Radioimmunoassay of free β-subunit of human chorionic gonadotropin as a prognostic test for...
5
Radioimmunoassay of free of human chorionic gonadotropin as a prognostic test for persistent trophoblastic disease in molar pregnancy M. B. Khazaeli, Ph.D., M. M. Hedayat, M.D., K. D. Hatch, M.D., A. C. W. To, Ph.D., S.-j. Soong, Ph.D., H. M. Shingleton, M.D., L. R. Boots, Ph.D., and A. F. LoBuglio, M.D. Birmingham, Alabama A new radioimmunoassay system was established with a monoclonal antibody (1 E5) that distinguishes the free l3-subunit of human chorionic gonadotropin in the presence of intact human chorionic gonadotropin, showing only 0.23% cross-reactivity with the intact human chorionic gonadotropin molecule and virtually no cross-reactivity with other glycoprotein hormones or their l3-subunits. Serum samples, taken at initial diagnosis from nine patients with hydatidiform mole and spontaneous remission and 12 patients with subsequent progression to persistent trophoblastic disease, were assayed for free and total levels of the 13- subunit of human chorionic gonadotropin. The assay results were expressed as a ratio of nanograms of free l3-subunit per 1000 mlU of total l3-subunit. Eight of nine patients with mole and spontaneous remission had a ratio value <4 whereas 10 of 12 patients with subsequent persistent disease had a ratio value >4. Statistical analysis with x 2 showed a highly significant correlation of high ratios with eventual progressive disease (p = 0.0009). This study suggests that excessive production of the free l3-subunit of human chorionic gonadotropin may identify patients with a high likelihood of developing persistent trophoblastic disease. (AM J DesTET GVNECOL 1986;155:320-4.) Key words: Monoclonal antibodies; free l3-hCG, gestational trophoblastic disease, persistent Human chorionic gonadotrophin (hCG) is a glyco- protein hormone composed of two dissimilar non- covalently linked subunits of a- and l3-chains. The a-chain is nearly identical to and immunologically in- distinguishable from the a-subunit of some other pi- tuitary glycoprotein hormones, including luteinizing hormone, follicle-stimulating hormone, and thyroid- stimulating hormone. The l3-subunits of these hor- mones differ in their amino acid sequences and in this way confer unique immunologic and biologic activity to each hormone. I The l3-subunit of hCG (l3-hCG) con- tains an extended COOH terminal of 30 amino acid residues not present in luteinizing hormone or other hormones. Conventional l3-hCG assay systems use an- tibodies that are raised against the structural differ- ences conferred on l3-hCG by these unique amino acid sequences. 2 Today, these conventional l3-hCG assays, while specific for l3-hCG, do not discriminate the free l3-subunit of hCG from intact hCG molecules. We have From the Division of HematologylOncology and the Biostatistic Core Unit, Comprehensive Cancer Center, and the Divisions of Gyne- cologic Oncology and Reproductive Endocrinology and Biology, Department of Obstetrics and Gynecology, University of Alabama at Birmingham. Received for publication January 28, 1986; revised April 1, 1986; accepted April 16, 1986. Reprint requests: M. B. Khazaeli, Ph.D., Division of Hematology/ Oncology, Comprehensive Cancer Center, 223H Tumor Institute, University of Alabama at Birmingham, Birmingham, AL 35294. 320 developed a monoclonal antibody (l E5) that distin- guishes the free l3-hCG in the presence of hCG and shows only 0.23% cross-reactivity with the intact hCG molecule and virtually no cross-reactivity with other glycoprotein hormones or their l3-subunits. A radio- immunoassay system has been established with this an- tibody.' At the present time, serial determination of serum l3-hCG concentrations, including measurement of both intact and free l3-hCG, is the standard follow-up pro- cedure after the initial diagnosis and suction curettage of patients with hydatidiform mole.1-7 Approximately 85% of these patients undergo spontaneous remission as evidenced by a gradual fall in the serum l3-hCG level while 15% of patients develop persistent trophoblastic disease with a progressive rise in the serial levels. In either case, the level of l3-hCG is a function of the half life of serum hCG and the rate of production of hCG by the trophoblastic tissue remaining in the uterus. The hCG polypeptide and variable quantities of its subunits have been found in tumors containing tro- phoblastic tissue. Some tumors secrete only one form of the hCG subunits and others secrete a combination of the hormone and its subunits. Secretion of only the a-subunit of hCG in the absence of either l3-subunit or the intact hCG molecule has been reported in a tumor of the stomach. 8 Metastatic testicular choriocarcinoma also demonstrates differential production of hCG sub-
Transcript of Radioimmunoassay of free β-subunit of human chorionic gonadotropin as a prognostic test for...

