Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid ...
11
Disease Markers 34 (2013) 295–304 295 DOI 10.3233/DMA-130974 IOS Press Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid of a rat model of diabetes mellitus and periodontitis Zhu-Ling Jiang a , Yu-Qiong Cui a , Rui Gao b , Ying Li a , Zhao-Chen Fu c , Bin Zhang a,∗ and Cheng-Chao Guan a,∗ a Department of Implantology, the 2nd Affiliated Hospital, Harbin Medical University, Harbin, Heilongjiang, China b Department of Orthodontics, the 1st Affiliated Hospital, Harbin Medical University, Harbin, Heilongjiang, China c Department of Oral and Maxillofacial Surgery, the 2nd Affiliated Hospital, Harbin Medical University, Harbin, Heilongjiang, China Abstract. OBJECTIVE: In this study, we sought to investigate the dynamic changes in the levels of TNF-α, IL-1β and LPS in the gingival crevicular fluid (GCF) in a rat model of diabetes mellitus (DM) and periodontitis (PD). Additionally, we evaluated alveolar bone loss and the histopathological response associated with experimental diabetes mellitus and experimental periodontitis. METHODS: DM and PD were induced together in 15 rats (group 1) by streptozotocin injection and ligature induction. Peri- odontitis alone was produced by ligature induction in 15 rats (group 2), diabetes alone was produced by streptozotocin injection in 15 rats (group 3), and fifteen systemically and periodontally healthy rats were used as controls (group 4). The gingival TNF-α, IL-1β and LPS levels were measured by using ELISA method. Periodontal destruction was assessed by measuring the alveolar bone loss. Periodontal inflammation was quantified by histopathological grading in H&E stained samples. RESULTS: Higher levels of TNF-α, IL1-β and LPS, increased alveolar bone loss and more serve histopathology were found in group 1 compared with group 2, group 3 and group 4 (p< 0.05). The quantities of TNF-α, IL1-β and LPS, the amount of alveolar bone loss and the severity of the histopathological finding were greater in group 2 than group 3 and group 4 (p< 0.05). Group 3 demonstrated higher levels of TNF-α, IL1-β and LPS, increased alveolar bone loss and more serve histopathology than group 4 (p< 0.05). Statistically significant differences were noted between all of the groups. CONCLUSIONS: These data indicate that DM may lead to enhanced TNF-α, IL1-β and LPS production in the periodontal tissues. The resorption values of alveolar bone and the histological inflammation were more severe in rats with periodontitis and diabetes mellitus than in those with periodontitis alone, diabetes mellitus alone and control rats. Our findings are consistent with the hypothesis that hyperglycemia contributes to the heightened inflammatory response associated with periodontitis. Keywords: TNF-α, IL-1β, LPS, GCF, diabetes mellitus, periodontitis, alveolar bone loss, histopathology 1. Introduction Diabetes mellitus and periodontal disease are both chronic inflammatory disorders that have a major im- pact on the health of millions of individuals worldwide. ∗ Corresponding authors: Bin Zhang and Cheng-Chao Guan, Department of Implantology, the 2nd Affiliated Hospital, Harbin Medical University, Harbin 150086, Heilongjiang, China. E-mail: [email protected], [email protected]. Periodontal disease is a recognized and well-docu- mented complication of diabetes. The evidence sup- porting this relationship is based on epidemiologic data and animal model studies that have helped to ex- plain the pathophysiology of periodontal disease as a complication of diabetes mellitus [1]. Periodontal dis- ease was proposed as the sixth complication of dia- betes mellitus. In 2008, Taylor and Borgnake [2] iden- tified periodontal disease as a possible risk factor for poor metabolic control in people with diabetes melli- ISSN 0278-0240/13/$27.50 c 2013 – IOS Press and the authors. All rights reserved
Transcript of Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid ...

Disease Markers 34 (2013) 295–304 295DOI 10.3233/DMA-130974IOS Press
Study of TNF-α, IL-1β and LPS levels in thegingival crevicular fluid of a rat model ofdiabetes mellitus and periodontitis
Zhu-Ling Jianga, Yu-Qiong Cuia, Rui Gaob, Ying Lia, Zhao-Chen Fuc, Bin Zhanga,∗ andCheng-Chao Guana,∗aDepartment of Implantology, the 2nd Affiliated Hospital, Harbin Medical University, Harbin, Heilongjiang, ChinabDepartment of Orthodontics, the 1st Affiliated Hospital, Harbin Medical University, Harbin, Heilongjiang, ChinacDepartment of Oral and Maxillofacial Surgery, the 2nd Affiliated Hospital, Harbin Medical University, Harbin,Heilongjiang, China
Abstract.OBJECTIVE: In this study, we sought to investigate the dynamic changes in the levels of TNF-α, IL-1β and LPS in the gingivalcrevicular fluid (GCF) in a rat model of diabetes mellitus (DM) and periodontitis (PD). Additionally, we evaluated alveolar boneloss and the histopathological response associated with experimental diabetes mellitus and experimental periodontitis.METHODS: DM and PD were induced together in 15 rats (group 1) by streptozotocin injection and ligature induction. Peri-odontitis alone was produced by ligature induction in 15 rats (group 2), diabetes alone was produced by streptozotocin injectionin 15 rats (group 3), and fifteen systemically and periodontally healthy rats were used as controls (group 4). The gingival TNF-α,IL-1β and LPS levels were measured by using ELISA method. Periodontal destruction was assessed by measuring the alveolarbone loss. Periodontal inflammation was quantified by histopathological grading in H&E stained samples.RESULTS: Higher levels of TNF-α, IL1-β and LPS, increased alveolar bone loss and more serve histopathology were foundin group 1 compared with group 2, group 3 and group 4 (p < 0.05). The quantities of TNF-α, IL1-β and LPS, the amount ofalveolar bone loss and the severity of the histopathological finding were greater in group 2 than group 3 and group 4 (p < 0.05).Group 3 demonstrated higher levels of TNF-α, IL1-β and LPS, increased alveolar bone loss and more serve histopathology thangroup 4 (p < 0.05). Statistically significant differences were noted between all of the groups.CONCLUSIONS: These data indicate that DM may lead to enhanced TNF-α, IL1-β and LPS production in the periodontaltissues. The resorption values of alveolar bone and the histological inflammation were more severe in rats with periodontitis anddiabetes mellitus than in those with periodontitis alone, diabetes mellitus alone and control rats. Our findings are consistent withthe hypothesis that hyperglycemia contributes to the heightened inflammatory response associated with periodontitis.
