UrinaryN-acetyl-β-glucosaminidase and guanidinoacetic acid levels in epileptic patients treated...
4
ELSEVIER Brain & Development 1994; 16:437-40 Original article Urinary N-acetyl-/3.glucosaminidase and guanidinoacetic acid levels in epileptic patients treated with anti-epileptic drugs Takayuki Otsuka, Yasuo Sunaga, Akio Hikima Department of Pediatrics, Gunma University School of Medicine, Maebashi, Japan Received 7 December 1993; accepted 26 June 1994 We investigated potential renal functional impairment induced by chronic use of anti-epileptic drugs (AEDs) in 79 epileptic children. They were divided into five groups: valproic acid (VPA) monotherapy where the serum concentration (SC) of VPA was no less than 60 ixg/ml (VPA [SC >__ 60]) (15 cases), VPA monotherapy where the SC VPA was less than 60 ltg/ml (VPA [SC < 60]) (29 cases), phenobarbital monotherapy (PB) (7 cases), carbamazepine monotherapy (CBZ) (16 cases), and polytherapy containing VPA (12 cases). Urinalysis (proteinuria and hematuria) and serum creatinine were normal except for two cases of proteinuria and two cases of hematuria. The level of urinary excretion of N-acetyl-13-glucosaminidase (u-NAG) was high in 29% of all patients, and 47% of VPA (SC > 60), 38% of CBZ, 25% of polytherapy, and 24% ofVPA (SC < 60) groups. There was a significant positive correlation between serum concentration of VPA and u-NAG/urinary creatinine (u-Cr). The level of guanidi- noacetic acid (u-GAA) excreted in the urine was normal except in one patient. U-NAG/u-Cr may be a more sensitive marker than u-GAA/u-Cr for renal functional impairment in AED therapy. Keywords: Guanidinoacetic acid (GAA); N-Acetyl-/3-glucosaminidase (NAG); Epilepsy; Anti-epileptic drug; Renal functional impairment 1. INTRODUCTION The possible side effects of anti-epileptic drugs (AEDs) include, but are not limited to, renal functional impairment and damage. Proximal tubular renal syndrome caused by valproic acid (VPA) [1] has been reported. Acute interstitial nephritis has been observed with administration of VPA [2], phenytoin (PHT) [3] and carbamazepine (CBZ) [4]. Acute renal failure has been described as a consequence of PHT [5] and CBZ treatments [6,7]. Urinary N-acetyl-/3-glucosamini- dase (u-NAG) [8,9] and /3-galactosidase [8] have been dis- cussed in several reports as markers of AED-induced renal functional impairment. Guanidinoacetic acid (GAA), one of the guanidino compounds, is produced mainly in the kidney from arginine and a precursor of creatinine (Cr). The urinary excretion of GAA (u-GAA) is known to reflect kidney func- tion [10-12] and is diminished in renal failure [13], hyperten- Correspondence address: T. Otsuka, MD, Department of Pedi- atrics, Gunma University School of Medicine, Shouwa-machi 3-39-15, Maebashi, Gunma 371, Japan. Fax: (81) (272) 20-8215. 0387-7604/94/$07.00 © 1994 Elsevier Science B.V. All rights reserved SSDI 0387-7604(94)00057-3 sion [14,15], and antibiotic therapy [16]. Shiraga et al. re- ported that the serum GAA level was low in epileptic pa- tients, especially those receiving VPA [17], however, there appear to be no reports discussing u-GAA levels in patients receiving AEDs. The aim of this study was to evaluate the significance of measuring urinary NAG and GAA in the chronic treatment of childhood epilepsies. 2. MATERIALS AND METHODS Seventy-nine epileptic patients (6-15 years) who had dif- ferent types of seizures, were treated for no less than 6 months with an AED or AEDs, and were taking no other drug for at least 2 weeks prior to examination, were studied. The patients were divided into five groups as follows: VPA monotherapy with the serum concentration (SC) of VPA no less than 60 /zg/ml (VPA [SC>60]) (15 cases), VPA monotherapy with the SC of VPA less than 60 gg/ml (VPA [SC < 60]) (29 cases), phenobarbital (PB) monotherapy (7 cases), CBZ monotherapy (16 cases), and polytherapy con- taining VPA (12 cases). The patterns of polytherapy with VPA were: VPA + clonazepam (CZP) (3 cases), VPA + PHT (3 cases), VPA + CBZ (1 case), VPA + zonisamide (ZNS) (1
Transcript of UrinaryN-acetyl-β-glucosaminidase and guanidinoacetic acid levels in epileptic patients treated...

