VEGF, TNF-α and 8-isoprostane levels in exhaled breath condensate and serum of patients with lung...
7
Lung Cancer 64 (2009) 219–225 Contents lists available at ScienceDirect Lung Cancer journal homepage: www.elsevier.com/locate/lungcan VEGF, TNF- and 8-isoprostane levels in exhaled breath condensate and serum of patients with lung cancer Eleftherios Dalaveris, Theodora Kerenidi, Alexandra Katsabeki-Katsafli, Theodoros Kiropoulos, Kalliopi Tanou, Konstantinos I. Gourgoulianis, Konstantinos Kostikas ∗ Respiratory Medicine Department, University of Thessaly Medical School, University Hospital of Larissa, Larissa 41110, Greece article info Article history: Received 16 June 2008 Received in revised form 21 August 2008 Accepted 29 August 2008 Keywords: TNF- VEGF 8-Isoprostane Oxidative stress Biomarkers Exhaled breath condensate Lung cancer abstract The aim of the present study was to evaluate the levels of VEGF, 8-isoprostane and TNF- in EBC and serum of patients with primary lung cancer prior to the initiation of any treatment, in order to evaluate their possible diagnostic role. Furthermore, associations between VEGF, 8-isoprostane and TNF- levels in EBC and serum with clinicopathologic factors were investigated. We enrolled 30 patients with lung cancer (mean age 65.2 ± 10.5 years) and 15 age and gender-matched healthy smokers as controls. Serum and EBC were collected before any treatment. TNF-, VEGF and 8- isoprostane levels in EBC and serum were analyzed by an immunoenzymatic method (ELISA). A statistically significant difference was observed between lung cancer patients and the control group regarding the values of TNF-, both in EBC (52.9 ± 5.0 pg/ml vs. 19.4 ± 3.9 pg/ml, p < 0.0001) and serum (44.5 ± 6.3 pg/ml vs. 22.2 ± 4.3 pg/ml, p =0.035). Moreover, EBC VEGF levels were higher in patients with T3–T4 tumor stage compared to T1–T2 (9.3 ± 2.8 pg/ml vs. 2.3 ± 0.7 pg/ml, p = 0.047). A statistically sig- nificant correlation was also observed between serum and EBC values of VEGF (r = 0.52, p = 0.019). In addition, serum levels of VEGF were higher in lung cancer patients than in controls (369.3 ± 55.1 pg/ml vs. 180.5 ± 14.7 pg/ml, p = 0.046). VEGF serum levels were also found higher in patients with advanced stage of disease (IIIB–IV) and distant nodal metastasis (N2–N3). No differences were observed in 8-isoprostane in EBC between lung cancer patients and controls. In contrast, serum 8-isoprostane levels were higher in lung cancer patients compared to controls (24.9 ± 3.6 pg/ml vs. 12.9 ± 1.6 pg/ml, p = 0.027) and were higher in patients with advanced disease. All three biomarkers presented acceptable reproducibility in the EBC on two consecutive days. In conclusion, we have shown that TNF-, VEGF and 8-isoprostane are elevated in the serum of lung cancer patients and increased serum VEGF and 8-isoprostane levels are related to advanced disease. In EBC, increased TNF- levels were observed in lung cancer patients, whereas increased VEGF levels were observed in advanced T-stage. Further longitudinal studies are warranted for the evaluation of the prognostic role of these biomarkers in lung cancer. © 2008 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Lung cancer was the leading cause of cancer death in Europe for 2006 and the third most common form of malignancy, gath- ering 12.1% of the entire number of cancer incidence [1]. Despite the efforts to find new, more sensitive diagnostic tools, able to anticipate the diagnosis of lung cancer, a significant percentage Abbreviations: EBC, exhaled breath condensate; VEGF, vascular endothelial growth factor; TNF-, tumor necrosis factor alpha; ROS, reactive oxygen species; BAL, bronchoalveolar lavage. ∗ Corresponding author. Tel.: +30 6944780616; fax: +30 2410670240. E-mail address: [email protected] (K. Kostikas). of patients still have poor prognosis because of the wide extent of disease during diagnosis. There is currently renewed interest in biological factors that are not only involved in the development of malignant diseases but may also serve as prognostic markers for survival and as predictive signals for the efficacy of a specific therapy [2]. Among these markers, TNF- has emerged from recent stud- ies, as one of the mediators interferes with both antiproliferative and tumorigenic effects [3]. However, the association of this fac- tor with tumor prognosis is not yet clearly defined. Additionally, an interesting line of research is presently directed towards the study of angiogenetic factors, such as vascular endothelial growth factor (VEGF) [4]. Angiogenesis plays an important role in tumor biology, especially in tumor progress and growth of metastasis [5]. Tumor 0169-5002/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.lungcan.2008.08.015
-
Upload
konstantinos -
Category
Documents
-
view
217 -
download
1
Transcript of VEGF, TNF-α and 8-isoprostane levels in exhaled breath condensate and serum of patients with lung...

