Παρουσίαση του εργαλείου Rundeck και use cases Αθήνα 16/01/2014
description
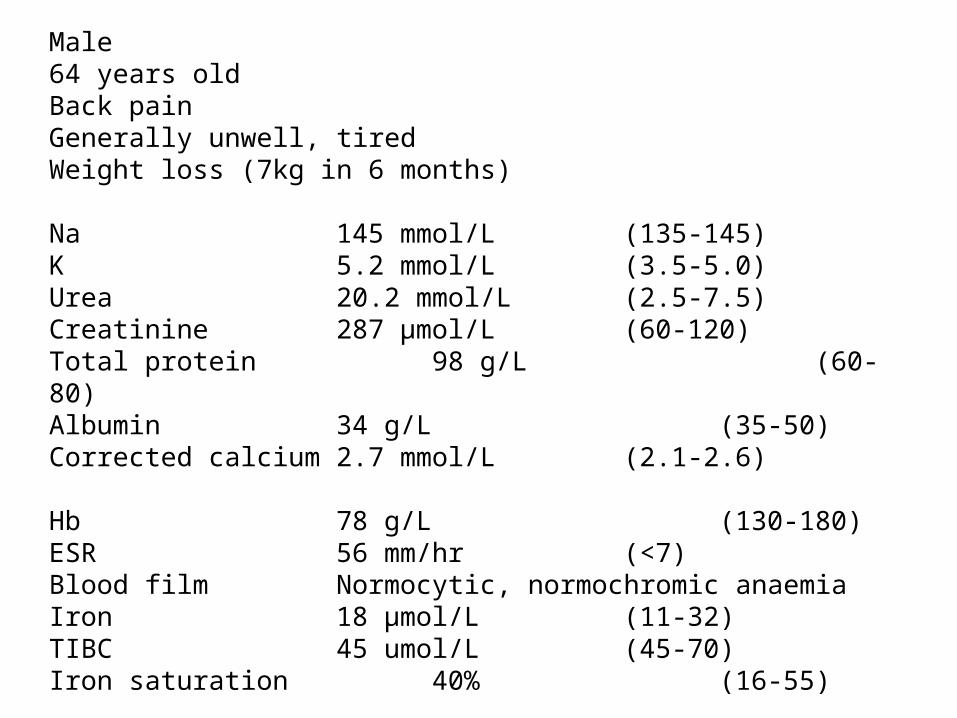
Male64 years oldBack painGenerally unwell, tiredWeight loss (7kg in 6 months)
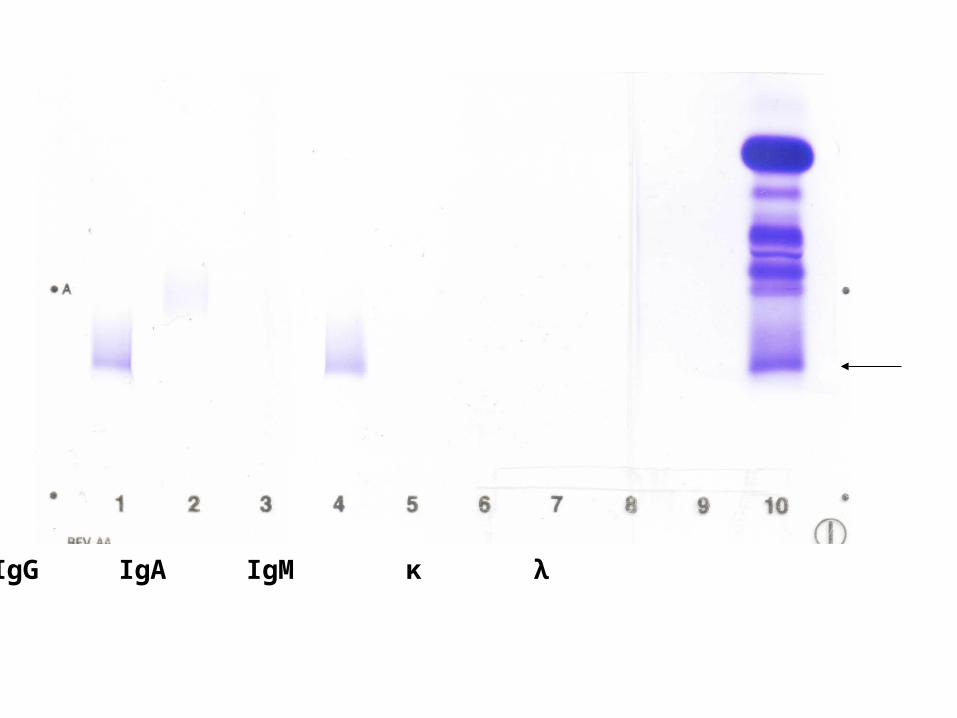
Na 145 mmol/L (135-145)K 5.2 mmol/L (3.5-5.0)Urea 20.2 mmol/L (2.5-7.5)Creatinine 287 μmol/L (60-120)Total protein 98 g/L (60-80)Albumin 34 g/L (35-50)Corrected calcium 2.7 mmol/L (2.1-2.6)
Hb 78 g/L (130-180)ESR 56 mm/hr (<7)Blood film Normocytic, normochromic anaemiaIron 18 μmol/L (11-32)TIBC 45 umol/L (45-70)Iron saturation 40% (16-55)
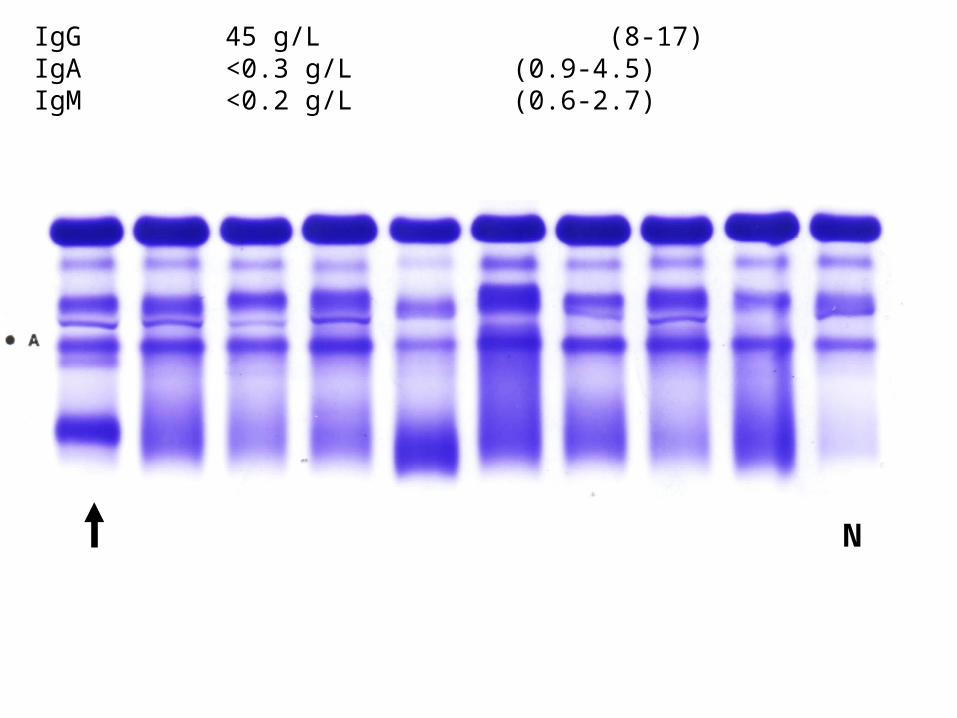
IgG 45 g/L (8-17)IgA <0.3 g/L (0.9-4.5)IgM <0.2 g/L (0.6-2.7)
N
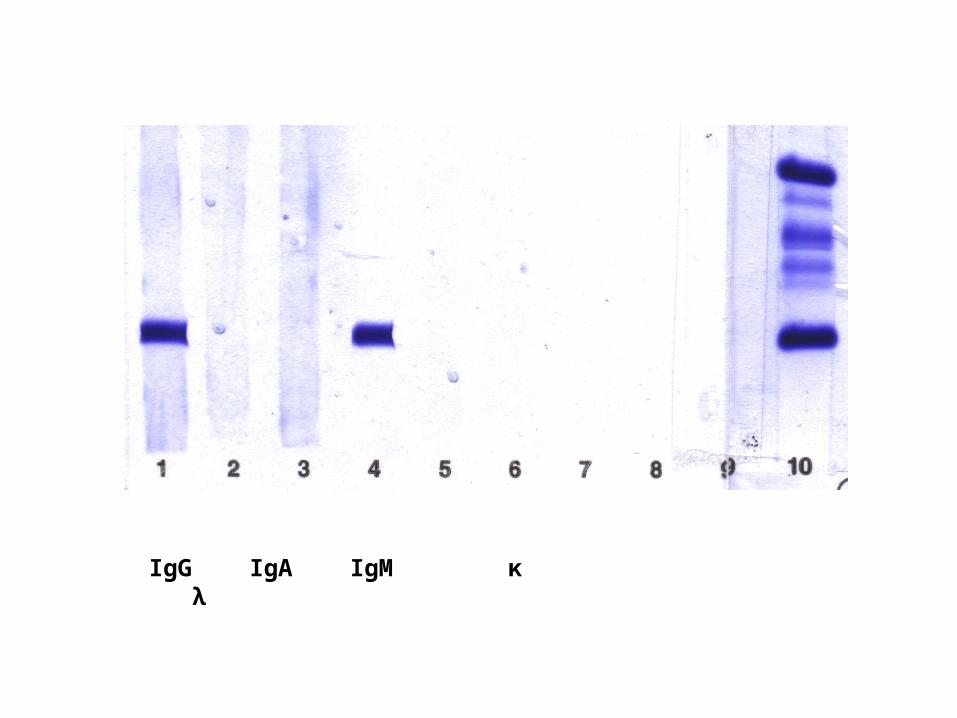
IgG IgA IgM κ λ
