ENVIRONMENTAL PROBLEMS Land pollution Water pollution Air pollution.
Upload
alexis-knightCategory
view
224download
1
SILICOSIS
S I L I C O S I SBy Fardad Ahmadzadeh MD ; Occupational and environmental medicine specialist


•Silicon dioxide, or silica, is the earth’s most abundant mineral.
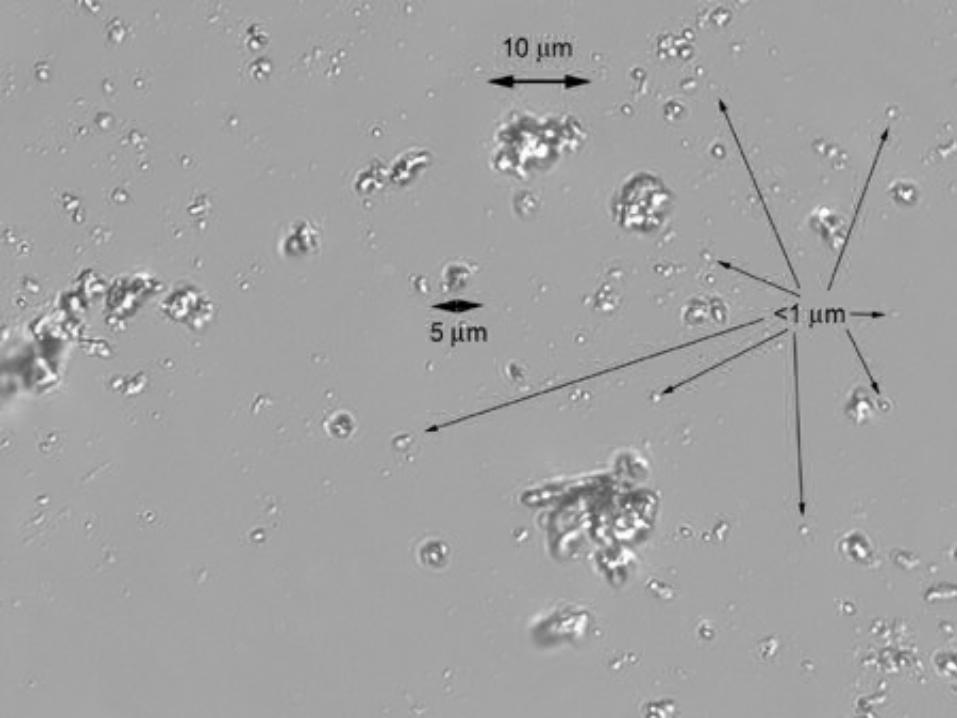
•Silicosis occur when workers are consistently exposed to silica particles of respirable size (0.5–5.0 μm in diameter) at levels exceeding those recognized to be safe.
•Between 1968 and 1990 there were 13,744 deaths in the US where the death certificate mentioned silicosis.
OSHA permissible exposure limit (PEL) is 100 μg/m3 for an 8-hour work exposure.
Bronchitis, a well-recognized effect of chronic dust inhalation, can occur with silica dust inhalation.
Silica exposure can be associated with: 1.Autoimmune diseases :
2.Nephropathy 3.Tuberculosis 4.lung cancer
Scleroderma
SLE
RA
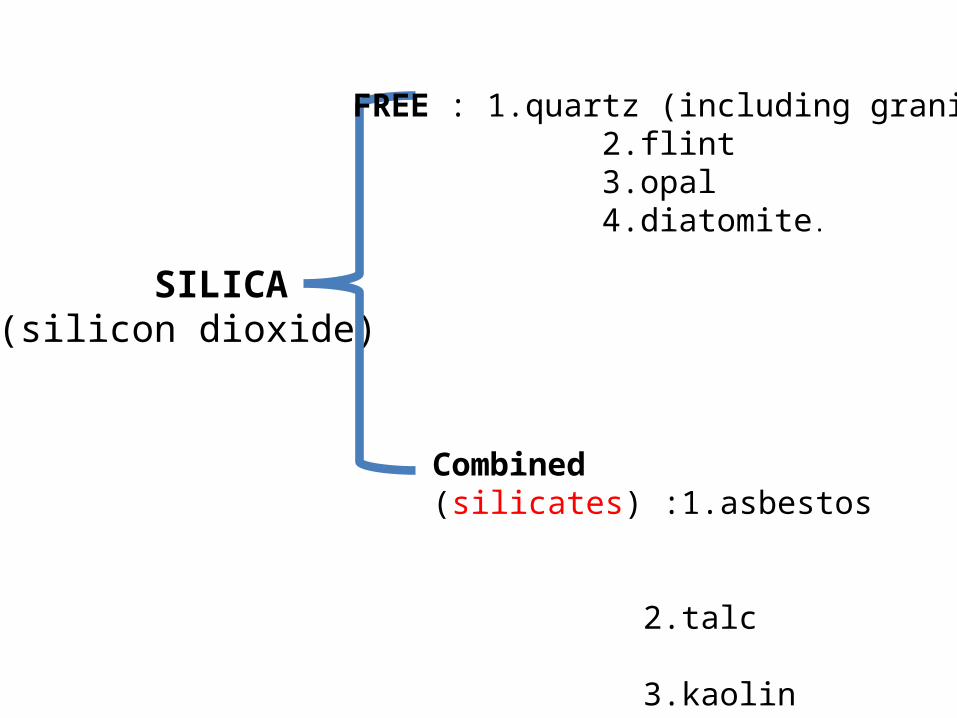
SILICA (silicon dioxide)
FREE : 1.quartz (including granite) 2.flint 3.opal 4.diatomite.
Combined (silicates) :1.asbestos 2.talc 3.kaolin

