Mysteries of 1-antitrypsin deficiency: emerging therapeutic strategies for a challenging disease
9
© 2014. Published by The Company of Biologists Ltd | Disease Models & Mechanisms (2014) 7, 411-419 doi:10.1242/dmm.014092 411 ABSTRACT The classical form of α1-antitrypsin deficiency (ATD) is an autosomal co-dominant disorder that affects ~1 in 3000 live births and is an important genetic cause of lung and liver disease. The protein affected, α1-antitrypsin (AT), is predominantly derived from the liver and has the function of inhibiting neutrophil elastase and several other destructive neutrophil proteinases. The genetic defect is a point mutation that leads to misfolding of the mutant protein, which is referred to as α1-antitrypsin Z (ATZ). Because of its misfolding, ATZ is unable to efficiently traverse the secretory pathway. Accumulation of ATZ in the endoplasmic reticulum of liver cells has a gain-of- function proteotoxic effect on the liver, resulting in fibrosis, cirrhosis and/or hepatocellular carcinoma in some individuals. Moreover, because of reduced secretion, there is a lack of anti-proteinase activity in the lung, which allows neutrophil proteases to destroy the connective tissue matrix and cause chronic obstructive pulmonary disease (COPD) by loss of function. Wide variation in the incidence and severity of liver and lung disease among individuals with ATD has made this disease one of the most challenging of the rare genetic disorders to diagnose and treat. Other than cigarette smoking, which worsens COPD in ATD, genetic and environmental modifiers that determine this phenotypic variability are unknown. A limited number of therapeutic strategies are currently available, and liver transplantation is the only treatment for severe liver disease. Although replacement therapy with purified AT corrects the loss of anti- proteinase function, COPD progresses in a substantial number of individuals with ATD and some undergo lung transplantation. Nevertheless, advances in understanding the variability in clinical phenotype and in developing novel therapeutic concepts is beginning to address the major clinical challenges of this mysterious disorder. KEY WORDS: α1-antitrypsin deficiency, Autophagy, Liver disease Introduction α1-antitrypsin deficiency (ATD) was first described 50 years ago when absence of the α1-globulin fraction was noticed in the serum specimens of individuals with chronic obstructive pulmonary disease (COPD; Box 1 provides a glossary of clinical terms) (Laurell and Eriksson, 1963). Later, this deficiency was found in an infant with cirrhosis (Sharp et al., 1969), establishing a link CLINICAL PUZZLE 1 Department of Pediatrics, University of Pittsburgh School of Medicine, One Children’s Hospital Drive, 4401 Penn Avenue, Pittsburgh, PA 15224, USA. 2 Children’s Hospital of Pittsburgh of UPMC, One Children’s Hospital Drive, 4401 Penn Avenue, Pittsburgh, PA 15224, USA. 3 Department of Cell Biology, University of Pittsburgh School of Medicine, 3500 Terrace Street, 5362 Biomedical Sciences Tower, Pittsburgh, PA 15261, USA. *Author for correspondence ([email protected]) This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution and reproduction in any medium provided that the original work is properly attributed. between ATD and liver disease; however, the mechanism by which ATD could lead to liver disease remained one of its most perplexing characteristics for many years and raised further questions about how the deficiency of an enzyme inhibitor could cause different diseases in two organ systems. Several breakthroughs led to the recognition that lung disease is caused predominantly by a loss-of-function mechanism whereas liver disease involves a gain-of-toxic-function mechanism. One of the breakthroughs was the realization that the major function of α1- antitrypsin (AT) is inhibition of neutrophil elastase and, when circulating levels of AT are reduced, this serine proteinase can destroy the connective tissue matrix of the lung, causing emphysema (Silverman and Sandhaus, 2009). This conceptual advance led to the protease-antiprotease imbalance paradigm that constitutes the molecular basis for COPD; i.e. excess protease and/or deficiency of antiprotease predisposes individuals to this disease. Another series of discoveries led to the recognition that ATD is characterized by a point mutation that renders AT, a hepatic secretory glycoprotein, prone to misfolding and accumulation in the early portions of the secretory pathway, specifically the endoplasmic reticulum (ER) of liver cells (reviewed in Perlmutter, 2011). Studies in transgenic mice have provided evidence that intracellular accumulation of the mutant misfolded protein, named α1-antitrypsin Z (ATZ), is proteotoxic. In the liver, the primary site of AT synthesis, ATZ accumulation causes liver fibrosis and carcinogenesis by a gain-of-function mechanism (Hidvegi et al., 2010). Together, these breakthroughs have shown that loss of antiprotease function is the dominant mechanism for lung disease and accumulation (proteotoxicity) of ATZ in hepatocytes is the primary mechanism for liver disease (Fig. 1). Another perplexing aspect of ATD that has emerged over the years is the marked variation in clinical severity of lung and liver disease among affected homozygotes. The classical form of ATD is an autosomal co-dominant disorder that affects 1 in 3000 live births in many populations; however, a significant number of homozygotes escape both liver and lung disease. There is also a marked variation in the age of onset and severity of lung disease (Silverman and Sandhaus, 2009). We now know that one environmental modifier, cigarette smoking, markedly increases the severity of lung disease and that other genetic and environmental modifiers are also involved. Analysis of a unique cohort of homozygotes identified by an unbiased newborn screening study carried out in Sweden has shown that only ~8% of homozygotes develop clinically significant liver disease in the first 4 decades of life (Piitulainen et al., 2005; Sveger, 1976), indicating that genetic and/or environmental modifiers play a major role in whether a homozygote falls into the subpopulation that is susceptible to liver disease or is somehow protected from liver disease. This variation in clinical phenotype has added to the challenge of detection and diagnosis of ATD and means that therapeutic strategies have to be tested in and designed for Mysteries of α1-antitrypsin deficiency: emerging therapeutic strategies for a challenging disease Raafe Ghouse 1,2 , Andrew Chu 1,2 , Yan Wang 1,2 and David H. Perlmutter 1,2,3, * Disease Models & Mechanisms
Transcript of Mysteries of 1-antitrypsin deficiency: emerging therapeutic strategies for a challenging disease

© 2014. Published by The Company of Biologists Ltd | Disease Models & Mechanisms (2014) 7, 411-419 doi:10.1242/dmm.014092
411
ABSTRACTThe classical form of α1-antitrypsin deficiency (ATD) is an autosomalco-dominant disorder that affects ~1 in 3000 live births and is animportant genetic cause of lung and liver disease. The proteinaffected, α1-antitrypsin (AT), is predominantly derived from the liverand has the function of inhibiting neutrophil elastase and severalother destructive neutrophil proteinases. The genetic defect is a pointmutation that leads to misfolding of the mutant protein, which isreferred to as α1-antitrypsin Z (ATZ). Because of its misfolding, ATZis unable to efficiently traverse the secretory pathway. Accumulationof ATZ in the endoplasmic reticulum of liver cells has a gain-of-function proteotoxic effect on the liver, resulting in fibrosis, cirrhosisand/or hepatocellular carcinoma in some individuals. Moreover,because of reduced secretion, there is a lack of anti-proteinaseactivity in the lung, which allows neutrophil proteases to destroy theconnective tissue matrix and cause chronic obstructive pulmonarydisease (COPD) by loss of function. Wide variation in the incidenceand severity of liver and lung disease among individuals with ATDhas made this disease one of the most challenging of the rare geneticdisorders to diagnose and treat. Other than cigarette smoking, whichworsens COPD in ATD, genetic and environmental modifiers thatdetermine this phenotypic variability are unknown. A limited numberof therapeutic strategies are currently available, and livertransplantation is the only treatment for severe liver disease. Althoughreplacement therapy with purified AT corrects the loss of anti-proteinase function, COPD progresses in a substantial number ofindividuals with ATD and some undergo lung transplantation.Nevertheless, advances in understanding the variability in clinicalphenotype and in developing novel therapeutic concepts is beginningto address the major clinical challenges of this mysterious disorder.
KEY WORDS: α1-antitrypsin deficiency, Autophagy, Liver disease
Introductionα1-antitrypsin deficiency (ATD) was first described 50 years agowhen absence of the α1-globulin fraction was noticed in the serumspecimens of individuals with chronic obstructive pulmonarydisease (COPD; Box 1 provides a glossary of clinical terms)(Laurell and Eriksson, 1963). Later, this deficiency was found inan infant with cirrhosis (Sharp et al., 1969), establishing a link
CLINICAL PUZZLE
1Department of Pediatrics, University of Pittsburgh School of Medicine, OneChildren’s Hospital Drive, 4401 Penn Avenue, Pittsburgh, PA 15224, USA.2Children’s Hospital of Pittsburgh of UPMC, One Children’s Hospital Drive, 4401Penn Avenue, Pittsburgh, PA 15224, USA. 3Department of Cell Biology, Universityof Pittsburgh School of Medicine, 3500 Terrace Street, 5362 Biomedical SciencesTower, Pittsburgh, PA 15261, USA.
