Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid ...

The Relationship of TransformingGrowth Factor-b1 Gene Polymorphism,Its Plasma Level, and GingivalOvergrowth in Renal TransplantRecipients Receiving DifferentImmunosuppressive RegimensMałgorzata Radwan-Oczko,* Maria Boratynska,† Marek Zietek,* Magdalena Zołedziewska,‡
and Anna Jonkisz‡
Background: Cyclosporin A (CsA) induces gingival overgrowth(GO) in patients who seem to be prone to this disorder. It is stillimpossible to determine which patients will develop GO. Patientstreated with the new immunosuppressive drug tacrolimus seem not tohave GO. The aims of this study were to investigate transforminggrowth factor-b1 (TGF-b1) gene polymorphisms in renal transplantrecipients treated with CsA or tacrolimus and to establish an associ-ation between these polymorphisms and TGF-b1 plasma concentra-tion and the incidence of GO.
Methods: The examined group consisted of 134 renal transplantrecipients. Ninety-two underwent CsA treatment (50 with and 42without GO), and 42 underwent tacrolimus treatment. Age, gender,time after transplantation, calcineurin inhibitor total dosage, numberof teeth, and sulcus bleeding index were analyzed. TGF-b1 plasmalevels were estimated in 60 CsA- and 30 tacrolimus-treated patients.Two biallelic polymorphisms of the TGF-b1 gene were studied at co-don 10 (at position +869) and at codon 25 (at position +915) in pa-tients from the examined group and in 108 healthy volunteers (thecontrol group).
Results:Thedistributionof thehigh, intermediate,and lowTGF-b1producer phenotypes was comparable in all the studied groupsand in the healthy controls. The high producer phenotype was morefrequent in patients with GO. TGF-b1 levels in the CsA group showedcorrelation with the phenotypes. The lowest incidence of GO was ob-served in the 10C/C genotype, whereas the highest was observed inthe 10T/C genotype.
Conclusion: High and intermediate TGF-b1 producer phenotypesand heterozygous genotype 10T/C might be considered risk factorsfor GO in patients treated with CsA. J Periodontol 2006;77:865-873.
KEY WORDS
Cyclosporin A; gene; gingival overgrowth; renal transplant;transforming growth factor-beta1; polymorphism.
The risk factors of gingivalovergrowth (GO) as a sideeffect of immunosuppres-
sive treatment with cyclosporinA (CsA) in renal transplant recip-ients have been investigated forthe last 23 years in a number ofstudies. Attention has been paidto local and systemic risk factorssuch as level of oral hygiene, peri-odontal conditions, unfavorableanatomical conditions, pretrans-planthyperplasia,gingivalfibroblastactivity and its collagen metabo-lism, ultrastructural changes inepithelial cells, and genetic pre-disposition to the human leuko-cyte antigen phenotype. Theconnection between the severityand degree of GO, age, gender,CsA total dosage, and CsA troughblood level, treatment duration,and pharmacokinetic propertiesalso has been studied, but thedefinite cause of this pathologyhas not been found.1-13 It wasfound that long-term CsA treat-ment significantly suppressed theactivity of cathepsin-B and -L,
* Department of Periodontology, Wrocław Medical University, Wrocław, Poland.† Department of Nephrology and Transplant Medicine, Wrocław Medical University.‡ Department of Forensic Medicine, Molecular Techniques Unit, Wrocław Medical University.
doi: 10.1902/jop.2006.050086
J Periodontol • May 2006
865

consequently decreasing protein degradation in gingi-val cells.14 Through decreasing phagocytic activity ofgingival fibroblasts, CsA decreases collagen degrada-tion.15 CsA-induced GO develops only in some pa-tients who seem to be prone to this disorder. Theinterruption of CsA therapy leads to regression of GO,while calcium channel blockers (such as nifedipine)used concomitantly with CsA intensify GO.16,17
In the late 1990s, a new calcineurin inhibitor,tacrolimus (FK-506), was introduced and used asan alternative to CsA. Tacrolimus seems not to haveany impact upon GO. Switching therapy from CsAto tacrolimus reverses CsA-induced GO.18-22
Transforming growth factor-b1 (TGF-b1) is a mul-tifunctional growth cytokine and mediator of woundhealing and tissue regeneration. TGF-b1 can activatefibrotic cascades and develop the differentiation ofmyoblasts into myofibroblastic cells in injured skele-tal muscle. Studies have shown that TGF-b1 has beenimplicated in the pathogenesis of pulmonary fibrosis,renal fibrosis, keloid formation, scleroderma, and he-reditary gingival fibromatosis. TGF- b1 expression byfibroblasts is related to drug use and hereditary fac-tors.23,24 TGF-b1 may be consider as one of the fac-tors responsible for CsA-induced gingival overgrowth.
