Peripheral T-cell Lymphomas - kaim.or.kr · PDF filePeripheral T-cell lymphomas ... HDAC class...
67
Peripheral T-cell Lymphomas Seok Jin Kim MD, PhD Department of Medicine Sungkyunkwan University Samsung Medical Center
Transcript of Peripheral T-cell Lymphomas - kaim.or.kr · PDF filePeripheral T-cell lymphomas ... HDAC class...
Peripheral T-cell Lymphomas Seok Jin Kim MD, PhD
Department of Medicine
Sungkyunkwan University Samsung Medical Center
T-cell and NK cell subsets
αβ T-cells CD4+ (mainly helper) or CD8+ (mainly cytotoxic)
γδ T-cells CD4-CD8- or CD4-CD8+
NK cells Usually CD4-CD8-, but may be CD8+ NK-associated antigen: CD11b, 16, 56, 57
Immune system
Innate immune system Primitive defense system in mucosa and skin NK-cells and γδ T-cells γδ T-cells: < 5% of normal T cells Splenic red pulp, intestinal mucosa, other epithelial
sites
Adaptive immune system αβ T-cells: majority of normal T cells Recognition of MHC-restricted antigen
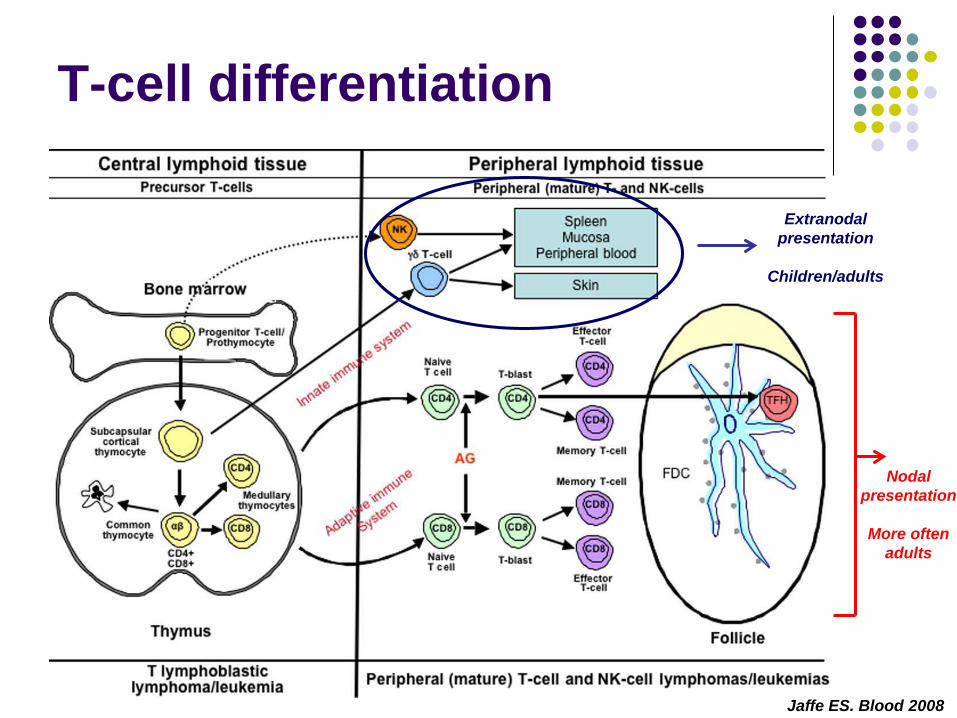
T-cell differentiation
Jaffe ES. Blood 2008
Extranodal presentation
Children/adults
Nodal presentation
More often
adults
Question 1
Adaptive immune system is 1) αβ T-cells 2) NK-cells 3) γδ T-cells 4) I don’t know 5) I don’t care
Peripheral T-cell lymphoma
Nodal
Extranodal Cutaneous
Disseminated and leukemic
Peripheral T-cell lymphomas Nodal Peripheral T-cell lymphoma, not otherwise
specified (PTCL-NOS) Angioimmunoblastic T-cell lymphoma (AITL) Anaplastic large cell lymphoma (ALCL)
Extranodal Extranodal NK/T-cell lymphoma, nasal type Enteropathy-associated T-cell lymphoma Hepatosplenic T-cell lymphoma
• Cell origin • αβ T-cells; γδ T-cells; NK cells
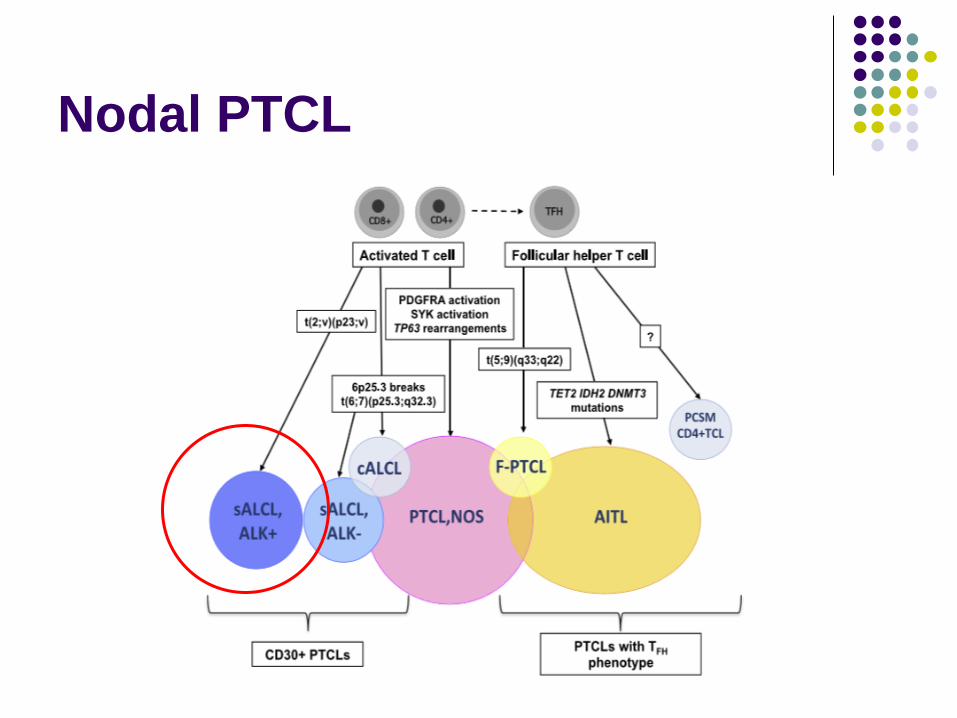
Nodal PTCL
ALCL, ALK+
Common in 10-30s Mostly stage III/IV
Lymphadenopathy Bone, skin, soft tissue, lung, liver Common B Sx
