Table 1. α/β et al - ASTRO 2004astro.abstractsnet.com/handouts/000245_2109post.pdfOver the past...
1
Click here to load reader
Transcript of Table 1. α/β et al - ASTRO 2004astro.abstractsnet.com/handouts/000245_2109post.pdfOver the past...

Biological Comparison of Partial Breast Irradiation Protocols Versus Standard Whole
Breast Irradiation: Implications for Tumor Control and Normal Tissue ToleranceStella C. Lymberis, Barry S. Rosenstein, Silvia C. Formenti. Department of Radiation Oncology, NYU School of Medicine, NYC, NY.
ABSTRACTPurpose/Objective: Over the past decade, a variety of partial breast irradiation(PBI) techniques have been used which are designed to treat only the portion of the breast at high risk for local recurrence. We present an analysis of dose/fractionation schedules currently used in ongoing clinical trials of partial breast irradiation (PBI) by comparing their biologically effective dose (BED) values to those of three standard whole breast protocols commonly used after segmental mastectomy in the treatment of breast cancer.
Materials/Methods: The BED equation derived from the linear quadratic model for radiation-induced cell killing was used to calculate BED values for a variety of external beam, as well as HDR brachytherapy PBI protocols and compared to whole breast radiotherapy protocols (Standards). External beam PBI protocols analyzed include published reports from Christie Hospital, William Beaumont Hospital, and New York University. HDR Brachytherapy protocols included National Institute of Hungary, London Regional Cancer Center, Ochsner Clinic, William Beaumont Hospital, RTOG 95-17, Mammosite Multicenter Trial, and Virginia Commonwealth University. The same method was applied to three commonly used whole breast radiotherapy protocols for comparison: 1) 50 Gy in 25 fractions (Standard50); 2) 60 Gy in 30 fractions (46 Gy whole breast plus 14 Gy to the tumor bed, Standard60); and 3) 66 Gy in 33 fractions (50 Gy whole breast plus 16 Gy to the tumor bed, Standard66).
Results: Assuming that the α/β value for breast carcinoma is 4 Gy (Williams et al., IJROBP 1985; 11:87-96), the BED values of most PBI protocols resulted in tumor control BEDs roughly equivalent to those of Standard50, but consistently lower than the BEDs for either the Standard60 or Standard66. Regarding normal tissue reactions, the BED values calculated for the acute radiation responses of erythema and desquamation (α/β values of 8 Gy and 11 Gy) were nearly all lower for the PBI schedules compared to standard treatments (see Table below). As expected, the late response BEDs for most PBI regimens were greater than the BEDs for the standards.
Conclusions: The enhanced risk of fibrosis and telangiectasia for the PBI hypo-fractionated protocols predicted by BED calculations should be tempered by the consideration that relatively small volumes of normal breast tissue receive the full treatment dose. Importantly, BED modeling raises the concern that inadequate dose might be delivered by PBI to assure optimal in-field tumor control. This is particularly relevant in view of level I evidence for dose response within the boost volume, as reported by the EORTC prospective randomized trial (Bartelink et al., N Engl J Med 2001; 345:1378-1387). Finding the balance between adequate imaging and irradiation of the target, and limiting the breast volume receiving the full treatment dose to avoid an increased risk of late radiation sequelae, together with correct selection of patients at low risk for recurrences outside the target volume, underlie the successful outcome of PBI trials. In addition, the carcinogenic risk associated with a relatively low dose to normal breast tissue outside of the target volume demands careful investigation. For all these reasons, and since equivalence to standard protocols for both efficacy and morbidity has yet to be proven, PBI regimens remain investigational.
ASTRO ATLANTA2004
BACKGROUNDLimiting adjuvant radiation to a volume inclusive of the tumor with sufficient margins among selected patients
enables the exploration of hypo-fractionated regimens (1-3). A number of protocols have since been developed with the intent to treat the original tumor bed with margins with larger fraction sizes, while maintaining a low risk of late effects. Hypo-fractionated, partial breast irradiation is actively being investigated by the use of several distinct techniques including interstitial brachytherapy, Mammosite® ballooon brachytherapy and external beam radiation using either three dimensional conformal radiotherapy (3D-CRT), intensity modulated radiotherapy (IMRT), or intra-operative electron beam therapy (IORT).
Although many PBI protocols are currently being used, relatively little data has been reported to justify the chosen schedules by predicting the biological effects associated with use of large dose fractions delivered over a short period. Since it is possible to compare the anticipated biological effects in terms of tumor control and normal tissue reactions by estimating a “biological dose” through appropriate computations of BED values, we are reporting such calculations to compare the different PBI regimens with three commonly used protocols for whole breast radiation.
