Pharmacokinetics and pharmacodynamics of GSK961081, a novel inhaled muscarinic antagonist β 2...
9
Click here to load reader
Transcript of Pharmacokinetics and pharmacodynamics of GSK961081, a novel inhaled muscarinic antagonist β 2...

Pharmacokinetics and Pharmacodynamicsof GSK961081, a Novel Inhaled MuscarinicAntagonist b2‐Agonist, and FluticasonePropionate Administered Alone,Concurrently and as a Combination BlendFormulation in Healthy Volunteers
Virginia Norris, Claire Ambery, and Trevor Riley
Abstract
Objective: To investigate the pharmacokinetics and pharmacodynamics of inhaled GSK961081 and fluticasonepropionate (FP) given alone, concurrently and as a combination blend formulation.Methods: The study was double‐blind, double‐dummy, four‐way crossover. Twenty‐four healthy volunteers took singledoses of the following in randomized order: (1) GSK961081 800mg; (2) FP 500mg; (3) GSK961081 800mg and FP 500mgas a blend formulation; and (4) GSK961081 800mg and FP 500mg concurrently via separate inhalers. The eLung breathingsimulator was also used for the in vitro characterization of the formulations.Results: There was no pharmacokinetic interaction when GSK961081 and FP were administered concurrently. MeanCmax and AUC(0�t) of GSK961081 were lower (�20%) and mean Cmax and AUC(0�t) of FP were higher (two fold)following GSK961081/FP blend formulation compared to concurrent or the individual components alone. There was anincrease in the FP in vitro ex‐throat dose for theGSK961081/FP blend from the eLung breathing simulator. Serum cortisolsuppression was greater with GSK961081/FP blend, with lower (�10%) cortisol levels than after GSK961081þ FPconcurrent or FP alone.Conclusion: GSK961081/FP blend formulation was associated with an increase in FP systemic exposure and greaterserum cortisol suppression.
Keywords
muscarinic receptor antagonist and b2‐adrenoreceptor agonist, bronchodilator, fluticasone propionate, bi‐functionalmolecule, GSK961081
It is recommended that treatment of chronic obstructivepulmonary disease (COPD) should be based on an
individualized, combined assessment that considers both
current disease, determined by assessment of symptomsand activity limitation, and future risk, determined from
airflow limitation or exacerbation history.1 Inhaled
bronchodilators are the mainstay of the symptomatictreatment of COPD, and both long-acting b2-agonists
(LABAs) and long-acting muscarinic antagonists
(LAMAs) are frequently prescribed as maintenancetherapy. The complementary activity of LAMA and
LABA has been shown to provide an additive effect in
COPD, giving rise to a greater degree of bronchodilationthan either of the components given alone.2,3 A
combination of these agents can provide greater efficacy
for patients who remain symptomatic on a monotherapywith a LABA or LAMA.1,4 The addition of an inhaled
corticosteroid (ICS) to dual bronchodilator therapy is
indicated for patients with high levels of symptoms andwho are at risk of frequent exacerbations.
Clinical Pharmacologyin Drug Development3(4) 305–313
© 2014, The AmericanCollege of ClinicalPharmacologyDOI: 10.1002/cpdd.105
GlaxoSmithKline, UK
Submitted for publication 15 April 2013; accepted 5 January 2014
Corresponding Author:Virginia Norris, GlaxoSmithKline, GSK House, 980 Great West Road,Brentford, Middlesex TW8 9GS, UK(e‐mail: [email protected])ClinicalTrials.gov identifier: NCT01449799.
Original Article

GSK961081 is a novel bifunctional molecule (or dualpharmacophore) that combines muscarinic antagonism
and b2-agonism in a single molecule5 (Figure 1) and is in
development for the treatment of COPD. In trials inpatients with COPD, GSK961081 showed clinically
meaningful bronchodilation with rapid onset of action
and a good safety and tolerability profile.6,7
The combination of the LABA and LAMA compo-
nents in a single, bifunctional molecule simplifies
formulation development and ensures the pharmacologi-cal and pharmaceutical compatibility of the active
ingredients.8 Combination of an ICS with a bifunctional
bronchodilator molecule has the potential to provide asimpler route to a triple therapy.
In this study, the systemic pharmacokinetics (PK),
systemic pharmacodynamics (PD), and safety of singledose GSK961081 given as a combination dry powder
blend with fluticasone propionate (FP) via a single
inhaler, concurrently with FP via separate inhalers, andeach component alone, were assessed. This is the first
study in which GSK961081 and FP have been adminis-
tered as a combination blend formulation to humans.The report also describes how comparative in vitro
data at healthy subject-relevant flow rates were generated
using the Electronic Lung (eLung)9,10 breathing simula-tor to compare the aerodynamic particle size distribution
(APSD) of the delivered dose for the investigational dry
powder inhaler (DPI) products used in this study.