Vs
EKR
a
ARRA
KTV8OBEL
1
feta
gB
0d
Lung Cancer 64 (2009) 219–225
Contents lists available at ScienceDirect
Lung Cancer
journa l homepage: www.e lsev ier .com/ locate / lungcan
EGF, TNF-� and 8-isoprostane levels in exhaled breath condensate anderum of patients with lung cancer
leftherios Dalaveris, Theodora Kerenidi, Alexandra Katsabeki-Katsafli, Theodoros Kiropoulos,alliopi Tanou, Konstantinos I. Gourgoulianis, Konstantinos Kostikas ∗
espiratory Medicine Department, University of Thessaly Medical School, University Hospital of Larissa, Larissa 41110, Greece
r t i c l e i n f o
rticle history:eceived 16 June 2008eceived in revised form 21 August 2008ccepted 29 August 2008
eywords:NF-�EGF-Isoprostanexidative stressiomarkersxhaled breath condensateung cancer
a b s t r a c t
The aim of the present study was to evaluate the levels of VEGF, 8-isoprostane and TNF-� in EBC andserum of patients with primary lung cancer prior to the initiation of any treatment, in order to evaluatetheir possible diagnostic role. Furthermore, associations between VEGF, 8-isoprostane and TNF-� levelsin EBC and serum with clinicopathologic factors were investigated.
We enrolled 30 patients with lung cancer (mean age 65.2 ± 10.5 years) and 15 age and gender-matchedhealthy smokers as controls. Serum and EBC were collected before any treatment. TNF-�, VEGF and 8-isoprostane levels in EBC and serum were analyzed by an immunoenzymatic method (ELISA).
A statistically significant difference was observed between lung cancer patients and the control groupregarding the values of TNF-�, both in EBC (52.9 ± 5.0 pg/ml vs. 19.4 ± 3.9 pg/ml, p < 0.0001) and serum(44.5 ± 6.3 pg/ml vs. 22.2 ± 4.3 pg/ml, p = 0.035). Moreover, EBC VEGF levels were higher in patients withT3–T4 tumor stage compared to T1–T2 (9.3 ± 2.8 pg/ml vs. 2.3 ± 0.7 pg/ml, p = 0.047). A statistically sig-nificant correlation was also observed between serum and EBC values of VEGF (r = 0.52, p = 0.019). Inaddition, serum levels of VEGF were higher in lung cancer patients than in controls (369.3 ± 55.1 pg/ml vs.180.5 ± 14.7 pg/ml, p = 0.046). VEGF serum levels were also found higher in patients with advanced stageof disease (IIIB–IV) and distant nodal metastasis (N2–N3). No differences were observed in 8-isoprostanein EBC between lung cancer patients and controls. In contrast, serum 8-isoprostane levels were higherin lung cancer patients compared to controls (24.9 ± 3.6 pg/ml vs. 12.9 ± 1.6 pg/ml, p = 0.027) and were
higher in patients with advanced disease. All three biomarkers presented acceptable reproducibility inthe EBC on two consecutive days.In conclusion, we have shown that TNF-�, VEGF and 8-isoprostane are elevated in the serum of lungcancer patients and increased serum VEGF and 8-isoprostane levels are related to advanced disease.In EBC, increased TNF-� levels were observed in lung cancer patients, whereas increased VEGF levelswere observed in advanced T-stage. Further longitudinal studies are warranted for the evaluation of the
omar
oob
prognostic role of these bi
. Introduction
Lung cancer was the leading cause of cancer death in Europe
or 2006 and the third most common form of malignancy, gath-ring 12.1% of the entire number of cancer incidence [1]. Despitehe efforts to find new, more sensitive diagnostic tools, able tonticipate the diagnosis of lung cancer, a significant percentageAbbreviations: EBC, exhaled breath condensate; VEGF, vascular endothelialrowth factor; TNF-�, tumor necrosis factor alpha; ROS, reactive oxygen species;AL, bronchoalveolar lavage.∗ Corresponding author. Tel.: +30 6944780616; fax: +30 2410670240.
E-mail address: [email protected] (K. Kostikas).
oft
iatio(e
169-5002/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.lungcan.2008.08.015
kers in lung cancer.© 2008 Elsevier Ireland Ltd. All rights reserved.
f patients still have poor prognosis because of the wide extentf disease during diagnosis. There is currently renewed interest iniological factors that are not only involved in the developmentf malignant diseases but may also serve as prognostic markersor survival and as predictive signals for the efficacy of a specificherapy [2].
