Low molecular weight heparin-induced increase in chylomicron-remnants clearance, is associated with...
5
Regular Article Low molecular weight heparin-induced increase in chylomicron-remnants clearance, is associated with decreased plasma TNF-α level and increased hepatic lipase activity Itamar Grosskopf a,b, ⁎, Aviv Shaish a , Assaf Ray a,b , Dror Harats a,c , Yehuda Kamari a,c a The Bert Strassburger Lipid Center, Sheba Medical Center, Tel Hashomer, Israel b Department of Medicine, Tel Aviv-Sourasky Medical Center, Tel Aviv, Israel c Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel abstract article info Article history: Received 24 July 2013 Received in revised form 17 December 2013 Accepted 15 January 2014 Available online 21 January 2014 Keywords: Post-prandial lipemia Insulin sensitivity Inflammation Objective: The acute effect of heparin on lipoprotein clearance is well characterized. Yet, the effect of prolonged low-molecular-weight-heparin (LMWH) administration on post-prandial lipemia has remained so far unex- plored. Recent reports suggest that LMWH could modify lipid and carbohydrate metabolism by diminishing TNFα-mediated inflammatory response. This, together with the known negative effect of TNF-α on insulin sen- sitivity, prompted us to hypothesize that LMWH would favorably affect post-prandial lipoprotein disposal. Methods: Twenty four patients were given a vitamin A-fat loading meal at the end of 6-week enoxaparin treat- ment and after 3-month washout period. Post-prandial lipemia was assessed by measuring retinyl-palmitate (RP) during 8 hours following the meal. Insulin sensitivity index (ISI), plasma lipolytic activity and plasma TNF-α were measured. Results: Enoxaparin did not impact fasting plasma lipids and lipoproteins levels. Enoxaparin increased RP clear- ance in the chylomicron remnant (CMR) fraction by 32% (P b 0.01). Additionally, enoxaparin decreased plasma TNF-α by 22% (P b 0.01), increased hepatic lipase (HL) activity by 81% (P b 0.01), along with a 2-fold increase in ISI (P b 0.01). The decrease in CMR correlated with the reduction in TNFα and the increase in ISI and HL activity (R = 0.48, -0.68, -0.56, respectively, p b 0.05). Significant correlations were also found between the reduction in TNFα and both the increase in ISI and increase in HL activity (R = -0.43, -0.54, respectively, P b 0.05). Conclusions: The association of the effect on post-prandial metabolism, plasma TNFα level and HL activity during prolonged enoxaparin treatment may support the hypothesis that the beneficial outcome of enoxaparin may possibly be linked to anti-inflammatory and lipase-potentiating impact. © 2014 Elsevier Ltd. All rights reserved. Introduction A substantial proportion of patients with coronary artery disease (CAD) manifest an array of metabolic abnormalities, including glucose intolerance, low high-density lipoprotein cholesterol, increased small dense low-density lipoprotein (LDL) particles, and exaggerated post- prandial lipemia. Insulin resistance was implicated as the pivotal player in the emergence of this cluster [1]. Intestinally-derived triglyceride- rich lipoproteins (TRL) i.e. chylomicrons (CM) and chylomicron remnants (CMR) make up a significant part of post-prandial lipemia. Unlike CM and large very-low-density lipoprotein (VLDL) particles, CMR are able to migrate through the endothelial layer and enter the subintimal space [2,3] where they promote the formation of athero- sclerotic plaques [4]. One remnant particle that enters the intima, de- livers from 5- to 20-fold more cholesterol than each LDL particle, and is therefore considered more atherogenic [5]. During the past 3 de- cades, a substantial body of evidence has accumulated supporting the role of intestinally-derived TRL in the pathogenesis of atheroscle- rosis [6,7]. Indeed, several studies recently demonstrated the associ- ation of post-prandial lipemia with increased risk for CAD [8–10]. In many cases, heparin is included in the standard treatment proto- col for CAD and a plethora of other surgical and medical conditions [11]. The lipolytic effect of acute intravenous administration of heparin was established some 50 years ago when it was shown that heparin dis- places lipoprotein lipase from the endothelium [12]. Evidence from recent trials strongly support the preferential use of low molecular weight heparin (LMWH) in a variety of clinical settings including Thrombosis Research 133 (2014) 688–692 Abbreviations: AUC, area under the curve; CAD, coronary artery disease; CM, chylomi- cron; CMR, chylomicron remnants; HL, hepatic lipase; hsCRP, high sensitive C-reactive protein; ISI, insulin sensitivity index; LDL, low density lipoprotein; LMWH, low molecular weight heparin; LPL, lipoprotein lipase; RP, retinyl palmitate; TNF-α, tumor necrosis factor alpha; TRL, triglyceride rich lipoprotein; VLDL, very low density lipoprotein. ⁎ Corresponding author at: The Bert Strassburger Lipid Center, Sheba Medical Center, Tel Hashomer 52621, Israel. Tel.: +972 35302939, +972 52 260 6060 (mobile); fax: +972 35304431. E-mail address: [email protected] (I. Grosskopf). 0049-3848/$ – see front matter © 2014 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.thromres.2014.01.019 Contents lists available at ScienceDirect Thrombosis Research journal homepage: www.elsevier.com/locate/thromres
Transcript of Low molecular weight heparin-induced increase in chylomicron-remnants clearance, is associated with...

