
Prognostic relevance of estrogen receptor-α Ser167 phosphorylation in stage II-III colon cancer...
10
Original contribution Prognostic relevance of estrogen receptor-α Ser167 phosphorylation in stage II-III colon cancer patients ☆,☆☆ Iker López-Calderero MD a,b , Amancio Carnero PhD a , Aurora Astudillo MD, PhD c , José Palacios MD, PhD d , Manuel Chaves MD b , Marta Benavent MD a,b , María L. Limón MD b , Rocio Garcia-Carbonero MD, PhD a,b, ⁎ a Instituto de Biomedicina de Sevilla (IBIS), HUVR/CSIC/Universidad de Sevilla, Center affiliated to the Red Temática de Investigación Cooperativa en Cancer (RTICC), Instituto Carlos III, Spanish Ministry of Science and Innovation, Seville, 41013, Spain b Department of Medical Oncology, Hospital Universitario Virgen del Rocío, Center affiliated to the Red Temática de Investigación Cooperativa en Cancer (RTICC), Instituto Carlos III, Spanish Ministry of Science and Innovation, Seville, 41013, Spain c Department of Pathology, Hospital Central de Asturias, Asturias, 33006, Spain d Department of Pathology, Hospital Universitario Virgen del Rocío, Seville, 41013, Spain Received 2 June 2014; revised 22 July 2014; accepted 5 August 2014 Keywords: Colon cancer; Tissue microarray; Estrogen receptor; Immunohistochemistry; Prognosis; Survival; Biomarkers Summary Preclinical and clinical data suggest a protective role for estrogens on colon cancer (CRC) risk. estrogen receptor (ER) β is the prevalent ER in normal colonic mucosa, whereas its expression is significantly reduced in CRC. An increased ERα/ β ratio has been documented in colon carcinomas and is associated with increased proliferation and decreased apoptosis. The aim of our study was to evaluate the expression of activated ERα and its prognostic implications in patients with stage II-III CRC. Phospho-ERα Ser167 (pERα Ser167 ) expression was assessed by immunohistochemistry in 218 CRC paraffin-embedded tumor samples. A high pERα Ser167 expression was more commonly observed in women, older patients, and patients with high baseline glucose levels. This higher pERα Ser167 expression was associated with decreased 5-year disease-free interval (DFI; 66% versus 78%, P = .07) and overall survival (65% versus 73%, P = .46). The negative impact of high pERα Ser167 expression on DFI was particularly significant ( P b .05) in women (85% versus 60%), young (82% versus 61%), nondiabetic (85% versus 66%), and stage II patients (86% versus 72% and low versus high pERα Ser167 , respectively). Multivariate analysis confirmed that pERα Ser167 score was a significant prognostic factor for both DFI and overall survival, independent of sex, age, glucose levels, tumor stage, bowel obstruction/ perforation, or adjuvant chemotherapy. These findings illustrate the relevance of estrogen pathways in colon cancer biology and may provide novel therapeutic avenues to be explored in this context. © 2014 Elsevier Inc. All rights reserved. ☆ Competing interests: The authors declare no conflicts of interest. ☆☆ Funding/Support: This work was partially supported by a grant from the Fondo de Investigación Sanitaria/Instituto de Salud Carlos III Spanish Cancer Networks RTICC (R12/0036/0008 and R12/0036/0028). R.G.C. is funded by the Fondo de Investigación Sanitaria/Instituto de Salud Carlos III (PI10/02164, PI13/02295), Servicio Andaluz de Salud (PI-0259/2007), and Fundacion Mutua Madrileña (P0497/2006). A.C. is funded by the Fondo de Investigación Sanitaria/Instituto de Salud Carlos III (FIS PI12/00137), Consejeria de Ciencia e Innovacion (CTS-6844, CM09/00207), and Consejeria de Salud of the Junta de Andalucia (PI-0135-2010 and PI-0306-2012). ⁎ Corresponding author at: Medical Oncology Department, Hospital Universitario Virgen del Rocio, Laboratorio de Oncologia Traslacional y Nuevas Terapias, Instituto de Biomedicina de Sevilla (IBIS), Avenida Manuel Siurot, s/n, 41013 Seville, Spain. E-mail address: [email protected] (R. Garcia-Carbonero). www.elsevier.com/locate/humpath http://dx.doi.org/10.1016/j.humpath.2014.08.008 0046-8177/© 2014 Elsevier Inc. All rights reserved. Human Pathology (2014) 45, 2437–2446
Transcript of Prognostic relevance of estrogen receptor-α Ser167 phosphorylation in stage II-III colon cancer...