*Author for correspondence ([email protected])
This is an Open Access article distributed under the terms of the Creative CommonsAttribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricteduse, distribution and reproduction in any medium provided that the original work is properlyattributed.
between ATD and liver disease; however, the mechanism by whichATD could lead to liver disease remained one of its mostperplexing characteristics for many years and raised furtherquestions about how the deficiency of an enzyme inhibitor couldcause different diseases in two organ systems. Severalbreakthroughs led to the recognition that lung disease is causedpredominantly by a loss-of-function mechanism whereas liverdisease involves a gain-of-toxic-function mechanism. One of thebreakthroughs was the realization that the major function of α1-antitrypsin (AT) is inhibition of neutrophil elastase and, whencirculating levels of AT are reduced, this serine proteinase candestroy the connective tissue matrix of the lung, causingemphysema (Silverman and Sandhaus, 2009). This conceptualadvance led to the protease-antiprotease imbalance paradigm thatconstitutes the molecular basis for COPD; i.e. excess proteaseand/or deficiency of antiprotease predisposes individuals to thisdisease. Another series of discoveries led to the recognition thatATD is characterized by a point mutation that renders AT, ahepatic secretory glycoprotein, prone to misfolding andaccumulation in the early portions of the secretory pathway,specifically the endoplasmic reticulum (ER) of liver cells(reviewed in Perlmutter, 2011). Studies in transgenic mice haveprovided evidence that intracellular accumulation of the mutantmisfolded protein, named α1-antitrypsin Z (ATZ), is proteotoxic.In the liver, the primary site of AT synthesis, ATZ accumulationcauses liver fibrosis and carcinogenesis by a gain-of-functionmechanism (Hidvegi et al., 2010). Together, these breakthroughshave shown that loss of antiprotease function is the dominantmechanism for lung disease and accumulation (proteotoxicity) ofATZ in hepatocytes is the primary mechanism for liver disease(Fig. 1).
Another perplexing aspect of ATD that has emerged over theyears is the marked variation in clinical severity of lung and liverdisease among affected homozygotes. The classical form of ATD isan autosomal co-dominant disorder that affects 1 in 3000 live birthsin many populations; however, a significant number of homozygotesescape both liver and lung disease. There is also a marked variationin the age of onset and severity of lung disease (Silverman andSandhaus, 2009). We now know that one environmental modifier,cigarette smoking, markedly increases the severity of lung diseaseand that other genetic and environmental modifiers are alsoinvolved. Analysis of a unique cohort of homozygotes identified byan unbiased newborn screening study carried out in Sweden hasshown that only ~8% of homozygotes develop clinically significantliver disease in the first 4 decades of life (Piitulainen et al., 2005;Sveger, 1976), indicating that genetic and/or environmentalmodifiers play a major role in whether a homozygote falls into thesubpopulation that is susceptible to liver disease or is somehowprotected from liver disease. This variation in clinical phenotype hasadded to the challenge of detection and diagnosis of ATD and meansthat therapeutic strategies have to be tested in and designed for
Mysteries of α1-antitrypsin deficiency: emerging therapeuticstrategies for a challenging diseaseRaafe Ghouse1,2, Andrew Chu1,2, Yan Wang1,2 and David H. Perlmutter1,2,3,*
Dis
ease
Mod
els
& M
echa
nism
s

412
specific subgroups of the affected, already rare, population. In thisreview, we will discuss advances in our understanding of liver andlung disease of ATD, pathogenic mechanisms, and novel therapiesthat are now being investigated to treat this clinically challengingdisease.
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
Box 1. Clinical terms• Ascites: pathologic accumulation of fluid in the peritoneal cavity• Augmentation therapy: treatment involving intravenous infusion of
pooled α1-antitrypsin collected from the plasma of healthy donors• Biliary atresia: end result of a destructive, idiopathic, inflammatory
process that affects intrahepatic and extrahepatic bile ducts, leadingto fibrosis and obliteration of the biliary tract and eventualdevelopment of biliary cirrhosis
• Bronchiectasis: abnormal, chronic enlargement of the bronchi• Cholestasis: physiologically defined as a measurable decrease in
bile flow and pathologically defined as the histological presence ofbile pigment in hepatocytes and bile ducts
• Chronic obstructive pulmonary disease (COPD): preventable andtreatable disease characterized by airflow limitation that is not fullyreversible. The airflow limitation is usually progressive and isassociated with an abnormal inflammatory response of the lungs tonoxious particles or gases, primarily caused by cigarette smoking.Although COPD affects the lungs, it produces significant systemicconsequences. Manifestations of COPD range from dyspnea, poorexercise tolerance, chronic cough with or without sputum productionand wheezing to respiratory failure
• Cirrhosis: diffuse liver process characterized by fibrosis and theconversion of normal liver architecture into structurally abnormalnodules. Cirrhosis represents a dynamic state reflecting thecompeting processes of cell injury (necrosis), response to injury(fibrosis) and regeneration (nodule formation)
• Dyspnea: shortness of breath• Ecchymoses: subcutaneous extravasation of blood causing
discoloration of the skin• Emphysema: pathological term for destruction of the gas-
exchanging surfaces of the lung• FEV1: also known as forced expiratory volume; a measure of the
maximum amount of air that can be expelled in the first secondduring a forced vital capacity (FVC) determination
• Fibrosis: the formation of excess fibrous connective tissue (scartissue) in an organ
• FVC: forced vital capacity; the volume delivered during an expirationmade as forcefully and completely as possible starting from fullinspiration
• Hepatocellular carcinoma: malignant tumor that arises from thehepatocytes
• Huntington’s disease: neurodegenerative genetic disorder thataffects muscle coordination and leads to cognitive decline andneuropsychiatric manifestations
• Hypercholesterolemia: the presence of high levels of cholesterol inthe blood
• Hypersplenism: disorder involving enlarged spleen size andpremature sequestration of circulating blood cells in the spleen, oftenresulting in abnormal decreases in circulating levels of white bloodcells, red blood cells and/or platelets; associated with a variety ofdisorders, including cirrhosis due to chronic liver disease (see also‘Splenomegaly’ and ‘Cirrhosis’)
• Jaundice: the visible yellow discoloration of soft tissues (skin, eyes)due to accumulation of bile pigments in these tissues; a commonmanifestation of chronic liver disease
• Lucency: in radiology, a region in an image caused by an absorberof lower X-ray attenuation than its surrounding tissues
• Portal hypertension: clinical syndrome hemodynamically definedas an increase in the pressure gradient across the liver (betweenportal pressure and inferior vena cava pressure) above the normalvalue of 5 mmHg
• Pruritus: sensation of intense, persistent itching; a common clinicalmanifestation of chronic liver disease
• Splenomegaly: enlargement of the spleen, as detected by clinicalexamination or radiological measurement of spleen size (see also‘Hypersplenism’)
Liver
Vessel
Blood
Liver
White blood cell(neutrophil)
Normal
α1-antitrypsin:synthesized in the liverand secreted into thebloodstream to inhibitneutrophil elastase.
Neutrophil elastase: produced by white blood cells to break down harmful bacteria. Potentially damaging to lungs if exposed..
α1-antitrypsin coats lungs, protecting them from neutrophil elastase.
White blood cell(neutrophil)
e
ATD
α1-antitrypsin: trapped in liver, causing liver damage.
Neutrophil elastase: uninhibited, causing lung damage.
Lungs lack α1-antitrypsin coating, leaving them open to damage by neutrophil elastase.
e
Lung
Liver
Lung
Bloodvessel
Bloodvessel
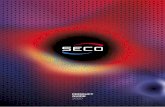
Fig. 1. Pathophysiology of α1-antitrypsin and its deficiency (ATD).Synthesis, secretion and function of AT in the circulation and lungs of anunaffected individual (top) and illustration of how the liver and lungs areadversely affected in the classical form of ATD (bottom) (image used withpermission from The University of Utah Genetic Science Learning Center,http://Learn.Genetics.utah.edu).
Dis
ease
Mod
els
& M
echa
nism
s

Clinical characteristics of ATD-associated liver diseaseHow is liver disease that is caused by ATD clinically recognized?Forms of this liver disease manifest in infancy, childhood,adolescence or later in adult life. The usual presentation in infants,persistent jaundice, is noted at 1-2 months of age. These infantsoften have elevated serum conjugated bilirubin and transaminaselevels, suggesting liver involvement. In some cases there might alsobe an enlarged liver. The infantile presentation of ATD can closelyresemble that of extrahepatic biliary atresia in terms of overallclinical appearance and laboratory evaluation. The clinicalpresentation can also be characterized by pruritus andhypercholesterolemia, and it is important to distinguish this frominborn errors of bile secretion that cause infantile cholestasis. Moresevere liver dysfunction reflecting portal hypertension, such asgastrointestinal bleeding, ascites, splenomegaly and hypersplenism,and poor growth, is occasionally seen in cases of ATD in infancy(reviewed in Perlmutter, 2011).