Recurrent genetic alteration: ALK+ ALK gene (2p23) with others e.g. NPM1 (5q35) NPM-ALK translocation: constitutive activation of ALK
tyrosine kinase Therapeutic target
Good prognosis with 5-yr OS: 70-80%
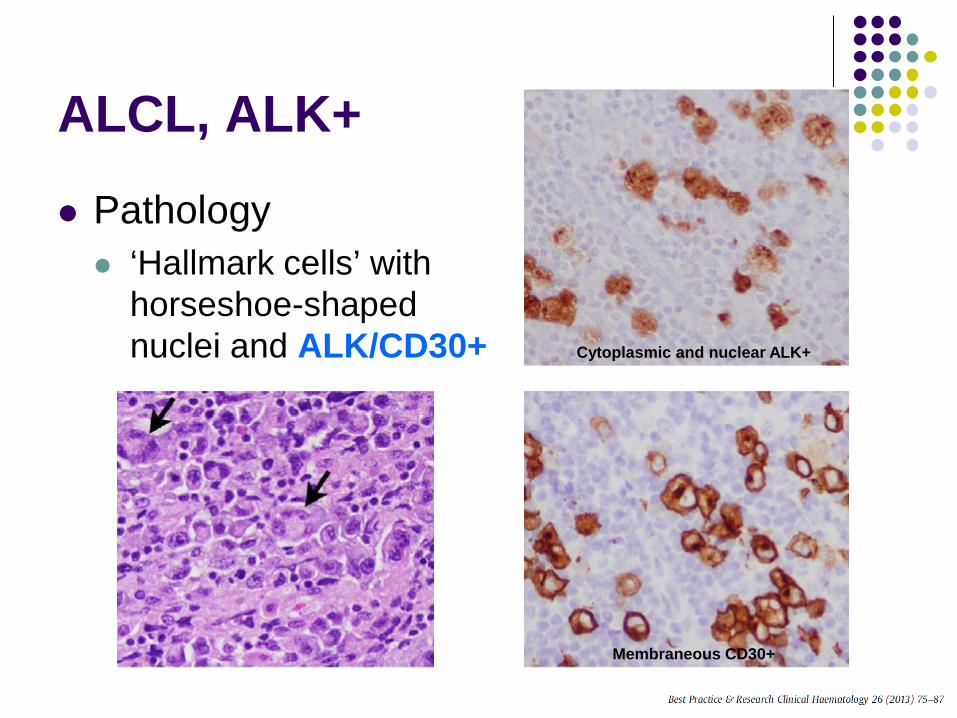
ALCL, ALK+
Pathology ‘Hallmark cells’ with
horseshoe-shaped nuclei and ALK/CD30+ Cytoplasmic and nuclear ALK+
Membraneous CD30+
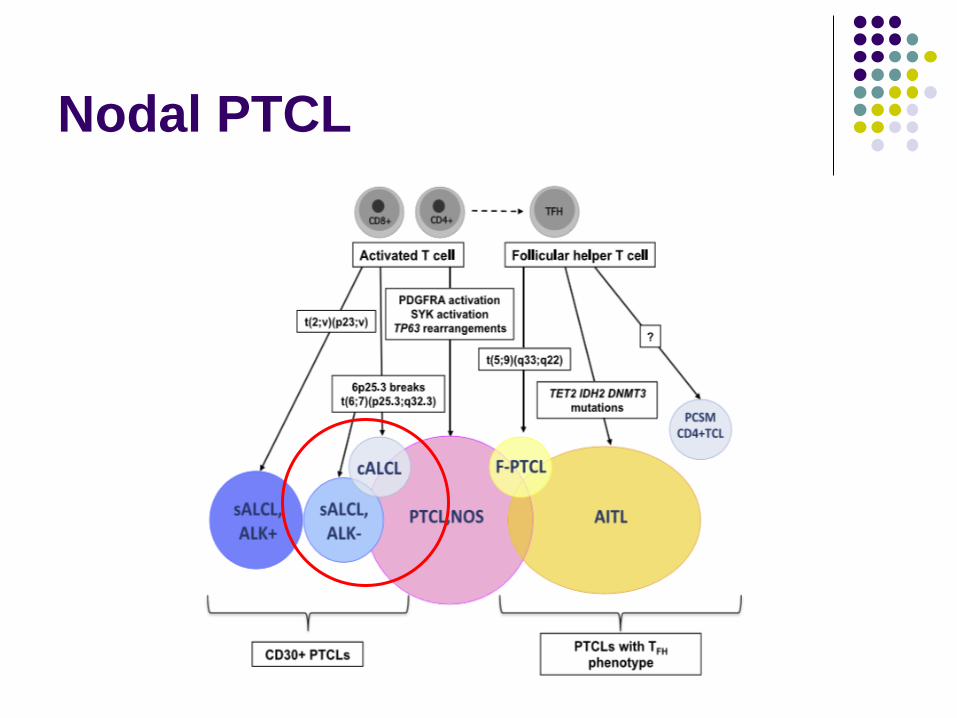
Nodal PTCL
ALCL, ALK-
Same morphology without ALK Age: 40 – 65 years Nodal invasion is more common than
extranodal invasion Pathology CD30: homogeneous strong positive
Differential diagnosis with HL PAX5: positive for HL
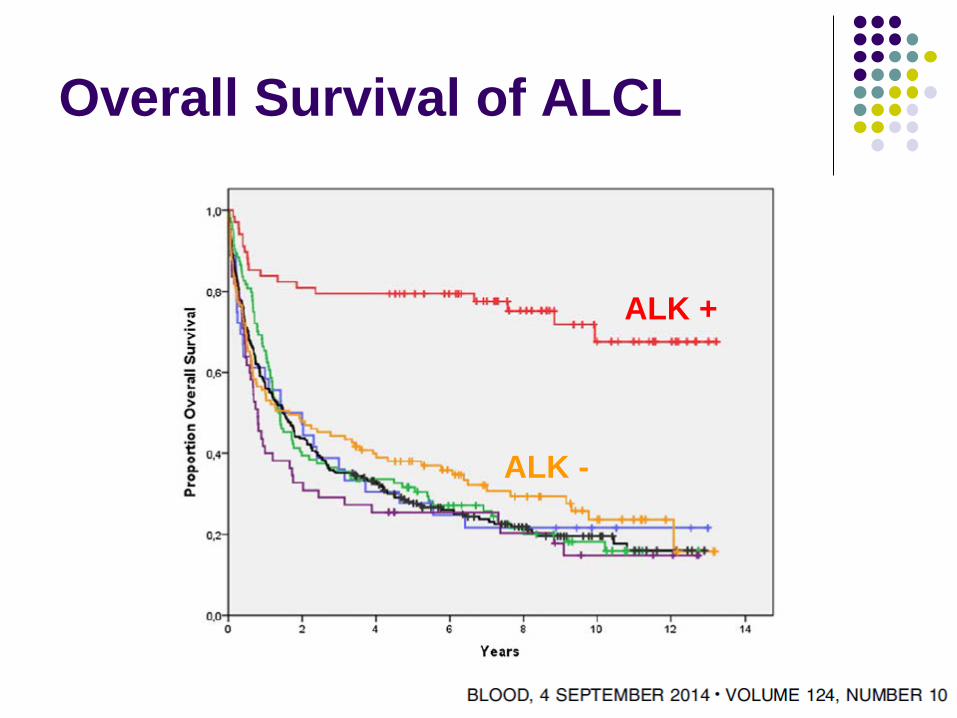
Overall Survival of ALCL
ALK +
ALK -
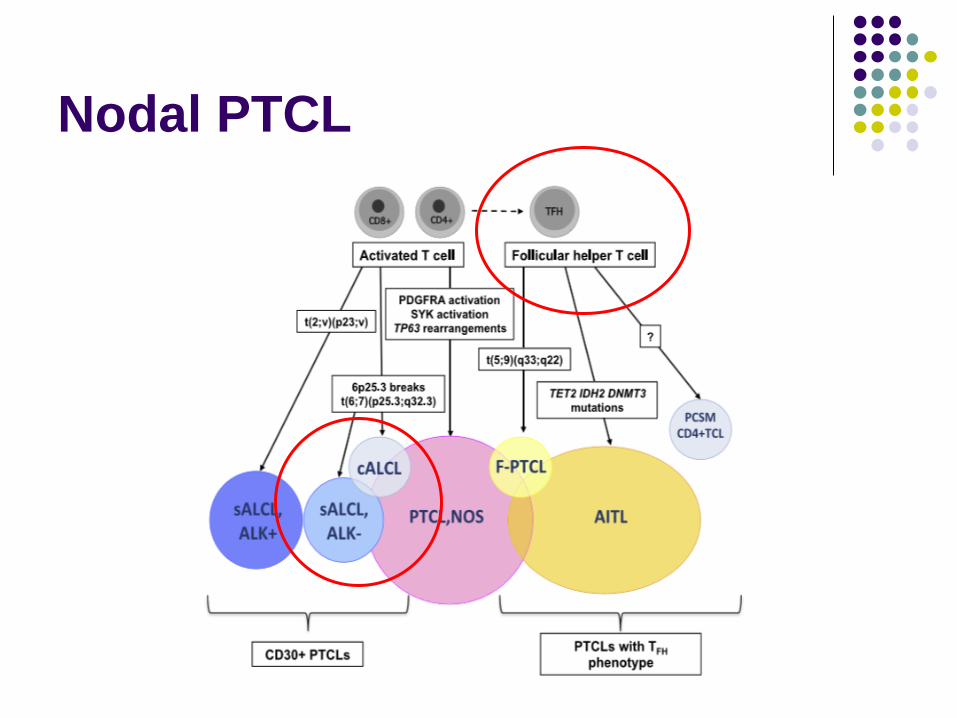
Nodal PTCL
T follicular helper cells (TFH)
Located in germinal center (GC) Interact with GC B-cells Contribute to high-affinity plasma cell/memory B
cells
Involved chemokine/receptor IL-21, CXCL13 for B-cell recruitment/activation CXCR5: receptor to CXCL13 Positive for PD1
AITL
De-novo T-cell lymphoma derived from αβ T-cells of follicular helper type (TFH)
Median age: 65, M:F = 1:1 No case in children
Advanced disease presentation Lymphadenopathy, hepatosplenomegaly Skin rash with pruritus Polyclonal hypergammaglobulinemia with
autoimmune phenomenon
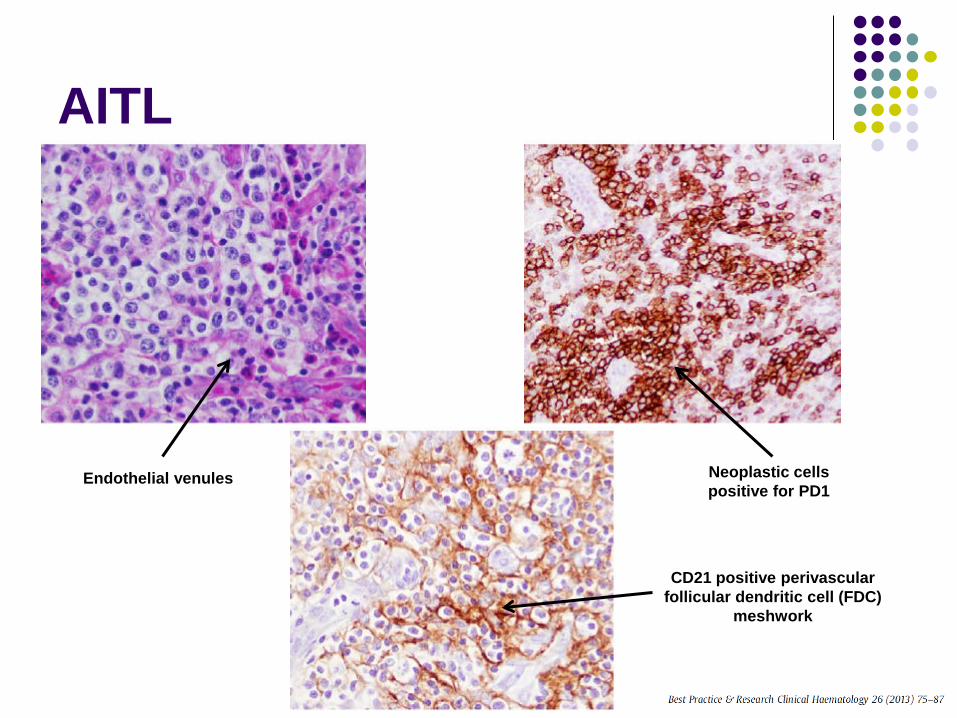
AITL
Neoplastic cells positive for PD1
CD21 positive perivascular follicular dendritic cell (FDC)
meshwork
Endothelial venules
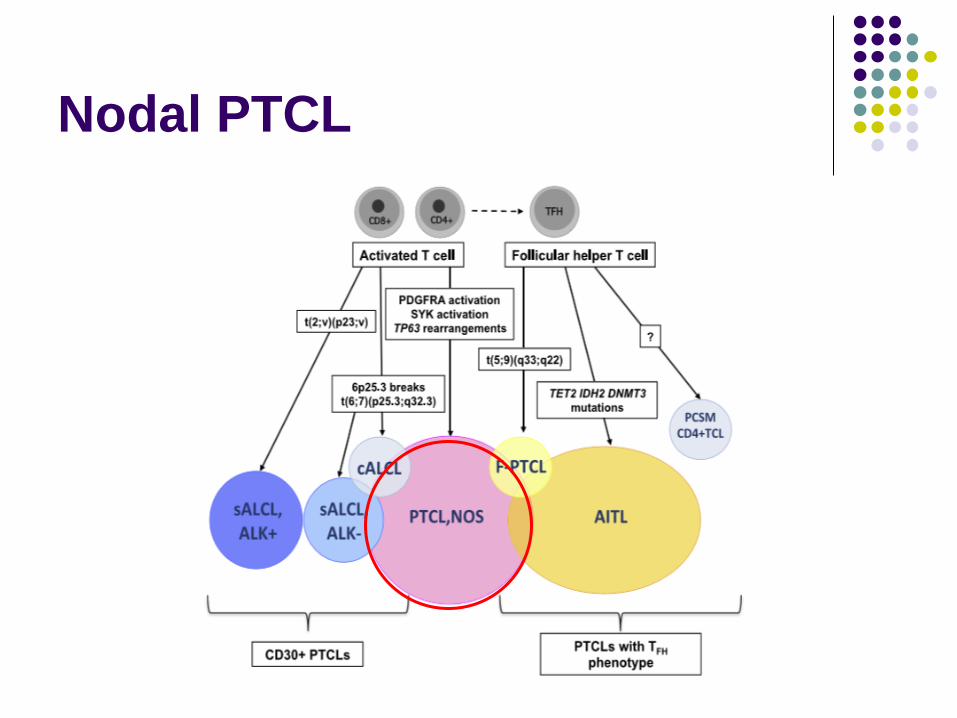
Nodal PTCL
PTCL, NOS 25% of all T-cell lymphomas Diagnosis of exclusion Similar to DLBCL, NOS
Mature T-cell phenotype Mostly, CD4 +
Clinical features Median age: 60, M:F = 2:1 Nodal presentation: ~90% Extranodal presentation: ~10%
Skin, GI tract
Question 2