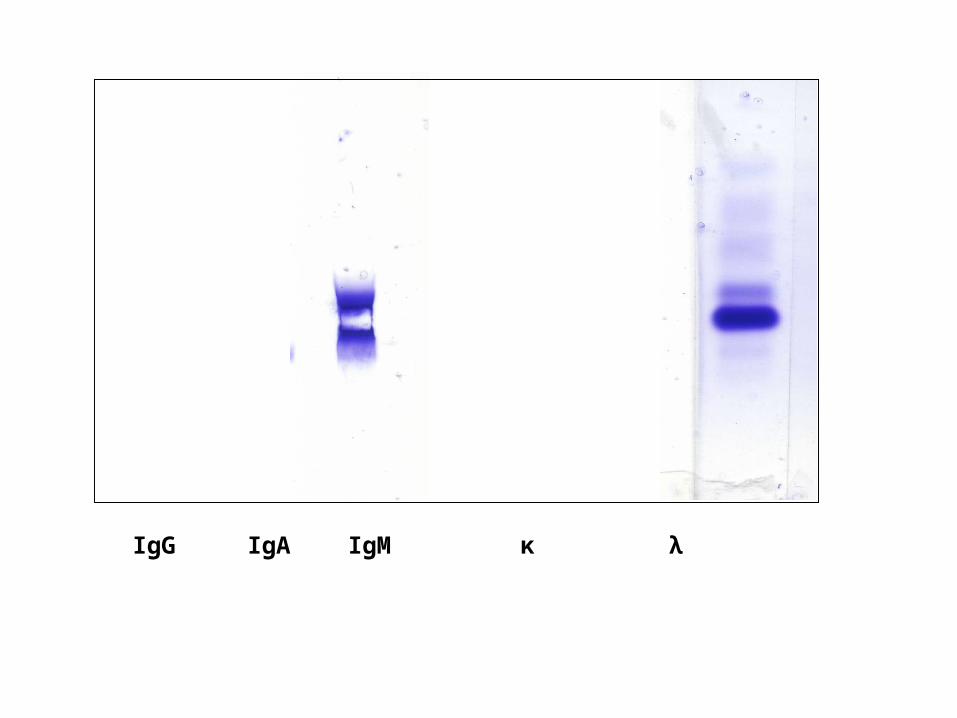
IgG IgA IgM κ λ
Further investigations
Bone marrow - increased numbers/atypical plasma cells
X-ray - skull, chest. Osteolytic lesions
Monoclonal gammopathies
•Monoclonal gammopathies of undetermined significance (62%)•Multiple myeloma (15%)•Amyloidosis (10%)•Waldenstroms macroglobulinaemia (3%)•Smouldering multiple myeloma (3-4%)•Lymphoproliferative disease (2.5%)•Solitary or extramedullary plasmacytoma (1.5%)•Other causes (2.5%)
Presentation of myeloma
•Bone pain (back or chest) – 60%•Weakness, fatigue (anaemia >60%)•Acute infections•Renal failure – creatinine >175 μmol/L in 20%•Hypercalcaemia – 15%•Serum paraprotein – 80% IgG 50%
IgA 20%BJP 20%IgD 2%Biclonal 1%
