The Regulation Effect of α7nAChRs and M1AChRs on ...
10
Review Article The Regulation Effect of α7nAChRs and M1AChRs on Inflammation and Immunity in Sepsis Song Hu, 1 Yundong Wang, 2 and Hongbing Li 3 1 General Surgery Department of Ezhou Central Hospital of Hubei Province, 436000, China 2 Infectious Diseases Department of Ezhou Central Hospital of Hubei Province, 436000, China 3 Emergency Department of the First People’s Hospital of Guiyang of Guizhou Province, 550002, China Correspondence should be addressed to Hongbing Li; [email protected] Received 5 June 2021; Revised 14 September 2021; Accepted 25 October 2021; Published 3 November 2021 Academic Editor: Markus H. Gräler Copyright © 2021 Song Hu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The inflammatory storm in the early stage and immunosuppression in the late stage are responsible for the high mortality rates and multiple organ dysfunction in sepsis. In recent years, studies have found that the body’s cholinergic system can spontaneously and dynamically regulate inflammation and immunity in sepsis according to the needs of the body. Firstly, the vagus nerve senses and regulates local or systemic inflammation by means of the Cholinergic Anti-inflammatory Pathway (CAP) and activation of α7-nicotinic acetylcholine receptors (α7nAChRs); thus, α7nAChRs play important roles for the central nervous system (CNS) to modulate peripheral inflammation; secondly, the activation of muscarinic acetylcholine receptors 1 (M1AChRs) in the forebrain can affect the neurons of the Medullary Visceral Zone (MVZ), the core of CAP, to regulate systemic inflammation and immunity. Based on the critical role of these two cholinergic receptor systems in sepsis, it is necessary to collect and analyze the related findings in recent years to provide ideas for further research studies and clinical applications. By consulting the related literature, we draw some conclusions: MVZ is the primary center for the nervous system to regulate inflammation and immunity. It coordinates not only the sympathetic system and vagus system but also the autonomic nervous system and neuroendocrine system to regulate inflammation and immunity; α7nAChRs are widely expressed in immune cells, neurons, and muscle cells; the activation of α7nAChRs can suppress local and systemic inflammation; the expression of α7nAChRs represents the acute or chronic inflammatory state to a certain extent; M1AChRs are mainly expressed in the advanced centers of the brain and regulate systemic inflammation; neuroinflammation of the MVZ, hypothalamus, and forebrain induced by sepsis not only leads to their dysfunctions but also underlies the regulatory dysfunction on systemic inflammation and immunity. Correcting the neuroinflammation of these regulatory centers and adjusting the function of α7nAChRs and M1AChRs may be two key strategies for the treatment of sepsis in the future. 1. Introduction Critical sepsis still has a very high incidence and mortality [1]. Studies have shown that the inflammatory storm induced by the hyperactivity of innate immunity in the early stage of sepsis [2], the chronic inflammatory state and disorders, or the suppression of innate immunity in the late stage of sepsis [3, 4] underlies the poor survival rate and poor quality of life in septic patients; therefore, correcting the disorders of inflam- mation and immunity should be a key strategy for the treat- ment of sepsis. The autonomic nervous system senses and regulates the functional state including the inflammatory state of internal organs (Figure 1). It innervates, regulates, and activates neutro- phils, lymphocytes, and other immune cells to meet the needs of the body’s immunity [5]. Overall, the nervous system regu- lates inflammation and immunity through two main mecha- nisms [6, 7]: firstly, the neuroendocrine system regulates the release of glucocorticoids through the hypothalamic-pituitary- adrenal (HPA) axis to suppress immunity [8]; and secondly, the Cholinergic Anti-inflammatory Pathway (CAP), belonging to the vagus system, is a rapid and specific regulatory way Hindawi Mediators of Inflammation Volume 2021, Article ID 9059601, 10 pages https://doi.org/10.1155/2021/9059601
Transcript of The Regulation Effect of α7nAChRs and M1AChRs on ...

Review ArticleThe Regulation Effect of α7nAChRs and M1AChRs onInflammation and Immunity in Sepsis
Song Hu,1 Yundong Wang,2 and Hongbing Li 3
1General Surgery Department of Ezhou Central Hospital of Hubei Province, 436000, China2Infectious Diseases Department of Ezhou Central Hospital of Hubei Province, 436000, China3Emergency Department of the First People’s Hospital of Guiyang of Guizhou Province, 550002, China
Correspondence should be addressed to Hongbing Li; [email protected]
Received 5 June 2021; Revised 14 September 2021; Accepted 25 October 2021; Published 3 November 2021
Academic Editor: Markus H. Gräler
Copyright © 2021 Song Hu et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The inflammatory storm in the early stage and immunosuppression in the late stage are responsible for the high mortality ratesand multiple organ dysfunction in sepsis. In recent years, studies have found that the body’s cholinergic system can spontaneouslyand dynamically regulate inflammation and immunity in sepsis according to the needs of the body. Firstly, the vagus nerve sensesand regulates local or systemic inflammation by means of the Cholinergic Anti-inflammatory Pathway (CAP) and activation ofα7-nicotinic acetylcholine receptors (α7nAChRs); thus, α7nAChRs play important roles for the central nervous system (CNS)to modulate peripheral inflammation; secondly, the activation of muscarinic acetylcholine receptors 1 (M1AChRs) in theforebrain can affect the neurons of the Medullary Visceral Zone (MVZ), the core of CAP, to regulate systemic inflammationand immunity. Based on the critical role of these two cholinergic receptor systems in sepsis, it is necessary to collect andanalyze the related findings in recent years to provide ideas for further research studies and clinical applications. By consultingthe related literature, we draw some conclusions: MVZ is the primary center for the nervous system to regulate inflammationand immunity. It coordinates not only the sympathetic system and vagus system but also the autonomic nervous system andneuroendocrine system to regulate inflammation and immunity; α7nAChRs are widely expressed in immune cells, neurons,and muscle cells; the activation of α7nAChRs can suppress local and systemic inflammation; the expression of α7nAChRsrepresents the acute or chronic inflammatory state to a certain extent; M1AChRs are mainly expressed in the advanced centersof the brain and regulate systemic inflammation; neuroinflammation of the MVZ, hypothalamus, and forebrain induced bysepsis not only leads to their dysfunctions but also underlies the regulatory dysfunction on systemic inflammation andimmunity. Correcting the neuroinflammation of these regulatory centers and adjusting the function of α7nAChRs andM1AChRs may be two key strategies for the treatment of sepsis in the future.
1. Introduction
Critical sepsis still has a very high incidence and mortality [1].Studies have shown that the inflammatory storm induced bythe hyperactivity of innate immunity in the early stage ofsepsis [2], the chronic inflammatory state and disorders, orthe suppression of innate immunity in the late stage of sepsis[3, 4] underlies the poor survival rate and poor quality of lifein septic patients; therefore, correcting the disorders of inflam-mation and immunity should be a key strategy for the treat-ment of sepsis.
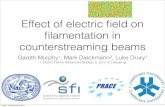
The autonomic nervous system senses and regulates thefunctional state including the inflammatory state of internalorgans (Figure 1). It innervates, regulates, and activates neutro-phils, lymphocytes, and other immune cells to meet the needsof the body’s immunity [5]. Overall, the nervous system regu-lates inflammation and immunity through two main mecha-nisms [6, 7]: firstly, the neuroendocrine system regulates therelease of glucocorticoids through the hypothalamic-pituitary-adrenal (HPA) axis to suppress immunity [8]; and secondly,the Cholinergic Anti-inflammatory Pathway (CAP), belongingto the vagus system, is a rapid and specific regulatory way
HindawiMediators of InflammationVolume 2021, Article ID 9059601, 10 pageshttps://doi.org/10.1155/2021/9059601

between the brain and the immune system. CAP includes threeparts: the afferent vagus nerve is responsible for perception andincoming inflammatory signals, the Medullary Visceral Zone(MVZ) is in charge of the integration and preliminary treat-ment of inflammatory signals, and the efferent vagus nerve reg-ulates the strength of inflammation. CAP spontaneously anddynamically regulates the inflammatory tone to ensure effec-tively preventing tissue damage and infection [9–11]. In addi-tion, the CAP and HPA axis collaborated with each other tomaintain a moderate inflammatory and immune state accord-ing to the body’s needs.