Liver disease caused by ATD that comes to clinical attention duringchildhood or adolescence is almost always recognized because of theeffects of portal hypertension. In adults, it is recognized either becauseof the sequelae of portal hypertension or because of hepatocellularcarcinoma (see Case study box). This reflects the pathological effectsof mutant ATZ accumulation in the liver, leading to fibrosis and/orcirrhosis, and hyperproliferation of hepatocytes. An autopsy studycarried out in Sweden showed a highly significant association of ATDand hepatocellular carcinoma, well beyond what might be associatedwith cirrhosis alone (Eriksson et al., 1986). Over the past 20 yearsthere seems to have been an increase in the prevalence of the ‘adult’form of ATD liver disease. Indeed, over the last 10 years, 85-90% ofall liver transplant procedures performed in the United States for ATDwere for adults, typically at around 50 to 65 years of age (UnitedNetwork of Organ Sharing website, http://optn.transplant.hrsa.gov/).A significant number of adult patients with ATD who come to clinicalattention have other causes of liver disease, including alcoholic liverdisease, non-alcoholic steatohepatitis, or features of hemochromatosisor autoimmune liver disease.
Much of what is known about the prevalence of liver disease inATD and its outcome comes from a prospective, relatively unbiasedstudy started in Sweden in the 1970s (Piitulainen et al., 2005;Sveger, 1976). In this nationwide screening study, 200,000newborns were screened and 127 homozygotes identified. From thisgroup of homozygotes, 14 had prolonged obstructive jaundice and9 of the 14 had severe liver disease. A little more than 50% of theremaining infants had elevated blood transaminase levels but noother signs of liver disease. This cohort has been followed relativelycompletely over the ensuing 40 years, and we know that only ~8%of the population has developed clinically significant liver disease.One of the limitations of this cohort study is that liver biopsies werenot performed, so many homozygotes could have smolderinghepatic fibrosis that will first present clinically as the ‘adult’ form ofthe disease in the sixth or seventh decade of life.
It is still very difficult to prospectively predict which individualswith ATD will develop severe liver disease. Treatment is directed atalleviating the complications of portal hypertension but livertransplantation is the only therapeutic strategy currently availablefor severe liver disease caused by ATD.
Clinical characteristics of lung disease in ATDWhat are the clinical effects of ATD on the lungs? ATD predisposesindividuals to premature development of COPD with panacinaremphysema. It is characterized by progressive decline in forcedexpiratory volume (FEV1). Dyspnea is the most common symptom,
and many patients report cough, phlegm production and wheezing,either chronically or with acute viral upper respiratory tractinfections (Janus et al., 1985). The long-term loss of pulmonaryfunctional capacity correlates with the incidence of respiratoryinfections (Dowson et al., 2001). COPD associated with ATD oftenshows a characteristic radiographic pattern with hyperinflation andmarked lucency at the lung bases (see Case study box). In one studyof individuals with ATD, emphysematous abnormalities were mostprominent at the bases in 64% of patients and at the apices in 36%(Parr et al., 2004).
ATD has also been associated with bronchiectasis. An early studyindicated that bronchiectasis was present in 11.3% of 246 individualswith ATD (Larsson, 1978). The estimated prevalence in other reportshas varied widely, from 2% to 43% (Piras et al., 2013; Cuvelier et al.,2000). The exact relationship between bronchiectasis and ATDremains a mystery. ATD should be considered in the differentialdiagnosis of bronchiectasis along with cystic fibrosis, primaryimmunodeficiency, allergic bronchopulmonary aspergillosis anddisorders that affect ciliary function, such as primary ciliarydyskinesia.
Lung disease does not affect ATD individuals during childhood.However, the onset of emphysema in ATD individuals can be earlierthan in non-ATD individuals, who usually present in the sixth andseventh decades of life. The National Heart, Lung, and BloodInstitute-sponsored registry for patients with ATD found the meanage to be 46 years (Alpha1-Antitrypsin Deficiency Registry StudyGroup, 1994). Multiple studies have demonstrated that ATD is astrong risk factor for early-onset COPD, but not every ATD
413
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
Case studyA 52-year-old male presents for evaluation of progressive fatigue andeasy bruising. His history is notable for a chronic intermittent cough andseveral episodes of pneumonia in the last few years, which were treatedwith outpatient antibiotics. He has experienced increased shortness ofbreath with physical exertion. He uses albuterol inhalers as neededduring intermittent respiratory symptoms and, despite counseling, hecontinues to smoke one pack of cigarettes daily. Family history revealsthat his father died from complications of pulmonary disease that wasattributed to heavy tobacco use. He also had a sibling twin who died ininfancy of liver failure of unknown etiology. On physical examination, hehas scattered ecchymoses along his extremities, diffuse wheezing andcrackles throughout his lung fields, a firm liver edge 2 inches below thecostal margin, and a palpable spleen. Laboratory assessments revealmild elevations in his liver transaminases (ALT=67 IU/l, AST=52 IU/l) withdecreased albumin (2.9 g/dl) and elevated INR (international normalizedratio for prothrombin time) (1.8). Chest X-ray shows hyperinflated,hyperlucent lung fields. Liver ultrasound reveals diffusely coarsenedechotexture suggestive of fibrosis as well as a 2 cm focal hypoechoiclesion in the right hepatic lobe. α1-antitrypsin phenotype returns as PiZZwith a decreased serum level of AT of 31 mg/dl.
This case presents several of the challenges found in ATD. Without ahigh degree of suspicion for ATD, clinicians might interpret pulmonaryabnormalities as evidence of other more common entities like asthma.Liver disease can follow an insidious course, with transaminases oftenbeing normal or minimally elevated, making them an unreliable indicatorof liver injury. Significant fibrosis and hepatocellular carcinoma might notbe detected until liver pathology is advanced. Even with early detection,there are currently no therapies for ATD-associated liver disease beyondtransplantation. For lung disease, augmentation therapy is available, butlong-term efficacy is questionable. Another interesting aspect of this caseis the sibling twin who died of liver disease, which could have been asevere infantile presentation of ATD-associated liver disease. Markedclinical variability is a hallmark of ATD and is probably a function ofgenetic modifiers such as polymorphisms in genes that regulateautophagy.
Dis
ease
Mod
els
& M
echa
nism
s

414
individual is destined to develop COPD. Risk factors includechronic bronchitis, frequent pneumonias, family history of COPD,and cigarette smoking. Cigarette smoking increases the risk ofdeveloping fixed airflow obstruction and can markedly acceleratethe onset of dyspnea by as much as 19 years, leading to earlier andmore severe pulmonary disease. The effect of cigarette smoking isthought to be due to oxidative and proteolytic inactivation ofresidual AT function by active oxygen intermediates andmetalloproteases released from mononuclear phagocytes (Crystal,1990; Stockley et al., 2009). The rate of decline in FEV1 is fourtimes greater in smoking than in nonsmoking persons with ATD(Janus et al., 1985).
Increased susceptibility to COPD in ATD is predominantly due toa loss-of-function mechanism. In normal individuals, AT bathes theelastin-rich extracellular matrix in the interstitium of the lungparenchyma, protecting them from neutrophil elastase.Homozygotes for ATD are susceptible to premature development ofemphysema because reduced AT activity in the lungs permitsuninhibited proteolytic damage to their connective tissue matrix.However, there is substantial variability in the development ofdisease among individuals who are homozygous for the Z alleleeven when cigarette smoking is taken into consideration (DeMeo etal., 2009). Genome-wide association studies and integrative genomicapproaches in COPD have demonstrated significant associations inATD patients for single-nucleotide polymorphisms (SNPs) in thechromosome 15q region that includes CHRNA3 (cholinergicnicotine receptor alpha3) and IREB2 (iron regulatory binding protein2) (Kim et al., 2012). Other potential modifiers of lung disease inATD include NOS3, GSTP1, TNF and IL10.
Most individuals with lung disease due to ATD are being treatedwith purified AT replacement therapy. Although this treatmentcorrects the anti-elastase deficiency, there is still limited evidence ofclinical efficacy (Dickens and Lomas, 2011). This could be becausethis therapy is only instituted clinically at a stage in which theemphysematous process is irreversible or, alternatively, that othermechanisms contribute to the lung disease pathogenesis. There is alsorecent evidence that pharmacological protocols for AT replacementtherapy have anti-inflammatory and immunomodulatory effects thatare independent of its elastase-inhibitory properties (Jonigk et al.,2013). Each year, a number of patients with ATD lung disease, oftenseverely affected at an early age, thereby undergo lung transplantation(Tanash et al., 2011).