Asbestos Mg3Si2O5(OH)4


Kaolin : Al2Si2O5(OH)4
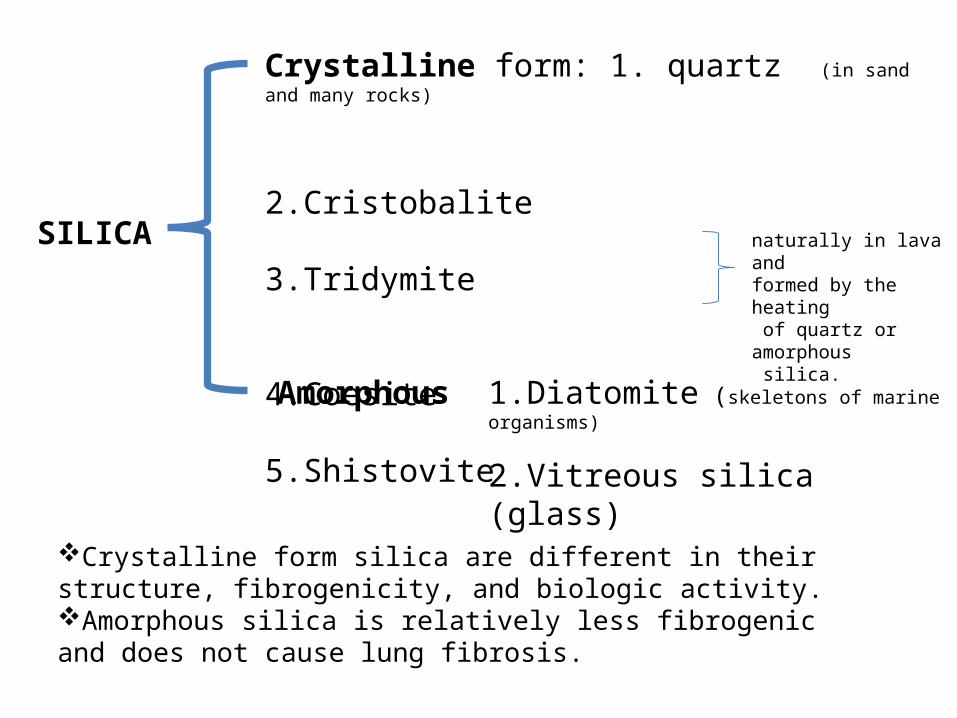
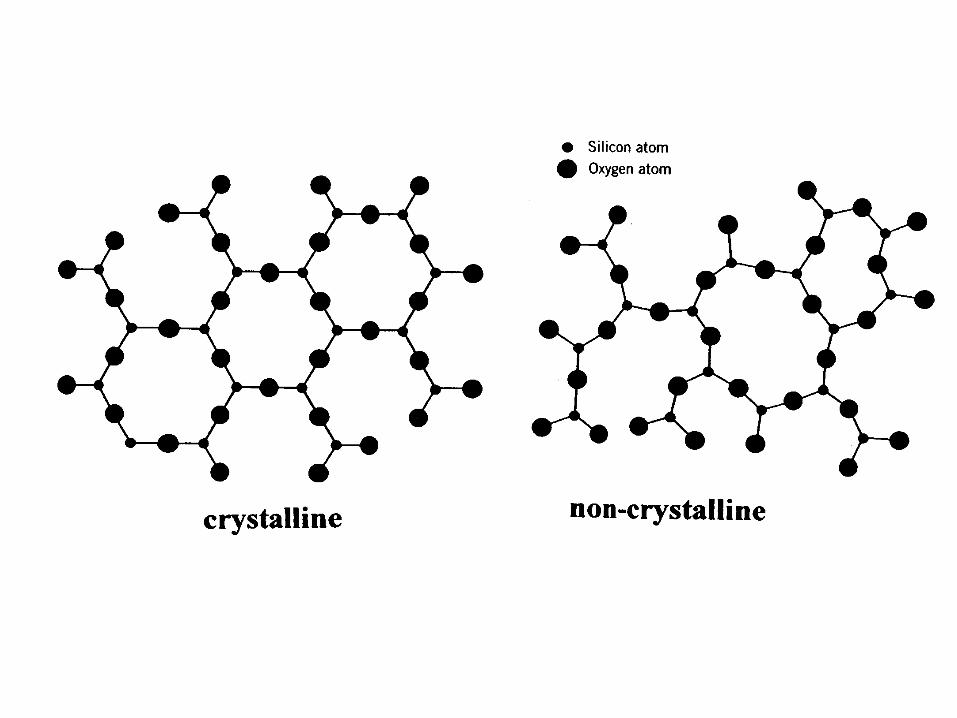
SILICA
Crystalline form: 1. quartz (in sand and many rocks)
2.Cristobalite 3.Tridymite
4.Coesite 5.Shistovite
naturally in lava andformed by the heating of quartz or amorphous silica.
Amorphous
Crystalline form silica are different in their structure, fibrogenicity, and biologic activity.Amorphous silica is relatively less fibrogenic and does not cause lung fibrosis.
1.Diatomite (skeletons of marine organisms)
2.Vitreous silica (glass)


