ORIGINAL ARTICLE INCREASED OXIDATIVE STRESS AND IRON ... · ORIGINAL ARTICLE INCREASED OXIDATIVE...
13
Hemoglobin, 35(1):67–79, (2011) Copyright © Informa Healthcare USA, Inc. ISSN: 0363-0269 print/1532-432X online DOI: 10.3109/03630269.2010.544624 ORIGINAL ARTICLE INCREASED OXIDATIVE STRESS AND IRON OVERLOAD IN JORDANIAN β-THALASSEMIC CHILDREN Maher Y. Abdalla, 1 Mohammad Fawzi, 1 Salem R. Al-Maloul, 1 Nasser El-Banna, 2 Reema F. Tayyem, 3 and Iman M. Ahmad 4 1 Department of Biological Sciences and Biotechnology, The Hashemite University, Zarqa, Jordan 2 Department of Clinical Nutrition and Dietetics, The Hashemite University, Zarqa, Jordan 3 Department of Medical Laboratory Sciences, The Hashemite University, Zarqa, Jordan 4 Department of Radiography, The Hashemite University, Zarqa, Jordan β -Thalassemia (β -thal) is associated with abnormal synthesis of hemoglobin (Hb). Repeated blood transfusions in patients with β -thal major (β -TM) leads to an enhanced generation of reactive oxygen species (ROS), and subjects patients to peroxidative injury. We studied the antioxidant status and oxidative damage to children with β -thal in Jordan. Samples from 40 children with β -thal and 40 healthy controls were used. All children were under 13 years of age. Our results showed that plasma thiobarbituric acid reactive substances (TBARS) were elevated in β -thalassemic children compared to controls together with compensatory increase in superoxide dismutase (SOD) activity and decrease in catalase (CAT) activity. Elevated serum ferritin showed positive correlation with elevated liver enzyme levels except gamma glutamyl transferase (GGT), confirming liver involvement due to iron overload. Serum ferritin also showed a positive correlation with elevated TBARS and SOD, suggesting that iron overload is involed in the oxidative stress shown in cells. Keywords Oxidative stress, Thalassemia, Glutathione (GSH), thiobarbituric acid reac- tive substances (TBARS) INTRODUCTION Thalassemias are a group of hereditary anemias which occur as a result of genetic disorders that affect the synthesis of normal hemoglobin (Hb), in which a reduced rate of synthesis of one or more of the globin chains leads Received 17 June 2010; Accepted 22 September 2010. Address correspondence to Maher Y. Abdalla, Ph.D., Center for Cancer Research, NCI, National Naval Medical Center, Bldg. 8, Rm. 5101, 8901 Wisconsin Avenue, Bethesda, MD 20889, USA; Tel: +301-402-5159; Fax: +301-496-0047; E-mail: [email protected] 67 Hemoglobin Downloaded from informahealthcare.com by Digestive Diseases Branch on 01/20/11 For personal use only.
Transcript of ORIGINAL ARTICLE INCREASED OXIDATIVE STRESS AND IRON ... · ORIGINAL ARTICLE INCREASED OXIDATIVE...

Hemoglobin, 35(1):67–79, (2011)Copyright © Informa Healthcare USA, Inc.ISSN: 0363-0269 print/1532-432X onlineDOI: 10.3109/03630269.2010.544624
ORIGINAL ARTICLE
INCREASED OXIDATIVE STRESS AND IRON OVERLOAD IN
JORDANIAN β-THALASSEMIC CHILDREN
Maher Y. Abdalla,1 Mohammad Fawzi,1 Salem R. Al-Maloul,1
Nasser El-Banna,2 Reema F. Tayyem,3 and Iman M. Ahmad4
1Department of Biological Sciences and Biotechnology, The Hashemite University, Zarqa, Jordan2Department of Clinical Nutrition and Dietetics, The Hashemite University, Zarqa, Jordan3Department of Medical Laboratory Sciences, The Hashemite University, Zarqa, Jordan4Department of Radiography, The Hashemite University, Zarqa, Jordan
� β-Thalassemia (β-thal) is associated with abnormal synthesis of hemoglobin (Hb). Repeatedblood transfusions in patients with β-thal major (β-TM) leads to an enhanced generation of reactiveoxygen species (ROS), and subjects patients to peroxidative injury. We studied the antioxidantstatus and oxidative damage to children with β-thal in Jordan. Samples from 40 children withβ-thal and 40 healthy controls were used. All children were under 13 years of age. Our results showedthat plasma thiobarbituric acid reactive substances (TBARS) were elevated in β-thalassemic childrencompared to controls together with compensatory increase in superoxide dismutase (SOD) activityand decrease in catalase (CAT) activity. Elevated serum ferritin showed positive correlation withelevated liver enzyme levels except gamma glutamyl transferase (GGT), confirming liver involvementdue to iron overload. Serum ferritin also showed a positive correlation with elevated TBARS andSOD, suggesting that iron overload is involed in the oxidative stress shown in cells.