Radioimmunoassay of free ~-subunit of human chorionic gonadotropin as a prognostic test for persistent trophoblastic disease in molar pregnancy
M. B. Khazaeli, Ph.D., M. M. Hedayat, M.D., K. D. Hatch, M.D., A. C. W. To, Ph.D., S.-j. Soong, Ph.D., H. M. Shingleton, M.D., L. R. Boots, Ph.D., and A. F. LoBuglio, M.D.
Birmingham, Alabama
A new radioimmunoassay system was established with a monoclonal antibody (1 E5) that distinguishes the free l3-subunit of human chorionic gonadotropin in the presence of intact human chorionic gonadotropin, showing only 0.23% cross-reactivity with the intact human chorionic gonadotropin molecule and virtually no cross-reactivity with other glycoprotein hormones or their l3-subunits. Serum samples, taken at initial diagnosis from nine patients with hydatidiform mole and spontaneous remission and 12 patients with subsequent progression to persistent trophoblastic disease, were assayed for free and total levels of the 13-subunit of human chorionic gonadotropin. The assay results were expressed as a ratio of nanograms of free l3-subunit per 1000 mlU of total l3-subunit. Eight of nine patients with mole and spontaneous remission had a ratio value <4 whereas 10 of 12 patients with subsequent persistent disease had a ratio value >4. Statistical analysis with x2 showed a highly significant correlation of high ratios with eventual progressive
disease (p = 0.0009). This study suggests that excessive production of the free l3-subunit of human chorionic gonadotropin may identify patients with a high likelihood of developing persistent trophoblastic
disease. (AM J DesTET GVNECOL 1986;155:320-4.)
Key words: Monoclonal antibodies; free l3-hCG, gestational trophoblastic disease, persistent
Human chorionic gonadotrophin (hCG) is a glycoprotein hormone composed of two dissimilar noncovalently linked subunits of a- and l3-chains. The a-chain is nearly identical to and immunologically indistinguishable from the a-subunit of some other pituitary glycoprotein hormones, including luteinizing hormone, follicle-stimulating hormone, and thyroidstimulating hormone. The l3-subunits of these hormones differ in their amino acid sequences and in this way confer unique immunologic and biologic activity to each hormone. I The l3-subunit of hCG (l3-hCG) contains an extended COOH terminal of 30 amino acid residues not present in luteinizing hormone or other hormones. Conventional l3-hCG assay systems use antibodies that are raised against the structural differences conferred on l3-hCG by these unique amino acid sequences.2 Today, these conventional l3-hCG assays, while specific for l3-hCG, do not discriminate the free l3-subunit of hCG from intact hCG molecules. We have
From the Division of HematologylOncology and the Biostatistic Core Unit, Comprehensive Cancer Center, and the Divisions of Gynecologic Oncology and Reproductive Endocrinology and Biology, Department of Obstetrics and Gynecology, University of Alabama at Birmingham.
Received for publication January 28, 1986; revised April 1, 1986; accepted April 16, 1986.
Reprint requests: M. B. Khazaeli, Ph.D., Division of Hematology/ Oncology, Comprehensive Cancer Center, 223H Tumor Institute, University of Alabama at Birmingham, Birmingham, AL 35294.
320
developed a monoclonal antibody (l E5) that distinguishes the free l3-hCG in the presence of hCG and shows only 0.23% cross-reactivity with the intact hCG molecule and virtually no cross-reactivity with other glycoprotein hormones or their l3-subunits. A radioimmunoassay system has been established with this antibody.'
At the present time, serial determination of serum l3-hCG concentrations, including measurement of both intact and free l3-hCG, is the standard follow-up procedure after the initial diagnosis and suction curettage of patients with hydatidiform mole.1-7 Approximately 85% of these patients undergo spontaneous remission as evidenced by a gradual fall in the serum l3-hCG level while 15% of patients develop persistent trophoblastic disease with a progressive rise in the serial levels. In either case, the level of l3-hCG is a function of the half life of serum hCG and the rate of production of hCG by the trophoblastic tissue remaining in the uterus.
