Molecular Genetics of Sodium Channel Myotonias Michael Hanna CINCH NDM Meeting Kansas 3 June 2007...
30
Molecular Genetics of Sodium Channel Myotonias Michael Hanna CINCH NDM Meeting Kansas 3 June 2007 MRC Centre for Neuromuscular Disease Institute of Neurology Queen Square London
-
date post
18-Dec-2015 -
Category
Documents
-
view
223 -
download
2
Transcript of Molecular Genetics of Sodium Channel Myotonias Michael Hanna CINCH NDM Meeting Kansas 3 June 2007...

Molecular Genetics of Sodium Channel Myotonias
Michael Hanna
CINCH NDM Meeting Kansas 3 June 2007
MRC Centre for Neuromuscular Disease
Institute of Neurology
Queen SquareLondon

Overview
• Sodium channel gene
• Known phenotype-genotype links
• Review recent UK study of SCN4A gene and myotonia

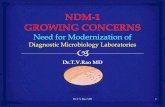
α-subunit Complete Ion channel without accessory subunits
++
++
++
++
Nav1.4
Cav1.1x1
COOH
I
IIIII
IV
NHCOOH
Kir2.1 x4
x2CLC-1
C
D
B
E F G HI J
K
L M NO
PQ
R
A
NH
COOH
+++
-
--
NH
I II III IV

Skeletal muscle Sodium channel gene
Chromosome 17q24 exons36 point mutations all missenseMultiple foundersImpaired inactivation
++
++
++
++

Phenotype Common genotype
• Hypo PP R672H/G/S• Hyper PP T704M• K sensitive normoPP R675G/Q/W• HyperPP/PC R1448C/H• Cold induced HypoPP/myt P1158S• Paramyotonia congenita T1313A/M• Painful cong myotonia V445M• PAM-MF MP G1306A/V/E

Queen Square PP Database
Genetically defined June 2007:
• CACNA1S 26 R528H 34 R1239H
1 R1239G
• SCN4A 40 T704M13 M1592V 4 R675G 1 R672S

SCN4A genotype-phenotype
40 T704M HyperPP+/- myt
13 M1592V HyperPP+/- myt
4 R675G K sens-Normo
1 R672S HypoK

UK study Sodium channel Myotonia
• Aim –identify a sodium channel myotonia cohort
• Source-UK NSCAG Clinical database muscle channelopathies
• Inclusion criteria- “relaxed”Paramyotonia Prominent history cold exacerbation +/-weaknessEMG myotonia
• DM1 /DM2 excluded
• SCN4A automated DNA analysis and detailed clinical analysis of mutation positive vs negative cases

UK study Sodium channel Myotonia
• 39 cases identified
27 exon 22/exon 24 12 SCN4A neg
3/27 PAM mts 2/27 new mts
2/12 T704M 1/12 new mts

Mutation Reported Phenotypes Phenotypes in UK Cohort Frequency in UK cohort (patients/kindred)
Q270K**** PMC PMC 1/1
T704M HyperPPHyperPP/PMC
HyperPP/PMC 2/1
G1306A PAM (MF) PMC/PAM 2/1
G1306E PAM (MP) PMC/PAM 1/1
T1313M PMC PMC 10/6
R1448C PMCHyperPP/PMC
PMCHyperPP/PMC
4/2
R1448H PMCHyperPP/PMC
PMCHyperPP/PMC
2/2
R1448L**** - PMC 1/1
G1456E PMC PMC 3/1
F1473S PMC PMC 1/1 [3/1]
V1589M PAM PMC
PMC 2/1
L1436P**** - PMC 1/1

PAM mutations PMC clinical phenotype
• G1306E Myotonia Permanens
• G1306A Myotonia Fluctuans
• Clinical impression vs EMG criteria

Mutation Frequency in our cohort (patients/kindred)
***Q270K 1/1*** D1-S5
T704M 2/1
G1306A 2/1
G1306E 1/1
T1313M 10/6
R1448C 4/2
R1448H 2/2
***R1448L 1/1*** D4-S4
G1456E 3/1
F1473S 1/1
V1589M 2/1
***L1436P 1/1 **** D4-S4
{I693T 1/1}

R1448L
• Typical PMC
• Paramyotonia
• Cold exacerbation myotonia
• Cold induced weakness
• Additional features – sensorineural deafness, generalised chorea ?unrelated


I693T
L1436P

L1436P
• PMC phenotype
• Newcastle
• Myositis-immunosuppression
• Coincidence?/ other cases

I693T
L1436P

I693T
L1436P

Q270K
• PMC
• Marked pain
• Domain I mutations and pain?
• Treatment resistant


I693T
L1436P

Mutation “negative” cases
• Clear paramyotonia with cold exacerbation• Older age at onset• Prominent painful myotonia• Upper and lower limbs equally affected• Fixed weakness
? Additional SCN4A mutations, ?CLCN1? Non-genetic phenocopies

Summary
• Exon 22/24 hotspot for PMC mutations DNA screening strategy
• Extending SCN4A analysis 75% hit rate
• Clinical distinction between PAM-PMC not always easy ? Genetic overlap cf EMG
• ? Further heterogeneity associated with PMC phenotype

Ion Channel GroupQueen Square
Research NSCAG Service Doreen Fialho Veronica Tann Susie Tomlinson Martin KoltzenburgDimitri Kullmann Emma StanleyNick Wood Cath Woodward
Mary DavisSanj Rajakulendran Mary SweeneyEmma Matthews Dennis StevensStephanie Schorge Andrew HaworthTracey GravesHugh Bostock Funding Support
MRC, Wellcome Trust, ERF, BRT,ULCH-NHS Trust Special Trustees DoH NSCAG. Action Research, CINCH



Copyright ©2005 American Society for Clinical Investigation
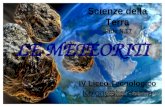
Inherited mutations alter ion channel function and structure and cause human disease

Periodic Paralysis
Nondystrophic Myotonias
Hypo-kalaemic
PP
Hyper-kalaemic
PP
Myotonia congenita
Paramyotoniacongenita
AndersenTawil
Syndrome
VG skeletal muscle Na+ channel Nav1.4 (SCN4A)
VG Ca2+ channel (Dihydropyridine receptor) Cav1.1 (CACNA1S)
VG skeletal muscle Cl- channel CLC-1 (CLCN1)
Inward rectifying K+ channel Kir 2.1 (KCNJ2)
Clinical
Classification
Molecular
Classification

Skeletal muscle Na+ channel NaV1.4