TNF-α antagonists and nail psoriasis: an open, 24-week, prospective cohort study in adult patients...
5
1. Introduction 2. Materials and methods 3. Results 4. Discussions Original Research TNF-a antagonists and nail psoriasis: an open, 24-week, prospective cohort study in adult patients with psoriasis Rosita Saraceno † , Lucia Pietroleonardo, Annamaria Mazzotta, Arianna Zangrilli, Luca Bianchi & Sergio Chimenti University of Rome Tor Vergata, U.O.C. of Dermatology, Rome, Italy Introduction: Treatment of nail psoriasis can be challenging and unsatisfac- tory. The aim of this study was to compare the efficacy of three different anti-TNF-a agents on nail psoriasis in patients affected by psoriasis. Materials and methods: Seventy-two patients with nail psoriasis were evalu- ated in this open, 24 weeks, prospective study. Patients were enrolled in three groups of treatment: adalimumab, etanercept or infliximab. Severity of nail psoriasis was assessed by the Nail Psoriasis Severity Index (NAPSI) at baseline, week 14, and 24. Results: Sixty patients were included in the study. The mean NAPSI was 33.77. In the adalimumab group, the mean NAPSI score was 33.1 (± 14.9) at baseline, 21 (± 8.91) at week 14 and 11.4 (± 4.6) at week 24 (p < 0.0002). In the etaner- cept group, the mean NAPSI was 34.8 (± 12.38) at baseline, 23.6 (± 10.43) at week 14, and 10.6 (± 5.25) at week 24 (p < 0.0016). In the infliximab group, the mean NAPSI was 33.3 (± 9.76) at baseline, 14.9 (± 4.20) at week 14 (p < 0.001) and 3.1 (± 3.27) at week 24 (p < 0.00001). At week 14 efficacy was higher in infliximab group compared to adalimumab and etanercept groups (p < 0.05). Conclusions: Among the three agents, in the infliximab group a significant improvement in nail psoriasis was observed as early as week 14 of therapy whereas in the adalimumab and etanercept groups at week 24. Keywords: adalimumab, etanercept, infliximab, nail psoriasis, NAPSI Expert Opin. Biol. Ther. (2013) 13(4):469-473 1. Introduction Nail psoriasis is reported in 10 -- 50% of psoriatic patients [1]. The incidence of nail involvement is higher among patients affected with psoriatic arthritis than among those with psoriasis alone [2]. The frequency of nail psoriasis is reported between 63% and 83% of psoriatic arthritis patients [3,4]. Nail psoriasis may vary from slight to debilitating forms, with functional and psychosocial impairments as well as severe impact on patient’s quality of life [5]. The nail involvement is generally associated with pain, restrictions in daily life activities and the visibility of fingernail disease may hinder social and business interactions. Treatment is challenging and often unsatisfactory and less than 50% of patients experience effective treatments [5]. The therapeutic options include corticosteroids, vitamin D3 analogues, tazarotene, 5-fluorouracil, urea, anthralin, cyclosporine, methotexate and radiotherapy [1,6,7]. Adalimumab, etanercept and infliximab are anti-TNF-a drugs used for the treat- ment of plaque-type psoriasis and psoriatic arthritis. Studies performed in large cohort of patients affected by moderate-to-severe plaque-type psoriasis and psoriatic arthritis demonstrated the efficacy of infliximab 10.1517/14712598.2013.736960 © 2013 Informa UK, Ltd. ISSN 1471-2598, e-ISSN 1744-7682 469 All rights reserved: reproduction in whole or in part not permitted Expert Opin. Biol. Ther. 2013.13:469-473. Downloaded from informahealthcare.com by University of Connecticut on 10/30/14. For personal use only.
Transcript of TNF-α antagonists and nail psoriasis: an open, 24-week, prospective cohort study in adult patients...