The hCG polypeptide and variable quantities of its subunits have been found in tumors containing trophoblastic tissue. Some tumors secrete only one form of the hCG subunits and others secrete a combination of the hormone and its subunits. Secretion of only the a-subunit of hCG in the absence of either l3-subunit or the intact hCG molecule has been reported in a tumor of the stomach.8 Metastatic testicular choriocarcinoma also demonstrates differential production of hCG sub-
Volume 155 Number 2
Free l3-hC~ in persistent trophoblastic disease 321
Table I. Patients with hydatidiform mole who underwent spontaneous remission
Free {3-hCG Total {3-hCG ng Free Patient No. (nglml) (mlUlml) {3-hCGI1000 mlU keG
I 10.5 5,100 2.1 2 84.2 52,290 1.6 3 143.3 462,100 0.3 4 139.9 165,560 0.9 5 14.1 8,716 1.6 6 8.9 3,927 2.3 7 11.2 1,902 5.9 8 27.5 23,000 1.2 9 7.4 9,600 0.7
Mean ± SD 49.6 ± 57.3 81,355 ± 152,009 1.8 ± 1.7
Table II. Patients with hydatidiform mole who developed persistent trophoblastic disease
Free {3-hCG Patient No. (nglml)
I 4550 2 41.8 3 47.7 4 86.8 5 501 6 27.2 7 44.6 8 41.3 9 19.7
10 107.5 II 24.2 12 46.1
Mean ± SD 461 ± 1294
units with a high ratio of free J3-hCG to total hCG molecule compared with that of normal pregnant subjects." The intact hCG secreted by these neoplastic tissues has not been shown to be different from that found secreted by the normal placenta.
The known clinicopathologic features of hydatidiform mole coupled with the knowledge that unbalanced synthesis of hCG subunits can occur in tumors with trophoblastic elements suggested that the quantitative measurement of hCG subunits might be useful in the laboratory evaluation of patients with molar pregnancy. This retrospective study was designed to provide preliminary data on whether measurement of the free J3-hCG fraction in sera taken at the time of molar evacuation is useful in predicting which patients will develop persistent trophoblastic disease.
Material and methods Serum samples obtained at initial diagnosis of molar
pregnancy from 21 patients were selected from the serum bank of the Southern Regional Trophoblastic Disease Center. The selection was based on the patient having adequate serial follow-up to clearly delineate the eventual outcome in regard to spontaneous regression (nine patients) or persistent trophoblastic disease (12 patients). The serum specimens had been stored at
Total {3-hCG ng Free (mlUlml) {3-hCGI1000 mlU hCG
401,900 11.3 5,927 7.1
14,670 3.3 12,674 6.8
480,000 1.0 3,236 8.4 8,295 5.4 6,102 6.8 4,308 4.6
20,640 5.2 3,049 7.9 3,865 13.7
80,388 ± 169,322 6.8 ± 3.4
- 20° C for periods ranging from 2 to 5 years. Samples were assayed for free J3-hCG and total J3-hCG individually without knowledge of clinical outcome of the patients or assay results of either component; that is, free J3-hCG was assayed without knowledge of total J3-hCG determination.
The free J3-hCG assay was carried out by means of the double-antibody technique of Midgley. IO All reagents were diluted in phosphate-buffered saline containing 0.1 % gelatin. The monoclonal antibody to free J3-hCG produced in mice ascites was used at a dilution previously found to bind 30% of the added iodinated free J3-hCG. The total assay volume was kept constant at 1.0 ml and included the following: 0.1 ml of unlabeled free J3-hCG (standard) or samples; 0.1 ml of iodine 125-labeled free J3-hCG (50,000 cpm); 0.2 ml of lE5 monoclonal antibody diluted as mentioned above; 0.1 ml of normal mouse serum diluted at 1 : 100 in gelphosphate-buffered saline; 0.1 ml of normal human serum. Gel-phosphate-buffered saline was used to bring the total volume to 1.0 ml. For standards and nonspecific binding controls, normal human serum was diluted to match the dilution of samples used in the assay. This reaction mixture was incubated for a minimum of 4 hours at room temperature. Then 1 ml of the second antibody, sheep anti mouse )'-globulin, was