•Urine paraprotein – 75%•Serum or urine paraprotein – 98%, 2% non-secretory•Most have >10% plasma cells in bone marrow

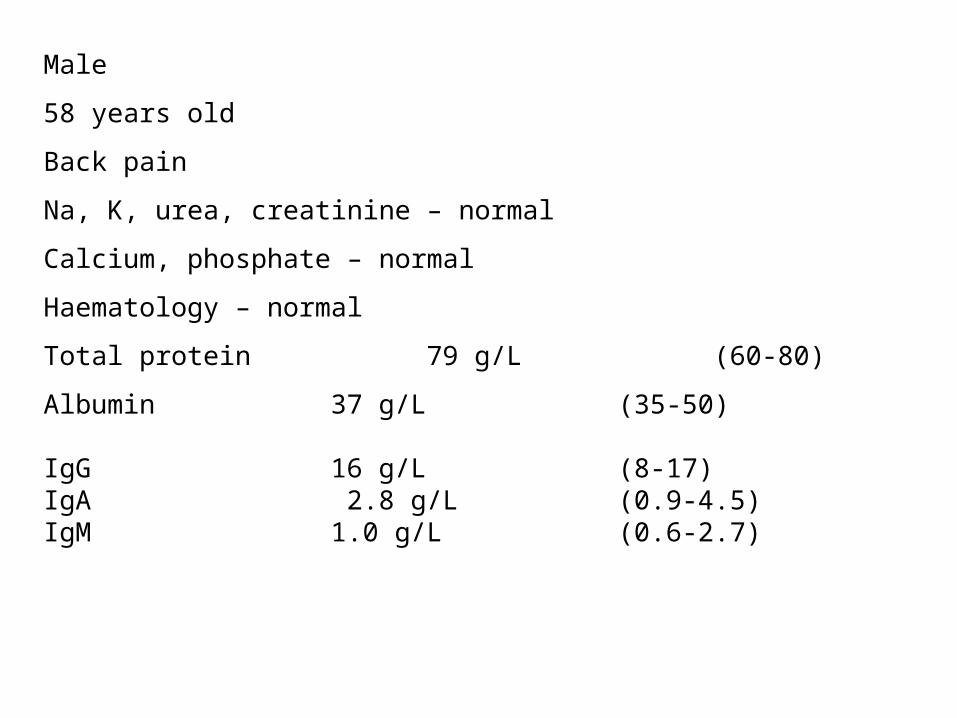
Male
58 years old
Back pain
Na, K, urea, creatinine – normal
Calcium, phosphate – normal
Haematology – normal
Total protein 79 g/L (60-80)
Albumin 37 g/L (35-50)
IgG 16 g/L (8-17)IgA 2.8 g/L (0.9-4.5)IgM 1.0 g/L (0.6-2.7)
IgG IgA IgM κ λ
Urine protein 0.04 g/24h <0.1
Urine protein electrophoresis No protein bands, no BJP
Serum paraprotein concentration = 3 g/L
No significant increase in next 3 years

Female
28 year old
Routine medical
ALT 135 U/L (<50)
ALP 129 U/L (<130)
Bilirubin 18 μmol/L (<20)
ALT persistently raised in next 6 months
Viral screen negative
Requests:
AFP
α1-antitrypsin