The cholinergic system effectively regulates inflammationand immunity by releasing acetylcholine to act on α7nAChRsand M1AChRs (Figure 1). Research confirmed that eitherM1AChR agonist TBPB or α7nAChR agonist GTS-21 cansignificantly reduce blood proinflammatory cytokine levelssuch as tumor necrosis factor- (TNF-) α, IL-1β, and IL-6 inexperimental septic mice and reduce mortality [12]. Then, it
is necessary to know the differences between these two recep-tors in the inflammation regulation process. At the same time,sepsis also induces neuroinflammation, which will inevitablyaffect the structure and function of regulatory centers such asMVZ, and these centers may lose their controlling abilitiesfor inflammation regulation andmay be blamed for the inflam-matory storm in the early stage of sepsis and the immune paral-ysis in the late stage. This review collects and analyzes relatedstudies on the cholinergic regulation of inflammation andimmunity to generalize the regulatory laws and provide ideasfor further research and clinical translation on sepsis.
2. Primary Regulation: α7nAChRs Mediated theInflammatory Reflex
Primary regulation involves the direct regulation of systemicand local inflammation by CAP through releasing acetylcho-line, which acts on α7nAChRs on immune cells or other
Parasympathetic and sympathetic nervoussystem regulate inflammation of internal organs
T1T2
T3T4
T5T6T7T8T9T10
T11T12
L1L2L3
Pupils
Salivary glands
Heart
Bronchi of lungs
LiverStomach
Small intestines
Adrenal glandKidney
Large intestine
Rectum
Bladder
Genitals
NE
β2-ARs
T-ChAT cells
MacrophagesACh
α7nAChR
Proinflammatorycytokines
NTSDMN
M 1 AChR
Spleen
Part A
Part B
Brain
Figure 1: Parasympathetic and sympathetic nervous systems regulate inflammation of internal organs. Sympathetic and parasympatheticsystems innervate almost all internal organs. Current studies have confirmed that the vagus nerve can sense inflammatory signals andtransmit them to the Nucleus Tractus Solitarius (NTS) of the Medullary Visceral Zone (MVZ). In MVZ, NTS links to the RostralVentrolateral Medulla (RVLM) and Vagus Dorsal Motor Nucleus (VDMN) to process the incoming information. On the other hand,MVZ connects the hypothalamus, basal forebrain (BF), and forebrain upwards and connects the locus coeruleus downwards so that thesympathetic and vagus systems, the autonomic nervous system, and the neuroendocrine regulation system can cooperate to regulateinflammation and immunity. (a) The regulation of Cholinergic Anti-inflammatory Pathways (CAP) on systemic inflammation. After theefferent vagus fibers from the Vagus Dorsal Motor Nucleus (VDMN) shift neurons in the upper abdominal cavity mesenteric ganglioncomplex, their postganglionic fibers enter the spleen and release norepinephrine which acts on the T lymphocytes to facilitatesynthesizing ACh, and the latter activate α7nAChRs on the monocytes to inhibit releasing proinflammatory cytokines. (b) The centralregulation pathway of the cholinergic system. After the inflammatory information from NTS is modified by BF, the postganglionic fibersof BF release ACh which bind to the M1AChRs on the cholinergic neuron of the forebrain to regulate the systemic inflammation andimmunity through MVZ.
2 Mediators of Inflammation

related cells. Therefore, α7nAChRs play key roles in the con-trol of central and peripheral inflammation and are consid-ered key components of the innate immune system [13, 14].
2.1. CAP Negatively Regulates Systemic or Local Inflammationand Immunity by means of Activating α7nAChRs. There arebidirectional communications between the central nervoussystem (CNS) and the immune system. Implantable electricvagus nerve stimulation can effectively reduce the bloodinflammatory mediators in sepsis [15], which reveals that thevagus is involved in the regulation of inflammation. Furtherstudies have confirmed that CAP participates in inflammationregulation [7, 16]. MVZ, which exists in the midcaudalsegment of the medulla oblongata of humans, rats, monkeys,and other animals, is an important regulatory center for stressand an integrating center between the autonomic nervoussystem and the immune system [17]. MVZ and the vagusnerve constitute a complete circuit for inflammation percep-tion and regulation, which is the so-called CAP. CAP isresponsible for monitoring and suppressing systemic or localinflammation and immunity to acquire a balance betweenremoving pathogens and restoring immune homeostasis.The following paths are involved in the regulatory process.The sensory vagus nerve endings sense the inflammatory sig-nals through the aortic body or other chemoreceptors, and theinflammatory signals were transmitted intoMVZ or advancedcenters such as the forebrain [16]. After the inflammatory sig-nals were integrated and processed among several centers suchas the MVZ, hypothalamus, basal forebrain (BF), and fore-brain, the final instructions were emanated from the VagusDorsal Motor Nucleus (VDMN) and terminated in the upperabdominal cavity mesenteric ganglion complex, from whichthe adrenergic postganglionic fibers were elongated to thespleen and activate the choline acetyltransferase of T lympho-cytes by releasing norepinephrine, which catalyzes the biosyn-thesis of acetylcholine [13, 18]. Acetylcholine is released andacts on α7nAChRs on innate immune cells (such as mono-cytes) to prevent the activation of monocytes (Figure 1(a));at the same time, activation of α7nAChRs inhibits releasingproinflammatory cytokines from the innate immune cellsthrough the negative regulation of TLR4 signals [19, 20];thereby, the immunity and inflammation were suppressed insepsis [21, 22]. In addition to immune regulation throughthe spleen, the vagus nerve also directly releases ACh and actson α7nAChRs on the intestinal macrophages [23], Kupffercells in the liver [24], and lung macrophages [25] to curb localinflammation. These studies suggest that the spleen-mediatedregulatory path of CAP mainly regulates acute and chronicsystemic inflammation such as sepsis, rheumatoid arthritis,and acute pancreatitis, while the vagus system also directlyregulates the local inflammation without spleen participation.
2.2. The Crosstalk Inside and Outside of MVZ. MVZ ismainly composed of the Nucleus Tractus Solitarius (NTS),Rostral Ventrolateral Medulla (RVLM), Vagus Dorsal MotorNucleus (VDMN), and other functional nuclei. They areclosely related in function and form the primary regulationcenter of inflammation and immunity. Most of the afferentvagus nerve terminates in NTS and conducts peripheral
information to NTS, which was processed by MVZ or trans-mitted to the advanced center such as BF. NTS, one of thecritical centers of the visceral reflex, inhibits the sympatheticactivity of RVLM; therefore, the damage of NTS will lead tostrong sympathetic output and intensify the inflammation[26]. RVLM is rich in catecholamine neurons, which areroughly divided into three groups. The catecholamine neu-rons which project to the hypothalamus regulate the releaseof vasopressin and ACTH, so they can regulate inflamma-tion through the hypothalamic-pituitary-adrenal (HPA)axis; the bulbospinal catecholamine neurons are presympa-thetic, which regulates most of the visceral functions; thethird group of catecholamine neurons regulates parasympa-thetic efferents to regulate inflammation and immunity [27].It can be seen that RVLM bridges between the sympatheticand parasympathetic systems, the autonomic nervous andneuroendocrine systems, and the afferent and efferent sys-tems of the vagus to coordinate the regulation of systemicinflammation. VDMN is the ultimate executor of CAP. Byoptogenetics and functional mapping, it reveals that cholin-ergic neurons in VDMN project to the superior mesentericganglion of the abdominal cavity. The activation of cholinergicneurons in VDMN significantly increases the activity of thesplenic nerve and inhibits the production of TNF-α, whichwere canceled by the pharmacology blocking or surgical tran-section of the vagus nerve, indicating that VDMN negativelyregulates innate immunity [28]. These studies confirmed thatMVZ is the primary center for regulating systemic inflamma-tion and immunity, especially innate immunity.