Cellular mechanisms that determine liver diseaseHow does the liver get damaged in ATD? It is now well establishedthat the mechanism of liver disease in ATD involves gain-of-toxic-function mechanisms. The strongest evidence comes from theoutcome of expressing the mutant ATZ gene in transgenic animals.The so-called PiZ mouse model of ATD was generated by using asa transgene a genomic fragment that encodes all exons and intronsof human ATZ, including ~2 kb of upstream and downstreamflanking regions (Sifers et al., 1987; Carlson et al., 1989). Inaddition to the intrahepatocytic globular inclusions that are thehistological hallmark of the disease, these mice develop hepaticfibrosis and hepatocellular carcinoma that closely phenocopies theliver in humans with ATD (Hidvegi et al., 2010; Marcus et al.,2010). Recently, a Caenorhabditis elegans model of ATD wasreported to show reduced longevity, delayed development anddecreased brood size, providing further validation for a proteotoxiceffect of ATZ accumulation in a living organism (Gosai et al., 2010).
Although the molecular details of the process by whichintracellular accumulation of mutant ATZ elicits proteotoxic effects
are not known, cellular responses to ATZ accumulation have beencharacterized in model systems to determine which intracellulardegradation pathways participate in the disposal of the mutantprotein and the signaling pathways that are activated, presumably tofacilitate cellular adaptation. The results of these studies have led tothe recognition that the proteasomal and autophagic degradationpathways play a major role in disposal of ATZ (Fig. 2). The role ofthe proteasomal pathway in ATZ disposal has been demonstrated inyeast and mammalian systems, and involves a process named ER-associated degradation (ERAD), in which substrates for degradationin the ER are delivered to the proteasome in the cytoplasm byretrograde translocation (Brodsky, 2012; Qu et al., 1996; Werner etal., 1996).
Autophagy also plays a major role in the disposal of accumulatedATZ. Autophagy is a ubiquitous pathway by which cells digestinternal constituents to generate amino acids as a mechanism forhomeostatic turnover and to survive stresses such as starvation. It ischaracterized by the formation of double-membrane vacuoles in thecytoplasm, which sequester cytoplasm and subcellular organellesand then fuse with lysosomes, with consequent degradation of theinternal constituents. The autophagic pathway has been shown toplay a crucial role in the degradation of aggregated proteins, anddefects in autophagic function, including the known decline inautophagy with aging, have been implicated in the pathogenesis ofdegenerative diseases (Rubinsztein et al., 2011). Autophagy was firstimplicated in ATD when abundant autophagosomes were observedin mammalian cell lines, in the PiZ mouse model and then in theliver of patients with ATD (Teckman and Perlmutter, 2000).Definitive evidence for the role of autophagy in the disposal of ATZwas provided by studies showing delayed degradation of ATZ inmammalian cell line and yeast models genetically engineered fordeficits in autophagy (Kamimoto et al., 2006; Kruse et al., 2006).Studies in a novel mouse model of ATD engineered for liver-specific inducible expression of ATZ and green fluorescentautophagosomes showed that the accumulation of ATZ is sufficientto activate autophagy, suggesting that autophagy is particularlyimportant in ATD because it is specifically activated when ATZaccumulates, and then plays a role in its disposal (Kamimoto et al.,2006). In yeast rendered autophagy-deficient by a mutation in ATG6(beclin 1 in mammals), ATZ disposal is only impaired when levelsof expression are high (Kruse et al., 2006). These results suggest thatthe ERAD/proteasomal pathway can handle ATZ at lower levels ofexpression, presumably because it is capable of degrading solubleforms of ATZ, but at higher levels of expression, as ATZaccumulates in polymers and insoluble aggregates, autophagybecomes critical for ATZ degradation. A recent study showed thatthe proteasomal and autophagic pathways play important roles inATZ disposal in a live, whole-organism model of ATD in C. elegans(Gosai et al., 2010).
Recently, a pathway from Golgi to lysosome that is mediated bysortilin has been shown to contribute to intracellular degradation ofATZ in yeast and mammalian cell line models (Gelling et al., 2012).This pathway probably participates in the disposal of any ATZmolecules that reach the Golgi or re-cycle into the ER-Golgiintermediate compartment. Polymorphic variation in sortilin hasbeen implicated in risk for cardiovascular disease and, based on itscontribution to intracellular degradation of ATZ, it is also acandidate modifier of ATD-associated liver disease. We suspect thatthere are still other mechanisms by which cells degrade ATZ thathave not yet been identified.
Several signaling pathways are specifically activated in responseto intracellular ATZ accumulation and presumably reflect protective
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
Dis
ease
Mod
els
& M
echa
nism
s

adaptations or what have been called ‘proteostasis’ mechanisms.Cell line and mouse models with inducible expression of ATZ havebeen particularly valuable for identification of these pathwaysbecause these types of systems are less prone to cellular adaptationsthat potentially occur in systems with constitutive expression of themutant protein. As mentioned above, a mouse model withhepatocyte-specific inducible expression of ATZ was used to showthat the autophagic response is activated when ATZ accumulates inthe liver, providing evidence for the importance of autophagy as aproteostatic response to hepatic ATZ accumulation (Kamimoto etal., 2006). Similar approaches have shown that NFκB and TGFβsignaling are also a part of the distinct adaptive response of cells toATZ accumulation (Hidvegi et al., 2005; Hidvegi et al., 2007).Because one of the downstream targets of NFκB is the transcriptionfactor Egr1, which is essential for hepatocyte proliferation in theregenerative response to partial hepatectomy (Liao et al., 2004), webelieve that NFκB activation is important in the effect of ATZaccumulation on liver cell proliferation and carcinogenesis in ATD(Hidvegi et al., 2007). Because it has been widely implicated inhepatic fibrosis (Wynn, 2007), TGFβ signaling is likely to be one ofthe mechanisms by which hepatic fibrosis develops in ATD.Intracellular accumulation of ATZ has minimal or no activation ofthe unfolded protein response (UPR) in most systems, or it leads torelatively limited activation of the UPR (Hidvegi et al., 2005). Thiscould be due to the tendency of ATZ to polymerize rather than‘unfold’, supported by the finding that UPR signaling is more robustwhen nonpolymerogenic AT variants accumulate in the ER in
comparable cell and mouse systems (Hidvegi et al., 2007). Therelative lack of UPR signaling when ATZ accumulates in the ERcompared with when nonpolymerogenic AT variants accumulatecould provide an explanation for why there is relatively limitedapoptosis in the liver in ATD. However, the relationship betweenATZ accumulation and UPR signaling is not well understood andawaits further in-depth investigation.
Studies by Rudnick et al. that investigated liver cell proliferation inthe PiZ mouse model of ATD have shed some light on the predilectionfor primary liver cancer in ATD (Rudnick and Perlmutter, 2005;Rudnick et al., 2004). Liver cells that have accumulated morepolymerized ATZ (so-called globule-containing hepatocytes) arerelatively impaired in proliferation but induce chronic hyper-proliferation in the globule-devoid hepatocytes by a trans-effect.Interestingly, most hepatocellular carcinomas described in individualswith ATD are negative for AT staining but in many cases aresurrounded by AT-positive, globule-containing hepatocytes, consistentwith the concept that globule-containing hepatocytes drive the chronichyper-proliferative process that leads to carcinoma (Hadzic et al.,2006; Zhou and Fischer, 1998; Zhou et al., 2000).
Presumably, clinically significant liver disease evolves when ATZaccumulation and the resulting proteotoxicity overwhelms thesecell-protective proteostatic mechanisms. According to thisconceptual paradigm, genetic and environmental modifiers are likelyto influence this delicate balance of proteotoxic and proteostaticforces. This idea has been validated to a certain extent by early workthat demonstrated a lag in intracellular degradation of ATZ in cell
415
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
Plasma membrane Extracellular space
Cytoplasm
Proteasomal
degradation
ATZ monomer
ER
Nucleus
Golgi
Ub
Autophagicdegradation
ATZ aggregates
Wild-type AT
Autophagosome
Lysosome
Secretion
Autophagy enhancers(Fluphenazine, Pimozide)
Autophagy-inducingpeptide
Carbamazepine
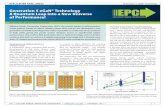
Fig. 2. Pathways for the disposal of the mutant form of AT, ATZ, as potential therapeutic targets in ATD. Unlike wild-type AT, which efficiently traversesthe conventional secretory pathway, the majority of mutant ATZ accumulates in the ER. Soluble forms of ATZ (ATZ monomers) are presumably degraded bythe proteasomal pathway, whereas insoluble forms of ATZ (ATZ aggregates) are degraded by autophagy. Emerging candidate therapies that target thesedisposal pathways include carbamazepine, which has been shown to increase both proteosomal and autophagic disposal of ATZ. Autophagy enhancers suchas certain phenothiazines and the novel Tat-beclin 1 peptide, an autophagy-inducing peptide, enhance autophagic disposal of ATZ. Ub, ubiquitin.