Keywords Oxidative stress, Thalassemia, Glutathione (GSH), thiobarbituric acid reac-tive substances (TBARS)
INTRODUCTION
Thalassemias are a group of hereditary anemias which occur as a resultof genetic disorders that affect the synthesis of normal hemoglobin (Hb), inwhich a reduced rate of synthesis of one or more of the globin chains leads
Received 17 June 2010; Accepted 22 September 2010.Address correspondence to Maher Y. Abdalla, Ph.D., Center for Cancer Research, NCI, National
Naval Medical Center, Bldg. 8, Rm. 5101, 8901 Wisconsin Avenue, Bethesda, MD 20889, USA; Tel:+301-402-5159; Fax: +301-496-0047; E-mail: [email protected]
67
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

68 M.Y. Abdalla et al.
to defective Hb production, and damage to the red cells or their precursors(1). β-Thalassemia (β-thal) is more common in Mediterranean countriesand islands including Cyprus, Sardinia, and Malta (2). However both α- andβ-thal types are common in Africans and Black Americans (3). Thalassemiais usually associated with many complications such as hepatosplenomegaly,infections, gall stones and bone deformities that alter facial features andresult in pathogenic fractures (4). Studies on β-thal patients suggest thatthey may develop symptoms of iron loading that includes chelating therapycomplications, heart and liver diseases, and endocrinopathies (5).
Normally, erythrocytes degrade reactive oxygen species (ROS) via theactions of superoxide dismutase (SOD), catalase (CAT) and glutathioneperoxidase (Gpx) (6). In β-thal major (β-TM), intraerythrocytic releaseof heme induces a glutathione (GSH)-dependent self-amplifying and self-propagating Hb oxidation pathway, resulting in injury to the thalassemiccell (6). In addition, iron can serve as a potent catalyst of lipid peroxidation(7). The presence of hypochromia may facilitate oxidation of the red cellmembrane by reducing the amount of Hb available for buffering protection(8). The peripheral red cells of patients with β-TM demonstrate a varietyof morphological, biochemical and metabolic changes, which specificallycontribute to the extent and severity of lipid peroxidation and hemolysis(9). Unpaired α-Hb chains may denature and bind to the cell membrane,thus giving rise to cytoskeleton alterations and lipid peroxidation (10). Thefree α chains in β-thal increase autoxidation rates by about two times fasterthan normal Hb A (7). It has been reported that the accumulation andautoxidation of the unpaired α-globin chains in severe β-thal would gen-erate ROS; superoxide (O2
−) and hydrogen peroxide (H2O2) that wouldcause accelerated apoptosis and ineffective erythropoiesis (6,11).
Therefore, we hypothesize that oxidative stress is a major factor ofmorbidity in Jordanian β-thalassemic children and is correlated with ironoverload and metabolic dysfunctions. In order to verify this hypothesis weevaluated different liver function enzymes such as aspartate amino trans-ferase (AST), alanine amino transferase (ALT), gamma glutamyl transferase(GGT), alkaline phosphatase (ALP) and correlated them to ferritin levelsin thalassemia patients receiving repeated blood transfusions. We also mea-sured oxidative stress parameters including the lipid oxidation biomarker;malondialdehyde (MDA) and major antioxidant enzymes such as SOD andCAT in the serum of thalassemic patients and normal controls.
MATERIALS AND METHODS
Patients and Controls
Forty Jordanian children with β-TM who underwent periodical bloodtransfusions and received deferoxamine (DFO) as a chelating agent were
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

Oxidative Stress and Pediatric Thalassemia in Jordan 69
recruited for this study. Patients were free of hepatitis B virus (HBV), hep-atitis C virus (HCV) and human immunodeficiency virus (HIV). This groupwas aged between 2 and12 years old and was treated at the ThalassemiaUnit at Princess Rahma Educational Hospital, Irbid, Jordan (20 female and20 male patients). Another 40 healthy children aged between 5 and 12 yearsold was used as the control group (20 males and 20 females).
Specimen Collection and Basic Analysis
Blood samples were collected from an antecubital vein of β-TM patientsand the control group. Blood was drawn in ethylene diamine tetracetic acid(EDTA), and plain tubes. All serum specimens (from patients and controls)were assayed directly for AST, ALT, GGT, ALP, enzymatic activity assays, aswell as serum ferritin concentration. All serum specimens were separatedand kept at −20◦C until assayed for MDA, SOD, and CAT tests.