MVZ is a transferring station in the communicationbetween the immune system and the brain [29]. NTS andRVLM connect with locus coeruleus (LC), which controlsspinal cord-derived catecholaminergic output to participatein immunomodulatory and anti-inflammatory activity;NTS also links to the paraventricular nucleus (PVN) of thehypothalamus; thereby, it regulates inflammation andimmunity by affecting the release of glucocorticoids throughthe HPA axis [30, 31]. Catecholaminergic neurons in MVZalso transmit inflammatory information to the central amyg-dala nucleus, which regulates the emotional response [32].In addition, MVZ neurons also project to the BF, and the lat-ter further project to the forebrain and influence the M1cholinergic neurons in the forebrain; at last, these choliner-gic neurons have a significant impact on VDMN [33].Thereby, the MVZ, BF, and forebrain form a regulatory loopand affect systemic inflammation and immunity throughα7nAChRs and M1AChRs.
It can be seen that MVZ is the central hub and primarycenter of the inflammatory reflex. It bridges between thevagus and sympathetic nerves and the autonomic nervousand neuroendocrine systems. It coordinates multiple centersto jointly regulate systemic inflammation and immunity.
2.3. The Intracellular Signaling Pathways That Activatedα7nAChRs Inhibit Inflammation. Activating α7nAChRs onmacrophages andmacrophage cell lines can inhibit them fromsecreting proinflammatory factors such as IL-1β, TNF-α, IL-6,and HMGB1 in a concentration-dependent manner but doesnot affect the secretion of anti-inflammatory cytokines such
3Mediators of Inflammation

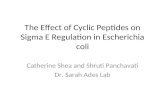
as IL-10 [34, 35]. The mechanism involves the regulation ofmultiple signaling pathways. Firstly, activated α7nAChRsupregulate the expression of IRAK-M [36], a negative regulatorof proinflammatory cytokines, which can inhibit the phosphor-ylation of upstream signaling molecules of IκB, thereby inhibit-ing the activity of NF-κB [37]; secondly, through promotingrecruitment of tyrosine kinase JAK2 and phosphorylation ofSTAT3, activated α7nAChRs promote pSTAT3 translocationto the nucleus and binding to DNA instead of NF-κB, therebyinhibiting the production of TNF-α and other cytokines [38,39]; thirdly, sirtuin (SIRT) plays an important role in curbinginflammation, and central activated α7nAChRs can increasethe expression of SIRT1 and deacetylate RelA/p65, therebypromoting RelA/p65 proteasome degradation and reducingcytokine expression [40, 41]; furthermore, activated α7nAChRscan upregulate miRNA-124, reduce the expression of IL-6mRNA, and inhibit the conversion of proTNF-α to TNF-αto reduce the production of inflammatory factors [42].α7nAChRs are involved in facilitating naive CD4+ T cells todifferentiate to CD4+ CD25+ FoxP3+ regulatory T cells(Tregs) [43], and the latter are immunosuppressive T cellsand negatively regulate systemic inflammation. From thesestudies, it can be seen that the activation of α7nAChRs cancut off the production of proinflammatory factors throughmultiple intracellular signaling pathways (Figure 2).
Other studies suggest that α7nAChRs have the characteris-tics of ligand-gated ion channels [44]. In macrophages, PNU-120596, the α7nAChRs’ allosteric modulator, can increase theopening duration and frequency of the calcium channels, whileantagonists reduce these effects of calcium channels induced bycholine [45]. As we all know, the content of intracellular
calcium will affect a wide range of inflammatory signal pathsin the cell; the specific mechanisms that activated α7nAChRsregulate inflammation through calcium channels need to befurther studied.
2.4. The Peripheral Effect of α7nAChRs Outside CNS. In sep-sis, macrophages and monocytes are first recruited to the siteof infection and initiate innate immunity [46]; however, theexcessive activation of these cells will cause the inflamma-tory storm in sepsis [47]. α7nAChRs are expressed on themembrane of macrophages, monocytes, and dendritic cells.Activation of α7nAChRs can promote the transformationof macrophages from proinflammatory type M1 to anti-inflammatory type M2 [48], which will limit the intensityand extension of inflammation [49]. In addition, to expressα7nAChRs, neutrophils and T and B lymphocytes also expressother nicotinic and muscarinic receptors, which suggests thatthe vagus regulates immunity through multiple paths in thesecells [50]. It can be seen that the excitement of the vagus willinfluence both innate immunity and acquired immunity,which contribute to the inhibition of systemic inflammationin sepsis.
Besides immune cells, α7nAChRs were also expressed onthe membranes of peripheral nerve fibers, skeletal muscle,and myocardial cells, which play an important role in control-ling the intensity of local inflammation. Sepsis induces asignificant upregulation of γ- or α7nAChRs in the sciatic nerveand causes demyelination and neuromuscular dysfunction[51]; however, the glial cell line-derived neurotrophic factor(GDNF) significantly reduces nerve demyelination, improvesneuromuscular dysfunction and patients’ prognosis, and
Cytokines
Cytokine receptors
JAK1 JAK2
STATP
P P
STATP
TOLL-like
receptors
MyD88 IRAK
P50P65
NF-κBI-κB
P50P65
NF-κB
DAMPS, PAMPS
α7nAChR
ACh
Pro-inflammationCytokines
MicroRNA-124
proTNF-α TNF-α
SIRT1
NF-κB
P50
P65
Figure 2: Some known paths of activated α7nAChRs to suppress inflammation. Activated α7nAChRs inhibit the generation ofproinflammatory cytokines through several intracellular paths. These mechanisms involve negatively regulating the NF-κB path andfacilitating the synthesis of P-STAT, SIRT1, and microRNA-124. DAMPs: damage-associated molecular patterns; PAMPs: pathogen-associated molecular patterns; JAK2: tyrosine kinase 2; STAT: signal transducer and activator of transcription; IRAK: interleukin-1receptor-associated kinase. Blue arrow, the normal signal path; red arrow, promoting; red line, blocking.
4 Mediators of Inflammation

reduces the expression of γ- or α7nAChRs [52]. It suggeststhat inflammation will facilitate the expression of α7nAChRson the nerve fibers and anti-inflammation will subside theirexpression. However, other studies suggested that the upregu-lation of γ or α7nAChRs on the muscle cell membraneinduced by sepsis is the molecular basis of muscle weakness[53]. In the spleen, mesenchymal stem cells downregulatethe expression of α7nAChRs and reduce the ratio of phos-phorylated STAT3 to total STAT3, thereby reducing the inten-sity of systemic inflammation and preventing organ damagecaused by sepsis, as well as in the heart [54]. These studiessuggest that sepsis facilitates the expression of α7nAChRs inperipheral tissue cells, which is related to local or systemicinflammation regulation. In fact, local pathological processessuch as cell degeneration and apoptosis should result fromsystemic or local inflammation rather than upregulatedα7nAChRs. Upregulated α7nAChRsmay be amarker for localinflammation and pathologies of degeneration and apoptosis.