Ceruloplasmin
Iron / Iron binding capacity
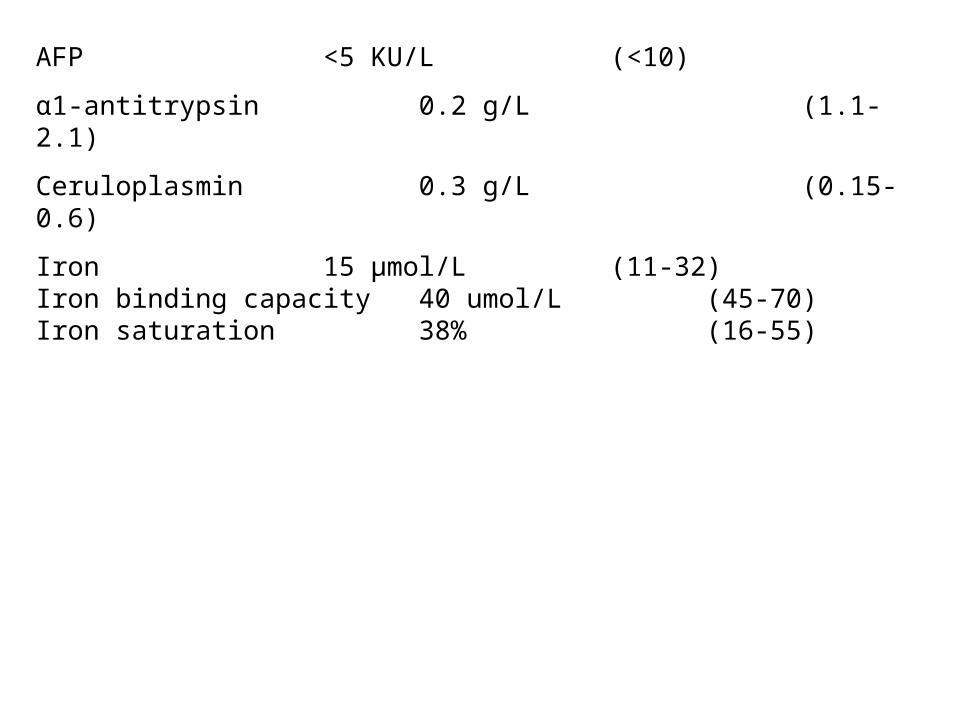
AFP <5 KU/L (<10)
α1-antitrypsin 0.2 g/L (1.1-2.1)
Ceruloplasmin 0.3 g/L (0.15-0.6)
Iron 15 μmol/L (11-32)Iron binding capacity 40 umol/L (45-70)Iron saturation 38% (16-55)
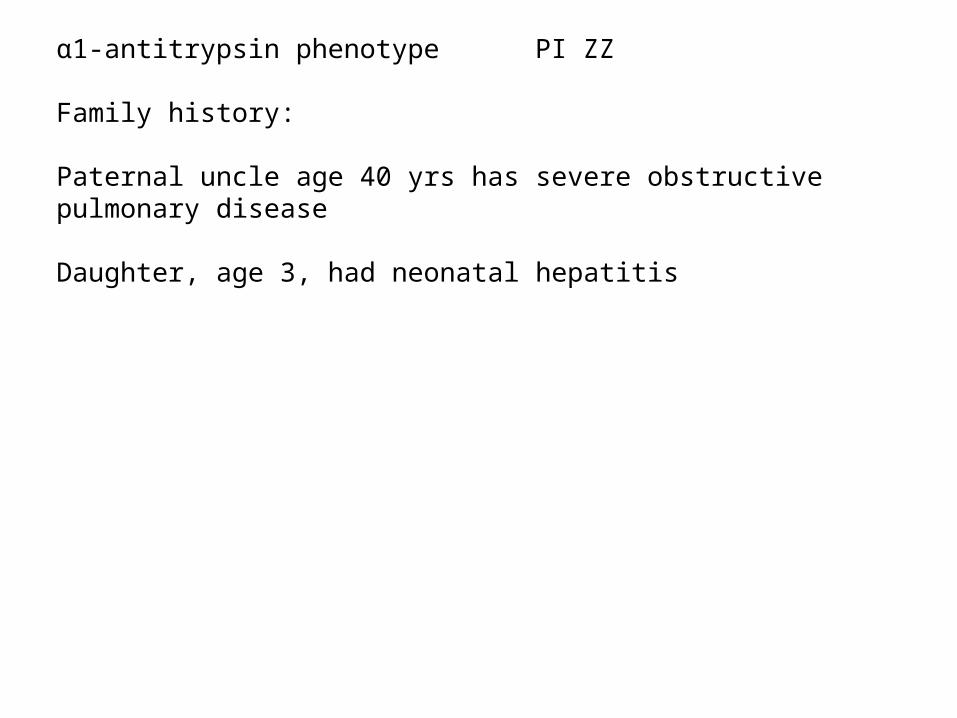
α1-antitrypsin phenotype PI ZZ
Family history:
Paternal uncle age 40 yrs has severe obstructive pulmonary disease
Daughter, age 3, had neonatal hepatitis
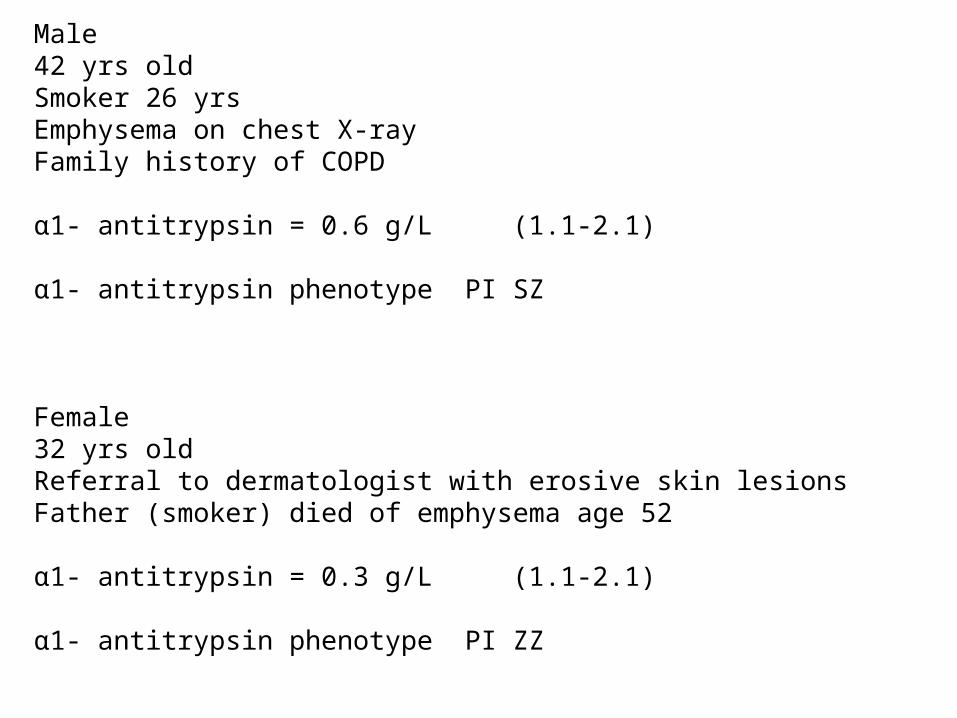
Male42 yrs oldSmoker 26 yrsEmphysema on chest X-rayFamily history of COPD
α1- antitrypsin = 0.6 g/L (1.1-2.1)
α1- antitrypsin phenotype PI SZ
Female32 yrs oldReferral to dermatologist with erosive skin lesionsFather (smoker) died of emphysema age 52
