Ocular Tension in the Trendelenburg Position* *From the Ophthalmology Service, Montefiore Hospital,...
4
Click here to load reader
Transcript of Ocular Tension in the Trendelenburg Position* *From the Ophthalmology Service, Montefiore Hospital,...

1040 BERNARD S L A T T
2. McAuley, F. D.: Progressive external ophthalmoplegia. Brit. J . Ophth., 40:686, 1956. 3. Nicolaissen, B., and Brodal, Α.: Chronic progressive external ophthalmoplegia. Arch. Ophth., 6 1 :
209, 1959. 4. Helfand, M.: Congenital familial external ophthalmoplegia without ptosis. Arch. Ophth., 21:823, 1939. 5. Li, Τ. M.: Congenital total bilateral ophthalmoplegia. Am. J . Ophth., 28:69, 1911. 6. Jonkers, G. H.: Familial ptosis congenita with other congenital defects of the ocular musculature.
Ophthalmologica, 120:372, 1950. 7. Chavasse, B.: The ocular palsies. Trans. Ophth. Soc. U. Kingdom, 58:483, 1938. 8. Bielschowsky, Α.: Cited by Duke-Elder, S.: Systems of Ophthalmology. St. Louis, Mosby, 1963, v.
3, p. 989. 9. Breinin, G. M.: Electromyography: A tool in ocular and neurologic diagnosis. Arch. Ophth., 57:
165-175,1957. 10. Davidson, S. I.: Abiotrophie ophthalmoplegia externa. Brit. J . Ophth., 44:590, 1960. 11. Kiloh, L. G., and Nevin, S.: Progressive dystrophy of the external ocular muscles (ocular myo
pathy). Brain, 74:115-143, 1951.
O C U L A R T E N S I O N I N T H E T R E N D E L E N B U R G P O S I T I O N *
SAMUEL GARTNER, M.D. , A N D WILLTAM BECK, M . D .
Bronx, New York
Intraocular pressure rises up to 3 .0 or 4 .0 mm Hg in the normal person in the supine position as compared to the tension when erect (Thibert, 1 Bailliart and La vat 2 and Wegner 3 ) . This has been confirmed recently by a number of reports. 4 - 7 In our study, intraocular pressure was measured in a reclining chair with the head six inches above the level of the feet, and then in the Trendelenburg position with the body inclined head down eight inches below the feet, a change of 1 4 inches. Intraocular pressure was taken at intervals of one, two and three minutes. Significant increases in tension were found in glaucoma patients but not in normal cases (table 1 ) .
Normal patients, aged 2 0 to 8 5 years, selected at random, were examined. Of 3 4 eyes, the average change of intraocular pressure was an increase of 0 . 4 2 mm Hg in the Trendelenburg position. The range of change in 3 3 eyes varied from — 3 . 9 mm to + 2 . 0 mm Hg. One patient had a rise of 9 . 8 mm Hg and was, therefore, considered to be a glaucoma suspect. Following the Trendelenburg test, a water provocative test was negative. However, tonography revealed impaired outflows ( C = 0 . 1 3 both eyes) .
* From the Ophthalmology Service, Montefiore Hospital, New York.
A second group of patients were glaucoma suspects. They had borderline elevations of intraocular pressures with normal outflows shown by tonography and negative provocative tests. In 2 4 eyes, when tested in the Trendelenburg position, the range of change was from — 9 . 8 to + 7 . 1 mm Hg. The average change was a decrease of 0 . 5 5 mm Hg with a maximum increase of 3 .3 mm Hg except in one eye which had an increase of 7 .1 mm Hg. This patient, a glaucoma suspect, had borderline tensions, a negative water provocative test and negative dark-room and mydriasis tests. Gonioscopy revealed narrow angles. Following the elevated intraocular pressure reading with the three-minute Trendelenburg test, tonography was performed. The outflows were 0 . 2 0 in the right eye and 0 . 1 5 in the left. The right eye had a negative Trendelenburg test but the left eye had a rise of 7 .1 mm Hg.
Thirty-nine glaucoma patients, varying in type from chronic narrow-angle glaucoma to chronic wide-angle glaucoma, well controlled at the time of this test by medical or surgical means, were examined in the Trendelenburg position. Thirty-nine eyes were studied and the average change was an increase of 2 . 7 4 mm Hg. The range varied from — 6 . 0 to + 1 5 . 7 mm Hg. Eleven of these 3 9 had

OCULAR TENSION IN THE TRENDELENBURG POSITION 1041
T A B L E 1
ANALYSIS OF OCULAR TENSION IN TRENDELENBURG POSITION
Normal Glaucoma Suspects
Glaucoma Patients
Controlled
Glaucoma Patients Off Medication
No. of eyes 34 24 39 23 Average change (mm Hg) + 0 . 4 2 - 0 . 5 S + 2 . 7 4 + 5 . 2 9 Range of change (mm Hg) - 3 . 9 to + 9 . 8 - 9 . 8 to + 7 . 1 - 6 . 0 to + 1 S . 7 - 2 . 2 to + 1 2 . 7 Cases with rise over 4.0 mm Hg 1 1 11 13
an increase of more than 4.0 mm Hg in the Trendelenburg position.
