Lithocholic acid-induced placental tumor necrosis factor-α upregulation and syncytiotrophoblast...
10
Original Article Lithocholic acid-induced placental tumor necrosis factor-a upregulation and syncytiotrophoblast cell apoptosis in intrahepatic cholestasis of pregnancy Qiaoling Du, 1 Youhua Zhang, 2 Youdong Pan 2 and Tao Duan 1 1 Department of Obstetrics, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine and 2 Institute of Biochemistry and Cell Biology, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences, Shanghai, China Aim: To investigate tumor necrosis factor (TNF)-a expression and its relationship with serum bile acids in placental tropho- blasts from patients with intrahepatic cholestasis of preg- nancy (ICP). Methods: Human placenta, including normal pregnancies (n = 10) and patients with ICP (n = 10), were collected at term and subject to TNF-a measurements. Bile acid-induced TNF-a expression and cell apoptosis were evaluated in cultured syn- cytiotrophoblasts in vitro. Results: ICP placental trophoblasts displayed apoptotic histological abnormalities. TNF-a levels in ICP tissue were significantly greater than those of controls as measured by quantitative polymerase chain reaction and western blot. Levels of placental TNF-a mRNA were positively correlated with serum bile acid concentration in ICP patients. In vitro, lithocholic acid (LCA) significantly enhanced TNF-a mRNA at both doses, by 2.07-fold at 15 mM and by 3.41-fold at 30 mM, whereas deoxycholic acid mildly increased TNF-a mRNA by 1.41-fold at 100 mM only. LCA treatment produced significantly higher percentage of caspase-3 positive cells than vehicle treatment, rescuable by the addition of a TNF-a inhibitor, indicative of apoptosis induced by LCA–TNF-a pathway. Conclusion: This study shows that the increase of TNF-a expression in placental trophoblasts is strongly associated with ICP pathology and is inducible by LCA in vitro, suggesting its potential value in the clinical prevention, diagnosis and treatment of ICP. Key words: bile acid, intrahepatic cholestasis of pregnancy, lithocholic acid syncytiotrophoblast, tumor necrosis factor-a INTRODUCTION I NTRAHEPATIC CHOLESTASIS OF pregnancy (ICP) is a common complication during pregnancy characterized by itching of the abdomen, palms and soles. Laboratory tests show elevated total bile acids and abnormal liver enzymes. 1 Severely affected patients may present with jaundice. All laboratory test abnormalities occuring during pregnancy will rapidly return to base- line after childbirth. 1 ICP endangers severely the health of both the mother and the fetus. With the increase of blood bile acid, adverse outcome such as premature birth, fetal intrauterine distress and dead fetus in utero markedly enhance. 2 Although a clear correlation between elevated bile acids and ICP onset and fetal outcome has long been established in clinical practice, 2 the mechanisms under- lying the pathophysiology of the disease have not been fully understood. On the maternal side, evidence so far suggests that there may be a genetic component to the disorder. 3 Other studies provided evidence that repro- ductive hormones may play a role. 4 The etiology of the fetal complications associated with ICP is poorly Correspondence: Professor Tao Duan, Department of Obstetrics, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai 200040, China. Email: [email protected]; Dr Youdong Pan, Institute of Biochemistry and Cell Biology, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences, Shanghai 200031, China. Email: ydpan@ sibcb.ac.cn Conflict of interest: The authors declare no conflicts of interests. Author contributions: Q. L. D., T. D. and Y. D. P. designed the experiments. Q. L. D. collected the samples. Q. L. D., Y. H. Z. and Y. D. P. performed experiments and analyzed the data. The manuscript was drafted by Q. L. D. and edited by T. D and Y. D. P. Received 13 January 2013; revision 12 April 2013; accepted 18 April 2013. Hepatology Research 2014; 44: 532–541 doi: 10.1111/hepr.12150 © 2013 The Japan Society of Hepatology 532
Transcript of Lithocholic acid-induced placental tumor necrosis factor-α upregulation and syncytiotrophoblast...

Original Article
Lithocholic acid-induced placental tumor necrosis factor-aupregulation and syncytiotrophoblast cell apoptosis inintrahepatic cholestasis of pregnancy
Qiaoling Du,1 Youhua Zhang,2 Youdong Pan2 and Tao Duan1
1Department of Obstetrics, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicineand 2Institute of Biochemistry and Cell Biology, Shanghai Institutes for Biological Sciences, Chinese Academy ofSciences, Shanghai, China
Aim: To investigate tumor necrosis factor (TNF)-a expressionand its relationship with serum bile acids in placental tropho-blasts from patients with intrahepatic cholestasis of preg-nancy (ICP).
Methods: Human placenta, including normal pregnancies(n = 10) and patients with ICP (n = 10), were collected at termand subject to TNF-a measurements. Bile acid-induced TNF-aexpression and cell apoptosis were evaluated in cultured syn-cytiotrophoblasts in vitro.
Results: ICP placental trophoblasts displayed apoptotichistological abnormalities. TNF-a levels in ICP tissue weresignificantly greater than those of controls as measured byquantitative polymerase chain reaction and western blot.Levels of placental TNF-a mRNA were positively correlatedwith serum bile acid concentration in ICP patients. In vitro,
lithocholic acid (LCA) significantly enhanced TNF-a mRNA atboth doses, by 2.07-fold at 15 mM and by 3.41-fold at 30 mM,whereas deoxycholic acid mildly increased TNF-a mRNA by1.41-fold at 100 mM only. LCA treatment produced significantlyhigher percentage of caspase-3 positive cells than vehicletreatment, rescuable by the addition of a TNF-a inhibitor,indicative of apoptosis induced by LCA–TNF-a pathway.
Conclusion: This study shows that the increase of TNF-aexpression in placental trophoblasts is strongly associatedwith ICP pathology and is inducible by LCA in vitro, suggestingits potential value in the clinical prevention, diagnosis andtreatment of ICP.