Dis
ease
Mod
els
& M
echa
nism
s

416
lines from ATD patients with severe liver disease (Wu et al., 1994).It is also supported by the observation that drugs that enhanceautophagy reduce the hepatic load of ATZ in the PiZ mouse model(Hidvegi et al., 2010). A polymorphism in ER mannosidase I, anenzyme involved in the ERAD pathway, has recently beenimplicated as a genetic modifier predisposing to infantile disease(Pan et al., 2009). This putative modifier mechanism is alsoconsistent with the conceptual model that disease occurs whenproteotoxicity overwhelms proteostasis mechanisms.
Autophagy enhancer drugs for proteotoxicityRecently, we investigated the possibility that intracellular disposalpathways could be used as targets for mitigating the ATZaccumulation/proteotoxicity that causes liver disease in ATD. Weselected the autophagy pathway as a target for several reasons: it isspecifically activated when ATZ accumulates in cells and in the liverin vivo (Kamimoto et al., 2006); it participates in the disposal ofATZ and is specialized for insoluble polymers or aggregates of ATZ(Kruse et al., 2006); and a number of drugs that stimulate autophagyhave been shown to reduce the cellular load of aggregation-proneproteins that cause neurodegenerative diseases, particularlyHuntington’s disease (Sarkar et al., 2007; Zhang et al., 2007). Fromthe list of available autophagy enhancer drugs, we focused oncarbamazepine (CBZ), an anticonvulsant and mood stabilizer,because it has been used so extensively in clinical practice. Theresults showed that CBZ could indeed mediate increasedintracellular degradation of ATZ. Even more importantly, whenadministered orally to PiZ mice the drug mediated a reduction inhepatic ATZ load and in hepatic fibrosis (Hidvegi et al., 2010).Because CBZ is approved by the FDA for use in clinical practice, ithas been moved into a Phase II/III clinical trial for patients withsevere liver disease due to ATD. The results of this study alsovalidate the concept that endogenous proteostasis mechanisms,mechanisms that probably protect ATD patients from hepaticproteotoxicity and disease, can be targeted for effective drug therapy.
By adapting a novel C. elegans model of ATD as a high-contentdrug-screening platform, we have identified several other drugs thatenhance the autophagic disposal of ATZ and reduce proteotoxicity(Gosai et al., 2010). To generate the C. elegans model, a chimericGFP-ATZ plasmid was used as a transgene and targeted forexpression in the intestine because the intestinal cells of C. eleganscarry out many of the functions attributed to the liver in higherorganisms. The model recapitulates the cellular defect of ATD withintracellular accumulation of GFP-ATZ and proteotoxicity. Becausethe degree of ATZ accumulation correlates with intensity of GFP+inclusions in the worm intestine and these fluorescent signals can bequantified, the model permits high-content analysis using automatedarray scanning and large-particle flow cytometry. As proof ofprinciple, an initial screen of the Library of PharmacologicallyActive Compounds (LOPAC) identified five hit compounds thatinduced significant, dose-dependent reductions in worm ATZ load.Of these, four compounds are known to enhance autophagic activityand are already in clinical use, providing the possibility that drug re-purposing can accelerate clinical trials for treatment of ATD-associated liver disease. Furthermore, two of the compounds arefrom the phenothiazine family, a drug family that is structurallyrelated to tricyclic antidepressants, including CBZ (Table 1; Fig. 2).The phenothiazines have also been shown to enhance autophagicdegradation of the aggregation-prone protein huntingtin (the proteinmutated in Huntington’s disease) (Tsvetkov et al., 2010; Zhang etal., 2007). Thus, this type of screening platform provides a powerfulnew model for drug discovery for ATD and two new strategies for
chemical and computational-based drug discovery using theautophagy enhancer drug paradigm and the phenothiazine structure.
In our initial study of CBZ, we speculated that a mechanismindependent of TOR (target of rapamycin) kinase was involved in theautophagy-enhancing activity because we could not detect any effectof rapamycin on cellular ATZ load in a mammalian cell line or in theliver of the ATD mouse model (Hidvegi et al., 2010). Consistent withthis, it seems that one of the phenothiazines discovered to enhanceautophagic degradation of Huntington mediates its effects by a TOR-independent mechanism (Xia et al., 2010). In this case, autophagy wasenhanced because of reduced intracellular calcium, which leads todiminished calpain-1-mediated cleavage of autophagy protein ATG5.We would predict that a number of different types of TOR-independent mechanisms for activation and enhancement ofautophagy will be uncovered in the future, because more evidence forTOR-independent pathways for autophagy induction have recentlyemerged (Tan et al., 2012; Boglev et al., 2013).
Several other exciting strategies for enhancing autophagy haverecently come to light. The laboratory of Beth Levine described anovel autophagy-inducing peptide termed Tat-beclin 1, building onprior observations that the HIV protein Nef inhibits autophagy bydirectly interacting with the autophagy regulatory factor beclin 1(Kyei et al., 2009; Shoji-Kawata et al., 2013). In their experiments,Shoji-Kawata et al. succeeded in identifying an 18-amino acid Nef-interacting domain of beclin 1 and linked it to the Tat sequence toincrease cell uptake (Shoji-Kawata et al., 2013). They went on toshow that Tat-beclin 1 peptide is a potent inducer of autophagy andenhances the degradation of mutant huntingtin and several invasivebacterial and viral pathogens. Their findings suggest that Tat-beclin1 could potentially be used as a therapeutic agent in ATD, in otherdiseases caused by aggregation-prone proteins and also possibly forcertain infectious diseases.
Using a novel gene therapy approach, Pastore et al. studied theeffect of transcription factor EB (TFEB), a master gene thatregulates autophagy and lysosomal gene expression (Pastore et al.,2013). In experiments using mouse embryonic fibroblasts (MEFs)co-transfected with TFEB and ATZ, they found that TFEB inducesATZ clearance and that this effect was autophagy-dependent,because the reduction in ATZ load was not observed in autophagy-deficient Atg7−/− MEFs. Using adenovirus-mediated gene transferof TFEB in the PiZ mouse model of ATD-associated liver disease,they found that TFEB transfer promoted hepatic ATZ clearance andreduced liver fibrosis in the mice. These findings further validate theconcept that enhancing autophagy is a plausible therapeuticapproach for ATD-associated liver disease (Table 1).
Other new therapeutic strategiesSeveral other novel therapeutic approaches are emerging. In somecases these approaches are designed to target the gain-of-functionproteotoxic mechanisms of ATD; however, several other of thesenew strategies target both gain-of-function and loss-of-functionmechanisms to potentially ameliorate liver and lung disease. Forexample, two recent studies have suggested that gene therapy couldbe used to knockdown expression of the mutant ATZ gene usingvectors that also encode the wild-type AT and therein wouldpotentially address both gain-of-function proteotoxicity and loss-of-function mechanisms for tissue damage in ATD (Li et al., 2011;Mueller et al., 2012). In one study, adeno-associated virus encodingshort-hairpin RNA to knockdown endogenous AT gene expressionwas used together with a codon-optimized wild-type AT transgenecassette (Li et al., 2011). In the other report, an adeno-associatedvirus encoding microRNA to silence endogenous AT gene
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
Dis
ease
Mod
els
& M
echa
nism
s

expression together with a microRNA-resistant wild-type AT genewas delivered (Mueller et al., 2012). These approaches both led tohigh levels of human AT in the serum of a transgenic mouse modelof ATD and significant reduction in hepatic ATZ accumulation.However, evidence that liver fibrosis was reduced by these strategieswas not strong; thus, it remains uncertain whether or not morepotent and widespread silencing would be needed within the liver toprevent proteotoxicity.
Several groups have utilized a strategy for ‘structure-based’ drugdevelopment that begins with designing peptides to preventpolymerization of the mutant ATZ molecule and theoreticallyinfluence its potential for secretion. For example, a small-moleculedrug that targets a lateral hydrophobic cavity in the ATZ protein wasfound to prevent polymerization of ATZ but, in a cell model, itincreased intracellular degradation rather than increased secretion(Mallya et al., 2007). Peptides that target the reactive center loop ofAT have also been tested, and these increase the rate of secretion ofmutant ATZ in a cell line model, although it is not clear whetherthey also led to increased intracellular accumulation (Alam et al.,2012). Furthermore, these peptides have not been tested in an animalmodel. Advancing the latter strategy will also depend on whetherdrugs based on the structure of these peptides can be identified andtested for safety and efficacy.