Hemoglobin Analyses
The Hb of whole blood was assayed using 50 μL anticoagulated blood ina blood analyzer (BC-2800 Mindray Auto Hematology Analyzer, Shenzhen,People’s Republic of China). The AST and ALT activity was assayedusing commercial kits according to the manufacturer’s instructions (TecoDiagnostics, Annaheim, CA, USA). Absorbance readings were recordedusing a Cecil 1010 Spectrophotometer (Cecil, Cambridge, Cambridgeshire,UK). The AST concentrations in IU/L was determined. Average absorbanceper minute was multiplied by factor 1768. The GGT activity was assayedusing a GGT kit according to the manufacturer’s instructions (Human,Wiesbaden, Germany). Concentration of GGT in IU/L was determined.Average absorbance per minute is multiplied by factor1421. The ALP activ-ity was assayed using a commercial kit according to the manufacturer’sinstructions (Teco Diagnostics). Concentration of ALP in IU/L was deter-mined. Average absorbance per minute was multiplied by factor 2187.Serum Ferritin concentration was assayed using a commercial kit (BioSystems, Barcelona, Spain). The concentration of serum ferritin in μg/Lwas determined by the following formula: concentration of serum ferritinsample (μg/L) = (A2-A1) sample/(A2-A1) standard) ∗ C where A1: firstabsorbance; A2: second absorbance; C standard: standard concentration.
The tissue thiobarbituric acid-reactive substances (TBARS) were mea-sured according to the method of Ohkawa et al. (12). Briefly, 0.5 mL ofserum was mixed with 0.5 mL of distilled water to bring the volume up to1 mL, and an equal volume of 20% trichloroacetic acid (TCA) was addedand incubated at 37◦C for 20 min. and then centrifuged at 1,000 rpm. To1 mL of TCA extract (the supernatant), 0.25 mL of 0.8% thiobarbituric acid(TBA) was added and heated in a water bath at 95◦C for 1 hour until a faint
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

70 M.Y. Abdalla et al.
pink color appeared. After cooling, the color was extracted in 1 mL butanoland the absorbance was read at 532 nm. 1,1,3,3 Tetraethoxypropane (0–15μmol/mL) was used as external standard.
Superoxide dismutase was assayed using a commercial kit (CaymanChemical Company, Ann Arbor, MI, USA). Briefly, the assay buffer, samplebuffer, radical buffer, and xanthine oxidase (XO) were prepared accordingto instructions provided by the manufacturing company. 0.01 mL of eachstandard and sample were added to the micro-titer plate. The reaction wasinitiated by adding 0.02 mL of diluted XO to all the wells, and then the platewas incubated on a shaker for 20 min. at room temperature. Absorbance at405 nm was read using a plate reader. The concentration of SOD in U/mLwas determined by using the following formula: SOD (U/mL) = [(samplelinearized rate: y intercept/slope) ∗ 0.23 mL/0.01 mL] ∗ sample dilution.
Catalase was assayed using a commercial kit (Cayman ChemicalCompany). Briefly, the assay solutions (assay buffer, sample buffer, formalde-hyde, CAT control, potassium hydroxide, H2O2, chromogen, potassiumperiodate and methanol) were prepared according to instructions providedby the manufacturing company. 0.02 mL of the standard or sample, 0.01 mLof assay buffer, 0.03 mL of methanol, and 0.02 mL of H2O2 were added tomicro-titer plate wells. All wells were covered and incubated on a shaker for20 min. at room temperature; the reaction was stopped by adding 0.03 mLpotassium hydroxide to each well, followed by 0.03 mL chromogen, cov-ering and incubating the plate on a shaker for another 10 min. at roomtemperature, then, 0.01 mL potassium periodate was added, and incu-bated for another 5 min. at room temperature. All wells are then read at405 nm using a plate reader. The concentration of CAT in nmo/min./mLwas determined according to the following formula: CAT activity = μM ofsample/20 min. ∗ Sample dilution.
Statistical Analyses
Data are presented as mean ± standard error of mean (SEM) usingSPSS version 15. The results were analyzed by analysis of variance (ANOVA)followed by the unpaired Student’s t-test. A p value of <0.05 was con-sidered significant. Correlations were calculated by Pearson’s correlationcoefficients.
RESULTS
Hemoglobin Concentrations
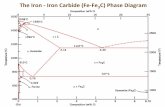
Mean Hb concentration for all β-TM patients was significantly lower(p < 0.05) compared to the controls (9.1 ± 0.9 g/dL vs. 12.0 ± 0.9 g/dL,respectively). The mean Hb concentrations was higher for females than
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

Oxidative Stress and Pediatric Thalassemia in Jordan 71
All patients
All Controls
Female Patients
Female Controls
Male Controls
Male patients
*
15
10
5
0
Hb (
g/d
l)
FIGURE 1 Significant decreased in Hb concentrations in β-TM patients compared to healthy controls.Results are expressed as mean ± SEM (n = 40). ∗p < 0.05 was considered significant.