322 Khazaeli et al.
100
c 0 80 :; .J:l
",E 60 '" 0
Q) > . .;::: 40 E :J E :J
20 U
~ 0
0 0 2 3 4 5
hCG (mIU/ml) x 10 5
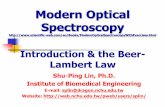
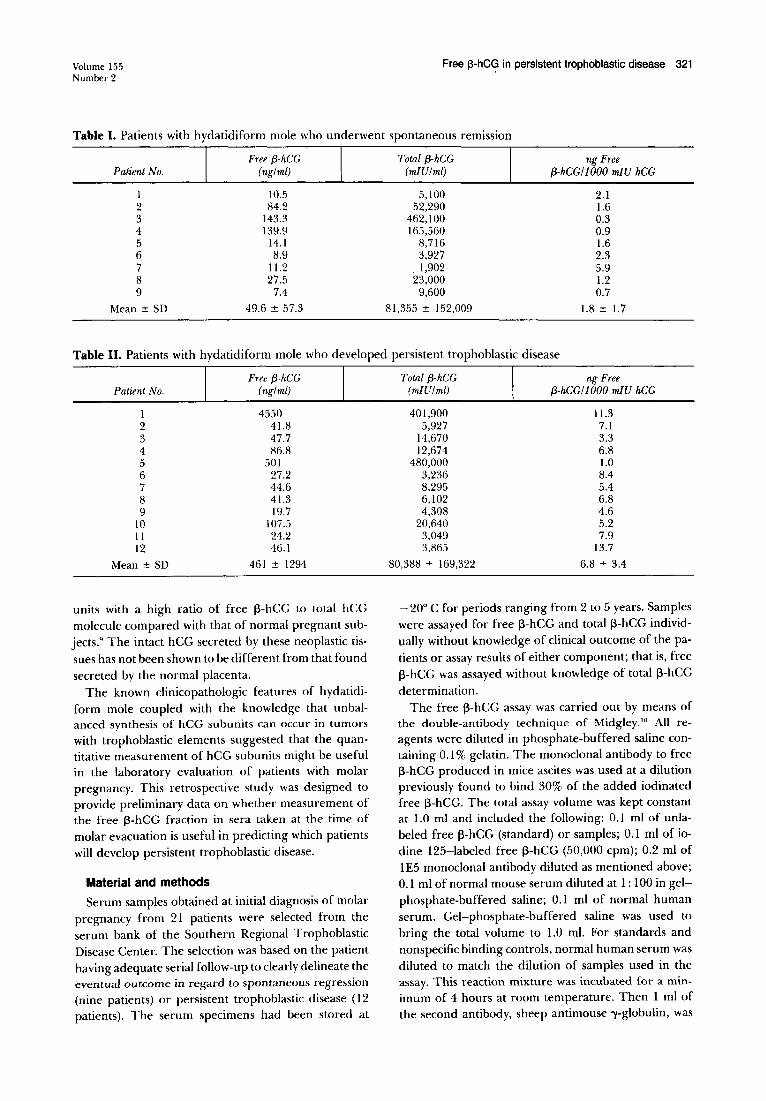
Fig. 1. Cumulative distribution of total hCG concentration in serum of patients with spontaneous remission (0) and those with subsequent persistent trophoblastic disease (D).
added at a dilution of 1: 100 in 2.5% polyethylene glycol and the incubation was continued for a minimum of 30 minutes at room temperature. Assay tubes were centrifuged at 7000 X gat 40 C for 20 minutes, decanted, and blotted, then counted in a Micromedics gamma counter (Micromedics Systems, Inc., Horsham, Pennsylvania). Data plots and calculations were performed on an MACC Micromedics computer interfaced with the gamma counter, with the use of a logit plot as previously described.'
Total/3-hCG was assayed with a commercially available immunoradiometric system for hCG (Serono Diagnostics, Randolph, Massachusetts). Patient samples, standards, and controls, respectively, were reacted with a mixture of three monoclonal antibodies to hCG. The antibodies reacted with both free /3-subunit and the intact hCG molecule. Two of the antibodies were labeled with 1251 and the third linked to fluorescein. Incubation was 15 minutes at 37° C. After incubation, antifluorescein coupled to a magnetic solid phase was added in large excess to bind to the hCG-monocional antibodies complex, which was precipitated in a magnetic field. The sensitivity of the assay is 5 mlU/ml of hCG. Calibration was against the first international reference preparation 75/537. Cross-reaction with luteinizing hormone and follicle-stimulating hormone was 0.55% and 0.68%, respectively. Precision of the assay, as expressed by interassay and intra-assay coefficients of variation, was < 10% each.