Key words: bile acid, intrahepatic cholestasis of pregnancy,lithocholic acid syncytiotrophoblast, tumor necrosis factor-a
INTRODUCTION
INTRAHEPATIC CHOLESTASIS OF pregnancy (ICP)is a common complication during pregnancy
characterized by itching of the abdomen, palms andsoles. Laboratory tests show elevated total bile acids andabnormal liver enzymes.1 Severely affected patients maypresent with jaundice. All laboratory test abnormalitiesoccuring during pregnancy will rapidly return to base-line after childbirth.1 ICP endangers severely the healthof both the mother and the fetus. With the increase ofblood bile acid, adverse outcome such as prematurebirth, fetal intrauterine distress and dead fetus in uteromarkedly enhance.2
Although a clear correlation between elevated bileacids and ICP onset and fetal outcome has long beenestablished in clinical practice,2 the mechanisms under-lying the pathophysiology of the disease have not beenfully understood. On the maternal side, evidence so farsuggests that there may be a genetic component to thedisorder.3 Other studies provided evidence that repro-ductive hormones may play a role.4 The etiology ofthe fetal complications associated with ICP is poorly
Correspondence: Professor Tao Duan, Department of Obstetrics,Shanghai First Maternity and Infant Hospital, Tongji UniversitySchool of Medicine, Shanghai 200040, China. Email:[email protected]; Dr Youdong Pan, Institute of Biochemistry andCell Biology, Shanghai Institutes for Biological Sciences, ChineseAcademy of Sciences, Shanghai 200031, China. Email: [email protected] of interest: The authors declare no conflicts of interests.Author contributions: Q. L. D., T. D. and Y. D. P. designed theexperiments. Q. L. D. collected the samples. Q. L. D., Y. H. Z.and Y. D. P. performed experiments and analyzed the data. Themanuscript was drafted by Q. L. D. and edited by T. D andY. D. P.Received 13 January 2013; revision 12 April 2013; accepted 18 April2013.
bs_bs_banner
Hepatology Research 2014; 44: 532–541 doi: 10.1111/hepr.12150
© 2013 The Japan Society of Hepatology532

understood, but is thought to relate to an increased fluxof bile acids into the fetal circulation.5
In recent years, damage caused directly by accumula-tion of bile acid has become a research focus in thisarea. Elevated bile salt levels can contribute to pretermdelivery by increasing oxytocin bioaction.6 In addition,bile salts may also have a role in unexplained intrau-terine fetal death by inducing vasoconstriction of chori-onic veins,7 oxidative stress and increased apoptosis inthe placenta and fetal liver8 or impairing fetal cardi-omyocyte function.9 The most immediate interfaceupon which the fetus and the mother interact witheach other is the placenta. Changes of trophoblasts inthe placenta may have direct influence on the fetusin utero. It has been recently reported that placentaltumor necrosis factor (TNF)-a expression increases ascompared to healthy controls.10 Previous studies alsoproved that an excessive amount of TNF-a maypromote trophoblast cell apoptosis and directlydamage the placenta.11
The present study was carried out to test the hypoth-esis that TNF-a is upregulated in ICP placenta in asso-ciation with trophoblast cell apoptosis. In addition, invitro experiments were performed to evaluate the directeffects of bile acids on TNF-a expression in culturedhuman syncytiotrophoblasts.
METHODS
Patients and sample collection
PRIOR INFORMED CONSENT for these investiga-tions was obtained from all patients, and the study
was approved by the Research Committee for HumanSubjects, Shanghai Tongji University School of Medi-cine. A total of 20 clinical samples were obtainedbetween December 2010 and December 2011 fromShanghai First Maternity and Infant Hospital, TongjiUniversity School of Medicine. ICP was diagnosed inwomen with the following symptoms: (i) presence ofclassical pruritus with no rash and quick disappearanceafter delivery; (ii) higher than normal serum total bileacid concentration (>10 mM); (iii) absence of itchingskin disease; and (iv) absence of any other causes ofliver dysfunction, including pre-eclampsia; hemolysis,elevated liver enzymes and low platelets (HELLP) syn-drome; acute fatty liver of pregnancy; primary biliarycirrhosis; viral hepatitis; and any ultrasound abnormal-ity. Exclusion criteria for the recruitment of control sub-jects were similar to those for ICP cases. The clinicalcharacteristics of the individuals from whom placentaltissue was obtained are shown in Table 1.
To avoid artifacts from the effects of labor on placen-tal gene-expression profiles, we included only placental
Table 1 Patient characteristics and baseline demographics
Patient no. Obstetric historygravida/para (GP)
Maternalage (years)
Gestational age(week + day)
Birthweight(g)
Total serum bile acidconcentration (mM)
Normal pregnancy1 G1P0 28 39 + 1 3225 2.32 G1P0 30 39 + 2 3420 3.13 G1P0 32 38 + 6 3350 1.84 G1P0 26 39 + 0 3260 4.25 G1P0 29 38 + 5 3500 2.66 G1P0 31 38 + 6 3850 6.17 G1P0 35 39 + 4 3400 3.98 G1P0 27 39 + 1 3280 5.19 G1P0 28 38 + 5 3600 1.9
10 G1P0 30 38 + 5 3250 3.3Intrahepatic cholestasis of pregnancy
1 G1P0 22 36 + 1 2950 35.22 G1P0 30 37 + 5 3100 22.63 G1P0 29 37 + 3 3250 18.44 G1P0 31 38 + 0 3450 19.25 G1P0 30 36 + 2 3150 30.86 G1P0 28 37 + 1 3400 15.37 G1P0 35 36 + 5 3250 40.88 G1P0 27 37 + 4 3100 28.59 G1P0 28 38 + 0 3450 29.2
10 G1P0 28 38 + 1 3300 31.5
Hepatology Research 2014; 44: 532–541 LCA-induced placental TNF-a in ICP 533
© 2013 The Japan Society of Hepatology

samples obtained from women who had not undergonelabor. All samples were collected immediately aftercesarean sections and randomly cut near the maternalsurface villous lobule to yield 5–6 sections. The sizeof sections were approximately 1 cm ¥ 1 cm ¥ 1 cm (forcryosections) or 4 cm ¥ 4 cm ¥ 3 cm (for cell culture).Tissues were stored in 4°C phosphate-buffered saline(PBS) buffer (including antibiotics) and taken back tothe laboratory immediately.
