
Use of β2 microglobulin to diagnose tubulo-interstitial renal lesions in children
8
Kidney International, Vol. 30 (1986), pp. 91—98 Use of /32 microglobulin to diagnose tubulo-.interstitial renal lesions in children RONALD J. PORTMAN, JOHN M. KI5SANE, and ALAN M. ROBSON, with the technical assistance of LINDA J. PETERSON and ANNE RICHARDSON From the Edward Mallinckrodt Department of Pediatrics and the Department of Pathology, Washington University School of Medicine and the Renal Division, St. Louis Children's Hospital, St. Louis, Missouri, USA Use of 132 microglobulin to diagnose tubulo-interstitial renal lesions in children. Fractional excretion (FE) of 132 microglobulin (f32M) was studied in children with glomerular (N 114), tubular (N 50) or other (N = 18) renal diseases. FE-f32M (normal C 0.36%) was signifi- cantly (P cc 0.001) lower in glomerular diseases (mean 0.104%) than in tubular lesions (mean 4.27%). Unexpectedly, several patients with glomerular disease were found to have increased values for FE-f32M. To determine whether this was due to a tubular component in a primary glomerular disease process, FE-132M was measured in 30 children with various glomerulopathies who underwent renal biopsy. Thirteen of these patients had tubulo-interstitial lesions in addition to their glomer- ular disease. FE-/32M in these patients averaged 3.76% (range 0.14 to 44.6%); only two results were normal. Mean FE-thM in the 17 patients without biopsy evidence of tubulo-interstitial disease was 0.063% (range 0.02 to 0.34%); all values were in the normal range. The types of glomerular diseases in the two groups of patients were similar. Patients with a glomerular lesion complicated by tubulo-interstitial lesions had a poorer prognosis than did those with a pure glomerular disease. The high incidence of tubulo-interstitial lesions in patients with glomerular diseases was unexpected. Our data demonstrates that FE-thM repre- sents a reliable non-invasive method to diagnose such involvement. Measurements of f32M also provide a convenient method to follow the course and response to treatment of renal tubular injury. j32-mieroglobulin (Ø2M), a protein with a molecular wt of 11,800 daltons, is present on the cell surface of most nucleated cells [I] as the small subunit of HLA class I antigens [2]. Measurable concentrations of the protein are present in most biologic fluids [3]. Levels in the serum reflect both the produc- tion and excretion rates of the protein. Under most conditions, production rates and serum concentrations of f32M are remark- ably stable, although increased values may be seen with malig- nancies [4, 51, in infections [6], and with certain immunologic disorders [7]. Since the kidney represents the major excretory pathway for the protein, alterations in serum Ø2M concentra- tions most often result from changes in the level of renal function. Indeed, it has been suggested that changes in the serum level of thM may be a better indicator of alteration in glomerular filtration rate (GFR) than equivalent levels of creat- mine [8]. Received for publication June 10, 1985, and in revised form December 16, 1985 © 1986 by the International Society of Nephrology 91 The removel of 2M from the serum is primarly by glomerular filtration although some peritubular uptake of the protein may also occur [91. The glomerular sieving coefficient for /32M exceeds 0.8 [10] so that large quantities of the protein are filtered each day. More than 99.9% of the filtered protein is reabsorbed and catabolized by the proximal convoluted tubule. Consequently, normal urine contains low concentnstions of f32M—typically less than 360 fkg/liter [11], except in the neo- nate. The urinary levels of f32M peak by the fifth day of life and show a gradual decline until normal adult values are reached by three months of age [12]. No tubular maximum (Tm) for human f32M reabsorption has been found [9] so that the filtered load of 2M has little, if any, effect on the urinary loss of this protein. Thus, most studies suggest that the urinary excretion of 132M is determined primarily by proximal tubular function. Tubular damage secondary to ischemia [131 and to a variety of toxins [14] and drugs [15—19] results in increased urinary levels of2M. The present study was undertaken to assess the clinical usefulness of /32M determinations in diagnosing tubular involve- ment in a wide variety of renal diseases in children. We investigated whether this noninvasive test could be helpful in separating tubular from glomerular diseases and in following the course and treatment of patients with tubular diseases. Methods One hundred and eighty-two children whose ages ranged from one to nineteen years and who had a variety of renal diseases (Table 1) were studied. The diagnosis was established by renal biopsy in those patients where it could not be estab- lished from clinical and laboratory data. Patients receiving known nephrotoxic drugs such as aminoglycosides [17], methieillin [18], methotrexate [19], those exposed to heavy metals [14], those receiving parental hyperalimentation [20] and those with active urinary tract infections [21, 22] or sepsis [231 were excluded from the study since the renal handling of p2M has been shown to be modified in these conditions. Patients receiving immunosuppressive agents were included in the study, These agents are not known to alter the tubular handling of f32M, although they can cause a reduction in serum levels by decreasing production [24]. Several of the patients were studied serially so that there were 241 observations on the 182 patients. Concentrations of $2M in serum and urine were measured in 172 of these children at the time that GFR was measured by
Transcript of Use of β2 microglobulin to diagnose tubulo-interstitial renal lesions in children

Kidney International, Vol. 30 (1986), pp. 91—98
Use of /32 microglobulin to diagnose tubulo-.interstitial renallesions in children
RONALD J. PORTMAN, JOHN M. KI5SANE, and ALAN M. ROBSON, with the technical assistanceof LINDA J. PETERSON and ANNE RICHARDSON