Recent studies have identified polymorphisms inthe TGF-b1 gene and have shown a connectionbetween gene polymorphisms and the production ofthis cytokine. These two polymorphisms of theTGF-b1 gene in the signal protein sequence havebeen associated with interindividual variation inTGF-b1 production both in vitro and in serum and rep-resent a change from the amino acid leucine to prolineat codon 10 at position +869 and a change from argi-nine to proline at codon 25 at position +915.25,26
According to these studies, genotypic combinationsT/T at codon 10, G/G at codon 25, and 10T/C25G/G were described as high producer phenotypes,combinations 10T/C 25G/C, 10C/C 25G/G, and10T/T 25G/C were described as intermediate pro-ducer phenotypes, and the other combinations(10C/C 25G/C, 10C/C 25C/C, 10T/T 25C/C, and10T/C 25C/C) were associated with low producerphenotypes. These polymorphisms have also beendescribed as being associated with pretransplant lungfibrosis and lung allograft fibrosis. According to onestudy, the polymorphism in codon 10 influences pro-tein transport, whereas the polymorphism in codon 25influences gene transcription.26 Another study de-scribed the TGF-b1 gene polymorphism at codon25 as an independent genetic determinant of severeGO.27 Many reports suggest that there is a possiblegenetic origin of this pathology.
The objective of the present study was to determinethe association between functional polymorphisms ofthe TGF-b1 gene and TGF-b1 plasma level as well as
the incidence and severity of GO in renal transplant re-cipients treated concomitantly with CsA and calciumchannel blockers.
MATERIALS AND METHODS
The researchstudywasconducted from2001 to2004 inthe Department of Nephrology and Transplant Medicineand Department of Periodontology in Wrocław MedicalUniversity. The protocol of research was approved bythe author’s institutional review committee for humansubjects, and the study was conducted in accordancewith the Helsinki Declaration of 1975, as revised in2000. There were 134 renal transplant recipients inthe examined group. A group of 92 patients (35 femalesand 57 males), which consisted of 50 patients with and42 without GO, was treated with CsA. The tacrolimus-treated group consisted of 42 patients (17 femalesand 25 males). In each group, CsA or tacrolimus wasused in combination with azathioprine and prednisoloneormycophenolatemofetil andprednisolone.Allpatientsprovided informed consent to participate in the study.
The dosage of CsA/tacrolimus depended uponthe time lapsed after transplantation. Patients alsoreceived calcium channel blockers: verapamil,amlodipine, or nitrendipine.
In the investigated groups, age, gender, time aftertransplantation, calcineurin inhibitor total dosage,SBI index, and number of teeth were analyzed.
TGF-b1 plasma levels were evaluated in 90 pa-tients (60 patients in the CsA group and 30 patientsin the tacrolimus group). Blood from all patients wassampled to EDTA tubes and centrifuged at 1,000 · gfor 30 minutes. The obtained plasma was additionallycentrifuged at 6,000 · g for 15 minutes at 2�C to8�C to remove platelets. TGF-b1 was measured byenzyme-linked immunosorbent assay kits.§
DNA StudiesTwo biallelic polymorphisms of the TGF-b1 gene werestudied in codon 10 (at position +869) and in codon25 (at position +915) in 134 patients from the inves-tigated group and in 108 healthy volunteers (the con-trol group).Isolation and amplification of genomic DNA. DNAfrom 100 ml frozen venous blood was extracted witha preparation kit.i To amplify the targeted sequenceof DNA exon 1 at position +869 (codon 10; T/C;Leu/Pro) and position +915 (codon 25; G/C; Arg/Pro) of the TGF-b1 gene from chromosome 19, theprimers described by Awad et al.28 were used. Alleleidentification was achieved by polymerase chain re-action (PCR) amplification of 1 to 20 ng of genomicDNA using an automated thermal cycler.¶ PCR was
§ Quantikine, R & D Systems, Minneapolis, MN.i Blood DNA Prep Plus, A&A Biotechnology, Gdansk, Poland.¶ Biometra UNO Thermoblock, Gottingen, Germany.
TGF-b1 Gene Polymorphism and Gingival Overgrowth Volume 77 • Number 5
866

carried out in a total volume of 11 ml containing 1 mMeach primer, 200 mM each deoxynucleotide triphos-phate (dNTP), 1· PCR buffer, and 1 unit of polymer-ase.# The PCR profile was as follows: initialdenaturation at 95�C for 11 minutes, followed by 31cycles of denaturation at 94�C for 1 minute, annealingfor 1 minute at 60�C, extension for 2 minutes at 72�C,and a final extension for 45 minutes at 60�C.