Among these markers, TNF-� has emerged from recent stud-es, as one of the mediators interferes with both antiproliferativend tumorigenic effects [3]. However, the association of this fac-
or with tumor prognosis is not yet clearly defined. Additionally, annteresting line of research is presently directed towards the studyf angiogenetic factors, such as vascular endothelial growth factorVEGF) [4]. Angiogenesis plays an important role in tumor biology,specially in tumor progress and growth of metastasis [5]. Tumor
2 g Canc
cusegltos[
ilttbwdbcmsaniptaDe
8poca
2
2
lDbsybmtaCphpac
2
dcG
amfna1ia[p3mc9t
2
eifcMu0ocCtPfa
2m
8cctt
2
tsbr<mdSS
3
20 E. Dalaveris et al. / Lun
ells themselves, are able to release many microangiogenetic stim-lating substances [6]. Furthermore, various markers of oxidativetress have been reported in the past to interfere with carcinogen-sis [7,8]. We have recently shown that serum vascular endothelialrowth factor is related to systemic oxidative stress in patients withung cancer [9]. 8-Isoprostane is a stable prostaglandin-like producthat is formed from arachidonic acid by the non enzymatic actionf reactive oxygen species and it is considered a marker of oxidativetress, though its exact role in lung cancer biology is still not clear10].
Exhaled breath condensate (EBC) represents a totally non-nvasive method for the evaluation of airways pathology duringung diseases [11], and recently considerable burden of informa-ion has accumulated and efforts for the standardization [12] andhe assessment of normal values of biomarkers in EBC [13] haveeen presented in the literature. Despite its advantages and itsidespread use in other lung disorders [12], the role of EBC in theiagnosis and the evaluation of patients with lung cancer has noteen widely evaluated, as the major part of biomarkers in lung can-er have been determined until nowadays in samples obtained withore invasive techniques, such as induced sputum, bronchial biop-
ies and bronchoalveolar lavage (BAL). However, EBC represents anttractive means of airway sampling since it represents a totallyon-invasive and easily repeatable method. Studies have shown
ncreased cytokine levels in the EBC of non-small cell lung canceratients, such as IL-6 [14] and TNF-�, IL-2 and leptin [15]. Addi-ional studies in EBC have shown increased levels of endothelin-1,mitogenic factor [16], as well as microsatellite alterations in theNA of lung cancer patients [17], providing a rationale for furthervaluation of EBC in lung cancer.
The aim of the present study was to evaluate the levels of VEGF,-isoprostane and TNF-� in the EBC and serum of patients withrimary lung cancer prior to the initiation of any treatment, inrder to evaluate their possible diagnostic role. Furthermore, asso-iations between VEGF, 8-isoprostane and TNF-� levels in the EBCnd serum with clinicopathologic factors were investigated.
. Materials and methods
.1. Patients
We enrolled prospectively 30 consecutive patients with histo-ogical evidence of primary lung cancer admitted to the Respiratoryepartment of the Medical School of University of Thessalyetween 2005 and 2007. Twenty-four of the patients were currentmokers and six were ex-smokers (mean ± S.E.M. 52 ± 14 pack-ears). For all patients, a diagnosis of lung cancer was confirmedy histologic examinations of biopsy and/or cytology speci-ens obtained during fiberoptic bronchoscopy or with CT-guided
ransthoracic needle aspiration biopsy. Stage was determinedccording to the staging system of American Joint Committee onancer (AJCC) TNM classification [18]. All serum and EBC sam-les were obtained prior to the initiation of any treatment. Fifteenealthy smokers, age and sex matched with the lung canceratients served as controls. The Ethics committee of our hospitalpproved this study and all subjects provided written informedonsent.
.2. Exhaled breath condensate and blood sample collection
Exhaled breath condensate was collected by means of a con-enser which allowed the non-invasive collection of non gaseousomponents of the expiratory air (Ecoscreen, Jaeger, Wurzburg,ermany). Patients came in the morning and, after supervised
�(oa
er 64 (2009) 219–225
bstinence from smoking for two hours, were asked to rinse theirouth with distilled water. Consequently, they were asked to per-
orm tidal breathing 15 min through a mouthpiece and a two wayon-rebreathing valve which also served as a saliva trap wearingnose clip. All patients were instructed to swallow saliva. At leastml of EBC was collected and transferred to Eppendorf tubes and
mmediately frozen at −80 ◦C. All EBC collections were performedccording to the ERS/ATS Task Force on exhaled breath condensate12]. Finally, fasting venous blood samples were collected from bothatients and healthy individuals and subsequently centrifuged at000 × g for 10 min at 4 ◦C. The supernatant was transferred intoicrotubes and frozen at −80 ◦C until use. All EBC and blood sample
ollections were performed early in the morning (between 8:00 and:00 a.m.) in order to avoid any influences of the circadian rhythmo the measured biomarkers.
.3. Measurements of TNF-˛, VEGF and 8-isoprostane
TNF-� levels was measured with a commercially availablenzyme-immunosorbent assay kit (Biosource Europe S.A.) accord-ng to the manufacturer’s protocol. The lower limit of detectionor TNF-� was 3 pg/ml. VEGF levels were measured with commer-ially available enzyme-immunosorbent assay kits (R&D Systems,inneapolis, MN, USA, Catalog No. DVE00), according to the man-
facturers’ protocols. The lower limit of detection for VEGF was.9 pg/ml. No purification was performed for the measurementsf TNF-� and VEGF. 8-Isoprostane levels were measured with aommercially available enzyme-immunosorbent assay kit (Caymanhemical, Ann Arbor, MI, USA) according to the manufacturer’s pro-ocol. The lower limit of detection for 8-isoprostane was 2.7 pg/ml.urification of samples for 8-isoprostane measurements were per-ormed according to the manufacturer’s protocol. The intra-assaynd inter-assay variabilities are ≤10%.