10000
*
1000
100
10
1
Ferr
itin
µg/L
All patients
All Controls
Female Patients
Female Controls
Male Controls
Male patients
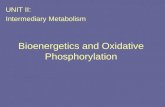
FIGURE 2 Increased serum ferritin in β-TM patients compared to healthy controls. All results shownare expressed as mean ± SEM (n = 40). ∗p < 0.05 was considered significant.
males (9.4 ± 0.8 g/dL vs. 8.7 ± 0.8 g/dL, respectively) (p >0.05). Little dif-ference in Hb concentrations was seen between healthy female and malecontrols (12.3 ± 0.9 g/dL and 11.9 ± 0.9 g/dL, respectively) (p >0.05)(Figure 1).
Serum Ferritin Levels
A significant increase in serum ferritin concentration (p <0.05) in β-TMmajor patients compared to controls (2172 ± 941 μg/L vs. 59 ± 27 μg/L,respectively). No significant difference was seen between male and femaleindividuals in patient and control groups (p >0.05) (Figure 2).
Liver Enzymes
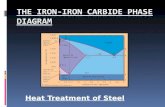
A significant increase in the liver enzymes, AST and ALT, was seen inβ-TM patients (p <0.05) compared to controls. The AST activity for β-TMpatients was 61 ± 2.7 IU/L. The mean serum AST activity for the healthyindividuals was 14 ± 2.2 IU/L (Figure 3). The ALT activity for β-TM patientswas 76 ± 3.2 IU/L, whereas the mean serum ALT activity for the healthyindividuals was 16 ± 0.8 IU/L (Figure 3). No significant different was seen in
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

72 M.Y. Abdalla et al.
All Patients
All Controls
100*
*80
60
40
20
0ALT
AST
GG
T
IU/L
FIGURE 3 Serum AST, ALT and GGT in β-TM patients and healthy controls. Results shown areexpressed as mean ± SEM (n = 40). ∗p < 0.05 was considered significant.
GGT between patients and controls (11 ± 0.6 IU/L vs.10 ± 0.5 IU/L, respec-tively) (p >0.05) (Figure 3). No significant differences were seen betweenmale and female patients and controls (data not shown) (p >0.05). Therewas a positive correlation between serum ALT (p = 0.035, r = 0.334) andAST (p = 0.042, r = 0.324) concentrations and serum ferritin levels in β-TMpatients compared to controls.
Alkaline Phosphatase Activity
The ALP reference range varies according to age subgroups. Thereforewe divided our test individuals according to age as follows: 1–3 years oldwith reference range 281 IU/L, 4–6 years old with reference range up to269 IU/L and 7–12 years old with reference range up to 300 IU/L.
For the 1–3 year old group, the β-TM patients mean ALP activity was326 ± 145.7 IU/L (n = 5), while for the healthy individuals it was 196 ±87.6 IU/L (p < 0.05). For the 4–6 year old group, the β-TM patients meanALP activity was 253 ± 84 IU/L (n = 9), while for the healthy individualsit was 196 ± 65 IU/L (p <0.05). For the 7–12 year old group, the β-TMpatients mean ALP activity was 287 ± 56 IU/L (n = 26). The mean serumALP activity for the healthy individuals was 196 ± 38 IU/L (p <0.05). A sig-nificant increase in ALP was found when the mean concentration of ALP ofall patients was compared to that of healthy controls (p <0.05) (Figure 4).
Lipid Peroxidation Measurements
Malondialdehyde is formed as an end product of lipid peroxidationwhich reacts with TBA reagent under acidic conditions to generate a pinkcolored product. When the TBARS levels were measured for β-TM patientsand controls, there was a significant increase in the TBARS in β-TM patients(3.8 ± 0. 15 IU/L vs. 1.6 ± 0.04 IU/L) (p <0.05) (Figure 5). There wereno significant differences between male and female levels in both controls
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

Oxidative Stress and Pediatric Thalassemia in Jordan 73
400
*
300
200
100
0
ALP
(IU
/L) All patients
All controls
FIGURE 4 Serum ALP in β-TM patients and healthy controls. Results shown are expressed as mean ±SEM (n = 40). ∗p < 0.05 was considered significant.
0
1
2
3
4All patients
All Controls
*
µM T
BA
RS
FIGURE 5 Increased lipid peroxidation in thalassemic patients. Serum TBARS in β-TM patients andhealthy controls. Results shown are expressed as mean ± SEM (n = 40). ∗p < 0.05 was consideredsignificant.
and β-TM patients (p >0.05) (data not shown). A positive correlation (p =0.044; r = 0.321) was found between TBARS generation and serum ferritinlevel in thalassemic patients compared to controls. However serum TBARSand ALT, AST levels in β-TM showed no significant correlation (p = 0.48,r = 0.088 and p = 0.59, r = 0.12, respectively).