HistologyHematoxylin–eosin (HE) staining was performed fol-lowing standard protocol. Briefly, human placentaltissue samples were fixed in 4% paraformaldehyde for4 h followed by 12-h dehydration in 30% sucrose/PBS.Optimum cutting temperature-embedded tissue thenunderwent cryosection cuts into 8-mm sections at -20°Cbefore being transferred on to poly-L-lysine-coated slidesand immediately fixed in pre-chilled acetone for 10 minat -20°C. After washing with PBS, slides were processedin the following sequence: hematoxylin for 1 min,running water wash for 30 min, 95% alcohol for 5 min,eosin A for 1 min, eosin B for 30 s, dehydration with aseries of alcohol for 5 min each and xylenes for 5 min.Finally, slides were mounted with neutral resin. Thestained sections were visualized using the OLYMPUSIX71 microscope (Olympus, Tokyo, Japan) and imagescaptured by Orca CCD camera (Q-IMAGING, Burnaby,BC, Canada).
RNA extraction, reverse transcription andquantitative reverse transcriptionpolymerase chain reaction (qRT–PCR)Human placental tissue was divided and dissectedseparately on ice-cooled RNase-free surfaces. The sameamount of samples from 10 healthy women and 10women with ICP were pooled into one tube, respec-tively. Tissues were homogenized using a Polytronmixer (Kinematica, Newark, NJ, USA) and RNA isola-tion performed using TRIzol reagent (Invitrogen, SanDiego, CA, USA). Standard cDNA synthesis was per-formed by a reverse transcriptase kit (TaKaRa). qRT–PCR was performed using an Applied Biosystems 7500Fast Real-Time PCR System (Applied Biosystems, FosterCity, CA, USA) using the following primer sets: TNF-asense 5′-CATGATCCGGGACGTGGAGC-3′ and anti-sense, 5′-CTGATTAGAGAGAGGTCCCTG-3′; and glycer-aldehyde 3-phosphate dehydrogenase (GAPDH) sense,5′-CGGAGTCAACGGATTTGGTC-3′ and antisense, 5′-GACAAGCTTCCCGTTCTCAG-3′.
Western blotThe tissue specimens from healthy pregnant women andwomen with ICP were mechanically homogenizedin RIPA lysis buffer (20 mM Tris-HCl, pH 7.4,150 mM NaCl, 10 mM ethylenediaminetetraacetic acid,1% Triton X-100, 0.05% Tween-20) with protease inhibi-tor. The homogenates were centrifuged at 10 000 g for10 min. The protein concentrations of the supernatantswere measured using the Bradford method. A 20-mgprotein sample from each homogenized tissue specimenwas resolved by electrophoresis in a 12% sodium dode-cylsulfate polyacrylamide gel electrophoresis gel andsubject to standard western blot protocol with thefollowing primary and secondary antibodies set:monoclonal rabbit anti-TNF-a (1:1000, Cell SignalingTechnology, Danvers, MA, USA); mouse anti-b-actin(1:10000, Sigma-Aldrich, St Louis, MO, USA); and sec-ondary antibodies (1:5000, Invitrogen). Densitometryanalyses were performed to assess the relative expressionamong samples ImageJ (National Institutes of Health).
Placental cytotrophoblast cell isolationand cultureHuman placental cytotrophoblasts were prepared usinga modification of the method of Kliman.12 Briefly,human placenta was obtained from normal womenafter elective cesarean section at term. Several aliquots oftissue were removed randomly from the maternal sideof the placenta, pooled and digested with 0.11% trypsin(Sigma Chemical, St Louis, MO, USA) and 0.03%deoxyribonuclease-I (Sigma) in Dulbecco’s modifiedEagle’s medium (DMEM; Gibco, Invitrogen, Carlsbad,CA, USA) at 37°C for three times, 20 min each time.The placental cells were loaded onto a 5–70% Percoll(Sigma) gradient at step increments of 5% Percoll, andcentrifuged at room temperature at 1250 g for 20 min toseparate different cell types. Cytotrophoblasts betweenthe density markers of 1.049 and 1.062 g/mL were col-lected and plated at a density of 3.5 ¥ 106 cells/mL inDMEM culture medium containing 10% fetal bovineserum (FBS; Gibco), 1% L-glutamine and 1% penicillin-streptomycin (Gibco). The cells were cultivated for3 days at 37°C in 5% CO2 and 95% O2 before bileacid treatment. Representative cultures were stainedwith 4′,6′-diamidino-2-phenylindole dihydrochloride(DAPI) and imaged using the OLYMPUS IX71 micro-scope and Orca CCD camera (Fig. S1).
ImmunofluorescenceCultured syncytiotrophoblasts were fixed in 3.7%paraformaldehyde/PBS for 15 min at room tempera-
534 Q. Du et al. Hepatology Research 2014; 44: 532–541
© 2013 The Japan Society of Hepatology

ture. Then, cells were permeated with 0.5% Triton X-100(v/v, in PBS) for 5 min. After blocking with 1% bovineserum albumin/PBS for 30 min at room temperature,immunofluorescence was performed using rabbit anti-cleaved caspase-3 antibody (1:300, Cell SignalingTechnology) followed by incubation with fluoresceinisothiocyanate-labeled antibody (1:500, Invitrogen).Then, the cells were rinsed in PBS and incubated for10 min at room temperature with DAPI. The fluorescentstaining was visualized using an OLYMPUS IX71 micro-scope and images captured by CCD camera.
