAP
• Stable HD on NE 0.04 μg/kg/min
• Early enteral nutrition (nasogastric route)
• Selective decontamination + PPI
Case history (2)
• Day 3 - Stable HD on NE 0.02 μg/kg/min
• PSV with FiO2 55% and PEEP 12
• Gastric aspirate volume has been > 500 mL over the previous day on EN1000 mL
• Slight abdominal distention and diminished bowel sounds
ICU fellow raises simple question
• What is the meaning of this and what is the influence on the prognosis?
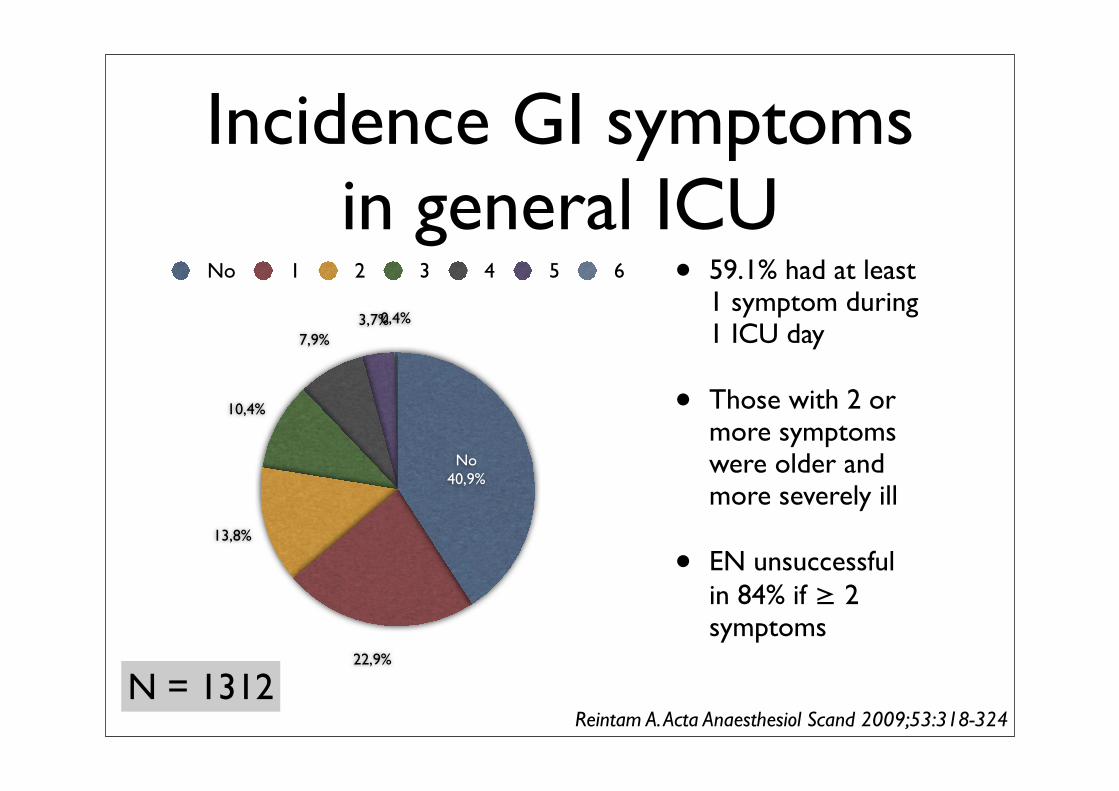
Incidence GI symptoms in general ICU
• 59.1% had at least 1 symptom during 1 ICU day
• Those with 2 or more symptoms were older and more severely ill
• EN unsuccessful in 84% if ≥ 2 symptoms
0,4%3,7%7,9%
10,4%
13,8%
22,9%
No40,9%
No 1 2 3 4 5 6
Reintam A. Acta Anaesthesiol Scand 2009;53:318-324N = 1312
GI symptoms
• Absent or abnormal bowel sounds
• Vomiting
• Nasogastric aspirate > 500 mL/day
• Diarrhoea
• Bowel distension
• GI bleeding
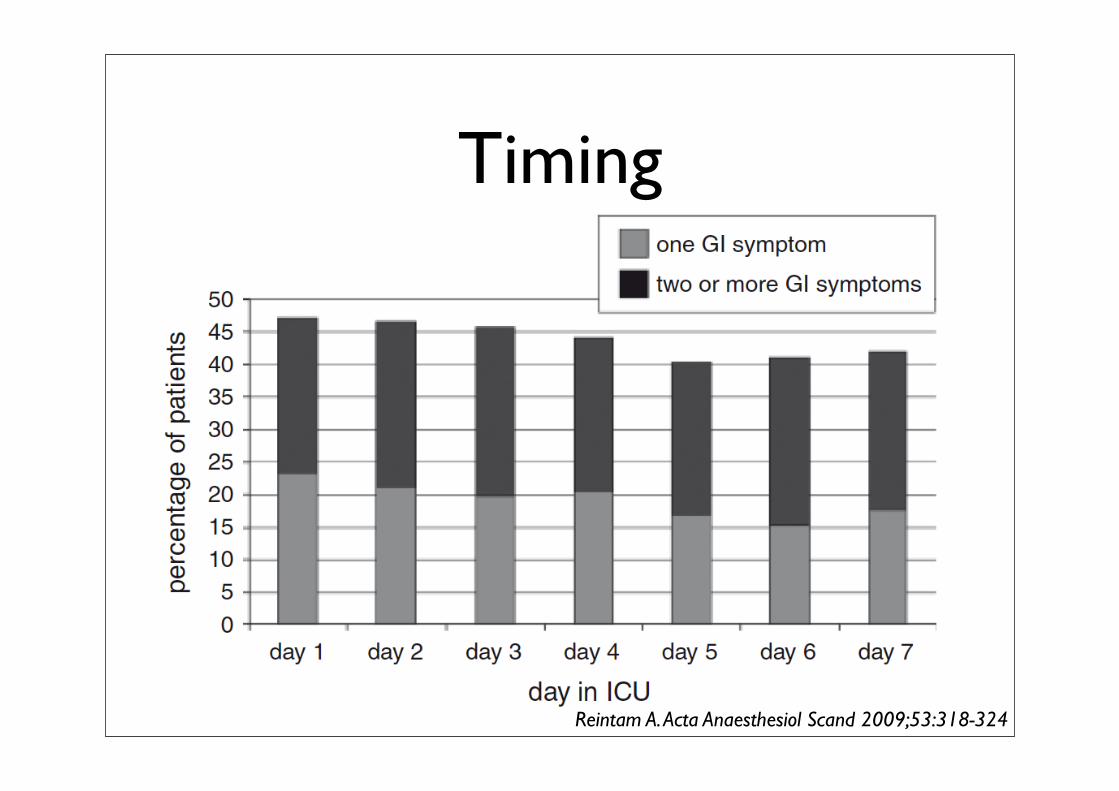
Timing
Reintam A. Acta Anaesthesiol Scand 2009;53:318-324

GI symptoms and LOS
0
15
30
45
60
No 1 2 3 4 ≥ 5
LOS
(day
s)
Number of symptoms
Reintam A. Acta Anaesthesiol Scand 2009;53:318-324
