Tumor necrosis factor-α gene expression in diabetic nephropathy: Relationship with urinary albumin...
5
Kidney International, Vol. 68, Supplement 99 (2005), pp. S98–S102 Tumor necrosis factor-a gene expression in diabetic nephropathy: Relationship with urinary albumin excretion and effect of angiotensin-converting enzyme inhibition JUAN F. NAVARRO,FRANCISCO J. MILENA,CARMEN MORA,CANDELARIA LE ´ ON,F ELIX CLAVERIE, CARLOS FLORES, and J AVIER GARC´ ıA Servicio de Nefrolog´ ıa, Unidad de Investigaci ´ on, y Servicio de Bioqu´ ımica Cl´ ınica, Hospital Universitario Nuestra Se ˜ nora de Candelaria, Tenerife, Spain; and Consejo Superior de Investigaciones Cient´ ıficas, Centro de Investigaciones Biol´ ogicas, Madrid, Spain Tumor necrosis factor-a gene expression in diabetic nephropa- thy: Relationship with urinary albumin excretion and effect of angiotensin-converting enzyme inhibition. Background. The pathogenic mechanisms and molecular events involved in the development and progression of diabetic nephropathy (DN) are not completely known. Recent data in- dicate that diabetes includes an inflammatory component that is related to diabetic complications. Tumor necrosis factor (TNF)- a, a cytokine with mainly proinflammatory activity, may be syn- thesized by renal cells. Our objective was to analyze intrarenal TNF-a gene expression and its relationship with urinary albu- min excretion (UAE). We also investigated the effect of inhi- bition of angiotensin-converting enzyme on TNF-a expression and UAE. Methods. Streptozotocin-induced diabetic rats received either no treatment or an angiotensin-converting enzyme in- hibitor (enalapril). After eight weeks, renal expression of TNF- a was evaluated by real-time polymerase chain reaction. Results. Renal cortical messenger RNA levels of TNF-a in- creased significantly and were twice as high in diabetic rats than in nondiabetic control rats. Enalapril administration nearly completely abolished the increase in TNF-a messenger RNA expression to the level observed in control rats. UAE was sig- nificantly correlated with urinary levels of TNF-a (r = 0.68, P < 0.05) and with renal TNF-a expression (r = 0.51, P < 0.05). Conclusion. DN was associated with increased renal expres- sion of TNF-a and UAE. Enalapril administration prevented this enhanced expression of TNF-a and decreased urinary cy- tokine excretion and albuminuria. These data provide a novel insight into the pathogenic mechanisms of DN, and support the hypothesis that inflammatory mechanisms may play a signifi- cant role in the development and progression of renal injury secondary to diabetes mellitus. Diabetic nephropathy (DN) is the leading cause of re- nal failure throughout the world. The exact pathogenic Key words: albuminuria, diabetic nephropathy, inflammation, tumor necrosis factor-a. C 2005 by the International Society of Nephrology mechanisms and the molecular events leading to the de- velopment and progression of this complication remain incompletely understood. The renin-angiotensin system (RAS) is critically im- portant in the earliest glomerular hemodynamic distur- bances observed in DN [1]. Angiotensin II (Ang II) is another key factor regulating the expression and synthe- sis of growth factors, chemokines, adhesion molecules, and cytokines that are involved in processes such as cell growth, apoptosis, fibrosis, and inflammation [2, 3]. There now are convincing data that diabetes includes an inflammatory component thought to be related to di- abetic complications. Plasma concentrations of inflam- matory molecules, including proinflammatory cytokines, are elevated in diabetic patients [4–6]. Recent studies have shown that the concentrations of these substances increase as nephropathy progresses [7, 8], and that these inflammatory molecules are independently related to uri- nary albumin excretion (UAE) [8, 9]. Cytokines are polypeptides that regulate immune and inflammatory events. Tumor necrosis factor-a (TNF-a ) is a proinflammatory cytokine with a wide range of bio- logic effects including the stimulation of the production of prostaglandins, platelet-activating factor, and plasmino- gen activator inhibitor; chemotaxis; the induction of ad- hesion molecules expression; and the synthesis of other inflammatory mediators [10, 11]. Renal cells are capable of synthesizing TNF-a , which may act in a paracrine or autocrine manner to induce a variety of effects on differ- ent renal structures [10–12]. There is growing evidence that proinflammatory cytokines play a significant role in the development and progression of several renal disor- ders [11], including DN [9, 13–15]. The aims of this preliminary study were to analyze the intrarenal gene expression of TNF-a in streptozotocin- induced diabetic rats and to investigate the relationship between TNF-a expression and the urinary excretion of S-98
Transcript of Tumor necrosis factor-α gene expression in diabetic nephropathy: Relationship with urinary albumin...