www.elsevier.com/locate/humpath
Human Pathology (2014) 45, 2437–2446
Original contribution
Prognostic relevance of estrogen receptor-αSer167 phosphorylation in stage II-III coloncancer patients☆,☆☆
Iker López-Calderero MDa,b, Amancio Carnero PhDa, Aurora Astudillo MD, PhD c,José Palacios MD, PhDd, Manuel Chaves MDb, Marta Benavent MDa,b,María L. Limón MDb, Rocio Garcia-Carbonero MD, PhDa,b,⁎
aInstituto de Biomedicina de Sevilla (IBIS), HUVR/CSIC/Universidad de Sevilla, Center affiliated to the Red Temática deInvestigaciónCooperativa enCancer (RTICC), InstitutoCarlos III, SpanishMinistry of Science and Innovation, Seville, 41013, SpainbDepartment of Medical Oncology, Hospital Universitario Virgen del Rocío, Center affiliated to the Red Temática de InvestigaciónCooperativa en Cancer (RTICC), Instituto Carlos III, Spanish Ministry of Science and Innovation, Seville, 41013, SpaincDepartment of Pathology, Hospital Central de Asturias, Asturias, 33006, SpaindDepartment of Pathology, Hospital Universitario Virgen del Rocío, Seville, 41013, Spain
Received 2 June 2014; revised 22 July 2014; accepted 5 August 2014
☆
RA(F
T
h0
Keywords:Colon cancer;Tissue microarray;Estrogen receptor;Immunohistochemistry;Prognosis;Survival;Biomarkers
Summary Preclinical and clinical data suggest a protective role for estrogens on colon cancer (CRC) risk.estrogen receptor (ER) β is the prevalent ER in normal colonic mucosa, whereas its expression is significantlyreduced in CRC. An increased ERα/β ratio has been documented in colon carcinomas and is associated withincreased proliferation and decreased apoptosis. The aim of our studywas to evaluate the expression of activatedERα and its prognostic implications in patients with stage II-III CRC. Phospho-ERαSer167 (pERαSer167)expression was assessed by immunohistochemistry in 218 CRC paraffin-embedded tumor samples. A highpERαSer167 expression was more commonly observed in women, older patients, and patients with high baselineglucose levels. This higher pERαSer167 expression was associated with decreased 5-year disease-free interval(DFI; 66% versus 78%, P = .07) and overall survival (65% versus 73%, P = .46). The negative impact of highpERαSer167 expression on DFI was particularly significant (P b .05) in women (85% versus 60%), young (82%versus 61%), nondiabetic (85% versus 66%), and stage II patients (86% versus 72% and low versus highpERαSer167, respectively). Multivariate analysis confirmed that pERαSer167 score was a significant prognosticfactor for both DFI and overall survival, independent of sex, age, glucose levels, tumor stage, bowel obstruction/perforation, or adjuvant chemotherapy. These findings illustrate the relevance of estrogen pathways in coloncancer biology and may provide novel therapeutic avenues to be explored in this context.© 2014 Elsevier Inc. All rights reserved.
☆ Competing interests: The authors declare no conflicts of interest.☆ Funding/Support: This work was partially supported by a grant from the Fondo de Investigación Sanitaria/Instituto de Salud Carlos III Spanish Cancer NetworksTICC (R12/0036/0008 andR12/0036/0028). R.G.C. is funded by the Fondo de Investigación Sanitaria/Instituto de Salud Carlos III (PI10/02164, PI13/02295), Serviciondaluz de Salud (PI-0259/2007), and Fundacion Mutua Madrileña (P0497/2006). A.C. is funded by the Fondo de Investigación Sanitaria/Instituto de Salud Carlos IIIIS PI12/00137), Consejeria de Ciencia e Innovacion (CTS-6844, CM09/00207), and Consejeria de Salud of the Junta de Andalucia (PI-0135-2010 and PI-0306-2012).⁎ Corresponding author at: Medical Oncology Department, Hospital Universitario Virgen del Rocio, Laboratorio de Oncologia Traslacional y Nuevaserapias, Instituto de Biomedicina de Sevilla (IBIS), Avenida Manuel Siurot, s/n, 41013 Seville, Spain.
E-mail address: [email protected] (R. Garcia-Carbonero).
ttp://dx.doi.org/10.1016/j.humpath.2014.08.008046-8177/© 2014 Elsevier Inc. All rights reserved.

2438 I. López-Calderero et al.
1. Introduction development and progression of breast cancer and is a useful
Colon cancer (CRC) is the third most common cancerworldwide, with 1 361 000 newly diagnosed cases and 694 000deaths registered in 2012 (http://globocan.iarc.fr). Incidencecrude rates are notably higher for men than for women (77.9versus 58.6 new cases/100 000 habitants/year diagnosed in theEuropean Union in 2012), and a similar sex disbalance is alsoobserved for mortality. Numerous epidemiologic observationsand experimental studies suggest a protective effect forestrogens on colon cancer risk. Indeed, controlled clinicaltrials have shown that hormone replacement therapy reducesthe risk of CRC by 30% to 40% in postmenopausal women,and also seem to decrease the incidence and recurrence ofadenomatous polyps [1,2]. Moreover, the greater declineobserved inmortality rates in agedwomen comparedwithmensince 1990 has been attributed by some investigators to theincreased use of hormone replacement therapy. Based on theseobservations, one may speculate that endogenous estrogenswould also play a protective role and could justify the overallreduced incidence and mortality of CRC observed in women.However, some case-control studies do not support thishypothesis because they have observed a positive associationbetween endogenous estradiol levels and the risk of CRC inpostmenopausal women [3,4].
Estrogens regulate growth, differentiation, and function of avariety of tissues, including the gastrointestinal tract [5].Biological activity of estrogens is mainly exerted through theirbinding to 2 specific receptors: estrogen receptor α (ERα) andERβ. Both belong to the nuclear receptor superfamily oftranscription factors that are activated upon ligand binding [6].ER proteins contain 3 major functional domains: a hypervar-iable N-terminal domain, which contains the ligand-indepen-dent transcription activation function 1 (AF-1) region; a highlyconserved DNA-binding domain; and a C-terminal domain,which is involved in ligand-binding and ligand-dependenttranscription activation functions (AF-2) [7–9]. Upon hor-mone binding, ERs form homodimers (ERα/ERα, ERβ/ERβ)or heterodimers (ERα/ERβ) [10], which act as ligand-activatedtranscriptional factors.
Estrogens play an important role in the normal develop-ment and function of reproductive and nonreproductivetissues. ER subtypes are, however, unevenly distributedamong different tissues: ERα is mainly expressed in breast,bone, urogenital tract, cardiovascular tissue, and centralnervous system, whereas ERβ is the prevalent form in thegastrointestinal tract [11]. These 2 receptors seem to haveopposite roles in the regulation of proliferation anddifferentiation of target tissues. Preclinical models showthat ERβ is able to modulate ERα activity, inhibitingestrogen-dependent proliferation and promoting apoptosis.Consistent with these observations, many lines of evidencesuggest a relationship between the perturbation of estrogensignaling and cancer initiation, progression, and response totreatment. More specifically, ERα has been involved in the
biomarker to predict response to hormonal therapy. On thecontrary, ERβ is the prevalent ER in normal colonic mucosa,whereas its expression is significantly reduced in CRC.Indeed, an increased ERα/β ratio has been documented incolon carcinomas, and this has been associated withincreased proliferation and decreased apoptosis [12–18].