2.5. The Central Effect of α7nAChRs. α7nAChRs are encoded bythe gene fragment of CHRFAM7A. They were first found onneurons and were most richly expressed in CNS and involvedin the regulation of neuroinflammation. Intracerebral injectionof the α7nAChR agonist PHA-543613 reduces neuroinflamma-tion by activating the JAK2-STAT3 pathway, thereby lesseningthe short-term and long-term sequelae after intracranial hemor-rhage (ICH), while the α7nAChR antagonist MLA has theopposite effect [55]; Transcutaneous vagus nerve stimulation(VNS) also has the effect of lessening brain damage after strokewhich may be related to the upregulation of α7nAChRs on themembrane of immune cells and neurons [56]. Activatedα7nAChRs on microglia and macrophages, which infiltratethe brain through the damaged blood-brain barrier, can reducenot only the local inflammatory cytokines such as TNF-α andIL-1β but also the death of the neurons in the hippocampalCA1 zone [57]. PHA568478, the selective α7nAChR agonist,can reduce the number of microglia/macrophages of the proin-flammatory M1 phenotype and increase the number of micro-glia/macrophages of the anti-inflammatoryM2 phenotype [58].It shows that α7nAChR activation of central immune cells orneurons, either by the direct agonist or by the indirect periph-eral VNS, can produce central anti-inflammatory effects [59].In addition to regulating acute or chronic neuroinflammation,activation of α7nAChRs is involved in improving cognitivefunction, mental health, and neurodegenerative diseases, evenenergy homeostasis and insulin sensitivity [60], and interferingwith α7nAChRs has broad prospects for clinical application.
Our preliminary experiments confirmed that activationof α7nAChRs significantly improved MVZ neuroinflamma-tion and apoptosis [61, 62]: in sepsis, intraperitoneallyadministered GTS-21, a specific agonist for α7nAChRs,significantly reduced the apoptosis of the cholinergic andcatecholaminergic neurons in MVZ in septic rats, accompa-nied by the elevated expression of tyrosine hydroxylase (TH)and choline acetyltransferase (CHAT), which significantlyreversed the inhibition of CAP and the inflammatory storm,while intraperitoneally administered MLA, a specific antago-nist for α7nAChRs, does the opposite. Therefore, activationof α7nAChRs not only directly inhibits the overactive sys-
temic inflammation and immunity but also resumes theinflammatory and dysfunctional MVZ, thereby restoringCAP’s regulation of inflammation. Our studies show thatthrough the central and peripheral mechanisms, activationof α7nAChRs coordinately promotes the abnormal inflam-matory state of sepsis to return to normal.
In addition, research suggests that the centrally adminis-tered α7nAChR agonist can significantly reduce the multipleorgan damage caused by sepsis, reverse the immunosuppres-sive state, improve the outcome of septic rats [63], reduceintestinal inflammation and the incidence of postoperativeintestinal obstruction [64, 65], inhibit the proinflammatoryphenotype of microglia activated by traumatic brain injury(TBI), and attenuate the systemic inflammatory response[66], while centrally administered methyllycaconitine, aselective antagonist of α7nAChRs, can exacerbate systemicinflammation and multiple organ dysfunction.
These studies have verified that CAP activation by periph-eral or central paths can improve the pathology of inflamma-tion regulation centers such as MVZ and restore their normalregulation activity in sepsis, which means central anti-inflammation may be an important strategy to reverse theinflammatory storm in the early stage of sepsis.
3. Advanced Regulatory Mechanism:Modification and Regulation ofInflammatory Information byActivating M1AChRs
3.1. Basal Forebrain “Modifies” the Afferent Signal of MVZand Regulates the MVZ Function through the Forebrain.The basal forebrain (BF) acts as a “goalkeeper” or a “filter”in the process of a variety of incoming sensory information[67]. In BF, cholinergic neurons account for only 5% of thetotal neurons, while GABAergic neurons account for 35%,and glutamatergic neurons account for 55% [68]. Such aneuronal composition allows BF to regulate the afferentintensity of various sensory information easily [69]; namely,the BF cholinergic neurons will amplify or weaken part ofincoming sensory information and plastically process themaccording to the body’s needs or the “importance” of thesesignals [70]. A study shows that inflammatory informationtransmitted to NTS via the vagus nerve succeeds to BF. Afterbeing modified by BF, the inflammatory information werecarried by the cholinergic efferent fibers of BF and projectedto the M1AChRs richly expressed in the forebrain [71]. Theactivation of M1AChRs in the forebrain will inhibit systemicinflammation and immunity [4, 72]. These studies suggestthat BF, as the advanced processing center of inflammatoryinformation, actively participates in the inflammatory reflexof MVZ through the forebrain M1AChR system.
3.2. Activation of M1AChRs in the Forebrain System RegulatesInflammation and Immunity of Sepsis through CAP.M1AChRsare G protein-coupled receptors with high selectivity [32]. Astudy [73] confirmed that intraperitoneal injection of cholines-terase inhibitors such as galantamine or Huperzine A, whichcan pass through the blood-brain barrier, significantly reducedplasma proinflammatory cytokines and mortality in septic rats,
5Mediators of Inflammation

whereas intraperitoneal injection of cholinesterase inhibitorswhich cannot pass through the blood-brain barrier has no sucheffect. This study shows that central acetylcholine has the effectof inhibiting systemic inflammation. A study also shows thatintraperitoneal administration of benzyl quinolone carboxylicacid (BQCA, positive allosteric regulator of M1AChRs, whichcan increase the affinity of ACh and M1AChRs by 129 timesin CNS [74]) can reduce the serum TNF-α levels, and it indi-cates that through activation of the central M1AChRs, centralacetylcholine has a negative regulation on inflammation insepsis, which may be related to the inflammation-controllingloop of BF-forebrain-MVZ.
In addition, direct activation of central M1AChRs also hasa significant anti-inflammatory effect. For example, adminis-tration of M1AChRs’ specific agonist CNI-1493 in the braininhibits serum TNF-α in murine endotoxemia [75]. M1AChRsare richly expressed in the forebrain. Should the forebrainM1AChRs be responsible for this anti-inflammatory function?The next research gave us the answer. In the forebrain, selectivegenetic ablation of the vesicular acetylcholine transporter(VAChT, which is necessary for the release of acetylcholine)(VAChT-/- mice) eliminates the synaptic release of acetylcho-line (ACh) and leads to increased serum TNF-α levels [76].From these studies, we can affirm that activating the forebrainM1AChRs is a key step to control systemic inflammation.Should the anti-inflammatory effect of the forebrainM1AChRsbe linked to CAP? The following studies revealed the answer.Intracerebroventricular injection of McN-A-343, the M1AChRagonist, reduced the severity of ulcerative colitis, but the effectwas eliminated by splenectomy [77]; other studies also con-firmed that the anti-inflammatory effect by the activation ofM1AChRs can be abolished by CAP disconnection [78, 79].These studies suggest that activating forebrain M1AChRs caninhibit systemic inflammation by means of CAP. A study alsoconfirmed that the forebrain has bidirectional fiber connec-tions with NTS [80]. Therefore, it can be certain that the regu-latory function of M1AChRs in the forebrain on inflammationand immunity is through MVZ and CAP [81] (Figure 1(b)).
4. Neuroinflammation Induced by SepsisCauses Extensive Damage to the CAP’sRegulation on Inflammation and Immunity
LPS can activate microglia and astrocytes to promote theexpression of various proinflammatory cytokines and lead toCNS inflammation. Proinflammatory cytokines affect thefunction of neurons and boost neuronal apoptosis, which willcause neuroregulation disorders [82, 83]. In sepsis, neither BFnor MVZ cannot escape from the attack of sepsis-inducedneuroinflammation [84, 85]. In MVZ, neuroinflammationhas a comprehensive influence on nerves architecture, synap-tic plasticity, and nerve function. Studies show that cholinergicand catecholaminergic neurons in MVZ went through signif-icant apoptosis and inactiveness, which contributes to theinhibition of CAP and the acceleration of the inflammatorystorm in early sepsis [61, 62]. Neuroinflammation facilitatesreactive glial cells in the brain, releasing cytokines anddamage-associated molecular patterns (DAMPs), which pro-
mote cell adhesion, migration, proliferation, and angiogenesis[86]. In sepsis, activation of the HMGB1-RAGE axis upregu-lates TH expression in dopaminergic neurons [87, 88] andaggravates oxidative stress, Ca2+ homeostasis disruption,endoplasmic reticulum stress, autophagic dysfunction, excito-toxicity, and free-radical generation, all of which could lead toapoptosis [89, 90]. Both inflammation and oxidative stress inthe hypothalamus can lead to excessive activation of paraven-tricular nucleus (PVN) neurons which project to RVLM,thereby triggering sympathetic excitation and blood pressureelevation [91, 92]. Furthermore, the attack by LPS in the hypo-thalamus can lead to neuroinflammatory and metabolic disor-ders, which lead to the downregulation of α7nAChRs and thedecreased activation of STAT3 and worsen neuroinflamma-tion [93, 94].