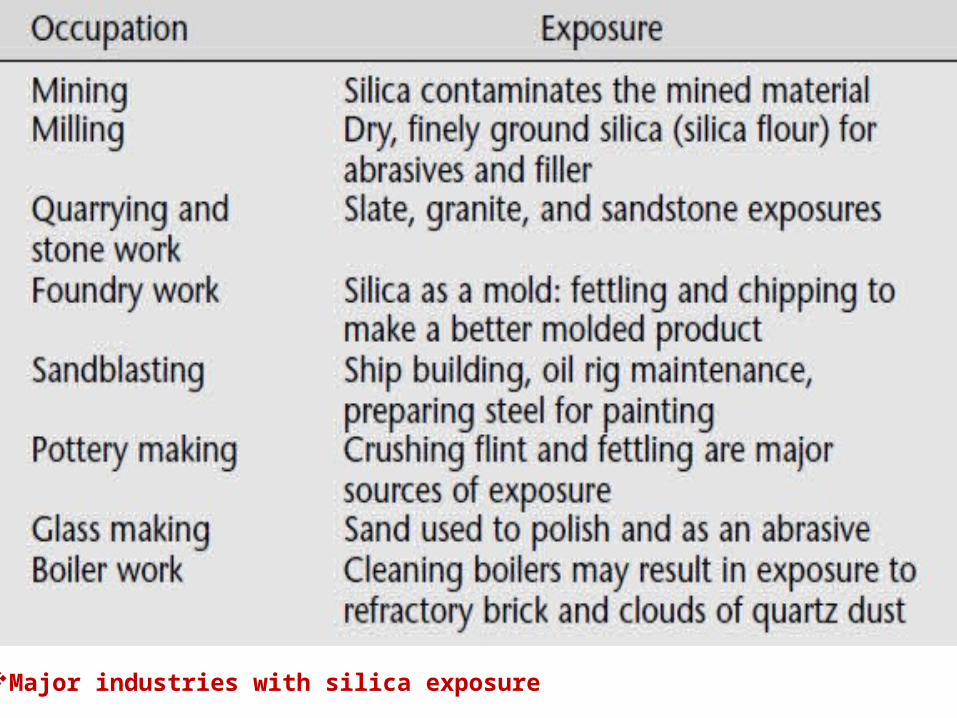
Major industries with silica exposure





silicosis, is caused by the inhalation of respirablesize silica particles, and can be categorized by recognizable findings on the chest radiograph.
Silicosis generally requires prolonged exposure to respirable crystalline free silica at levels exceeding government standards.
Some workers developing much more severe disease than others.
Most forms of silicosis develop slowly. Usually 10 to 30 years are required from the beginning of exposure to the onset of clinical manifestations.
Most important factors include:
1. Silica dust concentration in the air,2. Duration of dust exposure, 3. Crystalline structure of the silica 4. Percent of free silica,5. Particle size.
host factors such as genetics, smoking, and underlying diseases may play a part in the development of silicosis.
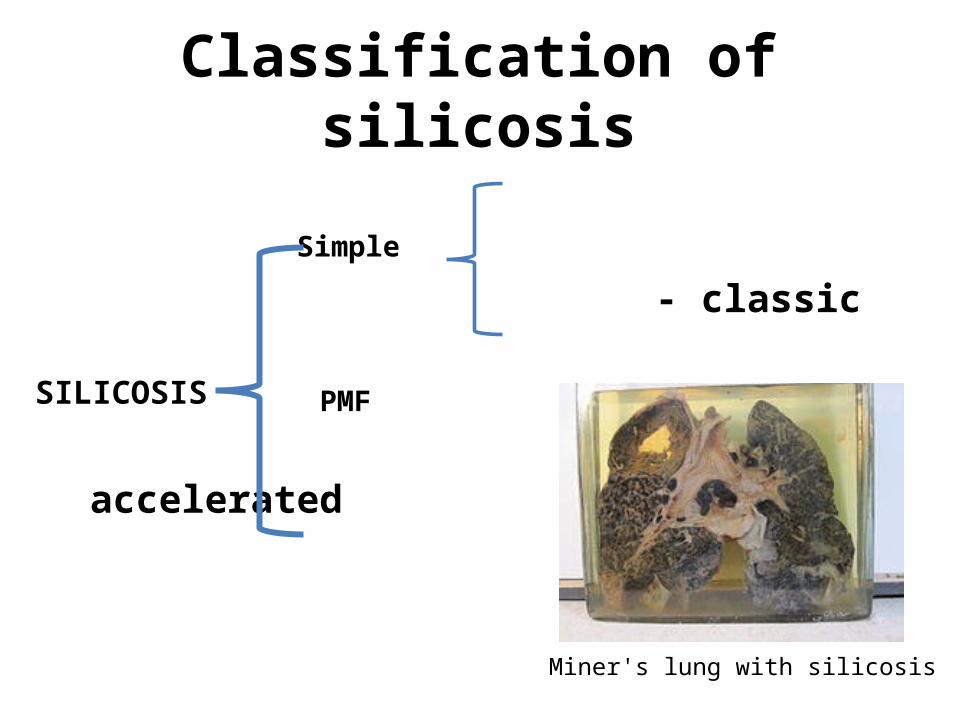
Classification of silicosis
Simple
- classic PMF
- accelerated
- acute
SILICOSIS
Miner's lung with silicosis

CLASSIC SILICOSIS
Ranging from simple silicosis (presenting as nodular pulmonary fibrosis with or without symptoms) to progressive massive fibrosis (severely disabling restrictive lung disease).
These features usually develop slowly and frequently require a working lifetime to develop.
in a small percentage of workers, the radiographic features of simple silicosis lead to progressive massive fibrosis in less than 10 years (accelerated Silicosis )
Development of these radiographic features so soon after beginning exposure to silica means that progre- ssion of disease and severe respiratory impairment is very likely to occur.
CLASSIC SILICOSIS