Keywords: TNF-α, IL-1β, LPS, GCF, diabetes mellitus, periodontitis, alveolar bone loss, histopathology
1. Introduction
Diabetes mellitus and periodontal disease are bothchronic inflammatory disorders that have a major im-pact on the health of millions of individuals worldwide.
∗Corresponding authors: Bin Zhang and Cheng-Chao Guan,Department of Implantology, the 2nd Affiliated Hospital, HarbinMedical University, Harbin 150086, Heilongjiang, China. E-mail:[email protected], [email protected].
Periodontal disease is a recognized and well-docu-mented complication of diabetes. The evidence sup-porting this relationship is based on epidemiologicdata and animal model studies that have helped to ex-plain the pathophysiology of periodontal disease as acomplication of diabetes mellitus [1]. Periodontal dis-ease was proposed as the sixth complication of dia-betes mellitus. In 2008, Taylor and Borgnake [2] iden-tified periodontal disease as a possible risk factor forpoor metabolic control in people with diabetes melli-
ISSN 0278-0240/13/$27.50 c© 2013 – IOS Press and the authors. All rights reserved

296 Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid
tus. This bidirectional relationship between periodon-tal disease and diabetes mellitus makes diabetes a dis-order of importance to dentists and dental hygienists aswell as dental patients.
Tumour necrosis factor (TNF-α) has been reportedto play a key role in the pathogenesis of type 2 di-abetes [3]. Several lines of evidence support this hy-pothesis. In animal [4] and in vitro human cell models,TNF-α inhibits the action of insulin. In human cross-sectional studies, elevated levels of circulating TNF-αare associated with insulin resistance [5] and type 2 di-abetes [6]. Longitudinal human study shows elevatedplasma TNF-α to be concomitant with worsening ofglycemic control [7]. Recently, Bretz et al. [8] showedthat circulating TNF-α was associated with more se-vere periodontitis in a large geriatric cohort. Subjectswith periodontitis appear to have an elevated TNF-α response, as lipopolysaccharide (LPS)-challengedmacrophages derived from periodontitis patients re-lease greater quantities of TNF-α compared with non-periodontitis controls. Salvi et al. [9] noted that mono-cytes from subjects with both diabetes and periodonti-tis appears to release greater quantities of TNF-α.
Meanwhile, Teles [10] compared the mean levels ofIL-1β in GCF samples from periodontally healthy sub-jects and subjects with chronic periodontitis and foundthat IL-1β displayed the strongest relationship to theclinical signs of periodontitis. These findings supportprevious reports [11] of associations between the lev-els of IL-1β and the clinical signs of periodontal dis-ease. Diabetes mellitus patients have elevated levels ofadvanced glycation end products (AGEs) [12] that caninteract with specific receptors, such as macrophages,stimulating the production of cytokines such as IL-1. Monocytes from diabetes mellitus patients producesignificantly greater amounts of IL-1β in vitro thanmonocytes from non-diabetic controls [13].
Lipopolysaccharide is one of the most important mi-crobial virulence factors in generating host-mediatedperiodontal tissue destruction. LPS provides a micro-be-associated molecular pattern that is recognized byreceptors on resident immune and non-immune cellswithin the periodontium [14]. Rogers [15] demon-strated that LPS endotoxin from the periodontal patho-gen A. actinomycetemcomitans initiated severe alveo-lar bone loss and significant elevations in the levels ofinflammatory cytokines and osteoclastogenesis. Bacte-rial LPS is a potent stimulator of many inflammatorymediators, including IL-1β and TNF-α [16].
It has been hypothesized that type 2 diabetes melli-tus-related alterations in the levels of inflammatory
mediators in the gingival crevicular fluid (GCF) lev-els of inflammatory mediators maybe part of the mech-anism by which diabetes affects periodontal health.Therefore, the aim of this study was to evaluate GCFlevels of TNF-α, IL-1β and LPS in a Sprague-Dawleyrat model with type 2 DM and/or periodontal disease.
2. Materials and methods
2.1. Statement of ethics
All animal work has been conducted in accordancewith international animal experimentation guidelines(NIH Pub. No. 85–23, revised 1996) and was approvedby Animal Care and Use Committee of the HarbinMedical University (Harbin, China). All necessary per-mits were obtained for the described field studies.
2.2. Production of experimental rats with DM
A total of 60 male Sprague-Dawley rats (200–220 g)were obtained from the experimental animal center ofthe second affiliated hospital of Harbin Medical Uni-versity (Harbin, China). The animals were acclima-tized for at least 1 week before the start of the ex-periment and were housed in a temperature-controlledanimal facility under a 12-hour light/dark cycle withenough laboratory chow and water. The experimentalprotocols were carried out following ethical principlesfor laboratory animal use. A total of 30 rats were fed anadequate HF diet [17] (34.5% fat, 17.5% protein, 48%carbohydrate; Beijing HFK Bio-Technology, China),and the other 30 rats were received normal chow forfour weeks. Then the rats that fed with HF diet wereinjected under low light with a single intraperitonealinjection of freshly prepared streptozocin [17] (STZ,30 mg/kg; i.p. in 0.1 mol/L citrate buffer, pH 4.5;Sigma Aldrich, Co., 3050 Spruce Street, St. Louis, MO63103 USA) to induce diabetes models after abrosiaedfor at least 12 hours. The blood glucose levels weremeasured randomly on the third and seventh days afterSTZ injection with a commercial blood glucose moni-toring kit in blood samples obtained from the tail vein.Rats with RBG > 11.1 mmol/L in two consecutiveanalyses were considered diabetic [18]. DM was con-firmed by the increase in the blood glucose level andthe body weight loss as described in the referred stud-ies.

Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid 297
2.3. Production of experimental rats with PD
A total of 15 systemically healthy rats were anes-thetized by a single intraperitoneal injection of 10%chloral hydrate (Traditional Chinese Medicine GroupChemical Reagent Co., Ltd. No: 20080325) at a doseof 0.3 ml per 100 g of body weight [19]. After theanesthesia, a 1-0 cotton ligature (Ethicon, Johnson andJohnson, São Paulo, SP, Brazil) was placed around themaxillary second molar in a submarginal position toinduce experimental periodontitis [20,21]. The ligaturewas knotted on the buccal side of the teeth. The liga-tures were left in place until the collection of GCF. Anew ligature was placed immediately after the collec-tion of GCF. Periodontitis was confirmed by the gradeof the infiltration of inflammatory cells in the gingivalhistopathological analysis and alveolar bone loss quan-tification at the experimental sites.
2.4. Production of experimental rats with DM and PD
A total of 15 diabetic rats underwent the proceduresdescribed above to induce periodontitis and diabetesmellitus.
The groups were as follows:
Group 1: rats with diabetes mellitus and periodon-titis (n = 15)Group 2: systemically healthy rats with periodon-titis (n = 15)Group 3: periodontally healthy rats with diabetesmellitus (n = 15)Group 4: systemically and periodontally healthyrats (n = 15)Gingival crevicular fluid (GCF) collection
Glucose concentrations and body weight were mea-sured once a week in all 60 rats. Five rats were ran-domly selected from each group for the collection ofgingival crevicular fluid (GCF) from the mesio-buccalregion of the maxillary right molar under anesthesia aspreviously described [22,23]. GCF was collected dur-ing the second, fourth and sixth weeks after inductionof periodontitis. The teeth were air dried and isolatedwith cotton rolls after removing the ligament. Withouttouching the marginal gingiva, GCF was collected us-ing adsorbent paper points (Beijing, Dayading Med-ical Apparatus and Instruments Co., Ltd.). The GCFcollection was repeated three times per site, and sevenabsorbent paper points were used for each collection.The last paper point used for each sampling was heldin the gingival sulcus for 30 seconds. After collection,
the paper points were immediately transferred into aplastic vial with 20 μl sample diluent (sample diluentfrom Rat TNF-α Platinum ELISA KIT, sample diluentfrom Rat IL-1β ELISA KIT, sample diluent from RatLPS ELISA KIT) and stored at −80◦C until the assay.
2.5. Analysis of TNF-α, IL-1β and LPS in the GCF
The TNF-α, IL-1β and LPS levels in the GCF fromeach group were measured using an enzyme-linked im-munosorbent assay (ELISA). This assay was a sand-wich ELISA and was performed according to manufac-turer’s instructions. All of the samples and standardswere assayed in duplicate, as suggested by the man-ufacturer (Rat TNF-α ELISA KIT eBioscience Cam-pus Vienna Biocenter2 1030 Vienna, Austria; Rat IL-1βELISA KIT NeoBioscience Technology Co., Ltd.;Rat LPS ELISA KIT Biovalue Technology Co., Ltd.).After appropriate dilution of the samples, 100 μL ofeach sample was added to the appropriate wells, andthe plate was sealed and incubated at 37◦C for 1 h. Fol-lowing incubation and washing seven times, 100 μLof the labeled antibody was pipetted into the wells,followed by incubation at 4◦C for 30 min. Then, theplate was washed nine times, and 100 μL of the sub-strate solution was added to each well followed by in-cubation at room temperature for 30 min in the dark.Lastly, 100 μL of stop solution was added to each well,and the plate was read immediately to determine theabsorbance of each well using a microplate (enzyme-linked immunosorbent assay) reader (Thermo Labsys-tems Multiskan Mk 3) set at a wavelength of 450 nm(OD450). The levels of IL-1β, TNF-α and LPS in thetested samples were computed using the standard curveplotted with the optical density values obtained fromthe assay.
2.6. Assessment of alveolar bone loss
The rats were sacrificed with an overdose of sodiumpentobarbital the same day after the GCF was col-lected, and the excised maxillae were fixed in 10%neutral buffered formalin for 48 hours. Both maxillaryhalves were fixed. Then, one lateral maxillary half wasused for measurement of alveolar bone loss. The eval-uation of the extent of periodontal destruction basedon the measurement of the alveolar bone loss was per-formed as described previously [24]. Quantificationwas performed by a investigator who was unaware ofthe samples analyzed through measuring the distancebetween the CEJ and the BC along the axis of each root

298 Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid
Table 1The concentrarions (mean ± SD, pg/ml) of TNF-α in samples collected at each time point in different groups throughout the study
Groups Week 2 Week 4 Week 6Diabetes and periodontitis 35.59 ± 2.80d 68.49 ± 1.20d,∗ 48.88 ± 3.65d,∗,#Periodontitis 29.46 ± 0.69c 57.76 ± 0.88c,∗ 33.87 ± 2.00c,∗,#Diabetes 26.02 ± 1.33b 41.52 ± 4.21b,∗ 28.92 ± 2.06b,∗,#Normal 16.38 ± 3.77a 19.38 ± 2.75a 14.53 ± 2.32a
Data are means ± SD. Data with different superscript letters are significantly different (P < 0.05) in the same time among four groups. ∗Differentfrom week 2 (P < 0.05). #Different from week 4 (P < 0.05).
Table 2The concentrarions (mean ± SD, pg/ml) of IL-1β in samples collected at each time point in different groups throughout the study
Groups Week 2 Week 4 Week 6Diabetes and periodontitis 121.82 ± 2.42d 145.10 ± 3.48d,∗ 196.89 ± 4.52d,∗,#Periodontitis 86.54 ± 3.20c 90.84 ± 4.63c 92.92 ± 3.07c
Diabetes 32.86 ± 3.92b 32.67 ± 4.76b 36.22 ± 2.07b
Normal 21.21 ± 2.34a 19.38 ± 4.09a 18.31 ± 2.08a
Data are means ± SD. Data with different superscript letters are significantly different (P < 0.05) in the same time among four groups. ∗Differentfrom week 2 (P < 0.05). #Different from week 4 (P < 0.05).