Superoxide Dismutase and Catalase Activity
When SOD activity was measured in β-TM patients and controls, therewas a significant increase in SOD activity in β-TM patients (210 ± 6.3 U/mLvs. 70 ± 3.1 U/mL) (p <0.05) (Figure 6). No significant differences werefound between male and female patients and controls (data not shown)(p >0.05). The opposite picture was seen for CAT activity. A significantdecrease in CAT activity was seen in β-TM patients when compared to con-trols (12.6 ± 3.1 nmol/min./mL vs. 59 ± 2.7 nmol/min./mL) (p <0.05)(Figure 6). There was no significant difference between male and female lev-els in both controls and β-TM patients (p >0.05) (data not shown). Therewas a statistically significant positive correlation between serum SOD andserum ferritin level in β-TM patients compared to controls (p = 0.046,
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

74 M.Y. Abdalla et al.
All Patients
All Controls
250
200
150
100
50
0
SOD
CAT
*
*
IU/L
FIGURE 6 Serum SOD and CAT activity in β-TM patients and healthy controls. Results shown areexpressed as mean ± SD (n = 40). ∗p < 0.05 was considered significant.
r = 0.32). In addition, a significant negative correlation between CATgeneration and serum ferritin levels (p = 0.048, r = −0.31) was noted.
DISCUSSION
β-Thalassemias result from a number of underlying genetic defects thatinterfere with the synthesis of normal β chain (13). This results in a num-ber of cellular defects that increase susceptibility to both endogenous andexogenous oxidants (14,15). The red blood cell (RBC) is unique amongcells in that it contains very large concentrations of both iron (i.e., Hb)and oxygen. To prevent any complications of this dangerous combination,RBCs are normally protected by a number of endogenous antioxidants suchas SOD, GSH, CAT, GSH/Gpx and membrane bound α-tocopherol (16–19).The Hb findings in β-TM and their control groups are shown in Figure 1. Allβ-TM patients’ Hb concentrations were significantly decreased compared tohealthy controls (p <0.05). This is expected in thalassemic patients, wherenormal Hb synthesis is impaired.
One complication of β-thal is iron overload (20,21). The serum ferritinof β-TM and the control groups are shown in Figure 2. All β-thal patients hadsignificant increases in serum ferritin levels compared to the healthy indi-viduals group (p <0.05). Ferritinemia was 37-fold more in β-TM patientscompared to controls. This increase in serum ferritin indicates an existingiron overload in β-TM patients, probably due to multiple blood transfu-sions. It is estimated that with regular blood transfusion therapy, 0.32–0.64mg/kg/day of iron is added to the body (20,21). Intestinal hyperabsorptionin transfused patients makes the condition even worse (20,21). It was foundthat iron overload is the major cause of long-term complications of β-thal,including cardiac dysfunction, liver impairment, and endocrine dysfunction(20–22). The complications of iron overload, together with complica-tions of the anemia, ineffective erythropoiesis and chelation therapy, are
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

Oxidative Stress and Pediatric Thalassemia in Jordan 75
major causes of morbidity and mortality in the transfusion-dependent β-thal patients (22). Indeed, iron intoxication can also lead to endocrinalcomplications such as hypogonadotrophin and hypoparathyroid (23,24).
Liver iron concentration exceeding the critical level may cause hep-atic iron accumulation. This may cause an increase in hepatocellular injuryand leakage of aminotransferase enzymes and ferritin to the plasma (5,25).Therefore, we assessed the extent of hepatocellular injury by determiningthe aminotransferases serum activity, which is mainly caused by leakage ofthe enzymes from cytoplasmic and mitochondrial compartments of injuredhepatocytes to the plasma (26,27). The basic biochemical parameters of β-TM patients and the normal group are shown in Figures 3 and 4. Serumlevels of AST, ALT, ALP but not GGT were significantly increased in β-TMpatients as compared to controls (p <0.05). Similar results were reported byLivrea et al. (28).
Elevated levels of AST do not necessarily reflect a medical problem.The elevation in AST levels could result from strenuous physical exerciseor other factors (29). In our study, we believe that the elevation in ASTactivity may be due to the iron overload seen in these patients. On the otherhand, ALT is highly specific for hepatocellular damage, and its elevationcould be due to liver damage secondary to iron overload (29). Our result isconsistent with what has been found in different studies, where thalassemicpatients showed increased liver enzymes (30–32). In our study, there wasno significant increase in GGT activity (p >0.05). The GGT enzymatic activ-ity is usually not tested alone; it may be tested in combination with ALP, todetermine the kind of liver disease, whether it is of a biliary tract or boneorigin. Our finding that ALP is high in thalassemic children could be dueto higher physiological levels of ALP in normal children. It was reportedthat the increase in ALP activity in both normal and thalassemic childrenis mainly because all children have higher levels of ALP for their boneformation (33).