Diagnosis
1.History of silica exposure sufficient to cause illness.2. Chest radiograph features consistent with silicosis.3. Absence of other illnesses that mimic silicosis.
Other chest illnesses : rheumatoid nodules, tumor, infection, other pneumoconiosis, or sarcoidosis
There are three requirements for the diagnosis of silicosis:
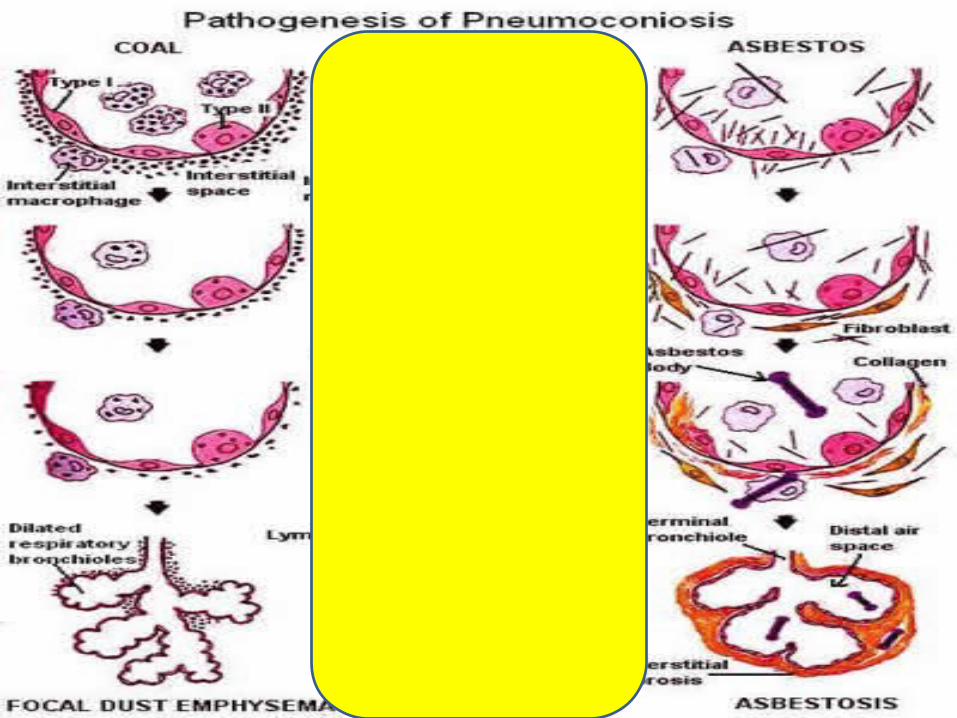
Pathogenesis and histologic features of classic silicosis
Particles less than 5.0 μm in diameter are depo sited in the alveoli, most often in the upper lung zones.Particles less than 1.0 μm in diameter are believed to be the most fibrogenic and most able to penetrate into the interstitium.Inhaled silica particles interact with alveolar macrophages and other lung cells in a complex cascade of events resulting in lung inflammation, fibrosis, and tissue remodeling forming silicotic nodules.
This nodule usually forms near the small bronchioles.
In some workers with relatively low silica exposure, inhaled silica is cleared from the lung and deposited inthe lymph nodes and presentation of calcified regional hilar lymph nodes on the chest radiograph maybe noted without an extensive background of smallrounded opacities.