The results on each sample were analyzed as the amount of free /3-hCG (nanograms per milliliter), the amount of total /3-hCG (milli-international units per milliliter), and a ratio of nanograms of free /3-hCG per 1000 mIU ofhCG. The sensitivity (or true positive rate) of the test was defined as the proportion of patients who had progressive disease and who were correctly identified by the test. The specificity (or true negative
c S? :J
.J:l . .:
100
80
August 1986 Am J Obstet Gynecol
1
Vi 60 0 Q) >
40 0
:J E :J
20 U
~ 0
O~~~~~~~~~~~~~-L~~~~
o 20 40 60 80 100 120 140 160 180 200
Free (3 hCG (ng/mg)
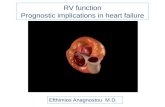
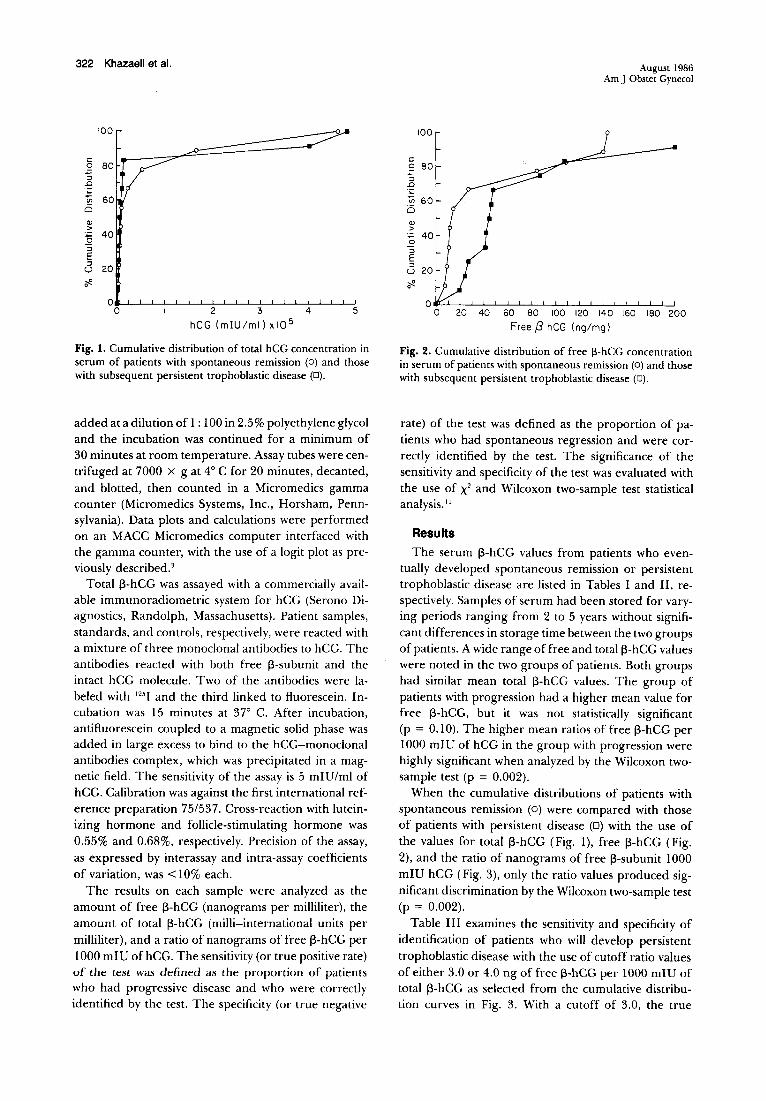
Fig. 2. Cumulative distribution of free l3-hCG concentration in serum of patients with spontaneous remission (0) and those with subsequent persistent trophoblastic disease (D).
rate) of the test was defined as the proportion of patients who had spontaneous regression and were correctly identified by the test. The significance of the sensitivity and specificity of the test was evaluated with the use of X2 and Wilcoxon two-sample test statistical analysis. 11
Results
The serum /3-hCG values from patients who eventually developed spontaneous remission or persistent trophoblastic disease are listed in Tables I and II, respectively. Samples of serum had been stored for varying periods ranging from 2 to 5 years without significant differences in storage time between the two groups of patients. A wide range of free and total/3-hCG values were noted in the two groups of patients. Both groups had similar mean total /3-hCG values. The group of patients with progression had a higher mean value for free /3-hCG, but it was not statistically significant (p = 0.10). The higher mean ratios of free /3-hCG per 1000 mlU of hCG in the group with progression were highly significant when analyzed by the Wilcoxon twosample test (p = 0.002).