From the Edward Mallinckrodt Department of Pediatrics and the Department of Pathology, Washington University School of Medicine andthe Renal Division, St. Louis Children's Hospital, St. Louis, Missouri, USA
Use of 132 microglobulin to diagnose tubulo-interstitial renal lesions inchildren. Fractional excretion (FE) of 132 microglobulin (f32M) wasstudied in children with glomerular (N 114), tubular (N 50) orother (N = 18) renal diseases. FE-f32M (normal C 0.36%) was signifi-cantly (P cc 0.001) lower in glomerular diseases (mean 0.104%) than intubular lesions (mean 4.27%). Unexpectedly, several patients withglomerular disease were found to have increased values for FE-f32M. Todetermine whether this was due to a tubular component in a primaryglomerular disease process, FE-132M was measured in 30 children withvarious glomerulopathies who underwent renal biopsy. Thirteen ofthese patients had tubulo-interstitial lesions in addition to their glomer-ular disease. FE-/32M in these patients averaged 3.76% (range 0.14 to44.6%); only two results were normal. Mean FE-thM in the 17 patientswithout biopsy evidence of tubulo-interstitial disease was 0.063%(range 0.02 to 0.34%); all values were in the normal range. The types ofglomerular diseases in the two groups of patients were similar. Patientswith a glomerular lesion complicated by tubulo-interstitial lesions had apoorer prognosis than did those with a pure glomerular disease. Thehigh incidence of tubulo-interstitial lesions in patients with glomerulardiseases was unexpected. Our data demonstrates that FE-thM repre-sents a reliable non-invasive method to diagnose such involvement.Measurements of f32M also provide a convenient method to follow thecourse and response to treatment of renal tubular injury.
j32-mieroglobulin (Ø2M), a protein with a molecular wt of11,800 daltons, is present on the cell surface of most nucleatedcells [I] as the small subunit of HLA class I antigens [2].Measurable concentrations of the protein are present in mostbiologic fluids [3]. Levels in the serum reflect both the produc-tion and excretion rates of the protein. Under most conditions,production rates and serum concentrations of f32M are remark-ably stable, although increased values may be seen with malig-nancies [4, 51, in infections [6], and with certain immunologicdisorders [7]. Since the kidney represents the major excretorypathway for the protein, alterations in serum Ø2M concentra-tions most often result from changes in the level of renalfunction. Indeed, it has been suggested that changes in theserum level of thM may be a better indicator of alteration inglomerular filtration rate (GFR) than equivalent levels of creat-mine [8].
Received for publication June 10, 1985,and in revised form December 16, 1985
© 1986 by the International Society of Nephrology
91
The removel of 2M from the serum is primarly by glomerularfiltration although some peritubular uptake of the protein mayalso occur [91. The glomerular sieving coefficient for /32Mexceeds 0.8 [10] so that large quantities of the protein arefiltered each day. More than 99.9% of the filtered protein isreabsorbed and catabolized by the proximal convoluted tubule.Consequently, normal urine contains low concentnstions off32M—typically less than 360 fkg/liter [11], except in the neo-nate. The urinary levels of f32M peak by the fifth day of life andshow a gradual decline until normal adult values are reached bythree months of age [12]. No tubular maximum (Tm) for humanf32M reabsorption has been found [9] so that the filtered load of2M has little, if any, effect on the urinary loss of this protein.Thus, most studies suggest that the urinary excretion of 132M isdetermined primarily by proximal tubular function. Tubulardamage secondary to ischemia [131 and to a variety of toxins[14] and drugs [15—19] results in increased urinary levels of2M.
The present study was undertaken to assess the clinicalusefulness of /32M determinations in diagnosing tubular involve-ment in a wide variety of renal diseases in children. Weinvestigated whether this noninvasive test could be helpful inseparating tubular from glomerular diseases and in following thecourse and treatment of patients with tubular diseases.
Methods
One hundred and eighty-two children whose ages rangedfrom one to nineteen years and who had a variety of renaldiseases (Table 1) were studied. The diagnosis was establishedby renal biopsy in those patients where it could not be estab-lished from clinical and laboratory data. Patients receivingknown nephrotoxic drugs such as aminoglycosides [17],methieillin [18], methotrexate [19], those exposed to heavymetals [14], those receiving parental hyperalimentation [20] andthose with active urinary tract infections [21, 22] or sepsis [231were excluded from the study since the renal handling of p2Mhas been shown to be modified in these conditions. Patientsreceiving immunosuppressive agents were included in thestudy, These agents are not known to alter the tubular handlingof f32M, although they can cause a reduction in serum levels bydecreasing production [24]. Several of the patients were studiedserially so that there were 241 observations on the 182 patients.
Concentrations of $2M in serum and urine were measured in172 of these children at the time that GFR was measured by

92 Portman et al
inulin clearance using standard clearance methodology [251. Inthese studies, after the volume of voided urine had beenmeasured, an aliquot of the urine was collected for /32Mdetermination. The pH of all these samples was > 5.5, a level atwhich $2M degradation does not occur [261, and in 215 of the226 samples, pH ranged between 6 and 7. Nevertheless, everysample was further alkalinized immediately with 0.1 N sodiumhydroxide to a pH of> 6.5 to ensure no decomposition of f32M
which occurs in acid urines [27]. The remaining 10 children allof whom had acute tubular necrosis, did not have inulinclearance measurements. In these children, FE-J32M was calcu-lated from creatinine and f32M levels in urine and plasmaobtained simultaneously.