1. Introduction
2. Materials and methods
3. Results
4. Discussions
Original Research
TNF-a antagonists and nailpsoriasis: an open, 24-week,prospective cohort study in adultpatients with psoriasisRosita Saraceno†, Lucia Pietroleonardo, Annamaria Mazzotta,Arianna Zangrilli, Luca Bianchi & Sergio ChimentiUniversity of Rome Tor Vergata, U.O.C. of Dermatology, Rome, Italy
Introduction: Treatment of nail psoriasis can be challenging and unsatisfac-
tory. The aim of this study was to compare the efficacy of three different
anti-TNF-a agents on nail psoriasis in patients affected by psoriasis.
Materials and methods: Seventy-two patients with nail psoriasis were evalu-
ated in this open, 24 weeks, prospective study. Patients were enrolled in three
groups of treatment: adalimumab, etanercept or infliximab. Severity of nail
psoriasis was assessed by the Nail Psoriasis Severity Index (NAPSI) at baseline,
week 14, and 24.
Results: Sixty patients were included in the study. The mean NAPSI was 33.77.
In the adalimumab group, the mean NAPSI score was 33.1 (± 14.9) at baseline,
21 (± 8.91) at week 14 and 11.4 (± 4.6) at week 24 (p < 0.0002). In the etaner-
cept group, the mean NAPSI was 34.8 (± 12.38) at baseline, 23.6 (± 10.43) at
week 14, and 10.6 (± 5.25) at week 24 (p < 0.0016). In the infliximab group,
the mean NAPSI was 33.3 (± 9.76) at baseline, 14.9 (± 4.20) at week
14 (p < 0.001) and 3.1 (± 3.27) at week 24 (p < 0.00001). At week 14 efficacy
was higher in infliximab group compared to adalimumab and etanercept
groups (p < 0.05).
Conclusions: Among the three agents, in the infliximab group a significant
improvement in nail psoriasis was observed as early as week 14 of therapy
whereas in the adalimumab and etanercept groups at week 24.
Keywords: adalimumab, etanercept, infliximab, nail psoriasis, NAPSI
Expert Opin. Biol. Ther. (2013) 13(4):469-473
1. Introduction
Nail psoriasis is reported in 10 -- 50% of psoriatic patients [1]. The incidence of nailinvolvement is higher among patients affected with psoriatic arthritis than amongthose with psoriasis alone [2]. The frequency of nail psoriasis is reported between63% and 83% of psoriatic arthritis patients [3,4]. Nail psoriasis may vary from slightto debilitating forms, with functional and psychosocial impairments as well as severeimpact on patient’s quality of life [5]. The nail involvement is generally associatedwith pain, restrictions in daily life activities and the visibility of fingernail diseasemay hinder social and business interactions. Treatment is challenging and oftenunsatisfactory and less than 50% of patients experience effective treatments [5].The therapeutic options include corticosteroids, vitamin D3 analogues, tazarotene,5-fluorouracil, urea, anthralin, cyclosporine, methotexate and radiotherapy [1,6,7].
Adalimumab, etanercept and infliximab are anti-TNF-a drugs used for the treat-ment of plaque-type psoriasis and psoriatic arthritis.
Studies performed in large cohort of patients affected by moderate-to-severeplaque-type psoriasis and psoriatic arthritis demonstrated the efficacy of infliximab
10.1517/14712598.2013.736960 © 2013 Informa UK, Ltd. ISSN 1471-2598, e-ISSN 1744-7682 469All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Bio
l. T
her.
201
3.13
:469
-473
.D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/3
0/14
. For
per
sona
l use
onl
y.

on nail psoriasis in the short- and long-term treatment [8-10].In contrast limited clinical observations showed the therapeu-tic effect of etanercept and adalimumab on nail disease [8].The aim of this study was to compare the clinical response
of three different anti-TNF-a agents, namely adalimumab,etanercept and infliximab, in nail psoriasis.