Estrogens also modulate gene expression and cell functionthrough a number of alternativemechanisms, including proteinphosphorylation and other nongenomic pathways. ERs can besometimes located at the inner face of the cell membrane,where they may associate with other growth factor receptorssuch as IGF-1R, EGFR, or HER2. The estrogen-boundmembrane ER can induce more rapid effects through theactivation of cell signal transduction pathways, such as themitogen-activated protein kinase and PI3K/AKT pathways.[19,20]. In addition to hormone-dependent activation, ERαfunction may be modulated by posttranslational modificationssuch as direct phosphorylation of ERα or coactivators in aligand-independent manner. The phosphorylated proteinforms a more stable transcription complex with the coactiva-tors and up-regulates the transcription activity of the ER, evenin the absence of hormone [21]. Ser167, locatedwithin the AF-1 region of ERα, is a major site of ERα phosphorylation inresponse to estradiol binding [22,23]. Both AKT and thekinase downstream of mitogen-activated protein kinase, p90ribosomal S6 kinase (pp90Rsk), can also phosphorylate ERαat Ser167 [14].Moreover, PI3Kmay be activated through ERαligand-dependent binding. As a consequence of PI3K-AKTactivation, thus, phosphorylated ERα induces, under estrogenenvironment, a positive feedback loop that amplifies the signal[23]. Interestingly, retrospective series and randomized clinicaltrials conducted in patients with breast cancer strongly suggestthat pSer118- and/or pSer167-ERα is associated withimproved response to hormonal therapy. However, thefunctional consequences of these complex estrogen signalingpathway regulations need to be further elucidated.
Based on these data, the aims of our study were toevaluate pSer167-ERα expression in a cohort of patients withsurgically resected stage II-III colon cancer and to assess itspotential association with relevant clinicopathological fea-tures and its influence on survival.
2. Materials and methods
2.1. Study population
Two hundred eighteen consecutive patients with stage II-III colon cancer attended at our institution from 2000 through2005 were retrospectively identified to be eligible for thisstudy. Patients had to meet the following inclusion criteria:(1) confirmed histologic diagnosis of primary colon cancer,(2) surgical resection with curative intent, (3) TNM stage II orIII, (4) adequate clinical data recorded in medical charts, and

2439Estrogen receptors and colon cancer prognosis
(5) tissue specimen available for additional immunohisto-chemical assays.
Medical records of selected patients were retrospectivelyreviewed according to a previously designed protocol, whichincluded the following clinical data: sex, age, weight, height,body mass index (BMI), performance status, baselinecarcinoembryonic antigen (CEA) levels, baseline plasmaglucose levels, history of diabetes, treatment with oralantidiabetic drugs (OADs) and/or insulin, date of diagnosis,date and type of surgery, emergency presentation (bowelobstruction or perforation), tumor location, World HealthOrganization histologic subtype, tumor differentiation, TNMstage, presence of lymphatic, vascular or perineural invasion,indication of adjuvant chemotherapy (CT), type of CTreceived, date of relapse, and date of last visit or death.Staging was assessed according to the American JointCommittee on Cancer TNM classification (fifth edition) [24].Performance status of patients was evaluated following theEastern Cooperative Oncology Group scale [25]. Allprocedures were performed in compliance with relevantlaws and institutional guidelines, and the correspondinginstitutional review board approved the study protocol.
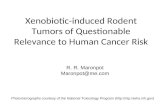
ig. 1 Immunohistochemistry for pERαSer167 expression in colonancer. A, Negative expression. B,Weak expression (1+). C,Moderateexpression (2+).
2.2. Immunohistochemistry
A total of 218 formalin-fixed, paraffin-embedded tumorsamples were provided by the Department of Pathology ofour institution. Blocks were assessed by a pathologist forsuitability to generate tissue microarray (TMA). ElevenTMAs were constructed with 2 tissue samples of eachpatient. One section of each TMA was stained withhematoxylin and eosin for histology verification and qualityassessment. Each TMA had 3 duplicate control cores ofnormal colon tissue. Histologic sections (5 μm) of eachTMA were stained with pSer167 ERα antibody at 1:25dilution (#2541; Cell Signaling Technology, Inc, MA) by apathologist at LVTECH XXI Biotechnology SL (La Rioja,Spain). Briefly, sections were dewaxed in 2 xylene baths(5 minutes each), taken through serial passes of ethanolsolutions (100%, 96%, and 70%), rehydrated in distilledwater, and then submitted to heat-induced antigen retrieval inthe presence of citrate solution (pH 6.0) and phosphate-buffered saline buffer. Blocking of the peroxidase solutionwas applied for 5 minutes, and then TMA slides wereincubated for 30 minutes with protein blocking solution.Finally, primary pSer167 ERα monoclonal antibody wasadded and a biotinylated antibody was used as a secondaryantibody (K0679 15 mL, K0690LSAB+ System-HRP;Dako, Carpinteria, CA).
Two independent pathologists blinded to clinical outcomeperformed the immunohistochemical analyses. TMA sectionswere scanned at low magnification, and the percentage ofpositively stained tumor cells was estimated from 0 to 100% ofthe total of tumor cells. Cellular sublocalization (membrane,cytoplasm, nucleus) of pSer167 ERα expression was assessed
and recorded. Tumor samples were also classified according tostaining intensity into 3 categories: no staining (0), weak (1+),and moderate (2+) intensity staining (Fig. 1). No tumor samplewas found to have strong intensity staining (3+). A phospho-ERαSer167 (pERαSer167) score was then calculated with thefollowing formula: higher intensity ×% of stained cells. Patientswere classified according to this score in 2 groups: lowpERαSer167 expression (pERαSer167 score bmedian) versus highpERαSer167 expression (pERαSer167 score ≥ median; Table 1).