Minisequencing. Five microliters of amplified prod-uct was purified of dNTPs and primers in a total vol-ume of 7 ml using 2 ml reagent** to avoid participationin subsequent primer-extension reactions. For theminisequencing reaction, a multiplex kit†† was usedthat detects single nucleotide polymorphisms (SNPs)by the extension of unlabeled SNP primer with fluores-cently labeled dideoxynucleotide triphosphates([F]ddNTPs). The ddNTPs are labeled with four colors:A,green(dR6G);C,yellow(dTAMRA);G,blue (dR110);and T, red (dROX). The reactions were performedin 5 ml total volume containing 0.1 mM extendingprimer and 1 ml purified PCR product. The minise-quencing primers 59-TTGCAGGTGGATAGTCCCGC-GGCCGGC-39 (27 bp; accession number 1800471)and59-AGCAGCGGTAGCAGCAGC-39(18bp;acces-sion number 1982073) were constructed according tothe sequence from the National Center for Biotechnol-ogy Information SNP database. Polymerase‡‡ wasused to add a single ddNTP to the 39 end of the primeron an amplified and purified template. After the ex-tension and labeling reaction, the unincorporatedddNTPs were removed by enzymatic treatment us-ing 1 unit of alkaline shrimp phosphatase§§ to avoidcomigration of the [F]ddNTPs with the fragment ofinterest.
Electrophoresis and detection. The products ofthe reaction were analyzed on a genetic analyzerii
equipped with analysis software.¶¶ To run a sample onthegeneticanalyzer,amodule##isrequiredthatencodesoptimal injection and electrophoresis parameters. Fora precise spectral overlap between dyes, a matrix filewas created.*** One microliter of the extension reac-tion product was denatured at 95�C for 5 minutes in 10ml formamide.††† For the fragment size detection, aninternal size standard‡‡‡ wasadded,andsamplesweresubjected to electrophoresis with laser excitation/fluorescence detection. On the electrophoregram,theallelesareshownaspeaks(19and28bp); thecolorof the peak differs according to the different nucleotideat the place of interrogation.
Observed GO was present in different degreesand extensiveness as interdental papilla overgrowthand/or marginal gingiva overgrowth. Degree of GOwas assessed on a four-degree scale: 0, no over-growth; 1, faint interdental papilla overgrowth; 2, mar-ginal gingiva and interdental papilla overgrowthreaching one-third of the tooth crown; and 3, marginal
gingiva and interdental papilla overgrowth reachingmore than half of the tooth crown.
In each patient, GO of 1, 2, or 3 degrees was clin-ically determined in a range from 38% to 100%.The modified sulcus bleeding index (SBI%) by Muhle-mann and Son was used in clinical evaluation ofbleeding.29 All patients were clinically investigatedby one dentist.
Statistical AnalysisResults are presented as mean values – SD. Compar-isons between two means were analyzed by Studentt and Mann-Whitney U tests, with a P value <0.05accepted as statistically significant.
RESULTS
The clinical data of CsA- and tacrolimus-treatedgroups are presented in Table 1. The age of patients,SBI% index, and number of teeth were comparable.The average TGF-b1 plasma level was 3.3 ng/ml inthe CsA-treated group and 2.6 ng/ml in the tacrolimus-treated group, and the difference was not significant.None of the patients taking tacrolimus had GO, despitethe fact that 67% of them were also treated with calciumchannel blockers. Calcium channel blockers were ad-ministered to 76% of the patients in the CsA group. Timelapse after transplant surgery was significantly longer inthe CsA group.
Comparison of clinical data between CsA sub-groups with and without GO is presented in Table 2.No significant differences were observed in the meanage, time after transplantation, TGF-b1 level, averagetotal CsA dose, and number of teeth between the stud-ied subgroups. The average SBI% score of patientswith GO was significantly higher compared to patientswithout GO (P <0.02).
The distribution of the phenotypes of high, interme-diate, and low TGF-b1 producers was comparable be-tween the studied patients (N = 134) and the healthyindividuals (N = 108) (Table 3). Distribution of thephenotypes was similar in the tacrolimus and CsAgroups. There were no statistical differences in the dis-tribution of these phenotypes between patients withand without GO, although in the subgroup of patientswith GO, phenotype H was present in 78% versus73.8% in the subgroup of patients without GO. Con-versely, the frequency of the low producer phenotype
# AmpliTaq Gold, PE Applied Biosystems, Foster City, CA.** ExoSAP-IT, USB, Cleveland, OH.†† SNaPshot, PE Applied Biosystems.‡‡ AmpliTaq DNA polymerase FS, PE Applied Biosystems.§§ USB.ii ABI PRISM 310, PE Applied Biosystems.¶¶ GeneScan version 3.1, PE Applied Biosystems.## GeneScan POP-4 (1 ml) E5, PE Applied Biosystems.*** Matrix Standard Set DS-02, PE Applied Biosystems.††† HD formamide, PE Applied Biosystems.‡‡‡ GeneScan 120 Liz, PE Applied Biosystems.