In microscopic view nodules are onion skin-like pattern
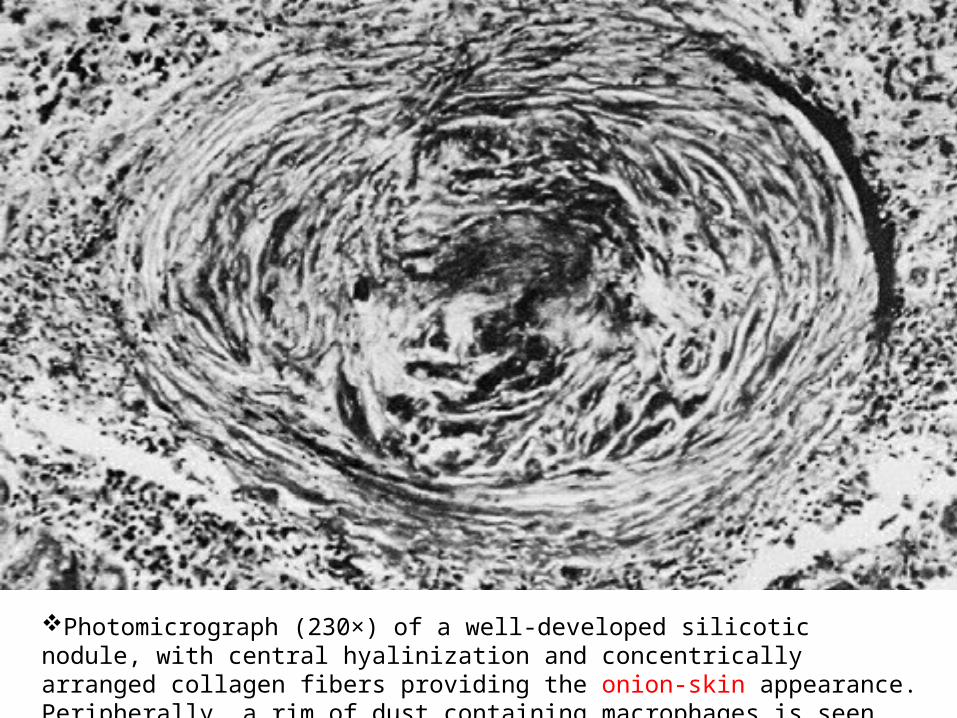
Photomicrograph (230×) of a well-developed silicotic nodule, with central hyalinization and concentrically arranged collagen fibers providing the onion-skin appearance. Peripherally, a rim of dust containing macrophages is seen.
Simple silicosisUsually do not have chest symptoms.
Some, however, report a chronic productive cough, a feature likely similar to industrial bronchitis from dust exposure.
Physical examination of the chest usually is unrem- arkable; audible coarse sounds are the result of coexisting bronchitis.
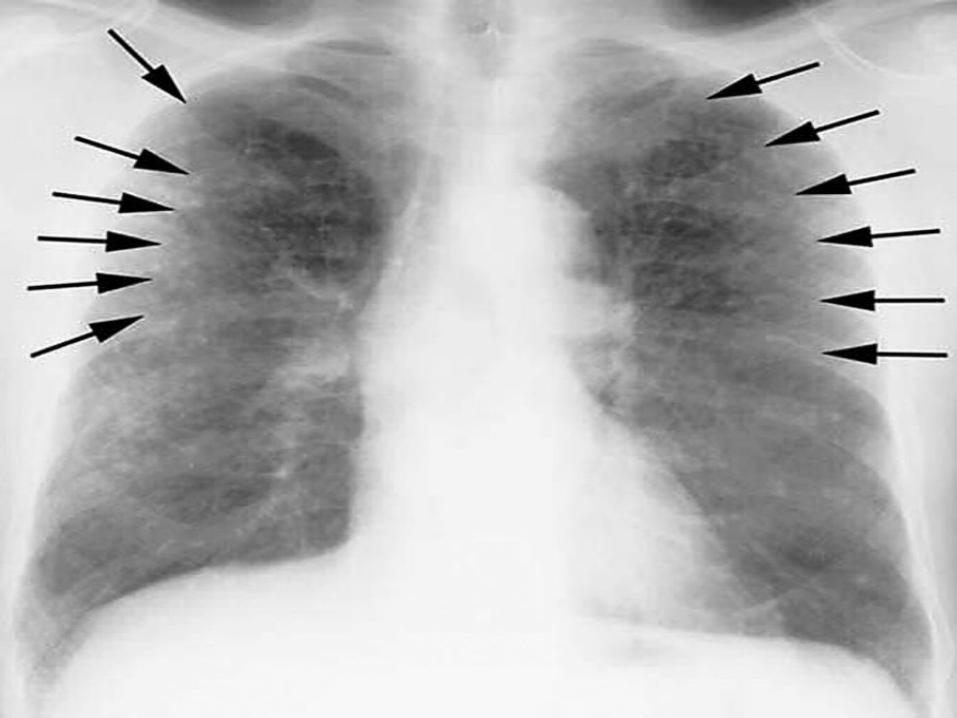
Roentgenographically, simple silicosis typically appears as an upper zone distribution of rounded opacities less than 1 cm in diameter.
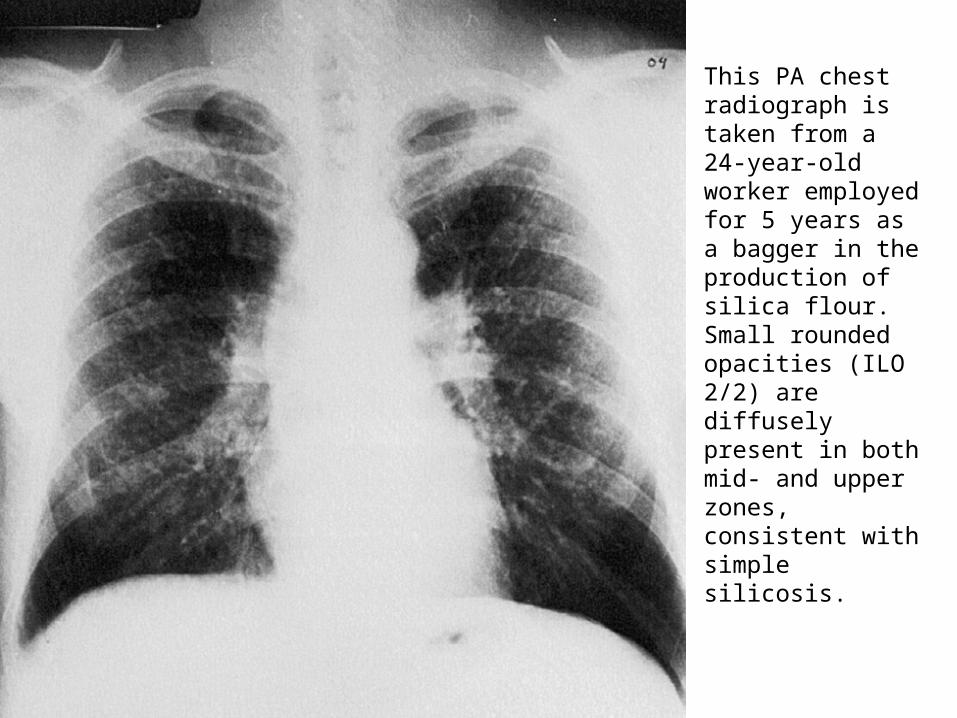
This PA chest radiograph is taken from a 24-year-oldworker employed for 5 years as a bagger in the production of silica flour. Small rounded opacities (ILO 2/2) are diffusely present in both mid- and upper zones, consistent with simple silicosis.