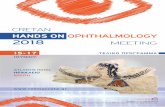
Twenty-three eyes of known glaucoma patients of various types were taken off medication, therefore, intraocular pressure at the time of the test was elevated in most of them. The rise of intraocular pressure during the three minutes in this group was considerable, averaging 5.29 mm Hg. The range extended from —2.2 to +12.7 mm Hg. Thirteen of these 23 glaucoma eyes showed a rise of over 4.0 mm Hg after three minutes in the Trendelenburg position (fig. 1 ) .
The curve (fig. 1) illustrates the rise in intraocular pressure during the three-minute Trendelenburg test of glaucoma patients off medication. The steepest rise is in the first two minutes. The treated glaucoma patients show a similar rise although of a lesser de-
TKAltíl QUWOWJl f A T f f f i n Γ,;>'τ·:ι«Α s w F T r t s
niTLU. π κ κ »
Fig. 1 (Gartner and Beck). Graph, showing range in pressure related to time in Trendelenburg position. Glaucoma patients off medication.
Treated glaucoma patients. —.·—.—.— Glaucoma suspects Normals.
gree. The steepest rise in this group is also in the first two minutes. The other two curves illustrate the insignificant changes in intraocular pressure in the normal group and in glaucoma suspects. The glaucoma suspects had a higher initial tension than the normal group.
A random group of normal patients (table 2 ) was studied to determine whether age influences the effect of position on intraocular pressure. The average change in intraocular pressure was slight, and showed a small decrease in all groups except the 50 to 60-year age group where a slight increase of 1.4 mm Hg was found. The range of change varied, with a wider range being found in the older age group. One patient in the 50 to 60-year group, one in the 60 to 70-year and one in the 70 to 85-year age group had rises over 4.0 mm Hg.
The effect of a water drinking test combined with the three-minute Trendelenburg measurement of intraocular pressure was striking (table 3 ) . Seven patients, six of whom had glaucoma, were given a 90-min-ute water provocative test. At varying inter-
TABLE 2 NORMAL PATIENTS
Age (yr) 10-50 50-60 60-70 70-85
No. of eyes 10 12 11 23 Average - 0 . 4 5 + 1 .4 - 0 . 4 8 - 0 . 3 9
change (mm Hg)
Range of - 3 . 9 - 2 . 7 - 5 . 1 - 9 . 8 change to to to to (mm Hg) + 3 . 3 + 9 . 8 + 7.2 + 7.1
Cases with 0 1 1 1 rise over 4.0 mmHg

1042 S A M U E L G A R T N E R A N D W I L L I A M B E C K
T A B L E 3
COMBINED WATER DRINKING AND TRENDELENBURG TESTS
Patient Diagnosis Eye Initial Tension
90 Min. Water
3 Min. Test in Trendelenburg during Water Test Initial
Tension Test 30 Min. 60 Min. 90 Min.
AF Wide-angle glaucoma OD OS
24 .4 20 .6
0 + 3 . 8
+ 4 . 6 + 7 . 2
+ 10 .1 + 10 .1 —
GS Wide-angle glaucoma OD OS
20 .6 24 .4
+ 6 . 6 0
0 0
+ 7 .1 0
—
FC Narrow-angle glaucoma OD OS
26 .6 26 .6
+ 9 . 2 + 3 . 8
— + 6.3 + 8 .5
AV Glaucoma suspect OD OS
20 .6 2 0 . 6
+ 1 .8 + 1 .8
+ 4 . 2 + 9 . 2
0 + 4 .2 —
SE Glaucoma suspect OD OS
20 .6 1 7 . 3
+ 6 . 0 + 5 . 1 —
— + 1 1 . 7 + 1 1 . 7
HG Glaucoma suspect OD OS
22 .4 22 .4
0 0 —
+ 3 . 8 + 8 .4 —
AS Normal OD OS
24 .4 24 .4
0 0
+ 3 .3 0 —
vals after the water drinking the three-minute Trendelenburg test was performed.
Only one eye showed a rise over 8.0 mm Hg during the 90-minute water provocative test. Yet the Trendelenburg test superimposed on the water drinking test, revealed seven eyes with a rise of over 8.0 mm Hg. The one normal patient in this series had a negative water provocative test, as well as an unremarkable rise in the Trendelenburg position. Four patients were glaucoma suspects with negative water provocative tests and normal tonography. They showed a positive test to the combined water drinking and Trendelenburg studies. Further studies, including fields, confirmed the diagnosis of chronic simple glaucoma which might have been missed otherwise. Tonometry in the Trendelenburg position combined with a water drinking test increases its sensitivity and reliability.
