Mitochondrial dysfunction in benign prostatic hyperplasia ...

Rapid Efficacy of the Highly Selective �1A-Adrenoceptor Antagonist
Silodosin in Men With Signs and Symptoms of Benign Prostatic
Hyperplasia: Pooled Results of 2 Phase 3 Studies
Leonard S. Marks,*,† Marc C. Gittelman,‡ Lawrence A. Hill,‡ Weining Volinn‡and Gary Hoel‡From the University of California at Los Angeles and Urological Sciences Research Foundation, Los Angeles, California (LSM), South FloridaMedical Research, Aventura, Florida (MCG), and Watson Laboratories, Salt Lake City, Utah (LAH, WV, GH)
Abbreviations
and Acronyms
AE � adverse event
BPH � benign prostatichyperplasia
I-PSS � International ProstateSymptom Score
LOCF � last observation carriedforward
Qmax � peak urinary flow rate
QoL � quality of life
Submitted for publication November 11, 2008.Supported by Watson Pharma, Inc.Study received institutional review board ap-
proval.Clinical Trial Registration NCT00224107,
NCT00224120 (www.clinicaltrials.gov).* Correspondence: Department of Urology,
Geffen School of Medicine at UCLA, 3831 HughesAve., Culver City, California 90232 (telephone: 310-559-9800; FAX: 310-559-7821; e-mail: [email protected]).
† Financial interest and/or other relationshipwith Allergan, American Medical Systems, Astellas,Bayer, Beckman Coulter, Diagnostic Ultrasound,GTX, GlaxoSmithKline, Gen-Probe, Indevus, LightSciences Oncology, Lilly/ICOS, Merck, Novartis,Onconome, Pfizer, Sanofi, Solvay, Watson, NationalInstitutes of Health, CapCURE, Pardee Foundationand Seder Foundation.
‡ Financial interest and/or other relationshipwith Watson Pharmaceuticals.
Purpose: We evaluated the efficacy and safety of silodosin for treatment ofbenign prostatic hyperplasia symptoms in 2 randomized, placebo controlled,phase 3 studies.Materials and Methods: Men 50 years or older with an International ProstateSymptom Score of 13 or greater and peak urinary flow rate of 4 to 15 ml persecond received placebo or 8 mg silodosin daily with breakfast for 12 weeks. Theprimary end point was International Prostate Symptom Score change from base-line to last observation. Change in peak urinary flow rate was a secondary endpoint. Differences in treatment efficacy were assessed by ANCOVA.Results: Of 923 patients (mean age 65 years) 466 received silodosin and 457placebo. After 0.5 week (range 3 to 4 days) of treatment patients receivingsilodosin vs placebo achieved significant improvement in total InternationalProstate Symptom Score (difference �1.9, p �0.0001) and irritative (–0.5,p � 0.0002) and obstructive (–1.4, p �0.0001) subscores. The mean � SD changefrom baseline in total International Prostate Symptom Score was �4.2 � 5.3 forsilodosin vs �2.3 � 4.4 for placebo. Differences (silodosin vs placebo) in Interna-tional Prostate Symptom Score and subscores increased by week 12 (p �0.0001).Mean change from baseline in peak urinary flow rate (ml per second) 2 to 6 hoursafter initial dose was greater (p �0.0001) with silodosin (2.8 � 3.4) than placebo(1.5 � 3.8). Differences remained significant (p �0.001) through week 12. Themost common treatment emergent adverse event was (mostly mild) retrogradeejaculation (silodosin 28.1% of patients, placebo 0.9%). Few patients receivingsilodosin (2.8%) discontinued because of retrograde ejaculation. Proportions ofpatients with treatment emergent orthostatic hypotension were similar for silo-dosin (2.6%) and placebo (1.5%).Conclusions: Treatment with silodosin produced rapid improvement in urinarysymptoms that was sustained for 12 weeks. Silodosin was well tolerated with alow incidence of orthostatic hypotension.
For another article on a related
topic see page 2780.