Kidney International, Vol. 68, Supplement 99 (2005), pp. S98–S102
Tumor necrosis factor-a gene expression in diabeticnephropathy: Relationship with urinary albumin excretion andeffect of angiotensin-converting enzyme inhibition
JUAN F. NAVARRO, FRANCISCO J. MILENA, CARMEN MORA, CANDELARIA LEON, FELIX CLAVERIE,CARLOS FLORES, and JAVIER GARCıA
Servicio de Nefrologıa, Unidad de Investigacion, y Servicio de Bioquımica Clınica, Hospital Universitario Nuestra Senora deCandelaria, Tenerife, Spain; and Consejo Superior de Investigaciones Cientıficas, Centro de Investigaciones Biologicas,Madrid, Spain
Tumor necrosis factor-a gene expression in diabetic nephropa-thy: Relationship with urinary albumin excretion and effect ofangiotensin-converting enzyme inhibition.
Background. The pathogenic mechanisms and molecularevents involved in the development and progression of diabeticnephropathy (DN) are not completely known. Recent data in-dicate that diabetes includes an inflammatory component that isrelated to diabetic complications. Tumor necrosis factor (TNF)-a, a cytokine with mainly proinflammatory activity, may be syn-thesized by renal cells. Our objective was to analyze intrarenalTNF-a gene expression and its relationship with urinary albu-min excretion (UAE). We also investigated the effect of inhi-bition of angiotensin-converting enzyme on TNF-a expressionand UAE.
Methods. Streptozotocin-induced diabetic rats receivedeither no treatment or an angiotensin-converting enzyme in-hibitor (enalapril). After eight weeks, renal expression of TNF-a was evaluated by real-time polymerase chain reaction.
Results. Renal cortical messenger RNA levels of TNF-a in-creased significantly and were twice as high in diabetic ratsthan in nondiabetic control rats. Enalapril administration nearlycompletely abolished the increase in TNF-a messenger RNAexpression to the level observed in control rats. UAE was sig-nificantly correlated with urinary levels of TNF-a (r = 0.68, P <
0.05) and with renal TNF-a expression (r = 0.51, P < 0.05).Conclusion. DN was associated with increased renal expres-
sion of TNF-a and UAE. Enalapril administration preventedthis enhanced expression of TNF-a and decreased urinary cy-tokine excretion and albuminuria. These data provide a novelinsight into the pathogenic mechanisms of DN, and support thehypothesis that inflammatory mechanisms may play a signifi-cant role in the development and progression of renal injurysecondary to diabetes mellitus.
Diabetic nephropathy (DN) is the leading cause of re-nal failure throughout the world. The exact pathogenic
Key words: albuminuria, diabetic nephropathy, inflammation, tumornecrosis factor-a.
C© 2005 by the International Society of Nephrology
mechanisms and the molecular events leading to the de-velopment and progression of this complication remainincompletely understood.
The renin-angiotensin system (RAS) is critically im-portant in the earliest glomerular hemodynamic distur-bances observed in DN [1]. Angiotensin II (Ang II) isanother key factor regulating the expression and synthe-sis of growth factors, chemokines, adhesion molecules,and cytokines that are involved in processes such as cellgrowth, apoptosis, fibrosis, and inflammation [2, 3].
There now are convincing data that diabetes includesan inflammatory component thought to be related to di-abetic complications. Plasma concentrations of inflam-matory molecules, including proinflammatory cytokines,are elevated in diabetic patients [4–6]. Recent studieshave shown that the concentrations of these substancesincrease as nephropathy progresses [7, 8], and that theseinflammatory molecules are independently related to uri-nary albumin excretion (UAE) [8, 9].