Bile acid treatmentThe cultured syncytiotrophoblasts were FBS-starved for12 h prior to bile acid treatment. A specific form ofbile acid per treatment group (i.e. chenodeoxycholicacid [CDCA], deoxycholic acid [DCA], lithocholicacid [LCA], glycocholic acid [GCA] or taurocholic acid[TCA]) was added to the medium for up to 6 h. Mean-while, a separate group of cells were treated with2 ng/mL interleukin (IL)-1b alone as a positive control.In addition, the effect of TNF-a inhibition on bileacid-induced apoptosis was examined by adding TNF-ainhibitor 654256 (50 mM, Calbiochem, Darmstadt,Germany) to the 6-h treatment.13 These experimentswere conducted at least three times in triplicate.
Statistical analysisStatistical analysis was carried out by two-tailed Stu-dent’s t-test (two-group comparisons) and one-wayANOVA plus Dunnett’s or Tukey’s multiple comparisonstest. Statistical significance was determined by a P-valueless than 0.05. Each experiment was repeated indepen-dently at least three times.
RESULTS
ICP placental trophoblasts displayedapoptotic histological abnormalities
THE HUMAN PLACENTA connects mother and fetusto allow nutrition uptake, waste elimination and
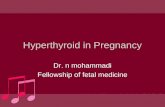
oxygen exchange, and is key to pregnancy outcome.Placental dysfunction leads to fetal developmental chal-lenges. Previous studies have reported ICP placentalapoptosis.14 Herein, we first assessed the histologicalproperties of the trophoblasts from both normal andICP pregnancies. HE staining showed that the placentaltrophoblasts aggregate around the blood vessels in bothgroups but were much decreased in number in ICP pla-cental tissue as compared to the healthy control (Fig. 1).
Additionally, the oval-shaped trophoblasts, as seen incontrol, lost their healthy appearance and became flat inshape with a higher length to width ratio in the ICPgroup (Fig. 1b). Figure 1(c) shows the terminal deoxy-nucleotidyl transferase dUTP nick end labeling stainingof the same samples, revealing increased cell apoptosissignals in ICP placental trophoblasts compared withthat in healthy pregnancy. Collectively, these data con-firmed that placental trophoblasts from women withICP underwent cell apoptosis.
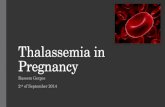
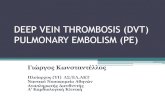
TNF-a expression was upregulated inICP placentaLymphohematopoietic cytokines present at the mater-nal fetal interface have a major impact on pregnancyoutcome.15 Providing the significant role of TNF-a incell proliferation, survival and apoptosis,16 we investi-gated the expression level of TNF-a in placental tissue.qRT–PCR results (Fig. 2a) revealed that the TNF-amRNA levels in the ICP group reached 2.74 1 0.23-foldof those from controls (P < 0.0001, N = 10). Addition-ally, we found that TNF-a mRNA level was positivelycorrelated with total serum bile acid concentrationin the placenta from ICP patients (Fig. 2b; Pearsonr = 0.94, P < 0.0001, n = 10). Western blot analysis(Fig. 2c) also showed that the protein expression ofTNF-a was significantly increased in ICP placentaas compared to control (ICP 3.43 1 0.20 vs control1.06 1 0.08, P < 0.0001, n = 10). Taken together, theseresults suggest that placental TNF-a upregulation isassociated with the onset of ICP.
Bile acids, LCA and DCA induced TNF-aexpression in placentalsyncytiotrophoblasts in vitroA specific biochemical feature of ICP is the rise of serumbile acids to levels between 12.4 and 219.4 mmol/L17
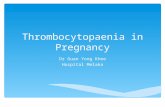
(value in healthy late gestation 211 mmol/L).18 To evalu-ate whether this enhanced bile acid level is causativelyconnected with placental TNF-a upregulation, wetreated the primary cultured human syncytiotropho-blasts from healthy pregnancies with various forms ofserum bile acids, including GCA, TCA, LCA, DCA andCDCA, and measured the level of cellular TNF-a expres-sions. qRT–PCR revealed that LCA and DCA, but notGCA, TCA or CDCA, dose-dependently induced theTNF-a upregulation after 6 h of treatment. Specifically,LCA significantly enhanced TNF-a mRNA at both doses,by 2.07-fold at 15 mM (P < 0.001 vs vehicle, n = 3) andby 3.41-fold at 30 mM (P < 0.001 vs vehicle, n = 3),whereas DCA mildly increased TNF-a mRNA by 1.41-
Hepatology Research 2014; 44: 532–541 LCA-induced placental TNF-a in ICP 535
© 2013 The Japan Society of Hepatology

fold at 100 mM only (P < 0.05 vs vehicle, n = 3) (Fig. 3).IL-1b was used as a positive control and showed signifi-cant TNF-a induction (9.37-fold of vehicle, P < 0.001,n = 3), verifying the molecular signaling integrity ofthese cultured cells (Fig. 3e). In summary, these resultsshowed that serum bile acids, LCA in particular, werethe primary stimuli inducing TNF-a gene upregulationin vitro, suggesting their potential role in the pathogen-esis of ICP.
