Research Article Effect of 17-β Estradiol and Iopromide on Rat · 2018. 4. 2. · iopromide-370,...
8
Central Annals of Vascular Medicine & Research Cite this article: Betala J, Lee JS, Langan EM III, LaBerge M (2018) Effect of 17-β Estradiol and Iopromide on Rat Primary Smooth Muscle Cell Hyperplastic Response in Static and Dynamic Conditions. Ann Vasc Med Res 5(2): 1088. *Corresponding author Martine LaBerge, Department of Bioengineering, Clemson University, 301 Rhodes Research Center, 118 Engineering Service Drive, Clemson, SC 29634, USA, Tel: 864-656-5557; Email: Submitted: 12 March 2018 Accepted: 21 March 2018 Published: 25 March 2018 ISSN: 2378-9344 Copyright © 2018 LaBerge et al. OPEN ACCESS Keywords • 17-β Estradiol • Smooth muscle cells • Proliferation • Iopromide-370 Research Article Effect of 17-β Estradiol and Iopromide on Rat Primary Smooth Muscle Cell Hyperplastic Response in Static and Dynamic Conditions Jayesh Betala 1 , Jeoung Soo Lee 1 , Eugene M. Langan III 2 , and Martine LaBerge 1 * 1 Department of Bioengineering, Clemson University, USA 2 Department of Vascular Surgery, Greenville Health System, USA Abstract Purpose: Endovascular stents to manage plaque formation in arteries cause restenosis with smooth muscle cells (SMCs) proliferation. Estrogen is known to exert cardiovascular protective effects and antiproliferative effects on vascular smooth muscle cells in vitro as well as in vivo. In this study, we evaluated the effect of estrogen (17-β estradiol) delivered with iopromide-370 (17-βE/Iop) on SMCs proliferation, apoptosis, protein expression and hypertrophy under static and dynamic strain conditions. Methods: Rat aortic SMCs were cultured in static and dynamic conditions for 24 hours, followed by short-term treatment with 17-βE/Iop. At a predetermined time, SMCs were analyzed for proliferation using MTT assay, apoptosis employing TUNEL assay, and hypertrophy by immunostaining for SM α-actin, and SM22α expression by western blot. Results: Rat aortic SMCs proliferation was significantly inhibited after treatment of 17-βE/Iop for 5 minutes, and inhibition was maintained up to 7 days in static conditions and up to 3 days in dynamic conditions as compared to untreated control. For apoptosis, hypertrophy, and protein expression levels, SMCs treated with 17-βE/Iop were not significantly different from untreated SMCs in both static and dynamic conditions. Conclusion: Estrogen with iopromide-370 (17-βE/Iop) showed significant SMCs proliferation inhibition with 5 minutes’ treatment; however, no other effects were observed after treatment in both static and dynamic conditions. INTRODUCTION Cardiovascular disease remains the leading cause of death in United States and around the world, with atherosclerosis being one of the underlying cause [1]. Atherosclerosis, a progressive disease with complex cellular and molecular pathology, begins with an accumulation of lipids and progresses to advanced lesions of lipid-rich necrotic debris and smooth muscle cells (SMCs) [1]. SMCs proliferate and migrate from the media into the intima, which causes phenotypic changes from a contractile to a synthetic state [2]. Phenotypic modulation of SMCs is also apparent with any vascular injury such as percutaneous stenting; such injuries cause SMCs to proliferate, migrate and deposit extracellular matrix (ECM), which leads to restenosis [3]. The mechanism of restenosis initially involves endothelial cell layer denudation, platelet aggregation, and stretching of SMCs and is later accompanied by apoptosis, migration and proliferation of SMCs [4]. Synthetic SMCs increase the number of organelles such as rough endoplasmic reticulum and decrease contractile protein markers α-actin, SM22α and SM-myosin heavy chain [3,5]. Recently, drug-eluting stents (DES) have mitigated restenosis to a large extent, but late stent thrombosis (LST) and delayed revascularization remain a problem [6,7]. Paclitaxel is an antiproliferative agent currently used on DES to mitigate restenosis [6]. One of the newer approaches to avoid LST and revascularize an artery is with non-stent based delivery of paclitaxel using a contrast agent such as iopromide-370 (Ultravist ® ) (Iop) coated on a balloon [8]. Contrast agents such as Iop, urea, shellac, and butyryl tri-hexyl citrate (BHTC) provide a matrix for antiproliferative drugs to facilitate their rapid uptake into the blood vessel wall [4,9]. Scheller et al., reported that such an approach has been successful in minimizing neointimal proliferation [4,9-12]. However, paclitaxel delays re-endothelialization, which is essential for remodeling after intervention. Estrogen, specifically 17-βE, is known to provide cardiovascular protective effects in premenopausal women as compared to men of the same age [13,14]. 17-βE has been proven to contribute cardiovascular protective effects at the cellular
Transcript of Research Article Effect of 17-β Estradiol and Iopromide on Rat · 2018. 4. 2. · iopromide-370,...

Central Annals of Vascular Medicine & Research
Cite this article: Betala J, Lee JS, Langan EM III, LaBerge M (2018) Effect of 17-β Estradiol and Iopromide on Rat Primary Smooth Muscle Cell Hyperplastic Response in Static and Dynamic Conditions. Ann Vasc Med Res 5(2): 1088.
*Corresponding authorMartine LaBerge, Department of Bioengineering, Clemson University, 301 Rhodes Research Center, 118 Engineering Service Drive, Clemson, SC 29634, USA, Tel: 864-656-5557; Email:
Submitted: 12 March 2018
Accepted: 21 March 2018
Published: 25 March 2018
ISSN: 2378-9344
Copyright© 2018 LaBerge et al.