2.3. Statistical analysis
All analyses were performed using Statistical Package forthe Social Sciences v.16 (SPSS Inc, Chicago, IL).Descriptive statistics were used to characterize the mostrelevant clinical parameters. The association of categoricalclinical and pathophysiologic features and ER expressionwas assessed by v2 test or Fisher exact test, when
Fc

Table 1 Phospho-ERαSer167 expression byimmunohistochemical staining
Intensity (I)0 39 (17.9)1+ 168 (77.1)2+ 11 (5.0)
Cellular location of pERαSer167 stainingNo staining 39 (17.9)Nuclear only 7 (3.1)Nuclear and cytoplasm 13 (6.0)Cytoplasm only 158 (72.5)Membranous 1 (0.5)
Percentage of stained cells (%)0-5 25%6-10 25%11-60 25%≥60 25%
Phospho-ER αSer167 score (I × %)Median (range) 12.5 (0-200)0-5 25%5-1-12.5 25%12.6-60 25%N60 25%
Values are presented as n (%), unless otherwise indicated.Abbreviation: NE, not evaluable.
2440 I. López-Calderero et al.
appropriate. Disease-free interval (DFI) was calculated fromthe histologic diagnosis of colon cancer to the date of relapseor last visit in the absence of relapse. Overall survival (OS)was calculated from histologic diagnosis to the date of deathfrom any cause or last visit in alive patients. DFI and OSwere estimated according to the Kaplan-Meier product-limitmethod [26], and differences observed among patientsubgroups were assessed by the log-rank test [27]. Coxproportional hazards regression model was used to evaluatethe prognostic influence of pERαSer167 expression on DFIand OS, while controlling for other potentially confoundingfactors such as age, sex, glucose levels, history of diabetes,OAD, tumor location, bowel obstruction, baseline CEAlevels, T and N stages, and adjuvant CT.
3. Results
3.1. Study population
Two hundred eighteen patients were included in thestudy, 214 of which were evaluable for immunohistochem-ical assessments (Table 2). Clinicopathological characteris-tics of the study cohort are detailed in Supplementary TableS1. The median age was 69 years (range, 28-92 years), 57%were male, 66% had stage II tumors, and 43% receivedadjuvant fluoropyrimidine CT. With a median follow-up of72 months (range, 0.43-153 months), 51 patients (25%) hadrelapsed and 67 (31%) had died, 19 of whom (28% of deaths)due to perioperative complications. Overall, DFI and OS at
5 years for the whole series were 71% and 67%, respectively.As expected, DFI was significantly greater for stage IIpatients than for stage III (78 % versus 58 %, P = .01), and asimilar trend was observed for OS (Table 3).
3.2. Correlation of pERαSer167 expression andclinicopathological features
Phospho-ERαSer167 expression was observed in 179tumor samples (82%). Staining intensity was weak (1+) in168 (77%) cases and moderate (2+) in 11 (5%). Staining wasnuclear in 9% of tumor samples, cytoplasmic in 73%, andmembranous in only 1 case. Half of the samples had positivestaining in more than 10% of tumor cells. MedianpERαSer167 score was 12.5 (range, 0-200; Table 1).
The associations observed between pERαSer167 expressionand different clinicopathological features are summarized inTable 3. High pERαSer167 score wasmore commonly observedin women versus men (56% versus 45%; P = .066), older (N65years) versus younger patients (40% versus 56%; P = .018),patients with baseline glucose levels higher than 120 mg/dLversus 120 mg/dL or lower (45% versus 66%; P = .013),patients treated with OADs versus nontreated (68% versus45%; P = .020), and in those who had received adjuvant CTversus those who had not (59% versus 49%; P = .019).
3.3. Impact of pERαSer167 expression on survival
The potential impact of different clinicopathologicalfeatures on DFI and OS was first assessed by univariateanalysis. As shown in Table 3, right colon tumor location(P = .002), T4 (P = .045), metastatic lymph nodes (P = .010),poor differentiation (P = .019), and stage III disease (P =.010) were features significantly associated with a shorterDFI. Moreover, age over 65 years (P = .004), high baselineCEA levels (P = .019), T4 (P = .064), and no adjuvant CT(P = .001) were all associated with a significantly worse OS.