What is correct about AITL? 1) More common in 40-50 year-old male 2) Combined with monoclonal gammopathy 3) Follicular helper γδ T-cells origin 4) PD1-positive neoplastic T cells 5) Loss of CD21+ follicular dendritic cell
(FDC) meshwork
Treatment of nodal PTCL Clinical trial (Preferred)
ALCL, ALK+
- CHOP-21, CHOEP-21
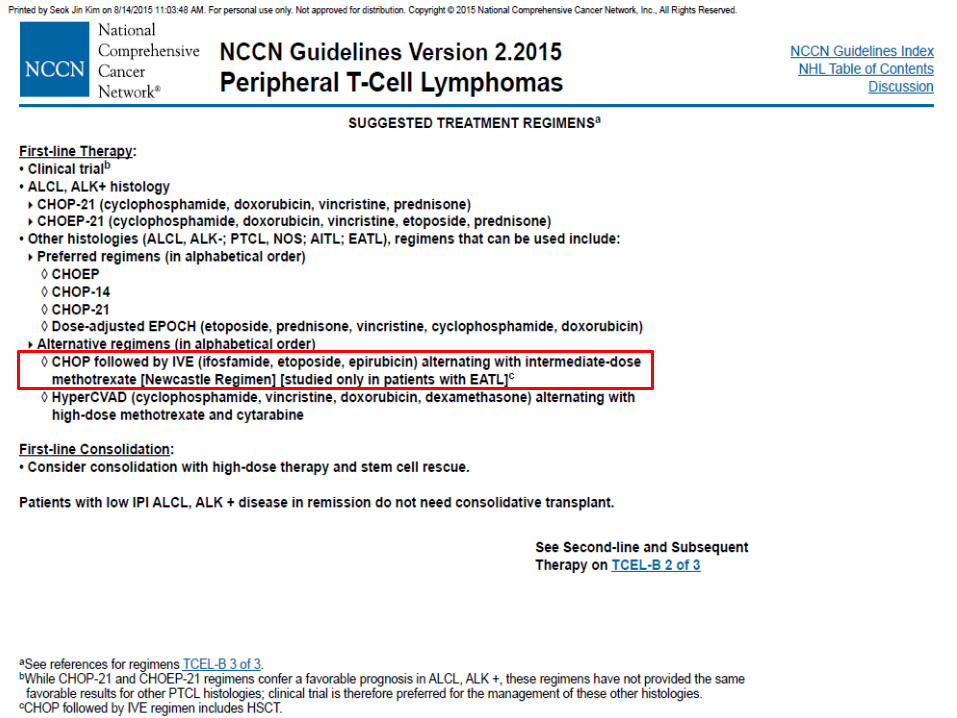
Other histology (ALCL, ALK-; PTCL, NOS; AITL; EATL)
- Preferred regimens (in alphabetical order)
CHOEP, CHOP-14, CHOP-21
Dose-adjusted EPOCH
- Alternative regimens (in alphabetical order)
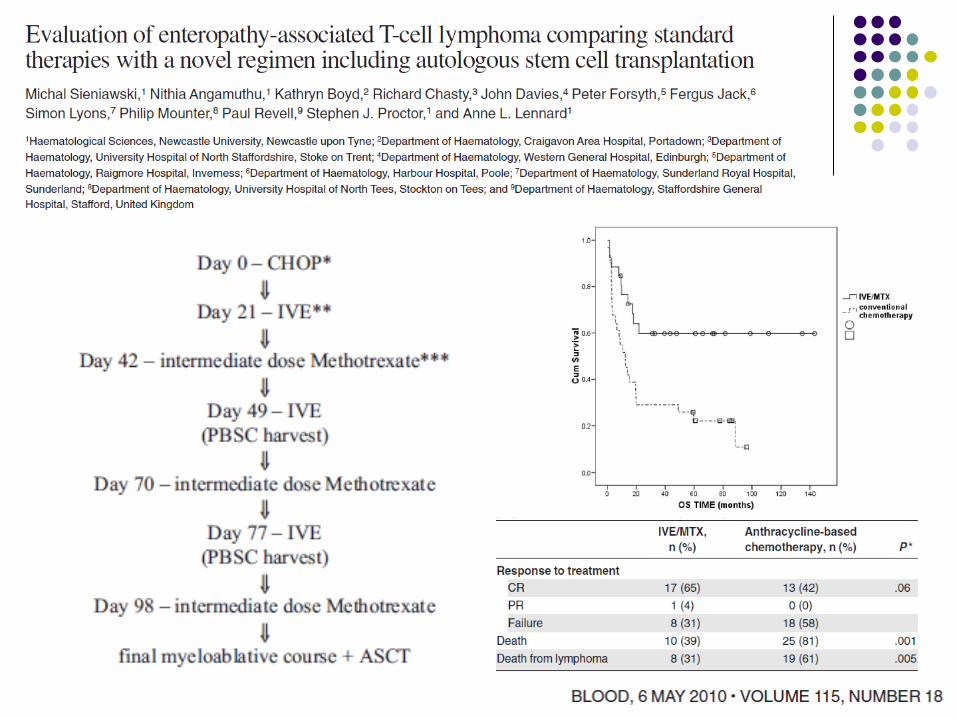
CHOP followed by IVE (ifosfamide, VP16, epirubicin) alternating
with intermediate-dose MTX
HyperCVAD alternating with high-dose MTX and cytarabine NCCN Guideline v.2. 2015
Question 3
A 57-year old male (newly diagnosed ALK-negative ALCL, stage II) achieved CR after 6 cycles of CHOP. What would you do next?
1) Observation 2) Involved field radiotherapy 3) Autologous stem cell transplantation 4) Allogeneic stem cell transplantation 5) Clinical trial with maintenance therapy
Question 4
A 57-year old male (newly diagnosed ALK-negative ALCL, stage IV) achieved CR after 6 cycles of CHOP. What would you do next?
1) Observation 2) Involved field radiotherapy 3) Autologous stem cell transplantation 4) Allogeneic stem cell transplantation 5) Clinical trial with maintenance therapy
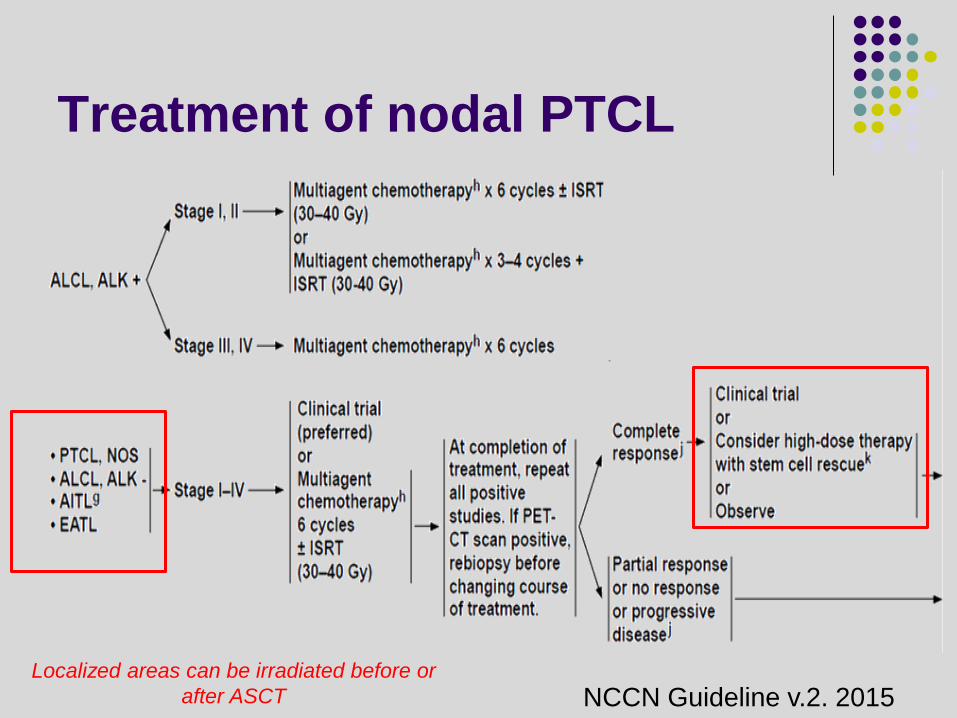
Treatment of nodal PTCL
NCCN Guideline v.2. 2015 Localized areas can be irradiated before or
after ASCT
First-line consolidation: SCT
Consolidation with high-dose chemotherapy and stem cell rescue should be considered
Patients with low IPI ALK+ ALCL in remission do not need consolidative transplant
NCCN Guideline v.2. 2015
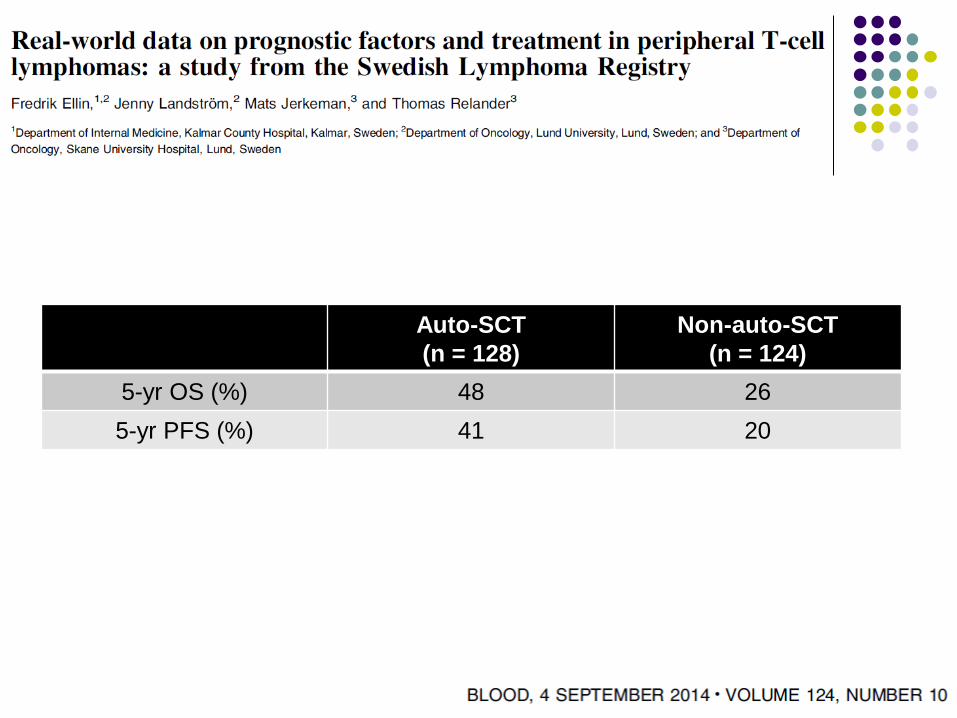
Auto-SCT (n = 128)
Non-auto-SCT (n = 124)
5-yr OS (%) 48 26 5-yr PFS (%) 41 20
Clin Cancer Res; 20(20); 5240–54.