OPEN ACCESS
Keywords•17-βEstradiol•Smooth muscle cells•Proliferation•Iopromide-370
Research Article
Effect of 17-β Estradiol and Iopromide on Rat Primary Smooth Muscle Cell Hyperplastic Response in Static and Dynamic ConditionsJayesh Betala1, Jeoung Soo Lee1, Eugene M. Langan III2, and Martine LaBerge1*1Department of Bioengineering, Clemson University, USA2Department of Vascular Surgery, Greenville Health System, USA
Abstract
Purpose: Endovascular stents to manage plaque formation in arteries cause restenosis with smooth muscle cells (SMCs) proliferation. Estrogen is known to exert cardiovascular protective effects and antiproliferative effects on vascular smooth muscle cells in vitro as well as in vivo. In this study, we evaluated the effect of estrogen (17-β estradiol) delivered with iopromide-370 (17-βE/Iop) on SMCs proliferation, apoptosis, protein expression and hypertrophy under static and dynamic strain conditions.
Methods: Rat aortic SMCs were cultured in static and dynamic conditions for 24 hours, followed by short-term treatment with 17-βE/Iop. At a predetermined time, SMCs were analyzed for proliferation using MTT assay, apoptosis employing TUNEL assay, and hypertrophy by immunostaining for SM α-actin, and SM22α expression by western blot.
Results: Rat aortic SMCs proliferation was significantly inhibited after treatment of 17-βE/Iop for 5 minutes, and inhibition was maintained up to 7 days in static conditions and up to 3 days in dynamic conditions as compared to untreated control. For apoptosis, hypertrophy, and protein expression levels, SMCs treated with 17-βE/Iop were not significantly different from untreated SMCs in both static and dynamic conditions.
Conclusion: Estrogen with iopromide-370 (17-βE/Iop) showed significant SMCs proliferation inhibition with 5 minutes’ treatment; however, no other effects were observed after treatment in both static and dynamic conditions.
INTRODUCTION Cardiovascular disease remains the leading cause of death in
United States and around the world, with atherosclerosis being one of the underlying cause [1]. Atherosclerosis, a progressive disease with complex cellular and molecular pathology, begins with an accumulation of lipids and progresses to advanced lesions of lipid-rich necrotic debris and smooth muscle cells (SMCs) [1]. SMCs proliferate and migrate from the media into the intima, which causes phenotypic changes from a contractile to a synthetic state [2]. Phenotypic modulation of SMCs is also apparent with any vascular injury such as percutaneous stenting; such injuries cause SMCs to proliferate, migrate and deposit extracellular matrix (ECM), which leads to restenosis [3]. The mechanism of restenosis initially involves endothelial cell layer denudation, platelet aggregation, and stretching of SMCs and is later accompanied by apoptosis, migration and proliferation of SMCs [4]. Synthetic SMCs increase the number of organelles such as rough endoplasmic reticulum and decrease contractile protein markers α-actin, SM22α and SM-myosin heavy chain [3,5].
Recently, drug-eluting stents (DES) have mitigated restenosis to a large extent, but late stent thrombosis (LST) and delayed revascularization remain a problem [6,7].
Paclitaxel is an antiproliferative agent currently used on DES to mitigate restenosis [6]. One of the newer approaches to avoid LST and revascularize an artery is with non-stent based delivery of paclitaxel using a contrast agent such as iopromide-370 (Ultravist®) (Iop) coated on a balloon [8]. Contrast agents such as Iop, urea, shellac, and butyryl tri-hexyl citrate (BHTC) provide a matrix for antiproliferative drugs to facilitate their rapid uptake into the blood vessel wall [4,9]. Scheller et al., reported that such an approach has been successful in minimizing neointimal proliferation [4,9-12]. However, paclitaxel delays re-endothelialization, which is essential for remodeling after intervention.
Estrogen, specifically 17-βE, is known to provide cardiovascular protective effects in premenopausal women as compared to men of the same age [13,14]. 17-βE has been proven to contribute cardiovascular protective effects at the cellular

Central
LaBerge et al. (2018)Email:
Ann Vasc Med Res 5(2): 1088 (2018) 2/8
level in both animal models and clinical studies [15-19]. SMCs express two different estrogen receptors (ERs), ERα and ERβ, which bind to 17-βE and provide a long-term effect by changes in gene expression affecting cell proliferation [15]. Additionally, 17-βE has been shown to decrease low density lipid proteins in the plasma of postmenopausal women, endothelial nitric oxide synthase (NOS) activity and platelet and monocyte aggregation [15].
Clinical studies conducted by Women’s Health Initiative (WHI) in addition to the Heart and Estrogen/Progestin replacement study (HERS) showed an increased risk of coronary heart disease in postmenopausal women using estrogen replacement therapy [20]. However, there is growing evidence of the benefits of estrogen on the cardiovascular system, such as inhibiting SMCs proliferation, inducing endothelial cell growth, reducing cytokine production by macrophages, changing the lipid plasma profile by decreasing low-density lipoprotein (LDL) and increasing high-density lipoprotein (HDL), and increasing production of nitric oxide (NO) [13,15,21-26]. This study was aimed at evaluating the inhibitory effect of 17-β estradiol/Iop on SMCs proliferation under clinically relevant conditions. Contrast agents, such as iopromide-370, adhere to the luminal surface of arteries, allowing more efficient uptake of antiproliferative agents [9]. In addition to being efficient delivery vehicles, they are also known to have beneficial effects in restenosis inhibition [27]. Consequently, Iop was chosen to enhance the uptake of 17-β estradiol by SMCs to achieve greater inhibition of proliferation.
Therefore, it was hypothesized that combining 17-βE with a contrast reagent such as Iop would enhances SMCs inhibition, thus providing an alternative to mitigation of balloon angioplasty-induced myointimal hyperplasia. Dynamic conditions were applied to SMCs to provide a strain level experienced in an atherosclerotic artery during balloon angioplasty. Initially, the effect of 17-βE on SMCs proliferation was evaluated SMCs under static conditions with and without Iop. Finally, SMCs were evaluated for proliferation, apoptosis, protein expression and hypertrophy under dynamic mechanical loading conditions after delivery of 17- βE with Iop using a custom built vascular simulator.