LCA induced syncytiotrophoblasticapoptosis in vitroWe showed above that the trophoblasts in the ICP pla-cental tissue presented apoptotic morphological abnor-
mality (Fig. 1) as well as TNF-a upregulation (Fig. 2).In vitro bile acid treatment suggested that the TNF-aupregulation in ICP trophoblasts may be derived fromLCA stimuli (Fig. 3). Here, in order to further explorethe direct contribution of LCA to trophoblast cell apo-ptosis, we performed the following experiments. Syncy-tiotrophoblasts cultured from healthy placenta weretreated with or without LCA and cell apoptosis wasevaluated by cleaved caspase-3 immunostaining. Asshown in Figure 4(a), cells treated with LCA for6 h presented more punctuated dense particles in thenucleus, representing chromatin condensation andnuclear fragmentation, which are hallmarks of apopto-sis.19 The percentage of apoptotic cells, calculated by the
a
c
Healthy ICP
HealthyTUNEL/DAPI
ICPTUNEL/DAPI
200μm
200μm
b Healthy ICP
50 μm
Figure 1 Histomorphology of healthyand intrahepatic cholestasis of preg-nancy (ICP) placenta. (a,b) Representa-tive hematoxylin–eosin staining ofplacental tissues from healthy pregnan-cies and women with ICP. Please notethat placental trophoblasts aggregatearound the blood vessels in bothgroups but were fewer in number in ICPplacenta. Arrows in panel (b) point outthat healthy placental trophoblastsappear oval in shape (left) whereas ICPplacental trophoblasts appear flatterwith a higher length : width ratio(right). (c) Representative terminaldeoxynucleotidyl transferase dUTP nickend labeling (TUNEL) staining imagesof placental tissues from healthy preg-nancy and women with ICP. TUNELpositive cells appear as an overlay ofgreen fluorescence from the TUNELstain with blue fluorescence from 4′,6′-diamidino-2-phenylindole dihydro-chloride (DAPI).
536 Q. Du et al. Hepatology Research 2014; 44: 532–541
© 2013 The Japan Society of Hepatology

number of cells with caspase-3 positive stainingover total cell count, was higher in the LCA-treatedsyncytiotrophoblasts (27.77 1 1.02%) than that in thecontrol group (14.22 1 0.77%; P < 0.0001 vs LCA;n = 3), and this LCA-induced apoptosis was rescuedby the addition of a TNF-a inhibitor (17.48 1 0.57%;P < 0.0001 vs LCA, P = NS vs vehicle; n = 3). (Fig. 4b,c).These data suggested that LCA can directly induce syn-cytiotrophoblastic apoptosis in vitro, possibly via theTNF-a pathway.
DISCUSSION
INTRAHEPATIC CHOLESTASIS OF pregnancy isdefined as pruritus with onset in pregnancy and
resolves following delivery. It is associated with liverfunction abnormality in the absence of other liver dis-
ease.1 Enhanced maternal serum bile acid has beenimplicated in the etiology of the fetal disease.2 However,the mechanisms by which bile acids contribute topathological fetal outcome are largely unknown. In thisstudy, using placental tissue from normal and ICP preg-nancy patients, we report for the first time that lympho-hematopoietic cytokine TNF-a is increased in the ICPplacental tissue and that its expression can be induced invitro by bile acid (LCA and DCA) treatment. The bileacid-derived upregulation of TNF-a is associated withplacental trophoblast cell apoptosis.
Tumor necrosis factor-a is a multifunctional cytokineexpressed in the ovary, oviduct, uterus and the pla-centa,20 as well as the embryonic tissues.21 The functionof TNF-a during pregnancy is multifaceted. An appro-priate amount of TNF-a is required in the regulation ofthe growth and differentiation of both the fetus and the
Healthy ICP
(a)
(b)TNF-α
β-actin
0
1
2
3
4
Rel
ativ
e m
RN
A le
vel
0
1
2
3
4
5
Rel
ativ
e pr
otei
n ex
pres
sion
*** ***(c)
Healthy ICP
ICP
0 5 10 15 20 25 30 35 40 45
0
1
2
3
4
5
6
Total serum bile acid (µM)
TN
F-α
mR
NA
Figure 2 Tumor necrosis factor (TNF)-a expression in placental tissue from healthy and intrahepatic cholestasis of pregnancy (ICP)placenta. Human placental tissue homogenates were subject to quantitative reverse transcription polymerase chain reaction andwestern blot analysis for TNF-a measurement. (a) TNF-a mRNA levels (normalized to glyceraldehyde 3-phosphate dehydrogenasein the ICP group are 2.74 1 0.23-fold of those from control (n = 10). (b) TNF-a mRNA level was positively correlated with totalserum bile acid concentration in the placenta from ICP patients (Pearson r = 0.94, P < 0.0001, n = 10). (c) Densitometry analysison western blot data revealing a significant increase in TNF-a expression (normalized to b-actin) in ICP placenta as compared tocontrol (ICP 3.43 1 0.20 vs control 1.06 1 0.08, n = 10). Representative western blot images (n = 4 in each group) are supplementedbelow the bar graphs showing TNF-a (top) and b-actin (bottom) detection in placental tissue. Data are presented asmean 1 standard error of the mean, ***P < 0.0001.
Hepatology Research 2014; 44: 532–541 LCA-induced placental TNF-a in ICP 537
© 2013 The Japan Society of Hepatology

placenta. It stimulates the synthesis and secretion ofprogestin and human chorionic gonadotropin by tro-phocytes and prevents the maternal rejection reactionagainst the fetus.22 However, an excess amount of TNF-atriggers apoptotic intracellular signaling events whichultimately lead to embryonic death.23 It has beenreported previously that TNF-a expression was increasedin placenta from ICP pregnancies.10 In this study, weconfirmed quantitatively that TNF-a expression in ICPplacenta was upregulated to a significantly higher levelthan healthy control and was associated with tropho-blast cell apoptosis, indicating that TNF-a-triggeredplacental apoptosis may be an important mechanismcontributing to fetal maldevelopment in ICP, namely,intrauterine growth retardation, fetal intrauterinedistress, premature birth, dead fetus and stillbirth. Itshould be noted though that in the present study we didalso observe some necrosis-like morphological changesin our LCA-treated cultured cells (Fig. 4a), suggestingthat apoptosis may not be the only cell death pathwaythat is induced by bile acids. It cannot be ruled out thatnecrosis is associated with TNF-a upregulation.