Thrombosis Research 133 (2014) 688–692
Contents lists available at ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r .com/ locate / th romres
Regular Article
Low molecular weight heparin-induced increase inchylomicron-remnants clearance, is associated with decreased plasmaTNF-α level and increased hepatic lipase activity
Itamar Grosskopf a,b,⁎, Aviv Shaish a, Assaf Ray a,b, Dror Harats a,c, Yehuda Kamari a,c
a The Bert Strassburger Lipid Center, Sheba Medical Center, Tel Hashomer, Israelb Department of Medicine, Tel Aviv-Sourasky Medical Center, Tel Aviv, Israelc Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Abbreviations: AUC, area under the curve; CAD, coronacron; CMR, chylomicron remnants; HL, hepatic lipase; hprotein; ISI, insulin sensitivity index; LDL, low density lipoweight heparin; LPL, lipoprotein lipase; RP, retinyl palmitaalpha; TRL, triglyceride rich lipoprotein; VLDL, very low d⁎ Corresponding author at: The Bert Strassburger Lipid
Tel Hashomer 52621, Israel. Tel.: +972 35302939, +9+972 35304431.
E-mail address: [email protected]
0049-3848/$ – see front matter © 2014 Elsevier Ltd. All rihttp://dx.doi.org/10.1016/j.thromres.2014.01.019
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 24 July 2013Received in revised form 17 December 2013Accepted 15 January 2014Available online 21 January 2014Keywords:Post-prandial lipemiaInsulin sensitivityInflammation
Objective: The acute effect of heparin on lipoprotein clearance is well characterized. Yet, the effect of prolongedlow-molecular-weight-heparin (LMWH) administration on post-prandial lipemia has remained so far unex-plored. Recent reports suggest that LMWH could modify lipid and carbohydrate metabolism by diminishingTNFα-mediated inflammatory response. This, together with the known negative effect of TNF-α on insulin sen-sitivity, prompted us to hypothesize that LMWHwould favorably affect post-prandial lipoprotein disposal.Methods: Twenty four patients were given a vitamin A-fat loading meal at the end of 6-week enoxaparin treat-ment and after 3-month washout period. Post-prandial lipemia was assessed by measuring retinyl-palmitate(RP) during 8 hours following the meal. Insulin sensitivity index (ISI), plasma lipolytic activity and plasmaTNF-α were measured.
Results: Enoxaparin did not impact fasting plasma lipids and lipoproteins levels. Enoxaparin increased RP clear-ance in the chylomicron remnant (CMR) fraction by 32% (P b 0.01). Additionally, enoxaparin decreased plasmaTNF-α by 22% (P b 0.01), increased hepatic lipase (HL) activity by 81% (P b 0.01), along with a 2-fold increase inISI (P b 0.01). The decrease in CMR correlated with the reduction in TNFα and the increase in ISI and HL activity(R= 0.48, -0.68, -0.56, respectively, p b 0.05). Significant correlationswere also found between the reduction inTNFα and both the increase in ISI and increase in HL activity (R = -0.43, -0.54, respectively, P b 0.05).Conclusions: The association of the effect on post-prandial metabolism, plasma TNFα level and HL activity duringprolonged enoxaparin treatment may support the hypothesis that the beneficial outcome of enoxaparin maypossibly be linked to anti-inflammatory and lipase-potentiating impact.© 2014 Elsevier Ltd. All rights reserved.
Introduction
A substantial proportion of patients with coronary artery disease(CAD) manifest an array of metabolic abnormalities, including glucoseintolerance, low high-density lipoprotein cholesterol, increased smalldense low-density lipoprotein (LDL) particles, and exaggerated post-prandial lipemia. Insulin resistance was implicated as the pivotal playerin the emergence of this cluster [1]. Intestinally-derived triglyceride-rich lipoproteins (TRL) i.e. chylomicrons (CM) and chylomicron remnants
ry artery disease; CM, chylomi-sCRP, high sensitive C-reactiveprotein; LMWH, lowmolecularte; TNF-α, tumor necrosis factorensity lipoprotein.Center, Sheba Medical Center,
72 52 260 6060 (mobile); fax:
(I. Grosskopf).
ghts reserved.
(CMR)make up a significant part of post-prandial lipemia. Unlike CMand large very-low-density lipoprotein (VLDL) particles, CMR areable to migrate through the endothelial layer and enter thesubintimal space [2,3] where they promote the formation of athero-sclerotic plaques [4]. One remnant particle that enters the intima, de-livers from 5- to 20-fold more cholesterol than each LDL particle, andis therefore considered more atherogenic [5]. During the past 3 de-cades, a substantial body of evidence has accumulated supportingthe role of intestinally-derived TRL in the pathogenesis of atheroscle-rosis [6,7]. Indeed, several studies recently demonstrated the associ-ation of post-prandial lipemia with increased risk for CAD [8–10].