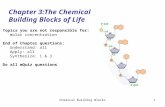
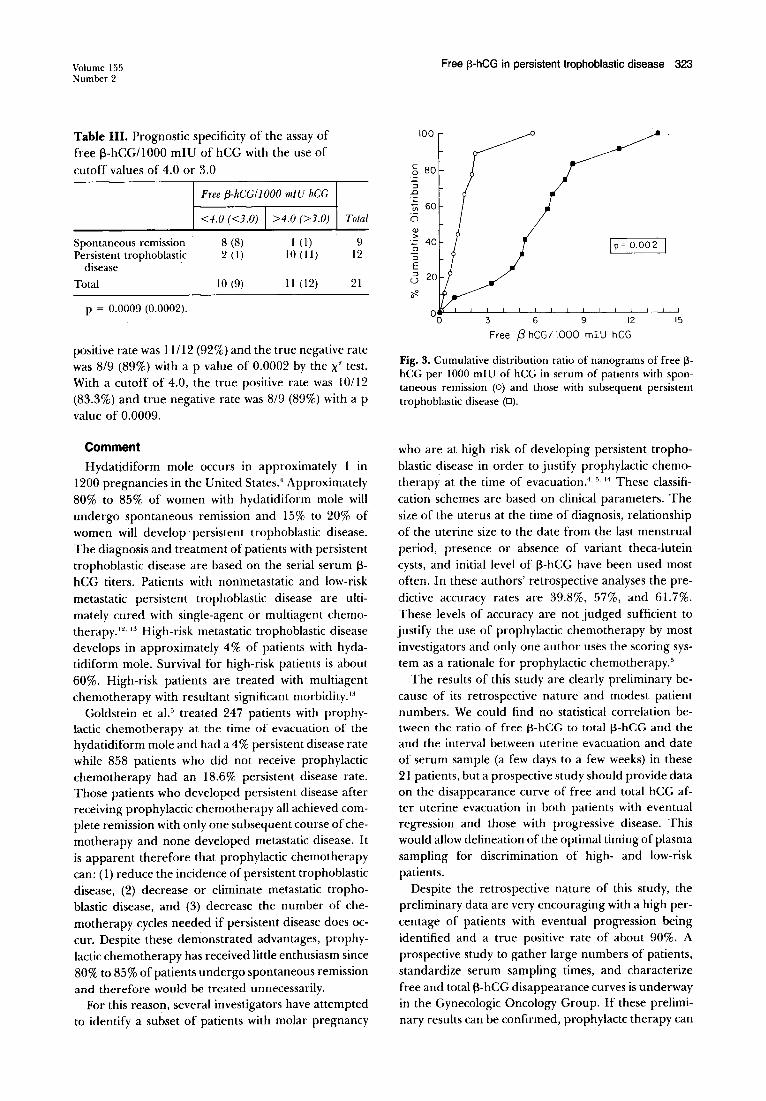
When the cumulative distributions of patients with spontaneous remission (0) were compared with those of patients with persistent disease (D) with the use of the values for total /3-hCG (Fig. I), free /3-hCG (Fig. 2), and the ratio of nanograms of free /3-subunit 1000 mlU hCG (Fig. 3), only the ratio values produced significant discrimination by the Wilcoxon two-sample test (p = 0.002).
Table III examines the sensitivity and specificity of identification of patients who will develop persistent trophoblastic disease with the use of cutoff ratio values of either 3.0 or 4.0 ng of free /3-hCG per 1000 mIU of total /3-hCG as selected from the cumulative distribution curves in Fig. 3. With a cutoff of 3.0, the true
Volume 155 Number 2
Table III. Prognostic specificity of the assay of free l3-hCG11000 mlU of hCG with the use of cutoff values of 4.0 or 3.0
Spontaneous remission Persistent trophoblastic
disease Total
p = 0.0009 (0.0002).
Free (3-hCG/J 000 mlU hCG
<4.0 «3.0) I >4.0 (>3.0)
8 (8) I (I) 2(1) 10(11)
10 (9) 11 (12)
Total
9 12
21
positive rate was 11112 (92%) and the true negative rate was 8/9 (89%) with a p value of 0.0002 by the X" test. With a cutoff of 4.0, the true positive rate was 10112 (83.3%) and true negative rate was 8/9 (89%) with a p value of 0.0009.