In addition, inflammation upsets the balance of neuro-transmitters between monoamine and glutamate, whichleads to decreased functional connectivity among multiplebrain regions around the ventromedial prefrontal cortex(vmPFC) [95]. Inflammation also leads to synaptic dysfunc-tion. IL-10, one of the main anti-inflammatory cytokines,can recover multiple neurofunction in sepsis [96]. The stresscaused by sepsis increases sympathetic tension and decreasesparasympathetic tension, thereby further aggravating neuro-inflammation and affecting the functions of the prefrontalcortex, hippocampus, amygdala, and septal areas [97]. Itcan be seen that the neuroinflammation of MVZ, forebrain,and hypothalamus in sepsis will inevitably affect theirinflammation regulation function, which may be a moreimportant mechanism of systemic inflammation andimmune disorders induced by sepsis.
5. Regulation of the Sympathetic System onInflammation and Immunity
As mentioned above, MVZ communicates upward with thehypothalamus, the sympathetic nerve center, and communi-cates downward with the locus coeruleus (LC) to furtheraffect the sympathetic neurons of the spinal cord, both ofwhich are involved in the regulation of systemic inflamma-tion. Besides participating in CAP to regulate inflammation[18, 98], the sympathetic system can also independently reg-ulate innate immunity and adaptive immunity [99]. Sympa-thetic nerves act on invariant NKT cells in the liver and turnthem from the proinflammatory Th1 type into the anti-inflammatory Th2 type to promote immunosuppression byreleasing IL-10, which can easily lead to bacterial infections[100, 101]. Sympathetic nerves affect the innate and adap-tive immunity by stimulating adrenergic receptors; the acti-vation of β2-adrenergic receptors has immunosuppressiveeffects on monocytes and macrophages [102, 103]. However,NE and β2 agonists activate β2-adrenergic receptors onlymphocyte B cells to increase antibody production toenhance adaptive immunity [104]. Existing research studiesare more inclined to support that the sympathetic systemparticipates in stress and promotes inflammation, whereasvagus nerves inhibit inflammation and prevent tissuedamage.
6 Mediators of Inflammation

6. Conclusion
The autonomic nervous system, especially the vagus system,plays a key role in regulating inflammation and immunity insepsis through α7nAChRs and M1AChRs. α7nAChRs areexpressed on central and peripheral cells to regulate local orsystemic inflammation; M1AChRs are expressed mainly inthe advanced center and regulate systemic inflammation andimmunity through MVZ. MVZ is the CAP’s center, whichcommunicates between the sympathetic and vagus systems,the autonomic nervous system, and the neuroendocrine sys-tem to regulate inflammation and immunity; the neuroinflam-mation of the regulation center may be a more noteworthymechanism why inflammation and immune disorders aredifficult to correct in sepsis.
Conflicts of Interest
The authors declare that there is no conflict of interestregarding the publication of this paper.
Authors’ Contributions
Song Hu and Yundong Wang equally contributed to thisreview, and they collected the documents and finished themanuscript writing. Hongbing Li checked the data and cor-rected the review.
Acknowledgments
This study was supported by two funders: (1) the GuizhouProvincial Science and Technology Foundation (No.[2019]1005) and (2) the Science and Technology Fund ofGuizhou Provincial Health Commission (No. gzwkj2021-001).
References
[1] K. E. Rudd, S. C. Johnson, K. M. Agesa et al., “Global,regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study,” TheLancet, vol. 395, no. 10219, pp. 200–211, 2020.
[2] L. F. Gentile, A. G. Cuenca, P. A. Efron et al., “Persistentinflammation and immunosuppression: a common syn-drome and new horizon for surgical intensive care,” Journalof Trauma and Acute Care Surgery, vol. 72, no. 6, pp. 1491–1501, 2012.
[3] H. C. Prescott, J. J. Osterholzer, K. M. Langa, D. C. Angus,and T. J. Iwashyna, “Late mortality after sepsis: propensitymatched cohort study,” BMJ, vol. 353, p. i2375, 2016.
[4] V. A. Pavlov and K. J. Tracey, “The vagus nerve and theinflammatory reflex–linking immunity and metabolism,”Nature Reviews Endocrinology, vol. 8, no. 12, pp. 743–754,2012.
[5] V. A. Pavlov and K. J. Tracey, “Neural regulation of immu-nity: molecular mechanisms and clinical translation,” NatureNeuroscience, vol. 20, no. 2, pp. 156–166, 2017.
[6] N. Quan and W. A. Banks, “Brain-immune communicationpathways,” Brain, Behavior, and Immunity, vol. 21, no. 6,pp. 727–735, 2007.
[7] K. J. Tracey, “The inflammatory reflex,” Nature, vol. 420,no. 6917, pp. 853–859, 2002.
[8] W.Wang, H. Xu, H. Lin, M. Molnar, and H. Ren, “The role ofthe cholinergic anti-inflammatory pathway in septic cardio-myopathy,” International Immunopharmacology, vol. 90,p. 107160, 2021.
[9] J. M. Huston, “The vagus nerve and the inflammatory reflex:wandering on a new treatment paradigm for systemic inflam-mation and sepsis,” Surgical infections, vol. 13, no. 4, pp. 187–193, 2012.
[10] S. S. Chavan, P. Ma, and I. M. Chiu, “Neuro-immune interac-tions in inflammation and host defense: implications fortransplantation,” American Journal of Transplantation,vol. 18, no. 3, pp. 556–563, 2018.
[11] V. A. Pavlov, S. S. Chavan, and K. J. Tracey, “Molecular andfunctional neuroscience in immunity,” Annual Review ofImmunology, vol. 36, no. 1, pp. 783–812, 2018.
[12] P. F. Zabrodskii, M. S. Gromov, and V. V. Maslyakov, “Com-bined effects of M1 muscarinic acetylcholine receptor agonistTBPB and α7n-acetylcholine receptor activator GTS-21 onmouse mortality and blood concentration of proinflamma-tory cytokines in sepsis,” Bulletin of Experimental Biologyand Medicine, vol. 162, no. 6, pp. 750–753, 2017.
[13] L. V. Borovikova, S. Ivanova, M. Zhang et al., “Vagus nervestimulation attenuates the systemic inflammatory responseto endotoxin,” Nature, vol. 405, no. 6785, pp. 458–462, 2000.
[14] M. Gallowitsch-Puerta and K. J. Tracey, “Immunologic roleof the cholinergic anti-inflammatory pathway and the nico-tinic Acetylcholine 7 receptor,” Annals of the New York Acad-emy of Sciences, vol. 1062, no. 1, pp. 209–219, 2005.
[15] M. Gu, X. L. Mei, and Y. N. Zhao, “Sepsis and cerebral dys-function: BBB damage, neuroinflammation, oxidative stress,apoptosis and autophagy as key mediators and the potentialtherapeutic approaches,” Neurotoxicity Research, vol. 39,no. 2, pp. 489–503, 2021.
[16] S. S. Chavan, V. A. Pavlov, and K. J. Tracey, “Mechanismsand therapeutic relevance of neuro-immune communica-tion,” Immunity, vol. 46, no. 6, pp. 927–942, 2017.
[17] K. J. Tracey, “Reflexes in immunity,” Cell, vol. 164, no. 3,pp. 343-344, 2016.
[18] M. Rosas-Ballina, P. S. Olofsson, M. Ochani et al., “Acetyl-choline-synthesizing T cells relay neural signals in a vagusnerve circuit,” Science, vol. 334, no. 6052, pp. 98–101, 2011.