ELSEVIER Brain & Development 1994; 16:437-40
Original article
Urinary N-acetyl-/3.glucosaminidase and guanidinoacetic acid levels in epileptic patients treated with anti-epileptic drugs
Takayuki Otsuka, Yasuo Sunaga, Akio Hikima Department of Pediatrics, Gunma University School of Medicine, Maebashi, Japan
Received 7 December 1993; accepted 26 June 1994
We investigated potential renal functional impairment induced by chronic use of anti-epileptic drugs (AEDs) in 79 epileptic children. They were divided into five groups: valproic acid (VPA) monotherapy where the serum concentration (SC) of VPA was no less than 60 ixg /ml (VPA [SC >__ 60]) (15 cases), VPA monotherapy where the SC VPA was less than 60 l t g / m l (VPA [SC < 60]) (29 cases), phenobarbital monotherapy (PB) (7 cases), carbamazepine monotherapy (CBZ) (16 cases), and polytherapy containing VPA (12 cases). Urinalysis (proteinuria and hematuria) and serum creatinine were normal except for two cases of proteinuria and two cases of hematuria. The level of urinary excretion of N-acetyl-13-glucosaminidase (u-NAG) was high in 29% of all patients, and 47% of VPA (SC > 60), 38% of CBZ, 25% of polytherapy, and 24% ofVPA (SC < 60) groups. There was a significant positive correlation between serum concentration of VPA and u-NAG/urinary creatinine (u-Cr). The level of guanidi- noacetic acid (u-GAA) excreted in the urine was normal except in one patient. U-NAG/u-Cr may be a more sensitive marker than u-GAA/u-Cr for renal functional impairment in AED therapy.
Keywords: G u a n i d i n o a c e t i c ac id ( G A A ) ; N-Acety l - /3 -g lucosaminidase (NAG) ; Epi lepsy; An t i - ep i l ep t i c drug; Rena l funct ional i m p a i r m e n t
1. I N T R O D U C T I O N
The possible side effects of anti-epileptic drugs (AEDs) include, but are not limited to, renal functional impairment and damage. Proximal tubular renal syndrome caused by valproic acid (VPA) [1] has been reported. Acute interstitial nephritis has been observed with administration of VPA [2], phenytoin (PHT) [3] and carbamazepine (CBZ) [4]. Acute renal failure has been described as a consequence of PHT [5] and CBZ treatments [6,7]. Urinary N-acetyl-/3-glucosamini- dase (u-NAG) [8,9] and /3-galactosidase [8] have been dis- cussed in several reports as markers of AED-induced renal functional impairment. Guanidinoacetic acid (GAA), one of the guanidino compounds, is produced mainly in the kidney from arginine and a precursor of creatinine (Cr). The urinary excretion of G A A (u-GAA) is known to reflect kidney func- tion [10-12] and is diminished in renal failure [13], hyperten-
Correspondence address: T. Otsuka, MD, Department of Pedi- atrics, Gunma University School of Medicine, Shouwa-machi 3-39-15, Maebashi, Gunma 371, Japan. Fax: (81) (272) 20-8215.
0387-7604/94/$07.00 © 1994 Elsevier Science B.V. All rights reserved SSDI 0387-7604(94)00057-3
sion [14,15], and antibiotic therapy [16]. Shiraga et al. re- ported that the serum G A A level was low in epileptic pa- tients, especially those receiving VPA [17], however, there appear to be no reports discussing u-GAA levels in patients receiving AEDs. The aim of this study was to evaluate the significance of measuring urinary NAG and GAA in the chronic treatment of childhood epilepsies.