Methods Breast Radiation Protocols A. Standard Fractionation Studies
Various fractionation regimens have been used for the radiation component of breast conservation treatment, however three main regimens were chosen as “standard” fractionation regimens with which to compare the partial breast radiation studies. The NSABP trials of breast preservation (4,5), as well as in the recent prospective randomized Canadian trial studying whole breast hypo-fractionation (6), used 50 Gray in 25 fractions over five weeks (Standard50). An alternative standard regimen is 46 Gy to the whole breast followed by an electron boost of 14 Gy to the tumor bed (7,8), (Standard60). The EORTC demonstrated the role of a boost to the tumor excision site and demonstrated an improvement in local control with irradiation of the entire breast with 50 Gy in 25 fractions followed by 16 Gy in 8 fractions for a total dose of 66 Gy (Standard66) (9,10).
B. Partial Breast Irradiation StudiesA variety of PBI protocols, using brachytherapy, 3D-conformal external beam radiotherapy, or intraoperativeradiation therapy (IORT), have been developed with the intent to treat the original tumor bed with margins and are summarized in Table 1. HDR Brachytherapy protocols include the National Institute of Hungary, London Regional Cancer Center, Ochsner Clinic, William Beaumont Hospital, RTOG 95-17, Mammosite Multicenter Trial, and Virginia Commonwealth University.
Table 1. Accelerated Partial Breast Irradiation Brachytherapy (HDR and LDR) and IORT Studies
CONCLUSIONS
1. Using an αααα/ββββ = 4Gy for tumor control, BED values for the PBI treatments were generally comparable to the BEDs obtained for Standard50.
2. However, BED values for PBI treatments were uniformly lower when compared to either Standard60, a fractionation regimen commonly used in the United States, or to Standard66. This is of potential concern since the Standard66 treatment resulted in a decreased incidence of tumor recurrence compared with the Standard50.
3. In addition, follow-up for both the brachytherapy and external techniques is too short for adequate assessment of long-term toxicity and fibrosis.
4. Since equivalence to standard protocols for both efficacy and morbidity has yet to be proven, PBI protocols remain investigational.
RESULTS
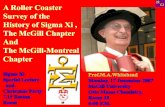
Figure 1. Histograms demonstrating BED Values for PBI External and Brachytherapy Protocols Compared to Standard Whole Breast Protocols for Tumor Control, Figures 1a and 1b, Acute Effects, Figure 1c, and Late Effects, Figure 1d.
Abbreviations in Figure are as follows: WBH for William Beaumont Hospital, NYU for New York University, NIO for National Institute of Oncology, LRCC for London Regional Cancer Center. * = RTOG 95-17, Mammosite ® Multi-center Trial, Virginia Commonwealth University, and William Beaumont Hospital.
Methods Breast Radiation Protocols
There have been three reported series of external beam partial breast radiation, summarized in Table 2, from Christie Hospital, William Beaumont Hospital and New York University.
Table 2. Accelerated Partial Breast Irradiation: External Beam Studies
PBI External Beam Techniques
William Beaumont Hospital (11) New York University (12)
Table 3. Dosimetric Comparison of External Beam Partial Breast Techniques
* Percent of Lung or Heart Volume receiving 5 Gy (D5) or 10 Gy (D10).
Calculation of biologically effective doses
The linear-quadratic model was used to determine whether a partial breast radiotherapy protocol should result in a roughly equal probability of tumor control compared with a standard schedule, but without increasing the potential for normal tissue damage shown below;
BED = nd (1+d / α/β)
where n is the number of fractions, d is the dose per fraction and α/β is a tissue and effect specific parameter.
A modification to this BED equation was also used to take into account cellular proliferation as follows;
BED = nd [1+d / α/β] – ln 2 (T) / (α Tpot)
where Tpot is the potential doubling time and T is the treatment time during which cellular proliferation occurs after any initial lag period. --08 IORT electro therapy
10-21 GyNeg.Excl.-< 2.5 All101European Institute
of Oncology
Ph I/II 4.4%
Ph III 0%
1-2Ph I/II 57
Ph III 30
Ph I/II HDR 4.33Gy x 7,5.2 Gy x 7;
Ph III HDR 5.2 Gy x 7
Neg.Excl.N0< 2 AllPh I/II 45
Ph III 63
National Institute of Oncology, Hungary
--> 121HDR3.4 Gy x 10, bid
Neg.Excl.N0< 2>45 43Mammosite ® Multi-center Trial
0 1-242LDR 45 Gy / 4 daysHDR 3.4 Gy x 10, bid
Neg.Excl.N1< 4All44Virginia CommonwealthUniversity
--232HDR 3.4 Gy x 10 bidLDR 45 Gy / 4 days
Neg.Excl.N1<3All100RTOG 95-17
16.2 %091HDR3.72 Gy / 10 fx bid
Pos.Pos.N0< 5All39London Regional Cancer Centre, Canada
1%1-2 65LDR 50 Gy / 4 daysHDR 4Gy x 8,
3.4 Gy x 10
Neg. Neg.N0< 3> 40 199William Beaumont Hospital
2%2-375LDR 45 Gy / 4 daysHDR 4 Gy x 8
Neg.Pos.N1 Tis &< 4
All50Ochsner Clinic
37%2 72 HDR55 Gy / 5 days
Pos.Pos.N0< 4< 70 27Guy’s Hospital Trial
5-year Ipsilateral
RecurrenceRate (%)
CTVMargin
(cm)
Median Follow-up
(mo)
Dose Fractionation
MarginsEICNT (cm)
Age(yrs)
Patients(n)
Series(Reference)
--1-1.5Architectural distortion,
and surgical clips on CT
3-5 Non-coplanarbeams
Supine6, 18 MVPhotons
103.4 Gy x 10 in 5 days, or
3.85 Gy x 10 in 5 days
Neg.N0< 350 31William Beaumont Hospital
0%1.5-2 Architectural distortion on
CT
2 co-planarmini
tangents
Prone 6 MV
Photons
17 6 Gy x 5 in 10 days
Neg.N0< 2Post-men.