[19] C. Zhao, X. Yang, E. M. Su et al., “Signals of vagal circuitsengaging with AKT1 in α7 nAChR+CD11b+ cells lessen E.coli and LPS-induced acute inflammatory injury,” Cell Dis-covery, vol. 3, no. 1, p. 17009, 2017.
[20] H. Yang, H. Liu, Q. Zeng et al., “Inhibition ofHMGB1/RAGE-mediated endocytosis by HMGB1 antago-nist box A, anti-HMGB1 antibodies, and cholinergic agonistssuppresses inflammation,”Molecular Medicine, vol. 25, no. 1,p. 13, 2019.
[21] F. M. Santos-Almeida, G. Domingos-Souza, C. A. Meschiariet al., “Carotid sinus nerve electrical stimulation in _conscious_rats attenuates systemic inflammation via chemoreceptor acti-vation,” Scientific Reports, vol. 7, no. 1, pp. 62–65, 2017.
[22] G. S. Bassi, D. P. M. Dias, M. Franchin et al., “Modulation ofexperimental arthritis by vagal sensory and central brainstimulation,” Brain, Behavior, and Immunity, vol. 64,pp. 330–343, 2017.
7Mediators of Inflammation

[23] G. Matteoli, P. J. Gomez-Pinilla, A. Nemethova et al., “A dis-tinct vagal anti-inflammatory pathway modulates intestinalmuscularis resident macrophages independent of the spleen,”Gut, vol. 63, no. 6, pp. 938–948, 2014.
[24] K. Hajiasgharzadeh and B. Baradaran, “Cholinergic anti-inflammatory pathway and the liver,” Advanced Pharmaceu-tical Bulletin, vol. 7, no. 4, pp. 507–513, 2017.
[25] Z. Shao, Q. Li, S. Wang, and Z. Chen, “Protective effects ofPNU-282987 on sepsis-induced acute lung injury in mice,”Molecular Medicine Reports, vol. 19, no. 5, pp. 3791–3798,2019.
[26] U. R. Anoop and K. Verma, “Pulmonary edema inCOVID19-a neural hypothesis,” ACS Chemical Neuroscience,vol. 11, no. 14, pp. 2048–2050, 2020.
[27] P. G. Guyenet, R. L. Stornetta, B. B. Holloway, G. M. P. R.Souza, and S. B. G. Abbott, “Rostral ventrolateral medullaand hypertension,” Hypertension, vol. 72, no. 3, pp. 559–566, 2018.
[28] A. M. Kressel, T. Tsaava, A. Yaakov, E. H. Chang, and K. J.Tracey, “Identification of a brainstem locus that inhibitstumor necrosis factor,” Proceedings of the National Academyof Sciences, vol. 117, no. 47, pp. 29803–29810, 2020.
[29] X. Ge, Z. Yang, L. Duan, and Z. Rao, “Retracted: Evidence forinvolvement of the neural pathway containing the peripheralvagus nerve, medullary visceral zone and central amygdaloidnucleus in neuroimmunomodulation,” Brain Research,vol. 914, no. 1-2, pp. 149–158, 2001.
[30] V. A. Pavlov, H. Wang, C. J. Czura, S. G. Friedman, and K. J.Tracey, “The cholinergic anti-inflammatory pathway: a miss-ing link in neuroimmunomodulation,” Molecular Medicine,vol. 9, no. 5-8, pp. 125–134, 2003.
[31] H. R. Berthoud and W. L. Neuhuber, “Functional and chem-ical anatomy of the afferent vagal system,” Autonomic Neuro-science, vol. 85, no. 1-3, pp. 1–17, 2000.
[32] S. Maeda, J. Xu, F. M. Kadji et al., “Structure and selectivityengineering of the M1 muscarinic receptor toxin complex,”Science, vol. 369, no. 6500, pp. 161–167, 2020.
[33] Q. Zhai, D. Lai, P. Cui et al., “Selective activation of basal fore-brain cholinergic neurons attenuates polymicrobial sepsis-induced inflammation via the cholinergic anti-inflammatorypathway,” Critical care medicine, vol. 45, no. 10, pp. e1075–e1082, 2017.
[34] M. Kox, J. F. van Velzen, J. C. Pompe, C. W. Hoedemaeker,J. G. van der Hoeven, and P. Pickkers, “GTS-21 inhibitspro-inflammatory cytokine release independent of the Toll-like receptor stimulated via a transcriptional mechanisminvolving JAK2 activation,” Biochemical Pharmacology,vol. 78, no. 7, pp. 863–872, 2009.
[35] M. Kox, J. C. Pompe, M. C. Gordinou de Gouberville, J. G.van der Hoeven, C. W. Hoedemaekers, and P. Pickkers,“Effects of the α7 nicotinic acetylcholine receptor agonistGTS-21 on the innate immune response in humans,” Shock,vol. 36, no. 1, pp. 5–11, 2011.
[36] C. M. Maldifassi, G. Atienza, F. Arnalich et al., “A new IRAK-M-mediated mechanism implicated in the anti-inflammatoryeffect of nicotine via α7 nicotinic receptors in human macro-phages,” PLoS One, vol. 9, no. 9, article e108397, 2014.
[37] H. Yoshikawa, M. Kurokawa, N. Ozaki et al., “Nicotineinhibits the production of proinflammatory mediators inhuman monocytes by suppression of I-κB phosphorylationand nuclear factor-κB transcriptional activity through nico-
tinic acetylcholine receptor α7,” Clinical and ExperimentalImmunology, vol. 146, no. 1, pp. 116–123, 2006.
[38] W. J. de Jonge, E. P. van der Zanden, F. O. The et al., “Stim-ulation of the vagus nerve attenuates macrophage activationby activating the Jak2-STAT3 signaling pathway,” NatureImmunology, vol. 6, no. 8, pp. 844–851, 2005.
[39] U. Andersson and K. J. Tracey, “Reflex principles of immuno-logical homeostasis,” Annual Review of Immunology, vol. 30,pp. 313–335, 2012.
[40] F. Jiao and Z. Gong, “The beneficial roles of SIRT1 inneuroinflammation-related diseases,” Oxidative Medicineand Cellular Longevity, vol. 2020, Article ID 6782872, 19pages, 2020.
[41] T. F. Liu, B. K. Yoza, M. El Gazzar, V. T. Vachharajani, andC. E. McCall, “NAD+-dependent SIRT1 Deacetylase Partici-pates in Epigenetic Reprogramming during Endotoxin Toler-ance,” Journal of Biological Chemistry, vol. 286, no. 11,pp. 9856–9864, 2011.
[42] Y. Sun, Q. Li, H. Gui et al., “MicroRNA-124 mediates thecholinergic anti-inflammatory action through inhibiting theproduction of pro-inflammatory cytokines,” Cell Research,vol. 23, no. 11, pp. 1270–1283, 2013.
[43] T. Fujii, M. Mashimo, Y. Moriwaki et al., “Expression andfunction of the cholinergic system in immune cells,” Frontiersin Immunology, vol. 8, 2017.
[44] E. X. Albuquerque, E. F. Pereira, M. Alkondon, and S. W.Rogers, “Mammalian nicotinic acetylcholine receptors: fromstructure to function,” Physiological Reviews, vol. 89, no. 1,pp. 73–120, 2009.
[45] A. C. Báez-Pagán, M. Delgado-Vélez, and J. A. Lasalde-Dominicci, “Activation of the macrophage α7 nicotinic ace-tylcholine receptor and control of inflammation,” Journal ofNeuroimmune Pharmacology, vol. 10, no. 3, pp. 468–476,2015.
[46] N. K. Iskander, M. F. Osuchowski, D. J. Stearns-Kurosawaet al., “Sepsis: multiple abnormalities, heterogeneousresponses, and evolving understanding,” PhysiologicalReviews, vol. 93, no. 3, pp. 1247–1288, 2013.
[47] O. Soehnlein, L. Lindbom, and C. Weber, “Mechanismsunderlying neutrophil-mediated monocyte recruitment,”Blood, vol. 114, no. 21, pp. 4613–4623, 2009.