Comment
Hydatidiform mole occurs in approximately 1 in 1200 pregnancies in the United States.' Approximately 80% to 85% of women with hydatidiform mole will undergo spontaneous remission and 15% to 20% of women will develop persistent trophoblastic disease. The diagnosis and treatment of patients with persistent trophoblastic disease are based on the serial serum 13-hCG titers. Patients with nonmetastatic and low-risk metastatic persistent trophoblastic disease are ultimately cured with single-agent or multiagent chemotherapy. 12. 13 High-risk metastatic trophoblastic disease develops in approximately 4% of patients with hydatidiform mole. Survival for high-risk patients is about 60%. High-risk patients are treated with multiagent chemotherapy with resultant significant morbidity.13
Goldstein et al. 5 treated 247 patients with prophylactic chemotherapy at the time of evacuation of the hydatidiform mole and had a 4% persistent disease rate while 858 patients who did not receive prophylactic chemotherapy had an 18.6% persistent disease rate. Those patients who developed persistent disease after receiving prophylactic chemotherapy all achieved complete remission with only one subsequent course of chemotherapy and none developed metastatic disease. It is apparent therefore that prophylactic chemotherapy can: (1) reduce the incidence of persistent trophoblastic disease, (2) decrease or eliminate metastatic trophoblastic disease, and (3) decrease the number of chemotherapy cycles needed if persistent disease does occur. Despite these demonstrated advantages, prophylactic chemotherapy has received little enthusiasm since 80% to 85% of patients undergo spontaneous remission and therefore would be treated unnecessarily.
For this reason, several investigators have attempted to identify a subset of patients with molar pregnancy
Free [3-hCG in persistent trophoblastic disease 323
100
c 80 S? "'3 .Q
Vi 0 Q)
>
a :J
E :J
U
~ 0
3 6 9 12 15
Free f3 hCGI 1000 mlU hCG
Fig. 3. Cumulative distribution ratio of nanograms of free [3-hCG per 1000 mlU of hCG in serum of patients with spontaneous remission (0) and those with subsequent persistent trophoblastic disease (D).
who are at high risk of developing persistent trophoblastic disease in order to justify prophylactic chemotherapy at the time of evacuation. ' · 5. 11 These classification schemes are based on clinical parameters. The size of the uterus at the time of diagnosis, relationship of the uterine size to the date from the last menstrual period, presence or absence of variant theca-lutein cysts, and initial level of l3-hCG have been used most often. In these authors' retrospective analyses the predictive accuracy rates are 39.8%, 57%, and 61.7%. These levels of accuracy are not judged sufficient to justify the use of prophylactic chemotherapy by most investigators and only one author uses the scoring system as a rationale for prophylactic chemotherapy.5
The results of this study are clearly preliminary because of its retrospective nature and modest patient numbers. We could find no statistical correlation between the ratio of free f3-hCG to total f3-hCG and the and the interval between uterine evacuation and date of serum sample (a few days to a few weeks) in these 21 patients, but a prospective study should provide data on the disappearance curve of free and total hCG after uterine evacuation in both patients with eventual regression and those with progressive disease. This would allow delineation of the optimal timing of plasma sampling for discrimination of high- and low-risk patients.
Despite the retrospective nature of this study, the preliminary data are very encouraging with a high percentage of patients with eventual progression being identified and a true positive rate of about 90%. A prospective study to gather large numbers of patients, standardize serum sampling times, and characterize free and totall3-hCG disappearance curves is underway in the Gynecologic Oncology Group. If these preliminary results can be confirmed, prophylactc therapy can

Khazaeli et al.
be reevaluated with this assay to select high-risk patients and eventually change the clinical care of patients with molar pregnancy.
REFERENCES
I. Saxena BB, Rathman P. Activity relationships of protein and polypeptide hormones. In: Margulies M, Greenwood FC, eds. Amsterdam: Excerpta Medical Foundation, 1971:122.
2. Vaitukaitis JL, Braunstein GD, Ross CT. A radioimmunoassay which specifically measures human chorionic gonadotropin in the presence of human luteinizing hormone. AMJ OBSTET GYNECOL 1972;113:751-8.
3. Khazaeli MB, England BG, Dieterle RC, Nordblom GD, Kabza GA, Beierwaltes WHo Development and characterization of a monoclonal antibody which distinguishes the ~-subunit of human chorionic gonadotropin (~ hCG) in the presence of the hCG. Endocrinology 1981; 109: 1290-2.