Chemical chaperones have also been investigated as a potentialtherapeutic class for treatment of ATD. These are compoundsthought to optimize the intracellular folding environment in a
general way and in so doing can at least partially correct cellularmislocalization of some mutant proteins (Engin and Hotamisligil,2010). In contrast to so-called pharmacological chaperones, whichbind to and stabilize proteins in a substrate-specific way, thechemical chaperones can facilitate folding of multiple misfoldedproteins non-selectively. We have found that two of the compoundsin the general category, glycerol and 4-phenylbutyric acid (PBA),mediate a marked increase in secretion of ATZ in a model cell linesystem (Burrows et al., 2000). This drug also mediated an increasein blood levels of human ATZ when administered orally to a mousemodel transgenic for human ATZ, with blood levels reaching 20-50% of the levels present in normal humans. Because PBA had beenused safely for years in children with urea-cycle disorders, this drugwas considered a candidate for chemoprophylaxis of both liver andlung disease in ATD. Although a pilot study in ten patients with liverdisease due to ATD did not show an increase in serum levels of ATafter 14 days of treatment with PBA, it is possible that this was nota sufficient duration of treatment or that the ability of patients withchronic liver disease to tolerate the large dose of PBA required foreffects in humans was limited (Teckman, 2004). Because PBAselectively affects secretion of ATZ and mediates its effect in vivo,and further because this kind of effect has not been observed for anyother pharmacological agent, it will be important to furtherinvestigate PBA if more favorable formulations become available.
Recently a drug with chemical properties very similar to PBA,suberoylanilide hydroxamic acid (SAHA), was shown to increase
417
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
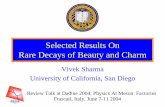
Table 1. Emerging candidates for the medical therapy of ATD-associated liver disease Name Structure Mechanism Methodology/disease models References
Carbamazepine (CBZ)
Mood-stabilizing agent shown to induce autophagic disposal of insoluble ATZ and proteosomal degradation of soluble ATZ
ATD: mammalian cell lines, mouse model
Hidvegi, 2010
Fluphenazine (FLU) Phenothiazine identified as an autophagy-inducing compound by high-throughput screening. Mechanism(s) of autophagic induction being determined
ATD: high-content screen, C. elegans model
Gosai, 2010
Pimozide (PMZ) Phenothiazine identified as an autophagy-inducing compound by high-throughput screening. Mechanism(s) of autophagic induction being determined
ATD: high-content screen, C. elegans model
Gosai, 2010
4-phenylbutyric acid (PBA)
Chemical chaperone that facilitates protein folding. Increases secretion of ATZ
ATD: mammalian cell lines, mouse model
Burrows, 2000
Suberoylanilide hydroxamic acid (SAHA)
Histone deacetylase 7 inhibitor with properties similar to PBA. Increases ATZ secretion and synthesis
ATD: mammalian cell lines Bouchecareilh, 2012
Tat-beclin 1 peptide YGRKKRRQRRR-GG-TNVFNATFEIWHDGEFGT
Novel autophagy-inducing peptide, which binds GAPR-1 and releases beclin-1 from Golgi, thereby increasing free beclin-1 in the cytosol to induce autophagy
Huntington’s disease: mammalian cell lines, mouse model.
Infectious disease: mammalian cell lines, mouse model
Shoji-Kawata, 2013
ATD, 1-antitrypsin deficiency.
Dis
ease
Mod
els
& M
echa
nism
s

418
secretion of ATZ in cell line models of ATD, and this effect wasproposed to be mediated by inhibition of the histone deacetylaseHDAC7 (Bouchecareilh et al., 2012). However, this drug was nottested in vivo. Furthermore, unlike PBA, SAHA mediates asubstantial increase in synthesis of ATZ through a transcriptionalactivation mechanism. It was not entirely clear whether the increasein ATZ in extracellular fluid could be largely attributable to theincrease in synthesis. Even if the results are consistent with increasesin ATZ synthesis as well as an increase in translocation through thesecretory pathway, the effect of this drug would be associated withincreased accumulation of ATZ in the ER and therein possibly withincreased proteotoxicity (Table 1).
Because transplanted hepatocytes can repopulate the diseasedliver, cell transplantation therapy for ATD has also been discussed.Indeed, Ding et al. demonstrated that wild-type donor hepatocytescan almost completely repopulate the liver of the PiZ mouse modelof ATD (Ding et al., 2011). Use of this type of ‘cellular’ therapycould be an alternative approach to replacement therapy to preventCOPD and perhaps also to prevent or treat liver disease, because thetransplanted hepatocytes have a selective proliferative advantageover endogenous hepatocytes and can eventually supplant the latter.
A combination of gene-targeting and cell-based therapy mightalso be a potential strategy for COPD and perhaps liver disease inATD. Yusa et al. recently reported exciting results in which themutation in the AT gene was corrected in human induced pluripotentstem cells (iPS cells) from a patient homozygous for ATZ by acombination of zinc-finger nucleases and transposon technology,and then the iPS cell line was shown to engraft into the liver of atransgenic mouse model (Yusa et al., 2011). This strategy, if it canbe adapted for human application, has the potential to correct boththe loss-of-function and gain-of-function mechanisms, and wouldhave the advantage of obviating the need for immunosuppression.
Conclusions and future directionsATD is unique in that the disease phenotype in one target organ, thelung, is caused by a loss-of-function mechanism, whereas, in anotherorgan, the liver, it is caused by gain-of-function proteotoxicity. ATDis the most common genetic cause of COPD, but modifiers such ascigarette smoking and consequences of infections play an importantrole in varying the age of onset and severity of lung disease.Although replacement therapy with purified AT corrects the loss-of-function mechanism for lung disease in ATD, this therapy has notbenefited all affected individuals and has had limited clinicalefficacy in other cases.
ATD is also the most common genetic cause of liver disease inchildhood. Different clinical forms present in infancy, childhood,adolescence or during adulthood. Epidemiological informationsuggests that genetic and/or environmental modifiers determinewhether or not ATD individuals develop clinically significant liverdisease and its age of onset. A series of studies suggest thatendogenous proteostasis mechanisms are candidates for thesemodifiers and autophagy is a particularly important mechanism bywhich the liver attempts to protect itself from proteotoxicity.Exciting new data indicates that FDA-approved drugs that enhanceautophagy reduce liver disease in mouse models of ATD and couldbe ideal candidates for chemoprophylaxis of ATD-associated liverdisease. Several other new therapeutic strategies, including genesilencing and the use of genetically engineered iPS-cell-derivedhepatocytes, are now under investigation.
The major challenges for clinical and basic research in the near-term include further elucidation of modifiers and characterization ofhow these modifiers act in cell and animal models (see Clinical and
basic research opportunities box). The use of iPS cell line modelswill help to understand the action of modifiers on ATZaccumulation/proteotoxicity and also to provide a personalizedapproach to the testing of treatment strategies. Further studies ofwhy AT replacement therapy has not had a more transformationaleffect on lung disease progression and of the prevalence of liverdisease among adults with ATD are needed. Identification ofbiomarkers of the hepatic and pulmonary diseases of ATD will beessential for clinical trials of the new therapeutic strategies currentlybeing developed.
This article is part of a review series on protein-folding diseases. See relatedarticles at http://dmm.biologists.org/site/protein-folding-disease.xhtml.
Competing interestsThe authors declare no competing financial interests.
FundingWe are grateful for grants from NIH (DK076918, DK084512, DK096990) andinstitutional funds from Children’s Hospital of Pittsburgh of UPMC that havesupported our studies reported here.
ReferencesAlam, S., Wang, J., Janciauskiene, S. and Mahadeva, R. (2012). Preventing and
reversing the cellular consequences of Z alpha-1 antitrypsin accumulation bytargeting s4A. J. Hepatol. 57, 116-124.
Alpha1-Antitrypsin Deficiency Registry Study Group (1994). A registry of patientswith severe deficiency of alpha1-antitrypsin: Design and methods. Chest 106, 1223-1232.
Boglev, Y., Badrock, A. P., Trotter, A. J., Du, Q., Richardson, E. J., Parslow, A. C.,Markmiller, S. J., Hall, N. E., de Jong-Curtain, T. A., Ng, A. Y. et al. (2013).Autophagy induction is a Tor- and Tp53-independent cell survival response in azebrafish model of disrupted ribosome biogenesis. PLoS Genet. 9, e1003279.
Bouchecareilh, M., Hutt, D. M., Szajner, P., Flotte, T. R. and Balch, W. E. (2012).Histone deacetylase inhibitor (HDACi) suberoylanilide hydroxamic acid (SAHA)-mediated correction of α1-antitrypsin deficiency. J. Biol. Chem. 287, 38265-38278.
Brodsky, J. L. (2012). Cleaning up: ER-associated degradation to the rescue. Cell151, 1163-1167.
