SPONTANEOUS ABORTION Incidence - Professional · and connective tissue disease, such as systemic...
14
259 14 Early Pregnancy Risks Peter S. Uzelac, MD, & Sara H. Garmel, MD SPONTANEOUS ABORTION ESSENTIALS OF DIAGNOSIS • Suprapubic pain, uterine cramping, and/or back pain. • Vaginal bleeding. • Cervical dilatation. • Extrusion of products of conception. • Disappearance of symptoms and signs of preg- nancy. • Quantitative β-human chorionic gonadotropin that is not properly increasing. • Abnormal ultrasound findings (eg, empty gesta- tional sac, fetal disorganization, lack of fetal growth). General Considerations Spontaneous abortion is the most common complica- tion of pregnancy and is defined as the passing of a pregnancy prior to completion of the 20th gestational week. It implies delivery of all or any part of the prod- ucts of conception, with or without a fetus weighing less than 500 g. Threatened abortion is bleeding of in- trauterine origin occurring before the 20th completed week, with or without uterine contractions, without di- latation of the cervix, and without expulsion of the products of conception. Complete abortion is the ex- pulsion of all of the products of conception before the 20th completed week of gestation, whereas incomplete abortion is the expulsion of some, but not all, of the products of conception. Inevitable abortion refers to bleeding of intrauterine origin before the 20th com- pleted week, with dilatation of the cervix without ex- pulsion of the products of conception. In missed abor- tion, the embryo or fetus dies, but the products of conception are retained in utero. In septic abortion, infection of the uterus and sometimes surrounding structures occur. Incidence Although the true incidence of spontaneous abortion is unknown, approximately 15% of clinically evident pregnancies and 60% of chemically evident pregnancies end in spontaneous abortion. Eighty percent of sponta- neous abortions occur prior to 12 weeks’ gestation. The incidence of abortion is influenced by the age of the mother and by a number of pregnancy-related fac- tors, including a history of a previous full-term normal pregnancy, the number of previous spontaneous abor- tions, a previous stillbirth, and a previous infant born with malformations or known genetic defects. Addition- ally, parental influences, including balanced translocation carriers and medical complications, may influence the rate of spontaneous abortion. Etiology An abnormal karyotype is present in approximately 50% of spontaneous abortions occurring during the first trimester. The incidence decreases to 20–30% in second-trimester losses and to 5–10% in third-trimester losses. As discussed in the next section, the first-trimester losses are typically au- tosomal trisomies or monosomy X, whereas later losses re- flect chromosomal abnormalities seen in neonates. Other suspected causes of spontaneous abortion ac- count for a smaller percentage of losses and include in- fection, anatomic defects, endocrine factors, immuno- logic factors, and maternal systemic diseases. In a significant percentage of spontaneous abortions, the eti- ology is unknown. A. MORPHOLOGIC AND GENETIC ABNORMALITIES Aneuploidy (an abnormal chromosomal number) is the most common genetic abnormality, accounting for at least 50% of early spontaneous abortions. Monosomy X or Turner’s syndrome is the single most common aneu- ploidy, comprising approximately 20% of these gesta- tions. As a group, the autosomal trisomies account for over half of aneuploid losses, with trisomy 16 being the most common. Autosomal trisomies have been noted for every chromosome except chromosome number 1. Polyploidy, usually in the form of triploidy, is found in approximately 20% of all miscarriages. Polyploid con-
Transcript of SPONTANEOUS ABORTION Incidence - Professional · and connective tissue disease, such as systemic...

259
14
Early Pregnancy Risks
Peter S. Uzelac, MD, & Sara H. Garmel, MD
SPONTANEOUS ABORTION
ESSENTIALS OF DIAGNOSIS
• Suprapubic pain, uterine cramping, and/or backpain.
• Vaginal bleeding.
• Cervical dilatation.
• Extrusion of products of conception.
• Disappearance of symptoms and signs of preg-nancy.
• Quantitative
β
-human chorionic gonadotropinthat is not properly increasing.
• Abnormal ultrasound findings (eg, empty gesta-tional sac, fetal disorganization, lack of fetal
growth).
General Considerations
Spontaneous abortion
is the most common complica-tion of pregnancy and is defined as the passing of apregnancy prior to completion of the 20th gestationalweek. It implies delivery of all or any part of the prod-ucts of conception, with or without a fetus weighingless than 500 g.
Threatened abortion
is bleeding of in-trauterine origin occurring before the 20th completedweek, with or without uterine contractions, without di-latation of the cervix, and without expulsion of theproducts of conception.
Complete abortion
is the ex-pulsion of all of the products of conception before the20th completed week of gestation, whereas
incompleteabortion
is the expulsion of some, but not all, of theproducts of conception.
Inevitable abortion
refers tobleeding of intrauterine origin before the 20th com-pleted week, with dilatation of the cervix without ex-pulsion of the products of conception. In
missed abor-tion,
the embryo or fetus dies, but the products ofconception are retained in utero. In
septic abortion,
infection of the uterus and sometimes surroundingstructures occur.
Incidence
Although the true incidence of spontaneous abortion isunknown, approximately 15% of clinically evidentpregnancies and 60% of chemically evident pregnanciesend in spontaneous abortion. Eighty percent of sponta-neous abortions occur prior to 12 weeks’ gestation.
The incidence of abortion is influenced by the age ofthe mother and by a number of pregnancy-related fac-tors, including a history of a previous full-term normalpregnancy, the number of previous spontaneous abor-tions, a previous stillbirth, and a previous infant bornwith malformations or known genetic defects. Addition-ally, parental influences, including balanced translocationcarriers and medical complications, may influence therate of spontaneous abortion.
Etiology
An abnormal karyotype is present in approximately 50% ofspontaneous abortions occurring during the first trimester.The incidence decreases to 20–30% in second-trimesterlosses and to 5–10% in third-trimester losses. As discussedin the next section, the first-trimester losses are typically au-tosomal trisomies or monosomy X, whereas later losses re-flect chromosomal abnormalities seen in neonates.
Other suspected causes of spontaneous abortion ac-count for a smaller percentage of losses and include in-fection, anatomic defects, endocrine factors, immuno-logic factors, and maternal systemic diseases. In asignificant percentage of spontaneous abortions, the eti-ology is unknown.
A. M
ORPHOLOGIC
AND
G
ENETIC
A
BNORMALITIES
Aneuploidy (an abnormal chromosomal number) is themost common genetic abnormality, accounting for atleast 50% of early spontaneous abortions. Monosomy Xor Turner’s syndrome is the single most common aneu-ploidy, comprising approximately 20% of these gesta-tions. As a group, the autosomal trisomies account forover half of aneuploid losses, with trisomy 16 being themost common. Autosomal trisomies have been noted forevery chromosome except chromosome number 1.
Polyploidy, usually in the form of triploidy, is foundin approximately 20% of all miscarriages. Polyploid con-

260 /
CHAPTER 14
ceptions typically result in empty sacs or blighted ova butoccasionally can lead to partial hydatidiform moles.
The remaining half of early abortuses appear to havenormal chromosomal complements. Of these, 20%have other genetic abnormalities that may account forthe loss. Mendelian or polygenic factors resulting in an-atomic defects may play a role. These factors tend to bemore common in later fetal losses.