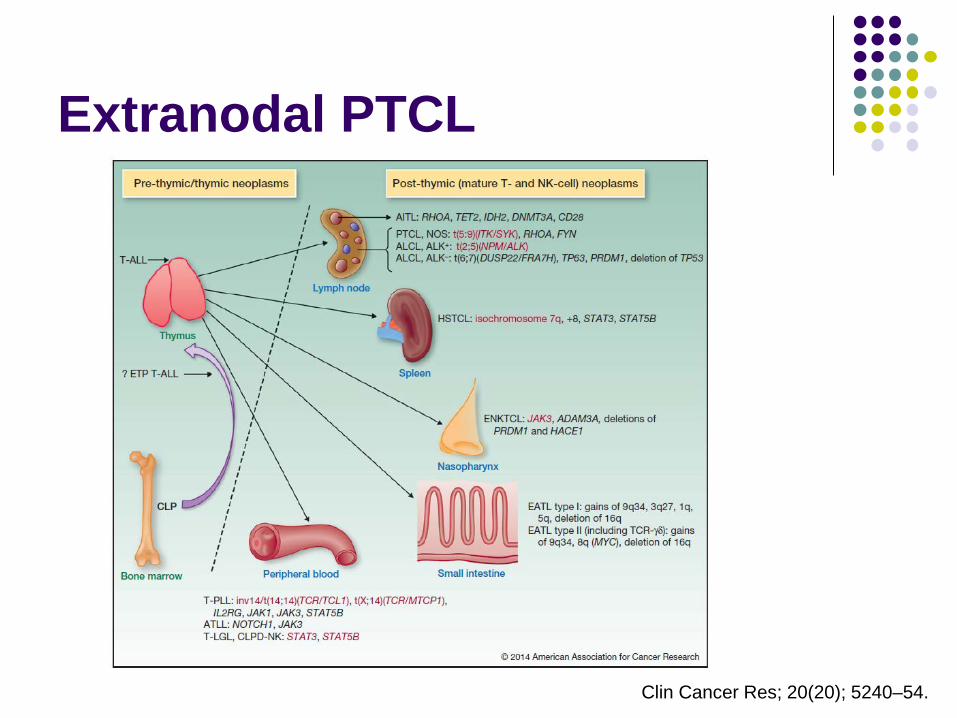
Extranodal PTCL
Extranodal NK/T-cell lymphoma, nasal type
Mainly upper aerodigestive tract EBV in situ +, CD56+, surface CD3-,
cytoplasmic CD3Ɛ+ Extranasal involvement: poorer prognosis Mainly NK cell origin, some cytotoxic T cell Synonyms Angiocentric T-cell lymphoma Malignant midline reticulosis Polymorphic reticulosis, Lethal midline granuloma
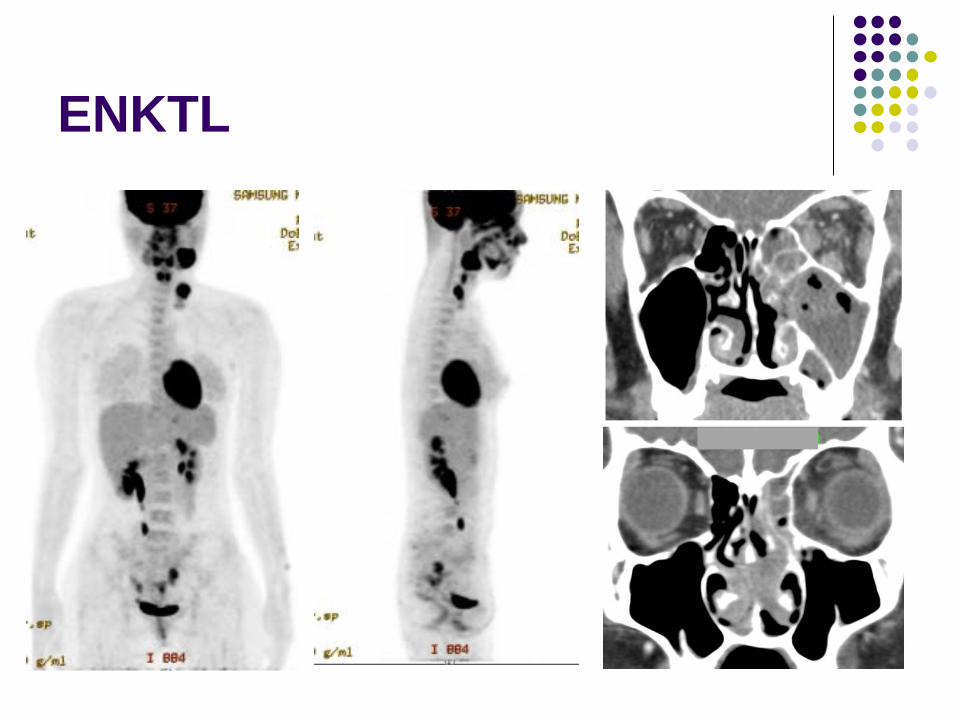
ENKTL
Treatment of extranodal NK/T-cell lymphoma
L-asparaginase-based combination chemotherapy AspaMetDex; SMILE
Concurrent chemoradiotherapy CCRT plus DeVIC or VIPD
Sequential chemoradiation SMILE or VIPD followed by RT
RT alone
NCCN Guideline v.2. 2015
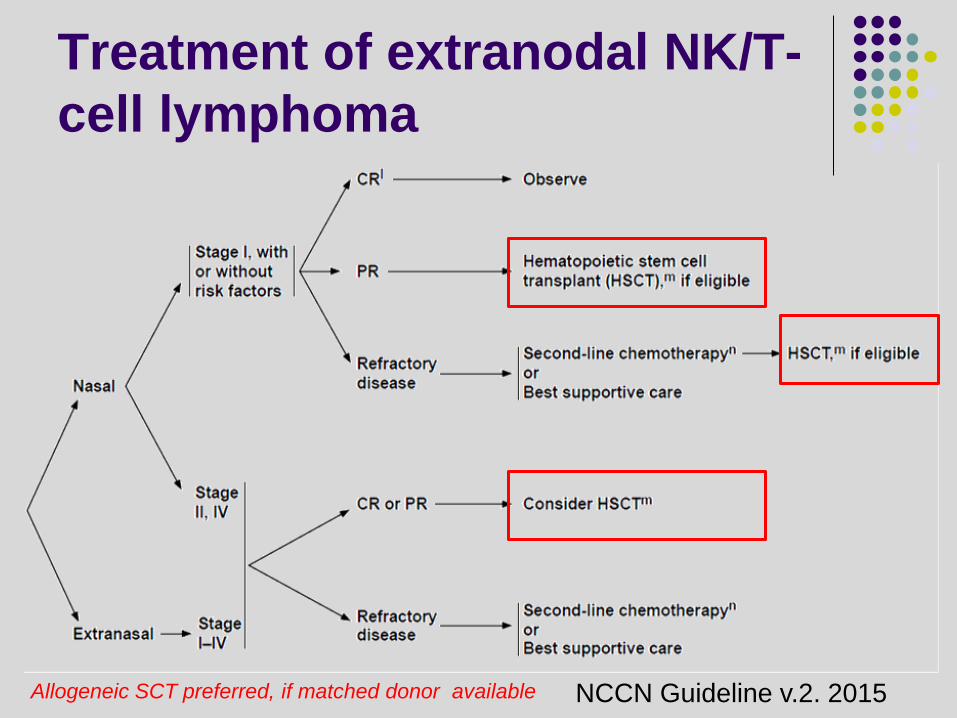
Treatment of extranodal NK/T-cell lymphoma
NCCN Guideline v.2. 2015 Allogeneic SCT preferred, if matched donor available
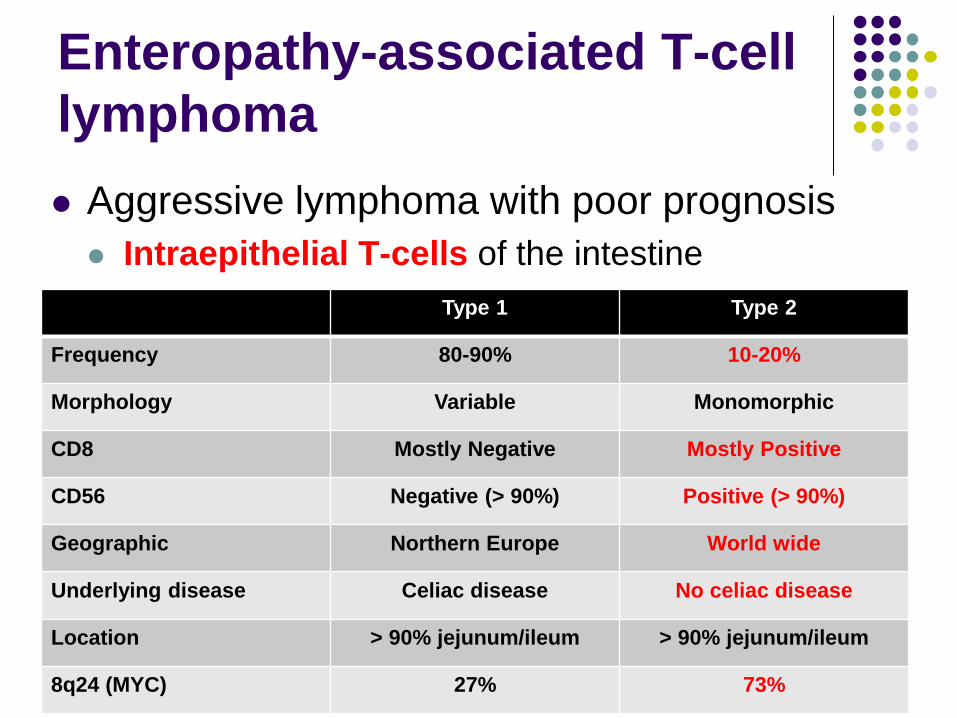
Enteropathy-associated T-cell lymphoma Aggressive lymphoma with poor prognosis Intraepithelial T-cells of the intestine
Type 1 Type 2
Frequency 80-90% 10-20%
Morphology Variable Monomorphic
CD8 Mostly Negative Mostly Positive
CD56 Negative (> 90%) Positive (> 90%)
Geographic Northern Europe World wide
Underlying disease Celiac disease No celiac disease
Location > 90% jejunum/ileum > 90% jejunum/ileum
8q24 (MYC) 27% 73%
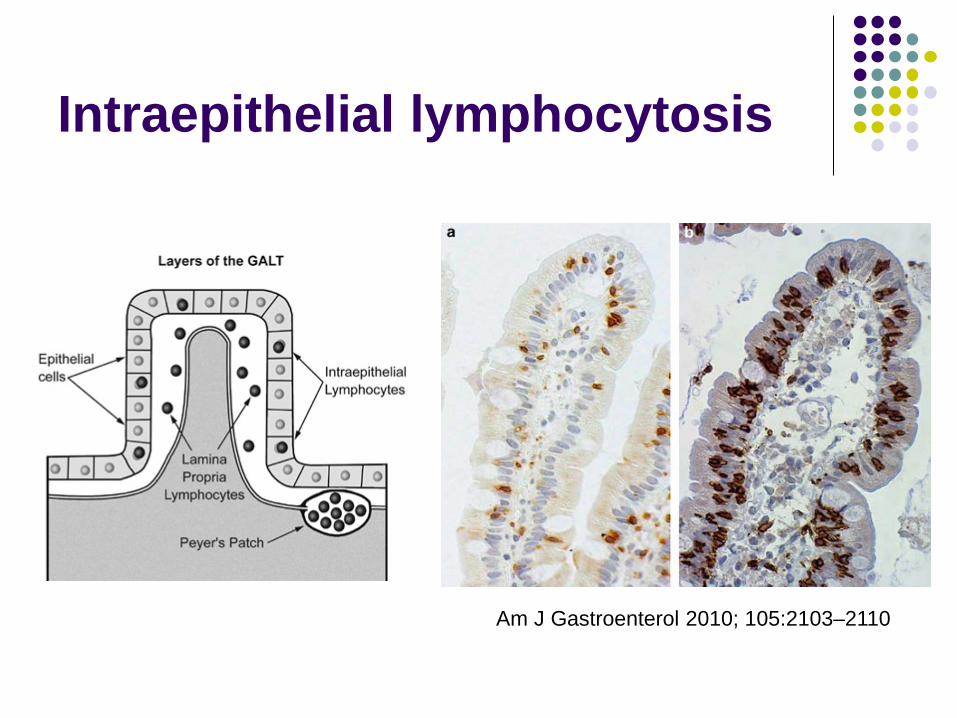
Intraepithelial lymphocytosis
Am J Gastroenterol 2010; 105:2103–2110
Question 5
What is correct about type II EATL? 1) More common in northern Europe 2) Combined with Celiac disease 3) Mostly intraepithelial γδ T-cells origin 4) CD8-negative/CD56-negative neoplastic
T cells 5) More frequent MYC amplification
Hepatosplenic T-cell lymphoma Aggressive lymphoma
originating from γδ cytotoxic T-cells (rarely, αβ T-cells)
Adolescents and young adults Strong male predominance Risk group Chronic antigenic stimulation Immunosuppression Crohn’s disease treated with IST
HSTL