Cytokines are polypeptides that regulate immune andinflammatory events. Tumor necrosis factor-a (TNF-a)is a proinflammatory cytokine with a wide range of bio-logic effects including the stimulation of the production ofprostaglandins, platelet-activating factor, and plasmino-gen activator inhibitor; chemotaxis; the induction of ad-hesion molecules expression; and the synthesis of otherinflammatory mediators [10, 11]. Renal cells are capableof synthesizing TNF-a, which may act in a paracrine orautocrine manner to induce a variety of effects on differ-ent renal structures [10–12]. There is growing evidencethat proinflammatory cytokines play a significant role inthe development and progression of several renal disor-ders [11], including DN [9, 13–15].
The aims of this preliminary study were to analyze theintrarenal gene expression of TNF-a in streptozotocin-induced diabetic rats and to investigate the relationshipbetween TNF-a expression and the urinary excretion of
S-98

Navarro et al: TNF-a gene expression in diabetic nephropathy S-99
TNF-a and albumin. We also studied the effect of inhibi-tion of angiotensin-converting enzyme (ACE) on thesevariables.
METHODS
Animals and experimental model
Twelve-week-old male Sprague Dawley rats (CharlesRiver Laboratories, Barcelona, Spain) weighing 150 to250 g were maintained on standard rodent chow andgiven tap water ad libitum. The animals were housedin a temperature-controlled (21 ± 1◦C) and humidity-controlled (60 ± 10%) room with a 12-hour dark/lightcycle. Animals were treated according to the Directiveby the Council of the European Communities (86/609/CEE) and the Directive by the European Parliament(2003/65/CE) on the protection of animals used for ex-perimental and other scientific purposes.
Experimental diabetes was induced by intraperitonealinjection of 65 mg/kg streptozotocin (STZ; Sigma, St.Louis, MO, USA) freshly dissolved in 0.9% sodium chlo-ride. To confirm the diabetic state, blood glucose concen-tration was measured three days after STZ injection. Thediabetic animals were divided into two groups (N = 6 ineach group): group A received no treatment and groupB received the ACE inhibitor enalapril maleate (Merck& Co, Inc., Rahway, NJ, USA) dissolved in drinking wa-ter (100 mg/L). None of the diabetic animals receivedinsulin treatment. Six animals served as nondiabetic con-trols (group C).
After eight weeks of follow-up, all animals were anes-thetized with an intraperitoneal injection of thiopental(40 mg/kg) and bled completely by cardiac puncture. Thekidneys were removed rapidly from each rat. The rightkidney was decapsulated and the cortex excised, placedon RNAlater stabilization solution (Ambion Inc., Austin,TX, USA), and stored at −80◦C. The left kidney was fixedin 10% phosphate-buffered formalin.
Total RNA isolation, reverse transcription, primers, andreal-time polymerase chain reaction
Total RNA was extracted from rat kidneys withTRIreagent (SIGMA, Steinheim, Germany) as describedin the manufacturer’s instructions. Isolated RNA wastreated with 5 U of RNase-free, FPLC pure DNase I(Amersham Pharmacia, Piscataway, NJ, USA) in thepresence of RNAguard RNase Inhibitor (AmershamPharmacia), followed by phenol-chloroform extraction.Total RNA integrity was checked by agarose gel elec-trophoresis and ethidium bromide staining, and wassubsequently used to synthesize cDNA with random hex-amers using the First Strand cDNA Synthesis Kit (Roche,Basel, Switzerland) with 20 U of AMV Reverse Tran-scriptase at 42◦C.