Key Words: prostatic hyperplasia, KMD 3213, signs and symptoms
S122 www.jurology.com
Please cite this article a
BENIGN prostatic hyperplasia is a chroniccondition associated with lower urinarytract symptoms. The prevalence of symp-
tomatic BPH in the United States rangess J Urol 2013;189: S122-S128. DOI: http://dx.do
0022-5347/13/1891-0122/0THE JOURNAL OF UROLOGY®
© 2013 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RES
from approximately 24% in men 40 to 49years old to approximately 44% in men70 years old or older.1 With an aging pop-
ulation the number of men affected byi.org/10.1016/j.juro.2012.11.020
http://dx.doi.org/10.1016/j.juro.2012.11.020Vol. 189, S122-S128, January 2013
EARCH, INC. Printed in U.S.A.

EFFICACY AND SAFETY OF �-BLOCKER SILODOSIN S123
BPH is likely to increase.2 Although prostate enlarge-ment is a frequent sign of BPH, the severity of BPHrelated urinary symptoms generally correlates poorlywith prostate size or the extent of bladder outlet ob-struction.2,3 Symptom severity appears to be depen-dent, at least in part, on smooth muscle tone in theprostate and bladder neck.3,4 In vitro studies usinghuman prostate tissue have demonstrated thatsmooth muscle tone is mediated by �1A-adrenoceptors,which are abundant in the prostate and the bladderneck.5 Consequently �1-adrenoceptor antagonists (�-blockers) have become the first line treatment for therelief of BPH symptoms. First generation �-blockerssuch as doxazosin have the potential to cause ortho-static hypotension in normotensive subjects, becausethey block not only �1A-adrenoceptors but also �1B-adrenoceptors, which help maintain vascular smoothmuscle tone.6,7 Concerns about the cardiovascularsafety of such agents prompted the development of�-blockers with increased �1A to �1B-adrenoceptor sub-type selectivity.4,8 Nonclinical and clinical pharmacol-ogy data suggest that more selective �-blockers areless likely than nonselective �-blockers to cause car-diovascular adverse effects.4,9 Preclinical studies of therecently developed �-blocker silodosin indicate thatsilodosin has greater �1A to �1B-adrenoceptor subtypeselectivity10,11 and greater selectivity for prostatic andurethral tissues vs vascular tissue7,12,13 than does anyother currently available �-blocker. Furthermore, un-like other �-blockers that require a waiting period be-tween meals and dosing, silodosin is a once daily medi-cation taken with a meal. In this article we presentpooled results from 2 phase 3 clinical studies evaluat-ing the efficacy and safety of silodosin in a large pop-ulation of men with signs and symptoms of BPH.
MATERIALS AND METHODS
Patients and Study DesignTwo 12-week, identically designed, parallel group, mul-ticenter, randomized, double-blind, placebo controlledphase 3 studies (SI04009, SI04010; Clinical Trials Regis-tration Numbers NCT00224107, NCT00224120) were con-ducted in the United States to evaluate the efficacy andsafety of silodosin in men with signs and symptoms ofBPH. Screening of patients began for both studies in May2005, and the last patients completed the studies in Au-gust 2006 (SI04009) and May 2006 (SI04010). Both stud-ies were approved by central or local institutional reviewboards before patient enrollment began, and were con-ducted in accordance with good clinical practice as de-scribed in the guidelines of the International Conferenceon Harmonization (Technical Requirements for Registra-tion of Pharmaceuticals for Human Use), the UnitedStates Code of Federal Regulations governing the protec-tion of human subjects and the Declaration of Helsinki.
Eligible men were at least 50 years old with an I-PSS of
13 or higher, a peak urinary flow rate of 4 to 15 ml persecond and a post-void residual volume less than 250 ml.Complete exclusion criteria are provided in the Appendix.Concomitant medications precluding study participationand prohibited during the trial were �-adrenoceptor an-tagonists and 5�-reductase inhibitors. Diuretics, antispas-modics and anticholinergics were allowed only if doseswere stable during the study.