Tumor necrosis factor-a can be induced by a variety ofmechanisms. During non-pregnant stages, it is secretedmainly by macrophages and to a lesser extent, byleukocytes, fibroblasts, glandular cells and endometrialepithelial cells. During pregnancy, trophoblasts become
one of the main sources of TNF-a and they also expressTNF-a receptors.17 Their exposure to high levels ofmaternal serum bile acids during ICP may translateto TNF-a signaling, cascading down to the abnormalplacental–fetal exchange. We therefore evaluated thebiological effects of bile acids on syncytiotrophoblastsin order to connect the link between ICP and TNF-aupregulation. We found in our studies that not only bileacids induced cellular apoptosis; they also significantlyenhanced the expression of TNF-a in cultured syncy-tiotrophoblasts. In particular, we identified that of allthe bile acids, LCA had the highest potency in stimulat-ing TNF-a expression, providing a novel connectionbetween LCA and ICP.
Serum bile acid measurement has been consideredthe most suitable biochemical marker for both the diag-nosis and monitoring of ICP.24 There are reports in thepublished work of elevations in serum bile acids as highas 100-fold the upper limit of normal.25,26 Of the variousbile acid species, LCA displays the highest level of tox-icity. It is the most potent of the naturally occurringsteroids that produce intense fever and inflammation27
and increase the production of bile duct hyperplasia andgallstones.28 In addition, it is reported that LCA couldstimulate cell proliferation and cell apoptosis and isimplicated in human and experimental animal carcino-genesis.29 In a previous study, total serum bile acid
(a) (b) (c)
***
Rel
ativ
e m
RN
A le
vel
0
1
2
3
4
0
1
2
3
4
0
1
2
3
4
0
1
2
3
4
0
2
4
6
8
10
GCA Vehicle 100 μM50 μM TCA LCA 30 μM15 μM
DCA CDCA IL-1β 2 ng/ml
*
***
***
NS NS NS NS
NS NSNS
Vehicle Vehicle
Vehicle Vehicle Vehicle
0
1
2
3
4
(d) (e) (f)
Rel
ativ
e m
RN
A le
vel
Rel
ativ
e m
RN
A le
vel
Rel
ativ
e m
RN
A le
vel
Rel
ativ
e m
RN
A le
vel
Rel
ativ
e m
RN
A le
vel
50 μM 100 μM
100 μM50 μM
100 μM50 μM
Figure 3 Bile acids treatment effects on tumor necrosis factor (TNF)-a expression in cultured syncytiotrophoblasts in vitro. Primarycultured human syncytiotrophoblasts from healthy pregnancies were subject to 6-h treatment with glycocholic acid (GCA) (a),taurocholic acid (TCA) (b), lithocholic acid (LCA) (c), deoxycholic acid (DCA) (d), chenodeoxycholic acid (CDCA) (e) orinterleukin (IL)-b (f) followed by TNF-a mRNA measurement by quantitative reverse transcription polymerase chain reaction. LCAand DCA, but not GCA, TCA or CDCA, dose-dependently induced the TNF-a upregulation. IL-b is used as a positive control. Dataare presented as mean 1 standard error of the mean, ***P < 0.0001, *P < 0.05, NS = not significant, vs vehicle (0).
538 Q. Du et al. Hepatology Research 2014; 44: 532–541
© 2013 The Japan Society of Hepatology

profile measured by capillary electrophoresis showedthat in women with ICP, CDCA, DCA and CA wereincreased moderately (P < 0.05), but LCA levels wereincreased 40-fold (P < 0.01) compared to those fromhealthy pregnant women. In the same study, the per-centage of LCA in total bile acids was higher than 5% oftotal serum bile acids in 31 out of 41 women with ICP,with a mean value of 25.2% (range, 0–97%).30 Ourpresent study displayed the unique potency of LCA ininducing TNF-a, further suggesting its potential value asa biomarker of ICP in clinical diagnosis.
The details underlying the molecular connectionamong bile acids, TNF-a and ICP fetal outcome couldnot be fully addressed by our studies. However, wespeculate the following mechanisms which set the plat-form of our future research in this area. There exists animmunological balance between the maternal body andfetus in normal pregnancy.18 When the immunological
reaction between the maternal body and fetus is abnor-mal, the rejection of the maternal body against the fetusis reinforced. It may activate TNF-a synthesis and secre-tion. Abnormal elevation of TNF-a in placental tissuemay damage the vascular endothelial cells of the pla-centa by causing apoptosis of placental villi trophocytes.It was shown that TNF-a may influence vascular endot-helial cells, enhance their procoagulant activity, reducethe expression of thrombomodulin, change the shape ofvascular endothelial cells, and cause damage to cellmembrane and organelles leading to cellular necrosis,exfoliation and increase of intercellular space.31 Oxida-tive stress can be another key player. It has been reportedthat TNF-a increased the superoxide anion level andenhanced the ability of superoxide anion to activatenitric oxide, leading to dysfunction of vascular endothe-lium.32 A third possible pathway is through hormoneregulation. The elevated estrogen level is associated with
(a)
(b)
DAPI
Merge
CleavedCaspase 3
LCA
LCA
Vehicle
Vehicle
20μm
(c)
% o
f apo
ptot
ic c
ells
***
LCAVehicle
100 μm
LCA + TNF-α inhibitor
0
10
20
30
40
50
LCA + TNF-α inhibitor
*
***
Figure 4 Lithocholic acid (LCA) effectson apoptotic markers in cultured syncy-tiotrophoblasts in vitro. Six-hour LCA(30 mM) treated cells were subject tomicroscopic evaluation and cleavedcaspase-3 staining. (a) LCA-treated cells(bottom) presented apoptotic nuclearmorphology (arrows). (b) Immun-ostaining of cleaved caspase-3 invehicle (left), LCA (middle) orLCA + tumor necrosis factor (TNF)-ainhibitor 654256-treated cells (right).(c) The percentage of apoptotic cells,calculated by the number of cells withcaspase-3 positive staining over totalcell count, was higher in the LCA-treated syncytiotrophoblasts (27.77 11.02%) than that in the control group(14.22 1 0.77%; P < 0.0001 vs LCA;n = 3), and this LCA-induced apoptosiswas rescued by the addition of a TNF-ainhibitor (17.48 1 0.57%; P < 0.0001vs LCA, P = not significant vs vehicle;n = 3). Data are presented as mean 1standard error of the mean, ***P <0.0001, n = 3. DAPI, 4′,6′-diamidino-2-phenylindole dihydrochloride.