α1- antitrypsin = 0.3 g/L (1.1-2.1)
α1- antitrypsin phenotype PI ZZ

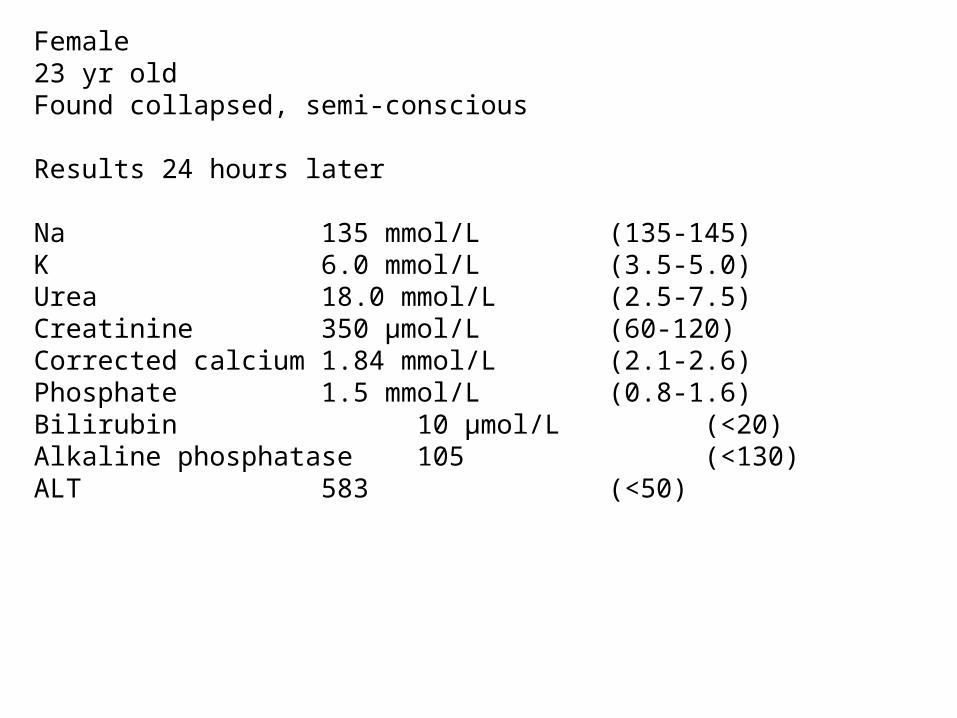
Female23 yr oldFound collapsed, semi-conscious
Results 24 hours later
Na 135 mmol/L (135-145)K 6.0 mmol/L (3.5-5.0)Urea 18.0 mmol/L (2.5-7.5)Creatinine 350 μmol/L (60-120)Corrected calcium 1.84 mmol/L (2.1-2.6)Phosphate 1.5 mmol/L (0.8-1.6)Bilirubin 10 μmol/L (<20)Alkaline phosphatase 105 (<130)ALT 583 (<50)
Random urine blood +++pigmented – dark red/brown
CK 80100 U/L (<170)Urine myoglobin 650000 μg/L (<15)
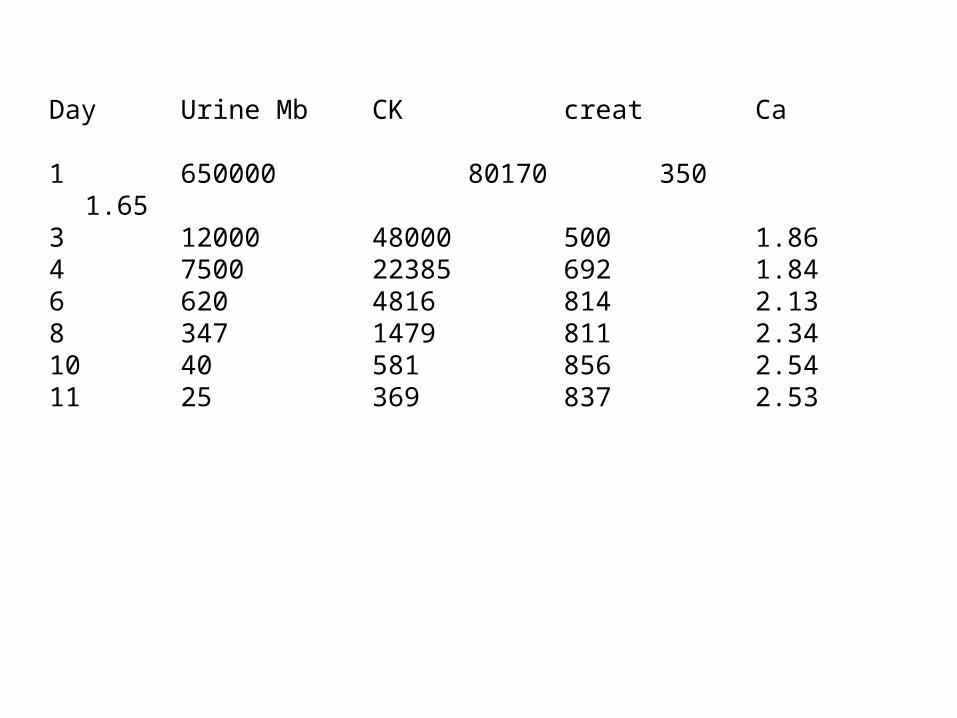
Day Urine Mb CK creat Ca
1 650000 80170 350 1.653 12000 48000 500 1.864 7500 22385 692 1.846 620 4816 814 2.138 347 1479 811 2.3410 40 581 856 2.5411 25 369 837 2.53