Burrows, J. A. J., Willis, L. K. and Perlmutter, D. H. (2000). Chemical chaperonesmediate increased secretion of mutant α 1-antitrypsin (α 1-AT) Z: A potentialpharmacological strategy for prevention of liver injury and emphysema in α 1-ATdeficiency. Proc. Natl. Acad. Sci. USA 97, 1796-1801.
Carlson, J. A., Rogers, B. B., Sifers, R. N., Finegold, M. J., Clift, S. M., DeMayo, F.J., Bullock, D. W. and Woo, S. L. (1989). Accumulation of PiZ alpha 1-antitrypsincauses liver damage in transgenic mice. J. Clin. Invest. 83, 1183-1190.
Crystal, R. G. (1990). Alpha 1-antitrypsin deficiency, emphysema, and liver disease.Genetic basis and strategies for therapy. J. Clin. Invest. 85, 1343-1352.
Cuvelier, A., Muir, J. F., Hellot, M. F., Benhamou, D., Martin, J. P., Bénichou, J. andSesboüé, R. (2000). Distribution of alpha(1)-antitrypsin alleles in patients withbronchiectasis. Chest 117, 415-419.
DeMeo, D. L., Campbell, E. J., Brantly, M. L., Barker, A. F., Eden, E., McElvaney, N.G., Rennard, S. I., Stocks, J. M., Stoller, J. K., Strange, C. et al. (2009). Heritabilityof lung function in severe alpha-1 antitrypsin deficiency. Hum. Hered. 67, 38-45.
Dickens, J. A. and Lomas, D. A. (2011). Why has it been so difficult to prove theefficacy of alpha-1-antitrypsin replacement therapy? Insights from the study ofdisease pathogenesis. Drug Des. Devel. Ther. 5, 391-405.
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
Clinical and basic research opportunities• Prevalence of liver and lung disease in adults with ATD• Identification of modifiers of ATD hepatic disease• Further elucidation of modifiers of ATD lung disease• Development of iPS cell line models to determine the mechanism of
action of modifiers and for personalized testing of novel therapeuticstrategies
• Screening of drug and RNAi libraries using the C. elegans model ofATD and computational pharmacological techniques for drugdiscovery
• Identification of biomarkers and design strategies for clinical trials ofnovel therapies
• Further studies of why AT replacement therapy does not have amore dramatic effect on the progression of lung disease due to ATD
• Further studies of the pathobiology of hepatocellular carcinoma inATD.
Dis
ease
Mod
els
& M
echa
nism
s

Ding, J., Yannam, G. R., Roy-Chowdhury, N., Hidvegi, T., Basma, H., Rennard, S.I., Wong, R. J., Avsar, Y., Guha, C., Perlmutter, D. H. et al. (2011). Spontaneoushepatic repopulation in transgenic mice expressing mutant human α1-antitrypsin bywild-type donor hepatocytes. J. Clin. Invest. 121, 1930-1934.
Dowson, L. J., Guest, P. J. and Stockley, R. A. (2001). Longitudinal changes inphysiological, radiological, and health status measurements in α(1)-antitrypsindeficiency and factors associated with decline. Am. J. Respir. Crit. Care Med. 164,1805-1809.
Engin, F. and Hotamisligil, G. S. (2010). Restoring endoplasmic reticulum function bychemical chaperones: an emerging therapeutic approach for metabolic diseases.Diabetes Obes. Metab. 12 Suppl. 2, 108-115.
Eriksson, S., Carlson, J. and Velez, R. (1986). Risk of cirrhosis and primary livercancer in alpha 1-antitrypsin deficiency. N. Engl. J. Med. 314, 736-739.
Gelling, C. L., Dawes, I. W., Perlmutter, D. H., Fisher, E. A. and Brodsky, J. L.(2012). The endosomal protein-sorting receptor sortilin has a role in trafficking α-1antitrypsin. Genetics 192, 889-903.
Gosai, S. J., Kwak, J. H., Luke, C. J., Long, O. S., King, D. E., Kovatch, K. J.,Johnston, P. A., Shun, T. Y., Lazo, J. S., Perlmutter, D. H. et al. (2010).Automated high-content live animal drug screening using C. elegans expressing theaggregation prone serpin α1-antitrypsin Z. PLoS ONE 5, e15460.
Hadzic, N., Quaglia, A. and Mieli-Vergani, G. (2006). Hepatocellular carcinoma in a12-year-old child with PiZZ α1-antitrypsin deficiency. Hepatology 43, 194.
Hidvegi, T., Schmidt, B. Z., Hale, P. and Perlmutter, D. H. (2005). Accumulation ofmutant α1-antitrypsin Z in the endoplasmic reticulum activates caspases-4 and -12,NFkappaB, and BAP31 but not the unfolded protein response. J. Biol. Chem. 280,39002-39015.
Hidvegi, T., Mirnics, K., Hale, P., Ewing, M., Beckett, C. and Perlmutter, D. H.(2007). Regulator of G Signaling 16 is a marker for the distinct endoplasmicreticulum stress state associated with aggregated mutant α1-antitrypsin Z in theclassical form of α1-antitrypsin deficiency. J. Biol. Chem. 282, 27769-27780.
Hidvegi, T., Ewing, M., Hale, P., Dippold, C., Beckett, C., Kemp, C., Maurice, N.,Mukherjee, A., Goldbach, C., Watkins, S. et al. (2010). An autophagy-enhancingdrug promotes degradation of mutant α1-antitrypsin Z and reduces hepatic fibrosis.Science 329, 229-232.
Janus, E. D., Phillips, N. T. and Carrell, R. W. (1985). Smoking, lung function, andalpha 1-antitrypsin deficiency. Lancet 325, 152-154.
Jonigk, D., Al-Omari, M., Maegel, L., Müller, M., Izykowski, N., Hong, J., Hong, K.,Kim, S.-H., Dorsch, M., Mahadeva, R. et al. (2013). Anti-inflammatory andimmunomodulatory properties of α1-antitrypsin without inhibition of elastase. Proc.Natl. Acad. Sci. USA 110, 15007-15012.
Kamimoto, T., Shoji, S., Hidvegi, T., Mizushima, N., Umebayashi, K., Perlmutter, D.H. and Yoshimori, T. (2006). Intracellular inclusions containing mutant α1-antitrypsin Zare propagated in the absence of autophagic activity. J. Biol. Chem. 281, 4467-4476.
Kim, W. J., Wood, A. M., Barker, A. F., Brantly, M. L., Campbell, E. J., Eden, E.,McElvaney, G., Rennard, S. I., Sandhaus, R. A., Stocks, J. M. et al. (2012).Association of IREB2 and CHRNA3 polymorphisms with airflow obstruction in severealpha-1 antitrypsin deficiency. Respir. Res. 13, 16.
Kruse, K. B., Brodsky, J. L. and McCracken, A. A. (2006). Characterization of anERAD gene as VPS30/ATG6 reveals two alternative and functionally distinct proteinquality control pathways: one for soluble Z variant of human α-1 proteinase inhibitor(A1PiZ) and another for aggregates of A1PiZ. Mol. Biol. Cell 17, 203-212.
Kyei, G. B., Dinkins, C., Davis, A. S., Roberts, E., Singh, S. B., Dong, C., Wu, L.,Kominami, E., Ueno, T., Yamamoto, A. et al. (2009). Autophagy pathway intersectswith HIV-1 biosynthesis and regulates viral yields in macrophages. J. Cell Biol. 186,255-268.
Larsson, C. (1978). Natural history and life expectancy in severe alpha1-antitrypsindeficiency, Pi Z. Acta Med. Scand. 204, 345-351.
Laurell, C.-B. and Eriksson, S. (1963) The electrophoretic α1-globulin pattern ofserum in. 1- antitrypsin deficiency. Scand. J. Clin. Lab. Invest. 15, 132-140.
Li, C., Xiao, P., Gray, S. J., Weinberg, M. S. and Samulski, R. J. (2011). Combinationtherapy utilizing shRNA knockdown and an optimized resistant transgene for rescueof diseases caused by misfolded proteins. Proc. Natl. Acad. Sci. USA 108, 14258-14263.
Liao, Y., Shikapwashya, O. N., Shteyer, E., Dieckgraefe, B. K., Hruz, P. W. andRudnick, D. A. (2004). Delayed hepatocellular mitotic progression and impaired liverregeneration in early growth response-1-deficient mice. J. Biol. Chem. 279, 43107-43116.
Mallya, M., Phillips, R. L., Saldanha, S. A., Gooptu, B., Brown, S. C., Termine, D.J., Shirvani, A. M., Wu, Y., Sifers, R. N., Abagyan, R. et al. (2007). Smallmolecules block the polymerization of Z α1-antitrypsin and increase the clearance ofintracellular aggregates. J. Med. Chem. 50, 5357-5363.