In many cases, heparin is included in the standard treatment proto-col for CAD and a plethora of other surgical andmedical conditions [11].The lipolytic effect of acute intravenous administration of heparin wasestablished some 50 years ago when it was shown that heparin dis-places lipoprotein lipase from the endothelium [12]. Evidence fromrecent trials strongly support the preferential use of low molecularweight heparin (LMWH) in a variety of clinical settings including

689I. Grosskopf et al. / Thrombosis Research 133 (2014) 688–692
acute coronary syndrome [13–16]. The few works that investigated theeffect of LMWH on lipolysis were carried out uniquely on patients un-dergoing hemodialysis. This is exceedingly remote from the vast major-ity of clinical settings in which LMWH is administered for preventiveand therapeutic purposes. Hence, characterization the effect of LMWHon plasma lipids and lipoproteins in setting other than hemodialysismay add important information on the action of this commonly usedmedication. Additionally, since prolonged circulatory residence time ofintestinally-derived TRL was shown to be associated with CAD even iffasting lipids were within normal limits [8] we reasoned that exploringthe role of LMWH in metabolism of post-prandial lipemia may providesome clinically relevant novel data.
Recently, LMWHwas reported to attenuate inflammation [17] and afew in vitro and in vivo studies showed that it decreased plasma level ofthe proinflammatory cytokine TNFα [18–21]. The crucial role of TNFα indeterioration of insulin resistance is well documented [22]. Notably,Skoog et al. showed that plasma TNFα level were associated with ahigher degree of alimentary lipemia, increased plasma VLDL triglyc-erides, and insulin resistance [23]. The recent reports on the favorableeffects of LMWH on inflammation and particularly on TNFα, led us tohypothesize that by decreasing TNFα level, LMWH may expedite post-prandial lipoprotein catabolism. The scarce data on the effect ofLMWH on plasma lipids/lipoproteins prompted us to test this hypothe-sis by challenging patients with a fatty meal during and subsequent toenoxaparin treatment in order to monitor the kinetics of intestinally-derived TRL clearance and TNFα level.
Methods
Patients
The institutional ethical committee approved the study protocol,and participants gave written informed consent before entering thestudy. Consecutive patients undergoing coronary catheterization wereasked to participate in the current study if their angiogramwas normal,i.e. there was no indication for revascularization. Specifically, up to7 days after patients had first presented with clinical manifestationsuggestive of anginal syndrome and were started on subcutaneousenoxaparin, they underwent coronary catheterization. Patients withnormal coronary arteries or non-significant CADwere asked to continuesubcutaneous enoxaparin 1 mg/kg/day for 6 additional weeks while allmedications but enoxaparin were discontinued.
Patientswere included in the study if their fasting blood glucosewasless than 6 mmol/l, fasting total cholesterol and triglyceride levels wereless than 6.2 and 2.3 mmol/l, respectively, and if they had no clinical andbiochemical evidence of liver, kidney or endocrine disease. Patientswere excluded if they had acute coronary event, overt heart failure,bleeding diathesis, were treated with statins, calcium channel blockersor ACE inhibitors. At the end of a 6-week treatment period with subcu-taneous enoxaparin, participants underwent laboratory tests, includingfasting glucose, fasting lipid profile and a standard glucose tolerance testfollowed by a vitamin A-fat loading test. A second set of laboratory tests,an oral glucose tolerance test and vitamin A-fat loading was performed3 months after the end of enoxaparin treatment. Participants weredischarged from the hospitalwithin 48 hours of initiation of enoxaparinand were instructed to resume their normal daily activity and regularnutrition within the following 3 days.
Vitamin A-fat Loading Test
Vitamin A-fat loading test was performed as previously described[24]. Briefly, after a 12-h overnight fasting, the subjects ate a fattymeal plus 60,000 U of aqueous vitamin A/m2 body surface. The fattymeal contained 50 g of fat/m2 body surface, consisting of 65% caloriesas fat, 20% as carbohydrate and 15% as protein. It contained 600 mgcholesterol/1000 calories, and the P/S ratio was 0.3. This was given as
a milkshake, scrambled eggs, bread, and cheese, and was consumed in10 min. The vitamin A was added to the milk shake. After the meal thesubjects fasted for 8 h, but drinking water as desired was allowed.Blood samples were drawn before the meal, 1, 2, 3, 4, 5, 6 and 8 hafter the meal. Vitamin A is known to specifically label intestinally de-rived TRL with retinyl palmitate (RP).
Analysis of Samples
Isolation of lipoproteins and the RP assay were performed as de-scribed elsewhere [24].
Lipid and Lipoprotein Determinations
Cholesterol and triglycerides were measured enzymatically usingthe reagents cholesterol 236991 and triglyceride 126012 (BoehringerMannheim, Indianapolis, IN, USA). HDL-cholesterol was determinedafter precipitation of whole plasma with dextran sulfate magnesium.LDL-cholesterol concentration was calculated using the Friedewald’sequation.
