Role of μ-opioid system in the formation of memory of placebo responses
3
Click here to load reader
Transcript of Role of μ-opioid system in the formation of memory of placebo responses

cocaine-dependent individuals.2,3 These observations raise thequestion of whether cocaine abuse might accelerate the processof normal ageing. Although this is a little-studied area, there areseveral reasons for assuming that chronic cocaine exposureinterferes with the processes of brain ageing.
We compared the effects of age on gray matter volume in 120individuals aged 18 -- 50 years (Supplementary Information). Halfof the sample met the standard diagnostic criteria for cocainedependence of the DSM-IV-TR;4 whereas the other half had nohistory of substance misuse disorders or major psychiatricdisorders. The two groups were matched for age (t118¼�0.12,P¼ 0.905), gender (w2¼ 2.8, P¼ 0.148), and verbal IQ (t115¼�0.36,P¼ 0.716), as described elsewhere.5 All participants underwent astructural MRI brain scan, which was analyzed using voxel-basedmorphometry5 to produce whole-brain maps of age-relatedchange in gray matter volume.
All participants showed a reduction of gray matter volume incortical and subcortical regions as a linear function of increasingcalendar age (Figures 1a and b). However, the annual rate ofglobal gray matter volume loss in cocaine-dependent individualswas almost twice the rate of healthy volunteers (that is, 3.08 ml peryear (standard error (s.e.): 0.49 ml) versus 1.69 ml per year (s.e.:0.41 ml)). Consequently, the rate of age-related gray mattervolume loss in cocaine-dependent individuals was significantlygreater than in healthy volunteers (F1,116¼ 4.7, P¼ 0.031); thisinteraction remained significant after excluding 16 individualswith comorbid alcohol dependence (F1,100¼ 6.4, P¼ 0.013).Accelerated ageing in cocaine-dependent individuals was alsodemonstrated by a significant age-by-group interaction on graymatter volume of the regions affected by age (Po0.001, seeFigure 1c). Cocaine-dependent individuals showed a significantlygreater-than-normal age-related decline in gray matter inprefrontal and temporal regions compared with healthy controls.By contrast, parts of the striatum appeared resistant to age-relatedvolume decline in the cocaine-using group. Enlarged striatalvolume has frequently been reported in stimulant-dependentindividuals,5,6 possibly reflecting a marker of reduced dopamineneurotransmission in this dopamine-rich brain region where drugslike cocaine work. Decline in striatal dopamine receptor densityhas been associated with normal age-related cognitive decline.7
The relative absence of age-related changes in the striatum ofcocaine-dependent people may thus reflect another feature of anabnormal brain ageing process.
Abnormal ageing in chronic cocaine users is an emerging publichealth concern, which has received little attention. Approximately1% (ref. 8) of the 21 million users of cocaine wordwide,9 areconsidered to develop cocaine dependence. These individualsmay potentially be at risk of premature brain ageing. Youngpeople taking cocaine today need to be educated about the long-term risk of ageing prematurely, specifically at a time when manydeveloped economies are facing the demographic challenge ofan ageing population. Our findings also draw attention to theincreasing number of older drug users seeking treatment for drugabuse.10 Drug-treatment services, however, mainly target drug usein young people, focusing on prevention and harm reduction; theneeds of older drug users are not so well catered for. As thepsychological and physiological challenges of ageing may havealso accelerated in individuals with long-term drug dependence,11
the effects of cocaine on the process of ageing should berecognized in order to design and administer age-appropriatetreatments for older drug users.
CONFLICT OF INTERESTThis work was funded and sponsored by GlaxoSmithKline (RG45422) and conductedwithin the GlaxoSmithKline Clinical Unit Cambridge (UK) and the Behavioural andClinical Neuroscience Institute at the University of Cambridge, which is jointly fundedby the Medical Research Council and the Wellcome Trust. KDE and PSJ, who are both
supported by an MRC research grant, declare no conflict of interest. GBW declaresthat he has no potential conflict of interest. TWR consults for Cambridge Cognition,Lilly, Lundbeck and GlaxoSmithKline, and is currently in receipt of research grantsfrom these companies. ETB is employed part-time by GlaxoSmithKline and part-timeby the University of Cambridge.