Urine and serum were analyzed for p2M by a commerciallyavailable radioimmunoassay (Phadebus-50, Pharmacia, Up-psala, Sweden). Samples not analyzed on the day of collection
Table 1. A summary of the patients studied and their results
Number Cj,,im
FE-/32M Urinary p2MNumber of Number of
Disease studied of mi/mm/I .73 normal normalnumber of patients observations m2 (%) observations (mg/I) observations
Glomerular diseases
Acute nephritis 12 84.3* 0.069** 11 0.058 11N = 12 (0.032—0.894) (0.021—1.89)
SLE nephritis 30 83.6 0.053 28 0.051 27N = 20 (0.003—3.8) (0.003—6.7)
Membranoproliferative GN 9 46.2 0.724 5 0.338 5N = 6 (0.06—16.1) (0.01—17.2)
Membranous GN 7 54.1 4.57 1 2.24 0N = 2 15.4 (0.32—16.7) (1.4—17.2)
HSP nephritis 22 96.2 0.091 19 0.06 21N = 18 (0.03—3.24) (0.01—2.6)
Hemolytic uremic syndrome 10 87.2 0.06 10 0.06 9N = 9 12.7 (0.01—0.30) (0.01—0.18)
IgAnephropathy 6 106.4 0.102 6 0.32 6N = 3 (0.03-0.2) (0.02—0.08)
Hem, and/or Prot.t 27 105.4 0.74 27 0.064 27N 27 10.8 (0.02—0.26) (0.01—0.12)
Familial nephritis 9 93.4 0.077 9 0.048 9N = 7 (0.02—0.16) (0.02—0.06)
MCNStt 7 96.6 0.079 7 0.128 6N = 7 (0.01—0.205) (0.05—1.3)
Focal sclerosing GN 4 80.1 1.51 1 3.24 1N = 3 (0.11—8.8) (0.1—17)
All glomerulopathies 143 88.3 0.104 124 0.274 122N 114 (0.01—16.7) (0.01—17.2)
Tubular diseases
Obstructionlpyelonephritis 23 51.3 1.045 11 0.492 11N = 22 (0.04—50.3) (0.006—22.4)
Dysplasia 10 32.8 5.5 1 2.82 3N = 8 (0.36—105) (0.11—67.2)
Cystinosis 4 64.6 52.0 0 3.24 1N = 4 (13.8—68.7) (0.05—25.9)
Fanconi syndrome 12 87.1 10.5 0 8.91 0N 2 (1.8-99.6) (10.4—27.9)Interstitial nephritis 7 47.0 2.95 1 1.66 1
N = 4 (0.08—36) (0.05—16.8)Acute tubular necrosis 15 — 11.8 1 6.76 0
N = 10 (0.27—80.7) (0.4—30.8)All tubular disorders 71 54.4 4.27 14 2.24 16
N = 50 (0.03—105) (0.01—67.2)Other diseases
Glycogen storage dis. 3 97.2 0.398 2 0.812 2N 3 (0.04—30) (0.02—14.6)
Polycystic kidney 5 112.6 0.068 5 0.039 5N = 5 (0.04—0.10) (0.01—0.09)
Renal tubular acidosis 11 101 0.155 8 0.151 8N = 8 (0.03—1.9) (0.04—1.3)
Renal artery stenosis 8 83.5 0.05 8 0.074 7N=2 (0.01—0.18) (0.02—0.44)
All other disorders 27 96.9 0.11 23 0.01 22N = 18 (0.01—30) (0.01—14.6)
* Mean so; ** Mean with observed range; Hematuria and/or proteinuria; Minimal change nephrotic syndrome.

132 Ivuicroglobulin in renal tubular disease 93
were frozen at —70°C until analyzed. Preliminary studiesshowed that freezing did not affect j32M concentration, althoughrepeated freezing and thawing did decrease these levels. Repro-ducibility in our laboratory for repeated /32M measurements onserum and urine samples was 4.8%. Fractional excretion(FE) of 2M was calculated from the standard formula [281using the inulin concentrations measured in the same urine andserum samples. In the age range of patients studied, the normalserum values for f32M range from 1.1 to 2.4 (mean 1.6) mg/liter,the normal range for FE-JM from 0.01 to 0.36% [241 and thenormal urine concentration of /32M is 360 .rg/liter or less [11, 28,29]. In 44 of the children, urine and plasma samples were alsoanalyzed for creatinine by a modified Jaffe method [301 topermit comparison of creatinine and inulin when calculatingFE-f32M.
Of the children studied, 30 who were thought to have aglomerulonephritis, underwent renal biopsy to determine thenature of their renal disease. The need for percutaneous renalbiopsy was determined by clinical criteria. In no case was thebiopsy performed to obtain data for the study. The biopsyspecimens were processed by standard pathological techniquesfor evaluation by light, immunofluorescent and electron micros-copy. The pathologist was asked to evaluate these specimensfor evidence of tubulointerstitial disease without knowledge ofthe 7M results which had been measured on the day before therenal biopsy was performed.
Data was analyzed by standard statistical methodology [31].Distribution of values for serum and urine /.32M were skewed.These values were subjected to logarithmic transformationbefore analysis. Statistical significance was considered estab-lished with a P value of < 0.05. The study was approved by theHuman Studies Committee of Washington University beforeany data was obtained.