Determination of Lipase Activity
Lipase activity was measured prior to glucose tolerance test accord-ing to Nilsson-Ehle and Schotz [25]. Briefly, [9,10-3H]-Triolein(American Radiolabeled Chemicals, Inc. Saint Louis, MO, USA) wasmixed with unlabeled triolein (600 mg; 2500 X 106 cpm) and lecithin(36 mg) was added. After evaporation of the solvents emulsification inglycerol (10mL)was carried out by homogenization on ice. Immediate-ly before the assay substrate was diluted in 4 volumes of 0.2M Tris–HClbuffer (pH 8.0) containing 3% bovine serum albumin (essentially freefrom fatty acid). Incubation at 37 °C was started by addition of 0.1 mLof pre- or post-heparin plasma to 0.1 mL substrate. After 20 minutesthe reactions were stopped by addition of methanol-chloroform-heptane 1.41: 1.25: 1 (3.25 ml) followed by 1.0 mL of 0.1 M potassiumcarbonate-borate buffer (pH 10.5). After vigorous mixing, the tubeswere centrifuged for 15 min at 3000 g. A 1-mL aliquot of themethanol–water upper phase was counted to determine the [3H]-oleicacid released. This assay measured total plasma lipolytic activity.Preincubation of plasma samples with anti-hepatic lipase monoclonalantibody (XHL1-1C, cat # sc-21741, Santa Cruz Biotechnology, Inc.,Santa Cruz, CA, USA) diluted 1:500 (10 μL/sample) at 0 °C for 1 hourto inactivate HL, selectivelymeasured LPL activity. HL activitywas calcu-lated as the difference between total plasma activity and activity mea-sured in the presence of the antibody. To validate the inhibitory effectof XHL1-1C antibody, HL activity was measured in normal plasmaafter inactivation of LPL either by removal of apoCII from the assaymix-ture or by incubation of plasma samples in 1 M NaCl (for 10 minutes at0 °C). Preincubation of samples with XHL1-1C anti-hepatic lipase anti-body decreased HL activity in these assays to less than 3% of initial activ-ity. We considered this to be complete inactivation of HL by theantibody. Assays with XHL1-1C antibody had intra-assay coefficient ofvariation of 2%-3% and inter-assay coefficient of variation of 5%-8%.
Determination of Blood Glucose and Insulin
Glucose levels were measured using an enzymatic kit (number315–100; Sigma-Aldrich). Plasma insulin concentration was measuredby radioimmunoassay using a commercial kit (SRI-13 K) obtainedfrom Linco Research (St. Charles, MO, USA). The insulin sensitivityindex (ISI) was calculated according to Matsuda and DeFronzo [26],i.e., 10,000/square root of (fasting glucose x fasting insulin) x (meanglucose x mean insulin during the oral glucose tolerance test).

690 I. Grosskopf et al. / Thrombosis Research 133 (2014) 688–692
Determination of Plasma TNFα and C Reactive Protein
Plasma TNFα and C Reactive Protein (CRP) levels were measuredusing Human TNF ELISA KIT II (Cat. No. 550610, BD OptEIA™) andhigh-sensitivity CRP (hs-CRP) test (microparticle enhanced nephelom-etry, BN, Dade-Behring, Germany).
Statistical Analysis
Calculating sample size found that a group size of 22–26 participantswould have 80% power to detect a 35% change at 2-tailed significancelevel of 0.05. Values are expressed asmean± standard error (SE) unlessindicated otherwise. The differences of fasting lipids and the size of thepost-prandial lipid and lipoprotein fractions (by using the trapezoidalrule to calculate the area under the triglyceride curve (AUC) in thewhole plasma, in the CM and in the CMR fractions, and by calculatingthe area under the RP curves in the whole plasma, the CM fraction andthe CMR fraction) between the treatment phase (with enoxaparin)and the non-treatment phase (without enoxaparin) were analyzed forsignificance using the paired-t, Mann–Whitney and Wilcoxon signedrank tests. Independent effects of TNFα, lipase activity and insulin sen-sitivity on AUC of RP in the post-prandial lipoprotein fractions wereassessed by evaluating the relations of the differences in parameters be-tween the treatment and the non-treatment phases using the Pearson’scorrelation coefficient and Spearman rho tests. To test for non-independent effects of TNFα, lipase activity and insulin sensitivity onAUC of RP in the post-prandial lipoprotein fractions, the differences inparameters between the treatment and the non-treatment phaseswere entered in a multiple linear regression model. A P value of lessthan 0.05 was considered significant.
Results
Twenty four patients were enrolled into the study. Participants tol-erated themeal well, and none had diarrhea or other symptoms ofmal-absorption. None of the participants reported any adverse effect duringenoxaparin administration. Participants (13males and 11 female) were55.3 ± 5.9 years old and had a BMI of 25 ± 4 kg/m2.
Enoxaparin treatment had no impact on fasting lipids level aswell asfasting glucose level (Table 1). As expected, enoxaparin treatmentlowered plasmaTNFα level by 22% (P b 0.01, Table 1). Enoxaparin treat-ment was accompanied by a mean 44% decrease in CRP level (p b 0.01,Table 1). Since members of affluent societies spent most of their lives inthe post-prandial state and in view of the fact that post-prandial lipo-proteins were shown to be atherogenic and their plasma level reflectsindividual's capacity to cope with oral caloric burden, we measured in
Table 1Salient characteristics of the study group and effect of enoxaparin on fasting parameters.