J Periodontol • May 2006 Radwan-Oczko, Boratynska, Zietek, Zołedziewska, Jonkisz
867

was lower (4%) in the subgroup with GO in contrastto the subgroup without GO (7.1%). There were nosignificant differences in allele distribution fromHardy-Weinberg rule between the controls and inves-tigated groups: with GO, without GO, and tacrolimus-treated groups (Table 4). No statistically significant
differences were found in TGF-b1 genotype frequen-cies at codons 10 and 25 between the comparedgroups (Table 4).
Codon 10 homozygous genotype T/T was iden-tified with lower frequency in all the recipients thanin the healthy individuals (34.3% versus 42.6%).
Table 2.
Clinical Characteristics of CsA-Treated Groups With and Without GO
Group With GO Group Without GOStudent t Test Mann-Whitney U Test
Mean SD N Mean SD N P P
Age (years) 40.2 10.4 50 39.3 12.3 42 NS NS
0.7004 0.7537
Time after treatment (months) 54.0 34.6 50 60.9 50.7 42 NS NS
0.4431 0.6241
TGF-b1 level 3.2 2.2 30 3.4 2.1 30 NS NS
0.7886 0.4077
SBI% index 31.8 30.3 50 18.4 20.6 42 0.0171* 0.0143*
CsA total dose (g) 292.0 183.1 50 255.7 117.5 42 NS NS
0.2754 0.7137
N teeth 22.9 5.6 50 22.2 5.8 42 NS NS
0.5824 0.4455
NS = not significant.* P <0.05.
Table 1.
Clinical Characteristics of Investigated CsA- and Tacrolimus-Treated Groups
CsA-Treated Group Tacrolimus-Treated GroupStudent t Test Mann-Whitney U Test
Mean SD N Mean SD N P P
Age (years) 39.8 11.2 92 38.3 12.5 42 NS NS
0.4843 0.4734
Time after treatment (months) 57.1 42.6 92 17.6 8.3 42 0.0000* 0.0000*
TGF-b1 level (ng/ml) 3.3 2.1 60 2.6 1.9 30 NS NS
0.1593 0.0951
SBI% index 25.7 27.0 92 17.3 18.6 42 NS NS
0.0696 0.1302
N teeth 22.6 5.7 92 21.8 6.3 42 NS NS
0.4889 0.6896
NS = not significant.* P <0.05.
TGF-b1 Gene Polymorphism and Gingival Overgrowth Volume 77 • Number 5
868

Tacrolimus-treated patients had a similar distributionof this genotype as in the healthy controls (45.2% ver-sus 42.6%). Genotype 10T/T was less frequent in theCsA group (29.4%). In the GO subgroup, it was foundin 28% versus 31% in the non-GO subgroup.
Inversely heterozygous genotype T/C at codon 10was observed more frequently in all the recipientsthan in the healthy controls (51.5% versus 43.5%).It occurred with 57.6% frequency in the CsA groupand in 38.1% of the tacrolimus group. The genotypeT/C occurred in 64% of patients of the GO subgroupand in 50% of the non-GO subgroup.
Homozygous genotype C/C at codon 10 occurredwith comparable frequency in the healthy controls asin all the transplant groups. Genotype C/C in the GO
subgroup appeared more rarely than in all the othergroups and was twice as less frequent than in thenon-GO subgroup (8% versus 19.1%).
There were no differences in frequencies at codon25 of homozygous (G/G) and heterozygous (G/C)genotypes in the studied groups (Table 4). None ofthe studied patients and healthy individuals werehomozygous for proline (C/C) at codon 25.
TGF-b1 levels (Figs. 1 through 4) in the CsA groupshowed correlation with the phenotype as a whole andin the non-GO patients. In patients with GO, the con-centration of TGF-b1 increased in order from low tohigh to intermediate producer phenotypes (Fig. 4).The highest average TGF-b1 plasma level was asso-ciated with the intermediate producer phenotype in
Table 3.