Hepatology Research 2014; 44: 532–541 LCA-induced placental TNF-a in ICP 539
© 2013 The Japan Society of Hepatology

pathogenesis of ICP.33 The disease is more common inmultiple than singleton pregnancies (20.9% vs 4.7%).34
TNF-a may promote the synthesis and secretion ofestrogen in placental tissue.35
One observation of note is that the addition of TNF-ainhibitor seemed not to have completely eliminatedthe LCA-induced apoptosis in syncytiotrophoblasts(Fig. 4b,c), indicating that there may be some apoptoticeffects by LCA that were elicited bypassing the TNF-apathway. Our speculation regarding this possibility isas following. Bile acids could disrupt cell membranesthrough their detergent action on lipid components andpromote the generation of reactive oxygen species,which could in turn oxidatively modify lipids and even-tually cause hepatocyte apoptosis.36–38 Studies on chole-static pregnant rats showed that hydrophobic bile acidaccumulation induced impairment of the placental anti-oxidant system and oxidative damage.38 Moreover, theaccumulation of hydrophobic bile acids in the fetalcompartment also causes marked oxidative damageand apoptosis in the fetal liver,8 which is evidenced byenhanced lipid peroxidation, caspase-3 activation andDNA fragmentation. Therefore, it is tempting to specu-late that LCA may exert its function by increasing theserum level of lipids and their oxidized compoundsduring the pathogenesis of ICP.
In conclusion, the present study suggests that theincrease of TNF-a in placental trophoblasts may play asignificant role in the ICP pathology, indicating itspotential value in the clinical prevention, diagnosis andtreatment of ICP. Further studies are in planning todetermine whether reduction or repression of TNF-amay alleviate the maternal and fetal pathologies causedby ICP.
ACKNOWLEDGMENTS
THIS WORK WAS supported by grants from theNational Key Basic Research Program of China
(81170628 and 81270759), China Postdoctoral ScienceFoundation (Grants 2011M500079 and 2012T50445)and the State Key Laboratory of Cell Biology, ShanghaiInstitute of Biochemistry and Cell Biology (SKL-CBKF2012002).
REFERENCES
1 Mullally BA, Hansen WF. Intrahepatic cholestasis of preg-nancy: review of the literature. Obstet Gynecol Surv 2002;57: 47–52.
2 Glantz A, Marschall HU, Mattsson LA. Intrahepaticcholestasis of pregnancy: relationships between bile acidlevels and fetal complication rates. Hepatology 2004; 40:467–74.
3 Reyes H, Ribalta J, Gonzalez-Ceron M. Idiopathic cholesta-sis of pregnancy in a large kindred. Gut 1976; 17: 709–13.
4 Reyes H, Simon FR. Intrahepatic cholestasis of pregnancy:an estrogen-related disease. Semin Liver Dis 1993; 13: 289–301.
5 Brites D. Intrahepatic cholestasis of pregnancy: changesin maternal-fetal bile acid balance and improvement byursodeoxycholic acid. Ann Hepatol 2002; 1: 20–8.
6 Germain AM, Kato S, Carvajal JA, Valenzuela GJ, ValdesGL, Glasinovic JC. Bile acids increase response and expres-sion of human myometrial oxytocin receptor. Am J ObstetGynecol 2003; 189: 577–82.
7 Sepulveda WH, Gonzalez C, Cruz MA, Rudolph MI. Vaso-constrictive effect of bile acids on isolated human placentalchorionic veins. Eur J Obstet Gynecol Reprod Biol 1991; 42:211–15.
8 Perez MJ, Macias RI, Duran C, Monte MJ, Gonzalez-Buitrago JM, Marin JJ. Oxidative stress and apoptosis infetal rat liver induced by maternal cholestasis. Protectiveeffect of ursodeoxycholic acid. J Hepatol 2005; 43: 324–32.
9 Williamson C, Gorelik J, Eaton BM, Lab M, de Swiet M,Korchev Y. The bile acid taurocholate impairs rat cardi-omyocyte function: a proposed mechanism for intra-uterine fetal death in obstetric cholestasis. Clin Sci (Lond)2001; 100: 363–9.
10 Zhang S. Immunohistochemical study on the expression ofTNF-a in placenta in intrahepatic cholestasis of pregnancy(in Chinese). Acta Acad Med Xuzhou 2007; 27: 451–2.
11 Carpentier PA, Dingman AL, Palmer TD. Placental TNF-alpha signaling in illness-induced complications of preg-nancy. Am J Pathol 2011; 178: 2802–10.
12 Kliman HJ, Nestler JE, Sermasi E, Sanger JM, Strauss JF, 3rd.Purification, characterization, and in vitro differentiationof cytotrophoblasts from human term placentae. Endocri-nology 1986; 118: 1567–82.
13 Tada Y, Yano S, Yamaguchi T et al. Advanced glycation endproducts-induced vascular calcification is mediated by oxi-dative stress: functional roles of NAD(P)H-oxidase. HormMetab Res 2013; 45: 267–72.
14 Chen M, Sun L, Ding H, Wu W. The relationship betweenintrahepatic cholestasis and placenta cells apoptosis inpregnancy (in Chinese). Mod Med 2007; 35: 428–31.
15 Gustafsson C, Hummerdal P, Matthiesen L, Berg G, Eker-felt C, Ernerudh J. Cytokine secretion in decidual mono-nuclear cells from term human pregnancy with or withoutlabour: ELISPOT detection of IFN-gamma, IL-4, IL-10,TGF-beta and TNF-alpha. J Reprod Immunol 2006; 71:41–56.