2. M A T E R I A L S AND METHODS
Seventy-nine epileptic patients (6-15 years) who had dif- ferent types of seizures, were treated for no less than 6 months with an AED or AEDs, and were taking no other drug for at least 2 weeks prior to examination, were studied. The patients were divided into five groups as follows: VPA monotherapy with the serum concentration (SC) of VPA no less than 60 /zg /ml (VPA [SC>60]) (15 cases), VPA monotherapy with the SC of VPA less than 60 g g / m l (VPA [SC < 60]) (29 cases), phenobarbital (PB) monotherapy (7 cases), CBZ monotherapy (16 cases), and polytherapy con- taining VPA (12 cases). The patterns of polytherapy with VPA were: VPA + clonazepam (CZP) (3 cases), VPA + PHT (3 cases), VPA + CBZ (1 case), VPA + zonisamide (ZNS) (1

438 7] Otsuka et al. /Brain & Development 1994; 16:437-40
Table 1 Control group
Age Group Number Age NAG GAA (years) (years) (U /g Cr) (mg/g Cr)
15 13 15.4_+0.2 2.06-+0.91 75.1 _+31.0 14 13 14.3_+0.2 2.09_+ 1.55 79.6_+43.1 13 15 13.3_+0.2 2.28_+1.17 94.1_+31.7 12 15 12.5_+0.3 1.57-+0.64 101.0_+26.0 11 14 11.4_+0.3 2.02_+1.25 102.6-+31.2 10 13 10.4_+0.3 1.86_+0.86 110.0_+35.6 9 15 9.5 +_ 0.3 2.44 _+ 1.93 85.6 -+ 39.3 8 14 8.4-+0.2 2.42_+1.04 108.4_+48.2 7 11 7.5 _+ 0.2 2.33 _+ 1.52 109.0 _+ 32.7 6 9 6.8_+0.1 2.12_+0.60 93.9_+25.9
Total 132 11 .4_+2.7 2.12_+1.26 96.5_+37.1
Each value is expressed as the mean_+ S.D. NAG, N-acetyl-/3-gluco- saminidase; GAA, guanidinoacetic acid; Cr, creatinine; U / g Cr, unit/g urinary creatinine.
case), V P A + C B Z + C Z P (1 case), V P A + C Z P + P B (1 case), and VPA + CZP + ZNS (2 cases). Age-matched nor- mal controls (132 volunteers) had neither proteinuria nor hematuria, were healthy, and had had no medication for at least a month. They were divided into ten groups by age (Table 1). Urine and blood samples were obtained on the same day and within 30 rain from the same patient. A first morning urine sample was collected from volunteers. Serum and urine samples were stored at - 2 0 ° C until analysis. In patients, urine and serum was analyzed for proteinuria, hematuria, u-NAG, u-GAA, u-Cr, serum Cr, and serum concentration of anticonvulsants. In polytherapy groups, serum concentration of VPA was determined as a represen- tative of AEDs. In volunteers, u-NAG, u - G A A and u-Cr were measured. Informed consent was obtained from all patients, volunteers and their parents.
Urinary N A G was determined by the fluorometric method, using sodio m-cresolsulfonphthaleinyl N-acetyl-/3-gluco- saminide as the substrate in the kit from Shionogi (Osaka, Japan) [18]. u - G A A was measured by the colorimetric method, developed by Shirokane et al. [19], using the kit from Kikkoman (Chiba, Japan). Serum- and urinary- creatinine (u-Cr) were measured by enzymatic determination with a kit from Denkaseiken (Tokyo, Japan) [20].
Proteinuria was defined as positive when more than one plus reaction was detected by a paper test for protein in uncentrifuged urine. Hematur ia was deemed positive when more than five red cells per high-power field were seen in the sediment. For both u - N A G / u - C r and u - G A A / u - C r , the values within the range of mean + 2 S.D. were considered to
be normal. The u - N A G / u - C r level was judged to be abnor- mal when it was above the mean + 2 S.D. while u - G A A / u - C r was abnormal when it was below the mean - 2 S.D.
One-way analysis of variance (one-way A N O V A ) and the Cochran-Cox test were used to evaluate the differences between A E D groups and normal control groups, and intra- control group differences. A linear regression test was done to analyze the correlation between SC of A E D or duration of A E D treatment and u - N A G / u - C r or u - G A A / u - C r level. In polytherapy groups, SC of VPA was used for the linear regression analysis. The comparisons were considered signifi- cant when P was less than 0.01.