Table 3The concentrarions (mean ± SD, eu/ml) of LPS in samples collected at each time point in different groups throughout the study
Groups Week 2 Week 4 Week 6Diabetes and periodontitis 0.572 ± 0.034d 0.701 ± 0.047d,∗ 0.662 ± 0.051d,∗Periodontitis 0.368 ± 0.034c 0.432 ± 0.025c,∗ 0.412 ± 0.013c,∗Diabetes 0.163 ± 0.009b 0.225 ± 0.011b,∗ 0.194 ± 0.014b,∗Normal 0.081 ± 0.003a 0.086 ± 0.005a 0.087 ± 0.005a
Data are means ± SD. Data with different superscript letters are significantly different (P < 0.05) in the same time among four groups. ∗Differentfrom week 2 (P < 0.05).
Table 4Values of alveolar bone absorption (mean ± SD, mm) of rats
Groups Week 2 Week 4 Week 6Diabetes and periodontitis 2.55 ± 0.20d 2.65 ± 0.15d 2.60 ± 0.25d
Periodontitis 1.65 ± 0.15c 1.75 ± 0.10c 1.80 ± 0.10c
Diabetes 1.20 ± 0.05b 1.30 ± 0.20b 1.30 ± 0.05b
Normal 0.95 ± 0.05a 0.90 ± 0.10a 0.95 ± 0.10a
Data are means ± SD. Data with different superscript letters are significantly different (P < 0.05) in the same period among four groups.
surface of the second molar teeth. Two recordings fortwo roots were made, and the total alveolar bone losswas obtained by taking the sum of the recordings fromthe buccal tooth surface [25].
2.7. Histopathological analysis
The other lateral half of maxillary was demineral-ized in 10% EDTA after fixation for histopathologicalanalysis. The specimens in EDTA were demineralizedfor no less than 30 days. They were then dehydratedand embedded in paraffin, and paraffin serial sections(6 μm) were obtained in the mesiodistal direction andstained with hematoxylin and eosin (H&E). The his-tological features where a ligature had been placedwere evaluated under a light microscope. Parameters
such as the inflammatory cell influx and the periodon-tal tissue integrity were analyzed by a histologist in asingle-blind fashion [26]. The grades were as follows:Score 0: the absence of or only discrete cellular infil-tration (inflammatory cell infiltration was sparse andrestricted to the marginal gingival region), preservedalveolar process and cementum. Score 1: moderate cel-lular infiltration (inflammatory cellular infiltration waspresent throughout the inserted gingiva), minor alveo-lar process resorption and intact cementum. Score 2:accentuated cellular infiltration (inflammatory cellularinfiltration was present in both the gingiva and the peri-odontal ligament), accentuated degradation of the alve-olar process, and partial destruction of the cementum.Score 3: accentuated cellular infiltrate, complete re-

Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid 299
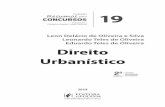
Fig. 1. Illustrates the group with STZ-induced diabetes and ligature-induced periodontitis. The histopathology of the periodontium of the ani-mals subjected to experimental diabetes and periodontitis revealed severe inflammatory cell infiltration coupled with cementum destruction andalveolar process destruction. (Colours are visible in the online version of the article; http://dx.doi.org/10.3233/DMA-130974)
sorption of the alveolar process and severe destructionof the cementum [27].
2.8. Statistical analysis
The data was expressed as the mean ± standard de-viation (SD). A test for normality was performed onthe data to meet the normal distribution before the two-way factorial ANOVA. When interaction and/or themain effects were significant, means were comparedusing the SNK post hoc test. Kruskal-Wallis test wasused to test for differences in pathological grading ofthe periodontium among four groups. Statistical anal-ysis was performed by using SPSS version 15.0.1 forWindows (SPSS Inc., USA). A p value less than 0.05was considered statistically significant.
3. Results
3.1. TNF-α, IL-1β and LPS levels in GCF
We sought to determine whether type 2 diabetesmellitus alters the TNF-α levels in GCF. The TNF-αlevels of the rats in this study (mean ± SD) are pro-vided in Table 1. The samples were analyzed individu-ally, and the data was pooled for each rat. The TNF-αlevels were significantly different among four groups atthe same time point. Rats with periodontitis (PD) anddiabetes (DM) had significantly higher levels of TNF-α in the GCF than those with PD alone (p < 0.05),DM alone (p < 0.05) or the control rats (p < 0.05).Animals subjected to PD alone had higher levels thanthose with DM alone (p < 0.05) or controls (p < 0.05).Additionally, the DM rats had higher levels comparedto the control rats (p < 0.05). While between the times,the levels of TNF-α were increased at week 4 and week
6 compared to week 2 (p < 0.05), and the differenceswere significant between week 4 and week 6 except fornormal group.
To detect if type 2 diabetes mellitus affect the IL-1β levels in the GCF. The results are provided in Ta-ble 2 and showed that IL-1β levels were significantlydifferent among the four groups at the same time point.Rats with PD and DM had significantly higher levels ofGCF IL-1β than those with PD alone (p < 0.05), DMalone (p < 0.05) and control rats (p < 0.05). Animalssubjected to PD alone had higher levels than those withDM alone (p < 0.05) and control rats (p < 0.05). Andthat the DM rats had higher levels compared to controlrats (p < 0.05). Between the different periods, onlyrats with PD and DM showed higher levels of IL-1βat week 4 and week 6 contrast to week 2 (p < 0.05).The increased level could be found between week 4and week 6 (p < 0.05).