Without Enoxaparin With Enoxaparin P
Age 55.3 ± 5.9⁎BMI (kg/m2) 25 ± 3 25 ± 4 NSFasting Glucose (mmol/l) 5.8 ± 1.2 5.5 ± 0.8 NSFasting Insulin (pmol/l) 159.0 ± 27.0 105.5 ± 68.0 b0.01Fasting G:I ratio 5.8 ± 0.8 12.0 ± 3.7 b0.01ISI 7.7 ± 1.3 15.3 ± 3.9 b0.01Fasting total cholesterol (mmol/l) 5.7 ± 0.64 5.8 ± 1.0 NSFasting triglycerides (mmol/l) 1.2 ± 0.44 1.29 ± 0.37 NSFasting LDL-cholesterol (mmol/l) 3.8 ± 0.67 4.0 ± 1.0 NSFasting HDL- cholesterol (mmol/l) 1.1 ± 0.23 1.1 ± 0.13 NSHs CRP (nmol/l) 135.4 ± 35.8 75.6 ± 31.8 b0.01TNFα (fmol/l) 359.0 ± 40.0 281.0 ± 23.0 b0.01Hepatic lipase (u/l) 249 ± 45 452 ± 59 b0.01Lipoprotein lipase (u/l) 156 ± 36 177 ± 32 NS
⁎ , values are mean ± SD; NS, non-significant; BMI, body mass index; G:I, glucose to in-sulin ratio, ISI, insulin sensitivity index32, LDL, low-density lipoprotein; HDL, high-densitylipoprotein; Hs CRP, high sensitive C Reactive Protein.
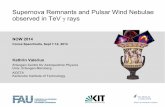
this work post-prandial triglyceride and RP (a marker for ingestedcholesterol) in the whole plasma as well as in CM (Sf N 1000) andCMR (Sf b 1000) fractions. Enoxaparin treatment was associated witha 22% decrease in the area under the triglycerides curve measured inthe whole plasma (p = 0.038, Table 2) and 27% in the CMR fraction(p = 0.023, Table 2). The area under the RP curve in the whole plasmawas 28% lower (p= 0.029, Table 2, Fig. 1) and in the CMR fraction - 32%lower (p b 0.01, Table 2, Fig. 1) during enoxaparin treatment comparedto the non-treatment phase. The decrement in the AUC of RP in the CMRfractionwas strongly related to the decrease in plasma TNFα level (R=0.48, p = 0.02). However, TNFα is not an established modulator ofpostprandial lipoprotein metabolism. To look into a possible mecha-nism for the enhanced catabolism of post-prandial lipoproteins byenoxaparin, wemeasured plasma post-heparin lipolytic activity. HL ac-tivity increased by 81% (P b 0.01, Table 1) during enoxaparin adminis-tration. The increment in HL activity significantly correlated with thedecrement in the AUC of RP in the CMR fraction (R = −0.56, p =0.02). Since insulin sensitivity is considered a key modulator of lipo-protein metabolism in the post-prandial phase, we assessed the effectof enoxaparin on insulin sensitivity. While mean fasting glucose wasnot affected by enoxaparin therewas a 34% decrease inmean fasting in-sulin during enoxaparin treatment (p b 0.01, Table 1), and a 2-fold in-crease in both fasting glucose to insulin ratio and ISI associated withenoxaparin administration (p b 0.01, Table 1). Therewas a robust corre-lation between the increase in ISI and the decrease in the AUC of RP inthe CMR fraction (R = −0.68, p = 0.01). Entering delta values (Δ =difference between values with and without treatment) of area underthe RP curve in the CMR fraction as the dependent variable and Δ ofTNFα, ISI and HL as the independent variables into a multivariate linearregression model gave a joint predictive power (R2) of 0.68 with a 0.01overall significance level. ΔISI and ΔHL were significant predictors of Δarea under the RP curve of the CMR fraction both with β-coefficient of0.46 (significance level of 0.05 for ΔISI, and 0.04 for Δ HL). ΔTNFα hadβ-coefficient of 0.38 at significance level of 0.09. Although the relationin this model does not imply causation, the high p value for TNFαmeans that TNFα does not affect the area under the RP curve of theCMR fraction. TNFα rather acts via change in either ISI or HL or both.Indeed there were significant correlations between ΔTNFα and ΔISI(R = −0.43, p = 0.04) and between ΔTNFα and ΔHL (R = −0.54,p = 0.02).
Discussion
The present study demonstrates that the LMWHenoxaparin acceler-ates the clearance of lipoproteinswithin theCMR fraction. In thepresentwork, the decrease in CMR was associated with a decrease in plasmaTNFαwhich in turn positively correlated with an increase in both insu-lin sensitivity and augmentation in HL activity.
Catabolism of intestinally derived TRL follows twomajor steps. First,large (up to 1200 nm) CM particles (that are formed in the intestinalwall from ingested lipids) are increasingly loaded with cholesterol es-ters as their core triglycerides are being hydrolyzed [27] in the circula-tion; they thus diminish in size and become CMR. Subsequently, CMRare rapidly removed from the circulation mainly by liver uptake via he-patocyte receptors that recognize apoE [27]. Based on the pivotal rolethat LPL and HL play in these two steps, respectively [27], we examinedthe effect of enoxaparin on plasma lipolytic activity. Enoxaparin treat-ment in the presentworkwas associatedwith an increase in HL activity.HL specifically facilitates the uptake of CMR in the liver by hydrolyzingtheir core triglycerides and surface phospholipids [4]. As a result, thesemacromolecules further diminish in size (30–50 nm) such that theycan enter the space of Disse [4], where they sequester and undergo en-docytosis. Additionally, HL bridges remnant particles to heparan sulfateproteoglycans on the hepatocyte surface, thus further facilitating theirtransfer to LDL receptor and LDL receptor-related protein [5]. It followsthat the increased activity of HL during enoxaparin treatment might

Table 2The effect of enoxaparin on post-prandial lipemia.