DISCUSSION
Intraocular pressure depends on a number of factors. The secretion and outflow of aqueous is, of course, basic and osmotic changes in the blood and ocular fluids have
their effects. Significant is the influence of the vascular system. Changes in blood pressure and blood volume affect intraocular pressure. In death, tension falls rapidly as blood flow and blood pressure drop. Arterial constriction by retrobulbar injection of adrenalin causes a prompt fall in tension.
Studies of retinal artery pressure by ophthalmodynamometry show a rise in intraocular pressure as the patient changes from the erect to the supine position.8
There is a similar rise in intraocular pressure with change from the erect to the supine position. The rise probably is secondary to the rise in intraocular blood pressure, possibly due in part to a rise in episcleral venous pressure and to changes in blood volume in the eye.
By performing tonometry in the erect and then in the Trendelenburg position at intervals of one, two, and three minutes, the rise in arterial and venous pressure and blood volume in the eye adds a burden to the mechanism regulating ocular tension. Normal patients, regardless of age, will compensate with little or no rise in intraocular pressure; however, most glaucomatous eyes

OCULAR TENSION IN THE TRENDELENBURG POSITION 1 0 4 3
will show a definite rise, which varies with the control of the glaucoma. Patients off medication or poorly controlled by medical or surgical means will show an abrupt and sustained rise in intraocular pressure during the three-minute Trendelenburg test. The defect in homeostatic control is increased when the water-drinking test is combined with the Trendelenburg test.
Four patients with borderline intraocular pressure, negative water provocative tests and negative tonography showed a marked rise in ocular tension when placed in the Trendelenburg position during the water-drinking test. The diagnosis of chronic simple glaucoma was confirmed in these patients by field studies and the findings of high ocular tensions at subsequent examinations.
The increase in intraocular pressure is most rapid during the first two minutes after the patient lies down. Unless this is considered in the evaluation of a patient, errors can result, for the tension readings may vary appreciably, depending on how long the patient was lying down before the tension was taken.
Varying the angle of inclination at
different examinations can introduce a further error. The angle at which a patient is resting when he lies down for tonometry often depends on the equipment used and the habits of the examiner. Some patients are placed flat, while others are examined with the head appreciably higher than the feet.
S U M M A R Y
Intraocular pressure is increased by a change from the erect to the supine position and further increased by lowering the patient to the Trendelenburg position. This increase is decidedly higher in many glaucoma patients due to a defect in the homeostatic control of intraocular pressure.
Combining examination in the Trendelenburg position with the water-drinking test exaggerates the increase in tension in many glaucoma patients. This can serve as a useful test for glaucoma.
Intraocular pressure varies with the position of the body and the length of time a patient lies down. These factors need to be carefully controlled if tonometry readings are to be properly evaluated.
1749 Grand Concourse (53).
REFERENCES
1. Thibert, M.: Influence du decubitus sur l'ophtalmotonus chez les glaucomateux. Bull. Soc. beige. Ophtal, 45 : 3 6 , 1 9 2 2 .
2 . Bailliart, M. M , and Lavat: Resultats comparis de la tonométrie en positions assise et couchée. Bull. Soc. Ophtal. Paris, 3 6 : 3 6 4 , 1 9 2 4 .
3 . Wegner, W . : Massagewirkung und Stauungsversuche am normalen und glaukomatösen Auge. Ztschr. Augenh, 55 : 3 8 1 , 1 9 2 5 .
4 . Strobl, G., and Follman, P . : Intraocular pressure, body position and determination of rigidity. Ophthalmologica, 1 4 4 : 5 7 , 1 9 6 2 .
5 . Armaly, M. F., and Salamon, S. S . : Schiøtz and applanation tonometry. Arch. Ophth., 7 0 : 6 0 3 , 1 9 6 3 . 6 . Galin, Μ. Α., Mclvor, J . W , and Magruder, G. B.: Influence of position on intraocular pressure.
Am. J . Ophth, 5 5 : 7 2 0 , 1 9 6 3 . 7 . Roberts, W , and Rogers, J . W . : Postural effects on pressure and ocular rigidity measurements.
Am. J . Ophth, 5 7 : 1 1 1 , 1 9 6 4 . 8. Cambiaggi, A , and Pastine, G.: Comportomento della pressione erteriosa retinica di soggetti normali
in seguito a variazioni di posizione del corpo. Riv. oto-neuro-oftal, 3 7 : 5 1 4 , 1 9 6 2 .