After a screening period of up to 4 weeks patientsreceived single-blind treatment with placebo for 4 weeks,which was followed immediately by the 12-week double-blind treatment period. Two weeks after the start and atthe end of the placebo run-in period, I-PSS and Qmax weredetermined to assess individual responses to placebo. Pa-tients with at least a 30% decrease in I-PSS or an increasein Qmax of 3 ml per second or greater during the run-inperiod were excluded from randomization. Eligible pa-tients were randomly assigned (1:1) to double-blind treat-ment with placebo or 8 mg silodosin once daily with break-fast. Treatment assignments were made according to arandomization schedule using PROC PLAN in SAS®, ver-sion 8.2. Randomization was performed with a permutedblock design and was not stratified by treatment center orregion. Blinding was maintained throughout the study bythe use of identical medication packaging with placebomatching silodosin in size and external appearance.Emergency information labels that indicated the patient’sassigned treatment were available to the investigator shouldknowledge of treatment assignment be needed to ensure thepatient’s well-being. If unblinding of the investigator, sitepersonnel or the patient was required in a particular casethat patient was to be discontinued from the study.
AssessmentsTotal I-PSS, irritative and obstructive I-PSS subscores,and QoL related to urinary symptoms were measured atweeks 0 (baseline), 0.5, 1, 2, 4 and 12. QoL was assessedwith use of the separately scored I-PSS question 8, “If youwere to spend the rest of your life with your urinarycondition the way it is now, how would you feel aboutthat?” (Responses were measured on a scale from 0 to 6,from delighted to terrible.) Qmax was assessed at baseline,2 to 6 hours after the first dose, and at weeks 1, 2, 4 and12. For all patients in both studies investigators deter-mined and reported urinary flow measurements. Subse-quently all urinary flow measurements were assessedagain by a blinded central reader (MCG) and any conflictswere resolved in discussion with the investigator. AE re-ports were collected at every visit except at post-random-ization week 0.5. Additional safety assessments included12-lead electrocardiograms, clinical laboratory tests andvital sign measurements including postural hypotensiontests and physical examinations.
Statistical AnalysisPooled data from the 2 studies were used for all analyses.Justification for sample sizes is provided in the Appendix.All randomized study participants who provided baselinedata for the primary efficacy variable were included in theefficacy analyses. The primary efficacy end point wasthe mean change from baseline to week 12 in total I-PSS. Thesecondary efficacy end point was mean change in Qmax
from baseline to week 12. Last observations were carried
forward to impute values missing for week 12. Safety
EFFICACY AND SAFETY OF �-BLOCKER SILODOSINS124
evaluations were based on all randomized study partici-pants who received at least 1 dose of a study drug (silodo-sin or placebo). Differences between treatment groupswere evaluated by ANCOVA with baseline measure usedas the covariate and treatment effect for each efficacyvariable included in the model. Results of these analyseswere calculated as adjusted means with 95% CI. A 2-sidedsignificance level of 5% was applied for all statistical tests.
RESULTS
Patient Disposition and Demographics
A total of 923 patients participated in the 2 stud-ies, 457 received placebo and 466 received 8 mg
Randomized 923
Completed 419 (91.7%)
Lost to follow-up 3 (0.7%)
Discontinued due to
Adverse events 10 (2.2%)
Protocol violation 3 (0.7%)
Voluntary withdrawal 14 (3.1%)Lack of efficacy 2 (0.4%)
Other reasons 6 (1.3%)
Placebo 457
Assessed for eligibility 2849
Discontinued/lost to follow-up 38 (8.3%)
Safety analysis 457Efficacy analysis 457
Entered placebo run-in 1538
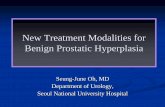
Figure 1. Flow diagram of
silodosin once daily (fig. 1). The 2 treatmentgroups had similar demographic characteristics(table 1). Most patients were white (89.3%). Meanage was 65 years, 45.0% of the patients were 65years old or older and 12.5% were 75 years old orolder. The overall proportion of patients who dis-continued was slightly higher among those receiv-ing silodosin (53 of 466, 11.4%) than among thosegiven placebo (38 of 457, 8.3%). Discontinuation bypatients receiving silodosin was most often attrib-utable to AEs (6.4%), voluntary withdrawal(1.3%), loss to followup (1.3%) and other reasons(1.3%). Discontinuation by those receiving placebo
Silodosin 466
Completed 413 (88.6%)
Lost to follow-up 6 (1.3%)
Discontinued due to
Adverse events 30 (6.4%)
Protocol violation 3 (0.6%)
Voluntary withdrawal 6 (1.3%)Lack of efficacy 6 (1.3%)
Other reasons 6 (1.3%)
Discontinued/lost to follow-up 53 (11.4%)
Safety analysis 466Efficacy analysis 466
Excluded during placebo run-in 615
Adverse event 21 (3.4%)
Investigator recommendation 20 (3.3%)
Lack of efficacy 3 (0.5%)
Lost to follow-up 8 (1.3%)Protocol violation 16 (2.6%)
Voluntary withdrawal 50 (8.1%)
)%8.08(794rehtO
patient disposition

EFFICACY AND SAFETY OF �-BLOCKER SILODOSIN S125
was most often attributable to voluntary withdrawal(3.1%), AEs (2.2%) and other reasons (1.3%).