47New York University
6% (21/355)
0Tumor bed at surgery
Single electronbeam
Supine with 10 MeV
electrons
96 5Gy x 8 in 10 days
-N0< 4 < 70 353Christie Hospital
Ipsi-Breast Rec.
Rate (%)
Margin(cm)
Definition ofTumor bed
(CTV)
FieldsTechniqueMedian Follow-up
(mo.)
Dose Fractionat
ion
EICNT(cm)
Age(yrs)
Pts(n)
Series(Reference)
D100%
(0-7%)
16% (0-37%)
60%(39-92%)
46%(34-60%)
35%(26-53%)
21%(14-39)
17%(11-22)
240(82-482)
William Beaumont Hospital (11)
D50%(0)
0%(0)
53%(27-82%)
46%(23-75%)
40%(20-68)
27%(10-45)
22%(10-55)
192(57-1118)
New York University (12)
MedianCardiac
DoseD10
or D5 *
MedianLungDosesD5 *
Median Ipsilateral
Breast Coverage
25%
Median Ipsilateral
Breast Coverage
50%
Median Ipsilateral
Breast Coverage
75%
Median Ipsilateral
Breast Coverage
100%
MedianPTV / TBV
(Total Breast Vol.)
Median PTV
Volume (cm3)
Series(Reference)
REFERENCES1. Kuske R, Winter, K, Arthur, D et al. A Phase I/II Trial of Brachytherapy Alone Following Lumpectomy for Select Breast Cancer: Toxicity Analysis of Radiation Therapy Oncology Group 95-17. Proc ASTRO, Int J Radiat Oncol Biol Phys 2002;54:87.
2. Vicini F, Kini VR, Chen P, et al. Irradiation of the tumor bed alone after lumpectomy in selected patients with early-stage breast cancer treated with breast conserving therapy. J Surg Oncol 1999;70:33-40.3. Fentiman IS, Poole C, Tong D, et al. Inadequacy of iridium implant as sole radiation treatment for operable breast cancer. Eur J Cancer 1996;32A:608-611.4. Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002;347:1233-1241.5. Fisher B, Bryant J, Dignam JJ, et al. Tamoxifen, radiation therapy, or both for prevention of ipsilateral breast tumor recurrence after lumpectomy in women with invasive breast cancers of one centimeter or less. J Clin Oncol 2002;20:4141-4149.6. Whelan T, MacKenzie R, Julian J, et al. Randomized trial of breast irradiation schedules after lumpectomy for women with lymph node-negative breast cancer. J Natl Cancer Inst 2002;94:1143-1150.7. Gage I, Recht A, Gelman R, et al. Long-term outcome following breast-conserving surgery and radiation therapy. Int J Radiat Oncol Biol Phys 1995;33:245-251.8. Abner AL, Recht A, Vicini FA, et al. Cosmetic results after surgery, chemotherapy, and radiation therapy for early breast cancer. Int J Radiat Oncol Biol Phys 1991;21:331-338.9. Romestaing P, Lehingue Y, Carrie C, et al. Role of a 10-Gy boost in the conservative treatment of early breast cancer: results of a randomized clinical trial in Lyon, France. J Clin Oncol 1997;15:963-968.10. Bartelink H, Horiot JC, Poortmans P, et al. Recurrence rates after treatment of breast cancer with standard radiotherapy with or without additional radiation. N Engl J Med 2001;345:1378-1387.11. Vicini FA, Remouchamps V, Wallace M, et al. Ongoing clinical experience utilizing 3D conformal external beam radiotherapy to deliver partial-breast irradiation in patients with early-stage breast cancer treated with breast-conserving therapy. Int J Radiat Oncol Biol Phys 2003;57:1247-1253.12. Formenti SC, Truong MT, Goldberg JD, et al. Prone accelerated partial breast irradiation after breast conserving surgery: Preliminary clinical results and dose-volume histogram analysis. Int J Radiat OncolBiol Phys, 2004; in press.