MATERIAL AND METHODS
Primary rat aortic smooth muscle cell culture and characterization
Female Sprague Dawley rats between 6-8 weeks of age were euthanized, and the aortae dissected using a protocol approved by the Clemson University Institutional Animal Care and Use Committee (IACUC). SMCs were isolated using a modified protocol [28]. Briefly, a rat aorta was dissected and cleaned of excess fat. Adventitia on the aorta was peeled off, and the media was cut longitudinally to open the intima facing upwards. Using a sterile scalpel, the endothelial layer was scraped off; and the medial layer was then minced into approximately 1mm2 pieces. Minced artery pieces were then transferred into a 6-well plate containing collagenase type 2 (Worthington Biochemical, USA) and elastase (Worthington Biochemical, USA) in Dulbecco’s Modified Eagle Medium (DMEM) (Thermo Fisher Scientific, Inc. USA) and incubated on a shaker plate for 60 minutes at 37°C.
DMEM containing digested tissue was then centrifuged at 1000 RPM for 5 minutes, and cells were transferred to a T25 flask. Cells were maintained in DMEM without phenol red supplemented with 10% fetal bovine serum (FBS) (Corning, USA), 2 mM L-glutamine (Corning, USA)and 1% antibiotic-antimycotic (Ab-Am) (Corning, USA) under standard cell culture conditions (37°C, 5% CO2 with 95% air, humidified environment). Cells were characterized by immunofluorescence for SMCs marker SM α-actin. All the experiments were carried out between passages 3-6.
Effect of 17-βE/Iop treatment on SMCs proliferation in static conditions
SMCs were seeded on collagen type 1-(Advanced Biomatrix, USA) coated 24-well plates in DMEM without phenol red containing 10% FBS, 2mm L-glutamine and 1 % Ab-Am at a density of 2×104 cells/ml and incubated for 24 hours. The growth of SMCs was then arrested by culturing in DMEM with 1% FBS and 1% Ab-Am for 24 hours. A 40mM stock solution of 17-βE (Sigma Aldrich, USA) in DMSO was used for all experiments. To evaluate the effect of 17-βE treatment on SMCs proliferation, SMCs were treated with17-βE (20 µM in DMEM) without (n=12/group) and with (n=9/group) iopromide-370 (Iop) (Ultravist®, Bayer Pharmaceuticals, Germany) for periods of 5, 15 and 30 minutes. A 40.5% (% V/V) Iop isosmotic solution was prepared by mixing Iop with sterile deionized water [9,10]. From stock concentration of 17-βE, it was diluted in the Iop solution to obtain a concentration of 40µM. The Iop solution was further diluted with DMEM at 1:1 ratio to obtain a final working concentration of 20 µM 17-βE and 20.25% Iop. A final concentration of 20 µM was chosen based on a rabbit study by Axel and collaborators focusing on the optimum paclitaxel concentration to inhibit SMCs proliferation and prevent neointimal formation after balloon angioplasty [29]. After treatment, DMEM containing 17-βE or 17-βE/Iop was replaced with fresh DMEM containing 1% FBS and 1% Ab-Am and incubated for 24 hours. Untreated SMCs and SMCs cultured in DMEM containing DMSO (0.05%) or Iop were used as controls.
To further evaluate the effect of 17-βE/Iop on proliferation, SMCs were maintained for longer incubation periods of 3 and 7 days (n=9/group). Iop alone in DMEM and untreated SMCs served as controls. After treatment, DMEM solution containing 17-βE/Iop or Iop alone was then replaced with fresh DMEM containing 1% FBS and 1% Ab-Am and incubated for 3 and 7 days after treatment.
Effect of 17-βE/Iop treatment on SMCs proliferation in dynamic conditions
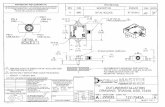
For the dynamic condition, a customized simulator was utilized [30]. Approximately 400 µm thick and 5.5 cm diameter biomedical-grade silicone discs (Specialty Manufacturing, USA) with a 40 Shore A hardness were sonicated in deionized water and assembled on the station plates. These assembled plates (Figure 1) were then autoclaved and placed into the simulator apparatus after silicone lubricant was applied to reduce friction between the surfaces (Loctite, USA). Following assembly, cleaned and sterile Teflon rings with an inner cross-sectional area of 2.75 cm2 and approximate height of 1.75 cm were placed on top of the center of the silicone membrane, above the loading post.

Central
LaBerge et al. (2018)Email:
Ann Vasc Med Res 5(2): 1088 (2018) 3/8
The cell-seeding silicone area enclosed by the rings was coated with collagen type 1 diluted to 50ug/ml with sterile deionized water for 24 hours under sterile conditions. After 24 hours, each membrane was rinsed with sterile Dulbecco’s phosphate buffered saline (DPBS)
SMCs were seeded on the collagen type 1-coated silicone membranes described above at a density of 2×104 cells/ml in DMEM, 10% FBS, and 1% Ab-Am for 24 hours and then growth-arrested for another 24 hours with DMEM containing 1% FBS and 1% Ab-Am and placed and cultured in a simulator with a preconditioning regimen of 0-5% cyclic strain at gradually increasing frequencies of 0.1 Hz for 2 hours, 0.5Hz for 6 hours, and 1 Hz for 16 hours. After 24 hours, SMCs were treated with 17-βE/Iop for 5 minutes (time point identified from static condition, which showed significant effect on SMCs proliferation) and cultured in the custom-built simulator described above with a preconditioning regimen of two 12% static circumferential stretches for 45 seconds each, simulating strains observed during balloon angioplasty [30]. After 5 minutes of treatment, SMCs were replenished with DMEM containing 1% FBS and 1% Ab-Am and underwent a cyclic strain regimen from 0 to 5% at a frequency of 1Hz for 24hours (n=6) and 72 hours (n=3). Untreated SMCs and Iop alone in DMEM served as controls for dynamic conditions.