B. M
ATERNAL
F
ACTORS
1. Systemic diseasea. Maternal infections—
Organisms such as
Trep-onema pallidum, Chlamydia trachomatis, Neisseria gonor-rhoeae, Streptococcus agalactiae,
herpes simplex virus, cy-tomegalovirus, and
Listeria monocytogenes
have beenimplicated in spontaneous abortion. Although theseagents have been identified in early losses, a causal rela-tionship has not been established.
b. Other diseases—
Endocrine disorders such as hy-perthyroidism and poorly controlled diabetes mellitus; car-diovascular disorders, such as hypertensive or renal disease;and connective tissue disease, such as systemic lupus erythe-matosus, may be associated with spontaneous abortion.
2. Uterine defects—
Congenital anomalies that distortor reduce the size of the uterine cavity, such as unicornu-ate, bicornuate, or septate uterus, carry a 25–50% risk ofmiscarriage. A diethylstilbestrol (DES)-related anomaly,such as a T-shaped or hypoplastic uterus, also carries anincreased risk of miscarriage. Acquired anomalies, partic-ularly submucous or intramural myomas, have been asso-ciated with spontaneous abortions as well.
Previous scarring of the uterine cavity following di-latation and curettage (D&C; Asherman’s syndrome),myomectomy, or unification procedures has been im-plicated in spontaneous miscarriage, as has anatomic orfunctional incompetence of the uterine cervix.
3. Immunologic disorders—
Blood group incompati-bility due to ABO, Rh, Kell, or other less common an-tigens has been associated with spontaneous abortions.Furthermore, similar maternal and paternal humanleukocyte antigen (HLA) status may enhance the possi-bility of abortion by causing insufficient maternal im-munologic recognition of the fetus.
4. Malnutrition—
Severe malnutrition has been impli-cated in spontaneous losses.
5. Emotional disturbances—
Emotional causes of abor-tion are speculative. No valid evidence supports theconcept that abortion may be induced by fright, grief,anger, or anxiety.
C. T
OXIC
F
ACTORS
Agents such as radiation, antineoplastic drugs, anes-thetic gases, alcohol, and nicotine have been shown to
be embryotoxic. Other agents such as lead, ethylene ox-ide, and formaldehyde have also been implicated.
D. T
RAUMA
Direct trauma, such as injury to the uterus from a gun-shot wound, or indirect trauma, such as surgical re-moval of an ovary containing the corpus luteum ofpregnancy, may result in spontaneous abortion.
Pathology
In spontaneous abortion, hemorrhage into the deciduabasalis often occurs. Necrosis and inflammation appearin the area of implantation. The pregnancy becomespartially or entirely detached. Uterine contractions anddilatation of the cervix result in expulsion of most or allof the products of conception.
Clinical Findings
A. T
HREATENED
A
BORTION
At least 20–30% of pregnant women have some first-trimester bleeding. In most cases, this is thought to repre-sent an implantation bleed. The cervix remains closed, andslight bleeding with or without cramping may be noted.
B. I
NEVITABLE
A
BORTION
Abdominal or back pain and bleeding with an open cer-vix indicate impending abortion. Abortion is inevitablewhen cervical effacement, cervical dilatation, and/orrupture of the membranes is noted.
C. I
NCOMPLETE
A
BORTION
(F
IG
14–1)
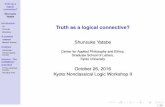
In incomplete abortion the products of conception havepartially passed from the uterine cavity. In gestations ofless than 10 weeks’ duration, the fetus and placenta areusually passed together. After 10 weeks, they may bepassed separately, with a portion of the products retainedin the uterine cavity. Cramps are usually present. Bleed-ing generally is persistent and is often severe.
D. C
OMPLETE
A
BORTION
(F
IG
14–2)
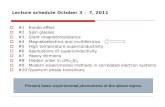
Complete abortion is identified by passage of the entireconceptus. Slight bleeding may continue for a shorttime, although pain usually ceases after pregnancy hastraversed the cervix.
E. M
ISSED
A
BORTION
Missed abortion implies that the pregnancy has been re-tained following death of the fetus. Why the pregnancyis not expelled is not known. It is possible that normalprogestogen production by the placenta continueswhile estrogen levels fall, which may reduce uterinecontractility.
EARLY PREGNANCY RISKS
/ 261
F. B
LIGHTED
O
VUM
Blighted ovum or anembryonic pregnancy represents afailed development of the embryo so that only a gesta-tional sac, with or without a yolk sac, is present. An al-ternative hypothesis proposes that the fetal pole hasbeen resorbed prior to ultrasound diagnosis.
Laboratory Findings
A. C
OMPLETE
B
LOOD
C
OUNT
If significant bleeding has occurred, the patient will beanemic. Both the white blood cell count and the sedi-mentation rate may be elevated even without the pres-ence of infection.
B. P
REGNANCY
T
ESTS
Falling or abnormally rising plasma levels of
β
-humanchorionic gonadotropin (hCG) are diagnostic of an ab-normal pregnancy, either a blighted ovum, spontaneousabortion, or ectopic pregnancy.
Ultrasonography
Transvaginal ultrasound is helpful in documenting intra-uterine pregnancies as early as 4–5 weeks’ gestation. Fetalheart motion should be seen in embryos > 5 mm fromcrown to rump or in embryos at least 5–6 weeks’ gesta-tion. Ultrasound is useful in determining which pregnan-cies are viable and which are most likely to miscarry.
In threatened abortion, ultrasound will reveal anormal gestational sac and viable embryo. However, a
large or irregular sac, an eccentric fetal pole, the pres-ence of a large (> 25% of sac size) retrochorionicbleed, and/or a slow fetal heart rate (< 85 bpm) carry apoor prognosis. Miscarriage becomes increasingly lesslikely the further the gestation progresses. If a viablefetus of 6 weeks or less is seen on ultrasound, the riskof miscarriage is approximately 15–30%. The risk de-creases to 5–10% at 7–9 weeks’ gestation and to lessthan 5% after 9 weeks’ gestation.
In incomplete abortion, the gestational sac usually isdeflated, and irregular, echogenic material representingplacental tissue is seen in the uterine cavity. In completeabortion, the endometrium appears closely apposed,with no visible products of conception.
An embryo or fetus without heart motion is consistentwith a missed abortion, whereas an abnormal gestationalsac, without a yolk sac or embryo, is consistent with ablighted ovum (Figs 14–3 to 14–6). Most pregnancies arelost weeks before mothers complain of signs or symptoms.
Ectopic pregnancy may cause similar symptoms ofmiscarriage, namely, menstrual abnormality and ab-dominal or pelvic pain. An adnexal mass may or maynot be present. Ultrasound can virtually exclude an ec-topic pregnancy by documenting an intrauterine preg-nancy, as the chance of a simultaneous intrauterine andextrauterine pregnancy (heterotopic pregnancy) is ex-ceedingly rare in spontaneous pregnancies, occurring inonly 1 in 15,000–40,000 pregnancies.
Hydatidiform mole usually ends in abortion beforethe fifth month. Theca lutein cysts, when present, causebilateral ovarian enlargement; the uterus may be unusu-ally large. Bloody discharge may contain hydropic villi.
Figure 14–1.
Incomplete abortion.
Right:
Product of incomplete abortion.
(Reproduced, with permis-sion, from Benson RC
: Handbook of Obstetrics & Gynecology,
8th ed. Lange, 1983.)
Figure 14–2.
Complete abortion.