Hilar lymph nodes are often enlarged with a distinctive peripheral calcification, described as eggshell calcification.


High-resolution CT scans have been to shown to have a good correlation with the nodular findings of silicosis on the chest radiograph, and a better description of the extent of emphysema compared to the chest radiograph.
Correlation between lung function tests and the chest radiograph and CT scan is variable.
PFT in simple silicosis may be a trend for values to progress toward airways obstruction.
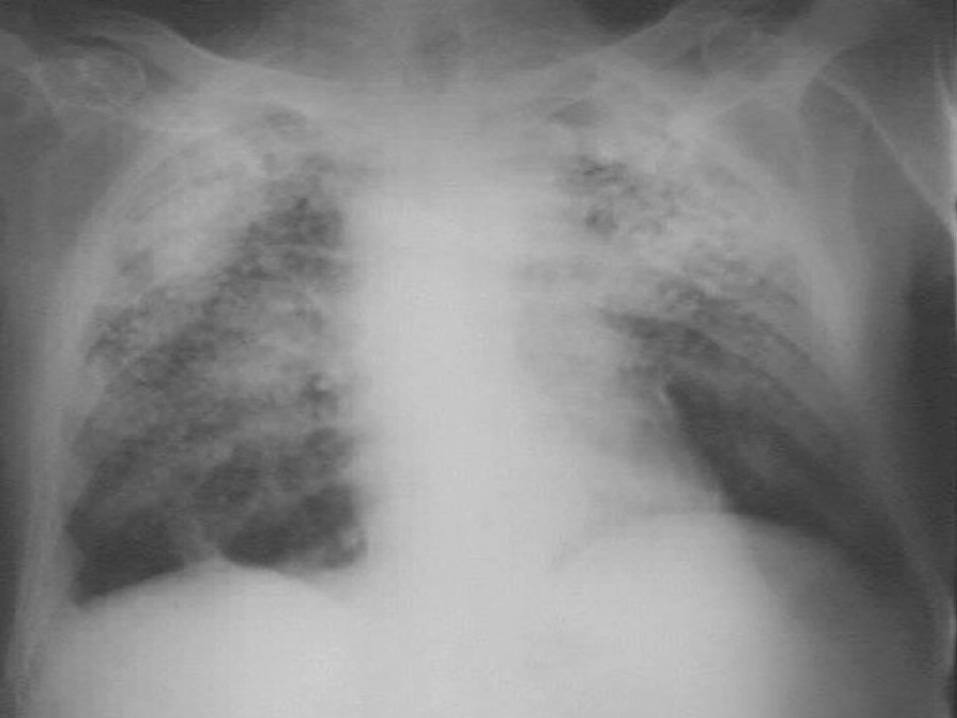
Progressive massive fibrosis
Is the result of the conglomeration of small rounded opacities.
It has been traditionally recognized that progressive massive fibrosis develops on a
background of advanced simple silicosis.
However, not all PMF patients have an advanced degree of simple coal workers’ pneumoconiosis
symptoms
The respiratory symptoms can be variable; ranging from only a chronic productive cough
to exertional dyspnea and, in some persons, ultimately to respiratory failure.
Physical examinationPhysical examination demonstrates
decreased breath sounds, and if the illness is extensive, signs of cor-pulmonale and impending respiratory failure.
Crackles usually are not audible, and clubbing, if present, is attributable to another cause.
CXR Nodules >1 cm in diameter on a background of
small rounded opacities characteristic of simple silicosis:
- begins peripherally and migrates centrally - prominently in the upper lobes .
As these fibrous masses in the upper lobe progressively enlarge, the hila are retracted upward and the lower zones become hyperinflated and appear emphysematous