.4. Reproducibility of TNF-˛, VEGF and 8-isoprostaneeasurements in EBC
The reproducibility of the measurements of TNF-�, VEGF and-isoprostane in EBC was checked on EBC samples obtained on twoonsecutive days in a total of 12 subjects (8 patients with lung can-er and 4 controls). All subjects were on stable condition betweenhe two collections and both collections were performed early inhe morning (between 8:00 and 9:00 a.m.).
.5. Statistical analysis
Data are expressed as means ± S.E.M., unless otherwise men-ioned. Comparisons of levels of the three biomarkers either inerum or in EBC were compared using unpaired t-tests. Correlationsetween EBC and serum levels were evaluated with Pearson’s cor-elation coefficient. Statistical significance was defined as p values0.05. For the evaluation of the reproducibility of the measure-ents of TNF-�, VEGF and 8-isoprostane in EBC on two consecutive
ays we have used the method described by Bland and Altman [19].tatistical analysis was made using Graph Pad Prism 5 (Graph Padoftware Inc., La Jolla, CA, USA).
. Results
Patients’ characteristics are summarized in Table 1. Both TNF-and 8-isoprostane were detected in all EBC and serum samples
Table 2); VEGF was detected in all serum samples but only in 20ut of 30 lung cancer patients and in 7 out of 15 healthy individu-ls.

E. Dalaveris et al. / Lung Cancer 64 (2009) 219–225 221
Table 1Demographic characteristics of lung cancer patients
Lung cancer
n 30Age (years) 65.2 ± 10.5Gender (male/female) 27/3Smoking (current/ex) 24/6Patients with NSCLC 22
Adenocarcinoma 6Squamous cell carcinoma 12Unclassified NSCLC 4
Stage NSCLCStage I 9Stage II 1Stage III 7Stage IV 5
Patients with SCLC 8Stage III 6Stage IV 2
TumorT1 2T2 15T3 1T4 12
Lymph nodesN0 13N1 1N2 13N3 5
MetastasisM0 23
Ds
3
cTppb
3
ci(
l
TEa
E
S
Dn
F
1dt(twsr
V
3
M1 7
ata are presented as mean ± S.E.M. NSCLC: non-small cell lung cancer; and SCLC:mall cell lung cancer.
.1. EBC and serum levels of TNF-˛
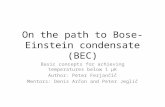
A statistically significant difference was observed between lungancer patients and the control group, regarding the values ofNF-� measured both in EBC (52.9 ± 5.0 pg/ml vs. 19.4 ± 3.9 pg/ml,< 0.001) and serum (44.5 ± 6.3 pg/ml vs. 22.2 ± 4.3 pg/ml,= 0.035) (Fig. 1A and B). No significant correlations were observedetween TNF-� levels and other clinicopathological parameters.
.2. EBC and serum levels of VEGF
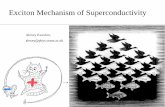
In EBC, VEGF levels of lung cancer patients did not differ signifi-
antly from controls. However, higher levels of VEGF were foundn patients with T3–T4 tumor stage than in those with T1–T29.3 ± 2.8 pg/ml vs. 2.3 ± 0.7 pg/ml, respectively; p = 0.047) (Fig. 2A).Serum levels of VEGF were found significantly higher inung cancer patients than in controls (369.3 ± 55.1 pg/ml vs.
able 2BC and serum levels of TNF-�, VEGF and 8-isoprostane in patients with lung cancernd healthy controls
Lung cancer Controls p value
BCTNF-� (pg/ml) 52.9 ± 5.0 19.48 ± 3.9 <0.0001VEGF (pg/ml) 5.8 ± 1.1 4.3 ± 1.2 0.5238-Isoprostane (pg/ml) 6.26 ± 0.8 6.11 ± 0.7 0.909
erumTNF-� (pg/ml) 44.6 ± 6.3 22.2 ± 4.3 0.035VEGF (pg/ml) 369.3 ± 55.2 180.5 ± 14.7 0.0278-Isoprostane (pg/ml) 24.9 ± 3.6 12.9 ± 1.6 0.027
ata are presented as mean ± S.E.M. EBC: exhaled breath condensate; TNF-�: tumorecrosis factor alpha; and VEGF: vascular endothelial growth factor.
laoo
cvped
3m
sr(d
ig. 1. TNF-� levels in lung cancer patients and controls (A) in serum and (B) in EBC.
80.5 ± 14.7 pg/ml, p = 0.046) (Fig. 2B). Furthermore, patients withistant nodal metastasis (N2–N3) presented higher VEGF concen-rations than those without or initial nodal metastasis (N0–N1)495.9 ± 96.4 pg/ml vs. 242.6 ± 31.8 pg/ml, p = 0.018) (Fig. 2C). Addi-ionally, higher serum levels of VEGF were measured in patientsith advanced stage (IIIB–IV) compared to those with locoregional
tage (I–IIIA) of disease (476.8 ± 91.9 pg/ml vs. 246.4 ± 35.1 pg/ml,espectively; p = 0.034) (Fig. 2D).