16 Argiles JM, Carbo N, Lopez-Soriano FJ. TNF and preg-nancy: the paradigm of a complex interaction. CytokineGrowth Factor Rev 1997; 8: 181–8.
540 Q. Du et al. Hepatology Research 2014; 44: 532–541
© 2013 The Japan Society of Hepatology

17 El Mourabet M, El-Hachem S, Harrison JR, Binion DG.Anti-TNF antibody therapy for inflammatory bowel diseaseduring pregnancy: a clinical review. Curr Drug Targets 2010;11: 234–41.
18 Gaujoux-Viala C, Eymard C, Dougados M, Gossec L. Preg-nancy appears difficult to obtain and TNF-alpha blockerscannot always be discontinued in women with rheumaticdiseases. Clin Exp Rheumatol 2009; 27: 1059.
19 Susin SA, Daugas E, Ravagnan L et al. Two distinct path-ways leading to nuclear apoptosis. J Exp Med 2000; 192:571–80.
20 Terranova PF, Hunter VJ, Roby KF, Hunt JS. Tumor necrosisfactor-alpha in the female reproductive tract. Proceedingsof the Society for Experimental Biology and MedicineSociety for Experimental Biology and Medicine New York,NY. 1995 Sep; 209: 325–42.
21 Kohchi C, Noguchi K, Tanabe Y, Mizuno D, Soma G.Constitutive expression of TNF-alpha and -beta genesin mouse embryo: roles of cytokines as regulator andeffector on development. Int J Biochem 1994; 26: 111–19.
22 Feinberg BB, Anderson DJ, Steller MA, Fulop V, BerkowitzRS, Hill JA. Cytokine regulation of trophoblast steroido-genesis. J Clin Endocrinol Metab 1994; 78: 586–91.
23 Fukushima K, Miyamoto S, Komatsu H et al. TNFalpha-induced apoptosis and integrin switching in humanextravillous trophoblast cell line. Biol Reprod 2003; 68:1771–8.
24 Walker IA, Nelson-Piercy C, Williamson C. Role of bileacid measurement in pregnancy. Ann Clin Biochem 2002;39: 105–13.
25 Heikkinen J, Maentausta O, Ylostalo P, Janne O. Changesin serum bile acid concentrations during normal preg-nancy, in patients with intrahepatic cholestasis of preg-nancy and in pregnant women with itching. Br J ObstetGynaecol 1981; 88: 240–5.
26 Sjovall K, Sjovall J. Serum bile acid levels in pregnancy withpruritus (bile acids and steroids 158). Clin Chim Acta 1966;13: 207–11.
27 Palmer RH, Glickman PB, Kappas A. Pyrogenic and inflam-matory properties of certain bile acids in man. J Clin Invest1962; 41: 1573–7.
28 Palmer RH, Ruban Z. Production of bile duct hyperplasiaand gallstones by lithocholic acid. J Clin Invest 1966; 45:1255–67.
29 Kozoni V, Tsioulias G, Shiff S, Rigas B. The effect of litho-cholic acid on proliferation and apoptosis during the earlystages of colon carcinogenesis: differential effect on apop-tosis in the presence of a colon carcinogen. Carcinogenesis2000; 21: 999–1005.
30 Castano G, Lucangioli S, Sookoian S et al. Bile acid profilesby capillary electrophoresis in intrahepatic cholestasis ofpregnancy. Clin Sci (Lond) 2006; 110: 459–65.
31 Zhao Y, Xia S, Zou L. The association between polymor-phism of TNF-alpha gene and hypertensive disorder com-plicating pregnancy. J Huazhong Univ Sci Technolog Med Sci2007; 27: 729–32.
32 Zelinkova Z, de Haar C, de Ridder L et al. High intra-uterine exposure to infliximab following maternal anti-TNF treatment during pregnancy. Aliment Pharmacol Ther2011; 33: 1053–8.
33 Torchinsky A, Markert UR, Toder V. TNF-alpha-mediatedstress-induced early pregnancy loss: a possible role of leu-kemia inhibitory factor. Chem Immunol Allergy 2005; 89:62–71.
34 Gonzalez MC, Reyes H, Arrese M et al. Intrahepaticcholestasis of pregnancy in twin pregnancies. J Hepatol1989; 9: 84–90.
35 Salama SA, Kamel MW, Diaz-Arrastia CR et al. Effect oftumor necrosis factor-alpha on estrogen metabolism andendometrial cells: potential physiological and pathologicalrelevance. J Clin Endocrinol Metab 2009; 94: 285–93.
36 Billington D, Evans CE, Godfrey PP, Coleman R. Effects ofbile salts on the plasma membranes of isolated rat hepa-tocytes. Biochem J 1980; 188: 321–7.
37 Sokol RJ, Straka MS, Dahl R et al. Role of oxidant stress inthe permeability transition induced in rat hepatic mito-chondria by hydrophobic bile acids. Pediatr Res 2001; 49:519–31.
38 Perez MJ, Velasco E, Monte MJ, Gonzalez-Buitrago JM,Marin JJ. Maternal ethanol consumption during pregnancyenhances bile acid-induced oxidative stress and apoptosisin fetal rat liver. Toxicology 2006; 225: 183–94.
SUPPORTING INFORMATION
ADDITIONAL SUPPORTING INFORMATION maybe found in the online version of this article at the
publisher’s website:
Figure S1 Isolation and culture of human placentalcytotrophoblast. (a) The distinct cell bands formed inthe 5–70% Percoll gradient tube after centrifuge.Cytotrophoblasts were located at the layer of 40–50%Percoll gradient. (b) A light microscopy observation offreshly isolated cytotrophoblasts. (c) Syncytial forma-tion by cytotrophoblasts cultured on a plastic dishfor 72 h. Nuclei were identified by 4′,6′-diamidino-2-phenylindole dihydrochloride staining.
Hepatology Research 2014; 44: 532–541 LCA-induced placental TNF-a in ICP 541
© 2013 The Japan Society of Hepatology