SMCs proliferation quantification
Proliferation of SMCs was analyzed by methylthiazolyldiphe-nyl-tetrazolium bromide (MTT) (Sigma Aldrich, USA) assay for both static and dynamic conditions. Briefly, MTT was dissolved in sterile DPBS at 2 mg/ml. SMCs were rinsed with sterile DPBS and incubated in DMEM containing MTT for another 4 hours. Forma-zan crystals produced by live cells were dissolved in DMSO, and
absorbance was measured at 570 nm. Cell proliferation was cal-culated using the formula % cell proliferation = (OD570 Sample/OD570 Control) × 100.
Effect of 17-βE/Iop on SMCs apoptosis in dynamic condition
After 24 hours, SMCs apoptosis was evaluated using Dead End Fluorometric TUNEL assay (Promega, USA) according to the manufacturer’s protocol. After the end of the experiments, SMCs were fixed in freshly prepared 4% formaldehyde in 1X DPBS. Cells were permeabilized using 0.2% Triton® X-100 (ThermoFisher Scientific Inc., USA) in DPBS for 5 minutes and incubated for one hour at 37°C in equilibration buffer containing nucleotide mix and rTdT enzyme. SMCs nuclei were then stained with DAPI (ThermoFisher Scientific Inc., USA). Fragmented DNA of apoptotic cells was stained green with fluoresce in and imaged at 525 nm and stained with DAPI (blue) at 460 nm. The percentage of apoptotic cells in each group was measured by counting the number of apoptotic cells (green) among all cells, stained with DAPI (blue). Six fields were imaged per sample for each group. For positive control, cells were treated with RNase-free DNase I (Promega, USA) as described in the manufacturer’s protocol. Negative controls were incubated with rTdT incubation buffer without rTdT enzyme.
Effect of 17-βE/Iop on SMCs phenotype
Contractile protein expression analysis of SM α-actin and SM22α using standard western blotting techniques were used to evaluate whether or not 17-βE/Iop treatment affects SMCs phenotype. The expression of GAPDH was used as an endogenous control. SMCs were treated with 17-βE/Iop for 5 minutes in static and dynamic conditions followed by 24 hour’s additional culture. SMCs were lysed using 0.5% Triton X-100, 1% sodium dodecyl sulfate (SDS) (Sigma Aldrich, USA), 20mM Tris (Bio-rad Laboratories Inc., USA) and 10µL/mL protease cocktail inhibitor (Sigma Aldrich, USA). Total protein concentration of the extracted lysate was determined using bicinchoninic acid protein assay (BCA) kit (Pierce, ThermoFisher Scientific Inc., USA) according to the manufacturer’s protocol. Samples were then subjected to 10% SDS-PGE gel and transferred to a polyvinylidene difluoride (PVDF) membrane (Bio-Rad Laboratories Inc., USA). After being blocked for one hour, blots were incubated overnight at 4°C with primary antibodies of anti-SM α-actin (1:500) (Abcam, USA), anti-SM22α (1:2000) (Abcam, USA) and anti-GAPDH (1:1000) (Abcam, USA). The blots were incubated with appropriate secondary antibodies and conjugated with horseradish peroxidase for one hour at room temperature (HRP). Chemiluminescent signals were detected using a Gel Doc system (Bio-rad Laboratories Inc., USA) after treating membranes with Western Blotting Luminol reagent (Santa Cruz Biotechnology, USA). ImageJ (National Institutes of Health, USA) software was used to evaluate the differences in protein expression level between treated and control groups. The expression values were then normalized to GAPDH levels and statistically evaluated.
Effect of 17-βE/Iop SMCs Hypertrophy
The effect of 17-βE/Iop on SMCs hypertrophy was evaluated by measuring cell size and aspect ratio. SMCs were treated with 17-
Figure 1 Custom-built simulator for SMCs culture in dynamic conditions. a) Outer ring, b) Silicone disc on top of an inner ring, c) Assembled inner and outer rings with silicone disc in between, and d) Assembled base plate consisting of silicone disc with assembled rings. SMCs were plated on center of silicone ring and subjected to cyclic strain from bottom of the plate.

Central
LaBerge et al. (2018)Email:
Ann Vasc Med Res 5(2): 1088 (2018) 4/8
βE (20µM)/Iop for 5 minutes in static and dynamic condition. At 24 hours’ additional culture, SMCs were fixed in freshly prepared 4% formaldehyde solution. SMCs were stained for cytoskeletal F-actin using Rhodamine-Phalloidin (Sigma Aldrich, USA), and the nuclei were counterstained with DAPI. Measurements of cell area, major axis, minor axis and aspect ratio were determined using Image J (National Institutes of Health, USA). The aspect ratio was calculated as the ratio between major and minor axes, with 1.0 considered to be a complete circle. At least 100 cells per sample from each group were analyzed for cell area and axes and statistically compared according to area and aspect ratio.
Statistical analysis
Data reported are mean ± standard error of mean (SEM). Statistical significance was determined using one-way analysis of variance (ANOVA) and Student’s t-test. All tests were performed with JMP software (SAS institute Inc., USA) and plotted with Excel (Microsoft, USA). All studies performed area combination of samples from at least two independent studies to provide a minimum of three samples per group. P-value of <0.05 was considered to be significant.
RESULTS
Effect of 17-βE (20µM)/Iop on SMCs proliferation in static conditions
First it was evaluated whether Iop can enhance the antiproliferative effect of 17-βE on SMCs cultured in static condition. SMCs were treated with 17-βE with and without Iop for 5, 15, and 30 minutes, and cells were cultured an additional 24 hours after treatment. Untreated cells were used as control and were considered to be 100% for all experiments. A proliferation rate of 91 ± 3% was observed for cells treated with Iop alone and was not significantly different with untreated control (p=0.08, n=9). 17-βE alone for 5-, 15-, and 30-minute treatments showed significant proliferation inhibition compared to untreated control, with a % proliferation of 84 ± 1.3, 82 ± 2.15, and 81 ± 1.2, respectively (n=12) (Figure 2). 17-βE/Iop showed significantly enhanced anti-proliferative effect when compared to17-βE without Iop at 1 day post-treatment, with proliferation rates of 60 ± 4%, 57 ± 3% and 49 ± 4% for 5, 15 and 30 minutes, respectively (n=9) (p<0.0001 compared to 17-βE). However, the antiproliferative effect of 17-βE both with (p=0.3, n=9) and without Iop (p=0.4, n=12) was not significantly different with duration of treatment. The inhibitory effect of 17-βE/Iop on SMCs proliferation in static conditions was examined at longer time points after treatment. 17-βE/Iop treatment for 5, 15, and 30 minutes showed significantly enhanced anti-proliferation effect after 3 and 7 days post-treatment. However, the treatment duration did not significantly affect cell proliferation atDays3 and 7 (p=0.1 for both groups, n=9) post-treatment (Figure 3).