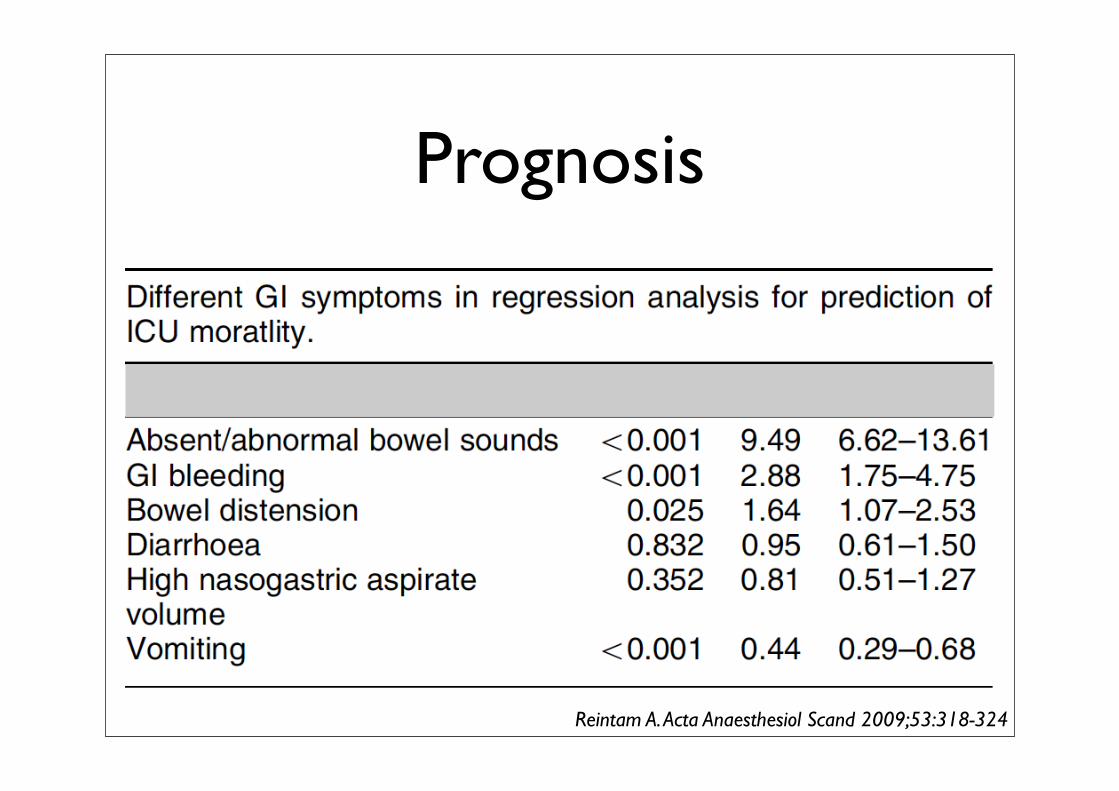
Prognosis
Reintam A. Acta Anaesthesiol Scand 2009;53:318-324

Case history (3)
• On day 4 the patient receives post pyloric feeding
• Gastric aspirate volumes decrease but the abdomen is slightly more distended, bowel sounds are diminished and bowel movements are absent
Case history (4)
• Enteral feeding is stopped - parenteral feeding is started including additional glutamine supplementation
ICU fellow raises two simple questions
• Are there any markers by which we can judge the severity of the mucosal damage?
• What is the evidence that glutamine improves gastro-intestinal barrier function in this situation?
Potential markers for mucosal damage
• Citrulline
• Intestinal fatty acid binding protein (I-FABP)
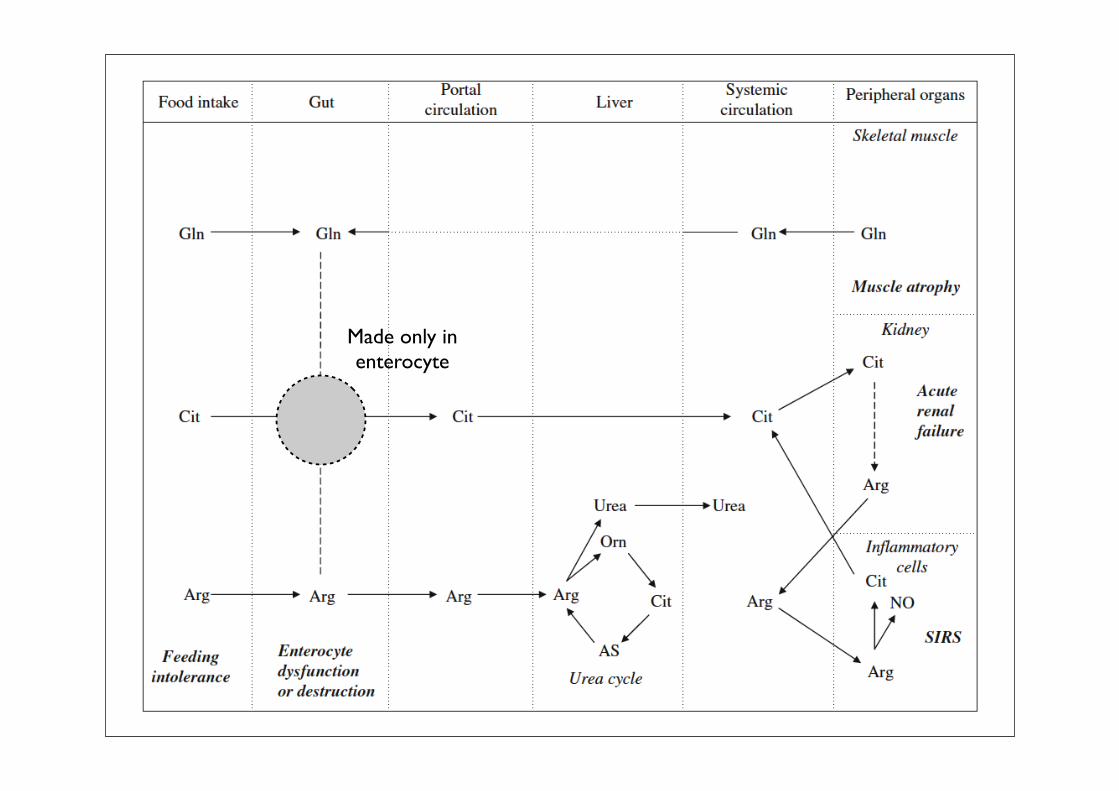
Made only inenterocyte
Citrulline
• Low plasma citrulline correlates with small bowel toxicity following chemotherapy and radiotherapy
• Low plasma citrulline correlates with the occurrence bacteremia (barrier function)
• Early indicator of rejection following SB Tx
Biomarker of reduced enterocyte mass
I-FABP