2. Materials and methods
This was an open prospective 24-week study conducted at theU.O.C. of Dermatology of the University of Rome TorVergata. The protocol was approved by the “Tor Vergata”Ethical Committee and the study registered (identifiernumber 4509). All volunteers provided a written consent atthe enrolment.A total of 72 Caucasian patients affected with nail psoriasis
were randomly and equally distributed (1:1:1) in the threestudy groups (adalimumab, etanercept and infliximab)accordingly with the European and Italian Guidelines forTNF antagonists [11-13].Enrolment was performed until a total of 60 subjects
(20 patients for each group of treatment) completed the studyand their results were eligible for data analysis.The main inclusion criteria were diagnosis of moderate-
to-severe plaque-type psoriasis or psoriatic arthritis,un-responsiveness to topical and at least two systemic conven-tional treatments, age ‡ 18 years, a > 6 months diagnosis ofnail psoriasis and a Nail Psoriasis Severity Index (NAPSI)score from moderate to severe (NAPSI > 15) [14]. Applicationof topical treatments and nail lacquers were not allowed dur-ing the study period. Patients were evaluated at baseline, week14 and week 24 and they were excluded if they did not con-clude the 24 weeks of treatment. Screening for nail infectionsincluding onychomycosis was performed in all patients andthose with a positive result were excluded.Nail psoriasis was assessed using NAPSI [14], a system for
grading the severity of psoriatic nail disease that can beapplied either to all nails or to a specified target nail. Forpatients with nail psoriasis at baseline, each nail affectedwith psoriasis was divided into quadrants, and graded foreight features of psoriasis, including four involving the nailmatrix (pitting, leukonychia, red spots in the lunula, andnail plate crumbling) and four involving the nail bed(onycholysis, splinter haemorrhages, oil drop discoloration-salmon patch, and nail bed hyperkeratosis) (Table 1). Onepoint was assigned for each quadrant of each nail that had
either nail matrix psoriasis or nail bed psoriasis, regardless ofseverity, for a total possible score of 80. The NAPSI wasused to assess the severity of the disease at baseline, weeks14, and 24.
Outcome measures were evaluated by two blinded, inde-pendent and trained evaluators at baseline, week 14 andweek 24 using the NAPSI. Patients’ response was classifiedat the end of treatment as no improvement--mild improve-ment (< 75% improvement), moderate and completeimprovement (> 75%).
Unpaired t-test was performed to evaluate the efficacy ofeach treatment after 14 and 24 weeks of treatment. Differen-ces in the primary outcomes between groups were performedby ANOVA test. Probability values less than 0.05 wereconsidered significant and sample size was calculated. TheStatistical Package for the Social Sciences (SPSS for Windows,Rel. 11.0.1) was used for the statistical analysis.
2.1 Pharmacological treatmentAdalimumab (Humira�, Abbott Laboratories), etanercept(Enbrel�, Wyeth Lederle S.p.A.) and infliximab (Remicade�,MSD) are anti-TNF-a drugs approved by the European Med-icines Agency (EMA) for the treatment of psoriasis that can beprescribed in patients who failed at least two systemic conven-tional therapies for lack of efficacy or adverse events, includingsystemic steroids, cyclosporine, methotrexate, oral retinoids,PUVA and fumarates [11-13]. Adalimumab was administratedsubcutaneously at the dose of 80 mg at week 0 followed by40 mg every other week from weeks 1 to 24. Infliximab wasgiven intravenously and continuously at the dose of 5 mg/kgat weeks 0, 2 and 6 and every 8 weeks thereafter. Etanerceptis an intermittent (cycles of 24 weeks) therapy and was given ata dose of 50 mg twice weekly self-administered subcutaneouslyfor 12 weeks followed by a dose reduction to 25 mg twiceweekly for 12 weeks. According to the Italian ministerial“Psocare” project, for the treatment of plaque-type psoriasis,etanercept can be administrated for a maximum period of24 weeks [11].