Efficacy
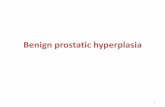
Patients in the silodosin and placebo groups hadsimilar baseline values for total I-PSS, irritative andobstructive I-PSS subscores, Qmax and QoL (I-PSSquestion 8) (table 1). At 0.5 week (ie 3 to 4 days) aftertreatment initiation (the earliest time of efficacyassessment) patients receiving silodosin achievedsignificant (p �0.0005) improvement (mean changefrom baseline � SD) in total I-PSS (�4.2 � 5.26 vsplacebo �2.3 � 4.37), and in irritative (�1.4 � 2.35vs placebo �0.8 � 2.16) and obstructive (�2.8 � 3.55vs placebo �1.4 � 2.99) I-PSS subscores (table 2,fig. 2, A to C). At week 12 including LOCF thedifferences in symptom improvement between pa-tients receiving silodosin and those receiving placebohad further increased with highly significant (p�0.0001) treatment effects noted for total I-PSS(�6.4 � 6.63 vs placebo �3.5 � 5.84), and irritative(�2.3 � 2.93 vs placebo �1.4 � 2.66) and obstructive(�4.0 � 4.31 vs placebo �2.1 � 3.76) subscores(table 2, fig. 2, A to C).
Rapid onset of improvement also was observed forQmax. Urinary flow measurements made 2 to 6 hoursafter patients received the first dose of medicationdemonstrated that those receiving silodosin had asignificantly (p �0.0001) higher increase from base-line in mean Qmax (2.8 � 3.44) than did those receiv-ing placebo (1.5 � 3.76). Overall this improvementwas sustained for the duration of the 12-week study
Table 1. Patient characteristics at baseline
Silodosin Placebo
No. pts 466 457No. race (%):
Black 14 (3.0) 22 (4.8)Asian 5 (1.1) 6 (1.3)White 425 (91.2) 399 (87.3)Hispanic 20 (4.3) 25 (5.5)Other 2 (0.4) 5 (1.1)
Age:Mean (SD) 64.6 (8.1) 64.7 (8.1)Range 50.2–86.1 44.9*–86.8
No. age (%):Younger than 65 259 (55.6) 249 (54.5)65 or Older 207 (44.4) 208 (45.5)Younger than 75 406 (87.1) 402 (88.0)75 or Older 60 (12.9) 55 (12.0)
Mean (SD) kg wt 89.7 (16.2) 89.1 (14.7)Mean (SD) cm ht 176.9 (7.3) 176.9 (7.3)Mean (SD) I-PSS 21.3 (5.1) 21.3 (4.9)Mean (SD) I-PSS irritative subscore 9.3 (2.6) 9.3 (2.5)Mean (SD) I-PSS obstructive subscore 12.0 (3.6) 12.0 (3.5)Mean (SD) Qmax 8.7 (2.6) 8.9 (2.8)
* One patient in the placebo group was 44.9 years old, which was younger thanthe age range stipulated in the protocol (50 years or older).
(LOCF, silodosin 2.6 � 4.43 vs placebo 1.5 � 4.36,
p � 0.0007) (table 2, fig. 2, D). During the course ofthe study QoL improved to a greater extent in pa-tients receiving silodosin than in those receivingplacebo (table 3). The percentage of patients de-lighted, pleased or mostly satisfied with the prospectof living with their current urinary condition for therest of their lives increased from 6.9% (32 of 466) to32.0% (149 of 466) in the silodosin group and from7.2% (33 of 457) to 22.5% (103 of 457) in the placebogroup.