Polymerase chain reaction (PCR) primers were de-signed for an annealing temperature of 60◦C using Primer3 software (http://frodo.wi.mit.edu/cgi-bin/primer3/primer3 www.cgi; Whiteheed Institute for BiomedicalResearch, Cambridge, MA, USA), except for b-actinprimers, which also anneal at 60◦C. The primer constructs(5′–3′ sequence) were: b-actin forward, TCCCTGGA-GAAGAGCTACGA (size, 362 bp), and TNF-a forward,CCACCACGCTCTTCTGT (150 bp). Reactions wereoptimized to a final volume of 25 lL with 1 × reactionbuffer, 0.2 mmol/L of each deoxynucleotide, 2.5 mmol/LMgCl2, 0.15 lmol/L of each primer, 1:100,000 SYBRGreen I (Molecular Probes, Leiden, Netherlands), and0.4 U of HotStart DNA Taq Polymerase (Ecogen/Bio-line, Madrid, Spain). Fluorescein was added to a finaldilution of 1:100,000 to normalize any differences in theamount of intercalating dyes caused by pipetting errors.Real-time PCR amplification was performed on aniCycler iQ Real Time PCR system (BioRad, Hercules,CA, USA) and analyzed with the provided software(iCycler software version 3.0). A three-step run protocolwas used: (1) an initial hold of nine minutes at 95◦C toactivate Taq polymerase and a fluorescence measure-ment to normalize the whole plate amount of fluoresceindye; (2) an amplification and quantification cycle with45 repeats (denaturation 20 seconds at 95◦C, annealing20 seconds at 60◦C and extension 20 seconds at 72◦Cwith a fluorescence measurement); and (3) a meltingcurve analysis from 65◦C to 95◦C to check the specificityof the amplified product. Agarose gel electrophoresiswas performed to confirm single-product amplificationswithout primer dimers. All fragments were also checkedfor specificity by direct sequencing of both strands withan ABI PRISM 310 Genetic Analyzer using Big DyeTerminator kit v 3.1 (Applied Biosystems, Foster City,CA, USA). After PCR amplification, values of the thres-hold cycle (Ct) were obtained for each sample anddefined as the point at which the fluorescence rises app-reciably above the background fluorescence. To obtainthe relative expression level, the Ct value of each geneof interest was normalized to the Ct value of thehousekeeping b-actin gene. The expression level ofcytokine mRNA was expressed as an arbitrary ratio ofthe quantity of RNA to that of b-actin.
Laboratory analysis and cytokine measurements
Serum blood glucose concentration was determinedby standard techniques. Urine samples were collectedfrom rats housed in metabolic cages. Urinary excretion ofTNF-a was measured by enzyme-linked immunosorbentassay using specific kits (Bender MedSystems GmbH,Vienna, Austria). The sensitivity was 17 pg/mL, and theintra- and inter-assay precision was <5% and 10%, re-spectively. Urinary albumin excretion was measured bynephelometry.

S-100 Navarro et al: TNF-a gene expression in diabetic nephropathy
Table 1. Physiologic and metabolic data at baseline and the end ofthe study
Variable Group Baseline Eight weeks
Body weight gDiabetic 198 ± 34 204 ± 60a
Diabetics + enalapril 227 ± 25 238 ± 54a
Nondiabetic control 190 ± 34 288 ± 52Blood glucose mg/dL
Diabetic 234 ± 16b 300 ± 92b
Diabetics + enalapril 313 ± 14b,c 295 ± 71b
Nondiabetic control 77 ± 8 88 ± 17
Baseline, 72 hours after streptozotocin injection.aP < 0.05.bP < 0.01 vs. nondiabetic control group.cP < 0.01, dP < 0.05 vs. diabetic group.
Statistical analysis
Results are expressed as mean ± SD, except for TNF-a data, which are presented as median and range. Datafrom the three groups were compared using Kruskal-Wallis analysis of variance. Regression analysis was per-formed with the Spearman rank correlation test. P <
0.05 was considered significant. Statistical analyses wereperformed using Statistica 5.5 (Statsoft Inc., Tulsa, OK,USA).
RESULTS
Table 1 summarizes the animals’ body weights andblood glucose concentrations at baseline (72 hours afterSTZ injection) and after eight weeks of follow-up. Bloodglucose concentration was significantly higher in diabeticthan in nondiabetic animals. The blood glucose concen-tration did not differ significantly between diabetic ratstreated with enalapril (group B) and untreated diabeticrats (group A). Basal mean body weights were similarbetween the three groups. However, at the end of thestudy, body weights were significantly lower in diabeticrats (groups A and B) than nondiabetic animals (groupC); body weight did not differ significantly between dia-betic groups A and B.
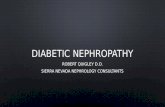
The mean basal levels of b-actin mRNA were simi-lar between groups for each set of PCR reactions, con-firming that the starting concentrations of cDNA weresimilar and not subjected to systematic error. The expres-sion level of TNF-a at the end of the study in diabeticrats (group A) was more than double the value in con-trol animals (group C) (Fig. 1). Interestingly, treatmentwith enalapril virtually abolished the elevation in mRNAlevels for TNF-a so that the expression level in enalapril-treated rats (group B) did not differ significantly fromthat in control rats (Fig. 1).