[48] L. Wang, D. Opland, S. Tsai et al., “_Pten_ deletion in RIP-Cre neurons protects against type 2 diabetes by activatingthe anti-inflammatory reflex,” Nature Medicine, vol. 20,no. 5, pp. 484–492, 2014.
[49] H. Wang, M. Yu, M. Ochani et al., “Nicotinic acetylcholinereceptor α7 subunit is an essential regulator of inflamma-tion,” Nature, vol. 421, no. 6921, pp. 384–388, 2003.
[50] D. B. Hoover, “Cholinergic modulation of the immune sys-tem presents new approaches for treating inflammation,”Pharmacology & Therapeutics, vol. 179, pp. 1–16, 2017.
[51] L. Liu, S. Min, W. Li et al., “Pharmacodynamic changes withvecuronium in sepsis are associated with expression of α7-and γ-nicotinic acetylcholine receptor in an experimentalrat model of neuromyopathy,” British Journal of Anaesthesia,vol. 112, no. 1, pp. 159–168, 2014.
[52] X. Wang, S. Min, F. Xie, J. Yang, L. Li, and J. Chen, “Glial cell-derived neurotrophic factor alleviates sepsis-induced neuro-muscular dysfunction by decreasing the expression of γ\-and α7-nicotinic acetylcholine receptors in an experimental
8 Mediators of Inflammation

rat model of neuromyopathy,” Biochemical and BiophysicalResearch Communications, vol. 496, no. 2, pp. 260–266, 2018.
[53] F. Xie, S. Min, L. Liu, L. Peng, X. Hao, and X. Zhu, “Advancedage enhances the sepsis-induced up-regulation of the γ-andα7-nicotinic acetylcholine receptors in different parts of theskeletal muscles,” Archives of Gerontology and Geriatrics,vol. 65, pp. 1–8, 2016.
[54] J. M. C. Capcha, C. E. Rodrigues, R. S. Moreira et al., “Whar-ton’s jelly-derived mesenchymal stem cells attenuate sepsis-induced organ injury partially via cholinergic anti-inflammatory pathway activation,” American Journal ofPhysiology-Regulatory, Integrative and Comparative Physiol-ogy, vol. 318, no. 1, pp. R135–R147, 2020.
[55] P. R. Krafft, D. McBride, W. B. Rolland, T. Lekic, J. J. Flores,and J. H. Zhang, “α7 nicotinic acetylcholine receptor stimula-tion attenuates neuroinflammation through JAK2-STAT3activation in murine models of intracerebral hemorrhage,”BioMed Research International, vol. 2017, Article ID8134653, 13 pages, 2017.
[56] J. N. Redgrave, L. Moore, T. Oyekunle et al., “Transcutaneousauricular vagus nerve stimulation with concurrent upperlimb repetitive task practice for poststroke motor recovery:a pilot study,” Journal of Stroke and Cerebrovascular Diseases,vol. 27, no. 7, pp. 1998–2005, 2018.
[57] Y.-Z. Guan, X.-D. Jin, L.-X. Guan et al., “Nicotine inhibitsmicroglial proliferation and is neuroprotective in globalischemia rats,” Molecular Neurobiology, vol. 51, no. 3,pp. 1480–1488, 2015.
[58] Z. Han, F. Shen, Y. He et al., “Activation of α-7 nicotinic ace-tylcholine receptor reduces ischemic stroke injury throughreduction of proinflammatory macrophages and oxidativestress,” PLoS One, vol. 9, no. 8, article e105711, 2014.
[59] Y. Ben-David, S. Kagan, H. Cohen Ben-Ami et al., “RIC3, thecholinergic anti-inflammatory pathway, and neuroinflamma-tion,” International Immunopharmacology, vol. 83,p. 106381, 2020.
[60] T. W. Costantini, T. W. Chan, O. Cohen et al., “Uniquelyhuman CHRFAM7A gene increases the hematopoietic stemcell reservoir in mice and amplifies their inflammatoryresponse,” Proceedings of the National Academy of Sciences,vol. 116, no. 16, pp. 7932–7940, 2019.
[61] H. B. Li, Y. Zhou, A. H. Zhao, and L. L. Guo, “Exploring themechanism on the medullary visceral zone inhibiting thecholinergic anti-inflammatory pathway induced by sepsis,”Mediators of Inflammation, vol. 2020, no. 9, Article ID1320278, 2020.
[62] H. Li, Y. Li, W. Wang, Z. Peng, and F. Wu, Nan Fang Yi KeDa Xue Xue Bao, vol. 40, no. 5, pp. 647–653, 2020.
[63] C. Ren, X. H. Li, S. B. Wang et al., “Activation of central alpha7 nicotinic acetylcholine receptor reverses suppressedimmune function of T lymphocytes and protects against sep-sis lethality,” International Journal of Biological Sciences,vol. 14, no. 7, pp. 748–759, 2018.
[64] F. O. The, G. E. Boeckxstaens, S. A. Snoek et al., “Activationof the Cholinergic Anti-Inflammatory Pathway AmelioratesPostoperative Ileus in Mice,” Gastroenterology, vol. 133,no. 4, pp. 1219–1228, 2007.
[65] F. O. The, C. Cailotto, J. van der Vliet et al., “Central activa-tion of the cholinergic anti-inflammatory pathway reducessurgical inflammation in experimental post-operative ileus,”British journal of pharmacology, vol. 163, no. 5, pp. 1007–1016, 2011.
[66] M. L. Kelso and J. H. Oestreich, “Traumatic brain injury: cen-tral and peripheral role of α7 nicotinic acetylcholine recep-tors,” Current Drug Targets, vol. 13, no. 5, pp. 631–636, 2012.
[67] H. Elizabeth, L. Brandel Ankrapp Katie, and R. Arenkiel Ben-jamin, “Dynamic cholinergic tone in the basal forebrainreflects reward-seeking and reinforcement during olfactorybehavior,” Frontiers in Cellular Neuroscience, vol. 15, article635837, 2021.
[68] D. Tingley, A. S. Alexander, L. K. Quinn, A. A. Chiba, andD. A. Nitz, “Cell assemblies of the basal forebrain,” The Jour-nal of Neuroscience, vol. 35, no. 7, pp. 2992–3000, 2015.
[69] T. S. Faezeh and D. Ward Ryan, “Basal Forebrain mediatesmotivational recruitment of attention by reward-associatedcues,” Frontiers in Neuroscience, vol. 30, no. 12, p. 786, 2018.
[70] A. Nunez-Parra, C. D. Rio, A. Christian, M. M. Huntsman,and D. Restrepo, “The basal forebrain modulates neuronalresponse in an active olfactory discrimination task,” Frontiersin cellular neuroscience, vol. 5, no. 14, p. 141, 2020.
[71] A. N. Suarez, T. M. Hsu, C. M. Liu et al., “Gut vagal sensorysignaling regulates hippocampus function through multi-order pathways,” Nature Communications, vol. 9, no. 1,p. 2181, 2018.
[72] S. B. Mazzone and B. J. Undem, “Vagal afferent innervationof the airways in health and disease,” Physiological reviews,vol. 96, pp. 975–1024, 2016.
[73] V. A. Pavlov, W. R. Parrish, M. Rosas-Ballina et al., “Brainacetylcholinesterase activity controls systemic cytokine levelsthrough the cholinergic anti-inflammatory pathway,” Brain,Behavior, and Immunity, vol. 23, no. 1, pp. 41–45, 2009.
[74] L. Ma, M. A. Seager, M. Wittmann et al., “Selective activationof the M1muscarinic acetylcholine receptor achieved by allo-steric potentiation,” Proceedings of the National Academy ofSciences of the United States of America, vol. 106, no. 37,pp. 15950–15955, 2009.