Regarding pERαSer167 expression, 5-year DFI was lowerfor patients with high versus low pERαSer167 score (≥medianversus bmedian), and the observed difference was ofborderline significance (66% versus 78%%; P = .066). Ofnote, a trend toward worse prognostic implications fornuclear staining versus cytoplasmatic staining was docu-mented, although the observed differences were notstatistically significant (DFI at 5 years: 81% for negativestaining, 71% for cytoplasmic staining, and 65% for nuclearstaining; P = .483). Similarly, patients with a highpERαSer167 score were found to have a shorter OS thanthose with a low score (65% versus 73% alive at 5 years; P =.462; Table 4). Tumors with nuclear pERαSer167 expressiontended to have lower 5-year DFI (65% versus 71%, P = .722)and OS rates (51% versus 68%, P = .871) than did those withcytoplasmic staining. In exploratory analysis, a highpERαSer167 score was significantly associated with a worse5-year DFI in the following subgroups: women (85% versus

Table 2 Study population characteristics and association with pERαSer167 expression
n (%) pERαser167score, n (%) v2, P
Low High
Sex .066Male 124 (57) 68 (55) 56 (45)Female 94 (43) 41 (44) 53 (56)
Age (y) .018 ⁎
≤65 82 (38) 49 (60) 33 (40)N65 136 (62) 60 (44) 79 (56)
ECOG PS a .2220 157 (72) 77 (49) 80 (51)1 18 (8) 5 (27) 13 (73)2 6 (3) 4 (67) 2 (33)
BMI a .286Nonobese (b30 kg/m2) 109 (50) 57 (52) 52 (47)Obese (≥30 kg/m2) 50 (23) 23 (46) 27 (54)
Type 2 diabetes a .175Yes 40 (18) 17 (43) 23 (47)No 141 (65) 74 (52) 67 (48)
Glucose levels a .013 ⁎
≤120 mg/dL 137 (63) 76 (55) 61 (45)N120 mg/dL 41 (19) 14 (34) 27 (66)
Oral antidiabetic agents a .020 ⁎
Yes 31 (14) 10 (32) 21 (68)No 143 (66) 78 (55) 65 (45)
CEA a .386Normal 52 (24) 29 (56) 23 (44)High 60 (27) 32 (53) 28 (47)
Tumor location .379Right colon 56 (26) 30 (53) 27 (47)Other 162 (74) 79 (49) 82 (51)
Bowel obstruction .158Yes 45 (21) 26 (58) 19 (42)No 173 (79) 83 (48) 90 (52)
Bowel perforation .398Yes 16 (7) 9 (56) 7 (44)No 202 (93) 100 (50) 102 (50)
T .317T3 189 (87) 92 (49) 97 (51)T4 25 (11) 14 (56) 11 (44)
N .798N0 145 (66) 71 (49) 74 (51)N1 56 (26) 30 (54) 26 (46)N2 17 (8) 9 (56) 8 (47)
Tumor grade a .225G1 98 (45) 50 (51) 48 (49)G2 86 (40) 38 (44) 48 (56)G3 19 (9) 13 (68) 6 (32)
TNM stage .299II 145 (67) 70 (49) 75 (51)III 73 (33) 39 (53) 34 (47)
Adjuvant CT a .019 ⁎
Yes 88 (40) 36 (41) 52 (59)No 128 (59) 72 (56) 56 (44)
Abbreviations: BMI, body mass index; CEA, carcinoembryonic antigen; CT, chemotherapy; ECOG PS, Eastern Cooperative Oncology Group performancestatus; T, tumor size, N, lymph node metastasis; M, distant metastasis.
a Parameters that include fewer total cases due to missing values (see Supplementary Table S1 for detailed information).⁎ Statistically significant.
2441Estrogen receptors and colon cancer prognosis

Table 3 DFI and OS according to clinicopathological features
n (%) DFI (% at 5 y) P OS (% at 5 y) P
Sex .754 .840Male 124 (57%) 73% 71%Female 94 (43%) 71% 71%
Age (y) .981 .004 ⁎
≤65 82 (38%) 73% 85%N65 136 (62%) 71% 63%
ECOG PS a .638 .6380 157 (72%) 74% 81%1 18 (8%) 67% 75%≥2 9 (4%) 60% 33%
BMI a .458 .678Nonobese 109 (50%) 78% 79%Obese (≥30 kg/m2) 50 (23%) 72% 83%
Type 2 diabetes a .946 .643No 141 (65%) 76% 75%Yes 40 (18%) 75% 72%
Glucose levels a .819 .873≤120 mg/dL 137 (63%) 77% 76%N120 mg/dL 41 (19%) 75% 76%
Oral antidiabetics a .321 .823Yes 31 (14%) 75% 74%No 143 (66%) 82% 78%
Baseline CEA a .147 .019 ⁎
Normal 52 (24%) 81% 81%High-UK 166 (76%) 68% .002 ⁎ 68% .209
Tumor locationRight colon 56 (26%) 56% 59%Other 162 (74%) 78% 76%
Bowel obstruction .135 .088 ⁎
Yes 45 (21%) 60% 63%No 173 (79%) 74% 74%
Bowel perforation .384 .117Yes 16 (7%) 60% 55%No 202 (93%) 73% 73%
T .045 ⁎ .046 ⁎
pT1-T3 193 (89%) 73% 74%pT4 25 (11%) 55% 71%
N .010 ⁎ .624pN0 144 (67%) 78% 73%pN1-2 73 (33%) 58% 71%
Tumor grade a .019 ⁎ .743G1 98 (45%) 79% 74%Other 110 (55%) 66% 71%
TNM stage .010 ⁎ .624II 144 (67%) 78% 73%III 73 (33%) 58% 71%
Adjuvant CT a .076 .001 ⁎
Yes 88 (40%) 66% 87%No 128 (59%) 77% 63%
Abbreviations: DFI, disease-free interval; OS, overall survival; ECOG PS, Eastern Cooperative Oncology Group performance status; BMI, body mass index;CEA, carcinoembryonic antigen; CT, chemotherapy; T, tumor size; N, lymph node metastasis; M, distant metastasis.
a Parameters that include fewer total cases due to missing values (see Table S1 for detailed information).⁎ Statistically significant.