TNF-a was not detectable in the urine of four controlrats. In contrast, urinary levels of TNF-a were detectablein all untreated diabetic rats. In rats receiving enalapril,TNF-a was not detectable in two animals, and the average
Group A Group B Group C
Not significant
*
3
2.5
2
1.5
1
0.5
0
Exp
ress
ion
ratio
Fig. 1. Quantitation of mRNA (normalized expression) for the proin-flammatory cytokine TNF-a in untreated diabetic rats (group A),enalapril-treated diabetic rats (group B), and nondiabetic control rats(group C). ∗P < 0.05 vs. groups B and C.
urinary concentration in the other four rats (22.8 pg/mL;range, 11.3–30.1) did not differ from the value in the con-trol animals (13.5 pg/mL; range, 11.8–15.9) but was signifi-cantly lower than in untreated animals (109 pg/mL; range,89.4–142; P < 0.01). Basal UAE did not differ betweengroups. However, at the end of the study, UAE was sig-nificantly higher in untreated diabetic rats (10.6 mg/day;range, 7.44–18.2) than in enalapril-treated (1.1 mg/day;range, 0.66–2.43) and control rats (1.98 mg/day; range,0.69–3.7) (P < 0.01 for each). UAE did not differ signifi-cantly between groups B and C.
The urinary level of TNF-a was significantly correlatedwith renal expression of TNF-a (r = 0.60, P < 0.05) andwith UAE (r = 0.68, P < 0.05). Renal expression of TNF-a was significantly correlated with UAE (r = 0.51, P <
0.05).
DISCUSSION
The levels of proinflammatory cytokines increasein diabetic patients, suggesting that inflammation maybe related to diabetic complications [4–9, 16]. In1991, Hasegawa et al [15] reported that peritonealmacrophages incubated with glomerular basement mem-branes from diabetic rats produced greater levels of TNF-a and interleukin (IL)-1 than macrophages incubatedwith membranes from normal rats. These authors sug-gested that proinflammatory cytokines might be involvedin the development of DN. Previous studies have shownthat mRNA levels of TNF-a increase in the glomeruliof diabetic rats for a long time (24 and 52 weeks) af-ter induction of diabetes [17, 18]. In contrast, a recentstudy showed that TNF-a mRNA increases in proximaltubule cells isolated from diabetic rats as early as 10 daysafter induction of diabetes [19]. Nakamura et al [17] re-ported a doubling of TNF-a mRNA expression in theglomeruli of diabetic rats after four weeks and triplingafter 12 weeks. In our study, eight weeks after induction

Navarro et al: TNF-a gene expression in diabetic nephropathy S-101
of diabetes, TNF-a mRNA expression was more thandouble the basal level, an intermediate value to thoseobserved by Nakamura et al.
TNF-a is one of the main proinflammatory cytokinesand may be produced intrinsically in renal cells [20]. Itis important to note that increased urinary and renalinterstitial concentrations of TNF-a precede the rise inalbuminuria [21, 22]. TNF-a is cytotoxic to glomerular,mesangial, and epithelial cells, and may induce direct re-nal damage [23, 24]. Moreover, TNF-a has a direct ef-fect on the protein permeability barrier of the glomerulus[25], independent of alterations in hemodynamic factorsor effects of recruited inflammatory cells. In our study,TNF-a expression was closely related to its urinary ex-cretion, and urinary excretion of TNF-a was positivelycorrelated with UAE. Interestingly, the decrease in TNF-a mRNA expression after enalapril treatment was asso-ciated with a reduction in both albuminuria and urinaryTNF-a excretion to levels similar to those observed innondiabetic control rats. These findings strongly suggestan intrarenal production of TNF-a, which may have a rolein the development and progression of renal damage inDN.