2.2 Safety assessmentsAt each study visit, physicians asked patients if they experiencedany adverse events (EAs) and their intensity was assessed asmild (noticeable discomfort without effect on daily activities),moderate (discomfort affecting daily activities), or severe(inability to work or perform normal daily activities). Physi-cians also assessed each AEs’ relationship to treatment as unre-lated, remote, possible, or probable. All serious AEs (SAEs)were reported on a standard SAE within 24 h. At each visitand a 60-day follow-up physical examination and standardlaboratory tests were performed as well as measure of vital signs.
3. Results
Sixty patients completed the study and 12 were excluded forthe following reasons: 6 patients had onychomycosis, 6 did
Table 1. Nail signs and anatomic site of disease.
Nail bed psoriasis Nail matrix psoriasis
Onycholysis PittingSplinter haemorrhages LeukonychiaOil drop discoloration Red spots in the lunulaNail bed hyperkeratosis Nail plate crumbling
R. Saraceno et al.
470 Expert Opin. Biol. Ther. (2013) 13(4)
Exp
ert O
pin.
Bio
l. T
her.
201
3.13
:469
-473
.D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/3
0/14
. For
per
sona
l use
onl
y.

not complete the 24 weeks of treatment (in the adalimumabgroup 1 patient had a lung infection and 1 withdrew the studyfor lack of efficacy; in the infliximab group 2 patients had agenito-urinary infection; in the etanercept group one patienthad herpes zoster).
These patients were not included in the statistical analysissince they were screening failure or they dropped out beforeweek 14.
All patients were unresponsive to topical and at least twosystemic and conventional treatment for psoriasis.
Thirty-four patients were affected with plaque-type psoriasisand 26 by psoriatic arthritis. The mean age was 46.5; malewere 43 and female 17. The groups were well balanced fordemographic and inflammatory disease features (Table 2). Allpatients enrolled in this study presented a severe nail disease(NAPSI > 15) [14] and had culture and microscopic KOHexamination negative for dermatophytes, yeasts, and moulds.
Distribution of data were normal (Gaussian) with equalvariances.
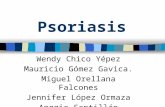
The mean NAPSI was 33.77. In the adalimumab group,the mean NAPSI score was 33.1 (± 14.9) at baseline, 21(± 8.91) at week 14 and 11.4 (± 4.6) at week 24(p < 0.0002). In the etanercept group the mean NAPSI was34.8 (± 12.38) at baseline, 23.6 (± 10.43) at week 14, and10.6 (± 5.25) at week 24 (p < 0.0016). In the infliximabgroup, the mean NAPSI was 33.3 (± 9.76) at baseline,14.9 (± 4.20) at week 14 (p < 0.001) and 3.1(± 3.27) atweek 24 (p < 0.00001) (Figures 1 and 2, and Table 3). Atweek 14 efficacy was higher in infliximab group comparedto adalimumab and etanercept groups (p < 0.05).
No significant differences were noticed between matrix andnail bed response among the three groups of treatments.
Treatments were well tolerated; SAEs and AEs for eachgroup are described in Table 4.
4. Discussions
We compare the clinical response induced by three differentTNF-a inhibitors in nail psoriasis. Many options exist for thetreatment of this disabling condition [1]. Since several topicaland systemic agents have been used with limited efficacy, there
Table 2. Patients demographics and disease characteristics at baseline.
Adalimumab Etanercept Infliximab
Mean age ± SD 48 ± 12 45 ± 10 50 ± 15Male/female 15/5 14/6 14/6Caucasians 20/20 20/20 20/20Age of onset, mean ± SD 20 ± 15 21 ± 15 18 ± 12Body weight (Kg) 82.1 ± 7.7 81.6 ± 10.4 80.9 ± 9.8Psoriasis vulgaris 11/20 12/20 11/20Psoriasis arthritis 9/20 8/20 9/20Mean PASI 24.6 24.1 25.3Nail matrix psoriasisPitting 15/20 17/20 18/20Leukonychia 8/20 9/20 8/20Nail plate crumbling 7/20 8/20 6/20Red spots in lunula 8//20 6/20 5/20Nail bed psoriasisOnycholysis 15/20 12/20 14/20Oil drop discoloration 10/20 12/20 13/20Nail bed hyperkeratosis 9/20 5/20 8/20Splinter haemorrhages 8/20 6/20 7/20
Anti-TNF-a groups were balanced for number, demographic and disease features.