Clinical features Systemic symptoms, thrombocytopenia, marked
hepatosplenomegaly Absence of lymphadenopathy
Prognosis Survival < 3 years Rapid relapse and fatal outcome even if very
good response to initial therapy
Peripheral T-cell lymphomas
Cutaneous Mycosis fungoides/Sezary syndrome Primary cutaneous CD30+ T-cell lymphoma Primary cutaneous anaplastic large cell lymphoma Subcutaneous panniculitis-like T-cell lymphoma Primary cutaneous γδ T-cells lymphoma Primary cutaneous CD8+ aggressive epidermotrophic
cytotoxic T-cell lymphoma
• Cell origin • αβ T-cells; γδ T-cells; NK cells
세조
세조는 꾸준한 온천 행궁에도 고질적인 피부병에 차도가 없었으며 결국 피부병과 정신질환이 악화돼 죽음을 맞았다.

천태종 구인사 벽화

Mycosis fungoides
Mycosis fungoides Definition Epidermotropic primary cutaneous T-cell lymphoma Infiltration of T-cells with cerebriform nuclei Skin lesion: patch, plaque and tumor
Indolent Clinical features Widespread skin lesion with slow progression Sometimes visceral involvement
Poor prognosis Advanced stage, Tumor stage Extracutaneous invasion
Sezary syndrome Triad Erythroderma Generalized lymphadenopathy Neoplastic T-cells with cerebriform nuclei (Sezary
cells) in skin, lymph nodes and blood Additional hematologic features: at least one Absolute Sezary cell count ≥ 1000/mm3
CD4/CD8 ratio > 10 Aggressive 5yr OS 10-20%, Opportunistic infection
MF vs. SS
Mycosis fungoides 50% of CTCL Adults/elderly Male CD4 T-cell origin Similar morphology Indolent
Sezary syndrome 5% of CTCL Over 60 years Male CD4 T-cell origin Similar morphology Aggressive
Treatment for MF/SS Skin Directed
Topical steroids
Topical nitrogen mustard: mechlorethamine
Topical bexarotene gel
Phototherapy
– NBUVB
– PUVA
Radiation therapy
– Total skin electron beam
– Localized electron beam
Systemic
Bexarotene capsules
Vorinostat capsules
Methotrexate
Interferon
Extracorporeal photochemotherapy
Denileukin diftitox
Single-agent chemotherapy
Combination chemotherapy