Ang II has important effects beyond its hemodynamicactions, including regulation of cell growth and extracel-lular matrix production, and shares many intracellularsignaling mechanisms with classic cytokines. Several cel-lular events are attributed to the newly identified prop-erties of Ang II, which seem to coincide with key stepsin inflammation [2, 3]. Recent data show that Ang II isa critical factor in the regulation of proinflammatory cy-tokine gene expression and synthesis, and that human pe-ripheral monocytes are able to produce TNF-a and IL-1when stimulated with Ang II [26, 27]. In rat renal resi-dent macrophages, Ang II upregulates TNF-a and IL-6gene expression [28], and incubation of tubules from themedullary thick ascending limb with Ang II promotesaccumulation of TNF-a mRNA [29]. Moreover, Ang IIinfusion into normal rats stimulates renal production ofthe proinflammatory cytokines TNF-a and IL-6 [30]. Wehypothesize that other angiotensin-dependent processes,such as those related to proinflammatory cytokine regu-lation, may play a significant role in the development andprogression of DN.
Evidence now indicates that inflammatory phenomenaare also involved in translating the primary metabolic andhemodynamic insults into renal damage in DN [21, 22, 31,32]. Modulation of these inflammatory processes mightbe useful in preventing or designing therapeutic agentsfor this complication. Utimura et al [33] demonstratedthat treating development of DN can be prevented bytreating diabetic rats with mycophenolate mofetil, andthat these actions were related to its antiproliferativeand anti-inflammatory properties instead of favorablemetabolic or hemodynamic effects. In a recent study,
DiPetrillo et al [19] showed that treatment of diabetic ratswith pentoxifylline, a substance with anti-TNF-a proper-ties, decreased renal TNF-a expression and urinary TNF-a excretion. Other studies have shown that pentoxifyllineadministration to diabetic patients significantly reducesurinary protein excretion and TNF-a levels [34–36], andthat the reduced proteinuria is significantly associatedwith the decrease in TNF-a [35, 36].
Accumulating evidence implies that ACE inhibitorshave beneficial properties beyond their originally iden-tified effects. Modulating inflammatory phenomena byblocking the RAS in DN is of great interest. Our studyshowed that the ACE inhibitor enalapril normalized therenal overexpression of TNF-a in diabetic rats, and thatthis effect was associated with a significant reduction inrenal cytokine production and UAE. Previous experi-mental investigations have shown that ACE inhibitorshave potent inhibitory effects on proinflammatory cy-tokine expression and synthesis [37–39]. Clinical stud-ies in patients with congestive heart failure or advancedchronic renal disease have demonstrated that therapywith ACE inhibitors decreases TNF-a and IL-6 activity[40, 41].
CONCLUSION
Our data show that TNF-a, one of the main proinflam-matory cytokines, is overexpressed in a rat model of DN,and that this overexpression is significantly associatedwith evidence of renal damage, such as UAE. Blockadeof RAS by enalapril prevents the enhanced expressionof TNF-a and reduces UAE. These data provide a novelinsight into the pathogenic mechanisms of DN, and sup-port the hypothesis that inflammatory phenomena, alongwith regulatory effects mediated by Ang II, may play asignificant role in renal injury secondary to diabetes mel-litus. Our data also suggest a need to study the potentialrenoprotective effects of therapies that modulate inflam-matory processes.
ACKNOWLEDGMENTS
This study was supported by Sociedad Espanola de Nefrologıa, Fun-dacion Canaria de Investigacion y Salud, and Asociacion Cientıfica parala Investigacion Nefrologica.