Distribution of the TGF-b1 Phenotypes in Investigated and Control Groups
Phenotype
CsA- and Tacrolimus-
Treated Group Control Group CsA-Treated Group
Tacrolimus-Treated
Group
CsA-Treated Group
With GO Without GO
H 75.4% 76.9% 76.1% 73.8% 78.0% 73.8%
101 83 70 31 39 31
I 19.4% 18.5% 18.5% 21.4% 18.0% 19.1%
26 20 17 9 9 8
L 5.2% 4.6% 5.4% 4.8% 4.0% 7.1%
7 5 5 2 2 3
Total 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
134 108 92 42 50 42
H = high producer phenotype; I = intermediate producer phenotype; L = low producer phenotype.
Table 4.
Distribution of the TGF-b1 Genotypes for Codons 10 and 25 in Investigatedand Control Groups
CsA-Treated Group
Codon
TGF-b1
Genotype
CsA- and Tacrolimus-Treated
Group (N = 134)
Control Group
(N = 108)
CsA-Treated Group
(N = 92)
Tacrolimus-Treated
Group (N = 42)
With GO
(N = 50)
Without GO
(N = 42)
10 T/T 34.3% 42.6% 29.4% 45.2% 28.0% 31.0%
0.64* 0.64 0.60 0.56
T/C 51.5% 43.5% 57.6% 38.1% 64.0% 50.0%
C/C 14.2% 13.9% 13.0% 16.7% 8.0% 19.1%
0.36 0.36 0.40 0.44
25 G/G 85.1% 86.1% 84.8% 85.7% 84.0% 85.7%
0.93 0.93 0.92 0.93
G/C 14.9% 13.9% 15.2% 14.3% 16.0% 14.3%
0.07 0.07 0.08 0.07
* The allele frequency is shown in boldface type.
J Periodontol • May 2006 Radwan-Oczko, Boratynska, Zietek, Zołedziewska, Jonkisz
869

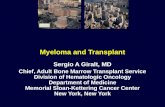
patients with GO. The TGF-b1 level was similar inpatients with and without GO; however, in the inter-mediate producer phenotype, the TGF-b1 level wasalmost two times higher in the GO patients (Figs. 2and4). Inpatients treatedwith tacrolimus, theTGF-b1level showed correlation with the intermediate andhigh producer phenotypes. It reached the maximumin the low producer phenotype, but only two patientshad this phenotype (Fig. 3).
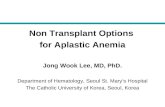
The average TGF-b1 plasma level for intermediateand high producer phenotypes was higher in the CsA-treated group compared to the tacrolimus-treatedgroupbutwasnotstatisticallysignificant(Figs.1and3).
We noticed the lowest degree of GO in associationwith the low producer phenotype and a comparable
degree of overgrowth in patients with intermediateand high producer phenotype (Fig. 5). Patients withlow producer phenotype suffered less frequently(40%) and less severely (only degrees 1 and 2)from GO. The frequency of GO in patients with inter-mediate and high producer phenotypes (53% and56%, respectively) was similar and higher than inthe low producer phenotype. The incidence of GO inrelationship to phenotypes and genotypes is shownin Figures 6 and 7.
DISCUSSION
Much evidence has been gathered in experimentaland clinical studies emphasizing the pathogeneticrole of TGF-b1 in CsA-induced GO. CsA stimulatesT lymphocytes and endothelial cells to produceTGF-b1. TGF-b1 enhances extracellular matrix (ECM)production and induces synthesis and accumula-tion of collagen and cell proliferation in connectivetissue. Enhanced TGF-b1 production reduces theproteolytic activities of fibroblasts derived from
Figure 1.Average TGF-b1 plasma levels for the high producer cytokinephenotype in CsA- and tacrolimus-treated groups. Error barsrepresent SD.
Figure 2.Average TGF-b1 plasma levels for the high producer cytokinephenotype in CsA-treated groups with and without GO. Error barsrepresent SD.
Figure 3.Average TGF-b1 plasma levels in CsA- and tacrolimus-treated groupsfor low (L), intermediate (I), and high (H) production phenotypes.
Figure 4.Average TGF-b1 plasma levels in CsA-treated groups with andwithout GO for low (L), intermediate (I), and high (H) productionphenotypes.
TGF-b1 Gene Polymorphism and Gingival Overgrowth Volume 77 • Number 5
870

hereditary gingival fibromatosis, which favors the ac-cumulation of ECM.30,31 The study of Gnoatto et al.32
indicates increased expression of proteoglycan-perlecan in overgrown gingiva, whereas decorine, anatural ECM component that inactivates TGF, wasnot increased.
Further studies showed an increased expression ofTGF-b1 at the tips of the dermal papillae of overgrowngingivae. Fibroblasts originating from overgrowngingivae were more sensitive to TGF-b1 in patientstreated with CsA.33 Wright et al.34 suggested thatthe higher local levels of TGF-b1 in gingival crevicularfluid could be a risk factor for developing GO.