Subjects and MethodsStudy PopulationSixteenmale and 8 female healthy volunteers participated
in the study at Hammersmith Medicines Research,London, UK between July 13, 2011 and September 21,
2011. All subjects provided written informed consent
before participation and the protocol was approved by theNational Research Ethics Committee London, Brent,
UK. The study was conducted in accordance with the
Declaration of Helsinki and Good Clinical Practiceguidelines.
Study DesignThis was a double-blind, single-center, single-dose,
double-dummy, four-way crossover study (GlaxoS-
mithKline study number MFP113423; www.clinical-trials.gov registration number NCT01449799). Subjects
received each of the following four treatments in
randomized order: (1) GSK961081/FP 800/500mg givenas a combination blend formulation (GSK961081/FP
blend); (2) GSK961081 800mg and FP 500mg given
concurrently via separate inhalers (GSK961081þFPconcurrent); (3) GSK961081 800mg; and (4) FP 500mg.The doses were selected to ensure adequate systemic
exposure for PK analysis. Subjects were admitted to theclinical unit the evening before dosing and were
discharged 24 hours after dosing. Each of the four
treatment periods was separated by a washout period of7–10 days. A follow-up visit was completed 10–14 days
after the final dose of study medication.
All treatments were administered by inhalation fromthe DISKUS1 device, which contains a foil blister strip in
which each blister contains 12.5mg of a blend of the
micronized drug substance(s) with lactose monohydrate.The following investigational DPI products were used:
GSK961081/FP combination DPI 400/250mg,GSK961081 DPI 400mg, FP DPI 250mg, and a placebolactose inhaler (PL). The treatments were administered as
follows, each by four inhalers: GSK961081/FP 800/
500mg blend (GSK961081/FP 400/250mg, GSK961081/FP 400/250mg, PL, PL); GSK961081 800mg and FP
500mg concurrently via separate inhalers (GSK961081
400mg, GSK961081 400mg, FP 250mg, FP 250mg);GSK961081 800mg (GSK961081 400mg; GSK961081400mg, PL, PL) and FP 500mg (FP 250mg, FP 250mg,PL, PL). Dosing of the four inhalers was completedwithin 2minutes. Further details of the dosing protocol
are provided in the Online Supplement.
The primary endpoints were plasma concentrationsand derived PK parameters (maximum plasma concen-
tration [Cmax] and area under the concentration curve
[AUC]) for GSK961081 and FP. The secondary endpointswere weighted mean serum cortisol (0–24 hours), urinary
cortisol excretion (0–24 hours), minimum and weighted
mean change from baseline potassium (0–4 hours),maximum and weighted mean change from baseline
glucose (0–4 hours), maximum and weighted mean
change from baseline heart rate (0–4 hours) and maxi-mum and weighted mean change from baseline QT
interval corrected for heart rate using Fridericia’s formula
(QTcF [0–4 hours]), adverse events (AEs) and othersafety measures including spirometric forced expiratory
volume in 1 second (FEV1).
PK AssessmentsBlood samples for the determination of plasma
GSK961081 and FP were collected via an indwellingFigure 1. Molecular structure of GSK961081.
306 Clinical Pharmacology in Drug Development 3(4)

cannula or by direct venepuncture pre-dose and at 0.25,0.5, 0.75, 1, 2, 3, 4, 6, 8, 10, 12, 16, and 24 hours post-
dose. GSK961081 and FP bioanalysis was performed by
Aptuit, Inc. (Verona, Italy) and York BioanalyticalSolutions, Ltd (York, UK), respectively. The lower limit
of quantification (LLQ) was 25 and 3 pg/mL for
GSK961081 and FP, respectively (see Online Supple-ment for additional analytical methods).
PD AssessmentsBlood samples for the determination of serum potassium
and blood glucose, were collected pre-dose and at 0.5, 1,
2, and 4 hours post-dose. Serum potassium and glucosemonitoring was performed using iSTAT portable chemi-
cal analysers at Hammersmith Medicines Research
(London, UK).Blood samples for the determination of serum cortisol
were collected pre-dose and at 1, 2, 3, 4, 6, 8, 10, 12, 16,
and 24 hours post-dose. Urine samples for the determina-tion of cortisol were collected pre-dose and continuously
up to 24 hours post-dose. Serum and urinary cortisol
analyses were performed by Simbec Research (MerthyrTydfil, UK) using an HPLC–MS/MS method. Further
details of assay methodology are provided in the Online
Supplement.
Safety AssessmentsAEs and serious AEs were documented by the investiga-tor from first dosing until the final follow-up visit via the
InForm data management system (Phase Forward,
Waltham, MA). Other safety assessments, performed atthe clinical site, included hematological, clinical chemis-
try and urinalytic laboratory analyses, vital signs, and
spirometry.