Iron may play a catalytic role in the initiation of free radical reactions,presumably through iron-initiated Fenton chemistry (34,35). The resultingROS have the potential to damage cellular lipids, nucleic acids, proteins andcarbohydrates. In animal models, high liver iron levels induce the elevationof lipid peroxides and oxidants (25,35). Increased lipid peroxidation mark-ers have previously been observed in thalassemia patients (36,37). Diricanet al. (38), reported that thalassemic RBCs were more susceptible than nor-mal cells to auto-oxidation. Plasma TBARS were studied as a marker oftissue injury and oxidative stress. Thiobarbituric acid reactive substancesare well-recognized biomarker of lipid peroxidation (39,40). The serumTBARS findings in β-TM patients and their control groups are shown inFigure 5. As shown, serum levels of TBARS were significantly increasedin β-TM as compared to controls (p <0.05). Our result is consistent withwhat has been found in different studies, where thalassemic patients show
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

76 M.Y. Abdalla et al.
increased TBARS (40–43). Regular blood transfusions and secondary ironoverload make thalassemic erythrocytes prone to peroxidative injury (43).Our study shows that oxidative alterations to cell components can be shownin serum as a marked increase of MDA, reflected by increase of TBARS inplasma.
Since its clear from our data and other data that β-thal induces oxida-tive stress, the study of antioxidant enzymes could be very informative.Antioxidants in blood such as SOD and CAT significantly contribute tothe total plasma antioxidant capacity (44), and are the first line of defenseagainst oxidative stress (45). Superoxide dismutase catalyzes conversion ofsuperoxide anion to H2O2 (46). As expected, our results show that serumlevels of SOD were significantly increased in β-TM as compared to con-trols (p <0.05). This increase in SOD may be a compensatory mechanismto scavenge excess superoxide anion which resulted from oxidative stress(17,44). It has been reported by Meral et al. (7) that SOD levels of β-TMpatients were elevated when compared to controls (45). On the other hand,when we studied CAT enzyme activity in both β-TM patients and controls,the enzyme activity was significantly decreased in β-TM patients as com-pared to controls (p <0.05). In fact, the loss of CAT activity impairs cellularprotection against the endogenously generated H2O2, and increases ironmediated injury to the thalassemic erythrocyte membranes (47). The mech-anism(s) underlying the decreased CAT activity was proposed by differentinvestigators who suggested that nicotinamide adenine dinucleotide phos-phatase (NADPH) is important in maintaining CAT activity, and that theloss of NADPH would adversely affect erythrocyte enzyme activity (46–49).Catalase monomer contains a high affinity binding site for NADPH, whichis crucial for the maintenance of CAT activity (49–51). β-Thalassemia majorpatients have demonstrated a significant decrease in NADPH (52,53). Theloss of NADPH is most likely mediated by the release of heme and ironand a subsequent inhibition of other metabolic enzymes (54,55). This mightexplain our findings.
Our study suggests that in β-thal, the first target organ dysfunction is theliver, enhanced by an iron overload leading to a status of oxidative stress andinitiates free radical reactions. Proper iron chelation and administrationof adequate antioxidants may represent a promising way of counteractingoxidative stress and its deleterious effect on the prognosis of the disease.
ACKNOWLEDGMENTS
This study was supported by a grant from The Deanship of Research andGraduate Studies, The Hashemite University, Zarqa, Jordan.
Declaration of Interest: The authors report no conflicts of interest. Theauthors alone are responsible for the content and writing of this article.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

Oxidative Stress and Pediatric Thalassemia in Jordan 77
REFERENCES
1. Manca L, Masala B. Disorders of the synthesis of human fetal hemoglobin. IUBMB Life.2008;60(2):94–111.
2. Clegg JB, Weatherall DJ. Thalassemia and malaria: new insights into an old problem. Proc AssocAm Phys.1999;111(4):278–282.
3. Sutcharitchan P, Saiki R, Huisman THJ, et al. Reverse dot-blot detection of the African-Americanβ-thalassemia mutations. Blood. 1995;86(4):1580–1585.
4. Hilliard LM, Berkow RL. The thalassemia syndromes. Primary Care Update for OB/GYNS.1996;3(5):157–162 (http://www.sciencedirect.com/science/article/B6TMB-3W3NBGY-2/2/b6ae9d3dcab796ef4e002acc7bab99b6).
5. Mehrvar A, Azarkeivan A, Faranoush M, et al. Endocrinopathies in patients with transfusion-dependent β-thalassemia. Pediatr Hematol Oncol. 2008;25(3):187–194.
6. Scott MD. H2O2 injury in β thalassemic erythrocytes: protective role of catalase and the prooxidanteffects of GSH. Free Radic Biol Med. 2006;40(7):1264–1272.
7. Meral A, Tuncel P, Sürmen-Gür E, Ozbek R, Oztürk E. Lipid peroxidation and antioxidant status inβ-thalassemia. Pediatr Hematol Oncol. 2000;17(8):687–693.
8. Advani R, Rubin E, Mohandas N, Schrier S. Oxidative red blood cell membrane injury in thepathophysiology of severe mouse β-thalassemia. Blood. 1992;79(4):1064–1067.
9. Olivieri O, De Franceschi L, Capellini MD, Girelli D, Corrocher R, Brugnara C. Oxidative damageand erythrocyte membrane transport abnormalities in thalassemias. Blood. 1994;84(1):315–320.