TGF-b1 is a cytokine that modulates the host im-mune response in chronic marginal periodontitis.Several morphologically different cell types that werefound in inflamed gingivae contained TGF-b1.35
Higher local concentrations of TGF-b1 must addition-ally be considered as being related to gingival inflam-mation. We observed that the SBI% was significantlyhigher in patients with GO. It was associated with den-tal plaque mass, the removal of which is more difficultin swollen, enlarged gingivae.
Our study of TGF-b1 polymorphisms attemptedto explain why only some patients treated with CsAdevelop GO. The study revealed similar distributionof genotypes at codon 25 in renal graft recipientstreated with CsA or tacrolimus, in the group of healthyvolunteers, and in the patients with GO. None of thestudied 242 individuals (white) were homozygousfor proline C/C at codon 25. Linden et al.28 also didnot find this genotype in the examined population.
Distribution of genotypes at position 10 differed inthe studied groups. Genotype 10T/T was underrepre-sented among renal graft recipients treated with CsA,particularly in the patients with GO. Heterozygousgenotype 10T/C was overrepresented in renal graftrecipients. Sixty-four percent of patients with GO werecarriers of the 10T/C genotype. Baan et al.36 associ-ated this genotype with CsA nephrotoxicity in patientsafter heart transplantation. TGF-b1 is also a majorfactor mediating CsA toxicity in the kidney. The asso-ciation of nephrotoxicity with the 10T/C genotypemay suggest increased activity of TGF-b1.
Homozygous genotype 10C/C in patients with GOappeared more rarely than in all the other groups andwas twice as less frequent than in the non-GO sub-group. Markedly higher incidence of genotype C/Cin renal recipients treated with CsA without GO maysuggest that this genotype exerts a protective effectsagainst GO or, inversely, lack of the genotype in pa-tients treated with CsA may be a risk factor of GO.
Linden et al.28 found different associations of TGF-b1 gene polymorphism with GO. In their study of 164renal transplant recipients treated with CsA and cal-cium channel blockers, higher overgrowth scores inpatients with genotype C/C at codon 10 comparedto 10T/T and 10T/C genotypes were reported. Pa-tients with heterozygous G/C genotype at codon 25also had a higher degree of GO.
In our study, a relationship of incidence of GOand TGF-b1 producer phenotypes was observed.
Figure 6.Frequency of GO in relationship to low (L), intermediate (I),and high (H) production phenotypes.
Figure 7.Frequency of GO in relationship to genotype in codons 10 and 25.
Figure 5.Degree of GO in association with low (L), intermediate (I),and high (H) phenotypes. Error bars represent SD.
J Periodontol • May 2006 Radwan-Oczko, Boratynska, Zietek, Zołedziewska, Jonkisz
871

Intermediate and high producer phenotypes were as-sociated with higher severity and prevalence of GOthan in the low producer phenotype. Distribution ofthe phenotypes was the same in all the patients, re-gardless of the immunosuppressive regimen, and inthe healthy controls. An association of TGF-b1 con-centration and intermediate and high producerphenotypes for patients treated with CsA and tacroli-mus was observed. Plasma level of TGF-b1 was lowerin patients treated with tacrolimus than in patientstreated with CsA in the intermediate and high pro-ducer phenotypes. Patients with GO had the highestconcentration of TGF-b1 in the intermediate producerphenotype.
The results obtained by other researchers con-cerning TGF-b1 gene polymorphism and productionor plasma level of the cytokine are controversial.Hoffmann et al.27 found no association among TGF-b1 genotypes and protein production after costimula-tion with anti-CD3/CD28 of cultured peripheral bloodlymphocytes. Yamada et al.25 described significantlyhigher plasma level of TGF-b1 in a healthy Japanesepopulation with C/C genotype at codon 10 comparedto T/C and T/T genotypes. Ochsner et al.37 found ahigher level of TGF-b1 in patients with high producergenotypes treated with CsA.
Our current study did not show why only some pa-tients treated with CsA with intermediate and highproducer phenotypes or T/C genotype at codon 10developed GO. Selective occurrence of GO may betriggered by other genetic factors (e.g., inflammatoryresponse, cytokine gene polymorphisms, receptorsfor TGF- b1, and tissue inhibitors of metalloprotein-ase). Our study showed only trends suggesting thatvariations in the TGF-b1 gene may regulate the pro-tein production and activity and thus affect the devel-opment of CsA-induced GO. The data were gatheredfrom a relatively large group of renal transplant recip-ients and healthy individuals; nevertheless, they arenot backed with strong statistical significance.