Right:
Product of complete abortion.
(Reproduced, with per-mission, from Benson RC
: Handbook of Obstet-rics & Gynecology,
8th ed. Lange, 1983.)

262 /
CHAPTER 14
Other entities that may be confused with abortioninclude cervical infection, extruding pedunculated my-oma, and cervical neoplasia. However, the pregnancytest will be negative unless a pregnancy coexists.
Complications
Severe or persistent hemorrhage during or followingabortion may be life threatening. The more advancedthe gestation, the greater the likelihood of excessiveblood loss. Sepsis develops most frequently after self-induced abortion. Infection, intrauterine synechia, and
infertility are other complications of abortion. Perfora-tion of the uterine wall may occur during D&C be-cause of the soft and vaguely outlined uterine wall andmay be accompanied by injury to the bowel and blad-der, hemorrhage, infection, and fistula formation.
Multiple pregnancy with the loss of 1 fetus and re-tention of another (“vanishing twin”) not only is pos-sible but has been well documented in 20% of earlypregnancies closely monitored by ultrasound. Usuallythe fetus is simply resorbed, but the loss of 1 fetus inmultiple gestation may be accompanied by crampingor vaginal bleeding.
Figure 14–3.
Intrauterine pregnancy at 8 weeks’ gesta-tion, demonstrating embryo (E) and yolk sac (Ys).
Figure 14–4.
Embryonic demise at 8 weeks’ gesta-tion, with irregular gestational sac.
Ys E
Figure 14–5.
Empty gestational sac, consistent with a blighted ovum.
Figure 14–6.
Empty uterus (U) with an adnexal mass (A) suspicious for an ectopic pregnancy.
β
-hCG at the time of transabdominal ultrasound was just over 100 mIU/mL.
UA

EARLY PREGNANCY RISKS
/ 263
Even with very early miscarriage, a loss can have asignificant effect on the family. The fact that most ofthese losses are unexpected intensifies this grief. Eachperson responds differently to his or her tragedy. It isthe health care worker’s responsibility to help parentsmourn by acknowledging their loss and identifying po-tential support systems.
Prevention
Some losses can be prevented by early obstetric care,with adequate treatment of maternal disorders such asdiabetes and hypertension, and by protection of preg-nant women from environmental hazards and exposureto infectious diseases.
Treatment of Abortions
Successful management of spontaneous abortion de-pends upon early diagnosis. Every patient should re-ceive a general physical examination, and a completehistory should be taken. Laboratory studies should in-clude a complete blood count, blood typing, and cervi-cal cultures to determine pathogens in case of infection.
If the diagnosis of threatened abortion is made, bedrest and pelvic rest typically are recommended, al-though neither has been shown to be helpful in pre-venting subsequent miscarriage. Prognosis is good whenbleeding and/or cramping resolve.
If the diagnosis of inevitable or incomplete abortion ismade, evacuation of the uterus by a surgical methodshould be considered. Significant bleeding or retainedproducts usually require a D&C; however, cases in whichblood loss is minimal can be observed for spontaneouscompletion. A type and cross-match for possible bloodtransfusion and determination of Rh status should be ob-tained. The prognosis for the mother is excellent if theretained tissue is promptly and completely evacuated.
If the diagnosis of complete abortion is made, thepatient should be observed for further bleeding. Theproducts of conception should be examined. As withinevitable and incomplete abortion, the prognosis forthe mother is excellent.
If abortion has occurred after the first trimester, hos-pitalization should be considered. Oxytocics are helpfulin contracting the uterus, limiting blood loss, and aid-ing in expulsion of clots and tissue. Ergot preparations,which contract the cervix and the uterus, may also begiven if needed. As with a first-trimester loss, a D&Cmay be necessary if significant bleeding persists or ifproducts of conception are retained.
Treatment of Complications
Uterine perforation may be manifested by signs of in-traperitoneal bleeding, rupture of the bowel or bladder,
or peritonitis. Oftentimes, there are no clinical signsand no sequelae. When uterine perforation is suspected,however, laparoscopy and/or laparotomy are indicatedto determine the extent of laceration or bowel injury.
RECURRENT ABORTION
General Considerations
Recurrent abortion
in its broadest definition is de-fined as 2 to 3 or more consecutive pregnancy lossesbefore 20 weeks of gestation, each with a fetus weigh-ing less than 500 g. Approximately 1% of women arehabitual aborters. Prognosis for a successful subse-quent pregnancy is correlated with the number of pre-vious abortions. The risk of having a spontaneousabortion for the first time is about 15%, and this riskis at least doubled in women experiencing recurrentabortion (Table 14–1).
Other factors with prognostic implications includematernal age and abortus karyotype. The former is di-rectly correlated with the risk of abortion. A normal kary-otype carries a higher recurrence risk than does an abnor-mal karyotype, as this subset presumably is susceptible tomaternal etiologies.
Table 14–1.
Probability of spontaneous abortion.
Type of Study
Number of Previous Abortions
0 1 2 3+
Retrospective studies
Stevenson et al (1959) 16.3 19.2 26.2Warburton and Fraser
(1964)12.3 26.2 32.2 30.2
Leridon (1976) 15.2 22.0 35.3Poland et al (1977) 19.0 35.0 47.0Naylor and Warburton
(1978)11.0 20.3 29.2 37.0
Cohort studies
Shapiro et al (1970) 10.9 18.0Awan (1974) 10.4 22.1 27.4
Prospective studies
Boué at al (1975) 13.8Harger et al (1983) 17.4 29.2Fitzsimmons et al (1983) 31.3 45.7Regan (1988) 5.6 11.5 29.4 36.4
Percentage of women aborting in relation to number of previousabortions.Reproduced, with permission, from Regan L: Prospective study ofspontaneous abortion. In: Beard RW, Sharp F (editors).
Early Preg-nancy Loss: Mechanisms and Treatment.
Royal College of Obstetri-cians and Gynaecologists, 1988.

264 /
CHAPTER 14
Despite some controversy regarding the evaluationand management of recurrent abortion, the prognosisfollowing repeated losses is good, with most couples hav-ing an approximately 60% chance of a viable pregnancy.
Etiology & Treatment
Chromosomal abnormalities, uterine malformations, andantiphospholipid syndrome are the three generally ac-cepted etiologies of recurrent miscarriages. Currently evi-dence is insufficient to support routine evaluation of othercauses, including hormonal abnormalities, infection, sys-temic disease, environmental agents, and alloimmune fac-tors. Table 14–2 summarizes a diagnostic work-up andpossible therapies for recurrent abortion.
A. G
ENETIC
E
RRORS
Genetic errors associated with recurrent abortion includeparental structural chromosome abnormalities and recur-rent aneuploidy. Balanced rearrangements of parentalchromosomes are found in approximately 2–5% of cou-ples with repetitive abortions. Of these, balanced translo-cations are the most common. In couples who have anormal chromosome analysis, recurrent fetal aneuploidyhas been proposed as a distinct etiology.
A careful reproductive history and pedigree shouldbe taken for both partners, and karyotype screeningshould be performed. Couples with a history of otherreproductive problems, such as stillbirth or congenitalanomalies, are more likely to be affected by a balanced
structural chromosome abnormality. If the defect is pa-ternal, artificial insemination by a donor is available.For a maternal defect, a donor egg may be fertilized bythe husband’s sperm. Preimplantation diagnosis is alsoan option.