• Located at the tips of of intestinal vili
• 2 - 3% of total protein of the enterocyte
• Generally undetectable in circulation
• Measure for enterocyte ischaemia/damage
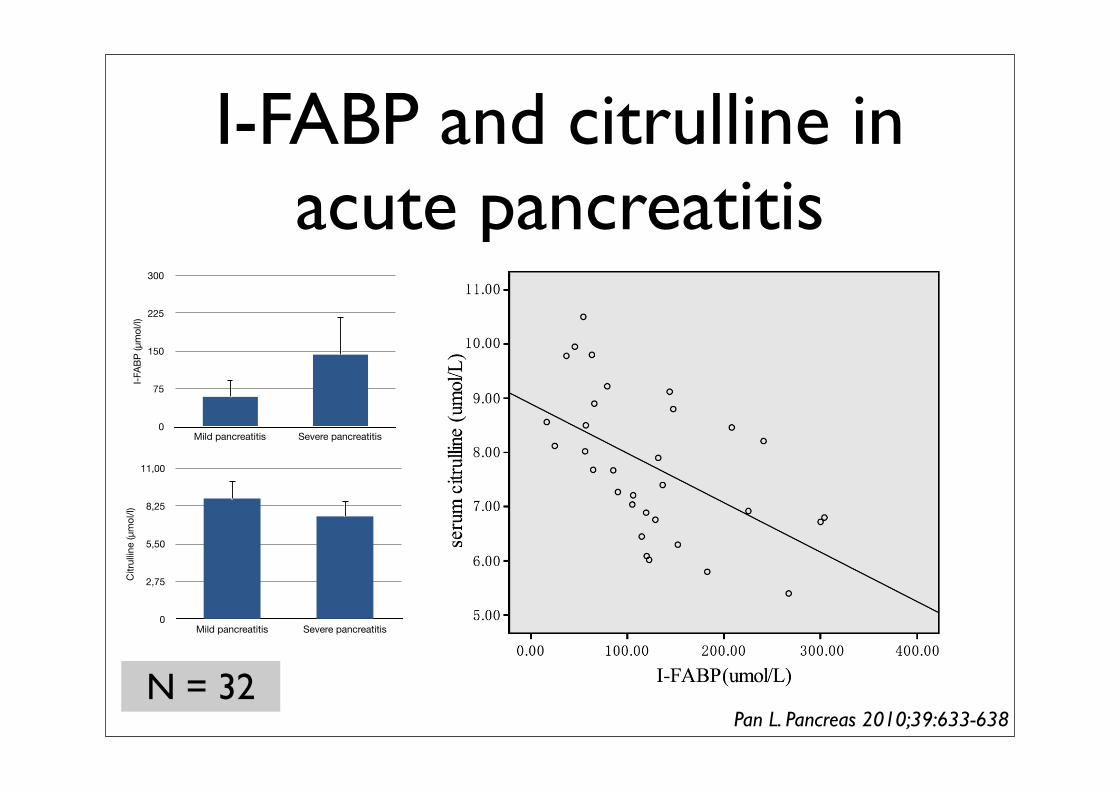
I-FABP and citrulline in acute pancreatitis
N = 32
0
75
150
225
300
Mild pancreatitis Severe pancreatitis
I-FAB
P (μ
mol
/l)
0
2,75
5,50
8,25
11,00
Mild pancreatitis Severe pancreatitis
Citr
ullin
e (μ
mol
/l)
Pan L. Pancreas 2010;39:633-638

I-FABP and citrulline in acute pancreatitis
Pan L. Pancreas 2010;39:633-638
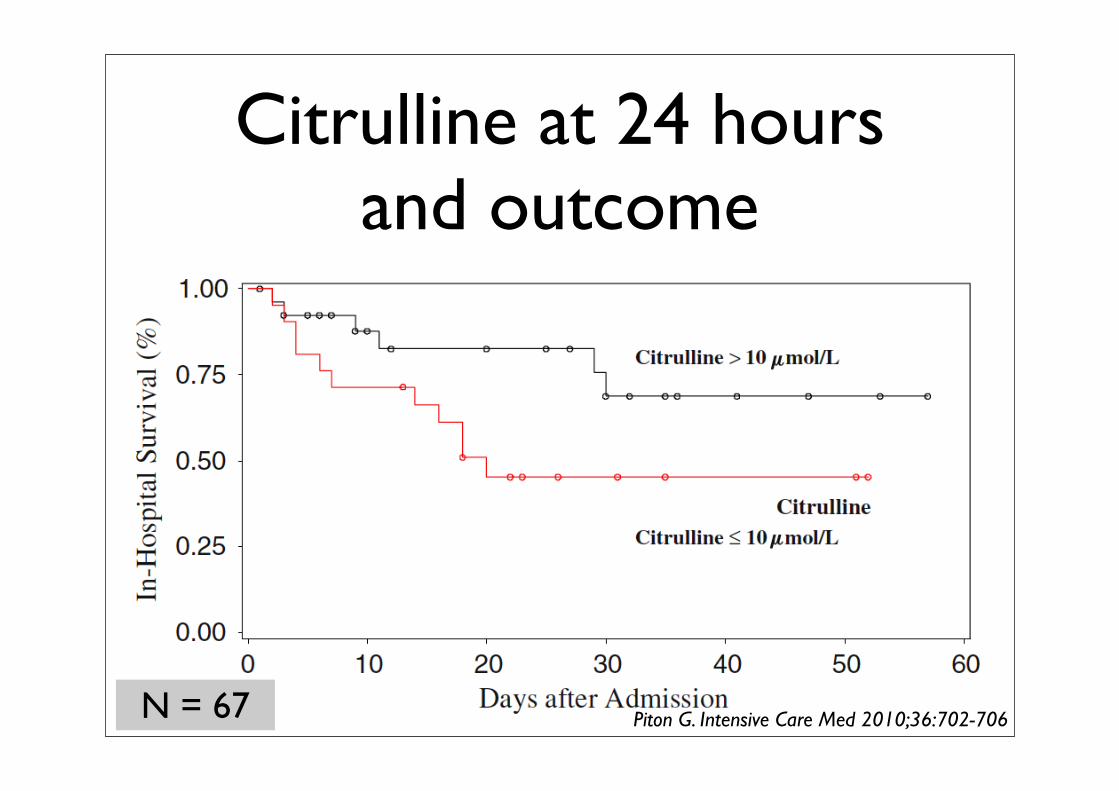
Citrulline at 24 hours and outcome
N = 67 Piton G. Intensive Care Med 2010;36:702-706
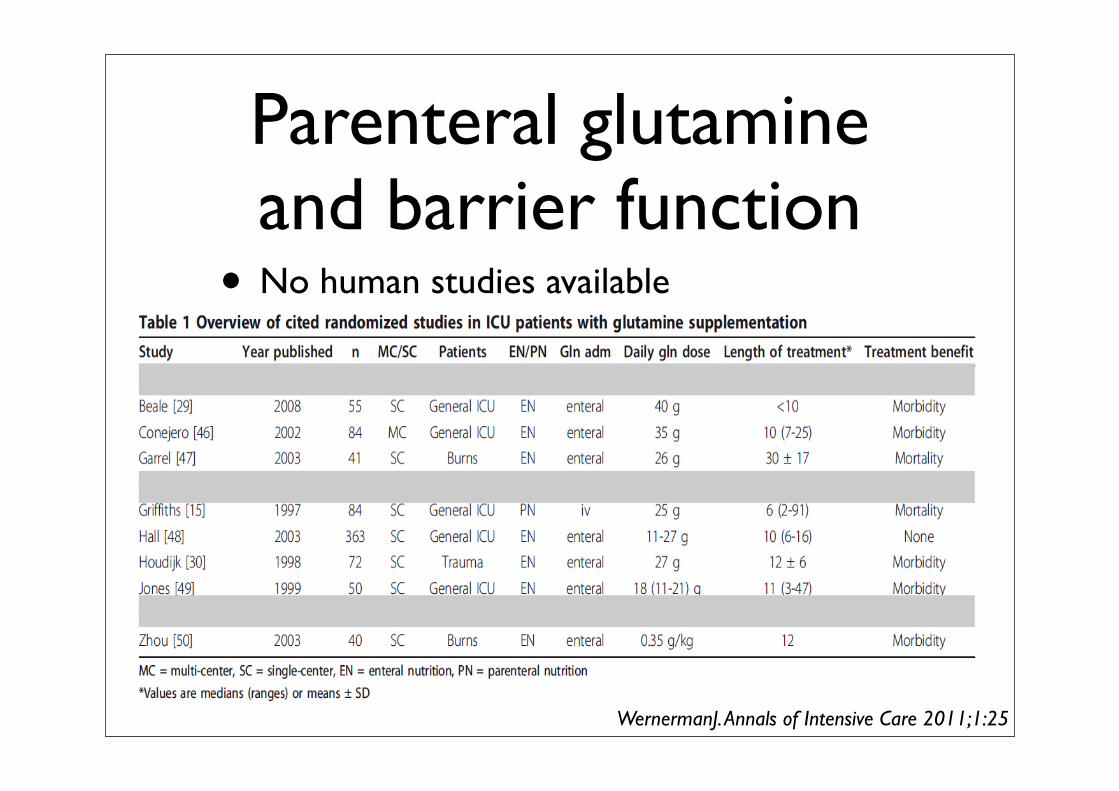
Parenteral glutamine and barrier function• No human studies available
WernermanJ. Annals of Intensive Care 2011;1:25
Case history (5)
• On the sixth day the abdomen is less distended and he passed stools after the i.v. infusion of neostigmine
• Enteral feeding is restarted but severe diarrhea develops. Because insufficient calories may be provided, TPN is restarted
ICU fellow raises two simple questions
• How should we evaluate diarrhea in the ICU?