KD Ersche1, PS Jones1, GB Williams1,2, TW Robbins1
and ET Bullmore1,3,4
1Behavioural and Clinical Neuroscience Institute and Department ofExperimental Psychology and Department of Psychiatry, University of
Cambridge, Cambridge, UK;2Wolfson Brain Imaging Centre, Department of Clinical
Neurosciences, University of Cambridge, Cambridge, UK;3Clinical Unit Cambridge, GlaxoSmithKline, Addenbrooke’s Centre for
Clinical Investigations, Cambridge, UK and4Cambridgeshire and Peterborough NHS Foundation Trust,
Cambridge, UKE-mail: [email protected]
REFERENCES1 Degenhardt L, Singleton J, Calabria B, McLaren J, Kerr T, Mehta S et al. Drug
Alcohol Depend 2011; 113: 88 -- 95.2 Verdejo-Garcia A, Perez-Garcia M. Psychopharmacology 2007; 190: 517 -- 530.3 Reece A. Immunity Ageing 2007; 4: 6.4 American Psychiatric Association. Diagnostic and Statistical Manual of Mental
Disorders, 4th edn., Text revision. American Psychiatric Association: Washington,DC, 2000.
5 Ersche KD, Barnes A, Jones PS, Morein-Zamir S, Robbins TW, Bullmore ET. Brain2011; 134: 2013 -- 2024.
6 Jacobsen LK, Giedd JN, Gottschalk C, Kosten TR, Krystal JH. Am J Psychiatry 2001;158: 486 -- 489.
7 Backman L, Nyberg L, Lindenberger U, Li SC, Farde L. Neurosci Biobehav Rev 2006;30: 791 -- 807.
8 Bucello C, Degenhardt L, Calabria B, Nelson P, Roberts A, Medina-Mora ME et al.NDARC Technical Report No. 30. National Drug and Alcohol Research Centre,University of NSW: Sydney, 2010.
9 UNDOC. Word Drug Report 2011. (United Nations Publication, Sales No. E.11.XI.10).10 Arndt S, Clayton R, Schultz SK. Am J Geriatr Psych 2011; 19: 704 -- 711.11 Beynon C, Stimson G, Lawson E. Br J Gen Pract 2010; 60: 481 -- 482.
Supplementary Information accompanies the paper on theMolecular Psychiatry website (http://www.nature.com/mp)
Role of m-opioid system in theformation of memory ofplacebo responsesMolecular Psychiatry (2013) 18, 135--137; doi:10.1038/mp.2012.16;published online 20 March 2012
Learning motivated behaviors seem critical for the development1
and presumably, sustainability of placebo responses. However,the neurobiology of long-term forms of placebo responses inhumans is largely unexplored. A body of literature has implicateddopaminergic neurotransmission in both, placebo responses2,3
and learning motivated behaviors.4 However, the contribution ofother placebo-related neurotransmitter systems, such as theendogenous opioid, to learning in a motivational context, hasnot been studied in humans. In vitro studies on neurons in thehippocampus have shown that m-opioid receptor agonists
Letters to the Editor
135
Molecular Psychiatry (2013), 134 -- 140& 2013 Macmillan Publishers Limited

facilitate long-term potentiation by increasing the excitability ofhippocampal pyramidal and dentate granule cells,5 and enkepha-lins have been involved in the attenuation of amnesia.6
A network of regions including the rostral anterior cingulate,dorsolateral prefrontal and orbitofrontal cortices, insula, ventralstriatum, amygdala, medial thalamus and periaqueductal gray areinvolved in acute placebo analgesia.2 These brain areas partlyoverlap and demonstrate substantial connectivity with traditionalmemory and cognitive circuits such as the cortico-limbic pathway,the Papez circuit or the septo-hippocampal pathway,7 where highconcentrations of m-opioid receptors have also been described.8
Here, we examined the relationships between measures ofregional m-opioid system activation using positron emissiontomography and the m-opioid receptor selective radiotracer[11C]carfentanil during a constant sustained pain challenge withand without placebo administration, as previously described,2 andthe recall of analgesic effects 24 h later. It was hypothesized that inaddition to already described acute placebo-responsive regions,2
the recall of placebo analgesia would induce the activation of them-opioid system in cognitive regions engaged during placeboadministration, providing a framework for the understanding ofneurocircuitry of long-term forms of placebo response.