B. U
TERINE
A
BNORMALITIES
Anatomic abnormalities were the first described causesof habitual abortion and account for up to 15% of re-current pregnancy losses. Defects include congenitaluterine anomalies, cervical incompetence, submucousleiomyomas, abnormalities due to DES exposure inutero, and Asherman’s syndrome. A major difficultyin counseling affected couples is that approximately50% of women with uterine defects have no repro-ductive problem. Septate uteri account for the vastmajority of patients with uterine malformations andrecurrent pregnancy loss. Unicornuate and bicornu-ate uteri are less commonly associated. Submucous lei-omyomas are responsible for a much smaller percent-age of repeated losses. Generally, losses from anatomicabnormalities occur in the second trimester. Interfer-ence with implantation, lack of an adequate bloodsupply, and growth restriction are possible mecha-nisms for recurrent loss.
Diagnosis of uterine anatomic abnormalities usuallyis accomplished by hysterosalpingography or hysteros-copy. Treatment is primarily surgical, with reportedsuccess rates of 70–85% after surgical correction.
Table 14–2.
Diagnosis and treatment of recurrent abortion.
Cause Diagnosis Treatment
Genetic error Obtain a 3-generation pedigree and karyotype of both parents and any previously aborted mate-rial.
Artificial insemination by donor, embryo transfer, preimplantation diagnosis, or prenatal testing on subsequent conceptions.
Anatomic abnormalities of reproductive tract
Perform hysterosalpingogram or hysteroscopy. Uterine operation: hysteroscopic resection, myo-mectomy. Cervical cerclage (abdominal or vagi-nal), reconstruction of cervical isthmus.
Hormonal abnormalities
Perform laboratory studies for T
4
and TSH, serum progesterone or endometrial biopsy during luteal phase, and consider glucose tolerance test.
Thyroid replacement, progesterone or clomiphene citrate, diabetic diet and/or insulin, as indicated.
Infection Obtain cervical cultures for
Chlamydia
and gon-orrhea, and consider cultures for
Mycoplasma
and
Ureaplasma.
Approriate antibiotics.
Autoimmune disease Evaluate blood pressure and kidney function, check for lupus anticoagulant and anticardio-lipin antibody.
Low-dose aspirin and heparin.
Exogenous agents Patient history and/or drug screen. Discourage smoking, alcohol, and recreational drug use.
Immunologic factors Testing not readily available. Treatment under investigation.

EARLY PREGNANCY RISKS
/ 265
Cervical incompetence may be due to congenitalabnormalities (eg, DES exposure), trauma from a vig-orous D&C or cone biopsy, and/or possibly hor-monal influences. It classically presents in mid-secondor early third trimester with rapid, painless cervical di-latation. If other causes of recurrent losses are ex-cluded and the presumed etiology is incompetent cer-vix, a cervical cerclage is recommended between 12and 14 weeks’ gestation. Success rates with cerclageare 85–90%. Complications include risks from anesthe-sia, bleeding, infection, rupture of membranes, andmiscarriage. Contraindications to cerclage placementinclude bleeding of unknown etiology, infection, la-bor, ruptured membranes, and congenital anomalies.
C. H
ORMONAL
C
AUSES
Possible hormonal causes of habitual abortion includehypothyroidism and hyperthyroidism, progesterone in-sufficiency, and uncontrolled diabetes mellitus.
Progesterone deficiency or luteal phase defect(LPD) is a controversial etiology of habitual abortion.A defective endometrium resulting in faulty implanta-tion is the proposed mechanism. Inadequate hor-monal support of the embryo may also be involved.The diagnosis usually is made by luteal phase endome-trial biopsies, which attempt to identify a lag in en-dometrial development when compared to menstrualage. Critics of the diagnosis of LPD note intraobserverand interobserver variations in biopsy results, the pres-ence of LPD in normal women, and the inconsistentoccurrence in women affected by LPD. Furthermore,controlled studies demonstrating an improvement inpregnancy outcome with progesterone treatment arelacking. For these reasons, many experts are skepticalabout the importance of LPD as an etiology of recur-rent pregnancy loss.
D. I
NFECTION
Infectious agents that have been implicated in repetitivelosses include
Mycoplasma hominis, Ureaplasma urealyti-cum, Toxoplasma gondii, C trachomatis, T pallidum,Borrelia burgdorferi, N gonorrhoeae, S agalactiae, Lmonocytogenes,
herpes simplex, and cytomegalovirus. Al-though these agents have been identified in early losses,a causal relationship has not been demonstrated.
E. S
YSTEMIC
D
ISEASE
Systemic causes of recurrent abortion include uncontrolleddiabetes, uncontrolled thyroid disease, and collagen vascu-lar disease. The incidence of systemic disease as a cause ofhabitual abortion is unknown but probably is low. Fur-thermore, in patients without risk factors, asymptomaticdisease is an unlikely culprit, precluding routine screening.Therapy involves treatment of the specific disease.
F. I
MMUNOLOGIC
F
ACTORS
Antiphospholipid antibodies (lupus anticoagulant andanticardiolipin antibodies) may damage platelets andvascular endothelium, resulting in thrombosis. This mayaccount for the relationship to miscarriage when foundin combination with clinical features of antiphospho-lipid syndrome. Low-dose aspirin and/or heparin arebeneficial in this situation.
Compared to women who carry a pregnancy toterm, women who are habitual aborters share moreHLAs with their partners and have blunted responsesto paternal antigen with lower levels of blocking anti-bodies or antileukocytotoxic antibodies. The maternalimmunologic response may not be as effective in pro-tecting the pregnancy, resulting in pregnancy loss.
Diagnostic tests for immunologic abnormalities areavailable in few centers. The efficacy of leukocyte im-munotherapy is unknown, and treatment such as pater-nal leukocyte immunization is still experimental.
In up to 50% of women with recurrent abortion, adefinitive cause may not be found. However, althoughthe loss rate may be higher than that in the general pop-ulation, the majority of these women will have a suc-cessful pregnancy in their reproductive lifetime.
SEPTIC ABORTION
General Considerations
Septic abortion is manifested by fever, malodorous vag-inal discharge, pelvic and abdominal pain, and cervicalmotion tenderness. Peritonitis and sepsis may be seen.Trauma to the cervix or upper vagina may be recog-nized if there has been a criminal abortion.
A complete blood count, urinalysis, endometrial cul-tures, blood cultures, chest x-ray, and abdominal x-rayto rule out uterine perforation should be obtained. Ul-trasound may be helpful in ruling out retained productsof conception.
Treatment
Treatment of septic abortion involves hospitalizationand intravenous antibiotic therapy. Selection of antibi-otic agents should provide for both anaerobic and aer-obic coverage. A D&C should be performed, and ahysterectomy may be necessary if the infection doesnot respond to treatment.
ECTOPIC PREGNANCY
In ectopic pregnancy, a fertilized ovum implants in anarea other than the endometrial lining of the uterus(Fig 14–7). More than 95% of extrauterine pregnan-cies occur in the fallopian tube.

266 /
CHAPTER 14
The incidence of ectopic pregnancy has increasedfrom 4.5 in 1000 in 1970 to 19.7 in 1000 in 1992.This may be due, at least in part, to a higher inci-dence of salpingitis, an increase in ovulation induc-tion and assisted reproductive technology, and moretubal sterilizations.