Results
Serum ,62M concentration
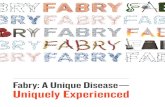
Serum f32M correlated well with FGR (Fig. I). Patients weredivided into those who had diseases which were primarilyglomerular, those with tubular disorders and those with otherrenal diseases. Visual inspection of the data suggested therewere no differences between results from these groups. Thiswas confirmed when data from each group was analyzedseparately. There were no significant differences between thelines of regression calculated by the method of least squares forthe three groups of patients.
Fractional excretion of l32M
The values for FE-2M in each of the disease categories aresummarized in Table 1. One hundred and forty-three observa-tions were made on 114 patients with glomerular diseases. Themean value for FE-p2M in this group was 0.104% (Table 1)which is well within the normal range. One hundred andtwenty-four of the individual results were normal. Abnormal(elevated) values were most often seen in patients with eithermembranoproliferative or membranous glomerulonephritis. In-creased values were observed occasionally in most otherglomerulopathies. Results from patients with nephrotic syn-drome varied depending on the underlying disease process.Normal values occurred in all patients who had minimal change
20 40 60 80 100 120 140
Cirh, mi/min/173 m2
Fig. I. The relationship between serum concentration of 132M and GFRin patients with different ftrms of renal disease. The regression line andcorrelation coefficient were calculated from all the values, irrespectiveof the underlying type of renal diseases. Symbols are: (.) glomerulardiseases; (0) tubular diseases; (A) other diseases. r = 0.78, P < 0.001.
nephrotic syndrome; in contrast, those with focal sclerosistended to have increased values for FE-/32M.
Of the 71 observations made on 50 patients with diseasesassociated with tubular damage, only 14 were in the normalrange. The mean value for FE-/32M in this group of patients was4.27% or almost 12 times the upper limit of normal. This valuewas signifcaritly (P <0.001) increased from that in patients withglomerular diseases. Markedly elevated levels were found inmany of the patients with tubular lesions. For example, thefractional excretion of f32M averaged 10.5% in subjects with theFanconi Syndrome, 11.8% in those with acute tubular necrosis,and more than 50% in those with cystinosis. Variable resultswere seen in patients with obstructive uropathy and chronicpyelonephritis. Some of these patients had very high values,others were in the normal range; none of these patients hadclinical or laboratory evidence for active infection at the time ofstudy to account for such a variation in results.
Most of the patients with other renal disorders had normalFE-7M values. For example, each of the patients with poly-cystic kidney disease had a normal result, although it should beemphasized that these studies were performed early in thecourse of the lesion when all the values for GFR were in thenormal range. Whether comparable results occur in patientswith longer standing lesions, was not evaluated,
Thirty-six of the 182 patients were studied twice. Values forFE-p2M agreed with one another in 34 of these children. One ofthe two patients with discordant values had membranoprolifera-live glomerulonephritis; the initial value was normal, the repealstudy six months later was elevated. FE-/32M was increased andGFR decreased in one patient during the acute nephritic phase
0
S000 00• 00•
0E
E
(/)
10
1.0
00
0SS &
S

c!.C0a)
xa)
a)C0C-)a)
U-
of Henoch—Schonlein purpura; both results were normal in thesecond study four months later. Two patients were studiedthree times; each value for FE-f32M was normal in both of thesepatients; FE-2M was consistently elevated in the two patientswith Fanconi syndrome who were studied a total of 12 times.Three patients had four studies each. In two of these patients allvalues for FE-2M were in agreement; in the third, who hadmembranous glomerulonephritis, the initial value was normalbut each of the three subsequent values was increased.
FE-/32M was related to GFR. Patients with reduced values forGFR tended to have the higher values for FE-132M. Since, as agroup, patients with glomerular diseases had better preservedlevels of GFR than did those with tubular lesions (88.3 26.7and 54.4 30.0 mlIminIl.73 m2 respectively; P < 0.001), thedata was re-analyzed to determine whether differences in GFRaccounted for the different values for FE-/32M in patients withglomerular and those with tubular diseases. In patients withtubular disorders, there was a significant inverse correlationbetween GFR and FE-/32M (r = 0.83; P < 0.001). Patients withglornerular diseases did not show an equivalent correlation (r =0.04; NS). In Figure 2, values for FE-f32M are compared inpatients with tubular and those with glomerular diseases atdifferent levels of GFR. At any given GFR, patients withtubular disorders had higher values for FE-/32M than did thosewith glomerular disorders. The higher values for FE-f32M atlower levels of GFR in the patients with tubular disease areapparent in this figure.
Creatinine as a glomerular marker
All of the preceeding values, except those in patients withacute tubular necrosis where clearances were not obtained,were calculated using inulin as the glomerular marker. Forty-four patients with varying diagnoses (25 patients with glomer-ular disease and 19 with tubular lesions) and a wide range ofvalues for inulin clearance (21 to 119 ml/min/1.73 m2) hadfractional excretions of f32M calculated from inulin and fromcreatinine concentrations determined on the same samples.There was excellent agreement between the results from thetwo methods with a correlation coefficient of 0.97 (P < 0.001).Thus, the data obtained in the present study can be appliedequally well in situations in which creatinine rather than inulinis used to measure renal function.