REFERENCES1. Spratt H, Boomer S, Irwin CR, et al. Cyclosporin
associated gingival overgrowth in renal transplantrecipients. Oral Dis 1999;5:27-31.
2. Thomason JM, Kelly PJ, Seymour RA. The distributionof gingival overgrowth in organ transplant patients.J Clin Periodontol 1996;23:367-371.
3. Daly CG. Resolution of cyclosporin A (CsA)-inducedgingival enlargement following reduction in CsA dos-age. J Clin Periodontol 1992;19:143-145.
4. Pernu HE, Pernu LM, Knuuttila ML. Effect of peri-odontal treatment on gingival overgrowth amongcyclosporine A treated renal transplant recipients.J Periodontol 1993;64:1098-1100.
5. Varga E, Lennon MA, Mair LH. Pre-transplant gingivalhyperplasia predicts severe cyclosporin-induced gin-
gival overgrowth in renal transplant patients. J ClinPeriodontol 1998;25:225-230.
6. Thomason JM, Seymour RA, Ellis JS, et al. Iatrogenicgingival overgrowth in cardiac transplantation. J Peri-odontol 1995;66:742-746.
7. David-Neto E, Lemos FBC, Furusawa EA, et al.Impact of cyclosporin A pharmacokinetics on thepresence of side effects in pediatric renal transplanta-tion. J Am Soc Nephrol 2000;11:343-349.
8. Thomason JM, Seymour RA, Ellis JS. Determinants ofgingival overgrowth severity in organ transplant pa-tients. An examination of the role of HLA phenotype.J Clin Periodontol 1996;23:628-634.
9. Radwan-Oczko M, Boratynska M, Klinger M, Zietek M.Risk factors of gingival overgrowth in kidney trans-plant recipients treated with cyclosporine A. AnnTransplant 2003;8:57-62.
10. Boratynska M, Radwan-Oczko M, Falkiewicz K,Klinger M, Szyber P. Gingival overgrowth in kidneytransplant recipients treated with cyclosporine and itsrelationship with chronic graft nephropathy. Trans-plant Proc 2003;35:2238-2240.
11. Mariani G, Calastrini C, Aleotti A. Ultrastructuralchanges in Langerhans cells in gingival overgrowthin cyclosporine A-treated transplant patients. Pathol-ogy 2004;36:242-246.
12. Afonso M, Oliveira Bello V, Shibli JA, Sposto MR.Cyclosporin A-induced gingival overgrowth in renaltransplant recipients. J Periodontol 2003;74:51-56.
13. Bartoli F, Castronovo G, Stabile A. Risk factors con-ditioning the incidence and severity of cyclosporineA-induced gingival overgrowth and methods of pre-vention. Minerva Stomatol 2004;53:165-170.
14. Yamaguchi M, Naruishi K, Yamada-Naruishi H, OmoriK, Nishimura F, Takashiba S. Long-term cyclosporineA exposure suppresses cathepsin-B and -L activity ingingival fibroblasts. J Periodontal Res 2004;39:320-326.
15. Paik JW, Kim CS, Cho KS, Chai JK, Kim CK, Choi SH.Inhibition of cyclosporin A-induced gingival over-growth by azithromycin through phagocytosis: Anin vivo and in vitro study. J Periodontol 2004;75:380-387.
16. Mathur H, Moretti AJ, Flaitz CM. Regression of cyclo-sporin-induced gingival overgrowth upon interruptionof drug therapy. Gen Dent 2003;51:159-162.
17. Margiotta V, Pizzo I, Pizzo G, Barbaro A. Cyclosporin-and nifedipine-induced gingival overgrowth in renaltransplant patients: Correlations with periodontaland pharmacological parameters, and HLA-antigens.J Oral Pathol Med 1996;25:128-134.
18. Berloco P, Rossi M, Pretagostini R, Sociu-Foca CortesiniN, Cortesini R. Tacrolimus as cornerstone immunosup-pressant in kidney transplantation. Transplant Proc2001;33:994-996.
19. Thorp M, DeMattos A, Bennett W, Barry J, Norman D.The effect of conversion from cyclosporine to tacrolimuson gingival hyperplasia, hirsutism and cholesterol.Transplantation 2000;69:1218-1224.
20. Kohnle M, Lutkes P, Zimmermann U, Philipp T,Heemann U. Conversion from cyclosporine to tacroli-mus in renal transplant recipients with gum hyperpla-sia. Transplant Proc 1999;31:44S-45S.
21. Busque S, Demers P, St-Louis G, et al. Conversionfrom Neoral (cyclosporine) to tacrolimus of kidneytransplant recipients for gingival hyperplasia or hy-pertrichosis. Transplant Proc 1998;30:1247-1248.