In Vitro Assessment of APSDThe eLung is a breathing simulator designed tocharacterize the APSD of an emitted aerosolized dose
at specified inhalation flow rates.10 An inhalation profile
with a peak inspiratory flow rate (PIFR) of 92 L/min wasselected to simulate that generated by healthy subjects
using the DISKUS inhaler.11,12 The eLung was used in
combination with a coated, anatomically correct humanthroat cast of average dimensions13 to provide a better
estimate of oropharyngeal deposition of the emitted dose.
The aerosolized dose passing beyond the throat cast iscaptured in a holding chamber and then drawn through a
next generation impactor (NGI) at a constant flow rate of
60 L/min to characterize the APSD of the aerosolizeddose.14 The throat cast, holding chamber and individual
stages of the NGI apparatus were washed with 50:50
acetonitrile/water to recover the deposited drug. Thesolutions were then analyzed by HPLC. The individual
stage drug deposition profiles and mean ex-throat dose
(sum of the chamber, pre-separator, and stages 1 through
to the micro orifice collector) were determined intriplicate.
Statistical MethodsSample Size. A formal sample size calculation was not
performed; an estimation approach was used. The sample
size required for this study was estimated on the basis ofpreviously observed estimates of within-subject variabil-
ity of log (AUC) and log (Cmax) for GSK961081
(unpublished data, GlaxoSmithKline, London, UK) andFP15 such that the bounds of the 90% confidence interval
(CI) for the primary treatment comparison would be
within 20% of the observed ratio. Based on theseestimates, 20 subjects would provide the study with
sufficient power for equivalence testing based on a 30%
equivalence range. Twenty-four subjects were enrolled toensure that at least 20 subjects completed all treatment
periods and all critical assessments.
PK AnalysesFrom the GSK961081 and FP plasma concentration–time
data, the following parameters were determined: Cmax,time at which Cmax occurs (tmax), area under the plasma
concentration–time curve to last quantifiable concentra-
tion (AUC(0�t)), area extrapolated to infinity(AUC(0�1)), or area to the last quantifiable concentration
within a subject across all treatments (AUC(0�t’)) and
time of last quantifiable concentration (tlast). To evaluatethe primary PK objectives, loge-transformed AUC and
Cmax for GSK961081 and FP were separately analyzed
using a mixed effects model. Period and treatment werefitted as fixed effects, and subject was fitted as a random
effect. For each comparison of interest, a point estimate
and associated 90%CI was constructed for the difference.The point estimate and associated 90% CI were then
back-transformed to provide a point estimate and 90% CI
for the ratio.
PD AnalysesStatistical analysis was performed on the loge-trans-formed weighted mean 0–24-hour serum cortisol and the
loge-transformed total 24-hour urinary cortisol excretion,
separately. A mixed effects model was fitted for each ofthe endpoints with treatment and period fitted as fixed
effects, and subject as a random effect. Subject and period
baseline were fitted as continuous covariates. Subjectbaseline was defined as the mean of the subject’s logebaseline measurement across all the periods. Period
baseline was defined as the difference between the logebaseline value for that period and the subject baseline.
Similar statistical analyses were conducted on:
minimum and weighted mean change from baselinepotassium (0–4 hours); maximum and weighted mean
change from baseline glucose (0–4 hours); maximum and
weighted mean change from baseline heart rate (0–
Norris et al 307

4 hours); and maximum and weighted mean change frombaseline QTcF (0–4 hours).
ResultsSubject Disposition and Baseline CharacteristicsTwenty-four healthy volunteers participated in the study.
All subjects completed the study as planned. All subjectswere included in the PK, PD, and safety populations.
Summary demographic data and details of eligibility
criteria are provided in the online supplement.
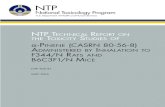
PK ResultsPeak plasmaGSK961081 concentrations occurred around1 hour post-dose (Figure 2) for all three GSK961081
containing treatments (tmax range: 0.25–1.02 hours),
following which concentrations rapidly declined andwere below the LLQ by 3–4 hours post-dose (tlast range:
0.28–10.0 hours; Table 1). Based on statistical analysis
results GSK961081 systemic exposure was lower afteradministration of the GSK961081/FP combination blend
formulation than after GSK961081þ FP concurrent
(AUC(0�t’) was 27% lower; AUC(0�t) was 32% lower)or GSK961081 alone (AUC(0�t’) was 13% lower;
AUC(0�t) was 29% lower). Similarly, maximal
GSK961081 systemic exposure was lower after adminis-tration of the GSK961081/FP blend than after
GSK961081þFP concurrent or GSK961081 alone
(Cmax was 14% lower after both treatments).GSK961081 systemic exposure was similar after
GSK961081þFP concurrent, and GSK961081 alone in
terms of Cmax and AUC(0�t); however, AUC(0�t’) was20% higher after GSK961081 and FP concurrent.