Adalimumab Etanercept Infliximab
NAPSI T0
NAPSI T14
NAPSI T24ME
AN
NA
PS
I
0.00
∗ ∗∗
∗5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Figure 1. The graph shows the variation of NAPSI in the
3 groups of treatment at baseline (T0), after 14 weeks (T14)
and after 24 weeks (T24). In the adalimumab group, the
mean NAPSI score was 33.1 at baseline, 21 at week 14 and
11.4 at week 24 (p < 0.0002). In the etanercept group, the
mean NAPSI was 34.8 at baseline, 23.6 at week 14, and
10.6 at week 24 (p < 0.0016). In the infliximab group, the
mean NAPSI was 33.3 at baseline, 14.9 at week 14 (p < 0.001)
and 3.1 at week 24 (p < 0.00001). NAPSI before (NAPSI 0),
after 14 weeks (NAPSI 14) and after 24 weeks (NAPSI 24) of
therapy with infliximab, etanercept and adalimumab.*p£ 0.01 un-paired t-test: baseline vs week 14 vs week 24.
Nail psoriasis and TNF-a antagonists
Expert Opin. Biol. Ther. (2013) 13(4) 471
Exp
ert O
pin.
Bio
l. T
her.
201
3.13
:469
-473
.D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/3
0/14
. For
per
sona
l use
onl
y.

is a strong need of treatment, which may induce a completeand long-lasting clinical remission, especially in those cases ofnail psoriasis refractory to most therapies [6-8].Several clinical trials have shown that anti-TNF-a
treatments have significant effects for the treatment of moder-ate-to-severe plaque-type psoriasis and psoriatic arthritis [15,16].Although early evidence indicates that TNF-a antagonists areeffective in the treatment of nail psoriasis, few studies havedemonstrated the efficacy of biological therapies in patientswith nail disease [8-10,17,18].Studies performed in large cohort of patients affected by
moderate-to-severe plaque-type psoriasis and psoriatic arthritisdemonstrated the efficacy of infliximab on nail psoriasis inboth short- and long-term treatment [8-10]. Reich et al. [9]
reported a significant efficacy in nail psoriasis as early as week10 of therapy with 5 mg/kg of infliximab. It was a Phase III,multicentre, double-blind trial, including 378 patients withmoderate-to-severe plaque psoriasis. At week 24, a 56%decrease in the NAPSI score was observed and this improve-ment was maintained through week 50. These results con-firmed our previous observations [10] in a pilot, open-label,not placebo-controlled study evaluating 25 psoriatic patientstreated for 22 weeks at the same dose regimen of infliximab.
In contrast limited clinical observations showed the efficacyof etanercept and adalimumab on nail psoriasis [17,18,16,19].Rallis et al. [17] described a case in which the efficacy of etaner-cept was remarkable after only 3 weeks’ administration. In alarger study, Luger et al. [18] reported the efficacy of etanercept(subcutaneously administered at the dose regimen of 25 mgtwice a week vs 50 mg twice a week) in a subgroup of patientsaffected with nail psoriasis enrolled in a randomized, open-label, multicentre study including 720 adult patients withmoderate-to-severe plaque psoriasis. An improvement ofNAPSI and quality of life indexes was observed at week12 in 28.9% of patients. Improvement of NAPSI was higherthan 50% after 54 weeks of both dose regimen treatment.