TGF-b1 Gene Polymorphism and Gingival Overgrowth Volume 77 • Number 5
872

22. Hernandez G, Arriba L, Cruz Frias M, et al. Conver-sion from cyclosporin A to tacrolimus as non-surgicalalternative to reduce gingival enlargement: A prelim-inary case series. J Periodontol 2003;74:1816-1823.
23. Wright HJ, Chapple IL, Matthews JB. TGF-beta iso-forms and TGF-beta receptors in drug-induced andhereditary gingival overgrowth. J Oral Pathol Med2001;30:281-289.
24. Li Y, Foster W, Deasy BM, et al. Transforming growthfactor-beta1 induces the differentiation of myogeniccells into fibrotic cells in injured skeletal muscle: A keyevent in muscle fibrogenesis. Am J Pathol 2004;164:1007-1019.
25. Yamada Y, Miyauchi A, Goto J, et al. Association of apolymorphism of the transforming growth factor-beta1gene with genetic susceptibility to osteoporosis inpostmenopausal Japanese women. J Bone Miner Res1998;13:1569-1576.
26. Hoffmann SC, Stanley EM, Cox ED. Association ofcytokine polymorphic inheritance and in vitro cyto-kine production in anti-CD3/CD28-stimulated periph-eral blood lymphocytes. Transplantation 2001;72:1444-1450.
27. Linden GJ, Haworth SE, Maxwell AP. The influence oftransforming growth factor-beta1 gene polymor-phisms on the severity of gingival overgrowth associ-ated with concomitant use of cyclosporin A and acalcium channel blocker. J Periodontol 2001;72:808-814.
28. Awad MR, El-Gamel A, Hasleton P, Turner DM, SinnottPJ, Hutchinson IV. Genotypic variation in the trans-forming growth factor-beta1 gene: Association withtransforming growth factor-beta1 production, fibroticlung disease, and graft fibrosis after lung transplanta-tion. Transplantation 1998;66:1014-1020.
29. Muhlemann HR, Son S. Gingival sulcus bleeding - Aleading symptom in initial gingivitis. Helv Odont Acta1971;15:107-111.
30. Coletta RD, Almeida OP, Reynolds MA, Sauk JJ.Alteration in expression of MMP-1 and MMP-2 but
not TIMP-1 and TIMP-2 in hereditary gingival fibro-matosis is mediated by TGF-b1 autocrine stimulation.J Periodontal Res 1999;34:457-463.
31. Martelli-Junior H, Cotrim P, Graner E, Sauk JJ,Coletta RD. Effect of transforming growth factor-beta1, interleukin-6, and interferon-gamma on theexpression of type I collagen, heat shock protein 47,matrix metalloproteinase (MMP)-1 and MMP-2 byfibroblasts from normal gingiva and hereditary gingi-val fibromatosis. J Periodontol 2003;74:296-306.
32. Gnoatto N, Lotufo RF, Toffoletto O, Marquezini MV.Gene expression of extracellular matrix proteoglycansin human cyclosporin-induced gingival overgrowth.J Periodontol 2003;74:1747-1753.
33. James JA, Irwin CR, Linden GJ. Gingival fibroblastresponse to cyclosporin A and transforming growthfactor beta 1. J Periodontal Res 1998;33:40-48.
34. Wright HJ, Chapple IL, Blair F, Matthews JB. Crevic-ular fluid levels of TGF-beta1 in drug-induced gingivalovergrowth. Arch Oral Biol 2004;49:421-425.
35. Steinsvoll S, Halstensen TS, Schenck K. Exten-sive expression of TGF-beta 1 in chronically-inflamedperiodontal tissue. J Clin Periodontol 1999;26:366-373.
36. Baan CC, Balk AH, Holweg CT, et al. Renal failure afterclinical heart transplantation is associated with theTGF-beta 1 codon 10 gene polymorphism. J HeartLung Transplant 2000;19:866-872.
37. Ochsner S, Guo Z, Binswanger U, Knoflach A. TGF-beta1 gene expression in stable renal transplant recip-ients: Influence of TGF-beta1 gene polymorphism andimmunosuppression. Transplant Proc 2002;34:2901-2903.
Correspondence: Dr. Małgorzata Radwan-Oczko, Depart-ment of Periodontology, Wrocław Medical University, ul.Krakowska 26, 50-425 Wrocław, Poland. Fax: 48-71-784-03-80; e-mail: [email protected].
Accepted for publication November 27, 2005.
J Periodontol • May 2006 Radwan-Oczko, Boratynska, Zietek, Zołedziewska, Jonkisz
873