Safety and Tolerability
Of the 923 patients 168 (36.8%) who received pla-cebo experienced 259 AEs and 257 (55.2%) who re-ceived silodosin experienced 462 AEs. Few patients(ie 7 [1.5%] in the placebo group and 6 [1.3%] in thesilodosin group) experienced serious AEs of which 1event was considered possibly drug (silodosin or pla-cebo) related. This event, a case of suspected syn-cope, occurred in an 85-year-old patient who re-ceived silodosin and was also taking the �-blockerprazosin. The use of prazosin, which usually is pre-scribed for hypertension and is well-known for itspotential to cause syncope, was prohibited in thestudy protocol.14 The most common treatment emer-gent AE was retrograde ejaculation, which was re-ported by 28% of patients who received silodosin(table 4). For most of these patients (79%) the eventswere mild. Only 2.8% of patients who received silo-dosin discontinued treatment because of retrogradeejaculation. The percentage with treatment emer-gent orthostatic hypotension was similar among pa-
Table 2. Summary of changes from baseline at weeks 0.5and 12
Mean (SD) Change FromBaseline Difference Silodosin vs Placebo
Efficacy Variable Silodosin PlaceboAdjusted
Mean (95% CI) p Value
Total I-PSS:Wk 0.5 �4.2 (5.26) �2.3 (4.37) �1.9 (�2.5, �1.3) �0.0001Wk 12 �6.4 (6.63) �3.5 (5.84) �2.8 (�3.6, �2.0) �0.0001
I-PSS irritativesubscore:
Wk 0.5 �1.4 (2.35) �0.8 (2.16) �0.5 (�0.8, �0.3) 0.0002Wk 12 �2.3 (2.93) �1.4 (2.66) �1.0 (�1.3, �0.6) �0.0001
I-PSS obstructivesubscore:
Wk 0.5 �2.8 (3.55) �1.4 (2.99) �1.4 (�1.8, �1.0) �0.0001Wk 12 �4.0 (4.31) �2.1 (3.76) �1.9 (�2.4, �1.4) �0.0001
Qmax (ml/sec):2–6 Hrs after
first dose2.8 (3.44) 1.5 (3.76) 1.3 (0.9, 1.8) �0.0001
Wk 12 2.6 (4.43) 1.5 (4.36) 1.0 (0.4, 1.5) 0.0007
Data analysis for week 12 was based on LOCF.

EFFICACY AND SAFETY OF �-BLOCKER SILODOSINS126
tients receiving placebo (1.5%) and those receivingsilodosin (2.6%) (table 4).
DISCUSSION
Combined data from 2 phase 3 studies enrollingmore than 900 patients with symptoms of BPHshowed that 12-week treatment with silodosin re-
BL LOC214215.0
Week
Total I-PSS
–10
–8
–6
–4
–2
0
Mea
n C
hang
e Fr
om B
asel
ine
PlaceboSilodosin
A
C
BL LOC214215.0
Week
–5
–3
–1
0
Mea
n C
hang
e Fr
om B
asel
ine
PlaceboSilodosin
I-PSS Obstructive Subscore
–4
–2
Figure 2. Mean changes from baseline (BL) in total I-PSS (A), I-PEarliest post-dose I-PSS measurements occurred at week 0.5 aninitial dosing. At all times differences between silodosin and plasubscore (p �0.001), obstructive subscore (p �0.0001) and Qm
ments were based on observed cases except where indicated.