Peak plasma FP concentrations occurred around
0.5 hours post-dose for all three FP containing treatments(tmax range: 0.25–2.02 hours; Figure 2). Plasma FP
concentrations were quantifiable to the last sampling
time point (24 hours) in the majority of subjects (tlastrange: 2.00–24.0; Table 1). Based on statistical analysis
results FP systemic exposure was higher after adminis-
tration of the GSK961081/FP blend than afterGSK961081þFP concurrent (AUC(0�t) was 93% higher;
AUC(0�1) was 48% higher) or FP alone (AUC(0�t) was
82% higher; AUC(0�1) was 40% higher). Similarly,maximal FP systemic exposure was higher after
administration of the GSK961081/FP blend than after
GSK961081þFP concurrent (Cmax was 98% higher) orFP alone (Cmax was 102% higher). FP systemic exposure
was similar after GSK961081þ FP concurrent and FP
alone.
PD ResultsAll treatments containing FP suppressed serum cortisolcompared with GSK961081 alone (considered placebo
for this endpoint; Table 2).Weighted mean serum cortisol
(0–24 hours) was similar after GSK961081þFP concur-rent and FP alone. However, FP suppression of serum
cortisol, although not statistically significant, was slightly
greater after administration of the GSK961081/FP blendthan after FP alone or GSK961081þFP concurrent;
weighted mean serum cortisol after GSK961081/FP
blend was 6% lower than FP alone (adjusted geometricmean ratio (95% CI)) 0.938 (0.838, 1.050), and 10%
lower than GSK961081þ FP concurrent (adjusted geo-
metric mean ratio (95% CI)) 0.905 (0.810, 1.011). Totalurinary cortisol (0–24 hours) data were consistent with
serum cortisol results (Table 2), that is, cortisol was lower
with the GSK961081/FP blend compared withGSK961081þFP or FP alone.
A summary of heart rate, serum potassium, blood
glucose, and QTcF is provided in Table 2. Maximum andweighted mean heart rate change from baseline (0–
4 hours) were similar after GSK961081/FP blend,
GSK961081þFP concurrent, and GSK961081 alone.Maximum and weighted mean heart rate changes from
baseline (0–4 hours) were greater after GSK961081/FP
blend and GSK961081þFP concurrent, compared withFP alone Maximum and weighted mean QTcF (0–
4 hours) results were consistent with heart rate results.
Minimum and weighted mean serum potassium change
Figure 2. (a) Arithmetic mean (SE) plasma concentration–time plots for GSK961081. (b) Arithmetic mean (SE) plasmaconcentration–time plots for FP.
308 Clinical Pharmacology in Drug Development 3(4)

from baseline (0–4 hours) was similar after GSK961081/
FP blend, GSK961081þFP concurrent, and GSK961081
alone. Minimum and weighted mean serum potassiumchanges from baseline (0–4 hours) were greater after
GSK961081/FP blend and GSK961081þFP concurrent
compared with FP alone (there were no differencesbetween any of the treatments for maximum or weighted
mean blood glucose change from baseline (0–4 hours).
Safety ResultsTwenty-one AEs were reported by 13 (54%) subjects. All
AEs were of mild or moderate intensity. There were noserious AEs and no AEs that resulted in premature
discontinuation of treatment. Five AEs were considered
by the investigator to be potentially related to studymedication: four instances of headache (GSK961081/FP
blend: two; GSK961081þFP concurrent: one; FP: one),
and one of dizziness (GSK961081þFP concurrent). Noclinically meaningful treatment effects on clinical safety
laboratory tests, vital signs, or 12-lead electrocardiogram
readings were seen. Spirometry showed a slight increase
from baseline FEV1 after all GSK961081 containing
treatments. No change from baseline in mean FEV1 was
seen after treatment with FP alone.
In Vitro APSD ResultsThe mean ex-throat doses for the investigational DPIproducts containing GSK961081 and FP tested by the
eLung are presented in Table 3. The drug deposition
profiles including the throat cast, holding chamber andindividual NGI stages are shown in Figure 3.
The GSK961081 individual stage deposition profile
for the GSK961081/FP combination blend DPI wassimilar to the GSK961081 single drug substance
comparator. A decrease of approximately 10% in the
GSK961081 ex-throat dose was observed for theGSK961081/FP blend relative to GSK961081 alone.