Ectopic pregnancy is a significant cause of maternalmorbidity and mortality, as well as fetal loss. It is theleading cause of pregnancy-related death in the first tri-mester and accounts for 9% of all pregnancy-relateddeaths. The development of sensitive
β
-hCG assays,along with the increasing use of ultrasound and laparos-copy, has allowed for earlier diagnosis of ectopic preg-nancy. This has resulted in a decrease in both maternalmorbidity and mortality.
Classification & Incidence
Ectopic pregnancy can be classified as follows (Fig 14–7).
1. Tubal (> 95%)—
Includes ampullary (55%),isthmic (25%), fimbrial (17%), and interstitial (2%).
2. Other (< 5%)—
Includes cervical, ovarian, andabdominal (primary abdominal pregnancies have beenreported, but most abdominal pregnancies are secon-dary pregnancies, from tubal abortion or rupture andsubsequent implantation in the bowel, omentum, ormesentery). Cesarean delivery scar pregnancy is becom-
ing an increasingly recognized clinical entity, with itsincidence presumably paralleling a rise in cesarean sec-tion rates.
3. Intraligamentous4. Heterotopic pregnancy—
An ectopic pregnancyoccurs in combination with an intrauterine pregnancyin 1 in 15,000–40,000 spontaneous pregnancies and inup to 1% of patients undergoing in vitro fertilization.
5. Bilateral ectopic—
These pregnancies have occa-sionally been reported.
Etiology
The etiology of ectopic pregnancy is not well under-stood. However, several risk factors have been found tobe associated with ectopic pregnancy (Table 14–3).
A. T
UBAL
F
ACTORS
Ectopic pregnancy is 5–10 times more common inwomen who have had salpingitis. In women with ec-topic pregnancies, up to 50% will have had salpingitispreviously, and in most of these patients, the unin-volved tube is also abnormal. Other tubal factors thatinterfere with the progress of the fertilized ovum in-clude adherent folds of tubal lumen due to salpingitisisthmica nodosa, developmental abnormalities of thetube or abnormal tubal anatomy due to DES exposurein utero, previous tubal surgery including tubal ligationwith a 16–50% ectopic pregnancy rate if pregnancy oc-
Figure 14–7.
Sites of ectopic pregnancies.
(Adapted, with permission, from Benson RC:
Handbook of Ob-stetrics & Gynecology,
8th ed. Lange, 1983.)
Abdominal cavity(abdominal pregnancy)
Intraligamentous
Ampullary (55%)
Interstitial(2%)
Ovarian
Cervical
Fimbrial (17%)
Isthmic with tubal rupture
(25%)
Table 14–3.
Risk factors for ectopic pregnancy.
Risk Factor Odds Ratio
1
High risk
Tubal surgery 21.0Sterilization 9.3Previous ectopic pregnancy 8.3In utero exposure to diethylstilbestrol 5.6Use of IUD 4.2–45.0Documented tubal pathology 3.8–21.0
Moderate risk
Infertility 2.5–21.0Previous genital infections 2.5–3.7Multiple sexual partners 2.1
Slight risk
Previous pelvic/abdominal surgery 0.9–3.8Cigarette smoking 2.3–2.5Vaginal douching 1.1–3.1Early age at first intercourse (< 18 years) 1.6
1
Single values indicate common odds ratio from homogeneousstudies; point estimates indicate range of values from heteroge-neous studies. Reproduced, with permission, from Pisarska MD,Carson SA, Buster JE: Ectopic pregnancy. Lancet 1998;351:1115.

EARLY PREGNANCY RISKS
/ 267
curs after tubal ligation, conservative treatment of anunruptured ectopic with a recurrent ectopic rate of 4–16%, and tubal anastomosis with a 4% ectopic rate.Adhesions from infection or previous abdominal sur-gery, endometriosis, and even leiomyomas have beenassociated with ectopic pregnancy. Most of these abnor-malities are bilateral and irreversible.
B. Z
YGOTE ABNORMALITIES
A variety of zygote abnormalities have been reported inectopic pregnancy, including chromosomal abnormali-ties, gross malformations, and neural tube defects. Intheory, these abnormal pre-embryos are more likely toresult in abnormal or ectopic implantation.
C. OVARIAN FACTORS
Ovarian factors that may result in the development ofan ectopic pregnancy are fertilization of an unextrudedovum, transmigration of the ovum into the contralat-eral tube with subsequent delayed and faulty implanta-tion, and postmidcycle ovulation and fertilization.
D. EXOGENOUS HORMONES
Abnormal hormonal stimulation and/or exogenous hor-mones may play a role in ectopic gestation. For example,4–6% of pregnancies occurring in women taking proges-tin-only oral contraceptives are ectopic. This may be dueto progesterone’s smooth muscle relaxant effects and sub-sequent “ovum trapping.” Patients with DES exposure arealso at risk, as are patients undergoing ovulation induction.
E. OTHER FACTORS
Intrauterine device (IUD) users are at risk for ectopicpregnancy if pregnancy occurs, although the risk ofectopic pregnancy is still lower than if no contraceptivemethod is used. Whether the IUD prevents intrauterinebut not ectopic pregnancy or whether an associated sal-pingitis is responsible for this increased risk is un-clear. Smoking and increasing age are also associatedwith ectopic pregnancy. Multiple previous electiveabortions are also believed to be a risk factor for ec-topic pregnancy, as postabortal infection may lead tosalpingitis.
Time of Rupture
Rupture usually is spontaneous. Isthmic pregnanciestend to rupture earliest, at 6 to 8 weeks’ gestation, be-cause of the small diameter of this portion of the tube.Ampullary pregnancies rupture later, generally at 8–12weeks. Interstitial pregnancies are the last to rupture,usually at 12–16 weeks, as the myometrium allowsmore room to grow than the tubal wall. Interstitial rup-ture is quite dangerous because its proximity to uterineand ovarian vessels can result in massive hemorrhage.
After rupture, the conceptus may be resorbed orremain as a mass in the abdominal cavity or cul-de-sac. Rarely, if not damaged during rupture, it mayimplant elsewhere in the abdominal cavity and con-tinue to grow.
Clinical Findings
No specific symptoms or signs are pathognomonic forectopic pregnancy, and many disorders can present sim-ilarly. Normal pregnancy, threatened or incompleteabortion, rupture of an ovarian cyst, ovarian torsion,gastroenteritis, and appendicitis can all be confusedwith ectopic pregnancy. Because early diagnosis is cru-cial, a high index of suspicion should be maintainedwhen any pregnant woman in the first trimester pre-sents with bleeding and/or abdominal pain. Fifteen totwenty percent of ectopic gestations will present as sur-gical emergencies.
A. SYMPTOMS
The following symptoms may assist in the diagnosis ofectopic pregnancy.
1. Pain—Pelvic or abdominal pain is present in closeto 100% of cases. Pain can be unilateral or bilateral, lo-calized or generalized. The presence of subdiaphrag-matic or shoulder pain is more variable, depending onthe amount of intra-abdominal bleeding.2. Bleeding—Abnormal uterine bleeding, usually spot-
ting, occurs in roughly 75% of cases and representsdecidual sloughing. A decidua cast is passed in 5–10%of ectopic pregnancies and may be mistaken for prod-ucts of conception.3. Amenorrhea—Secondary amenorrhea is variable.