Table 3. Summary of QoL related to urinary symptoms
No.Silodosin (%)
No.Placebo (%)
Baseline:Delighted, pleased or mostly satisfied 32 (6.9) 33 (7.2)Mixed about equally satisfied � dissatisfied 126 (27.0) 124 (27.1)Mostly dissatisfied, unhappy or terrible 308 (66.1) 300 (65.6)
Wk 12:Delighted, pleased or mostly satisfied 149 (32.0) 103 (22.5)Mixed about equally satisfied � dissatisfied 141 (30.3) 110 (24.1)Mostly dissatisfied, unhappy or terrible 176 (37.8) 244 (53.4)
Data analysis for week 12 was based on LOCF.
sulted in significant, rapid and sustained improve-ment in lower urinary tract symptoms as assessedby I-PSS, including irritative and obstructive sub-scores, and by Qmax. The onset of silodosin associ-ated effects was rapid. Significant improvement inQmax was observed 2 to 6 hours after initiation oftreatment, and significant reductions in total I-PSS,and in irritative and obstructive I-PSS subscoreswere observed by 3 to 4 days, when the first post-baseline assessment was conducted. These resultsare consistent with previously published data from aplacebo controlled phase 3 study conducted in Japan,where silodosin is currently marketed.15 In thatstudy patients with symptoms of BPH who weretreated with 4 mg silodosin twice daily showed sig-nificantly greater improvement in total I-PSS (vsplacebo) within 1 week. After 2 weeks of treatmentimprovement in I-PSS was also significantly greaterin the silodosin group than in a comparator grouptreated with the �1A-selective �-blocker tamsulosin
BL LOCF214215.0
Week
–3
–2
–1
0PlaceboSilodosin
I-PSS Irritative Subscore
BL LOCF21421h6-2
Week
0
1
3
4PlaceboSilodosin
Qmax
2
tative subscore (B), I-PSS obstructive subscore (C) and Qmax (D).iest post-dose Qmax measurements occurred 2 to 6 hours afterere statistically significant for total I-PSS (p �0.0001), irritative
0.005). Error bars indicate 95% confidence intervals. Measure-
F
Mea
n C
hang
e Fr
om B
asel
ine
B
D
F
Mea
n C
hang
e Fr
om B
asel
ine
SS irrid earlcebo w
ax (p �
(0.2 mg daily).

EFFICACY AND SAFETY OF �-BLOCKER SILODOSIN S127
Silodosin was safe and well tolerated. The onlyserious treatment emergent AE that occurred couldhave been attributable to concurrent use of another�-blocker that was prohibited in the study protocol.Retrograde ejaculation was the most common silo-dosin related AE (28%), leading to discontinuationin only 2.8% of patients treated with silodosin. Inthe Japanese study the percentage of patients re-ceiving silodosin who experienced abnormal ejacula-tion (22%) was similar to that in the present studyand the discontinuation rate due to abnormal ejac-ulation (2.9%) was equally low.15 Retrograde ejacu-lation is a characteristic adverse effect of �1A-selec-tive �-blockers4 that has been shown to be reversibleafter administration of the drug is stopped.16 In theoriginal phase 3 trials of tamsulosin (0.4 or 0.8 mgdaily) the percentages of patients receiving tamsu-losin who experienced abnormal ejaculation were8.4% (0.4 mg daily) and 18.1% (0.8 mg daily). It isworth noting that adherence to treatment with tam-sulosin at 1 and at 5 years was substantially greaterin patients who experienced abnormal ejaculationthan in those who did not.17
Although both of the studies reported here used arun-in period to exclude patients with substantialplacebo response, double-blind treatment with pla-cebo during 12 weeks improved I-PSS and Qmax. Aplacebo effect also was observed for QoL related tourinary symptoms (I-PSS question 8). Substantialplacebo effects despite the use of placebo run-in pe-riods also have been observed in double-blind, pla-cebo controlled studies of other �-blockers.18,19 A
Table 4. Summary of treatment emergent AEs occurringin more than 2% of patients receiving silodosin
Silodosin Placebo
Retrograde ejaculation:No. pts (%) 131 (28.1) 4 (0.9)No. events 134 4
Dizziness:No. pts (%) 15 (3.2) 5 (1.1)No. events 15 6
Orthostatic hypotension:No. pts (%) 12 (2.6) 7 (1.5)No. events 12 9
Diarrhea:No. pts (%) 12 (2.6) 6 (1.3)No. events 14 6
Nasopharyngitis:No. pts (%) 11 (2.4) 10 (2.2)No. events 11 10
Headache:No. pts (%) 11 (2.4) 4 (0.9)No. events 11 5
Nasal congestion:No. pts (%) 10 (2.1) 1 (0.2)No. events 11 1
Preferred terms from the Medical Dictionary for Regulatory Activities.
recent systematic literature review of studies of
medical therapy (including �-blockers) for BPHshowed that placebo responses of BPH related symp-toms and Qmax are common, may last 12 months orlonger and may lower baseline values for urinarysymptoms by up to 20%.20 Although the 4-week pla-cebo run-in period is a customary feature of clinicalstudies performed to evaluate the efficacy of ther-apies for BPH symptoms, this interval may be tooshort to allow identification of all patients whowould demonstrate a placebo response during sub-sequent treatment.