In contrast, a decrease in the throat cast deposition and
corresponding increase in deposition in NGI stages 3–6was observed for the FP component of the GSK961081/
FP blend DPI relative to the FP single drug substance
comparator. The increase in the FP ex-throat dose for the
Table 1. Summary of GSK961081 and FP PK Parameters
Treatment
GSK961081 (N¼ 24) FP (N¼ 24)
Arithmeticmean (SD)
Geometricmean (95% CI)a
Arithmeticmean (SD)
Geometricmean (95% CI)a
Cmax (pg/mL)081/FP blend 97.7 (63.0) 75.0 (51.6, 109) 201 (112) 137 (80.0, 234)081þ FP 111 (67.8) 86.8 (59.9, 126) 112 (64.3) 69.2 (37.6, 128)Alone 108 (64.6) 87.5 (64.4, 119) 108 (73.8) 67.8 (39.6, 116)
AUC(0�t) (pg�h/mL)081/FP blend 202 (173) 102 (52.5, 197) 1,077 (558) 726 (403, 1,308)081þ FP 267 (194) 150 (77.9, 287) 692 (402) 376 (176, 802)Alone 261 (241) 143 (78.9, 259) 711 (457) 399 (206, 775)
AUC(0�t’) or AUC(0�1)b (pg�h/mL)
081/FP blend 185 (158) 151 (86.4, 264) 1,163 (706) 1,092 (732, 1,631)081þ FP 213 (183) 205 (138, 305) 755 (489) 615 (389, 973)Alone 218 (201) 172 (101, 293) 674 (553) 615 (368, 1,028)
tmax (hour)081/FP blend 0.60 (0.31) 0.75 (0.25, 1.02) 0.39 (0.18) 0.50 (0.25, 0.75)081þ FP 0.76 (0.33) 1.00 (0.50, 1.00) 0.52 (0.27) 0.50 (0.25, 1.02)Alone 0.80 (0.28) 1.00 (0.28, 1.02) 0.74 (0.39) 0.75 (0.25, 2.02)
tlast (hour)081/FP blend 2.81 (1.95) 3.00 (0.50, 8.00) 21.9 (5.95) 24.0 (10.0, 24.1)081þ FP 3.63 (2.26) 4.00 (1.00, 10.00) 20.8 (7.94) 24.0 (2.00, 24.2)Alone 3.61 (2.50) 4.00 (0.28, 10.00) 20.2 (7.80) 24.0 (4.02, 24.0)
AUC(0�t), area under the plasma concentration–time curve to last quantifiable concentration; AUC(0�t’), area under the plasma concentration–timecurve to last quantifiable concentration within a subject across all treatments; AUC(0�1), area under the plasma concentration–time curve extrapolatedto infinity; CI, confidence interval; Cmax, maximumplasma concentration; 081¼GSK961081; FP, fluticasone propionate; n, number of subjects with non‐missing observations, including imputed non‐quantifiable values; tlast, time of last quantifiable concentration; tmax, time at which Cmax occurs. Forarithmetic mean (SD) missing values were imputed with zero. For geometric mean (95% CI) missing values were imputed as follows: AUC(0�t) andAUC(0�1) with half the lowest respective observed value; Cmax with half the LLQ; AUC(0�t’), tmax, and tlast no imputation.aGeometric mean (95% CI), except for tmax and tlast where median (minimum–maximum) is presented.bAUC(0�t’) for GSK961081 and AUC(0�1) for FP.
Norris et al 309

GSK961081/FP blend relative to FP alone was approxi-
mately 45%.
DiscussionThis was the first study in which GSK961081 and FP have
been administered as a combination blend formulation.
This study in healthy subjects was performed to
investigate the systemic PK, PD, and safety ofGSK961081 and FP when administered alone, concur-
rently, and as a blend, to assess the suitability of the blend
formulation for further development as a potential singleinhaled triple therapy for the treatment of COPD.
Systemic exposure to GSK961081 following adminis-
tration as the GSK961081/FP blend was �20% lowercompared with GSK961081þ FP concurrent and
GSK961081 alone. This minimal reduction in systemic
exposure did not alter the expected GSK961081 systemicPD response, with comparable potassium, heart rate,
glucose, and QTcF results obtained for GSK961081/FP
blend and GSK961081 alone. Systemic exposure to FPfollowing administration as the GSK961081/FP blend
was 50–100% higher than compared to GSK961081þFP
concurrent and FP alone. Variability associated with FPPK parameters was comparable when FP was adminis-
tered as the combination blend or alone. Associated with
the increased systemic FP exposure for the GSK961081/FP blend was �10% greater serum cortisol suppression
compared to FP alone or FP in combination with
GSK961081.Cortisol suppression is an ICS class effect16,17 and in
clinical investigation serum and urine cortisol suppres-
sion has been shown to be directly associated with FPAUC.15,18 In this study the increased systemic FP
exposure and cortisol suppression in healthy subjects
for the GSK961081/FP blend is likely to represent themost extreme scenario on the basis that plasma FP levels
are demonstrated to be lower in patients with COPD as
compared to healthy subjects.19 FP 500mg twice daily isthe approved regimen for the treatment of COPD in
Europe in combination with salmeterol. Treatment with
this regimen for periods of up to 3 years is not associatedwith any significant risk of adverse effects commonly
associated with prolonged systemic exposure to cortico-
steroids such as cataracts, osteoporosis or bone frac-tures.20 Clinical data also indicate that, in combination
with salmeterol, a 500mg/day FP dose may have utility in
COPD.21,22 Based on the systemic PK (and PD) results ofthis study, a GSK961081/FP blend containing 250mg of
FP could be an appropriate twice-daily formulation in
terms of safety and efficacy for exploration in furtherclinical studies.