10. Grinberg LN, Rachmilewitz EA, Kitrossky N, Chevion M. Hydroxyl radical generation inβ-thalassemic red blood cells. Free Radic Biol Med. 1995;18(3):611–615.
11. Schrier SL, Centis F, Verneris M, Ma L, Angelucci E. The role of oxidant injury in the pathophysi-ology of human thalassemias. Redox Rep. 2003;8(5):241–245.
12. Ohkawa H, Ohishi N, Yagi K. Assay for lipid peroxides in animal tissues by thiobarbituric acidreaction. Anal Biochem. 1979;95(2):351–358.
13. Setianingsih I, Williamson R, Marzuk S, Harahap A, Tamam M, Forrest S. Molecular basis ofβ-thalassemia in indonesia: application to prenatal diagnosis. Molec Diagn. 1998;3(1):11–20.
14. Scott MD, Eaton JW. Thalassaemic erythrocytes: cellular suicide arising from iron and glutathione-dependent oxidation reactions? Br J Haematol. 1995;91(4):811–819.
15. Chan AC, Chow CK, Chiu D. Interaction of antioxidants and their implication in genetic anemia.Proc Soc Exp Biol Med.1999;222(3):274–282.
16. Watkins JA, Kawanishi S, Caughey WS. Autoxidation reactions of Hemoglobin A free from other redcell components: a minimal mechanism. Biochem Biophys Res Commun. 1985;132(2):742–748.
17. Das SK, Nair RC. Superoxide dismutase, glutathione peroxidase, catalase and lipid peroxidation ofnormal and sickled erythrocytes. Br J Haematol. 1980;44(1):87–92.
18. Gaston BM. Nitric oxide and radicals in the pulmonary vasculature. Pediatr Pulmonol1998;25(5):353–354.
19. Geetha RK, Vasudevan DM. Inhibition of lipid peroxidation by botanical extracts of Ocimumsanctum: in vivo and in vitro studies. Life Sci. 2004; 76(1):21–28.
20. Kassab-Chekir A, Laradi S, Ferchichi S, et al. Oxidant, antioxidant status and metabolic data inpatients with β-thalassemia. Clin Chim Acta. 2003;338(1-2):79–86.
21. Borgna-Pignatti C, Rugolotto S, De Stefano P, et al. Survival and disease complications inthalassemia major. Ann NY Acad Sci. 1998;850:227–231.
22. Weatherall DJ, Clegg JB. Thalassemia - a global public health problem. Nat Med. 1996;2(8):847–849.23. Halle M, König D, Berg A, Keul J, Baumstark MW. Relationship of serum ferritin concentrations
with metabolic cardiovascular risk factors in men without evidence for coronary artery disease.Atherosclerosis. 1997;128(2):235–240.
24. Canale VC, Steinherz P, New M, Erlandson M. Endocrine function in thalassemia major. Ann NYAcad Sci. 1974;232:333–345.
25. Knutson MD, Walter PB, Ames BN, Viteri FE. Both iron deficiency and daily iron supplementsincrease lipid peroxidation in rats. J Nutr. 2000;130(3):621–628.
26. Poli G. Pathogenesis of liver fibrosis: role of oxidative stress. Molec Aspects Med. 2000;21(3):49–98.27. Boyd JW. The intracellular distribution, latency and electrophoretic mobility of l-glutamate-
oxaloacetate transaminase from rat liver. Biochem J. 1961;81(2):434–441.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

78 M.Y. Abdalla et al.
28. Livrea M, Tesoriere L, Pintaudi A, et al. A. Oxidative stress and antioxidant status in β-thalassemiamajor: iron overload and depletion of lipid-soluble antioxidants. Blood 1996; 88(9):3608–3614.
29. Panigrahi I, Agarwal S. Thromboembolic complications in β-thalassemia: beyond the horizon.Thromb Res. 2007;120(6):783–789.
30. Muretto P, Angelucci E, Lucarelli G. Reversibility of cirrhosis in patients cured of thalassemia bybone marrow transplantation. Ann Intern Med. 2002;136(9):667–672.
31. Prati D, Maggioni M, Milani S, et al. Clinical and histological characterization of liver dis-ease in patients with transfusion-dependent β-thalassemia. A multicenter study of 117 cases.Haematologica. 2004;89(10):1179–1186.
32. Sanyal AJ, American Gastroenterological Association. AGA technical review on nonalcoholic fattyliver disease. Gastroenterology. 2002;123(5):1705–1725.
33. De Gobbi M, Pasquero P, Brunello F, Paccotti P, Mazza U, Camaschella C. Juvenile hemochromato-sis associated with β-thalassemia treated by phlebotomy and recombinant human erythropoietin.Haematologica. 2000;85(8):865–867.
34. Zhihua Z, Goldstein BD, Witz G. Iron-stimulated ring-opening of benzene in a mouse livermicrosomal system: mechanistic studies and formation of a new metabolite. Biochem Pharmacol.1995;50(10):1607–1617.