• Should we give lactose free enteral feeding?
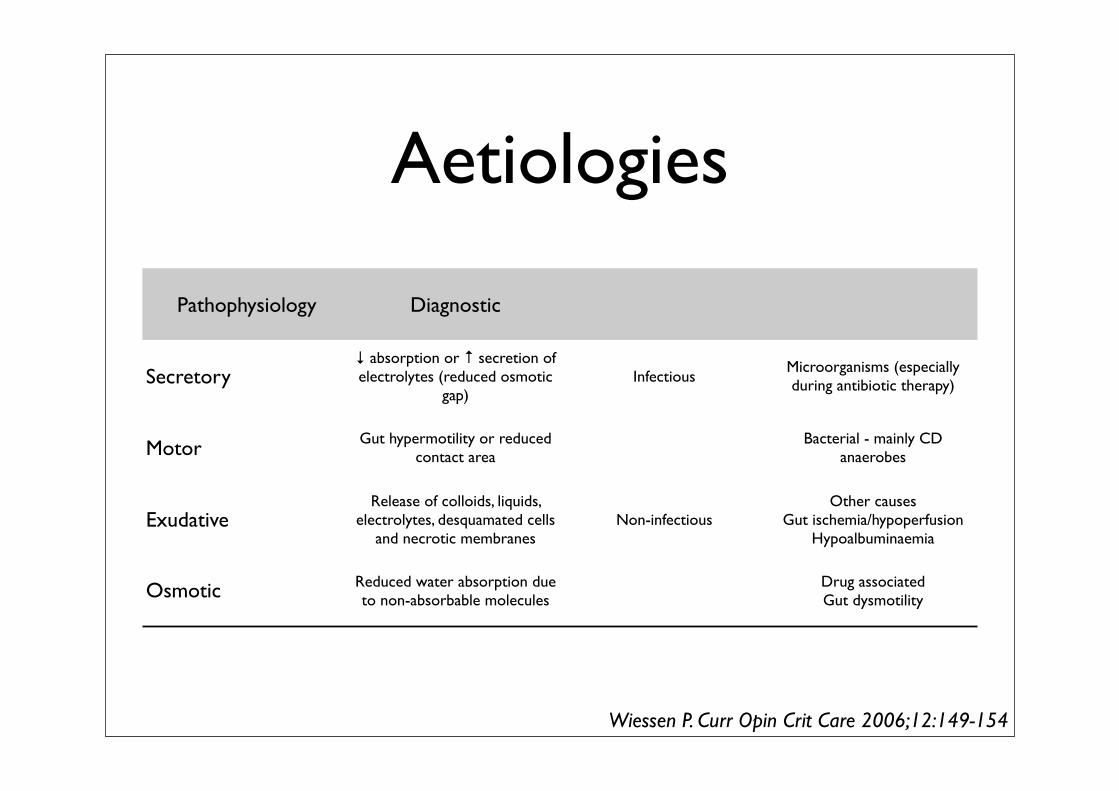
Aetiologies
Pathophysiology Diagnostic
Secretory↓ absorption or ↑ secretion of electrolytes (reduced osmotic
gap)Infectious
Microorganisms (especially during antibiotic therapy)
Motor Gut hypermotility or reduced contact area
Bacterial - mainly CDanaerobes
ExudativeRelease of colloids, liquids,
electrolytes, desquamated cells and necrotic membranes
Non-infectiousOther causes
Gut ischemia/hypoperfusionHypoalbuminaemia
Osmotic Reduced water absorption due to non-absorbable molecules
Drug associatedGut dysmotility
Wiessen P. Curr Opin Crit Care 2006;12:149-154
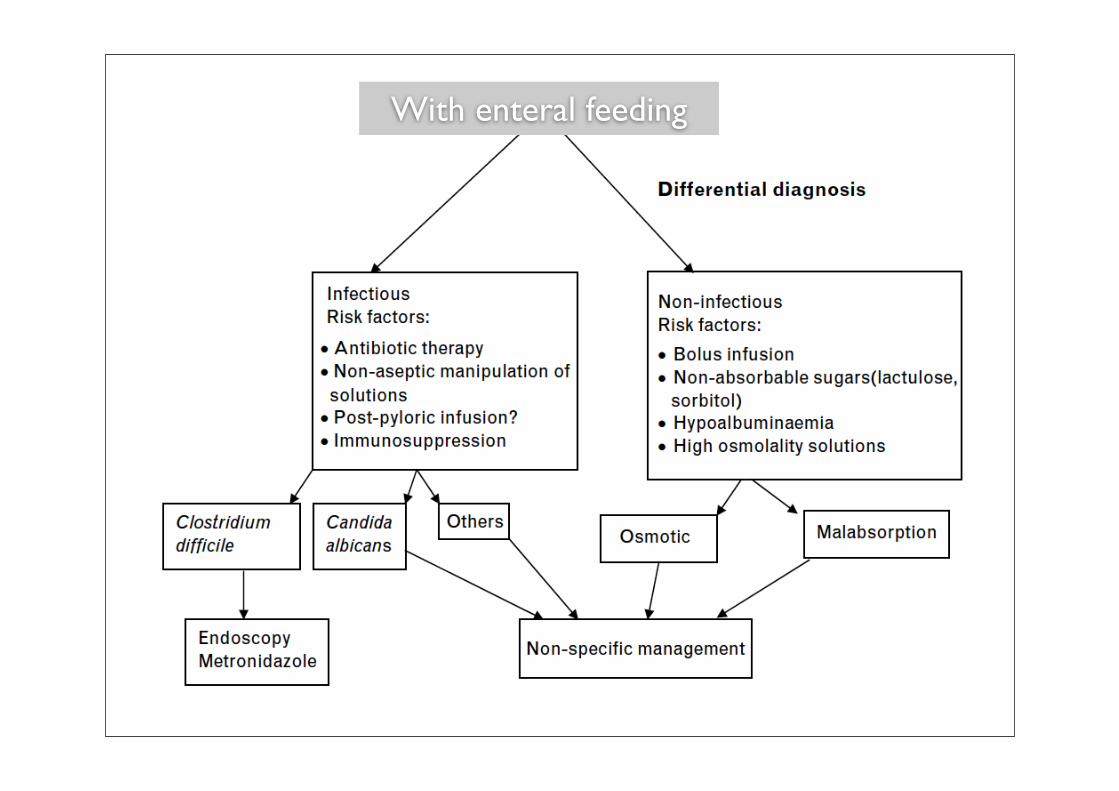
With enteral feeding
Lactase deficiency
Lactose deficiency in ICU
• Many articles state that lactase deficiency is very frequent in the ICU due to loss of villi and brush border
• However - Literature search negative

Case history (6)
• Lactose free enteral feeding reintroduced
• No recurrence of diarrhea
• Subsequently uncomplicated clinical course
• Discharge on D 15
Questions• Which items would you include in a GI
failure score and why?