Effect of 17-βE/Iop treatment on SMCs proliferation in dynamic conditions
Next, the antiproliferative effect of 17-βE/Iop was evaluated on SMCs cultured in dynamic conditions. SMCs were treated with 17-βE/Iop for 5 minutes and additionally cultured 1 and 3 days after treatment. Percent cell proliferation was calculated
similarly to static proliferation studies, where dynamic control was at 100% proliferation. In dynamic conditions, SMCs treated with 17-βE/Iop depicted 73% (n=6, p<0.005 compared to control and Iop alone) and 74% cell proliferation (n=3, p<0.05 in comparison with control and Iop alone) after 1 and 3 days of 17-βE/Iop treatment, respectively. When Iop alone in DMEM was delivered for 5 minutes (vehicle control), cell proliferation at Day1 and Day 3 were 101% (n=4, p=0.7 compared to control) and 92% (n=3, p=0.2 compared to control), respectively (Figure 4).
Figure 2 Effect of 17-βE (20µM) with/without Iop on SMCs proliferation in static condition by MTT assay. SMCs were treated with 17-βE (20µM) with/without Iop for 5, 15 and 30 minutes and cell proliferation was evaluated at 24 hours’ after treatment (n=12 without Iop and n=9 with Iop group).Data shown as Mean ± SEM. Student’s t-test was used to determine statistical difference. *indicates statistical significance with p<0.0001 between treated and untreated control cells, # indicates statistical significance with p<0.0001between 17-βE alone and 17-βE/Iop.
Figure 3 Effect of 17-βE(20µM)/Iop treatment duration on SMCs proliferation in static condition by MTT assay. SMCs were treated with 17-βE(20µM)/Iop for 5, 15, and 30 minutes and cell proliferation was evaluated at 1, 3, and 7 days’ post-treatment (n=9).Data shown as Mean ± SEM. Student’s t-test was used to determine statistical difference between treated and untreated control. *indicates statistical significance with p<0.001 between treated and untreated control. ANOVA was used to determine statistical difference between different periods of treatment time and no significant difference (NS) observed between different treatment time periods.

Central
LaBerge et al. (2018)Email:
Ann Vasc Med Res 5(2): 1088 (2018) 5/8
Effect of 17-βE/Iop on SMCs apoptosis in dynamic conditions
Smooth muscle cells have been shown to undergo apoptosis due to external forces experienced from the endovascular procedures [5]. In dynamic conditions, few apoptotic cells were observed in treatment and control groups after 24 hours (Figure 5). However, no apoptotic cells were observed in static conditions (Images not shown). The ratios of apoptotic cells for dynamic conditions were 2.1 ± 0.4 % for 17-βE/Iop, 2.55 ± 0.47 % for Iop alone, and 4.26 ± 0.5 % for the control (Figure 5). No difference was observed between both treated groups and control group, indicating no influence of 17-βE/Iop on SMCs apoptosis.
Effect of 17-βE/Iop on SMCs phenotype
Analysis of protein expression markers showed a decreased expression of both SM α-actin and SM22α for all dynamic groups in comparison with their respective static groups. However, no significant difference was observed between 17-βE/Iop group compared to untreated control or Iop groups in static or dynamic conditions (p-value=0.22 for SM α-actin and p-value= 0.51 for SM-22α). Expression of SM α-actin in dynamic groups was approximately 25% to 30% significantly less as compared to their respective static groups (P<0.001) (Figures 6a and 6b). Similarly, expression of SM-22α in dynamic conditions was approximately 25% to 20% significantly lower than static groups (P<0.05) (Figures 6a and 6c).
Effect of 17-βE/Iop on SMCs hypertrophy
After intervention, SMCs undergo hyperplasia and hypertrophy due to the change in phenotype from spindle-like to rhomboidal structure [5]. This leads to a greater cell area with decreased aspect ratio in synthetic SMCs. In this study, no significant difference was observed between control and 17-βE/Iop groups in either static or dynamic conditions with p-values
of 0.47 and 0.97 for cell area and aspect ratios, respectively. Dynamic control cells were, however, relatively smaller than respective static cells with measured areas of 2667 ± 615 µm2 and 3886 ± 1025 µm2, respectively for the control groups; 2231 ± 433 µm2 and 3800 ± 1282 µm2 for the Iop groups; and 1912 ± 373 µm2 3163 ± 832 µm2 for the 17-βE/Iop groups (n=3, p=0.47) (Figure 7A). Aspect ratios measured were 1.74 ± 0.41 and 1.95 ± 0.48 for dynamic and static controls, 2.23 ± 0.53 and 1.77 ± 0.39 for dynamic and static Iop alone groups, and 2.14 ± 0.44and 1.96 ± 0.49 for 17-βE/Iop dynamic and static groups, (n=3/group, p=0.97) (Figure 7B).
Figure 4 Effect of 17-βE (20µM)/Iop treatment on SMCs proliferation in dynamic condition by MTT assay. SMCs were treated with 17-βE(20µM)/Iop for 5 minutes and cell proliferation was evaluated at 1 and 3 days post-treatment under dynamic conditions. Percent cell proliferation was quantified from each group at Day 1 and 3 post-treatment. Data shown as Mean ± SEM and Student’s t-test used to determine statistical difference. *indicates statistical significance between treated cells and control with P<0.005 for Day 1 (n=6) and p<0.05 for Day 3 (n=3) compared to both control and Iop alone.