PFTInitially demonstrate a decrease incompli- ance, followed by decreases in lung
volumes and diffusing capacity.
If bronchial distortion and lower zone hyper- inflation are present, the forced expiratory time is likely to be prolonged and airflow obstruction is measurable.
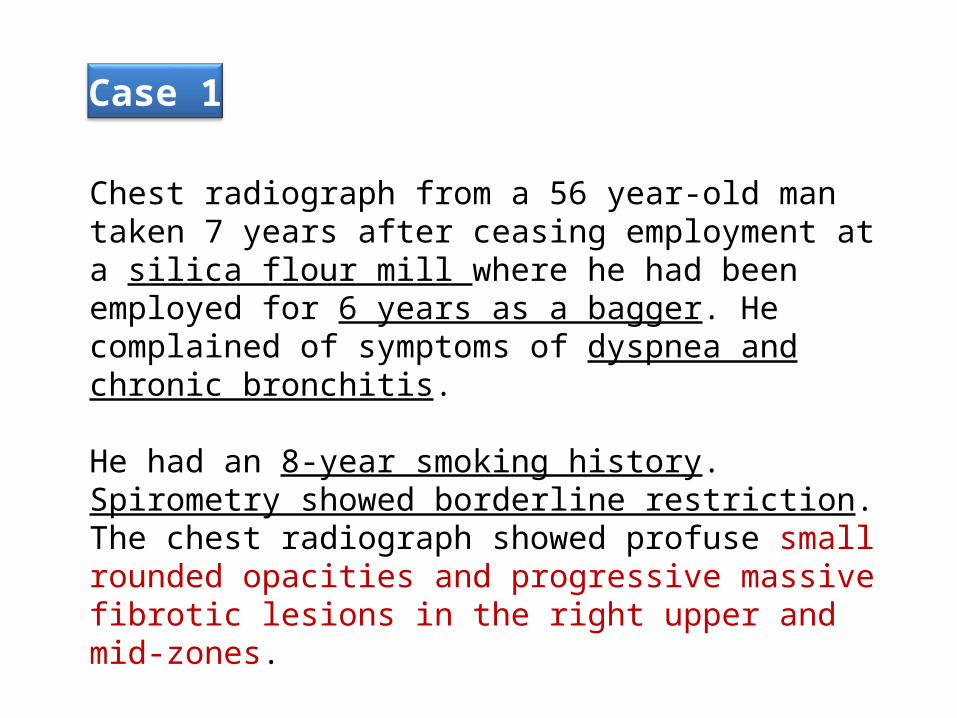
Chest radiograph from a 56 year-old man taken 7 years after ceasing employment at a silica flour mill where he had been employed for 6 years as a bagger. He complained of symptoms of dyspnea and chronic bronchitis.
He had an 8-year smoking history. Spirometry showed borderline restriction. The chest radiograph showed profuse small rounded opacities and progressive massive fibrotic lesions in the right upper and mid-zones.
Case 1
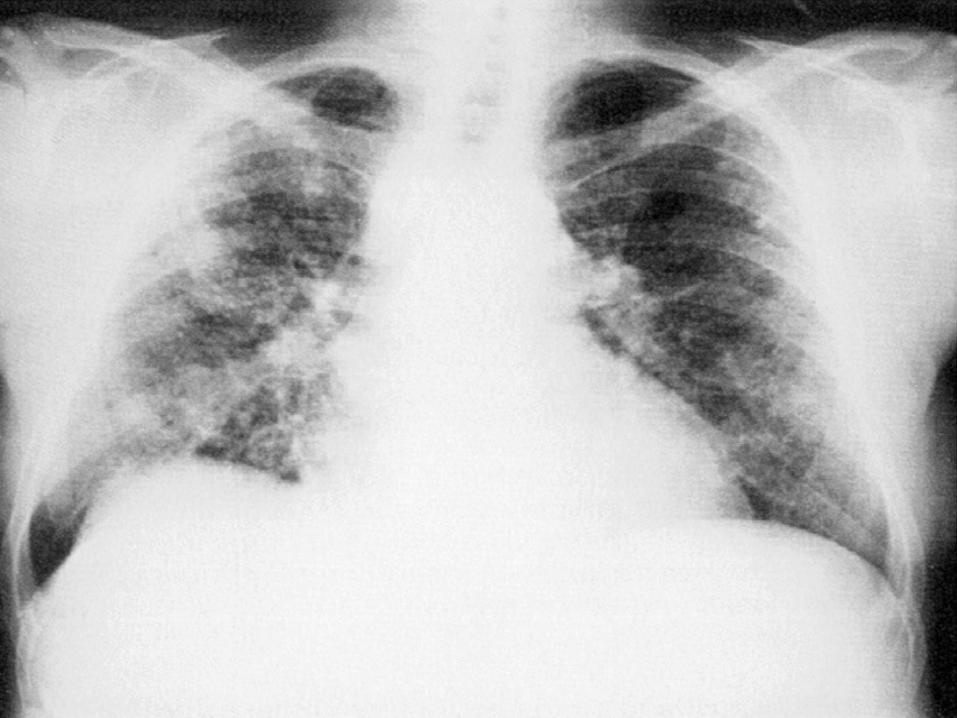
CX-Ray from a surface mine driller. smoked heavily for many years. Asymmetric bilateral upper zone progres -sive massive fibrotic lesions are present. larger and denser left-sided mass lesion raises concern of a pulmonary maligna- ncy.
Case 2
Chest radiograph from a worker employed for many years in a glass factory with silicosis who then experienced a relatively aggressive downhill course.
Investigation revealed infection with M. tuberculosis.Although he responded to multiple drug therapy, he still had severe progressive massive fibrosis, extensive emphysema, and impaired function.
Case 3