• Is there evidence to continue the use of stress ulcer prophylaxis?
• What is the role of neostigmine to stimulate bowel movements in ICU patients?
• Are probiotics useful in treating critically ill patients with diarrhea

Gastrointestinal Failure score
Points Clinical symptomatology
0 Normal gastrointestinal function
1 EN < 50% calculated needs or no feeding 3 days after abdominal surgery
2 Food intolerance or intra-abdominal hypertension
3 Food intolerance and intra-abdominal hypertension
4 Abdominal compartment syndrome
Reintam A. Crit Care 2008;12:R90N = 264
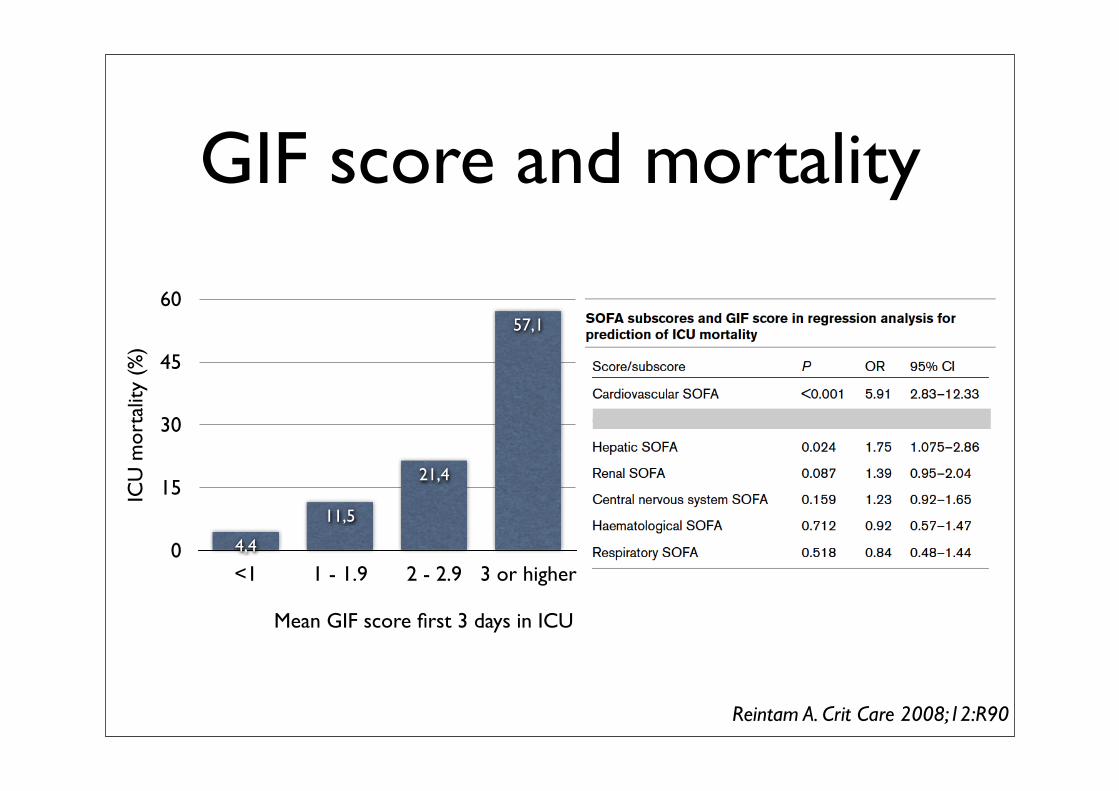
GIF score and mortality
0
15
30
45
60
<1 1 - 1.9 2 - 2.9 3 or higher
57,1
21,4
11,5
4,4
ICU
mor
talit
y (%
)
Mean GIF score first 3 days in ICU
Reintam A. Crit Care 2008;12:R90
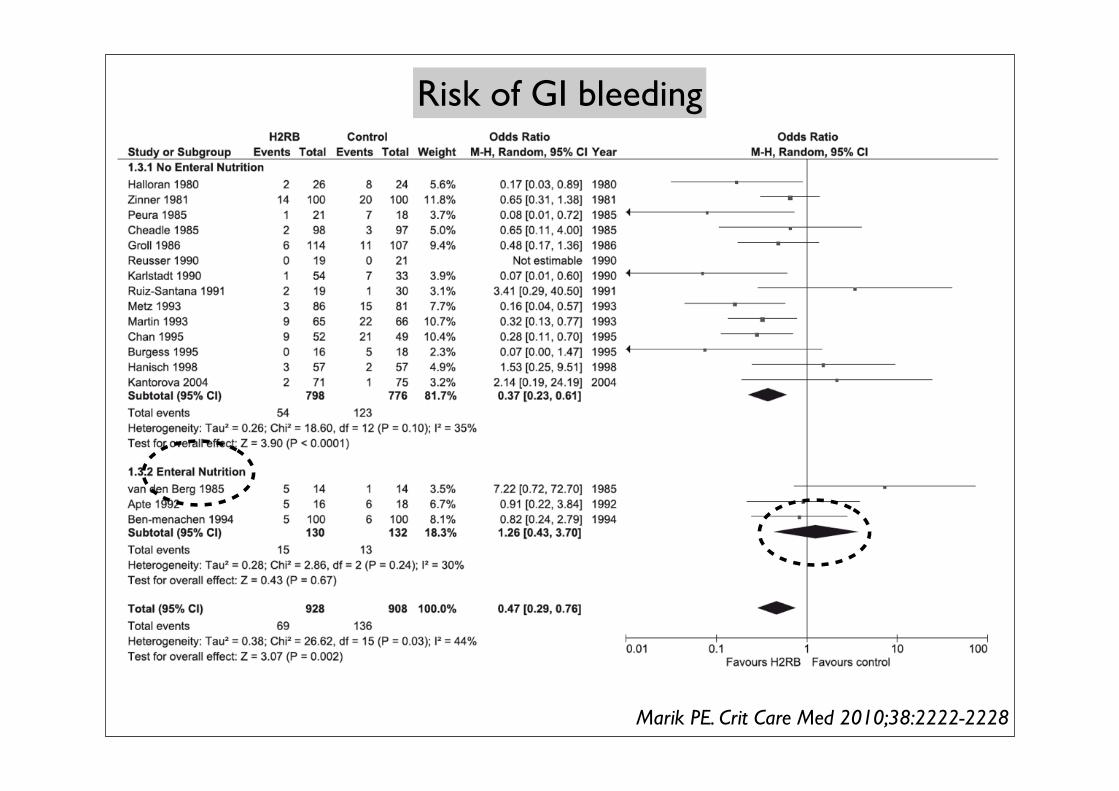
Risk of GI bleeding
Marik PE. Crit Care Med 2010;38:2222-2228
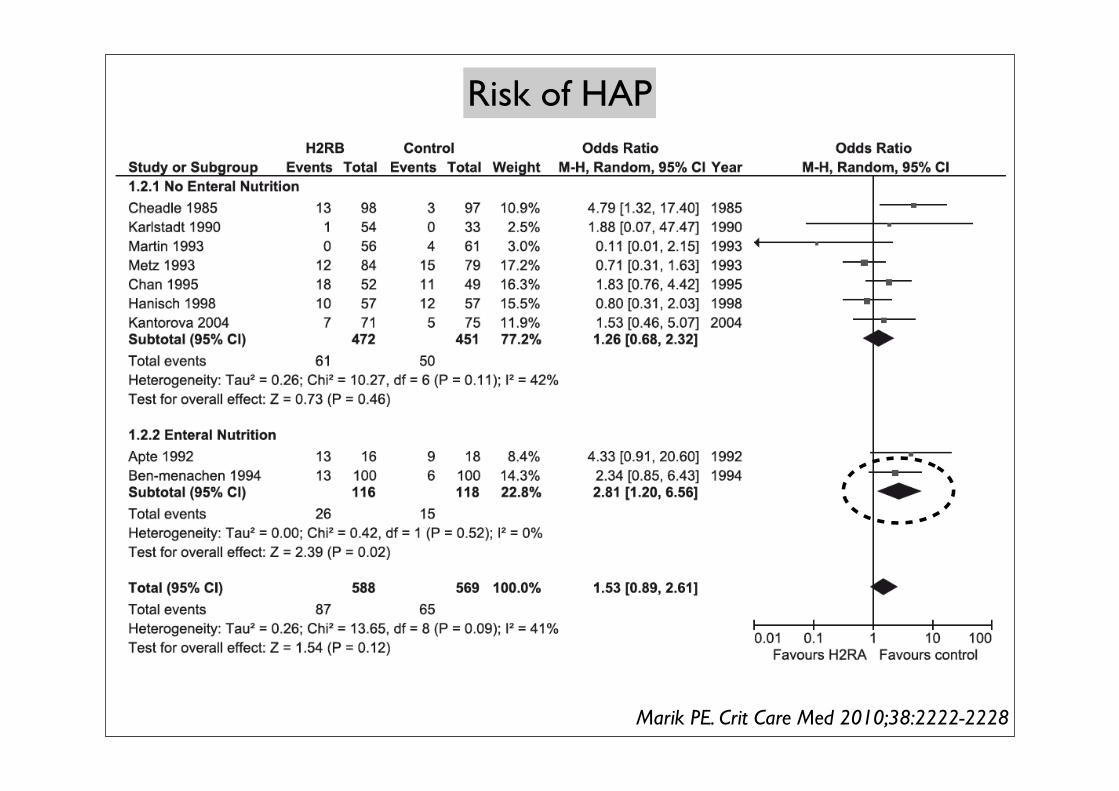
Risk of HAP
Marik PE. Crit Care Med 2010;38:2222-2228
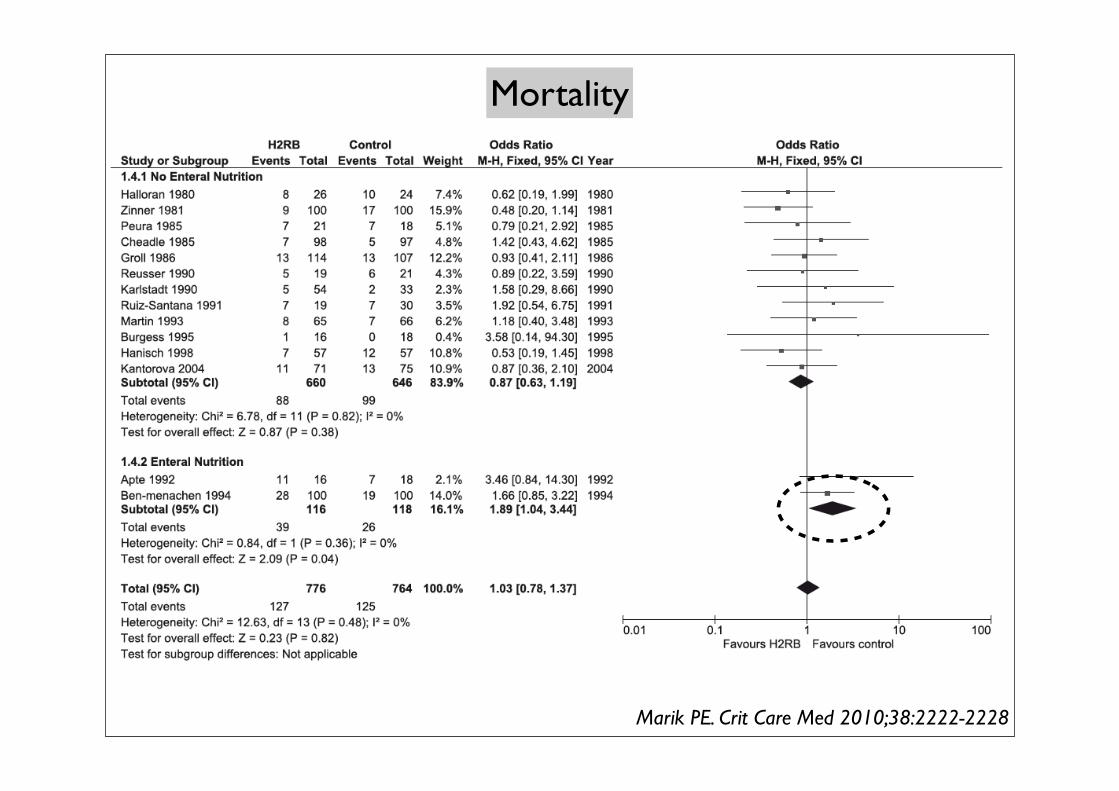
Mortality
Marik PE. Crit Care Med 2010;38:2222-2228
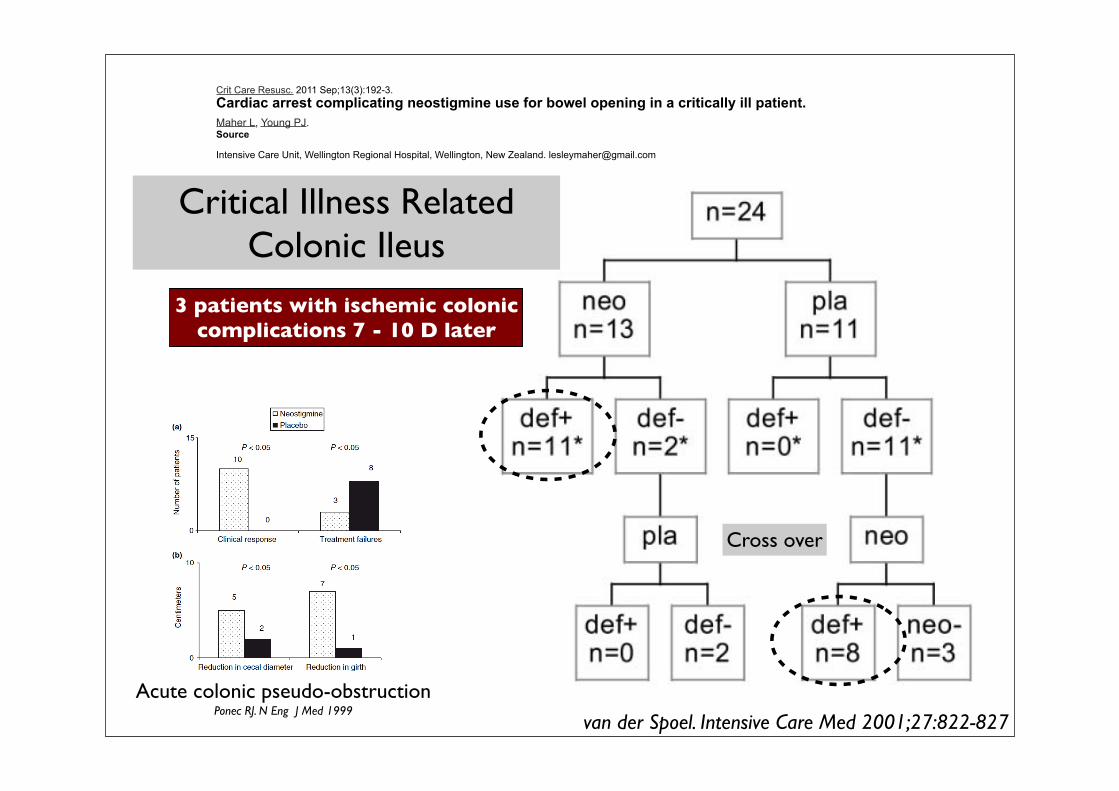
Crit Care Resusc. 2011 Sep;13(3):192-3.Cardiac arrest complicating neostigmine use for bowel opening in a critically ill patient.Maher L, Young PJ.Source
Intensive Care Unit, Wellington Regional Hospital, Wellington, New Zealand. [email protected]
van der Spoel. Intensive Care Med 2001;27:822-827
Critical Illness Related Colonic Ileus