Figure 5 Effect of 17-βE (20µM)/Iop treatment on SMCs apoptosis by TUNEL assay in dynamic conditions. SMCs were treated with 17-βE(20µM)/Iop for 5 minutes and the effect of treatment on apoptosis was evaluated at 1 day post-treatment. a) 17-βE/Iop treatment, Left: DAPI+ cells, Right: TUNEL + cells, b) Iop alone, Left: DAPI + cells, Right: TUNEL + cells c) Untreated Control, Left: DAPI + cells, Right: TUNEL + cells, d) % Apoptotic SMCs were quantified from each group. Data shown as Mean ± SEM. ANOVA was used to determine statistical difference between different periods of treatment time. No significant difference between treated and control samples was observed with p-value=0.068 (n=3/group). Scale bar- 400 µm.

Central
LaBerge et al. (2018)Email:
Ann Vasc Med Res 5(2): 1088 (2018) 6/8
DISCUSSIONInitially, SMCs were exposed to a high dose of 17-β estradiol
for a short period with or without Iop; significant enhancement was observed with Iop as compared to without Iop. After 17-β estradiol was delivered using Iop, the inhibitory effect on SMCs after Day 3 and Day 7 was also significantly enhanced after treatment periods of 5, 15 and 30 minutes. SMCs were also subjected to dynamic conditions to analyze the effects of 17-β estradiol using a custom-built simulator [30]. Dynamic conditions provide a clinically relevant environment as cells observe in vivo following endovascular procedures as compared to static conditions. SMCs were subjected to two injury cycles of high strain (12%) (experienced during balloon angioplasty) followed by cyclic tensile strain (0 to 5%) (to simulate arterial vessel dilation) [5]. Cyclic tensile and high strain conditions were chosen based on significant response by SMCs phenotype, as previously observed in our lab [5,30]. These conditions were applied to SMCs followed by treatment with 17-β estradiol delivered using Iop for 5 minutes to evaluate changes in cell proliferation, apoptosis, protein expression as an indication of phenotype change, and cell morphology.
SMCs tend to change their phenotype between contractile and synthetic state during remodeling [31,32]. This phenotypic change is known to cause cell proliferation, apoptosis and a decrease in contractile protein expression [2,5]. Dai-Do et al. [24], reported an approximately 20% decrease in proliferation in vitro after 10 days in both male and female saphenous vein SMCs after treatment with 1 µM 17-β estradiol for 48 hours. Similarly, Geraldes et al. [15], reported a decrease in proliferation in vitro in porcine SMCs after 72 hours of treatment with 0.1 µM 17-β estradiol. In accordance with these studies, treatment with 17-β estradiol for a short period significantly reduced SMCs proliferation after Days 1, 3 and 7 when enhanced with Iop. This significant inhibition was also achieved in dynamic conditions after Day 1 and Day 3, where approximately 25% inhibition was observed after 5 minutes of treatment. Authors have reported a 50% SMCs inhibition in rat carotid arteries by17-β estradiol after two weeks [17,33]. Chandrasekar et al. [18], and Kyriakides et al. [25], reported that in addition to inhibiting SMCs proliferation, 17-β estradiol does not delay reendothelialization of coronary arteries as compared to other anti-proliferative agents such as paclitaxel [7].
Increased proliferation of SMCs and apoptosis has been reported to cause restenosis [5,34,35]. However, contrary to several studies reporting17-β estradiol-induced SMCs apoptosis, no significant increase was observed in this study [36,37]. This could be attributed to the brief exposure period of 17-β estradiol as compared to continuous exposure for from 48 hours to 10 days in other studies [36,37]. However, a trend of change can be observed due to a smaller P-value between treated and control samples. Phenotypic change of SMCs also leads to a decrease in contractile protein markers commonly noticed in synthetic and proliferating SMCs [5,38]. Western blot analysis revealed a significant decrease after 24 hours in both contractile marker proteins, SM α-actin and SM22α, for dynamic groups as compared to static groups, similar to results previously reported by our lab [5]. However, treatment with 17-β estradiol/Iop or Iop alone
Figure 6 Effect of 17-βE (20µM)/Iop on contractile SMCs markers by western blot in dynamic and static conditions. SMCs were treated with 17-βE(20µM)/Iop for 5 minutes and lysed at 24 hours’ post-treatment. a) Phenotype marker expressions of SM α-actin, SM22α and GAPDH. Image representative of three experiments. b) and c) Protein expression levels of α-actin and SM22α, respectively, normalized to GAPDH (n=3). Data shown as Mean ± SEM. Student’s t-test used to determine statistical difference. No significant difference between dynamic treatment and control groups and static treatment and control groups was observed. (P-value=0.22 for SM α-actin and p-value= 0.51 for SM-22α).
did not affect contractile protein marker expression in either condition. Another indicator of SMCs phenotypic modulation is cell hypertrophy after an endovascular procedure; SMCs increase in size as compared to uninjured SMCs that are smaller and more elongated [5]. Although the mechanism is still not understood, estrogen is known to reduce cardiac hypertrophy in mice [39]. While limited data exist on the direct effect of 17-β estradiol on hypertrophy of SMCs, significance was not achieved between static and dynamic groups for cell area or aspect ratio. However, as in previous studies, cell area and aspect ratio were found to be lower and higher, respectively, in the dynamic group as compared to the static group [5]. In the literature over the decades, beneficial effects of estrogen, both in vitro and in vivo, on inhibition of SMCs proliferation has been documented substantially. Similar effects were also observed in this study

Central
LaBerge et al. (2018)Email:
Ann Vasc Med Res 5(2): 1088 (2018) 7/8
Figure 7 Effect of 17-βE (20µM)/Iop on SMCs hypertrophy after treatment for 5 minutes under dynamic and static conditions. At 24 hours post-treatment, SMCs were stained with phalloidin to measure cell area and aspect ratio. a) Cell area for treatment and control groups. No significant difference between treatment and control groups with p-value=0.472 (n=3). b) Cell aspect ratio for treatment and control groups. Data shown as Mean ± SEM. ANOVA was used to determine statistical difference between different periods of treatment time. No significant difference between treatment and control groups was observed with p-value=0.965 (n=3).
with short-term treatment in clinically relevant conditions when enhanced with contrast reagent such as iopromide-370.