Urine f32M concentrations
Results of the study were analyzed further using urine p2Mconcentrations rather than FE-J32M. The correlation betweenFE- and urinary concentration of f32M was highly significant (r= 0.90; P < 0.001: Fig. 3). The correlation coefficient washigher for patients with tubular lesions (r = 0.94) than for thosewith glomerular diseases (r = 0.67). In each disease categorythe number of normal results using either FE-f32M or urinaryf32M agreed well (Table 1). Presuming that FE-/32M predictedtubular function accurately, urinary f32M levels correlated withFE-/32M in predicting normal tubular function in 159 of 161instances (98.8% accuracy). Conversely, urinary 2M was
0.001 NS P < 0.001 P < 0.01 P < 0.01
94 Porimun at a!
10
1.0
0.1
0.01
Fig. 2. The fraclional excretion of f32M in patients with glomerular and those with tubular renal diseases at different levels of GFR. Patients withglomerular diseases that had biopsy proven tubulo-interstitial disease were excluded from this analysis. Mean values and standard deviations areshown. The number of patients in a group is depicted within each bar. Symbols are: tubular disease; glomerular disease.
<25 25—49 50—74 75—100 >100
ml/min/1.73 m2

132 Microglobulin in renal tubular disease 95
100
10
1_U
.9.. It?- $ 0I A •• .8
.I
Urinary p2M, mg/mi
Fig. 3 The relationship between fractional excretion and urinary con-centration of B2M in the 241 studies. The results are platted accordingto the patient's type of disease but the regression line and correlationcoefficient are calculated from all the observations. Symbols are sameas Figure 1. r = 0.89; P < 0.001.
accurate in 72 of 80 instances (90.0% accuracy) in predictingtubular damage based on the FE-/32M.
Repeated determinations of urinary [32M levels in individualpatients usually agreed, although consistency was slightly lessgood than that for FE-/32M. Discordant results were obtained inthree of the 36 patients studied twice, and in one sample eachfrom a patient studied three times and one studied four times.
Renal biopsy ond the FE-f32M
As indicated above, some patients with apparently pureglomerular disease had elevated values for FE-[32M (Table 1).One explanation for this unexpected observation is that thesepatients could have a tubular component to their diseaseprocess. To determine whether this might he the case, FE-[32Mwas measured prospectively in 30 children with glomerulardisease who were to undergo a renal biopsy. The renal biopsieswere reviewed by one of the authors (JMK) for evidence oftubulo-interstitial disease without knowledge of the 132M data.Of these 30 patients, 17 had no evidence of tubulo-interstitialdisease; their FE-$2M averaged 0.063% with an observed rangeof 0.02 to 0.34% (Table 2). Each value felt into the normalrange.
The remaining 13 patients had an interstitial nephritis. In six,the lesion consisted of focal areas of mild or moderate degreesof lymphocytic infiltration often accompanied by mildinsterstitial edema, More marked lesions, including focal areasof fibrosis, were present in another four patients, one of whomhad plasma cells as well as lymphocytes in the infiltrate.Tubular atrophy was seen in the remaining three patients. In
one this was associated with extensive areas of chroniclymphocytic and plasma cell infiltration in the interstitium. Inanother, eosinophils as well as mononuclear cells were presentin the infiltrate. The third had diffuse interstitial fibrosis withIgO, IgA, 1gM and C3 demonstrated in the interstitium byimmunofluoreseent microscopy. This was one of two patients inwhom immunoglobulins or complement were identified in theinterstitium.
Three patients had had previous renal biopsies. In two,biopsies performed two and four years earlier respectively,showed no evidence of interstitial disease. In both, the biopsiesperformed at the time of the /32M study demonstrated severechronic interstitial inflammation. The third patient showed aninflammatory interstitial infiltrate consisting primarily of neu-trophils at the time he presented with immune complex glomer-ulonephritis. Five years later, when he appeared to haverecovered clinically, scattered areas of lymphocytie infiltrationwere the only abnormalities in the interstitium on a repeatbiopsy. Twelve years after disease onset, the patient had rapiddeterioration in renal function, and a third biopsy revealedatrophic tubules accompanied by interstitial fibrosis and im-mune complex deposits as already described.
The presence or absence of tubulo-interstitial disease was notassociated with a particular glomerular or systemic disease.Thus, there were no tubulo-interstitial lesions in seven patientswith systemic lupus erythematosus, three with MCNS, twowith Henoch—Schoenlein Purpura, two with IgA nephropathyand one patient each with proliferative glomerulonephritis,membranous glomerulonephriti s, and mesangial glomerulone-phritis. The group with tubulo-interstitial involvement com-prised three patients with systemic lupus erythematosus, threewith membranous glomerulonephritis, two with Henoch—Schoenlein Purpura, two with membranoproliferative glomeru-lonephritis and one each with proliferative glomerulonephritis,rapidly progressive glomerulonephritis, and focal sclerosingglomerulonephritis.
FE-/32M in the 13 patients with tubulo-interstitial diseaseaveraged 3.76% (observed range 0.14 to 44.6%). Only two of the13 results were in the normal range. The highest values forFE-f32M tended to occur in patients with the most severepathologic changes but increased values occurred also in pa-tients in whom interstitial but no tubular lesions were seen onthe biopsy.
Measurements of urinary /32M concentrations forecast theabsence of tubulo-interstitial disease in 16 of 17 cases in whichthis lesion was not present, and predicted the presence of suchdisease in 10 of 13 cases. Thus the precision of urinary p2Mlevels was slightly less than that of FE-[32M.
The presence of tubulo-interstitial lesions was associatedwith a poor outcome. Eight of the 13 patients with this lesionprogressed to end—stage renal disease (ESRD). Only one of the17 patients without tubulo-interstitial lesions developed ESRD(P < 0.005). The length of follow-up for the two groups ofpatients was comparable when either time from study (Table 2)or time from onset of disease (6.9 2.9 yrs vs. 7.1 3.2 yrs,respectively: NS) to the present was analyzed. The nine pa-tients who developed ESRD have been followed for 57.6 15.1
months since study compared to 48.2 23.8 months (NS) forthose who did not develop ESRD.