Without Enoxaparin With Enoxaparin P
Area under Triglyceride Curve (mmol · l-1 · h) Whole Plasma 21.5 ± 1.9⁎ 16.8 ± 1.0 0.038Chylomicrons Fraction(Sf N 1000)
14.1 ± 2.4 11.1 ± 1.5 0.3
Chylomicron Remnant Fraction (Sf b 1000) 5.9 ± 0.6 4.3 ± 0.4 0.023Area under RP Curve (μmol/l-1 · h) Whole Plasma 60.0 ± 6.7 43.0 ± 2.9 0.029
Chylomicrons Fraction(Sf N 1000)
43.1 ± 6.0 31.6 ± 3.0 0.1
Chylomicron Remnant Fraction (Sf b 1000 17.0 ± 1.6 11.5 ± 0.9 b0.01
⁎, values are mean ± SE; RP; retinyl palmitate.
691I. Grosskopf et al. / Thrombosis Research 133 (2014) 688–692
well have contributed to the accelerated clearance of CMR. This is sup-ported by the positive correlation between the increase in plasma HLactivity and the decrease in the area under the RP curve in the CMR frac-tion during enoxaparin treatment.
To further understand possible mechanisms whereby enoxaparinbeneficially affects lipoprotein catabolism, we determined insulin sensi-tivity and plasma TNFα levels.We assessed plasma TNFα levels becausethere have been recently a few reports that convincingly demonstratedLMWH to alter plasma TNFα [18–21]. Insulin sensitivity was measuredsince it is a powerful determinant of TRLmetabolism [28] and because ithas been recently reported to be markedly modified by TNFα [29].Indeed, we found that fasting plasma TNFα levels were significantlylower during enoxaparin treatment and remained lower after the fatloading meal (data not shown). Moreover, there was a strong correla-tion between the decrement in fasting plasma TNFα levels and thedecrease in the AUC of RP in the CMR fraction, supporting a role for de-creased TNFα in enhancing the clearance of CMR cholesterol as a resultof enoxaparin treatment. Further support for this possibility came fromthe correlation between the decrement in TNFα and the increment inHL activity. It follows that a possible indirect effect of LMWHto augmentHL activity i.e. via TNFα, as shown bymultiple linear regression analysis,may be considered even if an explicit mechanism remains to beelucidated.
The molecular mechanism whereby LMWH diminishes plasmaTNFα level has not been fully clarified. It has been, however, shown
Fig. 1. Post- fat load retinyl palmitate (A, B) and triglyceride (C,D) curves in whole plasma (A, CEnoxaparin (open circles).
that disaccharide molecules do not neutralize TNFα but affect the pro-duction of this cytokine [30]. Determiningwhether TNFα directly affect-ed HL [31] or whether HL was actually modified by interleukin-1 [7], apro-inflammatory cytokine that tends to co- fluctuate with TNFα, wasbeyond the scope of this work.
Our current results show that insulin sensitivity increased withenoxaparin treatment. Although euglycemic insulin clamp is widelyaccepted as the gold standard for assessing insulin sensitivity, we feltthat the index (ISI) devised byMatsuda and DeFronzo [26] was a robustsurrogate for assessing insulin sensitivity. TNFα is an accepted inducerof insulin resistance [29]. The association of TNFαwith increased insulinresistance was reinforced by data from the Insulin Resistance Athero-sclerosis Study [32]. Noteworthy, TNFα has been shown to induce ser-ine phosphorylation of insulin receptor substrate 1 with subsequentresistance to insulin-stimulated tyrosine phosphorylation [33]. The re-sult is impairment in insulin-stimulated glucose transport [34]. Hence,it is reasonable to assume that the enoxaparin-induced decrease in plas-ma TNFα levels contributed to the increase in insulin sensitivity. A sup-port for this came from the significant correlation between the changesin plasma TNFα levels and ISI. The notion that reduction of insulin resis-tance is instrumental in enhancing the removal of CMR is supported bythe significant correlation between the increment in ISI and the decre-ment in CMR levels with enoxaparin treatment. Increased removal ofCMR as a consequence of improved insulin sensitivity is in agreementwith a previous report [35].
) and chylomicron remnants fraction (B, D) with Enoxaparin (closed circles) and without

692 I. Grosskopf et al. / Thrombosis Research 133 (2014) 688–692
However, our results suggest that enhanced insulin sensitivity dur-ing enoxaparin treatment accelerated clearance of CMR in an additionalway that paralleled augmentation in HL activity rather than contribut-ing directly to amplification of this enzyme. One approach to explainthe effect of insulin on hepatic uptake of CMRmay involve the reportedfacilitation of LDL receptor gene expression by increased insulin sensi-tivity [36], and insulin-mediated increase in cell surface presentationof LDL receptor-related protein [37,38]. Therefore, it is possible that aug-mentation of these receptors worked in concert with the observed aug-mentation in HL activity during enoxaparin treatment to enhanceremnants clearance.