The systemic PK (and PD) findings for the blend were
not observed for GSK961081 and FP given concurrently,
Table 2. Summary of Arithmetic Mean (SD) GSK961081 andFP PD Parameters
TreatmentMaximuma
(N¼ 24)Weighted
mean (N¼ 24)
Serum cortisol (0–24 hours) (ng/mL)081/FP blend N/A 51.8 (21.5)081þ FP N/A 58.9 (32.2)081 alone N/A 64.4 (31.2)FP alone N/A 56.3 (25.0)
Urinary cortisol (0–24 hours) (mg)081/FP blend N/A 20.2 (10.3)081þ FP N/A 28.5 (29.7)081 alone N/A 28.8 (10.5)FP alone N/A 21.0 (9.82)
Heart rate (0–4 hours) change from baseline (bpm)081/FP blend 4.15 (5.52) 0.25 (3.53)081þ FP 4.21 (3.72) 0.74 (3.28)081 alone 4.43 (4.06) 0.97 (3.19)FP alone 2.13 (5.46) �1.55 (4.78)
Serum potassium (0–4 hours) change from baseline (mmol/L)081/FP blend �0.31 (0.22) �0.17 (0.17)081þ FP �0.27 (0.22) �0.15 (0.19)081 alone �0.28 (0.17) �0.16 (0.18)FP alone �0.17 (0.19) �0.05 (0.16)
Blood glucose (0–4 hours) change from baseline (mmol/L)081/FP blend 0.08 (0.17) �0.09 (0.17)081þ FP 0.08 (0.20) �0.06 (0.21)081 alone 0.06 (0.20) �0.11 (0.18)FP alone 0.05 (0.17) �0.13 (0.19)
QTcF (0–4 hours) change from baseline (ms)081/FP blend 6.90 (8.14) 1.73 (5.85)081þ FP 8.43 (7.17) 1.26 (4.99)081 alone 8.77 (7.35) 2.02 (5.52)FP alone 4.10 (7.34) �3.02 (6.17)
bpm, beats per minute; CI, confidence interval; 081¼GSK961081; FP,fluticasone propionate; N/A, not applicable; QTcF,QT interval correctedfor heart rate using Fridericia’s formula. No values were imputed.aMinimum presented for potassium (0–4 hours).
Table 3. Summary of Arithmetic Mean (SD) eLung Ex‐Throat DoseData forGSK961081 400mg and FP 250mg Delivered ViaDISKUSInhaler at a Healthy Subject‐Representative Flow Rate of 92 L/min
Device GSK961081 ex‐throat dose, mg/blister FP ex‐throat dose, mg/blister
GSK961081 DISKUS 400mg/blister 102.2 (3.7) N/AFP DISKUS 250mg/blister N/A 38.4 (3.8)GSK961081/FP DISKUS 400/250mg/blister 92.5 (4.0) 55.8 (2.2)
FP, fluticasone propionate; N/A, not applicable.
310 Clinical Pharmacology in Drug Development 3(4)

with PK being comparable following GSK961081 and FP
given concurrently and the individual components givenalone. FP is a substrate for CYP3A4 and GSK961081 is a
substrate of CYP3A4 and P-glycoprotein with in vitro
studies with human liver microsomes indicating lowpotential for CYP450 inhibition. Therefore the absence of
any PK interaction when GSK961081 and FP were
administered concurrently was as expected.The findings in this study, whereby GSK961081 and
FP systemic exposure correlated with the in vitro APSD
differences observed in the eLung analysis, may beattributed in part to the use of the same inhalation device
(DISKUS) for all treatments. The aerosolization of
carrier-based blends on inhalation is influenced by thecomposition and surface properties of the blend con-
stituents as well as the mixing process.23 Based on
hypotheses presented in the literature as to how fineparticles influence the performance of carrier-based
DPIs, two potential mechanisms may be proposed to
explain the observed increase in FP ex-throat dose for thecombination blend inhaler.24 The micronized
GSK961081 particles either preferentially occupy areas
of high adhesion on the surface of the coarse lactosecarrier particles and/or formmixed agglomerates with the
FP particles which are more easily dispersed on
inhalation. Given that there is only a modest correspond-ing decrease in the GSK961081 ex-throat dose for the
combination blend, co-agglomeration of the drug sub-
stances is speculated to be the dominant mechanism bywhich enhancement of the respirable FP particles occurs.