Causes of rhadbomyolysis
•Trauma
•Ischaemia
•Surgery
•Exertion/stress
Exercise, seizures, heat
•Metabolic
alcohol, malignant hyperthermia, genetic eg, myophosphorylase deficiency, PFK deficiency, carnitine palmitoyl transferase deficiency, electrolyte depletion eg. K, P
•Toxic
drugs of abuse, venom, other toxins, prescribed drugs eg. Statins
•Myositis, idiopathic and familial myopathies
•Infection

Male MW
Age 24 yrs
Presented 1996 Rochdale
12 month history of elevated ALT (85-145 U/L)No jaundiceNo alcohol, drugsViral screen negative
AFP 4 KU/L (<10)α1-antitrypsin 1.4 g/L (1.1-2.1)Ceruloplasmin <0.06 g/L (0.15-0.6)Iron 15 μmol/L (11-32)Iron binding capacity 46 umol/L (45-70)Iron saturation 33% (16-55)
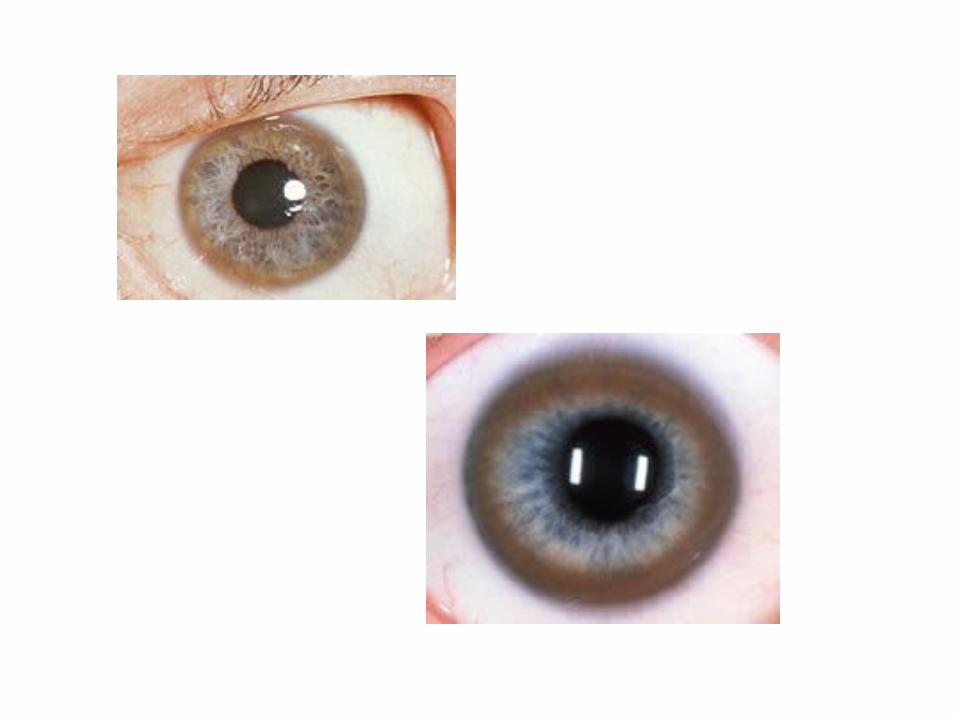
Slit lamp examination Kayser Fleischer rings
Serum copper 1.3 μmol/L (13-24)
Urine copper 4.3 μmol/24h (<1)
Given trientine 900 mg bd
Referred to Neurology Hope 2001
Irreversible brain damage
Severe disabilities
Wheelchair bound
Anarthric
Dysphagia and drooling
Spastic contractures of both limbs
Communicates via electronic keyboard
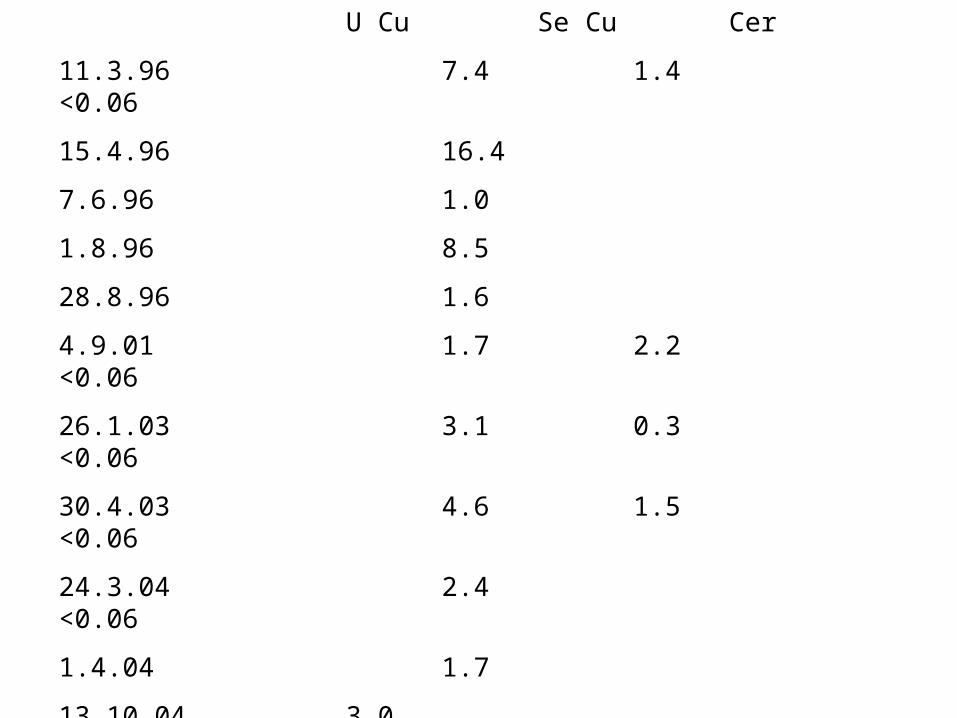
U Cu Se Cu Cer
11.3.96 7.4 1.4 <0.06
15.4.96 16.4
7.6.96 1.0
1.8.96 8.5
28.8.96 1.6
4.9.01 1.7 2.2 <0.06
26.1.03 3.1 0.3 <0.06
30.4.03 4.6 1.5 <0.06
24.3.04 2.4 <0.06
1.4.04 1.7
13.10.04 3.0
2.3.05 0.9 0.5
31.8.05 0.4 <0.06
10.9.05 2.3
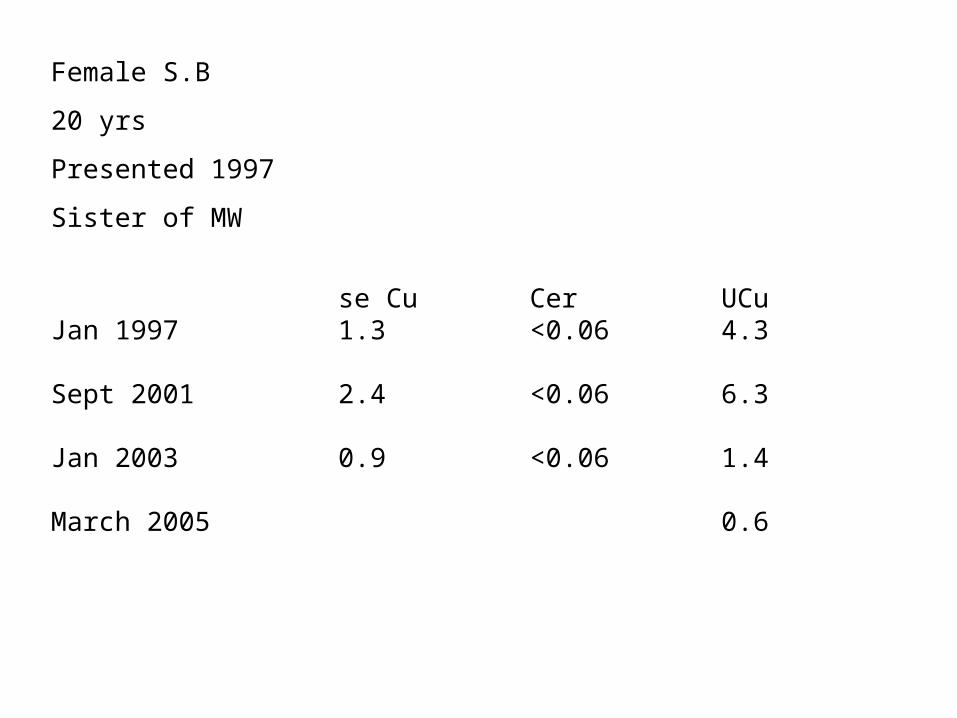
Female S.B
20 yrs
Presented 1997
Sister of MW