In summary, we show that administration of the LMWH enoxaparinwas associated with enhanced catabolism of CMR accompanied byincrease in plasma lipolytic activity and in insulin sensitivity possiblyattributable to concurrent reduction in plasma TNFα level. This prelim-inary study suggests an additional anti-atherogenic role of enoxaparinbeyond its anti- thrombotic effect. Our results call for a blinded random-ized study using a larger cohort in order to substantiate the beneficial ef-fect of LMWH on post-prandial lipemia.
Conflict of Interest Statement
We hereby certify that there is no conflict of interest with any finan-cial organization regarding the material presented in the manuscript.
Authors Contributions
Itamar Grosskopf – study design and conduct of the study, data col-lection and analysis, data interpretation and manuscript writing
Aviv Shaish – study design, data analysis, data interpretation andmanuscript writing
Assaf Ray – conduct of the study, data collectionDror Harats – data interpretationYehuda Kamari - study design, data interpretation and manuscript
writing
References
[1] Grundy SM, Brewer Jr HB, Cleeman JI, Smith Jr SC, Lenfant C. Definition of metabolicsyndrome: report of the National Heart, Lung, and Blood Institute/American HeartAssociation conference on scientific issues related to definition. Arterioscler ThrombVasc Biol 2004;24:e13–8.
[2] Mamo JC, Wheeler JR. Chylomicrons or their remnants penetrate rabbit thoracicaorta as efficiently as do smaller macromolecules, including low-density lipoprotein,high-density lipoprotein, and albumin. Coron Artery Dis 1994;5:695–705.
[3] Proctor SD, Mamo JC. Arterial fatty lesions have increased uptake of chylomicronremnants but not low-density lipoproteins. Coron Artery Dis 1996;7:239–45.
[4] Yu KC, Cooper AD. Postprandial lipoproteins and atherosclerosis. Front Biosci2001;6:D332–54.
[5] Wilhelm MG, Cooper AD. Induction of atherosclerosis by human chylomicronremnants: a hypothesis. J Atheroscler Thromb 2003;10:132–9.
[6] Goldberg IJ, Kako Y, Lutz EP. Responses to eating: lipoproteins, lipolytic products andatherosclerosis. Curr Opin Lipidol 2000;11:235–41.
[7] Ginsberg HN. New perspectives on atherogenesis: role of abnormal triglyceride-richlipoprotein metabolism. Circulation 2002;106:2137–42.
[8] Weintraub MS, Grosskopf I, Rassin T, Miller H, Charach G, Rotmensch HH, et al.Clearance of chylomicron remnants in normolipidaemic patients with coronary ar-tery disease: case control study over three years. BMJ 1996;312:935–9.
[9] Karpe F, Steiner G, Uffelman K, Olivecrona T, Hamsten A. Postprandial lipoproteinsand progression of coronary atherosclerosis. Atherosclerosis 1994;106:83–97.
[10] Meyer E, Westerveld HT, de Ruyter-Meijstek FC, van Greevenbroek MM, Rienks R,van Rijn HJ, et al. Abnormal postprandial apolipoprotein B-48 and triglyceride re-sponses in normolipidemic women with greater than 70% stenotic coronary arterydisease: a case–control study. Atherosclerosis 1996;124:221–35.
[11] Hirsh J, Anand SS, Halperin JL, Fuster V, American Heart A. Guide to anticoagulanttherapy: Heparin: a statement for healthcare professionals from the AmericanHeart Association. Circulation 2001;103:2994–3018.
[12] Anfinsen CB, Boyle E, Brown RK. The Role of Heparin in Lipoprotein Metabolism.Science 1952;115:583–6.
[13] Jolly S, Tan M, Mendelsohn A, Fitchett D, Armstrong PW, Langer A, et al. Com-parison of effectiveness of enoxaparin versus unfractionated heparin to reducesilent and clinically apparent acute myocardial infarction in patients presentingwith non-ST-segment elevation acute coronary syndrome. Am J Cardiol2007;99:186–8.
[14] Borja J. Role of low-molecular-weight heparin in the management of acute coronarysyndromes. Curr Opin Cardiol 2002;17:608–12.
[15] Goodman SG, Bozovich GE, Tan M, Dos Santos A, Gurfinkel EP, Cohen M, et al. Thegreatest benefit of enoxaparin over unfractionated heparin in acute coronary syn-dromes is achieved in patients presenting with ST-segment changes: the Enoxaparinin Non-Q-Wave Coronary Events (ESSENCE) Electrocardiogram Core LaboratorySubstudy. Am Heart J 2006;151:791–7.
[16] Weitz JI. Low-molecular-weight heparins. N Engl J Med 1997;337:688–98.[17] Iba T, Miyasho T. Danaparoid sodium attenuates the increase in inflammatory
cytokines and preserves organ function in endotoxemic rats. Crit Care2008;12:R86.
[18] Hochart H, Jenkins PV, Smith OP,White B. Low-molecular weight and unfractionatedheparins induce a downregulation of inflammation: decreased levels of proinflam-matory cytokines and nuclear factor-kappaB in LPS-stimulated human monocytes.Br J Haematol 2006;133:62–7.