2442 I. López-Calderero et al.
60%; P = .026), young (82% versus 61%; P = .019), obese(89% versus 60%; P = .050), nondiabetic (85% versus 66%;P = .008), low glucose levels (85% versus 66%; P = .015), no
oral antidiabetic treatment (82% versus 69%; P = .039), bowelobstruction (76% versus 31% P = .007), tumor location otherthan the right colon (87% versus 70%; P = .040), N0 (86%

Table 4 Kaplan-Meier survival analysis according to pERαSer167 expression
pERαSer167 score DFI (% at 5 y), ≤medianN P OS (% at 5 y), ≤medianN P
All patients 78%-66% .066 ⁎ 73%-65% .462Sex .080 ⁎ .456Male 73%-73% .723 69%-74% .794Female 85%-60% .026 ⁎ 80%-66% .144
Age (y) .062 ⁎ .794≤65 82%-61% .019 ⁎ 85%-81% .459N65 74%-69% .660 62%-66% .879
ECOG PS .115 .2270 78%-71% .299 82%-80% .2961 NE-53% .087 NE-64% .1442 67%-50% .886 0%-50% .157
BMI .038 ⁎ .634Nonobese 82%-74% .250 80-76% .900Obese 89%-60% .050 ⁎ 83-80% .315
Type 2 diabetes .048 ⁎ .592Yes 69%-79% .372 55%-84% .092No 85%-66% .008 ⁎ 81%-69% .139
Glucose levels .018 ⁎ .477≤120 mg/dL 85%-66% .015 ⁎ 78%-74% .465N120 mg/dL 83%-72% .670 79%-75% .899
Oral antidiabetics .021 ⁎ .477Yes NE-76% .242 56%-82% .138No 82%-69% .039 ⁎ 81%-75% .169
CEA .097 ⁎ .738Normal 84%-78% .401 82%-90% .690High 83%-63% .142 71%-66% .489
Tumor location .059 ⁎ .406Right colon 57%-54% .894 66%-51% .276Other 87%-70% .017 ⁎ 76%-77% .787
Bowel obstruction .026 ⁎ .314Yes 76%-31% .007 ⁎ 80%-34% .009 ⁎
No 79%-71% .271 71%-78% .758Bowel perforation .060 ⁎ .406Yes 33%-NE .053 ⁎ 44%-69% .405No 81%-85% .012 ⁎ 76%-71% .246
T .051 ⁎ .451T3 78%-69% .151 77%-72% .255T4 71%-33% .110 47%-66% .488
N .070 ⁎ .524N0 86%-72% .040 ⁎ 74%-72% .343N1-2 62%-53% .448 71%-70% .811
Tumor grade .071 ⁎ .533I 87%-72% .082 ⁎ 79%-69% .324NI 74%-61% .316 68%-71% .954
TNM stage .058 ⁎ .524II 86%-72% .040 ⁎ 74%-72% .343III 62%-53% .557 71%-70% .811
ECOG PS .115 .2270 78%-71% .299 82%-80% .2961 NE-53% .087 NE-64% .1442 67%-50% .886 0%-50% .157
Adjuvant CT .141 .208Yes 72%-62% .275 89%-84% .138No 82%-72% .312 65%-59% .575
Abbreviations: DFI, disease-free interval; OS, overall survival; ECOG PS, Eastern Cooperative Oncology Group performance status; BMI, body mass index;CEA, carcinoembryonic antigen; CT, chemotherapy; T, tumor size; N, lymph node metastasis; M, distant metastasis.
⁎ Statistically significant.
2443Estrogen receptors and colon cancer prognosis

P =
,066
AL
L P
AT
IEN
TS
Tim
e (m
on
ths)
AP
= ,0
26
Tim
e (m
on
ths)
FE
MA
LE
BP
= ,0
08
Tim
e (m
on
ths)
NO
N-D
IAB
ET
IC P
AT
IEN
TS
CP
= ,0
19
Tim
e (m
on
ths)
YO
UN
GE
R P
AT
IEN
TS
(<6
5y)
DP
= ,0
50
Tim
e (m
on
ths)
OB
ES
E P
AT
IEN
TS
E
Fig.2
DFIb
ypE
RαS
er167expression
(low
expression
:pERαS
er167scorebmedian;high
expression
:pERαS
er167score≥median)
inthefollo
wingpatientpo
pulatio
nsubsets.A,A
llpatients.
B,Fem
ale.C,Non
diabetic
patients.D,You
nger
patients(≤
65yearsold).E,Obese
patients(≥
30kg
/m2).
2444 I. López-Calderero et al.
versus 72%; P = .040), and stage II disease (86% versus 72%;P = .040; low versus high score, respectively; Table 4, Fig. 2).Similarly, a negative association was observed between highpERαSer167 expression and OS in the same subsets of patients,although the observed differences only achieved statisticalsignificance for bowel obstruction (P = .009). Of note, anopposite association seemed to occur in patients with type 2diabetes, in whom a high pERαSer167 expression was correlatedwith a nonsignificant trend for an improved 5-year DFI (79%versus 69%, P = .372) and OS (84% versus 55%, P = .092).
Cox multivariate regression analysis confirmed that highpERαSer167 expression was independently associated with apoorer prognosis, both in terms of DFI (hazard ratio [HR],3.109; P = .005) and OS (HR, 1.944; P = .049). Type 2diabetes, OAD therapy, right colon tumor location, and Tand N stage were also found to be significant prognosticfactors for DFI in multivariate analysis (Table 5). In addition,age, bowel obstruction, N stage, and adjuvant CT weresignificant independent prognostic factors for OS.
4. Discussion
CRC is one of the most common cancers worldwide.Several lines of evidence suggest a protective role forestrogens on colon cancer risk. ERβ is the prevalent ER innormal colonic mucosa, whereas its expression is signifi-cantly reduced in CRC. An increased ERα/β ratio has beendocumented in colon carcinomas, and this is associated withincreased proliferation and decreased apoptosis. In additionto hormone-dependent activation, ERα function may be alsomodulated by posttranslational modifications such as directphosphorylation of ERα or coactivators through ligand-independent pathways. In this context, the aim of our studywas to evaluate the expression of activated ERα and itsprognostic implications in a series of patients with surgicallyresected stage II-III CRC. Our data show that pERαSer167 ismore commonly expressed in women, older patients, andpatients with high baseline glucose levels, and this higherexpression is associated with a strong trend to an increasedprobability of tumor relapse (5-year DFI: 66% versus 78%for high versus low expression, P = .07) and death (5-yearOS: 65% versus 73% for high versus low expression, P =.46). Cox multivariate analysis confirmed that a highpERαSer167 expression was as an independent factor forpoor prognosis both in terms of DFI (HR, 3.109; P = .005)and in terms of OS (HR, 1.944; P = .049), after adjustmentfor other potential confounding factors such as age, sex,glucose levels, history of diabetes, tumor location, bowelobstruction, baseline CEA levels, T and N stage, andadjuvant CT. This is, to our knowledge, the first study toassess the incidence of pERαSer167 expression in tumorsamples of colon cancer patients and to establish acorrelation between pERαSer167 expression and prognosisin these patients.