3. R E S U L T S
Table 1 shows the mean + S.D. of u - N A G / u - C r and u - G A A / u - C r in normal control groups, There were no sig- nificant differences among the age groups by one-way A N O V A , for both u - N A G / u - C r and u - G A A / u - C r levels. Therefore, ten control groups can be treated as one group (combined control group) for either substance. The u- N A G / u - C r level was 2.12 + 1.26 (U/gCr ) , and the normal range was set at 0-4.64 (U /gCr ) . The u - G A A / u - C r level was 96.5 + 37.1 (mg/gCr) , and the normal range was 22.3-170.7 (mg/gCr) .
Proteinuria was seen in two patients, one was from the VPA monotherapy (SC > 60) group (the grade of proteinuria was of one plus) and the other one from the polytherapy group (one plus). Hematur ia was detected in the other two patients in the CBZ group. One was diagnosed as having familial hematuria (RBC count: 15-20 - high-power field) and the other 5 -7 - high-power field. Three out of these four patients had an abnormal u - N A G / u - C r level, but all were normal for u - G A A / u - C r level. No patient had an abnormal serum Cr level.
An abnormal u - N A G / u - C r level was detected in 23 (29%) patients. Seven (47%) were in the VPA (SC > 60), 7 (24%) in VPA (SC < 60), 0 (0%) in PB, 6 (38%) in CBZ, and 3 (25%) in polytherapy. VPA (SC >_ 60), CBZ and polytherapy groups had significantly higher levels compared with the combined control group by one-way A_NOVA and Cochran-Cox test. PB and VPA (SC < 60) groups were not significantly differ- ent from the combined control group (Table 2).
In terms of u - G A A / u - C r , all patients were normal, ex- cept one (1.3%) in the VPA (SC > 60) group. There were no significant differences among A E D s groups and the com-
Table 2 A E D groups and results
AED group Number Age S.C. Serum Cr NAG result GAA result (years) (/zg/ml) (mg/dl) (U/g Cr) (mg/g Cr)
VPA (SC >_ 60) 15 10.3_+2.2 75.9 _+15.5 0.49+0.12 6.46_+4.55 p < 0 . 0 1 104.0_+38.1 NS VPA (SC < 60) 29 11.5_+2.3 37.8 _+15.6 0 .59_+0 .13 2.82_+2.50 NS 119.1_+44.6 NS PLT 12 10.7_+2.8 56.2 +28.0 0.58_+0.15 3.71_+ 1.67 p < 0 . 0 1 93.9+_34.7 NS CBZ 16 11.5-+2.3 6.34-+ 2.76 0.52-+0.10 4.06_+2.64 p < 0 .01 114.0-+47.7 NS PB 7 11.3_+2.1 11.5 -+ 6.0 0.62-+0.15 1.86_+1.34 NS 109.5_+56.2 NS Control 132 11.4 -+ 2.7 2.12 _+ 1.26 96.5 _+ 37.1
Each value is expressed as the mean + S.D. AED, anti-epileptic drug; S.C., serum concentration; Cr, creatinine; dase; GAA, guanidinoacetic acid; VPA, valproic acid; PLT, polytherapy containing VPA; PB, phenobarbital; significant; U/Cr, unit/g urinary creatinine. (Serum concentration of PLT is that of VPA.)
NAG, N- acetyl-/3 -glucosamini- CBZ, carbamazepine; NS, not

T. Otsuka et aL /Brain & Development 1994; 16:437-40 439
Table 3 Results of linear regression analysis
AED Serum group concentration (number of cases)
Duration
VPA u-NAG/u-Cr +0.40 p < 0.01 -0.01 NS (n = 44) u-GAA/u-Cr -0.20 NS -0.21 NS PLT u-NAG/u-Cr +0.09 NS -0.62 NS (n= 12) u-GAA/u-Cr -0.20 NS -0.75 p <0.01 PB u-NAG/u-Cr -0.19 NS +0.37 NS (n = 7) u-GAA/u-Cr - 0.03 NS - 0.65 NS CBZ u-NAG/u-Cr -0.04 NS -0.10 NS (n = 16) u-GAA/u-Cr +0.11 NS +0.33 NS
AED, anti-epileptic drug; VPA, valproic acid; PLT, polytherapy containing VPA; PB, phenobarbital; CBZ, carbamazepine; u-NAG, urinary N-acetyl-/3-glucosaminidase; u-Cr, urinary creatinine; u- GAA, urinary guanidinoacetic acid; NS, not significant.