Approximately half of women with ectopic pregnancieshave some spotting at the time of their expected mensesand thus do not realize they are pregnant.4. Syncope—Dizziness, lightheadedness, and/or syn-
cope is present in one-third to one-half of cases andrepresent advanced stages of intra-abdominal bleeding.
B. SIGNS
On examination, the following signs are important inthe diagnosis of ectopic gestation.1. Tenderness—Diffuse or localized abdominal ten-
derness is present in over 80% of ectopic pregnancies.Adnexal and/or cervical motion tenderness is present inover 75% of cases.2. Adnexal mass—A unilateral adnexal mass is pal-
pated in one-third to one-half of patients. Occasionally,a cul-de-sac mass is present. The patient’s discomfortmay preclude an adequate examination, and effortshould be made to avoid an iatrogenic tubal rupturefrom an overzealous assessment.

268 / CHAPTER 14
3. Uterine changes—The uterus may undergo typi-cal changes of pregnancy, including softening and aslight increase in size.4. Hemodynamic instability—Vital signs will reflect
hemodynamic status of patients with tubal rupture andmassive intra-abdominal hemorrhage.
Laboratory Findings
Hematocrit: The hematocrit will vary depending onthe patient population and the degree, if any, of intra-abdominal bleeding.
β-hCG: The qualitative serum or urine β-hCGassay is positive in virtually 100% of ectopic pregnan-cies. The value of this test is limited, however, becausea positive result does not help to elicit the location ofthe pregnancy. More helpful is a quantitative β-hCGvalue that, in conjunction with transvaginal ultra-sound, can usually make the diagnosis. In an unclearclinical picture, serial titers can be followed that, inthe face of a normal pregnancy, should double every 2days. Two-thirds of ectopic pregnancies have abnor-mally rising values, whereas the remaining third showa normal progression.
Special Examinations
Several special procedures are helpful in diagnosing ec-topic pregnancy.
1. Ultrasound—Ultrasound is useful in evaluatingpatients at risk for ectopic pregnancy, namely, by doc-umenting the presence or absence of an intrauterinepregnancy. β-hCG titers and ultrasound complementeach another in detecting ectopic pregnancy and haveled to earlier detection with a subsequent decrease inadverse outcome. By correlating β-hCG titers with ul-trasound findings, an ectopic pregnancy often can bedifferentiated from an intrauterine pregnancy. Fur-thermore, ultrasound can help distinguish a normal in-trauterine pregnancy from a blighted ovum, incompleteabortion, or complete abortion.
A normal intrauterine sac appears regular and welldefined on ultrasound. It has been described as a“double ring,” which represents the decidual liningand the amniotic sac. In ectopic pregnancy, ultra-sound may reveal only a thickened, decidualized en-dometrium. With more advanced ectopics, decidualsloughing with resultant intracavitary fluid or bloodmay create a so-called “pseudogestational sac,” a smalland irregular structure that may be confused with anintrauterine gestation.
An intrauterine sac should be visible by transvaginalultrasound when the β-hCG level is approximately1000 mIU/mL and by transabdominal ultrasound ap-proximately 1 week later, when the β-hCG level is
1800–3600 mIU/mL. Thus, when an empty uterinecavity is seen with a β-hCG titer above this threshold,an ectopic pregnancy is more likely.
The presence of an adnexal mass with an emptyuterus raises the suspicion for an ectopic pregnancy,especially if the β-hCG titers are above the discrimi-natory zone. Although direct visualization of an ad-nexal gestational sac along with a yolk sac or embryosecures the diagnosis, it is more likely to detect a “tu-bal ring” or complex mass adjacent to, but separatefrom, both the uterus and ovary. If rupture has oc-curred, a dilated fallopian tube with fluid in the cul-de-sac may be visualized. Ultrasound is increasinglybeing relied upon to differentiate several less commontypes of ectopic pregnancies. Both interstitial tubaland cesarean section scar pregnancies can masqueradeas intrauterine gestations because of their proximity tothe intrauterine cavity.
The most likely alternative diagnosis to an adnexalmass in early pregnancy is a corpus luteum cyst, whichcan rupture and bleed, thus contributing to a highlyconfusing clinical picture.2. Laparoscopy—The need for laparoscopy in the
diagnosis of ectopic pregnancy has declined with theincreasing use of ultrasound. However, it still is usefulin certain situations where a definitive diagnosis is diffi-cult, especially in the case of a desired, potentially viableintrauterine pregnancy when a D&C is contraindica-ted. Laparoscopy may also be used as definitive man-agement in early ectopic gestation.3. D&C—D&C may confirm or exclude intrauter-
ine pregnancy in the case of an undesired pregnancy.D&C may interrupt an intrauterine gestation andshould not be performed if the pregnancy is desired,unless the β-hCG titers have plateaued or fallen andthe pregnancy is definitely abnormal. When chorionicvilli are recovered, the diagnosis of an intrauterinepregnancy is confirmed. On the other hand, if onlydecidua is obtained on D&C, ectopic pregnancy ishighly likely.4. Laparotomy—Laparotomy is indicated when the
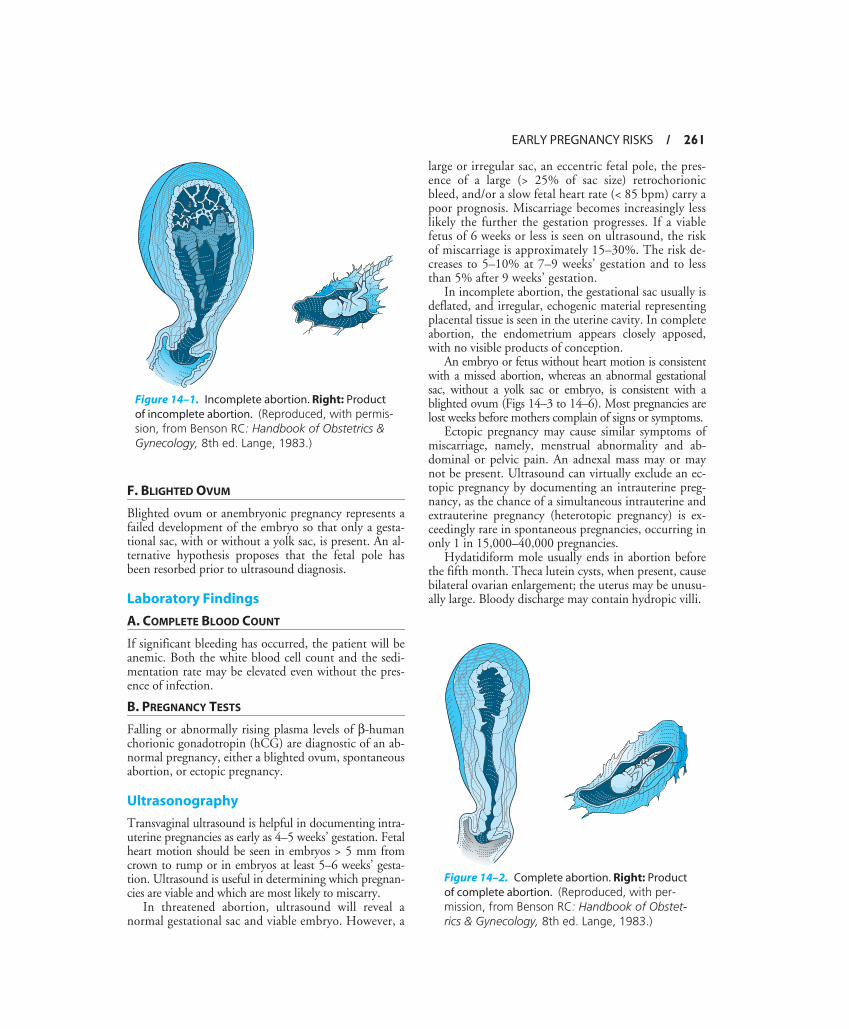
presumptive diagnosis of ectopic pregnancy in anunstable patient necessitates immediate surgery, orwhen definitive therapy is not possible by medical man-agement or laparoscopy.5. Culdocentesis—Culdocentesis, the transvaginal
passage of a needle into the posterior cul-de-sac in orderto determine whether free blood is present in the abdo-men (Fig 14–8), has largely been replaced by transvagi-nal ultrasound. 6. Magnetic resonance imaging—Magnetic reso-
nance imaging is a useful adjunct to ultrasound in caseswhere an unusual ectopic location is suspected. An accu-rate diagnosis of cervical, cesarean scar, or interstitial
EARLY PREGNANCY RISKS / 269
pregnancy urges conservative intervention withmethotrexate (MTX) in order to avoid the potentiallycatastrophic hemorrhage associated with surgical manage-ment of these sites.