For this purpose subjects were asked to recall their painexperience by completing the McGill Pain Questionnaire (MPQ) ina phone interview 24 h after completion of the scanning protocols(pain and painþplacebo scans). Subjects were considered placeborecall responders when MPQ scores 24 h after the painþplaceboscans were lower than during the scans when pain alone wasintroduced (n¼ 18); and placebo recall non-responders when MPQscores 24 h after the painþplacebo studies were the same or greaterthan during the studies where pain alone was introduced (n¼ 19)(Supplementary Figure 1). A mixed model was applied on a voxel byvoxel basis using SMP5, with placebo responder/non-responder
recall groups as the between-subject factor and m-opioid systemactivation during placebo administration as the dependentvariable using a threshold of Po0.001, with an extent 480 mm3
for regions previously implicated in placebo effects. For hypothe-sized regions involved in memory formation (the hippocampus,parahippocampus, mamillary bodies and septum), a volume ofinterest analysis and FWE correction for multiple comparisons atPo0.05 was employed (Supplementary Figure 2).
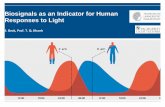
The whole brain analysis revealed a significant effect of recallgroup (placebo responders4non-responders) on m-opioid systemactivation in regions previously associated with placebo re-sponses: dorsolateral prefrontal cortex (x, y, z, MNI coordinates,�42, 26, 13; Z¼ 3.54), medial frontal gyrus/dorsal anterior cingulatecortex (�2, 9, 54; Z¼ 3.22), posterior insula (�51, �17, 0; Z¼ 3.48),amygdala (�27, �3, �22; Z¼ 3.75), putamen (�33, 5, �5; Z¼ 4.20),ventral striatum (19, 6, �15; Z¼ 3.38), ventral tegmental area (VTA)(�8, �15, �8; Z ¼ 3.5) and periaqueductal gray (�6, �29, �10;Z¼ 3.44) (Figure 1; Supplementary Table 1).
The ROI analysis detected effects of recall group (placeboresponders4non-responders) in regions involved in memoryprocessing: the left parahippocampus (�27, �45, �5; Z¼ 3.67),left hippocampus (�27, �5, �22; Z¼ 3.57) and left mamillarybodies (�6, �15, �8; Z¼ 3.10), and with trend levels in the righthemisphere for all regions. Conversely, and nearing significance(�2, 11, �1; Z¼ 2.6), greater m-opioid system activation duringplacebo administration in the non-responder group was singularlynoted in the septal region (placebo non-responders4responders)(Figure 1, Supplementary Table 1).
Consistent with animal models showing an effect of theenkephalinergic system and m-opioid receptors in learning andmemory,6 our data suggest that in addition to its immediateplacebo-analgesic effects, the m-opioid receptor system is involvedin the subsequent recall of placebo responses. Specifically, the
Figure 1. Placebo recall (red-yellow: responders4non-responders; dark-light blue: non-responders4responders) group effect on m-opioidsystem activation during placebo administration with expectation of analgesia.
Letters to the Editor
136
Molecular Psychiatry (2013), 134 -- 140 & 2013 Macmillan Publishers Limited

VTA and the Papez circuit (hypothalamus-mammillary bodies,mamillo-thalamic tract, anterior thalamic nuclei, cingulate cortexand hippo/parahippocampus), implicated in reward-motivatedlearning and memory processing,4 appeared to be involved inthese processes. Activation in the septal region in placebo non-responders recalling was also observed. If confirmed, this effectwould be consistent with the memory impairment observed afterintraseptal m-opioid agonist administration,9 through inhibition ofthe septohippocampal GABAergic neurons.10 This report extendsprevious findings on the role of the m-opioid neurotransmittersystem in acute placebo responses,2 and highlights a novel role ofthis system in the formation of memories of placebo analgesiceffects in distinct neural circuits. These processes provide aframework to understand stimulus learning and therapeutic effectassociations, of importance for the sustainability of placeboeffects.
CONFLICT OF INTERESTThe authors declare no conflict of interest.