Subcutaneous Panniculitis like T-cell lymphoma
Wide age distribution Median age: 35 years
Subcutaneous nodules on extremities and trunk
Pathology Subcutaneous lesion sparing dermis CD8+, CD56- Originating from cytotoxic αβ T-cells Positive cytotoxic markers: TIA1, perforin, granzyme B
SPTCL
Combined with autoimmune disease ~20%: e.g. SLE
Combined with hemophagocytosis ~15-20%, severe cytopenia and liver dysfunction Poor prognosis
Lymph node invasion and other sites involvement are rare
Relatively good prognosis 5-yr OS > 80%
Primary cutaneous ALCL Same morphology with ALCL, ALK- Cutaneous tumors of anaplastic large cells with
CD30 positivity Excellent prognosis: > 90% of 5-yr OS Regional LN involvement: not necessarily indicate
aggressive course Treatment strategy Local therapy: Main treatment modality Systemic therapy Watch and wait: Spontaneous regression is possible
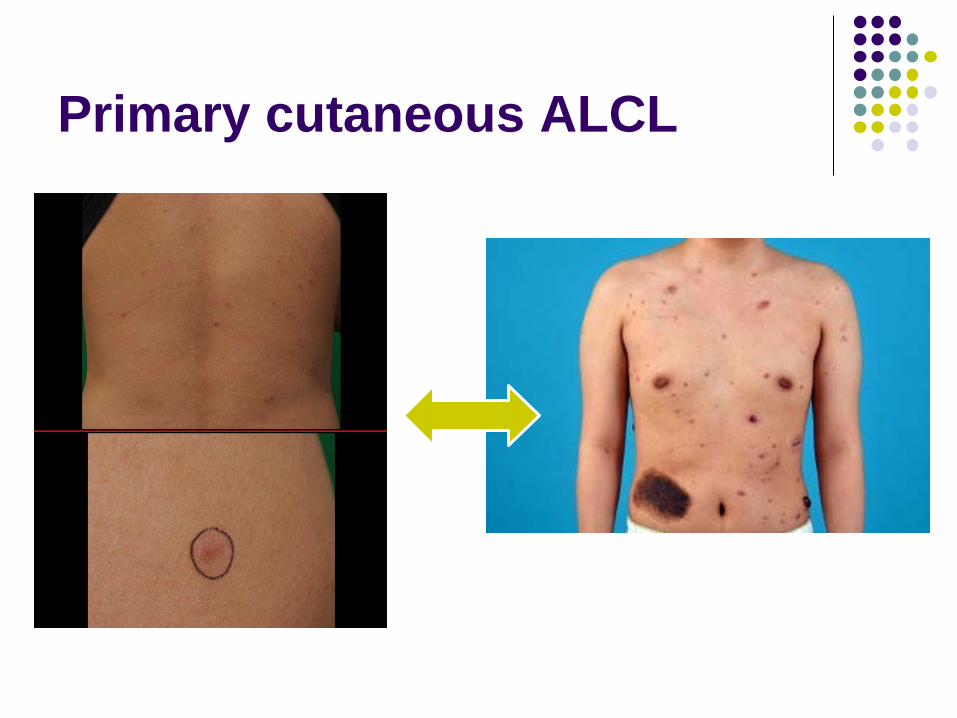
Primary cutaneous ALCL
Peripheral T-cell lymphomas
Disseminated/leukemic T-cell prolymphocytic leukemia T-cell large granular lymphocytic leukemia Chronic lymphoproliferative disorders of NK cells Aggressive NK cell leukemia EBV-positive T-cell lymphoproliferative disease Adult T-cell leukemia/lymphoma
• Cell origin • αβ T-cells; γδ T-cells; NK cells
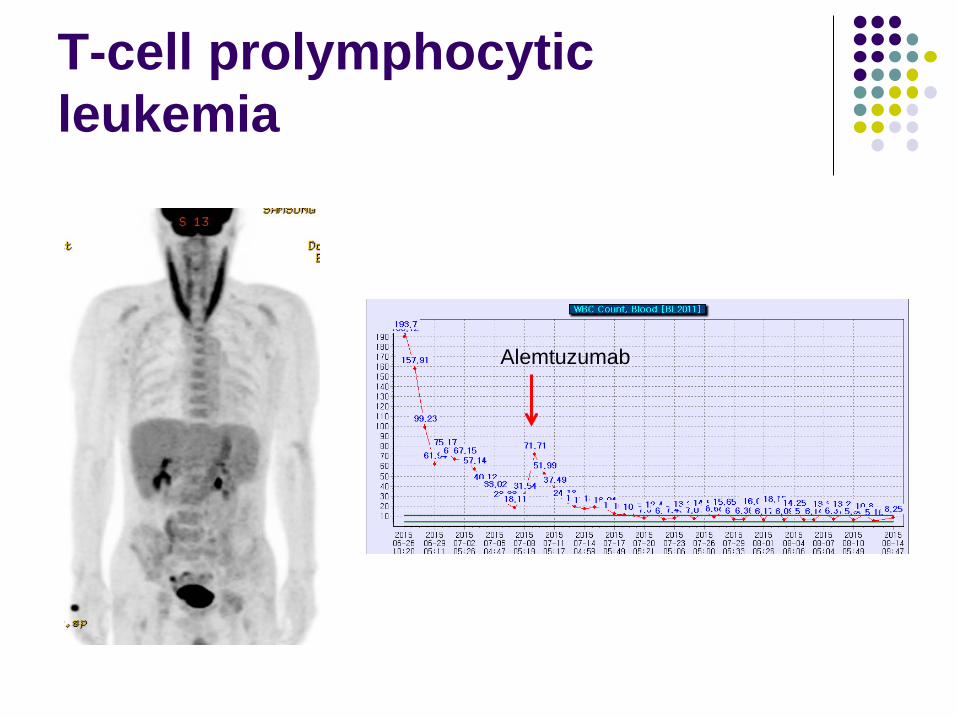
T-cell prolymphocytic leukemia
Alemtuzumab
Aggressive NK-cell leukemia
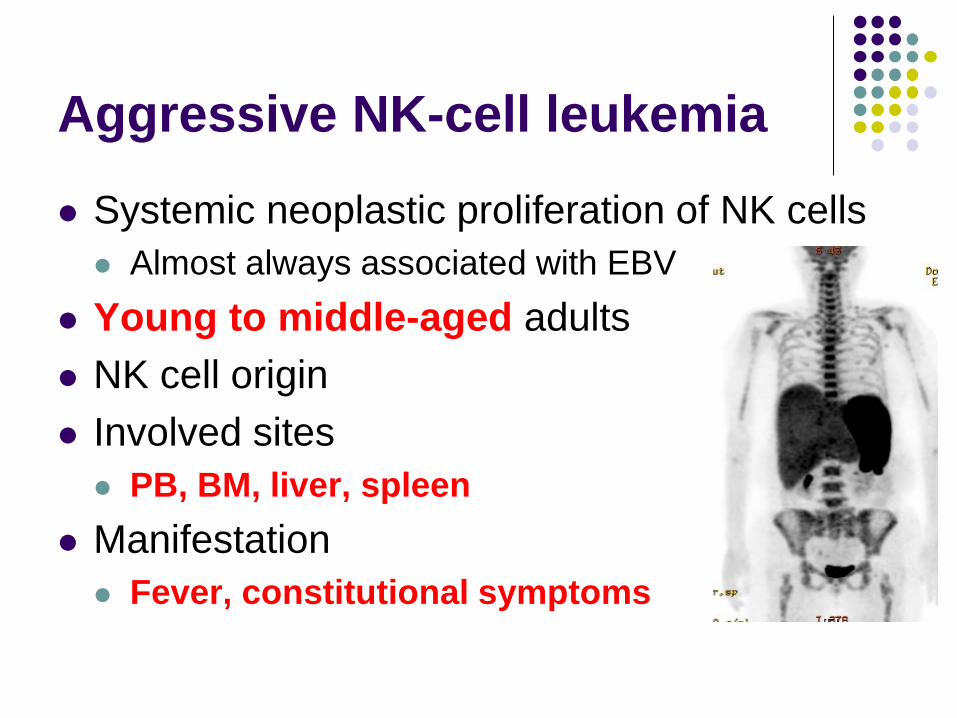
Systemic neoplastic proliferation of NK cells Almost always associated with EBV
Young to middle-aged adults NK cell origin Involved sites PB, BM, liver, spleen
Manifestation Fever, constitutional symptoms
Aggressive NK-cell leukemia
Lab Leukemic blood picture: low or high leukemic cells Pancytopenia with hemophagocytosis Markedly elevated serum LDH Coagulopathy
Pathology Identical to ENKTL
Prognosis Extremely poor: < 2 years
Question 6 : ANKL vs. ENKTL stage IV