Pathology
In tubal ectopic pregnancy, implantation typically oc-curs in the wall of the tube, in the connective tissuebeneath the serosa. There may be little or no decidualreaction and minimal defense against the permeatingtrophoblast. The trophoblast invades blood vessels,causing local hemorrhage. A hematoma in the subsero-sal space enlarges as pregnancy progresses. Progressivedistention of the tube eventually leads to rupture.
Vaginal bleeding is of uterine origin and is caused byendometrial involution and decidual sloughing. Atypi-cal changes in the endometrium may be suggestive ofectopic pregnancy. The Arias-Stella reaction consists ofhyperchromatic, hypertrophic, irregularly shaped nu-clei, and foamy, vacuolated cytoplasm. These changescan be seen in normal pregnancy and in miscarriageand therefore are not diagnostic of ectopic pregnancy.
Occasionally, endometrial tissue may be passed as a so-called decidual cast. Superficial secretory endometriumusually is present, but no trophoblastic cells are seen.
Prevention
Prevention of sexually transmitted disease, with earlyand vigorous treatment of cases that do occur, mayavoid tubal damage with subsequent ectopic pregnancy.Other risk factors for ectopic pregnancy are more diffi-cult to control. Early diagnosis of unruptured tubalpregnancy by maintaining a high index of suspicionand liberal use of β-hCG titers, ultrasound, and lap-
aroscopy will minimize potential problems of hemor-rhage, infertility, and extensive surgery.
Treatment
A. EXPECTANT MANAGEMENT
Because many ectopic pregnancies resolve spontane-ously, it may be reasonable to manage an asymptom-atic, compliant patient expectantly if β-hCG titers arelow (< 200 mIU/mL) or decreasing, and the risk of rup-ture is low.
B. MEDICAL MANAGEMENT
MTX, a folinic acid antagonist, has been shown to de-stroy proliferating trophoblast and may be effective inthe medical management of small, unruptured ectopicpregnancies in asymptomatic women. Exclusion criteriainclude a patient who is noncompliant or has com-pleted childbearing, peptic ulcer disease, immunodefi-ciency, pulmonary disease, liver disease, renal disease,blood dyscrasias, hemodynamic instability, free fluid inthe cul-de-sac plus pelvic pain, or known sensitivity toMTX. Relative contraindications include an adnexalmass ≥ 3.5 cm or an extrauterine gestation with fetalheart motion, because of the higher failure rate. In se-lect cases, approximately 90% of ectopics resolve, tak-ing on average just under 1 month. Protocols vary fromsingle to multiple injections, typically given systemi-cally. The dose of MTX depends on the patient’s bodysurface area, and nomograms are available for determin-ing the correct dose. Follow-up β-hCG levels, alongwith a complete blood count, serum creatinine, andserum aspartate transaminase, are obtained for compari-son with baseline values. β-hCG levels should decreaseby at least 15% between days 4 and 7 after MTX ad-
Figure 14–8. Culdocentesis.

270 / CHAPTER 14
ministration. Failure of MTX therapy is suggested by apersistent rise or plateau in β-hCG titer and can bemanaged by a second dose of MTX or surgery. A recur-rent episode of abdominal pain or enlargement of theadnexal mass during the first week of therapy may bepart of a normal response to successful MTX treatment.Vigilant observation should be the rule, and follow-upultrasound should be used liberally. Persistent andworsening pain in conjunction with a hemoperitoneumon ultrasound, and/or hemodynamic instability, man-dates immediate surgical intervention.
Available studies comparing MTX to traditional sur-gical management report similar subsequent tubal pat-ency and fertility rates. Arguments against its use includeits toxicity, namely, marrow suppression, dermatitis, andstomatitis, as well as potential for treatment failure andtubal rupture.
Chronic ectopics, with decreasing but persistent β-hCG titers, pose a management dilemma. Some will re-solve on their own, whereas others will require surgery.Unfortunately, at present it is impossible to predictwhich patients will fail expectant management.
C. SURGICAL TREATMENT
Once the mainstay of therapy for ectopic pregnancy,surgery is now mainly reserved for patients with contra-indications to medical management. The extent of sur-gery depends on the degree of damage to the uterus andadnexa. Preservation of the ovary should be attemptedif feasible. Conservative surgery (ie, preservation of thefallopian tube) may be indicated in the hemodynami-cally stable patient with an ampullary pregnancy whowishes to preserve fertility.
A linear salpingostomy may be performed with asmall (< 3 cm), intact ampullary pregnancy. The linearincision is allowed to heal by secondary intention, min-imizing recurrent ectopics as compared to salpingot-omy. Both methods yield similar subsequent pregnancyrates of 40–90%.
Depending on operator skill and comfort level,both of these procedures can be performed throughthe laparoscope, assuming the pregnancy is < 3 cm,unruptured, and easily accessible. With both salpin-gostomy and salpingotomy, a β-hCG titer should beobtained weekly after surgery to ensure adequate re-moval of trophoblast and rule out a persistent ectopic.In stable patients, laparoscopy is preferred over laparo-tomy because of the associated reduction in morbidityand cost.
“Milking” the pregnancy out of the distal end of thetube is often tempting but has been associated with per-sistent trophoblast and need for re-exploration, as wellas increased risks of recurrent ectopic pregnancy.
With an isthmic ectopic pregnancy, segmental resec-tion with subsequent anastomosis (usually at a later
date) is typically recommended. As opposed to ampul-lary ectopics, the muscularis is well developed, forcingthe pregnancy to grow in the lumen. More conservativetreatment, such as salpingostomy or salpingotomy,would likely cause scarring and compromise of the lu-men. Furthermore, a tubal fistula may result if the tubewere allowed to heal by secondary intention.
With fimbrial pregnancy, products of conceptionare often visible at the most distal end of the tube,which may be “plucked out.” As with ampullary ectop-ics, “milking” should be avoided.