CONCLUSIONS
Silodosin, a selective �1A-adrenoceptor antagonist, sig-nificantly reduced signs and symptoms of BPH duringa period of 12 weeks. Significant changes were observedat the earliest post-baseline assessments. I-PSS, includ-ing irritative and obstructive subscores, improved sig-nificantly (p �0.0005) within 3 to 4 days. Moreoversignificant improvement (p �0.0001) in Qmax was ob-served 2 to 6 hours after the first dose of silodosin.Silodosin was safe and well tolerated. Retrograde ejac-ulation was the most common drug related AE but itrarely resulted in discontinuation of treatment. In addi-tion, silodosin had a low incidence of orthostatic hypoten-sion and was associated with few events of dizziness. Therapid onset of clinical efficacy established for silodosinwould make it a useful option for the treatment of pa-tients with signs and symptoms of BPH.
ACKNOWLEDGMENTS
Roland Tacke, PhD and Marsha Hall from ScientificConnexions (Newtown, Pennsylvania) provided as-sistance with funding from Watson Pharma, Inc.
APPENDIX
1) Exclusion criteria included intravesical obstruction unrelated to BPH; bladdercalculi; history of or current condition affecting bladder function; prior surgicalintervention to relieve BPH or bladder neck obstruction; active urinary tractinfection or history of recurrent urinary tract infection within the past 2 years;prostatitis within the past 3 months; BPH unrelated urinary retention withinthe past 3 months; and a history of recurring prostatitis (more than 3 timeswithin the past year), prior or current prostate cancer or prostate specificantigen greater than 10 ng/ml; prior invasive bladder cancer; bladder cathe-terization or bladder or prostate instrumentation within the past 30 days andhistory of or current significant postural hypotension, including changes in systolic(greater than 30 mm Hg) or diastolic (greater than 20 mm Hg) blood pressure or heartrate (more than 20 beats per minute), and lightheadedness, fainting, blurred vision,profound weakness or syncope upon change in position.
2) Sample size for each of the 2 studies was based on providing an adequatenumber of patients for a safety database to meet the regulatory requirement of atleast 100 patients exposed for 1 year and 300 patients for 6 months. By using thecommon standard deviation of 5.2 in change from baseline in I-PSS total scoreobserved in a pilot phase 2 study of silodosin in the United States (Study US021),a sample size of 240 subjects per treatment group with 90% power and � � 0.05would detect a difference of 1.54 of mean I-PSS change from baseline betweentreatment groups. Thus, this sample size would be sufficient to detect a clinically
21
meaningful difference in mean I-PSS of 2 to 2.5.
EFFICACY AND SAFETY OF �-BLOCKER SILODOSINS128
REFERENCES
1. Wei JT, Calhoun EA and Jacobsen SJ: Benignprostatic hyperplasia. In: Urologic Diseases inAmerica. Edited by MS Litwin and CS Saigal.Bethesda, MD: National Kidney and Urologic Dis-eases Information Clearinghouse; 2007. NIH pub-lication 07-5512: 43-67. Available at: http://kidney.niddk.nih.gov/statistics/uda/ (updatedFebruary 2007). Accessed August 28, 2008.
2. Lepor H: Pathophysiology of lower urinary tractsymptoms in the aging male population. Rev Urol2005; 7: S3.
3. Andersson KE and Gratzke C: Pharmacology of�1-adrenoceptor antagonists in the lower urinarytract and central nervous system. Nat Clin PractUrol 2007; 4: 368.