The LPS levels in GCF of the rats included in thisstudy (mean ± SD) are provided in Table 3. We foundthat the levels were significantly different among thefour groups at the same time point. Rats with PD andDM showed higher levels of GCF LPS than those withPD alone (p < 0.05), DM alone (p < 0.05) and controlrats (p < 0.05). Rats subjected to PD alone had higherlevels than those with DM alone (p < 0.05) and controlrats (p < 0.05). Additionally, the DM rats had higherlevels compared to the control rats (p < 0.05). Rats inPD and DM group, PD group and DM group expressedhigh levels of LPS at week 4 and week 6 comparedwith week 2 (p < 0.05).
3.2. Macroscopic analysis
Table 4 shows the resorption values of the alveolarbone in the upper second molar in the four groups atdiffident time points. The rats with PD and DM showed

300 Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid
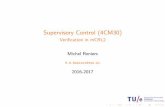
Fig. 2. Illustrates the group with ligature-induced periodontitis. Rats subjected to periodontitis revealed inflammatory cell infiltration accompaniedby cementum and alveolar bone destruction. (Colours are visible in the online version of the article; http://dx.doi.org/10.3233/DMA-130974)
Fig. 3. Illustrates the group with STZ-induced diabetes. Rats subjected to experimental diabetes alone did not manifest bone loss, but they did ex-hibit inflammatory changes in the periodontium. (Colours are visible in the online version of the article; http://dx.doi.org/10.3233/DMA-130974)
Fig. 4. Illustrates the control group. The histological analysis of group 4 shows the structure of a normal periodontium in which the gingiva,periodontal ligament, alveolar bone and cementum can be observed. (Colours are visible in the online version of the article; http://dx.doi.org/10.3233/DMA-130974)
Table 5Pathological grading of the periodontium of rats
Groups Week 2 Week 4 Week 6Diabetes and periodontitis 2,2,2,3,2 3,3,3,3,2 3,3,3,3,3Periodontitis 1,1,1,0,1 2,2,2,1,2 3,3,3,2,3Diabetes 0,0,0,0,0 1,1,1,0,1 1,1,1,1,1Normal 0,0,0,0,0 0,0,0,0,0 0,0,0,0,0
Data indicates the pathological grading scores of five rats at differenttime periods among four groups.
more alveolar bone loss than those with PD alone, DMalone and control rats at the same time point. Rats withPD and DM had significantly greater resorption values
of the alveolar bone than those with PD alone (p <0.05), DM alone (p < 0.05) and control rats (p <0.05). Animals subjected to PD alone had greater val-ues than those with DM alone (p < 0.05) and controlrats (p < 0.05). Additionally, the DM rats had highervalues compared to the control rats (p < 0.05).
3.3. Histological analysis
Rats subjected to experimental diabetic mellitus andperiodontitis exhibited inflammatory cell infiltrationcoupled with serve cementum destruction and alveolar

Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid 301
process destruction (Fig. 1), receiving scores rangingfrom 2 to 3 (Table 5). The periodontitis group revealedinflammatory cell infiltration accompanied by cemen-tum and alveolar bone destruction (Fig. 2), receivingscores ranging from 1 to 3 (Table 5). The diabetes mel-litus group showed moderate or an absence of cellu-lar infiltration, no or minor alveolar process resorptionand intact cementum (Fig. 3), receiving scores rangingfrom 0 to 1 (Table 5). The control group presented anormal periodontium in which the gingiva, periodon-tal ligament, alveolar bone and cementum could be ob-served (Fig. 4).
4. Discussion
The key findings of the present study was that ratswith PD and DM had high levels of TNF-α, IL-1β andLPS in GCF as well as substantial resorption of thealveolar bone and histological inflammation. The gin-gival crevicular fluid is a serum transudate that is en-riched with microbial and host products that arise asa result of the current inflammatory dynamics of thehost-biofilm interaction. GCF is derived from the peri-odontal tissues, and its analysis provides an early indi-cation of biochemical changes in the tissues that willultimately manifest as a clinical lesion. Another dis-tinct advantage of using GCF analysis as the basis for adiagnostic test is that the most popular collection sys-tem (precut methylcellulose filter strips) allows multi-ple sites in the mouth to be sampled and analyzed [28].
We chose to evaluate IL-1β, LPS, and TNF-α be-cause their expression occurs in periodontitis alongwith the loss of connective tissue and bone. The pro-inflammatory cytokines IL-1 and TNF-α can inducebone resorption indirectly by promoting differentiationof osteoclast precursors and subsequently by activatingosteoclasts. Earlier studies in models of experimentalgingivitis have demonstrated the increase in GCF lev-els of IL-1β [23]. Heasman [29] conducted a study todetermine the sequence of cytokine and lipid media-tor activation within the periodontium during the de-velopment of experimental gingivitis in humans. Theyfound that the GCF levels of IL-1β increased abruptlyfrom mean baseline values of 16.5 ± 9.3 ng/ml to131 ± 76.0 ng/ml at 1 week and remained at thislevel for the duration of the experiment. The findingsdescribed above are similar to our results in whichrats with PD had higher levels of IL-1β in the GCFthan control animals. Because Gram-negative microor-ganisms predominate in the subgingival environment
and contain LPS in their outer membranes, these bac-teria may be released during infection. Furthermore,it has been demonstrated that LPS elicits TNF pro-duction [30]. The priming of polymorphonuclear cells(PMNs) by LPS and TNF-α results in an enhanced ox-idative burst and enhanced degranulation [31]. The se-creted agents also enhance the production of numerousproinflammatory cytokines that contribute to the dis-ease, including TNF-α and IL-1β, among a broad arrayof biomolecules that have consistently been reported tobe elevated in the gingival crevicular fluid (GCF) andtissues of periodontitis patients [32]. IL-1β and TNF-α have been shown to dramatically enhance the oxida-tive burst of PMN in response to secondary stimula-tion [30]. These findings are accordance with our re-sults and account for the elevated levels of TNF-α, IL-1β and LPS in the GCF of periodontitis patients.