35. Ryan TP, Aust SD. The role of iron in oxygen-mediated toxicities. Crit Rev Toxicol.1992;22(2):119–141.
36. Selek S, Aslan M, Horoz M, Gur M, Erel O. Oxidative status and serum PON1 activity inβ-thalassemia minor. Clin Biochem. 2007;40(5-6):287–291.
37. Ludwiczek S, Aigner E, Theurl I, Weiss G. Cytokine-mediated regulation of iron transport in humanmonocytic cells. Blood. 2003;101(10):4148–4154.
38. Dirican M, Safak Ö, Uncu G, Sarandöl E. Susceptibility of red blood cell lipids to in vitro oxidationand antioxidant status in preeclampsia. Eur J Obstet Gynecol Reprod Biol. 2008;140(2):158–164.
39. Nielsen F, Mikkelsen BB, Nielsen JB, Andersen HR, Grandjean P. Plasma malondialdehyde asbiomarker for oxidative stress: reference interval and effects of life-style factors. Clin Chem.1997;43(7):1209–1214.
40. Grotto D, Santa Maria LD, Boeira S, et al. Rapid quantification of malondialdehyde inplasma by high performance liquid chromatography-visible detection. J Pharm Biomed Anal.2007;43(2):619–624.
41. Dorléac E, Morlé L, Gentilhomme O, Jaccoud P, Baudonnet C, Delaunay J. Thalassemia-likeabnormalities of the red cell membrane in Hemoglobin E trait and disease. Am J Hematol.1984;16(3):207–217.
42. Cighetti G, Duca L, Bortone L, et al. Oxidative status and malondialdehyde in β-thalassaemiapatients. Eur J Clin Invest. 2002;32(Suppl. 1):55–60.
43. Naithani R, Chandra J, Narayan S, Sharma S, Singh V. Thalassemia major – on the verge of bleedingor thrombosis? Hematology. 2006;11(1):57–61.
44. Miller NJ, Rice-Evans C, Davies MJ, Gopinathan V, Milner A. A novel method for measuring antiox-idant capacity and its application to monitoring the antioxidant status in premature neonates. ClinSci. 1993;84(4):407–412.
45. Naithani R, Chandra J, Bhattacharjee J, Verma P, Narayan S. Peroxidative stress and antioxidantenzymes in children with β-thalassemia major. Pediatr Blood Cancer. 2006;46(7):780–785.
46. Moreno-Manzano V, Ishikawa Y, Lucio-Cazana J, Kitamura M. Selective involvement of superoxideanion, but not downstream compounds hydrogen peroxide and peroxynitrite, in tumor necrosisfactor-α-induced apoptosis of rat mesangial cells. J Biol Chem. 2000;275(17):12684–12691.
47. Çimen MY. Free radical metabolism in human erythrocytes. Clin Chim Acta. 2008;390(1–2):1–11.48. Jaffe E. Clinical profile: hereditary hemolytic disorders and enzymatic deficiencies of human
erythrocytes. Blood. 1970;35(1):116–134.49. Vetrano AM, Heck DE, Mariano TM, Mishin V, Laskin DL, Laskin JD. Characterization of the
oxidase activity in mammalian catalase. J Biol Chem. 2005;280(42):35372–35381.50. Gibbons NCJ, Wood JM, Rokos H, Schallreuter KU. Computer simulation of native epidermal
enzyme structures in the presence and absence of hydrogen peroxide (H2O2): potential andpitfalls. J Invest Dermatol. 2006;126(12):2576–2582.
51. Churbanova IY, Sevrioukova IF. Redox-dependent changes in molecular properties of mitochon-drial apoptosis-inducing factor. J Biol Chem. 2008;283(9):5622–5631.
52. Walter PB, Fung EB, Killilea DW, et al. Oxidative stress and inflammation in iron-overloaded
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.

Oxidative Stress and Pediatric Thalassemia in Jordan 79
patients with β-thalassaemia or sickle cell disease. Br J Haematol. 2006;135(2):254–263.53. Cheng ML, Ho HY, Tseng HC, Lee CH, Shih LY, Chiu DT. Antioxidant deficit and enhanced sus-
ceptibility to oxidative damage in individuals with different forms of α-thalassaemia. Br J Haematol.2005;128(1):119–127.
54. Marín J, Rodríguez-Martínez MA. Nitric oxide, oxygen-derived free radicals and vascular endothe-lium. J Auton Pharmacol. 1995;15(4):279–307.
55. Cappellini MD, Tavazzi D, Duca L, et al. Metabolic indicators of oxidative stress correlatewith haemichrome attachment to membrane, band 3 aggregation and erythrophagocytosis inβ-thalassaemia intermedia. Br J Haematol. 1999;104(3):504–512.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dig
estiv
e D
isea
ses
Bra
nch
on 0
1/20
/11
For
pers
onal
use
onl
y.