4. Curry SL, Hammond CB, Tyrey L, Creasman WT, Parker RT. Hydatidiform mole: diagnosis, management and long-term follow-up of 347 patients. Obstet Gynecol 1975;45: 1-8.
5. Goldstein DP, Berkowitz RS, Bernstein MR. Management of molar pregnancy. J Reprod Med 1981 ;26:208-12.
6. Goldstein DP. Prevention of gestational trophoblastic disease by use of actinomycin D in molar pregnancies. Obstet GynecoI1974;43:475-9.
August 1986 Am J Obstet Gynecol
7. Hatch KD, Shingleton HM, Austin JM, Boots LR, Younger JB, Soong SJ. Southern regional trophoblastic disease center. South Med J 1978;71: 1334-40.
8. Rosen SW, Weintraub BD. Ectopic production of the isolated a-subunit of the glycoprotein hormone. N Engl J Med 1974;290:1441-7.
9. Khazaeli MB, Haghighi-Rad F, LaFeria JJ, Beierwaltes WHo Comparison of serum levels of human chorionic gonadotropin (hCG) and its free ~-subunit in normal and gestational trophoblastic disease using monoclonal antibodies [Abstract). J Reprod Immunol 1983;(suppl 112)5:102-3.
10. Midgley ARJr. Radioimmunoassay: a method for human chorionic gonadotropin and human luteinizing hormone. Endocrinology 1966;79: 105-18.
II. Ott L. In: An introduction to statistical methods and data analysis. North Scituate, Massachusetts: Duxbury Press, 1977:317.
12. Hammond CB, Parker RT. Diagnosis and treatment of trophoblastic disease. A report from the Southeastern Regional Center. Obstet Gynecol 1970;35: 132-41.
13. Hammond CB, Weed JC, Currie JL. The role of operation in the current therapy of gestational trophoblastic disease. AM J OBSTET GYNECOL 1980; 136:844-55.
14. Morrow CP, Kletzky OA, Disaia PJ, Townsend DE, Mishell DR, Nakamura RM. Clinical and laboratory correlates of molar pregnancy and trophoblastic disease. AMJ OBSTET GYNECOL 1977; 128 :424-9.
Methotrexate inhibition of normal trophoblasts in vitro
Peter K. Sand, M.D., Patricia A. Stubblefield, Ph.D., and Steven J. Ory, M.D.
Chicago, Illinois
Methotrexate is a folic acid inhibitor useful in the treatment of gestational trophoblastic disease. Its effect on normal trophoblast in vitro was studied to help establish a minimum effective dose in vivo for the
conservative treatment of ectopic pregnancy. In vitro inhibition of normal trophoblastic cell growth was measured after 48 hours of exposure to variable concentrations of methotrexate (10- 2 to 10-9moI/L) and rescue with leucovorin. A modification of Cotte's method of trophoblastic cell enrichment was used. Longterm (10 days) linear growth inhibition was observed at concentrations >10- 5mol/L. Leucovorin control cultures showed no inhibition of cell growth. The study demonstrates that methotrexate is effective in inhibiting normal trophoblastic cell culture growth in vitro at concentrations 1000 times those reported necessary to inhibit deoxyribonucleic acid synthesis in choriocarcinoma cell cultures. (AM J OaSTET
GVNECOL 1986;155:324-9.)
Key words: Methotrexate, trophoblast, tissue culture, and heG
The drug methotrexate (4-amino-4-deoxy-N 'O-methyl folic acid) is a tetrahydrofolate reductase inhibitor that blocks the formation of reduced folates nec-
From the Division of Endocrinology and Infertility, Department of Obstetrics and Gynecology, Northwestern University Medical School.
Receivedforpublicatianjanuary23, 1986; revised March 7,1986; accepted April 22, 1986.
Reprint requests: Peter K. Sand, M.D., 2880 Atlantic Ave., Suite 130, Long Beach, CA 90806.
324
essary for the transfer of one-carbon molecules. They are important in the biosynthesis of thymidylic acid and inosinic acid. Methotrexate, while S-phase specific in its inhibition of deoxyribonucleic acid synthesis, also acts throughout the cell cycle to inhibit amino acid interconversions. Its effects in vivo and in vitro on malignant trophoblasts have been studied extensively; however, no data are available regarding the effect of methotrexate on normal trophoblasts in vitro.
In vitro effects of methotrexate on choriocarcinoma