The efficacy of adalimumab on nail psoriasis has also beenreported by Rigopoulos et al. [16] The authors showed in thisopen, 24-week non-randomized, unblinded study performedon 21 psoriatic patients, a significant reduction in the meanNAPSI in fingernails and toenails [16]. The applied dose regi-men of adalimumab was the same as the one recommendedfor cutaneous psoriasis (40 mg eow). NAPSI and quality oflife indexes were measured at weeks 12 and 24 showing a sig-nificant improvement after the eighth injection. Similarly,Kyriakou et al. [19] showed that anti-TNF agents result in asignificant improvement of NAPSI score, with infliximabgiven the precedence and followed by etanercept and adalimu-mab. Similarly in our study we compared the efficacy of threeTNF-a inhibitors, showing and confirming that a significantimprovement on psoriatic nail signs was achieved at week14 in the infliximab group and at week 24 in theadalimumab and etanercept groups.
These results did not change if all the excluded subjectswere assumed to have failed their anti-TNF-a agent (bothITT and PP analysis were performed).
Amelioration of both matrix and nail bed psoriatic signswas observed without showing significant differences amongthe three groups of treatment and between patients affectedwith plaque-type psoriasis and psoriatic arthritis.
Limitations of the present study, that should be considered,include the open label design, small sample size, the drop-out rate and the short follow-up period. Although biologicaltherapies are effective in the treatment of psoriasis, they areconsidered as a second line treatment. Patients affected withpsoriasis can be treated with TNF-a antagonists only if theyare affected by moderate-to-severe psoriasis and if they havefailed or have contraindications to conventional treatmentssuch as methotrexate, cyclosporine, acitretin and PUVA
T24T0
Figure 2. Complete remission of severe nail and plaque-
type psoriasis (T0) after 24 weeks of treatment with an
anti-TNF-a inhibitor.
Table 3. Percentage of patients achieving
NAPSI > or < of 75% or no response after 24 weeks of
treatment with adalimumab, etanercept and infliximab.
Clinical response at week 24
Treatment > NAPSI 75 < NAPSI 75 No responseAdalimumab 10/20 (50%) 8/20 (40%) 2/20 (10%)Etanercept 9/20 (45%) 7/20 (35%) 4/20 (20%)Infliximab 13/20 (65%) 6/20 (30%) 1/20 (5%)
Table 4. Adverse events and severe adverse events*
observed in the study period.
Adverse events Adalimumab Etanercept Infliximab
Flu-like syndrome 2 1 --Genito-urinary infection 1 -- 2*Site injection reaction/Infusion reaction
1 2 3
Conjunctivitis 1 -- --Dislipedemia 1 2 1Lung infection 1* -- --Herpes zoster -- 1 --Otitis -- 1 --
R. Saraceno et al.
472 Expert Opin. Biol. Ther. (2013) 13(4)
Exp
ert O
pin.
Bio
l. T
her.
201
3.13
:469
-473
.D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/3
0/14
. For
per
sona
l use
onl
y.

therapy. According with these limitations, further studies inlarger groups of patients are necessary to confirm our resultsin the long-term and to assess changes in quality of life by spe-cific nail-questionnaires.
In conclusion, we observed that among TNF-a inhibitorsapproved for the treatment of psoriasis, infliximab showed asignificant improvement in nail psoriasis as early as week14 of therapy whereas adalimumab and etanercept groups atweek 24.
These results suggest different pharmacokinetic andpharmacodynamics properties possibly associated with the
half-life and distribution of each drug. These features couldbe further related to the different speed of onset of TNF-aantagonists effect and should be considered during the choiceof a biologic treatment in psoriasis.
Declaration of interest
S Chimenti serves as a consultant to MSD, Pfizer and Abbott.None of the other co-authors have any competing intereststo declare and no funding was received in preparation ofthis manuscript.
Bibliography
1. Jiaravuthisan MM, Sasseville D,
Vender RB, et al. Psoriasis of the nail:
anatomy, pathology, clinical presentation,
and a review of the literature on therapy.
J Am Acad Dermatol 2007;57:1-27
2. Gudjonsson JE, Karason A,
Antonsdottir AA, et al.