Finally, a statistically significant correlation was found betweenEGF levels in EBC and serum (r = 0.52, p = 0.019) (Fig. 2E).
.3. EBC and serum levels of 8-isoprostane
We did not observe any significant differences regarding theevels of 8-isoprostane in EBC between patients with lung cancernd controls. Additionally, no significant differences in the levelsf 8-isoprostane related to clinicopathological parameters werebserved.
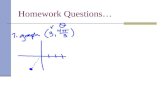
Serum concentrations of 8-isoprostane were higher in lungancer patients than in healthy individuals (24.9 ± 3.6 pg/mls.12.9 ± 1.6 pg/ml, respectively; p = 0.027) (Fig. 3A). In addition,atients with advanced stage (IIIB–IV) showed higher serum lev-ls of 8-isoprostane, than those with locoregional stage (I–IIIA) ofisease (32 ± 5.8 pg/ml vs. 16.8 ± 2.6 pg/ml, p = 0.032) (Fig. 3B).
.4. Reproducibility of TNF-˛, VEGF and 8-isoprostaneeasurements in EBC
The measurements of TNF-�, VEGF and 8-isoprostane in EBCamples collected on two consecutive days presented acceptableeproducibility. The mean difference with limits of agreement±2S.D.) for EBC TNF-� was 0.69 (−5.16 to 6.55) (Fig. 4A). The meanifference with limits of agreement (±2S.D.) for EBC VEGF was

222 E. Dalaveris et al. / Lung Cancer 64 (2009) 219–225
Fig. 2. (A) Exhaled breath condensate levels of VEGF in patients with T1–T2 stage and patients with T3–T4 stage; (B) Serum levels of VEGF in lung cancer patients comparedto controls; (C) Serum levels of VEGF in patients with distant nodal metastasis (N2–N3) and in those without or initial nodal metastasis (N0–N1); (D) Serum levels of VEGF inp f dise(
−aFa
4
ali�pwct
ci
satmhlsc
atients with advanced stage (IIIB–IV) and in those with locoregional stage (I–IIIA) or = 0.52, p = 0.019).
0.18 (−0.74 to 0.38) (Fig. 4B). The mean difference with limits ofgreement (±2S.D.) for EBC 8-isoprostane was 0.05 (−0.93 to 1.04)ig. 4C). All values were within the limits of agreement in the Blandnd Altman plots.
. Discussion
In the present study we have evaluated the levels of TNF-�, VEGFnd 8-isoprostane in the EBC and serum of patients with primaryung cancer. We have shown that all three biomarkers are elevatedn the serum of lung cancer patients, whereas in the EBC only TNF-
was elevated compared to controls, and EBC VEGF was higher inatients with locally advanced T-stage. In contrast, no differencesere observed in EBC 8-isoprostane levels in patients with lung
ancer. This is the first study to our knowledge that has assessedhe levels of VEGF and 8-isoprostane in the EBC of patients with lung
t[bpi
ase; (E) Correlation between serum and EBC values of VEGF in lung cancer patients
ancer, in an attempt to evaluate their possible use as biomarkersn patients with lung cancer.
Recent in vitro and in vivo studies have demonstrated a widepectrum of biologic activities of cytokines in the pathogenesisnd progression of malignancy. TNF-� is a significant mediatorhat presents both antiproliferative and tumorigenic effects in
alignant tumors, including lung cancer [3]. In this study, weave observed increased concentrations of TNF-� in the EBC of
ung cancer patients compared to healthy controls. This findingupports a possible local production of this cytokine in lung can-er, which is likely to be mediated by lymphomononuclear cells
hat infiltrate the tumor or by the malignant cells themselves20]. EBC levels of TNF-� measured in our study are compara-le to those observed by previous investigators in lung canceratients [14,21]. Furthermore, serum TNF-� levels were elevatedn lung cancer patients, in agreement with previously observed

E. Dalaveris et al. / Lung Canc
Fh(
h[
saSpimsb[ibMccdialcs
Voecgfa
irplss
lprwadfuated in the exhaled air or serum of lung cancer patients, despitethe fact that previous authors have reported enhanced lipid per-oxidation in tumor tissues [10,36]. In this study we have shownfor the first time that 8-isoprostane was detectable in EBC samples
ig. 3. (A) Serum concentration of 8-isoprostane in lung cancer patients and inealthy controls; (B) Serum levels of 8-isoprostane in patients with advanced stageIIIB–IV) and in those with locoregional stage (I–IIIA) of disease.
igher concentrations of this biomarker both in vitro and in vivo3,21].