4. Schwinn DA and Roehrborn CG: �1-Adrenoceptorsubtypes and lower urinary tract symptoms. IntJ Urol 2008; 15: 193.
5. Marshall I, Burt RP and Chapple CR: Noradrena-line contractions of human prostate mediated by�1A-(�1c-)adrenoceptor subtype. Br J Pharmacol1995; 115: 781.
6. Hatano A, Takahashi H, Tamaki M, Komeyama T,Koizumi T and Takeda M: Pharmacological evi-dence of distinct �1-adrenoceptor subtypes me-diating the contraction of human prostatic ure-thra and peripheral artery. Br J Pharmacol 1994;113: 723.
7. Murata S, Taniguchi T, Takahashi M, Okada K,Akiyama K and Muramatsu I: Tissue selectivity ofKMD-3213, an �1-adrenoreceptor antagonist, inhuman prostate and vasculature. J Urol 2000;
164: 578.8. Chapple C and Andersson KE: Tamsulosin: anoverview. World J Urol 2002; 19: 397.
9. de Mey C, Michel MC, McEwen J and MorelandT: A double-blind comparison of terazosin andtamsulosin on their differential effects on ambu-latory blood pressure and nocturnal orthostaticstress testing. Eur Urol 1998; 33: 481.
10. Shibata K, Foglar R, Horie K, Obika K, SakamotoA, Ogawa S et al: KMD-3213, a novel, potent,�1a-adrenoceptor-selective antagonist: character-ization using recombinant human �1-adrenocep-tors and native tissues. Mol Pharmacol 1995; 48:250.
11. Yamada S, Okura T and Kimura R: In vivo dem-onstration of �1A-adrenoceptor subtype selectiv-ity of KMD-3213 in rat tissues. J Pharmacol ExpTher 2001; 296: 160.
12. Yamagishi R, Akiyama K, Nakamura S, Hora M,Masuda N, Matsuzawa A et al: Effect of KMD-3213, an �1a-adrenoceptor-selective antagonist,on the contractions of rabbit prostate and rabbitand rat aorta. Eur J Pharmacol 1996; 315: 73.
13. Akiyama K, Hora M, Tatemichi S, Masuda N,Nakamura S, Yamagishi R et al: KMD-3213, auroselective and long-acting �1a-adrenoceptorantagonist, tested in a novel rat model. J Phar-macol Exp Ther 1999; 291: 81.
14. Minipress (prazocin hydrochloride) prescribing infor-mation. MedWatch Web site. Available at http://www.fda.gov/medwatch/safety/2001/jun01.htm(updated June 2001). Accessed August 28, 2008.
15. Kawabe K, Yoshida M and Homma Y: Silodosin, a
new �1A-adrenoceptor-selective antagonist fortreating benign prostatic hyperplasia: results of aphase III randomized, placebo-controlled, double-blind study in Japanese men. BJU Int 2006; 98:1019.
16. Höfner K, Claes H, De Reijke TM, Folkestad B andSpeakman MJ: Tamsulosin 0.4 mg once daily:effect on sexual function in patients with lowerurinary tract symptoms suggestive of benignprostatic obstruction. Eur Urol 1999; 36: 335.
17. van Dijk MM, de la Rosette JJ and Michel MC:Effects of �1-adrenoceptor antagonists on malesexual function. Drugs 2006; 66: 287.
18. Roehrborn CG, Van Kerrebroeck P and Nordling J:Safety and efficacy of alfuzosin 10 mg once-dailyin the treatment of lower urinary tract symptomsand clinical benign prostatic hyperplasia: apooled analysis of three double-blind, placebo-controlled studies. BJU Int 2003; 92: 257.
19. Lepor H: Phase III multicenter placebo-controlledstudy of tamsulosin in benign prostatic hyperpla-sia. Tamsulosin Investigator Group. Urology 1998;51: 892.
20. Madersbacher S, Marszalek M, Lackner J, BergerP and Schatzl G: The long-term outcome of med-ical therapy for BPH. Eur Urol 2007; 51: 1522.
21. American Urological Association. Clinical Guide-lines: Management of BPH (’03/Updated ’06). Chap-ter 3 with Appendix: results of the treatment out-comes analyses. Available at http://www.auanet.org/content/guidelines-and-quality-care/clinical-guidelines.
cfm?sub�bph. Accessed December 3, 2008.