What is more close to ANKL than ENKTL? 1) Older age 2) More frequent skin invasion 3) Lack of CD16 expression 4) Better outcome 5) Markedly elevated serum LDH
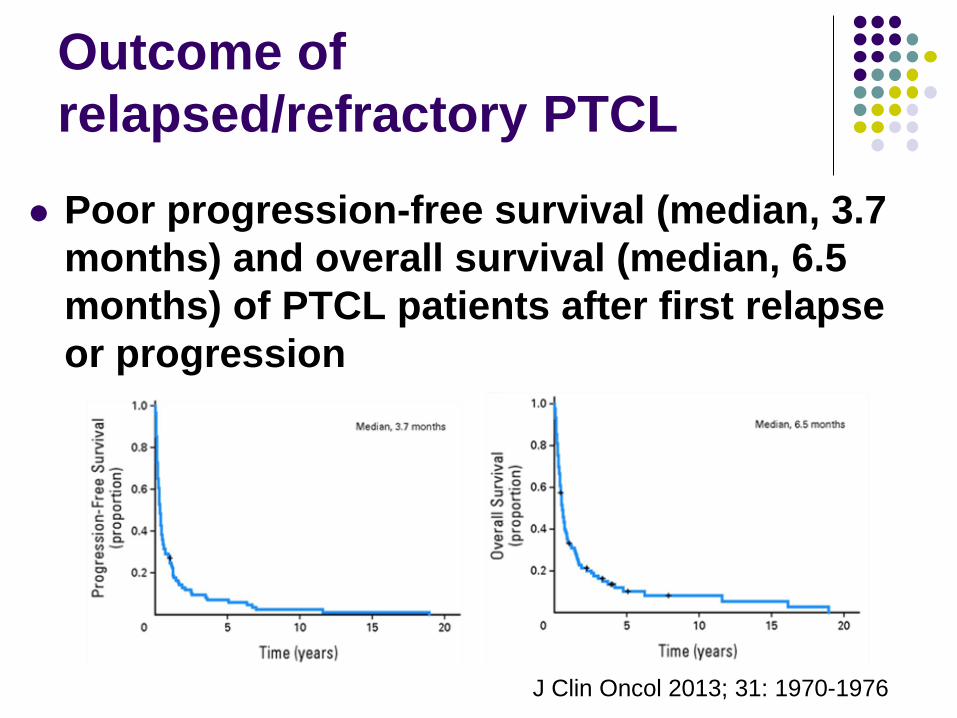
Outcome of relapsed/refractory PTCL
Poor progression-free survival (median, 3.7 months) and overall survival (median, 6.5 months) of PTCL patients after first relapse or progression
J Clin Oncol 2013; 31: 1970-1976
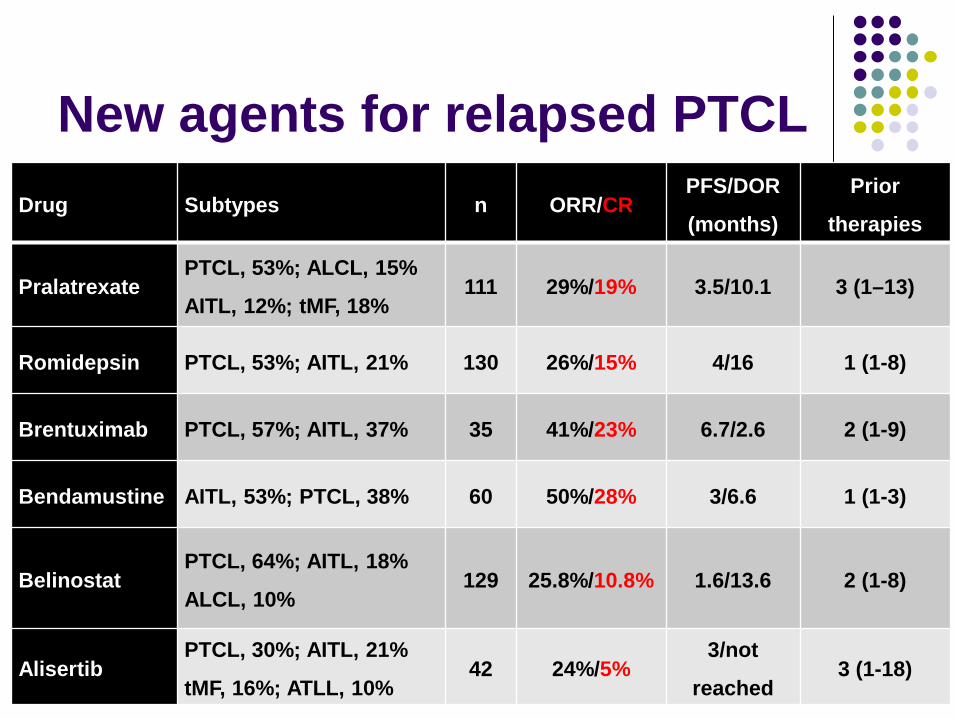
New agents for relapsed PTCL Drug Subtypes n ORR/CR
PFS/DOR
(months)
Prior
therapies
Pralatrexate PTCL, 53%; ALCL, 15%
AITL, 12%; tMF, 18% 111 29%/19% 3.5/10.1 3 (1–13)
Romidepsin PTCL, 53%; AITL, 21% 130 26%/15% 4/16 1 (1-8)
Brentuximab PTCL, 57%; AITL, 37% 35 41%/23% 6.7/2.6 2 (1-9)
Bendamustine AITL, 53%; PTCL, 38% 60 50%/28% 3/6.6 1 (1-3)
Belinostat PTCL, 64%; AITL, 18%
ALCL, 10% 129 25.8%/10.8% 1.6/13.6 2 (1-8)
Alisertib PTCL, 30%; AITL, 21%
tMF, 16%; ATLL, 10% 42 24%/5%
3/not
reached 3 (1-18)
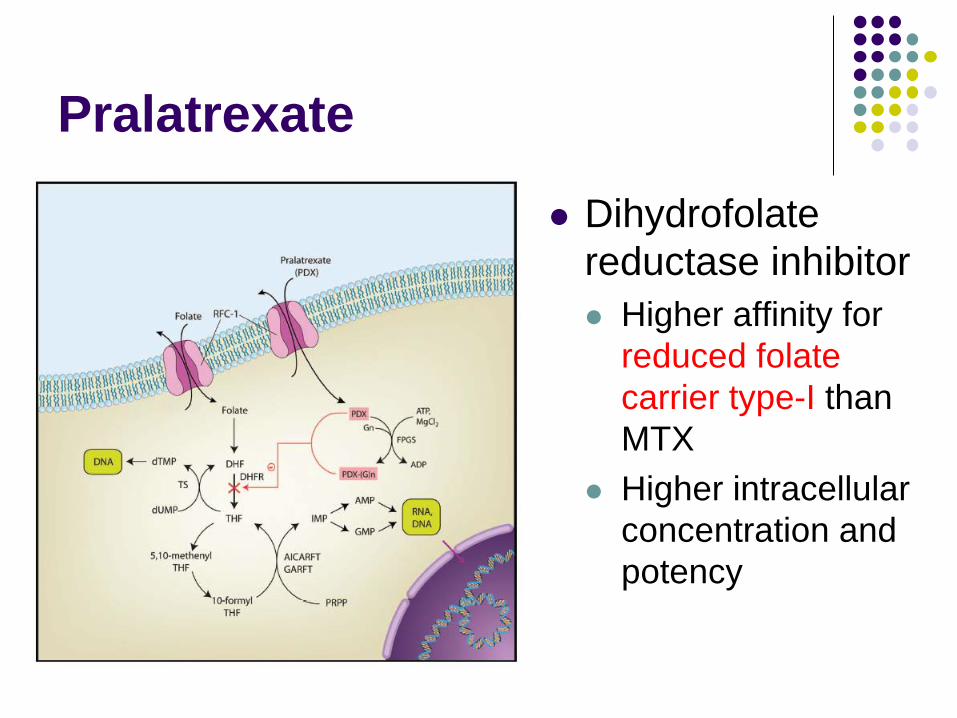
Pralatrexate
Dihydrofolate reductase inhibitor Higher affinity for
reduced folate carrier type-I than MTX
Higher intracellular concentration and potency
Romidepsin Cyclic peptide Intravenous agent HDAC class I target FDA approval: Relapsed CTCL/PTCL after at
least one prior systemic chemotherapy
Overall therapeutic effect Induction of apoptosis, cell cycle arrest,
autophagy, immune modulation etc
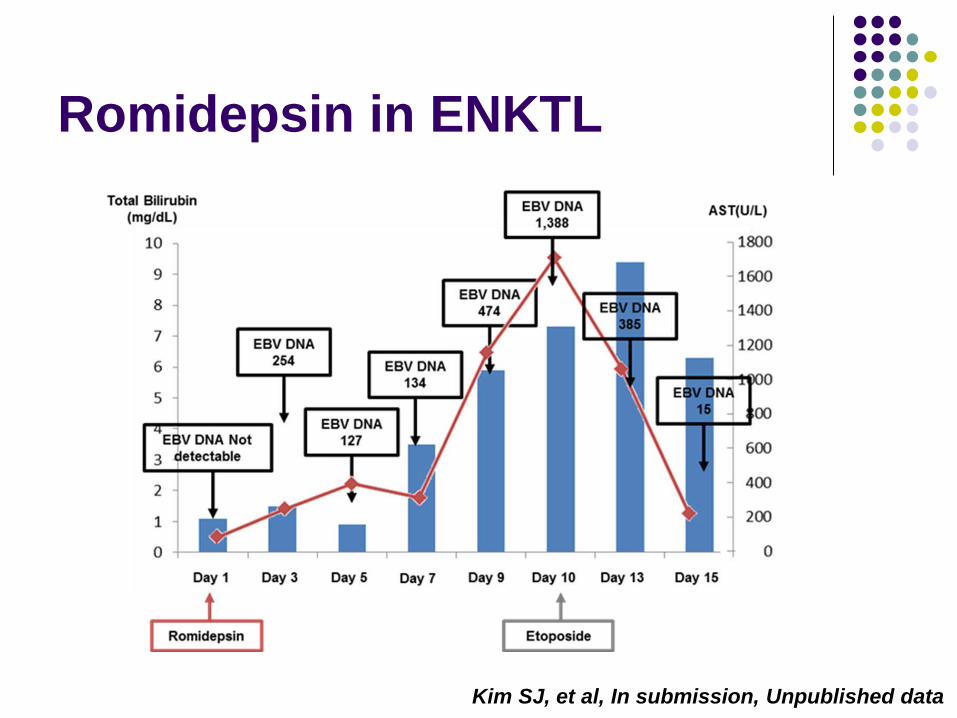
Romidepsin in ENKTL
Kim SJ, et al, In submission, Unpublished data
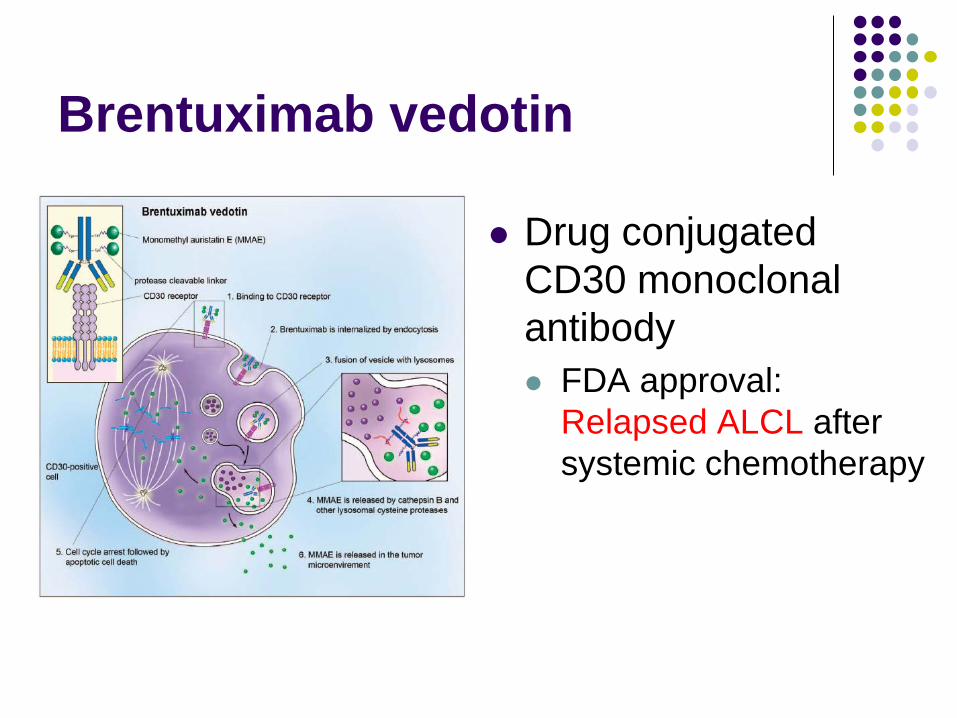
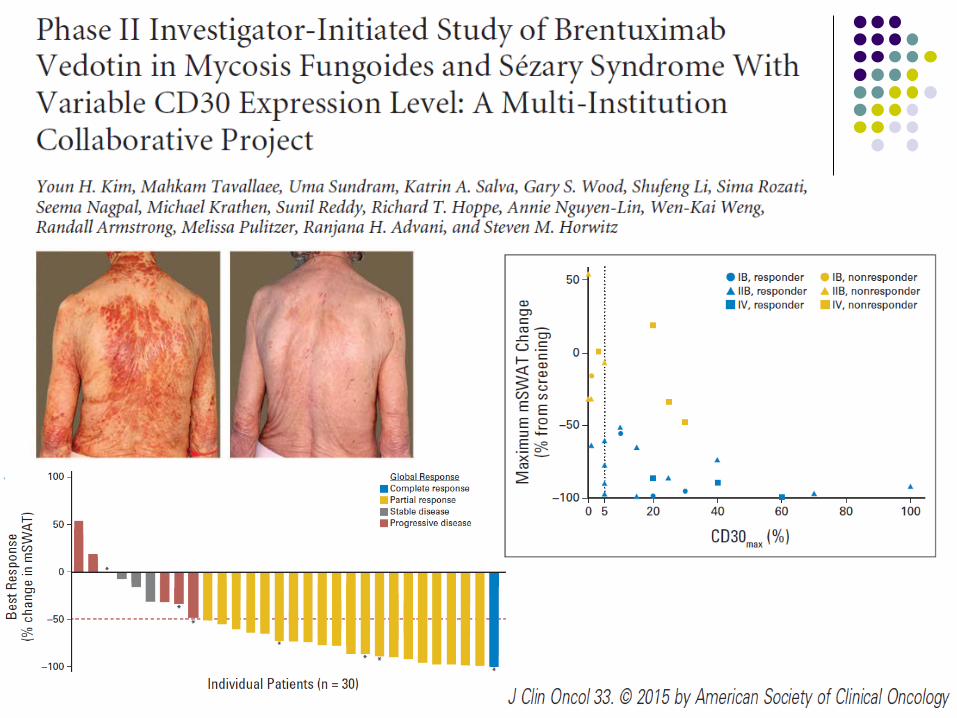
Brentuximab vedotin
Drug conjugated CD30 monoclonal antibody FDA approval:
Relapsed ALCL after systemic chemotherapy
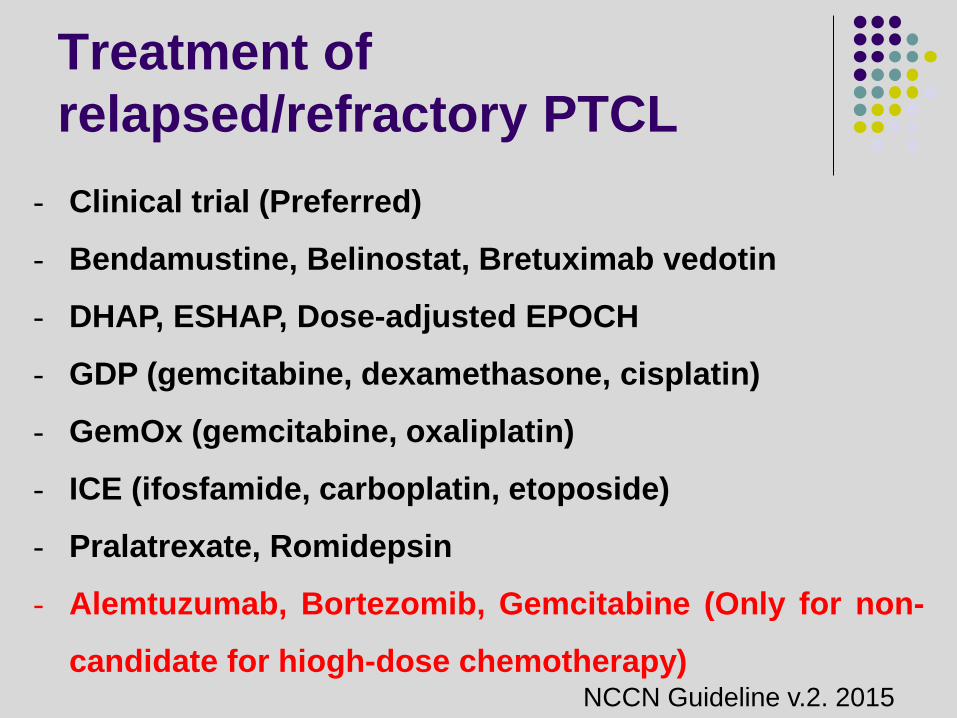
Treatment of relapsed/refractory PTCL
- Clinical trial (Preferred)
- Bendamustine, Belinostat, Bretuximab vedotin
- DHAP, ESHAP, Dose-adjusted EPOCH
- GDP (gemcitabine, dexamethasone, cisplatin)