3 patients with ischemic coloniccomplications 7 - 10 D later
Cross over
Acute colonic pseudo-obstructionPonec RJ. N Eng J Med 1999
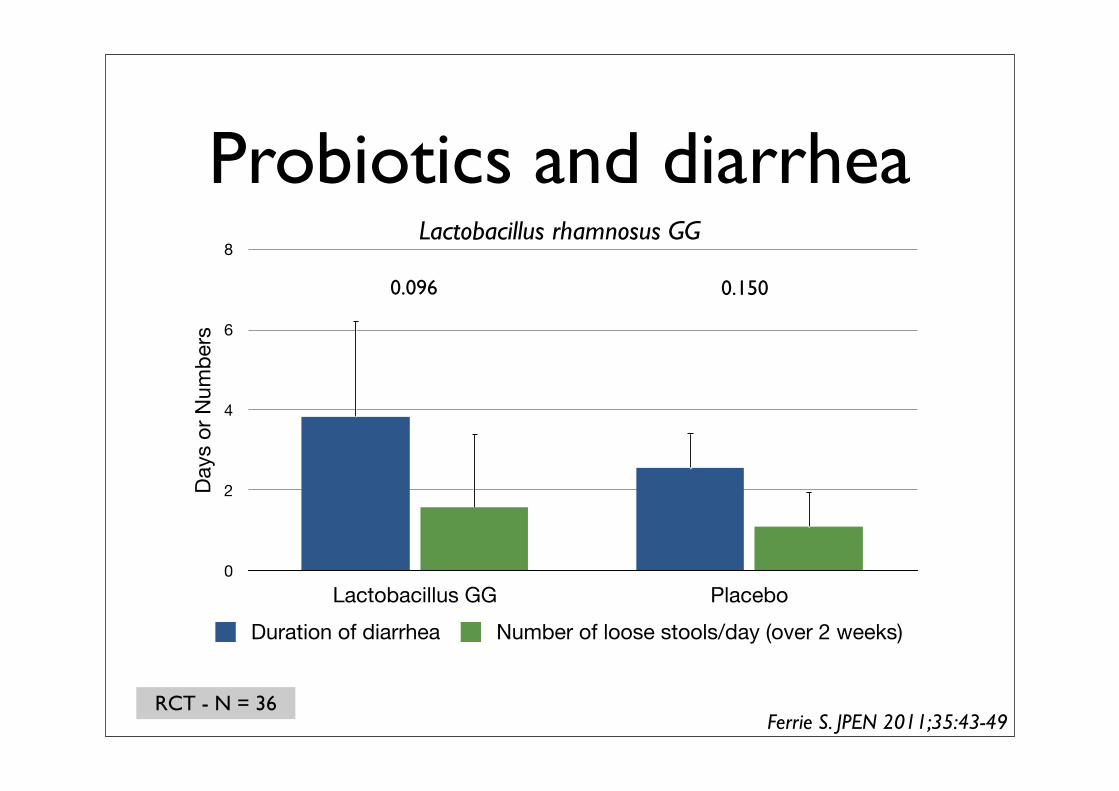
Probiotics and diarrhea
0
2
4
6
8
Lactobacillus GG Placebo
Days
or N
umbe
rs
Duration of diarrhea Number of loose stools/day (over 2 weeks)
Ferrie S. JPEN 2011;35:43-49RCT - N = 36
Lactobacillus rhamnosus GG
0.096 0.150
Only 4 trials (1 abstract) - no difference
Casus GIC-cursusdag Tractus Digestivus
(28 mei 2013) pagina 1 van 4
Casus GIC-cursusdag Tractus digestivus
(28 mei 2013)
Casus vrouw 67 jaar
Citaat uit de status:
Patiënt werd acuut onwel in de auto, direct niet aanspreekbaar. 112 gebeld en partner is begonnen
met reanimeren. Ambulance trof haar aan met fijnmazig VF. Er werd 8-9x gedefibrilleerd voordat
patiënte in XXX ziekenhuis aankwam. Op SEH aldaar persisterend VF. Daar 8x defibrillatie en na
20 min eigen ritme en output. Hierna weer VF waarvoor 1x defibrillatie. Daarna weer ritme en
output. Op ECG STEMI over voorwand. Dexa 1mg/kg gehad, noradrenalinepomp, perfanpomp,
dormicum, KCl, aspegic en heparine gehad.
pH na ROSC was 7.07
Daarna overgeplaatst naar XXX voor PCI. Bij aankomt cathkamer eigen sinusritme, gesedeerd
Stent geplaatst in de LAD. Percutane Coronaire Interventie (PCI)
Dominant systeem: Rechts Verslag: Primaire PCI van mid LAD, zeer verkalkt vat. 1.2 en 1.5 en 2,5 NC ballonen gevolgd door 2,5 x 30 Orsiro. Goed resultaat met TIMI 3 flow. RCA en Cx verkalkt en mild diffuse wandonregelmatigheden