5C0aC.)
a)CaC0(2(0U-
0.1 1.0 10

96 Portman el al
Table 2. Comparison of FE-2M results from patients with glomerular disease and biopsy proven presence or absence of tubulo-interstitialdisease
Fractional Patientsexcretion
of /32M%
No of values. progressingto ESRD
N
Length* offollow—up
monthsNormal Elevated
No tubulo-interstjtial lesions 0.0635* 17 0 1 52.7N = 17 (0.02—0.34)
2 11 8 48.7N = 13 (0.14—44.6)
P < O.0Ol P < 0.001" P < 0.005" NS
Symbols are: From time of study to present. Mean SD; ** Mean withobserved range; Determined by Student's t-test; Determined by Chi—square.
Discussion
Measurements of 132M have been used for a number of clinicalpurposes. Urinary concentrations of the protein can identifyrenal tubular injury from heavy metals [14] and acute tubularnecrosis [13]. Even mild tubular dysfunction, for example thatin neonates with meconium stained amniotic fluid, can beidentified by measurement of 132M [32]. Other reported uses forthe measurement of the protein include differentiation of upperfrom lower urinary tract infections [211 and assessment of renaltubular maturation in neonates [33]. Serum levels of /32M havebeen used to predict renal transplant rejection [34, 351 and tomonitor diabetic nephropathy [361. Indeed, it has been sug-gested that changes in serum levels of p2M may be a betterindicator of changes in GFR, especially in children, than serumcreatinine since the rate of production of /32M is not body massdependent as is creatinine. In one study of 250 patients withvarious renal diseases, GFR estimated from serum levels of/32M were almost as reliable as values calculated from theclearance of 99m TC-DTPA [37]. Other studies have not con-firmed such a relationship [38]. We found a statistically signif-icant correlation between levels of serum /32M and GFR (Fig.1). Moreover, values from patients with glomerular, tubular andother renal diseases overlapped completely. Unfortunately,serum f3,M values varied considerably at any level of GFR sothat it was not possible to predict GFR with accuracy fromserum /32M values.
Urinary measurements of M, in contrast to serum levels,permitted the separation of patients with tubular disorders fromthose with glomerular diseases. Elevated values for FE-2Mwere observed in children with tubular diseases (Table 1) andthe mean value for this group of patients was more than 40 timeshigher than the equivalent value in patients with glomerulopath-ies. At any given level of GFR, patients with tubular disordershad higher values for FE-/32M than did those with glomerulardiseases (Fig. 2) although there was overlap in results from thetwo groups of patients. It was at the lowest levels of GFR wherethe separation was most complete. In agreement with previousstudies [39] patients with glomerulonephritis and a markedlyreduced GFR had normal values for FE-2M; those withtubular diseases had elevated FE-f32M results. The excellentdiagnostic value of measurements of FE-2M in identifying theexistence of a tubular lesion is illustrated by the findings in the30 patients who were thought to have a glomerular disease andwho underwent renal biopsy. Thirteen of these patients had
tubulo-interstitial lesions of whom 11 had high values forFE-1M. None of the patients without tubulo-interstitial in-volvement had elevated FE-f32M levels. The high incidence ofthese tubulo-interstitial lesions in the biopsied patients probablyresulted from the indications used to establish the need for thebiopsy. The clinical and laboratory findings in these patientswere atypical and necessitated the establishment of an exacthistologic diagnosis. Tubular disease was not suspected prior tobiopsy, except in one patient who had had a previous biopsy.
These observations indicate that measurements of FE-/32Mhelp to differentiate tubular from glomerular disease and willidentify tubular involvement in a primary glomerular disease.The elevated values for FE-/32M in tubular disorders are mostlikely due to tubular damage, which reduces the ability of theproximal tubule to reabsorb the filtered load of this protein. Wewere unable to correlate the urinary excretion of 132M in ourpatients with the calculated filtered load of the protein, even ifthe sieving coefficient for f32M in renal disease was assumed tobe 1.0. Since serum J32M values from patients with glomerular,tubular and other renal diseases overlapped completely (Fig. I),there is no evidence that the sieving coefficient for this proteinvaried in the different disease categories, Thus, there is noevidence to support the concept that the elevated levels ofurinary /32M were due to a marked increase in filtered load of2M which overwhelmed tubular reabsorption of this protein.Other studies support this conclusion. For example, the maxi-mum tubular reabsorptive capacity for /32M could not beexceeded either when serum f32M levels were markedly in-creased in patients with normal renal function [38] or byinfusions of the protein [91.
Since 2M measurements appear to be such a good indicatorof tubular injury, they could have additional clinical uses tothose already discussed. We found that sequential measure-ments provided useful information about changes in the level oftubular function. For example, the initial FE-f32M values inpatients with acute tubular necrosis averaged 33.0 13.1%;they fell progressively to 9.0 4.2% by 10 to 20 days into thedisease course and eventually returned to normal in thosepatients who were followed long—term. Another example of theusefulness of repeated values was provided by a three year oldboy who had inflammatory bowel disease and chronic diarrhea.He developed a nephrotic syndrome. A renal biopsy demon-strated membranous glomerulonephritis and an immunologi-cally mediated tubulo-interstitial disease which was associatedwith the Fanconi syndrome. His initial value for FE-/32M was

[32 Microglobulin in renal tubular disease 97
96.6%. This value fell rapidly and progressively to below 6%within one month of instituting treatment with steroids. Re-lapses of the tubular disease were subsequently predicted byincreasing values for FE-J3M, which occurred before anychanges in GFR, amino—aciduria, or metabolic acidosis weredocumented.