Because all individuals are not equally susceptibleto the destructive effects of periodontal infections, pe-riodontitis is not only caused by bacterial infection butalso associated with host susceptibility. Several biolog-ically plausible mechanisms have been proposed to ex-plain the interactions between diabetes and periodon-tal diseases. Chronic gram-negative periodontal infec-tions may induce or perpetuate an elevated chronic sys-temic inflammatory state, contributing to increased in-sulin resistance and poor glycemic control [16]. In-creased serum concentrations of acute-phase responsemarkers and cytokines have been observed in patientswith diabetes [33], which indicates that circulating in-flammatory cytokines influence the risk for diabetes.The impact of glycemic control in diabetes on peri-odontal diseases and the mechanisms through whichthis effect might occur is less clear. In our studies,we found that rats with PD and DM had higher levelsof TNF-α, IL-1β and LPS in their GCF than animalswith PD alone; meanwhile, the levels of resorption ofthe alveolar bone were higher and histological inflam-mation was more severe than in rats with PD alone.To a certain extent, our results confirm previous find-ings that periodontitis was more severe in subjects withdiabetes compared with non-diabetics [34]. Our find-ing that higher levels of TNF-α, IL-1β and LPS werepresent in the GCF from the PD and DM group than thePD group indicated that diabetes influences the gingi-val cytokine and LPS levels in periodontitis and wors-ens the macroscopic and histopathological characteris-tics of periodontitis.
The levels of TNF-α, IL-1β and LPS were increasedat week 4 and week 6 compared to week 2. These couldbe due to the inflammation development process. From

302 Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid
the results we found that TNF-α levels decreased atweek 6 compared to week 4, but still remaining sig-nificantly above week 2. As periodontal tissue itselfcould make repair response to injury and the lower lev-els of TNF-α seem to be related to the preservation ofhomeostasis and to the remodeling/healing of damagedtissue through the activation and formation of fibrob-lasts [35]. Since there was no significantly increasedIL-1β at week 4 and week 6 compared to week 2 in PDgroup and DM group, diabetes or periodontitis alonemay not be sufficient to elicit marked changes in IL-1βlevels over a short time. And further research is neededto study the influence of time on the gradual secreteprocess of cytokines.
Alveolar bone resorption is an inevitable result ofperiodontitis, and it has also been observed in di-abetic conditions [36]. The mechanisms of alveolarbone metabolism and/or resorption in DM have beenexplained previously. Mishima et al. [37] and Villarinoet al. [38] suggested that streptozotocin-induced DMmight have had short-term effects on bone metabolismand may have reduced the rate of bone turnover in thealveolar wall surrounding the root. These are in ac-cordance with our findings that we observed enhancedalveolar bone resorption in the DM and PD group com-pared with the other groups.
The main pathogenic component of bacterial bio-films is LPS, and these films have been shown tobe necessary for the initiation of gingival inflamma-tion and subsequent destruction of periodontal tis-sues. Based on an established model of pathogene-sis, the presence of a bacterial biofilm alone is in-sufficient to explain disease initiation and progres-sion. Evidence [37] suggests that periodontal tissue de-struction is mainly due to the host’s inflammatory re-sponse to the bacterial challenge. Investigations intothe mechanisms of the host-mediated response in pe-riodontal disease have revealed that it involves the ac-tivation of the broad axis of innate immunity, specif-ically by upregulation of proinflammatory cytokines(TNF-α, IL-1β and so on) from monocytes and poly-morphonuclear leukocytes. Toll-like receptors are themost studied pattern recognition receptors, and theyare present at the cell surface as transmembrane re-ceptors. Toll-like receptor-4 recognizes lipopolysac-charide on macrophages. Binding to the pattern recog-nition receptors activates the nuclear factor-κB (NF-κB) signaling pathway, which induces immune re-sponse genes, especially those for inflammatory cy-tokines. Inappropriate secretion of these cytokines, interms of either type or quantity, characterizes a dys-
regulated immune response that leads to destructionof the periodontal tissues in the presence of a Gram-negative bacterial biofilm. These locally produced cy-tokines move into the systemic circulation, where theymay perpetuate an elevated inflammatory state, wors-ening the patient’s diabetes by increasing insulin re-sistance and glucose levels [39]. These are the mecha-nisms through which periodontal infections contributeto diabetes mellitus.
In subjects with diabetes, chronically elevated bloodglucose levels lead to the accelerated formation ofadvanced glycation end products (AGEs). Endothe-lial cells and monocytes possess specific receptors forAGEs located on their cell surfaces. The interactionof macrophages with AGEs has been shown to stim-ulate increased secretion of pro-inflammatory media-tors, such as TNF-α and IL-1β [40]. As demonstratedby a 2.9-fold increase in the risk for periodontitis inindividuals with poorly controlled glycemia comparedwith normal individuals, diabetes mellitus is a majorrisk factor for the development of periodontitis. How-ever, the mechanisms by which hyperglycemia can in-duce periodontal destruction have not to be fully eluci-dated. The results of our studies revealed elevated lev-els of TNF-α, IL-1β and LPS in the GCF of rats withPD and DM compared to rats with PD alone, rats withDM alone and control rats. The resorption values ofthe alveolar bone and histological inflammation werethe lowest in the control rats, higher in the DM aloneand PD alone groups and highest in the PD and DMgroup. These results might indicate that diabetes melli-tus promotes periodontitis through elevated inflamma-tory cytokines (TNF-α and IL-1β) and bacterial endo-toxin (LPS).
Periodontitis worsens the manifestations of dia-betes through the LPS-TLR4-NF-κB signaling path-way. Toll-like receptors (TLRs) are a family of pat-tern recognition receptors (PRRs) that recognize mi-crobial components and mediate the activation of hostresponse [41]. After Toll-like receptor-4 recognizeslipopolysaccharide on macrophages, they bind thenmicrobial LPS utilizes TLR4 to activate nuclear factor-κB (NF-κB), leading to inappropriate secretion of pro-inflammatory cytokines. These locally produced cy-tokines move into the systemic circulation increas-ing insulin resistance and glucose levels [39]. Accord-ing to our results, it is unclear whether diabetes mel-litus promotes periodontitis through the LPS-TLR4-NFκB signaling pathway as well. Whether treatmentbased on inhibiting a part of this pathway may curediabetes mellitus or periodontitis remains to be deter-mined. Therefore, additional studies are warranted.

Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid 303
Acknowledgements
The authors thank Nai-qian Wang (Department ofPathology, Harbin Medical University) for his excel-lent technical assistance.
Funding
This work was supported by Natural Science Foun-dation of China (No. 81170960). The funders sup-ported study design, data collection and analysis, deci-sion to publish, and preparation of the manuscript.
Conflict of interest
The authors declare that there is no duality of inter-est associated with this manuscript.
References
[1] Pontes Andersen CC, Flyvbjerg A, Buschard K, Holmstrup P,Relationship between periodontitis and diabetes: lessons fromrodent studies, J Periodontol (2007), 78: 1264–1275.
[2] Taylor GW, Borgnakke WS, Periodontal disease: Associa-tions with diabetes, glycemic control and complications, OralDis (2008), 14: 191–203.
[3] Nishimura F, Iwamoto Y, Mineshiba J, Shimizu A, Soga Y,Murayama Y, Periodontal disease and diabetes mellitus: Therole of tumor necrosis factor-alpha in a 2-way relationship, JPeriodontol (2003), 74: 97–102.
[4] Hotamisligil GS, Peraldi P, Budavari A, Ellis R, White MF,Spiegelman BM, IRS-1-mediated inhibition of insulin recep-tor tyrosine kinase activity in TNF-alpha- and obesity-inducedinsulin resistance, Science (1996), 271: 665–668.
[5] Mishima Y, Kuyama A, Tada A, Takahashi K, Ishioka T, Ki-bata M, Relationship between serum tumor necrosis factor-alpha and insulin resistance in obese men with Type 2 diabetesmellitus, Diabetes Res Clin Pract (2001), 52: 119–123.
[6] Fernandez-Real JM, Lainez B, Vendrell J, Rigla M, Castro A,Peñarroja G, Broch M, Pérez A, Richart C, Engel P, RicartW, Shedding of TNF-alpha receptors, blood pressure, and in-sulin sensitivity in type 2 diabetes mellitus, Am J Physiol En-docrinol Metab (2002), 282: E952–959.
[7] Lechleitner M, Herold M, Dzien-Bischinger C, Hoppichler F,Dzien A, Tumour necrosis factor-alpha plasma levels in el-derly patients with Type 2 diabetes mellitus-observations over2 years, Diabet Med (2002), 19: 949–953.
[8] Bretz WA, Weyant RJ, Corby PM, Ren D, Weissfeld L,Kritchevsky SB, Harris T, Kurella M, Satterfield S, VisserM, Newman AB, Systemic inflammatory markers, periodon-tal diseases, and periodontal infections in an elderly popula-tion, J Am Geriatr Soc (2005), 53: 1532–1537.
[9] Salvi GE, Beck JD, Offenbacher S, PGE2, IL-1 beta, andTNF-alpha responses in diabetics as modifiers of periodontaldisease expression, Ann Periodontol (1998), 3: 40–50.
[10] Teles R, Sakellari D, Teles F, Konstantinidis A, Kent R,Socransky S, Haffajee A, Relationships among gingivalcrevicular fluid biomarkers, clinical parameters of periodontaldisease, and the subgingival microbiota, J Periodontol (2010),81: 89–98.
[11] Cetinkaya B, Guzeldemir E, Ogus E, Bulut S, Pro- and Anti-inflammatory Cytokines in Gingival Crevicular Fluid andSerum of Rheumatoid Arthritis and Chronic Periodontitis Pa-tients, J Periodontol 2012 Mar 13. [Epub ahead of print].
[12] Ryan ME, Carnu O, Kamer A, The influence of diabetes onthe periodontal tissues, J Am Dent Assoc (2003), 134: 34S–40S.
[13] Salvi GE, Collins JG, Yalda B, Arnold RR, Lang NP, Offen-bacher S, Monocytic TNF alpha secretion patterns in IDDMpatients with periodontal diseases, J Clin Periodontol (1997),24: 8–16.
[14] Akira S, Hemmi H, Recognition of pathogen-associatedmolecular patterns by TLR family, Immunol Lett (2003), 85:85–95.
[15] Jill E. Rogers, Fei Li, Derek D. Coatney, Actinobacillus acti-nomycetemcomitans Lipopolysaccharide-Mediated Experi-mental Bone Loss Model for Aggressive Periodontitis, J Pe-riodontol (2007), 78: 550–558.
[16] Hersh D, Weiss J, Zychlinsky A, How bacteria initiate inflam-mation: Aspects of the emerging story, Curr Opin Microbiol(1998), 1: 43–48.
[17] K. Srinivasan, B. Viswanad, Lydia Asrat, C.L. Kaul, P.Ramarao, Combination of high-fat diet-fed and low-dosestreptozotocin-treated rat: A model for type 2 diabetesand pharmacological screening, Pharmacological Research(2005), 52: 313–320.
[18] Ti Y, Xie GL, Wang ZH, Bi XL, Ding WY, Wang J, JiangGH, Bu PL, Zhang Y, Zhong M, Zhang W, TRB3 gene silenc-ing alleviates diabetic cardiomyopathy in a type 2 diabetic ratmodel, Diabetes (2011), 60: 2963–2974.
[19] Semenoff Segundo A, Semenoff TA, Borges AH, Pedro FL,Sakai VT, Methodological model of chronic stress associ-ated with ligature-induced periodontitis in rats: a radiographicstudy, Braz Oral Res (2010), 24: 455–459.
[20] Semenoff TADV, Semenoff-Segundo A, Bosco AF, NagataMJ, Garcia VG, Biasoli ER, Histometric analysis of liga-tureinduced periodontitis in rats: A comparison of histologicalsection planes, J Appl Oral Sci (2008), 16: 251–256.