In this study we have evaluated the levels of VEGF in the EBC anderum of lung cancer patients. VEGF is a potent angiogenic medi-tor with important effects on tumor growth and metastasis [4].ystemic hypoxemia, induces elevation of serum VEGF especially inatients with lung cancer [22]. It has also been reported that VEGF
s associated with increased tumor vessel density, development ofalignant effusions and metastasis, as well as with cancer progno-
is [22,23]. VEGF has been previously measured in serum, tissue,ronchoalveolar lavage and pleural fluid of lung cancer patients24–27], but, to the best of our knowledge, it has never measuredn the EBC of lung cancer patients. Our data show that VEGF cane detected in the majority of EBC samples in lung cancer patients.oreover, a significant increase was observed in EBC VEGF con-
entrations of patients with advanced tumor stage (T3–T4) diseaseompared to patients with T1–T2, suggesting a possible local pro-uction of VEGF. This finding is in accordance with a previous study
n EBC that observed local production of endothelin-1, anotherngiogenic factor, in lung cancer patients [16]. This association withocal tumor extension may indicate a possible prognostic signifi-ance of EBC VEGF that needs to be further evaluated in longitudinaltudies.
Moreover, we have found an increased concentration of serumEGF in lung cancer patients than in controls, confirming previousbservations [6,9,28,29]. Our observation that serum VEGF lev-ls are higher in patients with advanced stage of disease (IIIB–IV)
omes in agreement with previous authors [30,31] who have sug-ested a strong association of VEGF with tumor progression. Weurther observed a positive association between circulating VEGFnd distant nodal metastasis (N2–N3), supporting previous find-Fipal
er 64 (2009) 219–225 223
ngs that VEGF correlates with up regulated lymphangiogenesis andegional nodal metastasis [32]. An interesting novel finding of theresent study is the statistically significant correlation between the
evels of VEGF in EBC and serum. The associations of both EBC anderum VEGF with tumor extension may reflect concurrent local andystemic role of this mediator in tumor progression.
In a previous study we have shown a significant positive corre-ation between circulating VEGF and systemic oxidative stress inatients with lung cancer [9]. In an attempt to evaluate the localelation between VEGF and oxidative stress in the present studye measured 8-isoprostane, a stable end-product of arachidonic
cid metabolism that is considered a biomarker of lipid peroxi-ation [33]. Elevated EBC 8-isoprostane concentrations have beenound in several lung disorders [13,34,35], yet it had not been eval-
ig. 4. Assessment of reproducibility of EBC measurements on two consecutive daysn 12 subjects (8 with lung cancer and 4 controls) presented in Bland and Altmanlots (differences against mean values, presented in pg/ml) for: (A) TNF-�, (B) VEGFnd (C) 8-isoprostane. Dotted lines represent the mean difference value and theimits of agreement (±2S.D.).

2 g Canc
oisiEtctfppmfoca
c(isnono
ipirFnaofsasnl
iaalitc
C
ot
A
Os
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
24 E. Dalaveris et al. / Lun
f lung cancer patients. However, 8-isoprostane was not elevatedn the EBC of lung cancer patients compared to controls, and noignificant associations were observed between its levels and clin-copathological parameters. Based on our findings we suggest thatBC 8-isoprostane may not represent a significant biomarker forhe evaluation of lung cancer patients. The absence of a signifi-ant correlation between EBC 8-isoprostane and VEGF, in contrasto our previous observations in serum [9], may reflect the dif-erent aspects of oxidative stress that have been assessed. In theresent study we have evaluated 8-isoprostane, a biomarker of lipideroxidation whereas in our previous study we used a universaleasurement of total hydroperoxides [9]. That method was not
easible in EBC, thus we evaluated 8-isoprostane, a well-establishedxidative stress biomarker in EBC. Further studies are needed to elu-idate the possible local mechanisms connecting oxidative stressnd VEGF in lung cancer patients.
In contrast, serum 8-isoprostane levels were higher in lung can-er patients compared to controls. Interestingly, advanced stageIIIB–IV) was associated with even higher serum levels of 8-soprostane. The latter finding is in accordance with a previoustudy reporting increased oxidative stress production in advancedon-small cell lung cancer [37]. Our results suggest a possible rolef serum 8-isoprostane as a biomarker of advanced disease, thateeds to be prospectively evaluated in long-term survival studiesf patients with lung cancer.
The present study presents some limitations. Despite the non-nvasive nature and the wide use of EBC in clinical research, itsossible application in clinical practice requires further standard-
zation [12]. However, in the present study we have used all theecommendations provided by the recent ERS/ATS Task Force [12].urthermore, the fact that VEGF was detected in the majority butot in all EBC samples of lung cancer patients and controls does notllow for safe conclusions on this biomarker, and further refinementf current techniques with lower limits of detection is necessaryor its proper evaluation. Finally, this is a preliminary observationaltudy for the evaluation of TNF-�, VEGF and 8-isoprostane in EBCnd serum as possible biomarkers for the diagnosis and the clas-ification of the extent of disease. Further longitudinal studies areeeded for the evaluation of their prognostic value in patients with
ung cancer.In conclusion, we have shown that TNF-�, VEGF and 8-
soprostane are elevated in the serum of lung cancer patientsnd increased serum VEGF and 8-isoprostane levels are related todvanced disease. In EBC, increased TNF-� levels were observed inung cancer patients, whereas increased VEGF levels were observedn advanced T-stage. Further longitudinal studies are warranted forhe evaluation of the prognostic role of these biomarkers in lungancer.
onflict of interest
All authors disclose any financial or personal relationships withther people or organizations that could inappropriately influencehe present study.
cknowledgements
The authors wish to thank Miss Irene Tsilioni and Miss Smaragdaikonomidi for their assistance in the handling of serum and EBC
amples.
eferences
[1] Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of thecancer incidence and mortality in Europe in 2006. Ann Oncol 2007;18:581–92.