[19] Tsukada S, Enomoto N, Takei Y, Hirose M, Ikejima K, Kitamura T, et al. Dalteparin so-dium prevents liver injury due to lipopolysaccharide in rat through suppression oftumor necrosis factor-alpha production by Kupffer cells. Alcohol Clin Exp Res2003;27:7S–11S.
[20] Cahalon L, Lider O, Schor H, Avron A, Gilat D, Hershkoviz R, et al. Heparin disaccha-rides inhibit tumor necrosis factor-alpha production by macrophages and arrest im-mune inflammation in rodents. Int Immunol 1997;9:1517–22.
[21] Attanasio M, Gori AM, Giusti B, Pepe G, Comeglio P, Brunelli T, et al. Cytokine geneexpression in human LPS- and IFNgamma-stimulated mononuclear cells is inhibitedby heparin. Thromb Haemost 1998;79:959–62.
[22] Shoelson SE, Lee J, Goldfine AB. Inflammation and insulin resistance. J Clin Invest2006;116:1793–801.
[23] Skoog T, Dichtl W, Boquist S, Skoglund-Andersson C, Karpe F, Tang R, et al. Plasmatumour necrosis factor-alpha and early carotid atherosclerosis in healthy middle-aged men. Eur Heart J 2002;23:376–83.
[24] Iaina A, Silverberg DS, Wollman Y, Judevics R, Baruch R, Levhar C, et al. Postprandialintestinal-derived chylomicron and chylomicron remnants in essential hypertensivepatients before and after prolonged captopril therapy. Am J Hypertens 1995;8:34–9.
[25] Nilsson-Ehle P, Schotz MC. A stable, radioactive substrate emulsion for assay oflipoprotein lipase. J Lipid Res 1976;17:536–41.
[26] Matsuda M, DeFronzo RA. Insulin sensitivity indices obtained from oral glucosetolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care1999;22:1462–70.
[27] Ginsberg HN. Lipoprotein metabolism and its relationship to atherosclerosis. MedClin North Am 1994;78:1–20.
[28] Kim HS, Abbasi F, Lamendola C, McLaughlin T, Reaven GM. Effect of insulin resis-tance on postprandial elevations of remnant lipoprotein concentrations in post-menopausal women. Am J Clin Nutr 2001;74:592–5.
[29] Ruan H, Lodish HF. Insulin resistance in adipose tissue: direct and indirect effects oftumor necrosis factor-alpha. Cytokine Growth Factor Rev 2003;14:447–55.
[30] Lider O, Cahalon L, Gilat D, Hershkoviz R, Siegel D, Margalit R, et al. A disaccharidethat inhibits tumor necrosis factor alpha is formed from the extracellular matrixby the enzyme heparanase. Proc Natl Acad Sci U S A 1995;92:5037–41.
[31] Levy E, Gurbindo C, Lacaille F, Paradis K, Thibault L, Seidman E. Circulating tumor ne-crosis factor-alpha levels and lipid abnormalities in patients with cystic fibrosis.Pediatr Res 1993;34:162–6.
[32] Olson NC, Callas PW, Hanley AJ, Festa A, Haffner SM,Wagenknecht LE, et al. Circulat-ing levels of TNF-alpha are associated with impaired glucose tolerance, increased in-sulin resistance, and ethnicity: the Insulin Resistance Atherosclerosis Study. J ClinEndocrinol Metab 2012;97:1032–40.
[33] Hotamisligil GS, Peraldi P, Budavari A, Ellis R, White MF, Spiegelman BM. IRS-1-me-diated inhibition of insulin receptor tyrosine kinase activity in TNF-alpha- andobesity-induced insulin resistance. Science 1996;271:665–8.
[34] Kanety H, Feinstein R, Papa MZ, Hemi R, Karasik A. Tumor necrosis factor alpha-induced phosphorylation of insulin receptor substrate-1 (IRS-1). Possible mecha-nism for suppression of insulin-stimulated tyrosine phosphorylation of IRS-1. JBiol Chem 1995;270:23780–4.
[35] Boquist S, Hamsten A, Karpe F, Ruotolo G. Insulin and non-esterified fatty acidrelations to alimentary lipaemia and plasma concentrations of postprandialtriglyceride-rich lipoproteins in healthy middle-aged men. Diabetologia2000;43:185–93.
[36] Streicher R, Kotzka J, Muller-Wieland D, Siemeister G,MunckM, Avci H, et al. SREBP-1 mediates activation of the low density lipoprotein receptor promoter by insulinand insulin-like growth factor-I. J Biol Chem 1996;271:7128–33.
[37] Descamps O, Bilheimer D, Herz J. Insulin stimulates receptor-mediated uptake ofapoE-enriched lipoproteins and activated alpha 2-macroglobulin in adipocytes.J Biol Chem 1993;268:974–81.
[38] Ko KW, Avramoglu RK, McLeod RS, Vukmirica J, Yao Z. The insulin-stimulated cellsurface presentation of low density lipoprotein receptor-related protein in 3 T3-L1adipocytes is sensitive to phosphatidylinositide 3-kinase inhibition. Biochemistry2001;40:752–9.