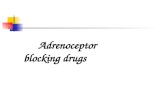
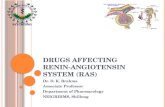
300 [ Y:-12.3x+I46.2 r :-0.75(p<0.01) ~ : n . r .
zoo l 0 E
.~ 100
0 2 4 6 8
Duration of polytherapy (Years)
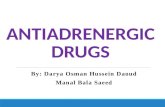
Fig. 2. The correlation between duration of anti-epileptic drug ther- apy and urinary guanidinoacetic acid/creatinine level in polytherapy group. Linear regression (P < 0.0l) revealed a significant negative correlation, n.r., normal range of control; Cr, creatinine; U/g Cr, unit/g urinary creatinine.
bined control group by one-way ANOVA and Cochran-Cox test (Table 2).
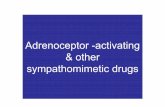
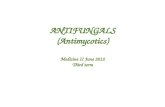
Table 3 shows the results of a linear regression test. There was a significant positive correlation between the SC of VPA in VPA monotherapy groups (VPA [SC > 60] group + VPA [SC < 60] group) and u-NAG/u-Cr level (r = 0.39, P < 0.01) (Fig. 1). The other monotherapy and polytherapy groups had no significant correlation with serum concentration. Al- though there was a significant negative correlation between duration of AEDs treatment and the u -GAA/u-Cr level in the polytherapy group, u -GAA/u-Cr levels were within nor- mal limits (r = -0.75, P < 0.01).
4. DISCUSSION
In the study subjects, only four patients showed abnormal findings in routine urinalysis: two had proteinuria (2.5%) and two (2.5%) hematuria. This result is similar to that of Cam- field et al. [21]: they investigated 199 asymptomatic children with epilepsy and urinalysis was normal in all patients except one (proteinuria). Public health service of urinary screening in Japan revealed that the prevalence of proteinuria and hematuria among elementary school children was 0.08% and 0.54%, respectively, and among junior high-school children
20 Y=O,GX+O.6 r =0.40< p<o.oI > mJ:n.r. •
10 • •
0 20 40 60 80 100
Serum Concentration of VPA (JJg/ml)
Fig. 1. The correlation between serum concentration of valproic acid and urinary N-acetyl-/3-glucosaminidase/creatinine level. There is a significant positive correlation in the linear regression test (P < 0.01). n.r., normal range of control; Cr, creatinine; U/g Cr, unit/g urinary creatinine.
was 0.37% and 0.94%, respectively, both based upon a paper test [22]. Thus, the incidence of both proteinuria and hema- turia in this study was slightly higher than the figures cited above.
The present study also showed that the level of u- NAG/u-Cr was abnormal in VPA (SC > 60), CBZ and poly- therapy groups compared with the age-matched normal con- trol group, and that the u-NAG/u-Cr level showed a signifi- cant positive correlation with SC of VPA. There are several reports showing increased excretion of NAG during long-term AED treatment, especially VPA, polytherapy [8,9], and CBZ [9]. Some authors found increasing excretion of NAG with proximal renal tubular damage [23,24], but the possibility exists that AED(s) causes renal tubular enzyme induction or activation.
Recently u-GAA was reported to reflect the metabolic function of the kidneys. Ishizaki et al. [10] and Isoda et al. [11] noted u-GAA excretion was a better marker than serum Cr or Cr clearance for rejection in kidney transplantation. Cisplatin [25] and gentamicin [16] administration also de- creased u-GAA excretion. As far as we know there have been no reports discussing the normal level in children. Nako described the u -GAA/u-Cr level in healthy neonates (n = 38) and healthy adults (n = 73) as 111.76 _+ 78.9 mg/g Cr and 67.1 + 32.1 mg/g Cr, respectively [12]. In the present study, the level of u -GAA/u-Cr in the control group showed no age-dependent difference in the 6-15 year old range, and was at an intermediate level between the neonate and adult levels. This suggests that the u -GAA/u-Cr level may be relatively high in the neonate, and then gradually fall to the adult level, u-GAA was measured by an enzymatic method in this study which has been shown to have satisfactory accuracy and precision comparable with that of high-performance liquid chromatography [19].