[21] Souza DM, Rocha RF, Low caloric value of ethanol itself in-creases alveolar bone loss in ligature-induced periodontitis inmale rats, Bras Oral Res (2009), 23: 460–466.
[22] Lamster IB, Oshrain RL, Celenti R, Levine K, Fine JB, Corre-lation analysis for clinical and gingival crevicular fluid param-eters at anatomically related gingival sites, J Clin Periodontol(1991), 18: 272–277.
[23] Hagai Hazan-Molina, Abraham Z. Reznick, Hanna Kauf-man,Dror Aizenbud, Assessment of IL-1β and VEGF concen-tration in a rat model during orthodontic tooth movement andextracorporeal shock wave therapy, Archives of Oral Biology2012 October 22, [Epub ahead of print].
[24] Lalla E, Lamster IB, Feit M, Huang L, Schmidt AM, A murinemodel of accelerated periodontal disease in diabetes, J Peri-odontal Res (1998), 33: 387–399.
[25] de Lima V, Bezerra MM, de Menezes Alencar VB, Vidal FD,da Rocha FA, de Castro Brito GA, de Albuquerque RibeiroR, Effects of chlorpromazine on alveolar bone loss in experi-mental periodontal disease in rats, Eur J Oral Sci (2000), 108:123–129.
[26] Carvalho RS, de Souza CM, Neves JC, Holanda-Pinto SA,

304 Z.-L. Jiang et al. / Study of TNF-α, IL-1β and LPS levels in the gingival crevicular fluid
Pinto LM, Brito GA, de Andrade GM, Effect of venlafaxineon bone loss associated with ligature-induced periodontitis inWistar rats, J Negat Results Biomed (2010), 9: 3.
[27] Leitão RF, Ribeiro RA, Chaves HV, Rocha FA, Lima V, BritoGA, Nitric oxide synthase inhibition prevents alveolar boneresorption in experimental periodontitis in rats, J Periodontol(2005), 76: 956–963.
[28] Steven Offenbacher, DDs, PhD, MMSC, 1 Silvana Barros,DDS, PhD, 1 L Mendoza, DDS, S Mauriello, MS, J Preisser,PhD, K Moss, Marko de Jager, PhD, MMSc, 2 and MarceloAspiras, PhD2, Changes in Gingival Crevicular Fluid Inflam-matory Mediator Levels during the Induction and Resolutionof Experimental Gingivitis in Humans, J Clin Periodontol(2010), 37: 324–333.
[29] Heasman PA, Collins JG, Offenbacher S, Changes in crevic-ular fluid levels of interleukin-1 beta, leukotriene B4, pro-staglandin E2, thromboxane B2 and tumour necrosis factor al-pha in experimental gingivitis in humans, J Periodontal Res(1993), 28: 241–247.
[30] Beutler BA, Milsark IW, Cerami A, Cachectin/tumor necrosisfactor: Production, distribution, and metabolic fate in vivo, JImmunol (1985), 135: 3972–3977.
[31] Danchuk S, Ylostalo JH, Hossain F, Sorge R, Ramsey A,Bonvillain RW, Lasky JA, Bunnell BA, Welsh DA, ProckopDJ, Sullivan DE, Human multipotent stromal cells attenuatelipopolysaccharide-induced acute lung injury in mice via se-cretion of tumor necrosis factor-α-induced protein 6, StemCell Res Ther (2011), 2: 27.
[32] Bretz WA, Weyant RJ, Corby PM, Ren D, Weissfeld L,Kritchevsky SB, Harris T, Kurella M, Satterfield S, Visser M,Newman AB, Systemic inflammatory markers, periodontaldiseases, and periodontal infections in an elderly popula-
tion, J Am Geriatr Soc (2005), 53: 1532–1537.[33] Spranger J, Kroke A, Möhlig M, Hoffmann K, Bergmann
MM, Ristow M, Boeing H, Pfeiffer AF, Inflammatory cy-tokines and the risk to develop type 2 diabetes: Results of theprospective population-based European Prospective Investi-gation into Cancer and Nutrition (EPIC)-Potsdam Study, Di-abetes (2003), 52: 812–817.
[34] Orbak R, Tezel A, Canakçi V, Demir T, The influence ofsmoking and non-insulin-dependent diabetes mellitus on pe-riodontal disease, J Int Med Res (2002), 30: 116–125.
[35] Tracey K, Cerami A, Metabolic responses to cachectin/TNF,Annals of the New York academy of sciences (1990), 587:325–331.
[36] Lalla E, Cheng B, Lal S, Kaplan S, Softness B, GreenbergE, Goland RS, Lamster IB, Diabetes mellitus promotes peri-odontal destruction in children, J Clin Periodontol (2007), 34:294–298.
[37] Mishima N, Sahara N, Shirakawa M, Ozawa H, Effect ofstreptozotocin-induced diabetes mellitus on alveolar bone de-position in the rat, Arch Oral Biol (2002), 47: 843–849.
[38] Villarino ME, Sánchez LM, Bozal CB, Ubios AM, Influenceof short-term diabetes on osteocytic lacunae of alveolar bone.A histomorphometric study, Acta Odontol Latinoam (2006),19: 23–28.
[39] Santos Tunes R, Foss-Freitas MC, Nogueira-Filho Gda R, Im-pact of periodontitis on the diabetes-related inflammatory sta-tus, J Can Dent Assoc (2010), 76: a35.
[40] Nassar H, Kantarci A, van Dyke TE: Diabetic periodontitis, amodel for activated innate immunity and impaired resolutionof inflammation, Periodontol 2000 (2007), 43: 233–244.
[41] Akira S, Takeda K, Toll-like receptor signalling, Nat Rev Im-munol (2004), 4: 499–511.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com


![Oridonin protects LPS-induced acute lung injury by ......and acute lung injury (ALI) [1, 2]. Lipopolysaccharide (LPS), from the outer membrane of gram-negative bacteria, has been widely](https://static.fdocument.org/doc/165x107/608e9a4b0654131b49646243/oridonin-protects-lps-induced-acute-lung-injury-by-and-acute-lung-injury.jpg)