Marcus, N. Y., Brunt, E. M., Blomenkamp, K., Ali, F., Rudnick, D. A., Ahmad, M.and Teckman, J. H. (2010). Characteristics of hepatocellular carcinoma in a murinemodel of alpha-1-antitrypsin deficiency. Hepatol. Res. 40, 641-653.
Mueller, C., Tang, Q., Gruntman, A., Blomenkamp, K., Teckman, J., Song, L.,Zamore, P. D. and Flotte, T. R. (2012). Sustained miRNA-mediated knockdown ofmutant AAT with simultaneous augmentation of wild-type AAT has minimal effect onglobal liver miRNA profiles. Mol. Ther. 20, 590-600.
Pan, S., Huang, L., McPherson, J., Muzny, D., Rouhani, F., Brantly, M., Gibbs, R.and Sifers, R. N. (2009). Single nucleotide polymorphism-mediated translationalsuppression of endoplasmic reticulum mannosidase I modifies the onset of end-stage liver disease in alpha1-antitrypsin deficiency. Hepatology 50, 275-281.
Parr, D. G., Stoel, B. C., Stolk, J. and Stockley, R. A. (2004). Pattern of emphysemadistribution in α1-antitrypsin deficiency influences lung function impairment. Am. J.Respir. Crit. Care Med. 170, 1172-1178.
Pastore, N., Blomenkamp, K., Annunziata, F., Piccolo, P., Mithbaokar, P., MariaSepe, R., Vetrini, F., Palmer, D., Ng, P., Polishchuk, E. et al. (2013). Gene transferof master autophagy regulator TFEB results in clearance of toxic protein andcorrection of hepatic disease in alpha-1-anti-trypsin deficiency. EMBO Mol. Med. 5,397-412.
Perlmutter, D. H. (2011). Alpha-1 Antitrypsin Deficiency. In Schiff’s Diseases of theLiver (ed. E. R. Schiff, M. F. Sorrell and W. C. Maddrey), pp.845-867. Oxford: Wiley-Blackwell.
Piitulainen, E., Carlson, J., Ohlsson, K. and Sveger, T. (2005). α1-antitrypsindeficiency in 26-year-old subjects: lung, liver, and protease/protease inhibitorstudies. Chest 128, 2076-2081.
Piras, B., Ferrarotti, I., Lara, B., Martinez, M. T., Bustamante, A., Ottaviani, S.,Pirina, P., Luisetti, M. and Miravitlles, M. (2013). Clinical phenotypes of Italian andSpanish patients with α1-antitrypsin deficiency. Eur. Respir. J. 42, 54-64.
Qu, D., Teckman, J. H., Omura, S. and Perlmutter, D. H. (1996). Degradation of amutant secretory protein, α1-antitrypsin Z, in the endoplasmic reticulum requiresproteasome activity. J. Biol. Chem. 271, 22791-22795.
Rubinsztein, D. C., Mariño, G. and Kroemer, G. (2011). Autophagy and aging. Cell146, 682-695.
Rudnick, D. A. and Perlmutter, D. H. (2005). Alpha-1-antitrypsin deficiency: a newparadigm for hepatocellular carcinoma in genetic liver disease. Hepatology 42, 514-521.
Rudnick, D. A., Liao, Y., An, J.-K., Muglia, L. J., Perlmutter, D. H. and Teckman, J.H. (2004). Analyses of hepatocellular proliferation in a mouse model of α-1-antitrypsin deficiency. Hepatology 39, 1048-1055.
Sarkar, S., Perlstein, E. O., Imarisio, S., Pineau, S., Cordenier, A., Maglathlin, R.L., Webster, J. A., Lewis, T. A., O’Kane, C. J., Schreiber, S. L. et al. (2007). Smallmolecules enhance autophagy and reduce toxicity in Huntington’s disease models.Nat. Chem. Biol. 3, 331-338.
Sharp, H. L., Bridges, R. A., Krivit, W. and Freier, E. F. (1969). Cirrhosis associatedwith alpha-1-antitrypsin deficiency: a previously unrecognized inherited disorder. J.Lab. Clin. Med. 73, 934-939.
Shoji-Kawata, S., Sumpter, R., Leveno, M., Campbell, G. R., Zou, Z., Kinch, L.,Wilkins, A. D., Sun, Q., Pallauf, K., MacDuff, D. et al. (2013). Identification of acandidate therapeutic autophagy-inducing peptide. Nature 494, 201-206.
Sifers, R. N., Carlson, J. A., Clift, S. M., DeMayo, F. J., Bullock, D. W. and Woo, S.L. (1987). Tissue specific expression of the human alpha-1-antitrypsin gene intransgenic mice. Nucleic Acids Res. 15, 1459-1475.
Silverman, E. K. and Sandhaus, R. A. (2009). Clinical practice. Alpha1-antitrypsindeficiency. N. Engl. J. Med. 360, 2749-2757.
Stockley, R. A., Mannino, D. and Barnes, P. J. (2009). Burden and pathogenesis ofchronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 6, 524-526.
Sveger, T. (1976). Liver disease in alpha1-antitrypsin deficiency detected by screeningof 200,000 infants. N. Engl. J. Med. 294, 1316-1321.
Tan, S. H., Shui, G., Zhou, J., Li, J. J., Bay, B. H., Wenk, M. R. and Shen, H. M.(2012). Induction of autophagy by palmitic acid via protein kinase C-mediatedsignaling pathway independent of mTOR (mammalian target of rapamycin). J. Biol.Chem. 287, 14364-14376.
Tanash, H. A., Riise, G. C., Hansson, L., Nilsson, P. M. and Piitulainen, E. (2011).Survival benefit of lung transplantation in individuals with severe α1-anti-trypsindeficiency (PiZZ) and emphysema. J. Heart Lung Transplant. 30, 1342-1347.
Teckman, J. H. (2004). Lack of effect of oral 4-phenylbutyrate on serum alpha-1-antitrypsin in patients with alpha-1-antitrypsin deficiency: a preliminary study. J.Pediatr. Gastroenterol. Nutr. 39, 34-37.
Teckman, J. H. and Perlmutter, D. H. (2000). Retention of mutant α(1)-antitrypsin Z inendoplasmic reticulum is associated with an autophagic response. Am. J. Physiol.279, G961-G974.
Tsvetkov, A. S., Miller, J., Arrasate, M., Wong, J. S., Pleiss, M. A. and Finkbeiner,S. (2010). A small-molecule scaffold induces autophagy in primary neurons andprotects against toxicity in a Huntington disease model. Proc. Natl. Acad. Sci. USA107, 16982-16987.
Werner, E. D., Brodsky, J. L. and McCracken, A. A. (1996). Proteasome-dependentendoplasmic reticulum-associated protein degradation: an unconventional route to afamiliar fate. Proc. Natl. Acad. Sci. USA 93, 13797-13801.
Wu, Y., Whitman, I., Molmenti, E., Moore, K., Hippenmeyer, P. and Perlmutter, D.H. (1994). A lag in intracellular degradation of mutant alpha 1-antitrypsin correlateswith the liver disease phenotype in homozygous PiZZ alpha 1-antitrypsin deficiency.Proc. Natl. Acad. Sci. USA 91, 9014-9018.
Wynn, T. A. (2007). Common and unique mechanisms regulate fibrosis in variousfibroproliferative diseases. J. Clin. Invest. 117, 524-529.
Xia, H.-G., Zhang, L., Chen, G., Zhang, T., Liu, J., Jin, M., Ma, X., Ma, D. and Yuan,J. (2010). Control of basal autophagy by calpain1 mediated cleavage of ATG5.Autophagy 6, 61-66.
Yusa, K., Rashid, S. T., Strick-Marchand, H., Varela, I., Liu, P.-Q., Paschon, D. E.,Miranda, E., Ordóñez, A., Hannan, N. R. F., Rouhani, F. J. et al. (2011). Targetedgene correction of α1-antitrypsin deficiency in induced pluripotent stem cells. Nature478, 391-394.
Zhang, L., Yu, J., Pan, H., Hu, P., Hao, Y., Cai, W., Zhu, H., Yu, A. D., Xie, X., Ma, D.et al. (2007). Small molecule regulators of autophagy identified by an image-basedhigh-throughput screen. Proc. Natl. Acad. Sci. USA 104, 19023-19028.
Zhou, H. and Fischer, H. P. (1998). Liver carcinoma in PiZ alpha-1-antitrypsindeficiency. Am. J. Surg. Pathol. 22, 742-748.
Zhou, H., Ortiz-Pallardó, M. E., Ko, Y. and Fischer, H. P. (2000). Is heterozygousalpha-1-antitrypsin deficiency type PIZ a risk factor for primary liver carcinoma?Cancer 88, 2668-2676.
419
CLINICAL PUZZLE Disease Models & Mechanisms (2014) doi:10.1242/dmm.014092
Dis
ease
Mod
els
& M
echa
nism
s