Thuismedicatie:
chloortalidon 25mg 1dd1, metoprolol ter 100mg 1dd1, amlodipine 5mg 1dd1
fosinopril 20mg 1dd1, mirtazapine 30mg 1dd1, symbicort turb 400/12 2dd1
spiriva 18mcg 1dd1
Klinische conditie voor opname:
Patiënt is ADL zelfstandig. De inspanningstolerantie is redelijk. Er is een normaal cognitief
functioneren. Patiënt is in goede voedingstoestand.
Opname ICU:
N: E1 M1 V1tube, gesedeerd, pupillen isocoor en lichtreactief
R: NAG bdz
C: S1S2, geen souffle, perifeer koel
Abd: bolle, soepele buik
Extr: tekenen van veneuze insufficiëntie
Botboor in situ in tibiaplateau rechts
ECG: SR 80/min, neg T in V2 en aVL, geen ST afwijkingen meer
Casus GIC-cursusdag Tractus Digestivus
(28 mei 2013) pagina 2 van 4
Kweken:
Materiaal: uitstrijk SDD rectum
Afgenomen op: 22-04-13
Ontvangen op: 22-04-13
Kweek: 1: +/- 100 kolonies: coliforme gram - staven
2: 15-100 kolonies: groei van gram positieve flora
3: > 1000 kolonies: gisten geisoleerd
4: geen V.R.E. geisoleerd
Antibiogram: 1
Cefotaxim S
Tobramycine S
Ciprofloxacine S
Polymyxine S
Materiaal: uitstrijk SDD keel
Afgenomen op: 22-04-13
Ontvangen op: 22-04-13
Kweek: 1: > 1000 kolonies: groei van gram positieve flora
2: > 1000 kolonies: gisten geisoleerd
3: +/- 100 kolonies: coliforme gram - staven
Antibiogram: 3
Cefotaxim S
Tobramycine S
Ciprofloxacine S
Polymyxine S
Sputumkweek: Pseudomonas aer. Voor alle geteste AB gevoelig
Vraag 1
Wat is bij deze patiënt de rol van translocatie (pro-con)?