Interstitial pregnancies pose a high surgical risk withthe potential for massive intra-abdominal bleeding.Most cases are managed with a cornual wedge resection,uterine reconstruction, and, sometimes, salpingectomyon the affected side. If extensive tissue damage ispresent or if the patient is unstable, a hysterectomy maybe needed. Likewise, cervical ectopics may be associatedwith massive vaginal bleeding with the potential forhysterectomy. Attempts at medical management withMTX should be considered for both.
Ovarian pregnancy requires oophorectomy andsometimes salpingectomy on the affected side. Abdomi-nal pregnancy involves delivery of the fetus (sometimesat term) with ligation of the umbilical cord close to theplacenta. The placenta is usually left in place to avoidhemorrhage following removal.
D. EMERGENCY TREATMENT
Immediate surgery is indicated when the diagnosis ofectopic pregnancy with hemorrhage is made. Bloodproducts should be available because transfusion isoften necessary. There is no place for conservative ther-apy in a hemodynamically unstable patient.
Rho (D) immunoglobulin should be given to anyRh-negative mother with the diagnosis of ectopic preg-nancy because sensitization may occur.
EXPOSURE TO FETOTOXIC AGENTSMany variations occur in the complex process ofhuman development. Although population heterogene-ity is based on such events, some deviations from theusual developmental process result in aberrations ofnormal structure and function. These adverse alter-ations have been scrutinized in an effort to determinetheir cause. The clinician investigating the effects of ex-posure to fetotoxic agents must consider whether thepatient is known to have reproductive risks, whetherthe patient has been exposed to fetotoxic agents duringpregnancy, and whether structural or functional abnor-malities are likely to develop in the fetus.
Many harmful agents are responsible for alteringthe biologic process of human development (eg, radia-tion, viruses, medications, and drugs). Aberrations

EARLY PREGNANCY RISKS / 271
that result from fetal exposure to harmful agents is es-pecially tragic because such exposure often is prevent-able. However, even the most careful investigationwill fail to reveal the cause in the majority of develop-mental handicaps.
Approximately 3–5% of newborns in the UnitedStates have abnormalities at birth that are seriousenough to require some form of treatment. Moreover,full recognition of malformations, anomalies, or de-fects may take years. Thus, estimates that as much as10% of the total population suffers from some struc-tural or functional developmental disability do not ap-pear unreasonable.
Evaluation
The timing of exposure is crucial, as fetal organs orstructures are most vulnerable to adverse influencesduring organogenesis. Table 14–4 lists some of the po-tential adverse effects related to the timing of fetotoxicexposure. The route of exposure, the length of expo-sure, and the total dose received during exposure mayalso influence the outcome of the pregnancy.
Evaluation of studies of potential toxic exposures isdifficult because of the large number of possible feto-toxic agents and interactive effects of certain agents, theretrospective nature of most studies, the difficulty evalu-ating damage, the presence or absence of influences thatmay alter the effects of an agent, and the presence or ab-sence of certain genotypes that might alter an individ-ual’s susceptibility. Therefore, specific criteria for recog-nizing teratogens in humans have been defined (Table14–5). Table 14–6 summarizes the known mechanismsof abnormal development and outlines a working hy-pothesis of the pathogenesis, common pathways, andfinal manifestations of abnormal development.
Counseling of parents should include review of theexposure history and discussion of the particular agentinvolved, as well as possible sequelae. In some cases, in-tervention may be possible. In other cases, if an abnor-mal pregnancy is found, the parents may elect to abortan affected fetus. Effective counseling should providethe best information available to assist the parents inwhat is always a very difficult decision.
Table 14–4. Potential adverse effects of fetotoxic exposure at selected stages of development.
Week Since Ovulation Potential Adverse Effect
1–8 Miscarriage, structural malformations
9–40 Central nervous system abnormalities, growth restrictions, neurobehavioral ab-normalities, reproductive effects
Table 14–5. Criteria used to recognize teratogens in humans.
Abrupt increase in the incidence of a particular defect or asso-ciation of defects
Known environmental change coincident with this increase.Known exposure to the environmental change early in preg-
nancy, yielding characteristically affected infants.Absence of other factors common to all pregnancies, yielding
infants with the characteristic defects.
Table 14–6. General principles of teratology.
Mechanisms MutationChromosome disruptionMitotic interferenceAltered nucleic acid integrity or
functionPrecursor or substrate deprivationAltered energy sourcesChanged membrane characteristicsAltered osmolar balanceEnzyme inhibition
Pathogenesis Excessive or reduced cell interactionsFailed cell interactionsReproduced biosynthesisImpeded morphogenetic movementMechanical disruption of tissues
Common pathways Too few cells or cell products to af-fect localized morphogenesis or functional maturation
Other imbalances in growth and dif-ferentiation
Final defects MalformationGrowth retardationFunctional disorderDeath

272 / CHAPTER 14
The United States Food and Drug Administration(FDA) standards for drug labeling with regard to ter-atogenicity are listed in Table 14–7.
REFERENCES
American College of Obstetricians and Gynecologists: Early Preg-nancy Loss. ACOG Technical Bulletin No. 212. AmericanCollege of Obstetricians and Gynecologists, 1995.
American College of Obstetricians and Gynecologists: Medical Man-agement of Tubal Pregnancy. ACOG Practice Bulletin No. 3.American College of Obstetricians and Gynecologists, 1998.
American College of Obstetricians and Gynecologists: Management ofRecurrent Early Pregnancy Loss. ACOG Practice Bulletin No. 24.American College of Obstetricians and Gynecologists, 2001.
Centers for Disease Control and Prevention: Current Trends Ec-topic Pregnancy—United States, 1990–1992. MMWR MorbMortal Wkly Rep 1995;44:46.
Levine D: Ectopic pregnancy. In: Callen PW (editor): Ultrasonog-raphy in Obstetrics and Gynecology, 4th ed. Saunders, 2000.
Nanda K, Peloggia A, Grimes D, Lopez L, Nanda G: Expectantcare versus surgical treatment for miscarriage. Cochrane Data-base Syst Rev 2006;Apr19:CD003518.
Pisarska MD, Carson SA, Buster JE: Ectopic pregnancy. Lancet1998;351:1115.
Regan L: Prospective study of spontaneous abortion. In: Beard RW,Sharp F (editors): Early Pregnancy Loss: Mechanisms and Treat-ment. Royal College of Obstetricians and Gynaecologists, 1988.
Seeber BE, Barnhart KT: Suspected ectopic pregnancy. Obstet Gy-necol 2006;107:399.
Tulandi T: New protocols for ectopic pregnancy. Contemp ObstetGynecol 1999;44:42.
Yao M, Tulandi T: Current status of surgical and nonsurgical man-agement of ectopic pregnancy. Fertil Steril 1997;67:421.
Table 14–7. Teratogenicity drug labeling now required by the FDA.1
Category A: Well-controlled human studies have not dis-closed any fetal risk.
Category B: Animal studies have not disclosed any fetal risk; or have suggested some risk not confirmed in controlled studies in women; or no adequate studies in women are available.
Category C: Animal studies have revealed adverse fetal ef-fects; no adequate controlled studies in women are avail-able.
Category D: Some fetal risk, but benefits may outweigh risk (eg, life-threatening illness, no safer effective drug).
Category X: Fetal abnormalities in animal and human stud-ies; risk not outweighed by benefit. Contraindicated in pregnancy.
1The FDA has established 5 categories of drugs based on their po-tential for causing birth defects in infants born to women whouse them during pregnancy. By law, the label must provide avail-able information on teratogenicity.