Reprint requests to Juan F. Navarro, M.D., Servicio de Nefrologıa,Hospital Universitario Nuestra Senora de Candelaria, 38010 Santa Cruzde Tenerife, Spain.E-mail: [email protected]
REFERENCES
1. ZATZ R, DUNN BR, MEYER TW, et al: Prevention of diabeticglomerulopathy by pharmacologic amelioration of glomerular cap-illary hypertension. J Clin Invest 77:1925–1930, 1986
2. SADOSHIMA J: Cytokine actions of angiotensin II. Circ Res 86:1187–1189, 2000

S-102 Navarro et al: TNF-a gene expression in diabetic nephropathy
3. RUIZ-ORTEGA M, LORENZO O, SUZUKI Y, et al: Proinflammatoryactions of angiotensins. Curr Opin Nephrol Hypertens 10:321–329,2001
4. PICKUP J, MATTOCK M, CHUSNEY G, BURT D: NIDDM as a disease ofthe innate immune system: Association of acute-phase reactants andinterleukin-6 with metabolic syndrome X. Diabetologia 40:1286–1292, 1997
5. KATSUKI A, SUMIDA Y, MURASHIMA S, et al: Serum levels of tumornecrosis factor-a are increased in obese patients with noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab 83:859–862,1998
6. PICKUP J, CHUSNEY G, THOMAS S, BURT D: Plasma interleukin-6,tumor necrosis factor alpha and blood cytokine production in type2 diabetes. Life Sci 67:291–300, 2000
7. BRUNO G, MERLETTI F, BIGGERI A, et al: Casale Monferrato Study:Progression to overt nephropathy in type 2 diabetes. Diabetes Care26: 2150–2155, 2003
8. FESTA A, D’AGOSTINO R JR, HOWARD G, et al: Inflammation andmicroalbuminuria in nondiabetic and type 2 diabetic subjects: TheInsulin Resistance Atherosclerosis Study. Kidney Int 58:1703–1710,2000
9. NAVARRO JF, MORA C, MACıA M, GARCıA J: Inflammatory param-eters are independently associated with urinary albumin excretionin type 2 diabetes mellitus. Am J Kidney Dis 42:53–61, 2003
10. MARIANO F, BUSSOLATI B, PICCOLI G, CAMUSSI B: Renal vasculareffects of cytokines. Blood Purif 15:262–272, 1997
11. NORONHA IL, NIEMIR Z, STEIN H, WALDHERR R: Cytokines andgrowth factors in renal disease. Nephrol Dial Transplant 10:775–786, 1995
12. OSTENDORF T, BURG M, FLOEGE J: Cytokines and glomerular injury.Kidney Blood Press Res 19:281–289, 1996
13. NAVARRO J: Nefropatıa diabetica: ¿Una cuestion de inflamacion?Hipotesis del dano renal inflamatorio en la diabetes mellitus tipo 2.Nefrologıa 23:381–389, 2003
14. MORA C, NAVARRO J: Inflammation and pathogenesis of diabeticnephropathy. Metabolism 53:265–266, 2004
15. HASEGAWA G, NAKANO K, MANABU S, et al: Possible role of tumornecrosis factor and interleukin-1 in the development of diabeticnephropathy. Kidney Int 40:1007–1012, 1991
16. SEKIZUKA K, TOMINO Y, SEI C, et al: Detection of serum IL-6 inpatients with diabetic nephropathy. Nephron 68:284–285, 1994
17. NAKAMURA T, FUKUI M, EBIHARA I, et al: mRNA expression ofgrowth factors in glomeruli from diabetic rats. Diabetes 42:450–456,1993
18. SUGIMOTO H, SHIKATA K, WADA J, et al: Advanced glycation endproducts-cytokine oxide sequence pathway in the development ofdiabetic nephropathy: Aminoguanidine ameliorates the overex-pression of tumour necrosis factor-a and inducible nitric oxide syn-thase in diabetic rat glomeruli. Diabetologia 42:878–886, 1999
19. DIPETRILLO K, GESEK FA: Pentoxifylline ameliorates renal tumornecrosis factor expression, sodium retention, and renal hypertrophyin diabetic rats. Am J Nephrol 24:352–359, 2004
20. EMANCIPATOR SN, SEDOR JR: Cytokines and renal disease, in Cy-tokines in Health and Disease: Physiology and Pathophysiology,edited by Kunkel SL, Remick DG, New York, Marcel Dekker Inc.,1992, pp 467–488
21. KALANTARINIA K, AWAS AS, SIRAGY HM: Urinary and renal intersti-tial concentrations of TNF-a increase prior to the rise in albuminuriain diabetic rats. Kidney Int 64:1208–1213, 2003
22. DIPETRILLO K, COUTERMARSH B, GESEK FA: Urinary tumor necrosisfactor contributes to sodium retention and renal hypertrophy duringdiabetes. Am J Physiol Renal Physiol 284:F113–F121, 2003