Measurements of FE-f32M could have additional diagnosticvalue. For example, all the children with nephrotic syndromesecondary to MCNS had normal FE-M results; those withother causes such as focal sclerosis, membranous glomerulone-phritis or membranoproliferative glomerulonephritis frequentlyhad elevated values. Children with polycystic kidney diseasehad normal values for FE-7M; those with renal dysplasiatended to have elevated levels, Perhaps most importantly,FE-f32M may help to determine prognosis for patients. Wefound that patients who had a glomerular disease complicatedby tubular involvement had elevated values for FE-f32M and apoorer prognosis than did those in whom only the glomeruliwere diseased (Table 2). The correlation between tubulo-inter-stitial lesions and poor prognosis has been noted previously[401, our observations indicate that measurements of FE-/32Mhelp to identify those patients at risk.
The current observations suggest that measurements of uri-nary /32M concentration represent an excellent screening testfor detecting tubulo-interstitial disease. If these values areelevated, FE-J32M should be measured for a more preciseindicator of the presence of renal tubular disease. It must beremembered, however, that all of the current studies wereperformed under standardized conditions of mild diuresis whichwas induced to increase the accuracy of simultaneous measure-ments of inulin clearance. In addition, urine samples werealkalinized immediately upon collection to minimize the decom-position of 132M which occurs in an acid urine [27]. Whetherrandom samples obtained under a variety of non-standardconditions would be equally reliable as a diagnostic tool was notevaluated in this study. In summary, the present study demon-strates that measurement of 2M, especially FE-p2M, providesa reliable method to identify tubular injury in renal diseasestates and may provide a useful guide to help determineprognosis in patients with these lesions,
AcknowledgmentThis study was supported in part by Clinical Research Center Grant
00036.
Reprint requests to Alan M. Robson, M.D., Department of Pediat-rics, 400 S. Kingshighway Blvd., P.O. Box 14871, St. Louis, Missouri63178, U.S.A.
References
I, PETERSON PA, SEGE K, ANUNDI H: 132-microglobulin on the cellsurface. Acta Clin BeIg 31(Suppl.8):5—l3, 1976
2. CRESSWELL P, SPRINGER T, SFROMINGER JL, TURNER MJ, GREYI-TM, Kuuo RT: Immunological identity of the small subunit ofHL-A antigens and /32-microglobulin and its turnover on the cellmembrane. Proc NatI Acad Science USA 7! :2123—2l27, 1974
3. EVRIN PE, PETERSON PA, WIDE L, BERGGARD I: Radio-immunoassay of [32-microglobulin with human biologic fluids.Scand J Clin Lob Invest 28:439—443, 1971
4. CASSUTO iF, KREBS BP, VI0T G, DUJARDIN F, MASSEYEFF R:f32-microglobulin, a tumor marker of lymphoproliferative disorders.Lancet 2:108—109, 978
5. SHUSTER 3, GOLD P, POULIK MD: f32-microglobulin levels in
cancerous and other disease states. C/in Chirn Ada 67:307—313,1976
6. IBsEN KK, KRABBE S, HESSE J: [32-microglobulin serum levels ininfectious mononucleosis in childhood. Acta Path Microbiol Scand89:205—208, 1981
7. MANICOURT D, ORLOFF S, BRAUMAN H: Studies on [32-microglo-bulin in synovial fluid from arthritis patients in [32M in ProliferativeDisorders and heavy Metal Intoxication, edited by PETERSON PA,LAUWERYS R, Gent—Belgium, European Press, 1978, pp. 93—103
8. TROLLFORS B, NORRBY R: Estimation of glomerular filtration rateby serum creatinine and serum 132-microglobulin. Nephron28:l96—199, 1981
9. HALL PW, CHUNG—PARK M, VACCA CV, LONDON M, CROWLEYAQ: The renal handling of /32-microglobulin in the dog. Kidney mt22:156—161, 1982
10. KARLSSON FA, WII3ELL L, EVRIN PE: 132-Microglobulin in clinicalmedicine. Scand J C/in Lab Invest 40:27—37, 1980
11. PETERSON PA, EVRIN PE, BERGGARD I: Differentiation of glomer-ular, tubular and normal proteinuria: determinations of urinaryexcretion of 132-microglobulin, albumin, and total protein. J C/inInvest 48:1189—1198, 1969
12. KARLSS0N FA, HANDELL L, HELLSING K: A prospective study ofurinary proteins in early infancy. Acta Ped Scond 68:663—667, 1979
13. HALL PW: [32-microglobulin in the differential diagnosis of renaldisorders, in 132-microglobu/in in Renal Diseases, edited by An-nersten A, Uppsala, Sweden, Pharmacia Diagnostics AB, 1979, pp.39—51