The u-GAA/u-Cr level was marginally abnormal in the monotherapy and polytherapy groups, while the u-NAG/u-Cr level was abnormal in about one-third of patients, u-GAA is formed from arginine by L-arginine-glycine amidinotrans- ferase, which is located mainly in the proximal convoluted tubules [26] and mitochondria [27] of rat kidney. NAG is located in the proximal tubules and in lysosomes [28]. VPA, for example, is known to affect and damage the metabolism of the renal cortical tubules in rats [29-31] and dogs [32], and

440 Z Otsuka et aL / Brain & Development 1994; 16:437-40
as a result, u - N A G / u - C r excretion may increase. If thc damage was minimal or limited to the cortical tubules, u- G A A / u - C r production could be maintained by the kidney as a whole, whereas the u - N A G / u - C r level would be abnormal. Our results suggest that the u - N A G / u - C r level is a bet ter marker than the u - G A A / u - C r level for the detect ion of renal damage in A E D therapy. In the polytherapy group there was a significant negative correlation between the u - G A A / u - C r level and the duration of A E D therapy, but the u - G A A / u - C r levels were all within normal limits. This result suggests that the function of the kidney as a whole, as far as it was judged by the u - G A A / u - C r level, will be maintained during chronic A E D therapy.
ACKNOWLEDGEMENTS The authors wish to express their thanks, for assistance in collecting volunteers' urine, to The Kodama Junior High School, its President, Teruo Odaka, Mrs. Yoshiko Maruyama and Mrs. Masako Nakajima; to The Osawa Elementary School and its President, Haruo Taguchi, and Miss Tomoko Naka- hara; and to Mr. Hisaei Nakajima, the Chief of The Department of the Board of Education of Kamisatomachi in Saitama Prefecture.
REFERENCES
1. Lenoir GR, Perignon JL, Gubler MC, Broyer M. Valproic acid: a possible cause of proximal tubular renal syndrome. J Pediatr 1981; 98: 503-4.
2. Lin CY, Chiang H. Sodium-valproate-induced interstitial nephri- tis. Nephron 1988; 48: 43-6.
3. Sheth KJ, Casper JT, Good TA. Interstitial nephritis due to phenytoin hypersensitivity. J Pediatr 1977; 91: 438-41.
4. Hogg R J, Sawyer M, Hecox K, Eigenbrodt E. Carbamazepine induces acute tubulointerstitial nephritis. J Pediatr 1981; 98: 830-2.
5. Brajesh NA. Diphenylhydantoin-induced acute renal failure. Nephron 1977; 18: 249-51.
6. Ray-Chaudhuri K, Pye IF, Boggild M. Hypersensitivity to carba- mazepine presenting with a leukemoid reaction, eosinophilia, erythroderma, and renal failure. Neurology 1989; 39: 436-8.
7. Imai H, Nakamoto Y, Hirokawa M, Akihama T, Miura AB. Carbamazepine-induced granulomatous necrotizing angiitis with acute renal failure. Nephron 1989; 51: 405-8.
8. Novo MLP, Izumi T, Yokota K, Fukuyama Y. Urinary excretion of N-acetyl-/3-glucosaminidase and /3-galactosidase by patients with epilepsy. Brain Dev 1993; 15: 157-60.
9. Tseng CL, Wang PJ, Tsau-YK, Lin MY, Shen YZ. Urinary N-acetyl-/3-glucosaminidase (NAG) in children receiving anti-epi- leptic drugs. Acta Paediatr Sin 1992; 33: 251-6.
10. Ishizaki M, Kitamura H, Takahashi H, Asano H, Miura K, Okazaki H. Evaluation of the efficacy of anti-rejection therapy using the quantitative analysis of guanidinoacetic acid (GAA) urinary excretion as a guide. In: Mori A, Choen BD, Lowenthal A, eds. Guanidines. New York: Plenum, 1985: 353-63.
l 1. Isoda K, Mitarai T, Imamura N, et al. The significance of serum and urinary metabolic function in patients with kidney transplan- tation. In: Mori A, Choen BD, Koide H, eds. Guanidines Vol 2. New York: Plenum, 1989: 337-43.
12. Nako Y. Urinary excretion of guanidinoacetic acid, /32-micro- globulin, and N-acetyl-/3-D-glucosaminidase in neonate (in Japanese). Kitakanto Medical Journal 1991; 41: 545-55.