se Cu Cer UCuJan 1997 1.3 <0.06 4.3
Sept 2001 2.4 <0.06 6.3
Jan 2003 0.9 <0.06 1.4
March 2005 0.6
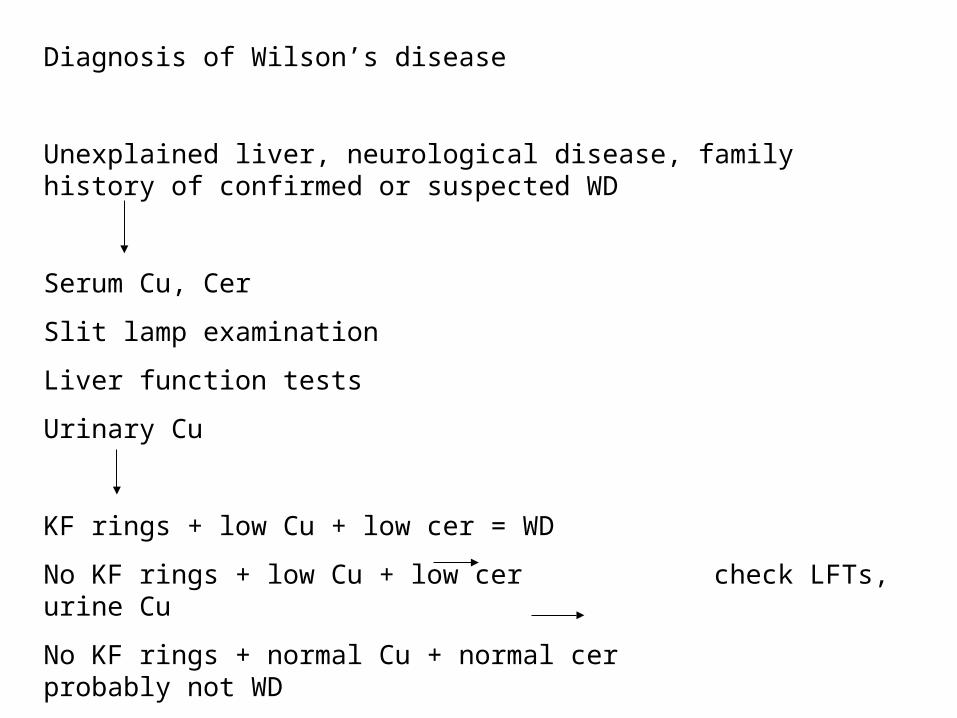
Diagnosis of Wilson’s disease
Unexplained liver, neurological disease, family history of confirmed or suspected WD
Serum Cu, Cer
Slit lamp examination
Liver function tests
Urinary Cu
KF rings + low Cu + low cer = WD
No KF rings + low Cu + low cer check LFTs, urine Cu
No KF rings + normal Cu + normal cer probably not WD
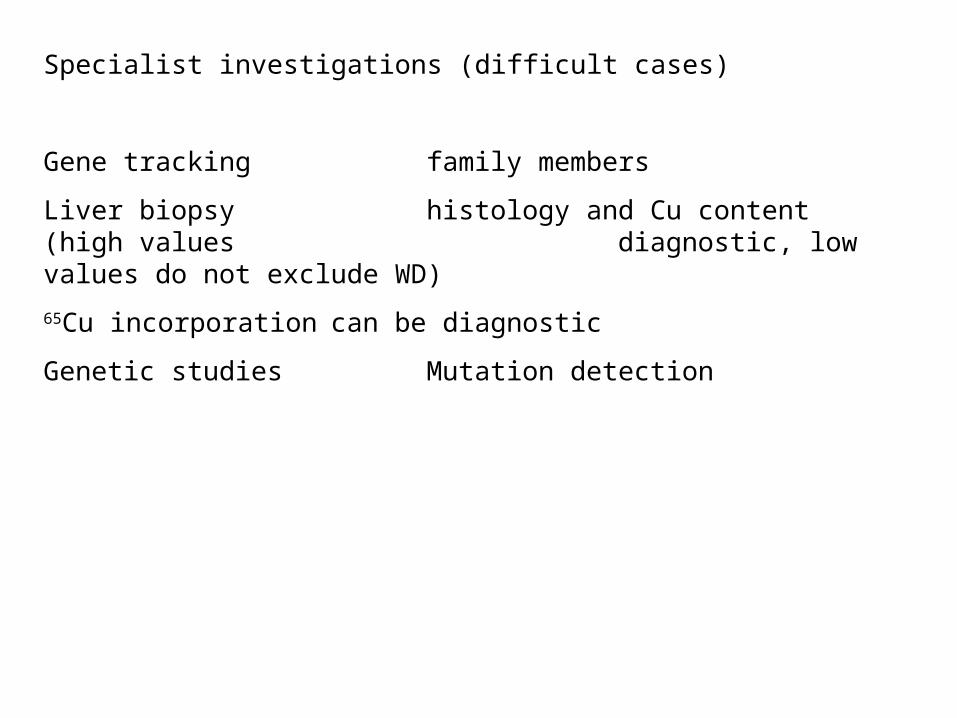
Specialist investigations (difficult cases)
Gene tracking family members
Liver biopsy histology and Cu content (high values diagnostic, low values do not exclude WD)
65Cu incorporation can be diagnostic
Genetic studies Mutation detection