In principle, in vitro APSD data could be used to guide
dose selection for any future GSK961081/FP combina-tion blend in consideration for clinical investigation,
given the correlation of systemic exposure differences
and ex-throat dose in this study. However this would notreplace thorough clinical investigation.
All treatments were well tolerated, with no serious
AEs or withdrawals and no clinically meaningful
treatment effects on safety laboratory parameter tests,
vital signs or 12-lead electrocardiogram readings. This isconsistent with those from earlier studies with
GSK961081 in patients with COPD.6,7
The doses of GSK961081 (800mg) and FP (500mg)used in this study were selected to enable the single-dose
PK profiles to be adequately characterized and were
expected to be well tolerated. The dose of FP used(500mg) was selected because it had previously been
shown to have a measurable effect on serum cortisol
following single-dose administration.15 The PK and PDresults for FP alone and GSK961081 alone in this study
were consistent with those previously reported. Steady-
state systemic exposures, although not investigated in thisstudy, can be predicted from single-dose data and then
assessed in PDmodel such as the cortisol model proposed
by Mackie and Bye.18
ConclusionsAdministration of GSK961081 and FP as a blend was
associated with an increase in FP systemic exposurerelative to GSK961081þFP concurrent or FP alone,
and greater serum cortisol suppression. The PK findings
correlate with an increase in the FP in vitro ex-throatdose for the blend as determined using the eLung
breathing simulator. There was no PK or PD interaction
when GSK961081 and FP were administered concur-rently and so these finding suggest that the increase in
FP systemic exposure for the combination formulation
could be due to physical interactions in the blendinfluencing oropharyngeal deposition following deliv-
ery via the DPI.
Acknowledgments
We wish to acknowledge Hiran Cooray for operational support,
and the investigators, staff and subjects at the study site,
Figure 3. (a) Comparison of arithmetic mean (SE) eLung‐determined deposition of GSK961081 in throat cast, holding chamber andNGI stages 1–MOC for GSK961081/FP 400/250mg and GSK961081 400mg delivered via DISKUS inhaler at a healthy subject‐representative flow rate of 92 L/min. (b) Comparison of arithmetic mean (SE) eLung‐determined deposition of FP in throat cast, holdingchamber and NGI stages 1–MOC for GSK961081/FP 400/250mg and FP 250mg delivered via DISKUS inhaler at a healthy subject‐representative flow rate of 92 L/min.
Norris et al 311

Hammersmith Medicines Research, London, UK. We thank
Richard Martin, Daniel Alexander, Paul Hopkins, and Melanie
Hamilton for the generation of in vitro Electronic Lung data, and
David Prime for his helpful input to the data interpretation.
Editorial support (in the form of development of a draft outline
in consultation with the authors, assembling tables and figures,
collating author comments, copyediting, fact checking,
referencing and graphic services) was provided by Ian Grieve
at Gardiner-Caldwell Communications and was funded by
GlaxoSmithKline.
Declaration of Conflicting Interests
V.N., C.A., and T.R. are employees of and hold stock in
GlaxoSmithKline.
Funding
All authors meet the criteria for authorship set forth by the
International Committee for Medical Journal Editors. All
authors had full access to the data and confirm the accuracy
and completeness of the data and the data analysis. All authors
developed and revised the manuscript for important intellectual
content. V.N. and C.A. designed the clinical study, contributed
to the analysis including approval of the statistical plan, and
interpreted the data. T.R. interpreted the clinical and in vitro
data. This study was funded by GlaxoSmithKline (study number
MFP113423; ClinicalTrials.gov identifier NCT01449799).
References
1. The Global Initiative for Chronic Obstructive Lung disease
(GOLD) revised 2011. http://www.goldcopd.org/guide-
lines-global-strategy-for-diagnosis-management.html. Ac-
cessed February 6, 2013.
2. Sansores R, Ramirez-Vanegas A, Reddy C,Mejia-Alfaro R.
Effect of the combination of two bronchodilators on
breathlessness in patients with chronic obstructive pulmo-
nary disease. A crossover clinical trial. Arch Med Res.
2003;34(4):292–297.
3. Celli BR, MacNee W, Agusti A, et al. Standards for the
diagnosis and treatment of patients with COPD: a summary
of the ATS/ERS position paper. Eur Respir J. 2004;
23(6):932–946.
4. Cazzola M, Molimard M. The scientific rationale for
combining long-acting b2-agonists and muscarinic antag-
onists in COPD. Pulm Pharmacol Ther. 2010;23(4):257–
267.