HLA-Cw6-positive and
HLA-Cw6-negative patients with
Psoriasis vulgaris have distinct clinical
features. J Invest Dermatol
2002;118:362-5
3. Williamson L, Dalbeth N, Dockerty JL,
et al. Extended report: nail disease in
psoriatic arthritis clinically important,
potentially treatable and often
overlooked. Rheumatology
2004;43:790-4
4. Elkayam O, Ophir J, Yaron M, Caspi D.
Psoriatic arthritis: interrelationships
between skin and joint manifestations
related to onset, course and distribution.
Clin Rheumatol 2000;19:301-5
5. de Jong EM, Seegers BA, Gulinck MK,
et al. Psoriasis of the nail associated with
disability in a large number of patients:
results of a recent interview with
1728 patients. Dermatology
1996;193:300-3
6. De Berker D. Management of nail
psoriasis. Clin Exp Dermatol
2000;25:357-62
7. Bianchi L, Soda R, Diluvio L,
Chimenti S. Tazarotene 0.1% gel for
psoriasis of the fingernails and toenails:
an open prospective study.
Br J Dermatol 2003;149:1207-9
8. Lawry M. Biological therapy and nail
psoriasis. Dermatol Ther 2007;20:60-7
9. Reich K, Nestle FO, Papp K, et al.
Infliximab induction and maintenance
therapy for moderate-to-severe psoriasis:
a phase III, multicentre, double-blind
trial. Lancet 2005;366:1367-74
10. Bianchi L, Bergamin A, de Felice C,
et al. Remission and time of resolution
of nail psoriasis during infliximab
therapy. J Am Acad Dermatol
2005;52:736-7
11. Nijsten T, Wakkee M. Psocare: italy
shows the way in postmarketing studies.
Dermatology 2008;217:362-4
12. Pathirana D, Ormerod AD, Saiag P,
et al. European S3-guidelines on the
systemic treatment of psoriasis vulgaris.
J Eur Acad Dermatol Venereol
2009;23:1-70
13. Smith CH, Anstey AV, Barker JN, et al.
British Association of Dermatologists’
guidelines for biologic interventions for
psoriasis 2009. Br J Dermatol
2009;161:987-1019
14. Rich P, Scher RK. Nail Psoriasis Severity
Index: a useful tool for evaluation of nail
psoriasis. J Am Acad Dermatol
2003;49:206-12
15. Weinberg JM. An overview of infliximab,
etanercept, efalizumab, and alefacept as
biological therapy for psoriasis. Clin Ther
2003;25:2487-505
16. Rigopoulos D, Gregoriou S,
Lazaridou E, et al. Treatment of nail
psoriasis with adalimumab: an open label
unblinded study. J Eur Acad
Dermatol Venereol 2010;24(5):530-4
17. Rallis E, Stavropoulou E, Rigopoulos D,
Verros C. Rapid response of nail
psoriasis to etanercept. J Rheumatol
2008;35:544-5
18. Luger TA, Barker J, Lambert J, et al.
Sustained improvement in joint pain and
nail symptoms with etanercept therapy in
patients with moderate-to-severe
psoriasis. J Eur Acad Dermatol Venereol
2009;23(8):896-904
19. Kyriakou A, Patsatsi A, Sotiriadis D.
Anti-TNF agents and nail psoriasis:
a single-center, retrospective, comparative
study. J Dermatolog Treat
2012; [Epub ahead of print]
AffiliationRosita Saraceno† MD, Lucia Pietroleonardo MD,
Annamaria Mazzotta MD,
Arianna Zangrilli MD, Luca Bianchi MD &
Sergio Chimenti MD†Author for correspondence
University of Rome Tor Vergata,
Department of Dermatology,
Policlinico Tor Vergata,
Viale Oxford 81, 00133,
Rome, Italy
Tel: +39 06 26902743;
Fax: +39 06 20902742;
E-mail: [email protected]
Nail psoriasis and TNF-a antagonists
Expert Opin. Biol. Ther. (2013) 13(4) 473
Exp
ert O
pin.
Bio
l. T
her.
201
3.13
:469
-473
.D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Con
nect
icut
on
10/3
0/14
. For
per
sona
l use
onl
y.