[
[
er 64 (2009) 219–225
[2] Kaminska J, Kowalska M, Kotowicz B, Fuksiewicz M, Glogowski M, Wojcik E, etal. Pretreatment serum levels of cytokines and cytokine receptors in patientswith non-small cell lung cancer, and correlations with clinicopathologicalfeatures and prognosis. M-CSF—an independent prognostic factor. Oncology2006;70:115–25.
[3] Boldrini L, Calcinai A, Samaritani E, Pistolesi F, Mussi A, Lucchi M, et al. Tumournecrosis factor-alpha and transforming growth factor-beta are significantlyassociated with better prognosis in non-small cell lung carcinoma: puta-tive relation with BCL-2-mediated neovascularization. Br J Cancer 2000;83:480–6.
[4] Papaioannou AI, Kostikas K, Kollia P, Gourgoulianis KI. Clinical implicationsfor vascular endothelial growth factor in the lung: friend or foe? Respir Res2006;7:128.
[5] Takigawa N, Segawa Y, Fujimoto N, Hotta K, Eguchi K. Elevated vascular endothe-lial growth factor levels in sera of patients with lung cancer. Anticancer Res1998;18:1251–4.
[6] Tas F, Duranyildiz D, Oguz H, Camlica H, Yasasever V, Topuz E. Serum vascularendothelial growth factor (VEGF) and interleukin-8 (IL-8) levels in small celllung cancer. Cancer Invest 2006;24:492–6.
[7] Chung-man Ho J, Zheng S, Comhair SA, Farver C, Erzurum SC. Differentialexpression of manganese superoxide dismutase and catalase in lung cancer.Cancer Res 2001;61:8578–85.
[8] Gromadzinska J, Wasowicz W. The role of reactive oxygen species in the devel-opment of malignancies. Int J Occup Med Environ Health 2000;13:233–45.
[9] Katsabeki-Katsafli A, Kerenidi T, Kostikas K, Dalaveris E, Kiropoulos TS, Gogou E,et al. Serum vascular endothelial growth factor is related to systemic oxidativestress in patients with lung cancer. Lung Cancer 2008;60:271–6.
10] Zieba M, Nowak D, Suwalski M, Piasecka G, Grzelewska-Rzymowska I, TyminskaK, et al. Enhanced lipid peroxidation in cancer tissue homogenates in non-smallcell lung cancer. Monaldi Arch Chest Dis 2001;56:110–4.
11] Kharitonov SA, Barnes PJ. Exhaled markers of pulmonary disease. Am J RespirCrit Care Med 2001;163:1693–722.
12] Horvath I, Hunt J, Barnes PJ, Alving K, Antczak A, Baraldi E, et al. Exhaled breathcondensate: methodological recommendations and unresolved questions. EurRespir J 2005;26:523–48.
13] Koutsokera A, Loukides S, Gourgoulianis KI, Kostikas K. Biomarkers in theexhaled breath condensate of healthy adults: mapping the path towards refer-ence values. Curr Med Chem 2008;15:620–30.
14] Carpagnano GE, Resta O, Foschino-Barbaro MP, Gramiccioni E, Carpagnano F.Interleukin-6 is increased in breath condensate of patients with non-small celllung cancer. Int J Biol Markers 2002;17:141–5.
15] Carpagnano GE, Spanevello A, Curci C, Salerno F, Palladino GP, Resta O, et al. IL-2,TNF-alpha, and leptin: local versus systemic concentrations in NSCLC patients.Oncol Res 2007;16:375–81.
16] Carpagnano GE, Foschino-Barbaro MP, Resta O, Gramiccioni E, Carpagnano F.Endothelin-1 is increased in the breath condensate of patients with non-small-cell lung cancer. Oncology 2004;66:180–4.
17] Carpagnano GE, Foschino-Barbaro MP, Spanevello A, Resta O, CarpagnanoF, Mule G, et al. 3p Microsatellite signature in exhaled breath condensateand tumor tissue of patients with lung cancer. Am J Respir Crit Care Med2008;177:337–41.
18] Carpagnano GE, Foschino-Barbaro MP, Mule G, Resta O, Tommasi S, Mangia A,et al. 3p Microsatellite alterations in exhaled breath condensate from patientswith non-small cell lung cancer. Am J Respir Crit Care Med 2005;172:738–44.