5. Steinfeld T, Hughes AD, Klein U, Smith JA, Mammen M.
THRX-198321 is a bifunctional muscarinic receptor
antagonist and beta2-adrenoreceptor agonist (MABA)
that binds in a bimodal and multivalent manner. Mol
Pharmacol. 2011;79(3):389–399.
6. Wielders PL, Ludwig-Sengpiel A, Locantore N, Baggen S,
Chan R, Riley JH. A new class of bronchodilator improves
lung function in COPD: a trial with GSK961081.Eur Respir
J. 2013;42(4):972–981.
7. Norris V, Zhu C, Ambery C. The pharmacodynamics of
GSK961GSK961081 in patients with COPD. Eur Respir J.
2011;38(Suppl 55):138s.
8. Hughes AD, Jones LH. Dual-pharmacology muscarinic
antagonist and b2-agonist molecules for the treatment of
chronic obstructive pulmonary disease. Future Med Chem.
2011;3(13):1585–1605.
9. Burnell PKP, Malton A, Reavill K, Ball MHE. Design,
validation and initial testing of the Electronic LungTM
device. J Aerosol Sci. 1998;29(8):1011–1025.
10. Brindley A, Sumby BS, Smith IJ. The characterisation of
inhalation devices by an inhalation simulator: The
electronic lung. J Aerosol Med. 1994;7(2):197–200.
11. Broeders MEAC, Molema J, Vermue NA, Folgering HTM.
Peak inspiratory flow rate and slope of the inhalation
profiles in dry powder inhalers. Eur Respir J.
2001;18(5):780–783.
12. de Koning JP, van der Mark TW, Coenegracht PMJ, Tromp
TFJ, Frijlink HW. Effect of an external resistance to airflow
on the inspiratory flow curve. Int J Pharm. 2002;234(1–
2):257–266.
13. Burnell PKP, Asking L, Borgstrom L, et al. Studies of the
human oropharyngeal airspaces using magnetic resonance
imaging IV—the oropharyngeal retention effect for four
inhalation delivery systems. J Aerosol Med. 2007;20(3):
269–281.
14. Marple VA, Roberts DL, Romay FJ, et al. Next generation
pharmaceutical impactor (a new impactor for pharmaceuti-
cal inhaler testing). Part I: Design. J Aerosol Med.
2003;16(3):283–299.
15. Mollmann H, Wagner M, Krishnaswami S, et al. Single-
dose and steady state pharmacokinetic and pharmacody-
namic evaluation of equipotent doses of inhaled fluticasone
propionate and budesonide in healthy subjects. J Clin
Pharmacol. 2001;41(12):1329–1338.
16. Bernstein DI, Allen DB. Evaluation of tests of hypothalam-
ic-pituitary-adrenal axis function used to measure effects of
inhaled corticosteroids. Ann Allergy Asthma Immunol.
2007;98(2):118–127.
17. Dahl R. Systemic side effects of inhaled corticosteroids in
patients with asthma. Respir Med. 2006;100(8):1307–1317.
18. Mackie AE, Bye A. The relationship between systemic
exposure to fluticasone propionate and cortisol reduction in
healthy male volunteers. Clin Pharmacokinet. 2000;39
(Suppl 1):47–54.
19. Dalby C, Polanowski T, Larsson T, Borgstrom L, Edsbacker
S, Harrison TW. The bioavailability and airway clearance
of the steroid component of budesonide/formoterol and
salmeterol/fluticasone after inhaled administration in
patients with COPD and healthy subjects: a randomized
controlled trial. Respir Res. 2009;10(1):104.
20. Calverly PMA, Anderson JA, Celli B, et al. Salmeterol and
fluticasone propionate and survival in chronic obstructive
pulmonary disease. N Engl J Med. 2007;356(8):775–789.
312 Clinical Pharmacology in Drug Development 3(4)

21. Anzueto A, Ferguson GT, Feldman G, et al. Effect of
fluticasone propionate/salmeterol (250/50) on COPD ex-
acerbations and impact on patient outcomes. COPD.
2009;6(5):320–329.
22. Ferguson GT, Anzueto A, Fei R, Emmett A, Knobil K,
Kalberg C. Effect of fluticasone propionate (250/50mg) or
salmeterol (50mg) on COPD exacerbations. Respir Med.
2008;102(8):1099–1108.
23. de Boer AH, Chan HK, Price R. A critical view on lactose-
based drug formulation and device studies for dry powder
inhalation: which are relevant and what interactions to
expect? Adv Drug Deliv Rev. 2012;64(3):257–274.
24. Jones MD, Price R. The influence of fine excipient particles
on the performance of carrier-based dry powder inhalation
formulations. Pharm Res. 2006;23(8):1665–1674.
Supporting InformationAdditional supporting information may be found in the
online version of this article at the publisher’s web-site.
Norris et al 313