CONCLUSIONBeneficial effects of estrogen on cardiovascular disease
and SMCs response have been widely reported over decades. In this study, it was observed that Iopromide-370 can enhance inhibitory effects of estrogen on SMCs. 17-β estradiol/Iop showed significant inhibition of SMCs, with 5 minutes’ treatment, as compared to untreated control cells in both static and dynamic conditions. However, no significant effect on contractile markers such as SM-α actin and SM22α, apoptosis and hypertrophy, was observed by in both static and dynamic conditions. A combination of estrogen and Iopromide-370 can serve as alternate treatment to address restenosis after stent implantation.
ACKNOWLEDGEMENTThis work was supported by an Institutional Development
Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number P20GM103444 and Page Morton Hunter Endowment.
REFERENCES1. Lusis AJ. Atherosclerosis. Nature. 2000; 407: 233-241.
2. Thyberg J, Hedin U, Sjolund M, Palmberg L, Bottger BA. Regulation of Differentiated Properties and Proliferation of Arterial Smooth muscle Cells. Arteriosclerosis. 1990; 10: 966-990.
3. Rensen SS, Doevendans PA, van Eys GJ. Regulation and characteristics of vascular smooth muscle cell phenotypic diversity. Neth Heart J. 2007; 15: 100-108.
4. Betala JV, Langan III EM, LaBerge M. Drug-Coated Percutaneous Balloon Catheters. Critical Reviews™ in Biomedical Engineering. 2014; 42: 193-212.
5. Acampora KB, Nagatomi J, Langan III EM, LaBerge M. Increased Synthetic Phenotype Behavior of Smooth Muscle Cells in Response to In Vitro Balloon Angioplasty Injury Model. Ann Vasc Surg. 2010; 24: 116-126.
6. Iakovou I, Schmidt T, Bonizzoni E, Lei G, Sangiorgi G, Stankovic G, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005; 293: 2126-2130.
7. Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, et al. Pathology of Drug-Eluting Stents in Humans: Delayed Healing and Late Thrombotic Risk. J Am Coll Cardiol. 2006; 48: 193-202.
8. Stolzenburg N, Breinl J, Bienek S, Jaguszewski M, Löchel M, Taupitz M, et al. Paclitaxel-Coated Balloons: Investigation of Drug Transfer in Healthy and Atherosclerotic Arteries – First Experimental Results in Rabbits at Low Inflation Pressure. Cardiovasc Drugs and Ther. 2016; 30: 263-270.
9. Scheller B, Speck U, Schmitt A, Böhm M, Nickenig G. Addition of paclitaxel to contrast media prevents restenosis after coronary stent implantation. J Am Coll Cardiol. 2003; 42: 1415-1420.
10. Scheller B, Speck U, Romeike B, Schmitt A, Sovak M, Böhm M, et al. Contrast media as carriers for local drug delivery: Successful inhibition of neointimal proliferation in the porcine coronary stent model. Eur Heart J. 2003; 24: 1462-1467.
11. Byrne RA, Joner M, Alfonso F, Kastrati A. Drug-coated balloon therapy in coronary and peripheral artery disease. Nat Rev Cardiol. 2014; 11: 13-23.
12. Cremers B, Biedermann M, Mahnkopf D, Böhm M, Scheller B. Comparison of two different paclitaxel-coated balloon catheters in the porcine coronary restenosis model. Clin Res Cardiol. 2009 98: 325-330.
13. Orshal JM, Khalil RA. Gender, sex hormones, and vascular tone. Am J Physiol Regul Integr Comp Physiol. 2004; 286: 233-249.
14. Nathan L, Chaudhuri G. Estrogens and atherosclerosis. Annu Rev Pharmacol Toxicol. 1997; 37: 477-515.
15. Geraldes P, Sirosis MG, Bernatchez PN, Tanguay JF. Estrogen Regulation of Endothelial and Smooth Muscle cell Migration and Proliferation: Role of p38 and p42/p44 Mitogen-Activated Protein Kinase. Arterioscler Thromb Vasc Biol. 2002; 22: 1585-1590.
16. Hwang K-C, Lee K-H, Jang Y. Inhibition of MEK1,2/ERK mitogenic pathway by estrogen with antiproliferative properties in rat aortic smooth muscle cells. J Steroid Biochem Mol Biol. 2002; 80: 85-90.
17. Chen SJ, Li H, Durand J, Oparil S, Chen YF. Estrogen Reduces Myointimal Proliferation After Balloon Injury of Rat Carotid Artery. Circulation. 1996; 93: 577-584.
18. Chandrasekar B, Tanguay JF. Local Delivery of 17-Beta-Estradiol Decreases Neointimal Hyperplasia after Coronary Angioplasty in a Porcine Model. J Am Coll Cardiol. 2000; 36: 1972-1978.

Central
LaBerge et al. (2018)Email:
Ann Vasc Med Res 5(2): 1088 (2018) 8/8
Betala J, Lee JS, Langan EM III, LaBerge M (2018) Effect of 17-β Estradiol and Iopromide on Rat Primary Smooth Muscle Cell Hyperplastic Response in Static and Dynamic Conditions. Ann Vasc Med Res 5(2): 1088.
Cite this article
19. Abizaid A, Albertal M, Costa MA, Abizaid AS, Staico R, Feres F, et al. First human experience with the 17-beta-estradiol–eluting stent: the estrogen and stents to eliminate restenosis (EASTER) trial. J Am Coll Cardiol. 2004; 43: 1118-1121.