Na 2 dagen citaat status:
Abdominaal
Enterale voeding: Fresubin 2Kcal HP 227 ml. Maag retentie 800 ml, nu voor het eerst
bloedbijmenging. Laatste def hedenochtend Totaal gister 125 ml def. Kcal intake gisteren 481 Kcal
Gemiddelde VCO2 over de afgelopen dag 239 ml/min (passend bij een energiebehoefte van 1912
kcal). Eiwit intake 23 g, bij gewenste intake van 92.2 g/dag ( = 1.5g/kg LBM = 61*1.5)
LO: stille, wat bolle wel soepele buik, oogt niet drukpijnlijk
Na 4 dagen X-BOZ:
Conform oudere foto's uitgezette darmlissen zonder evidente tekenen van darmwandverdikkingen.
De duodenum sonde bevindt zich in de maag.
Casus GIC-cursusdag Tractus Digestivus
(28 mei 2013) pagina 3 van 4
Vragen
2. Wat is de rol van de tr dig in het multipel orgaan falen (hoe kan de tr dig falen bij een primair
cardiale ziekte en hoe is vervolgens de interactie tussen de falende tr dig en de overige
organen).
3. Hoe kunnen we dit therapeutisch benaderen?
4. Wat is de pathogenese en de benadering van de hoge tr dig bloeding?
Na 7 dagen citaat status:
Abdominaal
Neostigmine (Prostigmin) 6 ml/uur
Enterale voeding: Fresubin 2Kcal HP 960 ml. Maag retentie 4050 ml Laatste def 26-04Meest
recente blaasdruk 20 mmHg
Kcal intake gisteren 2008 Kcal Gemiddelde VCO2 over de afgelopen dag 233 ml/min (passend bij
een energiebehoefte van 1864 kcal).
Eiwit intake 116 g, bij gewenste intake van 92.2 g/dag ( = 1.5g/kg LBM = 61*1.5)
LO: heel bol en gespannen, diffus drukpijnlijk, geen peristaltiek
CT abdomen:
Onderzoek volgens darmischemie protocol; arteriële scan en porta-veneuze scan na toediening van
oraal water. Geen oud onderzoek ter vergelijking.
Uitgebreide vaatwandcalcificaties in de aorta abdominalis en de origo van de truncus coeliacus en
AMS. Goed contrastaanbod in de aorta en de viscerale vaten. Geen aanwijzingen voor vaatocclusie.
Normale aankleuring van de gastro-intestinale structuren. Geen aanwijzingen voor lucht in de
wanden.
Chirurgische-naad in het kleine bekken bij status na sigmoïdresectie. Prominent aspect van het
coecum en colon transversum met normalisatie van het colon ter hoogte van de flexura lienalis en
colon descendens. Prominente dunnedarmstructuren. Geen evidente kalibersprongen. Geen
aanwijzingen voor interne herniatie.
Homogene lever. Normaal beeld van galblaas en galwegen. Normaal aspect van het pancreas. Normale
milt. Normaal beeld van de nieren. Beiderzijds slank verzamelsysteem.
Geen intra-abdominaal vrij lucht.
Intra-abdominaal vocht perihepatisch en perisplenisch met tevens vocht tussen darmstructuren en
in het kleine bekken. Congestie van vocht in de weke delen.
Pleuravocht beiderzijds en een pneumonie rechts basaal.
Sigmoidoscopie: geen tekenen van ischaemie
Na 10 dagen:
Verslag chirurg: Nu in consult gevraagd ivm fors inotropie afhankelijk in de nacht, vullingsbehoeftig
en oplopende blaasdrukken. Nor nu op 20, buikdruk 23. Bolle, harde en pijnlijke buik, pasteus, rood
in de rechter flank. Kan niet meer onttrokken worden met de CVVH. Hb daling, maar deels vulling.
Passeerde niet wv sinds 2 dagen neostigmine.
OK: subtotale colectomie ivm perforaties bij ischaemie colon na low flow state tijdens reanimatie op
22-4-13
aanleg eindstandig ileostoma
Casus GIC-cursusdag Tractus Digestivus
(28 mei 2013) pagina 4 van 4
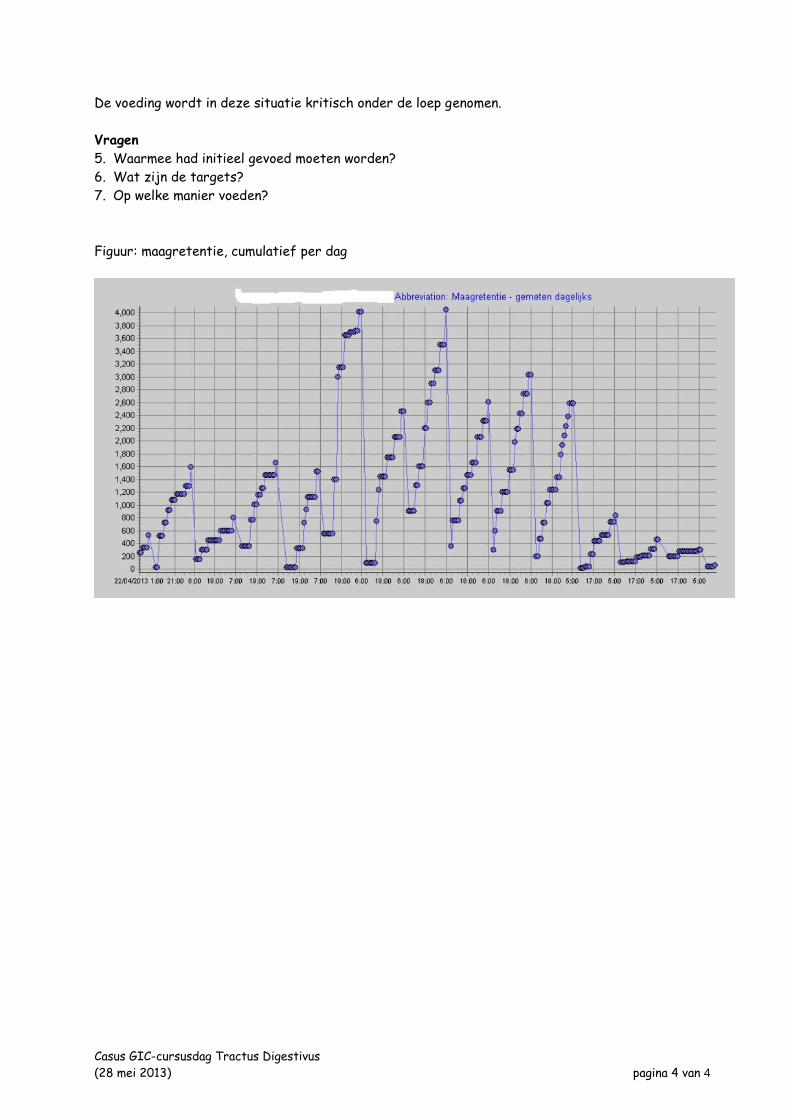
De voeding wordt in deze situatie kritisch onder de loep genomen.
Vragen
5. Waarmee had initieel gevoed moeten worden?
6. Wat zijn de targets?
7. Op welke manier voeden?
Figuur: maagretentie, cumulatief per dag
Top Related