23. BERTANI T, ABBATE M, ZOJA C, et al: Tumor necrosis factor inducesglomerular damage in rabbit. Am J Pathol 134:419–430, 1989
24. ORTIZ A, GONZALEZ-CUADRADO S, BUSTOS C, et al: Tumor necro-sis factor as a mediator of glomerular damage. J Nephrol 8:27–34,1995
25. MCCARTHY E, SHARMA R, SHARMA M, et al: TNF-a increases albu-min permeability of isolated rat glomeruli through the generationof superoxide. J Am Soc Nephrol 9:433–438, 1998
26. DORFFEL Y, LATSCH C, STUHLMULLER B, et al: Preactivated periph-eral blood monocytes in patients with essential hypertension. Hy-pertension 34:113–117, 1999
27. HAHN AW, JONAS U, BUHLER FR, RESINK TJ: Activation of humanperipheral monocytes by angiotensin II. FEBS Lett 347:178–180,1994
28. FERRERI N, ESCALANTE A, ZHAO Y, et al: Angiotensin II induces TNFproduction by the thick ascending limb: Functional implications.Am J Physiol Renal Physiol 243:F148–F155, 1998
29. NAKAMURA A, JOHNS EF, IMAIZUMI A, et al: Effect of beta(2)-adrenoceptor activation and angiotensin II on tumour necrosis fac-tor and interleukin 6 gene transcription in the rat renal residentmacrophage cells. Cytokine 11:759–765, 1999
30. RUIZ-ORTEGA M, RUPEREZ M, LORENZO O, et al: Angiotensin II reg-ulates the synthesis of proinflammatory cytokines and chemokinesin the kidney. Kidney Int 62(Suppl 82):S12–S22, 2002
31. YOUNG BA, JOHNSON RJ, ALPERS CE, et al: Cellular events in theevolution of experimental diabetic nephropathy. Kidney Int 47:935–944, 1995
32. CORTES P, ZHAO X, RISER BL, NARINS RG: Role of glomerular me-chanical strain in the pathogenesis of diabetic nephropathy. KidneyInt 51:57–68, 1997
33. UTIMURA R, FUJIHARA CK, MATTAR AL, et al: Mycophenolatemofetil prevents the development of glomerular injury in experi-mental diabetes. Kidney Int 63:209–216, 2003
34. GUERRERO-ROMERO F, RODRıGUEZ-MORAN M, PANIAGUA-SIERRA J,et al: Pentoxifylline reduces proteinuria in insulin-dependent andnon-dependent diabetic patients. Clin Nephrol 43:116–121, 1995
35. NAVARRO JF, MORA C, RIVERO A, et al: Urinary protein excretionand serum tumor necrosis factor in diabetic patients with advancedrenal failure: Effects of pentoxifylline administration. Am J KidneyDis 33:458–463, 1999
36. NAVARRO J, MORA C, MUROS M, GARCıA J: Additive antiproteinuriceffect of pentoxifylline in type 2 diabetic patients under angiotensinII receptor blockade: A short term randomised controlled trial. JAm Soc Nephrol 16:2119–2125, 2005
37. KANETO H, MORRISEY JJ, MCCRACKEN R, et al: The expression ofmRNA for tumor necrosis factor a increases in the obstructed kid-ney of rats soon after unilateral ureteral ligation. Nephrology 2:161–166, 1996
38. PEETERS AC, NETEA MG, KULLBERG BJ, et al: The effect of renin–angiotensin system inhibitors on pro- and anti-inflammatory cy-tokine production. Immunology 94:376–379, 1998
39. WE GC, SIROI Mg, QU R, et al: Effects of quinapril on myocardialfunction, ventricular remodelling and cardiac cytokine expression incongestive heart failure in the rat. Cardiovasc Drugs Ther 16:29–36,2002
40. GULLESTAD L, AUKRUST P, UELAND T, et al: Effect of high- versuslow-dose angiotensin converting enzyme inhibition on cytokine pro-duction levels in chronic heart failure. J Am Coll Cardiol 34:2061–2067, 1999
41. STENVINKEL P, ANDERSON P, WANG T, et al: Do ACE-inhibitors sup-press tumor necrosis factor-alpha production in advanced chronicrenal failure? J Intern Med 246: 503–507, 1999


![of senescence and angiotensin II on expression and processingof … · 2018-01-31 · including Alzheimer’s disease (AD) [1-4]. The amyloid cascade hypothesis remains the most frequently](https://static.fdocument.org/doc/165x107/5e453e9defc5be29bb7ef72b/of-senescence-and-angiotensin-ii-on-expression-and-processingof-2018-01-31-including.jpg)