[75] V. A. Pavlov, M. Ochani, M. Gallowitsch-Puerta et al., “Cen-tral muscarinic cholinergic regulation of the systemic inflam-matory response during endotoxemia,” Proceedings of theNational Academy of Sciences of the United States of America,vol. 103, no. 13, pp. 5219–5223, 2006.
[76] M. A. al-Onaizi, G. M. Parfitt, B. Kolisnyk et al., “Regulationof cognitive processing by hippocampal cholinergic tone,”Cerebral Cortex, vol. 27, pp. bhv349–bhv328, 2016.
[77] P. Munyaka, M. F. Rabbi, V. A. Pavlov, K. J. Tracey,E. Khafipour, and J. E. Ghia, “Central muscarinic cholinergicactivation alters interaction between splenic dendritic celland CD4+CD25− T cells in experimental colitis,” PLoS One,vol. 9, no. 10, article e109272, 2014.
[78] R. Lehner Kurt, A. Silverman Harold, E. Addorisio Meghanet al., “Forebrain cholinergic signaling regulates innateimmune responses and inflammation,” Frontiers in Immu-nology, vol. 10, p. 585, 2019.
[79] F. A. Koopman, S. S. Chavan, S. Miljko et al., “Vagus nervestimulation inhibits cytokine production and attenuates dis-ease severity in rheumatoid arthritis,” Proceedings of theNational Academy of Sciences of the United States of America,vol. 113, no. 29, pp. 8284–8289, 2016.
[80] M. C. Whitehead, A. Bergula, and K. Holliday, “Forebrainprojections to the rostral nucleus of the solitary tract in thehamster,” The Journal of Comparative Neurology, vol. 422,no. 3, pp. 429–447, 2000.
9Mediators of Inflammation

[81] M. R. Gielow and L. Zaborszky, “The input-output relation-ship of the cholinergic basal forebrain,” Cell Reports, vol. 18,no. 7, pp. 1817–1830, 2017.
[82] E. O'Loughlin, J. M. P. Pakan, D. Yilmazer-Hanke, and K. W.McDermott, “Acute in utero exposure to lipopolysaccharideinduces inflammation in the pre- and postnatal brain andalters the glial cytoarchitecture in the developing amygdala,”Journal of neuroinflammation, vol. 14, no. 1, p. 212, 2017.
[83] M. Gevezova, V. Sarafian, G. Anderson, and M. Maes,“Inflammation and mitochondrial dysfunction in autismspectrum disorder,” CNS & Neurological Disorders Drug Tar-gets, vol. 19, no. 5, pp. 320–333, 2020.
[84] N. Zaghloul, M. E. Addorisio, H. A. Silverman et al., “Fore-brain cholinergic dysfunction and systemic and brain inflam-mation in murine sepsis survivors,” Frontiers in Immunology,vol. 8, p. 1673, 2017.
[85] M. R. Amorim, J. L. de Deus, R. A. Cazuza et al., “Neuroin-flammation in the NTS is associated with changes in cardio-vascular reflexes during systemic inflammation,” Journal ofNeuroinflammation, vol. 16, no. 1, p. 125, 2019.
[86] Y. Chao, S. C. Wong, and E. K. Tan, “Evidence of inflamma-tory system involvement in Parkinson’s disease,” BioMedResearch International, vol. 2014, Article ID 308654, 9 pages,2014.
[87] S. J. Kim, M. J. Ryu, J. Han et al., “Activation of the HMGB1-RAGE axis upregulates TH expression in dopaminergic neu-rons via JNK phosphorylation,” Biochemical and biophysicalresearch communications, vol. 493, no. 1, pp. 358–364, 2017.
[88] G. P. Sims, D. C. Rowe, S. T. Rietdijk, R. Herbst, and A. J.Coyle, “HMGB1 and RAGE in inflammation and cancer,”Annual Review of Immunology, vol. 28, no. 1, pp. 367–388,2010.
[89] M. L. Pearn, I. R. Niesman, J. Egawa et al., “Pathophysiologyassociated with traumatic brain injury: current treatmentsand potential novel therapeutics,” Cellular and MolecularNeurobiology, vol. 37, no. 4, pp. 571–585, 2017.
[90] S. Schiavone, M. Neri, L. Trabace, and E. Turillazzi, “TheNADPH oxidase NOX2 mediates loss of parvalbumin inter-neurons in traumatic brain injury: human autoptic immuno-histochemical evidence,” Scientific Reports, vol. 7, no. 1,p. 8752, 2017.
[91] X. Tan, P. L. Jiao, Y. K. Wang et al., “The phosphoinositide-3kinase signaling is involved in neuroinflammation in hyper-tensive rats,” CNS Neuroscience & Therapeutics, vol. 23,no. 4, pp. 350–359, 2017.
[92] M. L. Xu and X. J. Yu, “Calcitriol ameliorated autonomic dys-function and hypertension by down-regulating inflammationand oxidative stress in the paraventricular nucleus of SHR,”Toxicology and Applied Pharmacology, vol. 394, p. 114950,2020.
[93] J. P. Thaler, C. X. Yi, E. A. Schur et al., “Obesity is associatedwith hypothalamic injury in rodents and humans,” The Jour-nal of clinical investigation, vol. 122, pp. 153–162, 2012.
[94] A. C. Souza, C. M. Souza, C. L. Amaral et al., “Short-termhigh-fat diet consumption reduces hypothalamic expressionof the nicotinic acetylcholine receptor α7 subunit (α7nAChR)and affects the anti-inflammatory response in a mouse modelof sepsis,” Frontiers in immunology, vol. 10, p. 565, 2019.
[95] L. Yin, X. Xu, G. Chen et al., “Inflammation and decreasedfunctional connectivity in a widely-distributed network indepression: centralized effects in the ventral medial prefrontalcortex,” Brain, Behavior, and Immunity, vol. 80, pp. 657–666,2019.
[96] R. R. Patel, S. A.Wolfe, M. Bajo et al., “IL-10 normalizes aber-rant amygdala GABA transmission and reverses anxiety-likebehavior and dependence-induced escalation of alcoholintake,” Progress in Neurobiology, vol. 199, p. 101952, 2021.
[97] V. Michopoulos, A. Powers, C. F. Gillespie, K. J. Ressler, andT. Jovanovic, “Inflammation in fear- and anxiety-based dis-orders: PTSD, GAD, and beyond,” Neuropsychopharmacol-ogy, vol. 42, no. 1, pp. 254–270, 2017.
[98] H. Ji, M. F. Rabbi, B. Labis, V. A. Pavlov, K. J. Tracey, and J. E.Ghia, “Central cholinergic activation of a vagus nerve-to-spleen circuit alleviates experimental colitis,”Mucosal Immu-nology, vol. 7, no. 2, pp. 335–347, 2014.
[99] T. L. Ben-Shaanan, H. Azulay-Debby, T. Dubovik et al.,“Activation of the reward system boosts innate and adaptiveimmunity,” Nature Medicine, vol. 22, no. 8, pp. 940–944,2016.
[100] E. F. Trakhtenberg and J. L. Goldberg, “Neuroimmune com-munication,” Science, vol. 334, no. 6052, pp. 47-48, 2011.
[101] C. H. Wong, C. N. Jenne, W. Y. Lee, C. Léger, and P. Kubes,“Functional innervation of hepatic iNKT cells is immunosup-pressive following stroke,” Science, vol. 334, no. 6052,pp. 101–105, 2011.
[102] D. Lorton and D. L. Bellinger, “Molecular mechanismsunderlying β-adrenergic receptor-mediated cross-talkbetween sympathetic neurons and immune cells,” Interna-tional Journal of Molecular Sciences, vol. 16, no. 12,pp. 5635–5665, 2015.
[103] J. C. Padro and V.M. Sanders, “Neuroendocrine regulation ofinflammation,” Seminars in Immunology, vol. 26, no. 5,pp. 357–368, 2014.
[104] L. D. Bellinger and D. Lorton, “Autonomic regulation of cel-lular immune function,” Autonomic Neuroscience, vol. 182,pp. 15–41, 2014.
10 Mediators of Inflammation