Accelerated silicosis is characterized by the same features as classic silicosis except that the time from initial exposure to silica to the development of radio- graphic changes and ensuing respiratory impairment is much shorter. The chest radiograph may demonstrate rounded opacities as early as 4 years after initial silica exposure.
Result of exposure to grossly excessive levels of dust.
Rapid progression to progressive massive fibrosis is associated with severe respiratory impairment.
Accelerated silicosis
After a short duration of exposure to a high concentra- tions of respirable free silica.
The worker has a relatively rapid onset of chest symptoms and progressive respiratory impairment.
Deaths of a large number of these workers occurred within a year after the onset of symptoms.
Acute silicosis
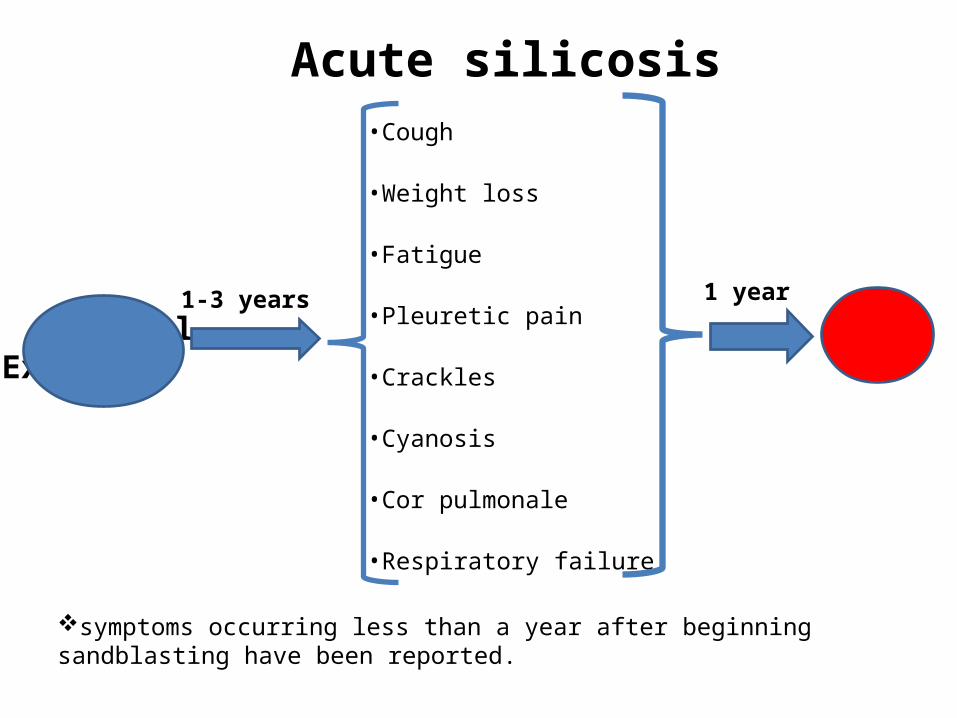
Initial Exposure
•Cough
•Weight loss
•Fatigue
•Pleuretic pain
•Crackles
•Cyanosis
•Cor pulmonale
•Respiratory failure
1-3 years 1 year
Death
Acute silicosis
symptoms occurring less than a year after beginning sandblasting have been reported.
ASSOCIATED ILLNESSES
• Mycobacterial infections• Carcinoma of the lung• Connective tissue disease• Renal and extra pulmonary
involvement
Silica particles increase the susceptibility to mycobacterial infection by altering cell mediated immunity.
The incidence of tuberculosis is likely to be greater in workers with accelerated or acute silicosis.
Silica exposure, by itself and in the absence of silicosis, is a risk factor for tuberculosis.
The frequency of mycobacterial infection increase as the extent of radiographic changes.
Silica exposure can impress on mortality in T.B patients.( 4 years earlier)
Mycobacterial infection

The diagnosis of tuberculosis in workers with silicosissometimes can be difficult Because :
1. tuberculous infections can be walled off in the lung by silica-induced fibrosis.2. A false-negative acid-fast-staining sputum smear may occasionally be present.3. Constitutional symptoms, such as fatigue, fever, dyspnea, and weight loss, can be seen in workers with worsening silicosis independent of a mycobacterial infection.4. Finally, the radiographic changes of tuberculosis may mimic advanced silicosis.
Mycobacterial infection
The combination of silicosis and tuberculosis is more difficult to treat.
Those with silicosis should undergo regular PPD skin testing.
Mycobacterial infection

When you doubt to T.B in a silicotic worker?
Radiographic progression over a short time period.
Coalescence of nodules in the upper lung fields, or cavitation of a pre-existing lesion .

(IARC) concluded that there is sufficient evidence to judge silica a carcinogen
for humans.
The risk of lung cancer is highest in workers with silicosis who also smoke.
The risk in those exposed to silica but without silicosis is less clear.
Carcinoma of lung
A number of studies demonstrate increased rates of arthritis, scleroderma, rheumatoid arthritis, musculoskeletal disease, and renal insufficiency in silica exposed populations.
workers with dust exposure and rheumatoid arthritis upper zone peripheral nodules appeared more frequently in the lungs . This presentation of rheumatoid nodules in workers with silica exposure has been termed Caplan’s syndrome.
Connective tissue disease
• Renal disease has been attributed both to a toxic effect or silica or an immunologically mediated process.
• Silicotic lesions have also been described in the liver , spleen, bone marrow, and remote lymph nodes. ( the result of lymphatic or hematogenous spread )
Renal & extra pulmonary involvement
Product substitution of silica with less toxic particles in abrasive blasting.
Control of air-borne dust concentration through engineering interventions.
Appropriate use of respiratory protective devices.
Prevention & management
Medical screening of silica-exposed workers is generally recommended,
using
questionnaires chest x-raysspirometry.And….PPD
Prevention & management
in countries with a high endemic rate of tuberculosis, yearly testing and if TB is
less frequent, less frequent testing would be appropriate.
With a PPD+ test without clinical evidence of
active tuberculosis, at least 1 year of Isoniazid therapy is indicated.
Prevention & management

The rate of FEV1 and FVC decline increased with profusion of opacities.
According to one study:
Decline in FEV1 at year
Decline in FEC at year
silica-exposed without silicosis
15 37
most extensive disease
128 116
Prevention & management
Once a diagnosis of silicosis is made the worker should be removed from further silica exposure.
Clinical suspicion of the development of mycobacterial infection must be high.
Standard tuberculosis treatment regimens are effective.
Prevention & management
Corticosteroid therapy : in patients with acute and chronic forms especially when silicosis is associated with autoimmune disease.
Isoniazid prophylaxis is appropriate when corticosteroid therapy is prescribed.
Tetrandrine, a plant alkaloid with antioxidant and anti inflammatory properties ,has been shown to arrest the progression of silicosis.
lung transplantation for workers with extensive silicosis.
Prevention & management


Thanks for attention