14. ROELS H, BERNARD A, PUCI-IOT JP: Response of /32-microglobulinand other proteins in workers exposed to cadmium, lead or mer-cury, in f32M in Proliferative Disorders and heavy Metal Intoxica-tion, edited by Peterson PA, Lauwerys R, Gent—Belgium, Euro-pean Press, 1978, pp. 78—92
15. COHEN Al, HARBERG J, CnRiat DL: Measurement of urinary[32-microglobulin in the detection of cisplatin nephrotoxicity. Can-cer Treatment Report.s 65:1083—1085, 1981
16. LATT D, WEISS, JB, JAYs0N MIV: j32-microglobulin levels in serumand urine of rheumatoid arthritis patients on gold therapy. AnnRheum Dis 40:157—160, 1981
17. SCHENTAG JJ, PLAUI ME: Patterns of urinary [32-microglobulinexcretion by patients treated with aminoglycosides. Kidney mt17:654—661, 1980
18. BORDER WA, LEHMAN DH, EGAN JD, SASS NJ, GLODE JE,WILSON CB: Antitubular basement membrane antibodies in
methicillin—associated interstitial nephritis. N Engi J Med291:381—384, 1974
19. CONDIT PT, CHANES RE, JOEL W: Renal toxicity of methotrexate.Cancer 23:126—131, 1969
20. MOGENSEN CE, SOLLING K: Studies on renal tubular proteinreabsorption: partial and near complete inhibition by certain aminoacids. Scand J C/in Lab Invest 37:477-486, 1977
21. SCHARDIJN G, STATIUS VAN Es LW, SWAAK AJG, KAGER JCGM,PERSIJN JP: Urinary /32-microglobulin in upper and lower urinarytract infections. Lancet 1:805—807, 1979
22. SCHARDIJN G, SIArIuS VAN EPS LW, STOUT—ZONNEVELD AAM,KAGER JCGM, PERSIJN JP: Urinary f32-microglobulin excretion inurinary tract infections, Acto Clin Beig 35(Suppl.10):21—29, 1980
23. LINTON AL, SIBBALD Wi, PETRAKAS A, RICHMOND JM: Patternsof urinary protein excretion in patients with sepsis. (abstract)Kidney mt 21:153, 1982
24. REVILIARD JP, VINCENT C: Clinical significance of f32-microglo-bulin determination. Acta Clin Beig 35(Suppl.10):14—20, 1980
25. CoI.E BR, GIANGIAC0MO J, INGELFINGER JR, ROBSON AM: Mea-surement of renal function without urine collection, N Engi J Med287:1109—1114, 1972
26. EVRIN PE, WIBELL L: The serum levels and urinary excretion of/32-microglobulin in apparently healthy subjects. Scand J C/in LobInvest 29:69—74, 1972
27. DAVEY PG, GOSLING P: -Microglobulin instability in pathologicalurine. C/in Chem 28:1330—1333, 1982
28. FELDERRA, TINA LU, CALCAGNO PL: Urinary concentration of/32microglobulin in a pediatric population. (abstract) InternationalPediatric Nephrology Symposium, Philadelphia, 1980
29. PHADEBUS [3-M1cRo TEST. Expected values. Pharmacia Diagnos-

98 Portman et a!
tics. Piscataway, New Jersey, 197830. SCHWARTZ GJ, HAYCOCK GB, EDELMANN CM JR, SPITZER A: A
simple estimate of glomerular filtration rate in children derived frombody length and plasma creatinine. Pediatrics 58:259—263, 1976
31. ARMITAGE P: Statistical Methods in Medical Research. Oxford,Blackwell, 1980, pp. 99—118
32. COLE JW, PORTMAN RJ, LIM Y, PERLMAN JM, ROBSON AM:Urinary 132-microglobulin in full term newborns: evidence forproximal tubular dysfunction in infants with meconium stainedamniotic fluid. Pediatrics 76:958—964, 1985
33. ENGLE WD, ARANT BS JR: Renal handling of j32-microglobulin inthe human neonate. Kidney in! 24:358—363, 1983
34. EDWARDS LC, HELDERMAN JH, HAMM LL, LuDwIN D,GAILIUNAS P JR., HULL AR: Non-invasive monitoring of renaltransplant function by analysis of f32-microglobulin. Kidney mt23:767—770, 1983
35. FIRLIT CF, GREENSLADE T, BASHOOR R: The prognostic value of
/3-microglobulin in pediatric renal transplantation. Proc Clin DialTrans Forum 8:219, 1978
36. VIBERTI GC, KEEN H, MACKINTOSH D: f32-microglobulinaemia: asensitive index of diminishing renal function in diabetes. Br Med J282:95—98, 1981
37. BRAREN V, GODDARD J, BRILL AB, TOUYA JJ: 32-Microglobulin asrenal diagnostic agent. Urology 13:624—628, 1979
38. HALL PW, RICANATI ES: Renal handling of 32-microglobulin inrenal disorders; with special reference to hepatorenal syndrome.Nephron 27:62—66, 1981
39. J0HANssON BG, RAVNSKOV U: The serum level and urinaryexcretion of a2-microglobulins, /32-microglobulin and lysozyme inrenal disease. Scand J Urol Nephrol 6:249—256, 1972
40. SHERMAN RL, DRAYER DE, LEYLAND—JONES BR, REIDENBERGMM: N-acetyl-acetyl-/3-glucosaminidase and J32-microglobulin:their urinary excretion in patients with renal parenchymal disease.Arch intern Med 143:1183—1185, 1983














![Review Multimodality Imaging of Integrin αvβ3 Expression · Theranostics 2011, 1 136 ponents of the interstitial matrix such as vitronectin, fibronectin and thrombospondin [10].](https://static.fdocument.org/doc/165x107/5d55927188c9937f558bbd52/review-multimodality-imaging-of-integrin-v3-expression-theranostics-2011.jpg)