19] Bland JM, Altman DG. Statistical methods for assessing agreement between twomethods of clinical measurement. Lancet 1986;1:307–10.
20] Mantovani G, Maccio A, Pisano M, Versace R, Lai P, Esu S, et al. Tumor-associatedlympho-monocytes from neoplastic effusions are immunologically defective incomparison with patient autologous PBMCs but are capable of releasing highamounts of various cytokines. Int J Cancer 1997;71:724–31.
21] De Vita F, Orditura M, Auriemma A, Infusino S, Catalano G. Serum concentrationsof proinflammatory cytokines in advanced non small cell lung cancer patients.J Exp Clin Cancer Res 1998;17:413–7.
22] Matsuyama W, Hashiguchi T, Mizoguchi A, Iwami F, Kawabata M, Arimura K, etal. Serum levels of vascular endothelial growth factor dependent on the stageprogression of lung cancer. Chest 2000;118:948–51.
23] Volm M, Koomagi R, Mattern J. PD-ECGF, bFGF, and VEGF expression in non-small cell lung carcinomas and their association with lymph node metastasis.Anticancer Res 1999;19:651–5.
24] Beinert T, Binder D, Oehm C, Ziemer S, Priem F, Schweigert M, et al. Increasedlevels of vascular endothelial growth factor in bronchoalveolar lavage ofpatients with bronchial carcinoma effect of tumour activity and oxidative stressdue to radio-chemotherapy? Eur J Med Res 1999;4:328–34.
25] Brattstrom D, Bergqvist M, Hesselius P, Larsson A, Lamberg K, Wernlund J, et al.Elevated preoperative serum levels of angiogenic cytokines correlate to largerprimary tumours and poorer survival in non-small cell lung cancer patients.Lung Cancer 2002;37:57–63.
26] Cheng D, Rodriguez RM, Perkett EA, Rogers J, Bienvenu G, Lappalainen U, et al.Vascular endothelial growth factor in pleural fluid. Chest 1999;116:760–5.
27] Saji H, Nakamura H, Awut I, Kawasaki N, Hagiwara M, Ogata A, et al. Significanceof expression of TGF-beta in pulmonary metastasis in non-small cell lung cancertissues. Ann Thorac Cardiovasc Surg 2003;9:295–300.
28] Bremnes RM, Camps C, Sirera R. Angiogenesis in non-small cell lung cancer:the prognostic impact of neoangiogenesis and the cytokines VEGF and bFGF intumours and blood. Lung Cancer 2006;51:143–58.

g Canc
[
[
[
[
[
[
[
[
content of lipid peroxidation products in lung cancer tissue and pulmonary
E. Dalaveris et al. / Lun
29] Brattstrom D, Bergqvist M, Hesselius P, Larsson A, Wagenius G, Brodin O. SerumVEGF and bFGF adds prognostic information in patients with normal plateletcounts when sampled before, during and after treatment for locally advancednon-small cell lung cancer. Lung Cancer 2004;43:55–62.
30] Tas F, Duranyildiz D, Oguz H, Camlica H, Yasasever V, Topuz E. Serum vascularendothelial growth factor (VEGF) and bcl-2 levels in advanced stage non-smallcell lung cancer. Cancer Invest 2006;24:576–80.
31] Kaya A, Ciledag A, Gulbay BE, Poyraz BM, Celik G, Sen E, et al. The prognosticsignificance of vascular endothelial growth factor levels in sera of non-small
cell lung cancer patients. Respir Med 2004;98:632–6.32] Nagy JA, Vasile E, Feng D, Sundberg C, Brown LF, Detmar MJ, et al. Vascularpermeability factor/vascular endothelial growth factor induces lymphangio-genesis as well as angiogenesis. J Exp Med 2002;196:1497–506.
33] Baraldi E, Ghiro L, Piovan V, Carraro S, Ciabattoni G, Barnes PJ, et al. Increasedexhaled 8-isoprostane in childhood asthma. Chest 2003;124:25–31.
[
er 64 (2009) 219–225 225
34] Kostikas K, Papatheodorou G, Psathakis K, Panagou P, Loukides S. Oxida-tive stress in expired breath condensate of patients with COPD. Chest2003;124:1373–80.
35] Montuschi P, Corradi M, Ciabattoni G, Nightingale J, Kharitonov SA, Barnes PJ.Increased 8-isoprostane, a marker of oxidative stress, in exhaled condensate ofasthma patients. Am J Respir Crit Care Med 1999;160:216–20.
36] Zieba M, Suwalski M, Kwiatkowska S, Piasecka G, Grzelewska-RzymowskaI, Stolarek R, et al. Comparison of hydrogen peroxide generation and the
parenchyma. Respir Med 2000;94:800–5.37] de Castro J, Hernandez-Hernandez A, Rodriguez MC, Llanillo M, Sanchez-Yague
J. Comparison of changes in erythrocyte and platelet fatty acid compositionand protein oxidation in advanced non-small cell lung cancer. Cancer Invest2006;24:339–45.