13. Tsubakihara Y, lida N, Yuasa S, et al. Guanidinoacetic acid (GAA) in patients with chronic renal failure (CRF) and diabetes
mellitus (DM). In: Mori A, Choen BD, Lowenthal A, eds. Guanidines. New York: Plenum, 1985: 306-16.
14. Takano Y. Gejyo F, Shirokane Y, Nakajima M, Arakawa M. Urinary excretion rate of guanidinoacetic acid in essential hyper- tension. Nephron 1988: 48: 167-8.
15. Takano Y, Aoike I, Gejyo F, Arakawa M. Urinary excretion rate of guanidinoacetic acid as a new marker in hypertensive renal damage. Nephron 1989; 52: 273-7.
16. Nakayama S, Junen M, Kiyatake I, Koide H. Urinary guanidi- noacetic acid excretion as an indicator of gentamicin nephrotoxi- city in rats. In: Mori A, Choen BD, Koide H, eds. Guanidines Vol 2. New York: Plenum, 1989: 303-12.
17. Shiraga H, Watanabe Y, Mori A. Guanidino compound levels in the serum of healthy adults and epileptic patients. Epilepsy Res 1991; 8: 142-8.
18. Noto A, Ogawa Y, Mori S, et al. Simple rapid spectrophotometry of urinary N-acetyl-/3-D-glucosaminidase, with use of a new chro- mogenic substrate. Clin Chem 1983; 29: 1713-6.
19. Shirokane Y, Utsushikawa M, Nakajima M. A new enzymic determination of guanidinoacetic acid in urine. Clin Chem 1987; 33: 394-7.
20. Sugita O, Uchiyama K, Yamada T, Sato T, Okada M, Takeuchi K. Reference value of serum and urine creatinine, and of creati- nine clearance by a new enzymatic method. Ann Clin Biochem 1992; 29: 523-8.
21. Camfield C, Camfield P, Smith E, Tibbles JAR. Asymptomatic children with epilepsy: little benefit from screening for anticon- vulsant-induced liver, blood, or renal damage. Neurology 1986; 36: 838-41.
22. Murakami M, Yamamoto H, Ueda Y, Murakami K, Yamauchi K. Urinary screening of elementary and junior high-school chil- dren over a 13-year period in Tokyo. Pediatr Nephrol 1991; 5: 50-3.
23. Price RG, Dance N, Richards B, Cattle WR. The excretion of N-acetyl-/3-glucosaminidase and /3-galactosidase following surgery to the kidney. Clin Chim Acta 1970; 27: 57-72.
24. Scherberich JE. Urinary proteins of tubular origin. Am J Nephrol 1990; 10 (suppl 1): 43-51.
25. Tasaki K, Yoshida K, Gejyo F, Arakawa M. Metabolism of guanidinoacetic acid in renal tubular tissue culture. In: Mori A, Choen BD, Koide H, eds. Guanidines Vol 2. New York: Plenum, 1989: 323-9.
26. McGuire DM, Gross MD, Elde RP, Van Pilum JF. Localization of l.-arginine-glycine amidinotransferase protein in rat tissue by immunofluorescence microscopy. J Histochem Cytochem 1986; 34: 429-35.
27. Margi E, Baldoni G, Grazi E. On the biosynthesis of creatinine. Intramitochondrial localization of transaminidase from rat kid- ney. FEBS Lett 1975; 55: 91-3.
28. Kunin CM, Chesney RW, Craig WA, England AC, DeAngelis C. Enzymuria as a marker of renal injury and disease. Pediatrics 1978; 62: 751-60.
29. Ponchaut S, Draya JP, Veitch K, Hoof FV. Influence of chronic administration of valproate on ultrastructure and enzyme con- tent of peroxisomes in rat liver and kidney. Biochem Pharmacol 1991; 41: 1419-28.
30. Doval M, Culebras M, Lopez-Farre A, et al. Effect of valproate on lactate and glutamine metabolism by rat renal cortical tubules. Proc Soc Exp Biol Med 1989; 1911: 357-64.
31. Rumbach L, Cremel G, Marescaux C, Warter JM, Waksman A. Valproate-induced hyperammonemia of renal origin. Biochem Pharmacol 1989; 38: 3963-7.
32. Gougoux A, Vinay P. Metabolic effects of valproate on dog renal cortical tubules. Can J Physiol Pharmacol 1989; 67: 88-97.