Table 5 Cox multivariate analysis of prognostic factors for DFI and OS in stage II-III colon cancer patients
Factors DFI OS
HR P 95% CI HR P 95% CI
Sex 0.65 .287 0.31-1.42 0.78 .475 0.40-1.54Age 1.00 .907 0.97-1.04 1.03 .048 * 1.00-1.07Glucose levels 1.00 .432 0.99-1.01 1.01 .159 0.99-1.02Type 2 diabetes 3.46 .048 * 1.01-11.9 2.12 .203 0.67-6.77OAD 0.11 .007 * 0.23-0.55 0.25 .061 0.06-1.07Tumor location 0.47 .047 * 0.23-0.99 1.15 .692 0.57-2.35Bowel obstruction 1.91 .170 0.76-4.82 3.48 .001 * 1.64-7.38CEA 1.15 .736 0.50-2.68 1.86 .129 0.83-4.13T 4.11 .003 * 1.62-10.4 1.81 .196 0.73-4.50N 3.12 .013 * 1.27-7.68 2.34 .033 * 1.07-5.11Adjuvant CT 0.84 .696 0.35-2.01 0.22 .001 * 0.09-0.53pERαSer167 3.10 .005 * 1.40-6.92 1.94 .049 * 1.00-1.07
Abbreviations: DFI, disease-free interval; OS, overall survival; HR, hazard ratio; CI, confidence interval; OAD, oral antidiabetic agents; CEA,carcinoembryonic antigen; T, tumor size; N, lymph node metastasis; CT, chemotherapy.
* P value b 0.05.
2445Estrogen receptors and colon cancer prognosis
Interestingly, although pERαSer167 was more commonlyexpressed in women, older patients, and patients with highbaseline glucose levels, the prognostic impact of thisexpression differed in the different patient subgroups.Whereas a high pERαSer167 score was significantly associ-ated with a worse 5-year DFI in women (85% versus 60%;P = .026), this effect was not observed for older or diabeticpatients. On the contrary, the negative impact of pERαSer167
expression on DFI was rather observed in young (82%versus 61%; P = .019), obese (89% versus 60%; P = .050),and nondiabetic patients (85% versus 66%; P = .008), or inpatients with low baseline glucose levels (85% versus 66%;P = .015; low versus high pERαSer167 score, respectively).Of note, this negative effect on prognosis was particularlyobserved in demographic subgroups in which estrogens areexpected to exert a greater influence, such as women, young,or obese patients. It is well known that estrogens (especiallyestradiol) are mainly produced by the ovary in women ofchildbearing potential. However, other organs such as theadipose tissue can significantly contribute to the circulatingpool of estrogens by converting androstenedione to estrone,which is subsequently reduced to estradiol in peripheraltissues. This extraglandular conversion of androgens toestrogens is catalyzed by aromatases. Aromatase expressionin adipose tissue increases as a function of body weight andage. This is the main source of estrogens in postmenopausalwomen and in men, and a more preponderant source inoverweight patients [11,28].
In contrast, the higher expression of pERαSer167 observedin older patients was not associated with a poorer outcome.As phosphorylation of ERα at Ser167 may occur alsothrough hormone-independent pathways, it is plausible thatin the elderly, this phosphorylation may have been due to theactivation of other kinases, such as AKT, pp90RSK, S6K1,IKK3, CK2, or RET [29]. These alternative pathways of ERactivation may likely have different functional conse-quences and prognostic implications. Similarly, although a
high pERαSer167 expression was more commonly encoun-tered among patients with high baseline glucose levels, thiswas again not associated with a worse survival in this patientsubset. On the contrary, pERαSer167 expression was, indeed,a poor prognostic factor in normoglycemic patients.Estrogens modulate glucose and lipid metabolism indifferent tissues: they increase glucose uptake in cells,regulate glucose and lipid synthesis in the liver, and favorinsulin release by pancreatic cells, overall leading toantidiabetic effects [30]. Insulin, on the other hand, is apotent regulator of human sexual steroid hormone produc-tion and modulates their signals at the receptor level. Morespecifically, insulin resistance and excessive insulin pro-duction associated with hyperglycemia provoke hyperan-drogenism and estrogen deficiency in women [31].Therefore, as observed in the elderly, it is likely thatestrogen-independent pathways may be involved in Ser167ERα phosphorylation in diabetic patients. Based on all theseobservations, a plausible hypothesis would be that onlyestrogen-induced ERα activation would have a negativeimpact on colon cancer patient's survival.
In conclusion, pERαSer167 is expressed in a highproportion of patients with CRC and is associated with aworse prognosis, particularly in women, young, nondiabetic,and stage II patients. These findings suggest that ERs play amajor role in colon cancer biology, which appears to be morerelevant in clinical subsets under greater estrogen influence.Whether antiestrogens, alone or in combination with othertargeted agents (ie, PI3K or AKT inhibitors), can be effectiveantineoplastic drugs in this context remains to be elucidatedbut certainly deserves to be explored.
Supplementary data
Supplementary data to this article can be found online athttp://dx.doi.org/10.1016/j.humpath.2014.08.008.

2446 I. López-Calderero et al.
Acknowledgments
The authors would like to thank the donors and theAndalusian Public Health System Biobank Network (ISCIII-Red de Biobancos RD09/0076/00085) for the human tumorspecimens provided for this study.
References
[1] Grodstein F, Newcomb PA, Stampfer MJ. Postmenopausal hormonetherapy and the risk of colorectal cancer: a review and meta-analysis.Am J Med 1999;106:574-82.