20. Barrett-Connor E. Hormones and Heart Disease in Women: The Timing Hypothesis. Am J Epidemiol. 2007; 166: 506-510.
21. Bracamonte MP, Miller VM. Vascular effects of estrogens: arterial protection versus venous thrombotic risk. Trends Endocrinol Metab. 2001; 12: 204-209.
22. Nofer JR. Estrogens and atherosclerosis: insights from animal models and cell systems. J Mol Endocrinol. 2012; 48: 13-29.
23. Dubey RK, Jackson EK, Gillespie DG, Zacharia LC, Imthurn B, Keller PJ. Clinically Used Estrogens Differentially Inhibit Human Aortic Smooth Muscle Cell Growth and Mitogen-Activated Protein Kinase Activity. Arterioscler Thromb Vasc Biol. 2000; 20: 964-972.
24. Dai-Do D, Espinosa E, Liu G, Rabelink TJ, Julmy F, Yang Z, et al. 17β-Estradiol inhibits proliferation and migration of human vascular smooth muscle cells: similar effects in cells from postmenopausal females and in males. Cardiovasc Res. 1996; 32: 980-985.
25. Kyriakides ZS, Lymberopoulos E, Papalois A, Kyrzopoulos S, Dafnomili V, Sbarouni E, et al. Estrogen decreases neointimal hyperplasia and improves re-endothelialization in pigs. Int J Cardiol. 2006; 113: 48-53.
26. Sbarouni E, Iliodromitis EK, Bofilis E, Kyriakides ZS, Kremastinos DT. Short-Term Estrogen Reduces Myocardial Infarct Size in Oophororectomized Female Rabbits in a Dose-Dependent Manner. Cardiovasc Drugs Ther. 1998; 12: 457-462.
27. Batchelor WB, Granger CB, Kleiman NS, Phillips HR, Ellis SG, Betriu A, et al. A comparison of ionic versus nonionic contrast medium during primary percutaneous transluminal coronary angioplasty for acute myocardial infarction (GUSTO IIb). Global Use of Strategies to Open Occluded Coronary Arteries in Acute Coronary Syndromes. Am J Cardiol. 2000; 85: 692-697.
28. Campbell JH, Kocher O, Skalli O, Gabbiani G, Campbell GR. Cytodifferentiation and expression of alpha-smooth muscle actin mRNA and protein during primary culture of aortic smooth muscle cells. Correlation with cell density and proliferative state. Arteriosclerosis. 1989; 9: 633-643.
29. Axel DI, Kunert W, Göggelmann C, Oberhoff M, Herdeg C, Küttner A, et al. Paclitaxel Inhibits Arterial Smooth Muscle Cell Proliferation and Migration In Vitro and In Vivo Using Local Drug Delivery. Circulation. 1997; 96: 636-645.
30. Acampora KB, Langan III EM, Miller RS, LaBerge M. Development of a Novel Vascular Simulator and Injury Model to Evaluate Smooth Muscle Cell Response following Balloon Angioplasty. Ann Vasc Surg. 2007; 21: 734-741.
31. Owens GK. Regulation of differentiation of vascular smooth muscle cells. Physiol Rev. 1995; 75: 487-517.
32. Yutani C, Imakita M, Ishibashi-Ueda H, Tsukamoto Y, Nishida N, Ikeda Y. Coronary atherosclerosis and interventions: Pathological sequences and restenosis. Pathol Int. 1999; 49: 273-290.
33. Watanabe T, Miyahara Y, Akishita M, Nakaoka T, Yamashita N, Iijima K, et al. Inhibitory effect of low-dose estrogen on neointimal formation after balloon injury of rat carotid artery. Eur J Pharmacol. 2004; 502: 265-270.
34. Pollman MJ, Hall JL, Gibbons GH. Determinants of Vascular Smooth Muscle Cell Apoptosis after Balloon Angioplasty Injury: Influence of Redox State and Cell Phenotype. Circ Res. 1999; 84: 113-121.
35. Perlman H, Maillard L, Krasinski K, Walsh K. Evidence for the Rapid Onset of Apoptosis in Medial Smooth Muscle Cells After Balloon Injury. Circulation. 1997; 95: 981-987.
36. Mori-Abe A, Tsutsumi S, Takahashi K, Toya M, Yoshida M, Du B, et al. Estrogen and raloxifene induce apoptosis by activating p38 mitogen-activated protein kinase cascade in synthetic vascular smooth muscle cells. J Endocrinol. 2003; 178: 417-426.
37. Montague CR, Hunter MG, Gavrilin MA, Phillips GS, Goldschmidt-Clermont PJ, Marsh CB. Activation of Estrogen Receptor Alpha Reduces Aortic Smooth Muscle Differentiation. Circ Res. 2006; 99: 477-484.
38. Gomez D, Owens GK. Smooth muscle cell phenotypic switching in atherosclerosis. Cardiovasc Res. 2012; 95: 156-164.
39. Murphy E. Estrogen Signaling and Cardiovascular Disease. Circ Res. 2011; 109: 687-696.







![A Casson Fluid Model for multiple Stenosed Artery in the ...e-jst.teiath.gr/issues/issue_42/Bali_42.pdf · non-Newtonian aspects of blood flow through stenosed arteries [18],flow](https://static.fdocument.org/doc/165x107/60f1e291199db767cb7d41fe/a-casson-fluid-model-for-multiple-stenosed-artery-in-the-e-jst-non-newtonian.jpg)





![arXiv:1711.01094v3 [cs.CV] 20 Mar 2018 · tation of cardiac SSFP images in an end-to-end di eren-tiable CNN framework, allowing for thelocalization, align-ment, and segmentation tasks](https://static.fdocument.org/doc/165x107/5fd1f014b0ebb801ad4c6f49/arxiv171101094v3-cscv-20-mar-2018-tation-of-cardiac-ssfp-images-in-an-end-to-end.jpg)