- GemOx (gemcitabine, oxaliplatin)
- ICE (ifosfamide, carboplatin, etoposide)
- Pralatrexate, Romidepsin
- Alemtuzumab, Bortezomib, Gemcitabine (Only for non-
candidate for hiogh-dose chemotherapy) NCCN Guideline v.2. 2015
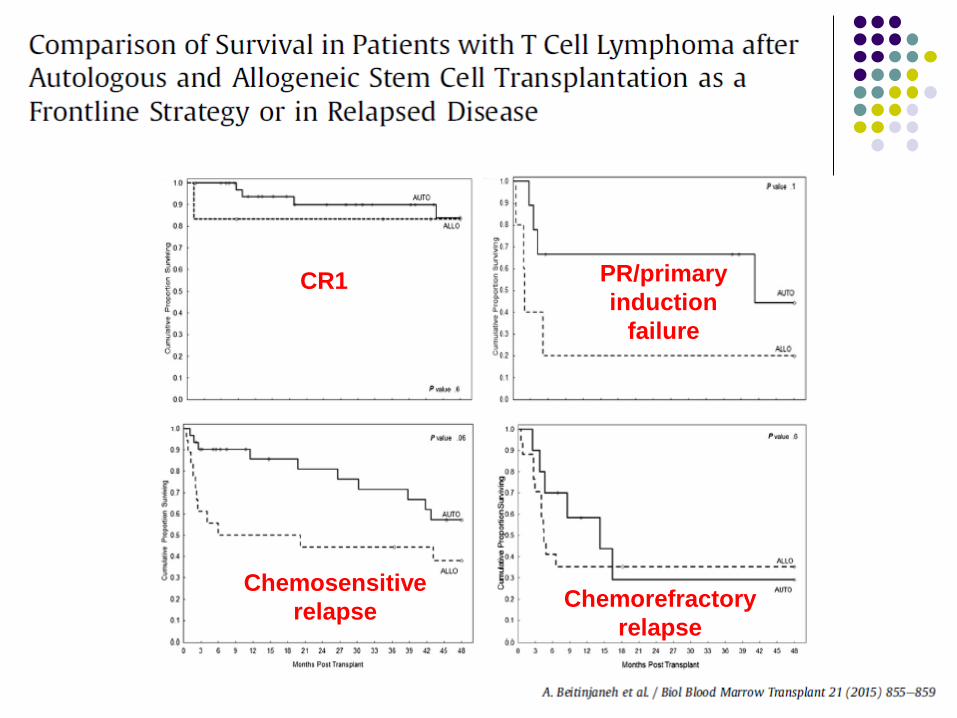
CR1 PR/primary induction
failure
Chemosensitive relapse Chemorefractory
relapse
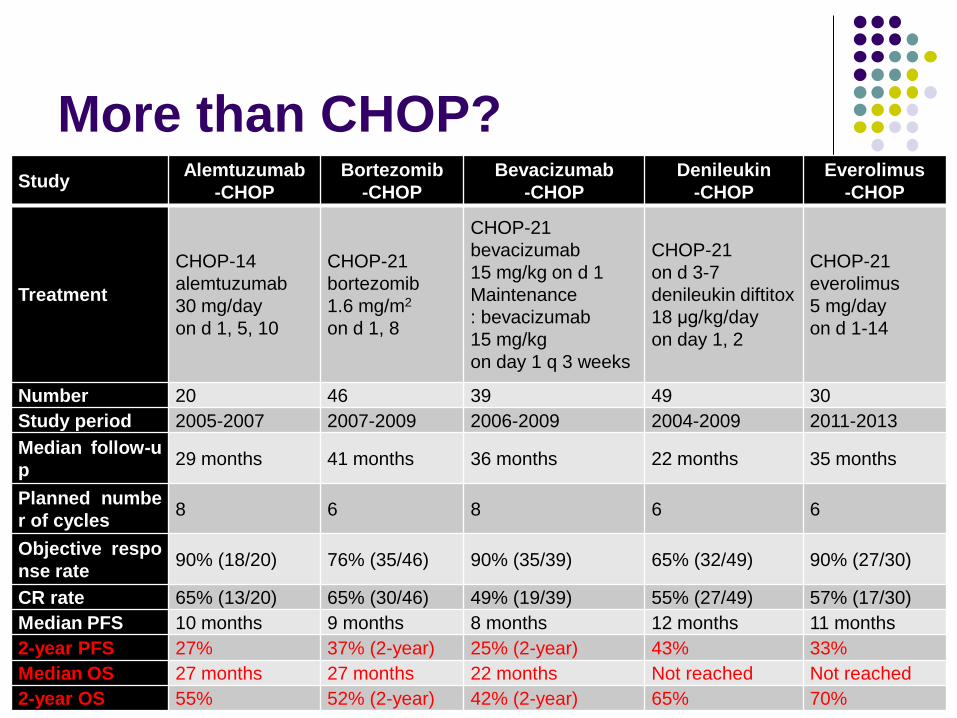
More than CHOP? Study Alemtuzumab
-CHOP Bortezomib
-CHOP Bevacizumab
-CHOP Denileukin
-CHOP Everolimus
-CHOP
Treatment
CHOP-14 alemtuzumab 30 mg/day on d 1, 5, 10
CHOP-21 bortezomib 1.6 mg/m2 on d 1, 8
CHOP-21 bevacizumab 15 mg/kg on d 1 Maintenance : bevacizumab 15 mg/kg on day 1 q 3 weeks
CHOP-21 on d 3-7 denileukin diftitox 18 μg/kg/day on day 1, 2
CHOP-21 everolimus 5 mg/day on d 1-14
Number 20 46 39 49 30 Study period 2005-2007 2007-2009 2006-2009 2004-2009 2011-2013 Median follow-up 29 months 41 months 36 months 22 months 35 months
Planned number of cycles 8 6 8 6 6
Objective response rate 90% (18/20) 76% (35/46) 90% (35/39) 65% (32/49) 90% (27/30)
CR rate 65% (13/20) 65% (30/46) 49% (19/39) 55% (27/49) 57% (17/30) Median PFS 10 months 9 months 8 months 12 months 11 months 2-year PFS 27% 37% (2-year) 25% (2-year) 43% 33% Median OS 27 months 27 months 22 months Not reached Not reached 2-year OS 55% 52% (2-year) 42% (2-year) 65% 70%
Ongoing study for newly diagnosed PTCL
Romidepsin-CHOP (Ro-CHOP) vs CHOP Estimate number: 420 over 43 months
Pralatrexate vs. Observation following CHOP Pralatrexate IV 30 mg/m2 weekly for 3 weeks of a 4-
week cycle (n = 549) Brentuximab/CHOP for CD30-positive mature
T-cell lymphomas Comparison of Brentuximab/CHP with CHOP
Take Home Message
Problems of PTCL Heterogeneous subtypes Efficacy of induction therapy: unsatisfactory Efficacy of SCT: auto vs. allo
Development of novel drugs Expansion of new indication Combination with other drugs
Identification of newer therapeutic targets is warranted