[2] Woodson K, Lanza E, Tangrea JA, et al. Hormone replacementtherapy and colorectal adenoma recurrence among women in the polypprevention trial. Rep J Natl Cancer Inst 2001;93:1799-805.
[3] Galluzzo P, Caiazza F, Moreno S, Marino M. Role of ERbetapalmitoylation in the inhibition of human colon cancer cellproliferation. Endocr Relat Cancer 2007;14:153-67.
[4] Gunter MJ, Hoover DR, Yu H, et al. Insulin, insulin-like growthfactor-I, endogenous estradiol, and risk of colorectal cancer inpostmenopausal women. Cancer Res 2008;68:329-37.
[5] Singh S, Langman MJ. Oestrogen and colonic epithelial cell growth.Gut 1995;37:737-9.
[6] Mangelsdorf DJ, Thummel C, Beato M, et al. The nuclear receptorsuperfamily: the second decade. Cell 1995;83:835-9.
[7] Pace P, Taylor J, Suntharalingam S, Coombes RC, Ali S. Humanestrogen receptor alpha binds DNA in a manner similar to anddimerizes with estrogen receptor. J Biol Chem 1997;272:25832-8.
[8] Bevan C, Parker M. The role of coactivators in steroid hormone action.Exp Cell Res 1999;253:349-56.
[9] Glass CK, Rosenfeld MG. The coregulator exchange in transcriptionalfunctions of nuclear receptors. Genes Dev 2000;14:121-41.
[10] Cowley SM, Hoare S, Mosselman S, Parker MG. Estrogen receptors alphaand beta form heterodimers on DNA. J Biol Chem 1997;272:19858-62.
[11] Nelson LR, Bulun SE. Estrogen production and action. J Am AcadDermatol 2001;45:S116-24.
[12] Shanle EK, Xu W. Selectively targeting estrogen receptors for cancertreatment. Adv Drug Deliv Rev 2010;62:1265-76.
[13] Thomas C, Gustafsson JÅ. The different roles of ER subtypes in cancerbiology and therapy. Nat Rev Cancer 2011;11:597-608.
[14] Fiorelli G, Picariello L, Martineti V, Tonelli F, Brandi ML. Functionalestrogen receptor beta in colon cancer cells. Biochem Biophys ResCommun 1999;261:521-7.
[15] Campbell-Thompson M, Jeanette Lynch I, Bhardwaj B. Expression ofestrogen receptor (ER) subtypes and ER β isoforms in colon cancer.Cancer Res 2001;61:632-40.
[16] Fraumeni Jr JF, Lloyd W, Smith EM, Wagoner SK. Cancer mortalityamong nuns: role of marital status in etiology of neoplastic disease inwomen. J Natl Cancer Inst 1969;42:455-68.
[17] Colditz GA. Relationship between estrogen levels, use of hormonereplacement therapy, and breast cancer. J Natl Cancer Inst 1998;90:814-23.
[18] Hankinson SE, Colditz GA, Willett WC. Towards an integrated modelfor breast cancer etiology: the lifelong interplay of genes, lifestyle, andhormones. Breast Cancer Res 2004;6:213-8.
[19] Roman-Blas JA, Castañeda S, Largo R, Herrero-Beaumont G. Osteoar-thritis associated with estrogen deficiency. Arthritis Res Ther 2009;11:241.
[20] Hawse JR, Subramaniam M, Ingle JN. Estrogen-TGFβ cross-talk inbone and other cell types: role of TIEG, Runx2, and other transcriptionfactors. J Cell Biochem 2008;103:383-92.
[21] Castana E, Vorojeikina D,Notides A. Phosphorylation of serine-167 on thehuman oestrogen receptor is important for oestrogen response elementbinding and transcriptional activation. Biochem J 1997;326:149-57.
[22] Lannigan D. Estrogen receptor phosphorylation. Steroids 2003;68:1-9.[23] Simoncini T, Hafezi-Moghadam A, Brazil DP, Ley K, Chin WW, Liao
JK. Interaction of oestrogen receptor with the regulatory subunit ofphosphatidylinositol-3-OH kinase. Nature 2000;407:538-41.
[24] Sobin LH, Fleming ID. TNM classification of malignant tumors, fifthedition (1997). Union Internationale Contre le Cancer and theAmerican Joint Committee on Cancer. Cancer 1997;80:1803-4.
[25] OkenMM, Creech RH, TormeyDC, et al. Toxicity and response criteria oftheEasternCooperativeOncologyGroup.AmJClinOncol 1982;5:649-55.
[26] Kaplan EL, Meier P. Non parametric estimation from incompleteobservation. J Am Stat Soc A 1972;35:185-206.
[27] Peto R, Peto J. Asymptotically efficient rank invariant test procedures.J R Stat Soc A 1972;135:185-207.
[28] Burger HG, Dudley EC, Robertson DM. Hormonal changes in themenopause transition. Recent Prog Horm Res 2002;57:257-75.
[29] Murphy LC, Seekallu SV, Watson PH. Clinical significance of estrogenreceptor phosphorylation. Endocr Relat Cancer 2011;18:1-14.
[30] Barros RP, Gustafsson JÅ. Estrogen receptors and the metabolicnetwork. Cell Metab 2011;14:289-99.
[31] López-Calderero I, Sánchez Chávez E, García-Carbonero R. Theinsulin-like growth factor pathway as a target for cancer therapy. ClinTransl Oncol 2010;12:326-38.













![Genistein induces apoptosis of colon cancer cells by ...€¦ · pathway [3]. In this study, we demonstrated that GEN can inhibite proliferation and induce apoptosis of colon cancer](https://static.fdocument.org/doc/165x107/6091035508039222da437990/genistein-induces-apoptosis-of-colon-cancer-cells-by-pathway-3-in-this-study.jpg)