M Pecina1, CS Stohler2 and J-K Zubieta1,3
1Molecular and Behavioral Neuroscience Institute, University ofMichigan, Ann Arbor, MI, USA;
2School of Dentistry, University of Maryland, Baltimore, MD, USA and3Departments of Psychiatry and Radiology, Medical School, University of
Michigan, Ann Arbor, MI, USAE-mail: [email protected]
REFERENCES1 Colloca L, Miller FG. Philos Trans R Soc Lond B Biol Sci 2011; 366: 1859--1869.2 Scott DJ, Stohler CS, Egnatuk CM, Wang H, Koeppe RA, Zubieta JK. Arch Gen
Psychiatry 2008; 65: 220--231.3 de la Fuente-Fernandez R. Parkinsonism Relat Disord 2009; 15(Suppl 3): S72--S74.4 Adcock RA, Thangavel A, Whitfield-Gabrieli S, Knutson B, Gabrieli JD. Neuron 2006;
50: 507--517.5 Simmons ML, Chavkin C. Int Rev Neurobiol 1996; 39: 145--196.6 Rigter H. Science 1978; 200: 83--85.7 Liu MG, Chen J. Neurosci Bull 2009; 25: 237--266.8 Arvidsson U, Riedl M, Chakrabarti S, Lee JH, Nakano AH, Dado RJ et al. J Neurosci
1995; 15(5 Part 1): 3328--3341.9 Bostock E, Gallagher M, King RA. Behav Neurosci 1988; 102: 643--652.
10 Alreja M, Shanabrough M, Liu W, Leranth C. J Neurosci 2000; 20: 1179--1189.
Supplementary Information accompanies the paper on theMolecular Psychiatry website (http://www.nature.com/mp)
Autism recurrence in halfsiblings: strong support forgenetic mechanisms oftransmission in ASDMolecular Psychiatry (2013) 18, 137--138; doi:10.1038/mp.2012.9;published online 28 February 2012
Current estimates of the heritability of autism spectrum disorders(ASD) derived from existing clinical twin studies1--4 are potentiallyconfounded by a number of factors, including low sample size,
inconsistency in case definition and the role of de novo mutation(currently estimated to contribute to some 20% of cases), and thepossibility that heritable causes of ASD in a twin could result inenvironmentally engendered affectation of a non-identical co-twinin utero, especially if mediated by humoral or immune mechanisms.To minimize these confounds, we compared autism recurrence inhalf siblings versus that in full siblings, using data (6 June 2011)from over five thousand families enrolled in the Interactive AutismNetwork (IAN), a national volunteer register for ASD, detailedcharacteristics of which have been previously described by ourgroup.5,6 Recurrence rate among full siblings was observed to beapproximately twice that among half siblings, providing strongevidence of genetic transmission of ASD.
The data included 5237 families with (a) an ASD-affected childand (b) at least one additional sibling. Among these, 619 includedat least one maternal half-sibling, 55 included a paternal half-sibling and 4832 contained at least one full sibling of an ASDproband. A maximum of one full sibling and one maternal halfsibling per family (selected at random in families in which morewere available) were incorporated into the analysis. Samplecharacteristics are provided in Supplementary Table 1.
The recurrence rate was 0.052 for maternal half siblings (0.081for males, 0.020 for females), 0.00 for the small number of paternalhalf siblings and 0.095 for full siblings (0.141 for males, 0.050 forfemales). There was no difference in the full sibling recurrence ratein families with additional half siblings (0.100) compared withthose without. The full sib recurrence rate is in agreementwith numerous prior studies of sibling recurrence for categoricalASD-affectation status among school-aged children using moderncategorical case definitions.5 In a logistic regression model adjustingfor sibling type (full versus maternal half sibling), gender anddifference in age between proband and sib, gender (Po0.0001)and sibling type (P¼ 0.004) were highly statistically significant, with acalculated point estimate (for risk incurred by half sibling status incomparison to full sibling status) of 0.56, and a 95% confidenceinterval of 0.38--0.83.
Structural equation modeling generated robust heritabilityestimates of 50--70% over a broad range of assumptions forpopulation prevalence (Figure 1 and Supplementary Table 2).
Figure 1. Heritability, as a function of assumed population pre-valence of autism spectrum disorders (ASD, %), estimated byimplementing structural equation modeling of Interactive AutismNetwork (IAN) registry data on recurrence of ASD among fullsiblings (n¼ 4832) and maternal half siblings (n¼ 619) of ASDprobands.
Letters to the Editor
137
Molecular Psychiatry (2013), 134 -- 140& 2013 Macmillan Publishers Limited