SERUM βHCG AS A PREDICTOR OF PREGNANCY INDUCED...
112
SERUM βHCG AS A PREDICTOR OF PREGNANCY INDUCED HYPERTENSION Dissertation submitted in partial fulfilment of the Requirement for the award of the Degree of M.S. DEGREE – BRANCH VI OBSTETRICS AND GYNAECOLOGY APRIL 2017 TIRUNELVELI MEDICAL COLLEGE HOSPITAL THE TAMIL NADU DR.M.G.R. MEDICAL UNIVERSITY, CHENNAI, TAMIL NADU
Transcript of SERUM βHCG AS A PREDICTOR OF PREGNANCY INDUCED...
SERUM βHCG AS A PREDICTOR OF
PREGNANCY INDUCED HYPERTENSION
Dissertation submitted in partial fulfilment of the
Requirement for the award of the Degree of
M.S. DEGREE – BRANCH VI
OBSTETRICS AND GYNAECOLOGY
APRIL 2017
TIRUNELVELI MEDICAL COLLEGE HOSPITAL
THE TAMIL NADU DR.M.G.R. MEDICAL UNIVERSITY,
CHENNAI,
TAMIL NADU
CERTIFICATE
This is to certify that the Dissertation entitled “SERUM βHCG AS A
PREDICTOR OF PREGNANCY INDUCED HYPERTENSION”
submitted by Dr.Jayalakshmi, MBBS., to The Tamilnadu Dr.M.G.R. Medical
University, Chennai, in partial fulfilment for the award of M.S (Obstetrics
and Gynaecology) is a bonafide work carried out by her under my guidance
and supervision during the academic year 2013-2017. This dissertation
partially or fully has not been submitted for any other degree or diploma of
this university or other.
GUIDEProf.Dr.MUTHU PRABHA, MD(OG)
Department Obstetrics andGynaecology,
Tirunelveli Medical College,Tirunelveli- 627011.
HODProf.Dr.MEENA,MD.,DGO.,DNB.,
Department Obstetrics andGynaecology,
Tirunelveli Medical College,Tirunelveli- 627011.
Dr.K.Sithy Athiya Munavarah,THE DEAN,
Tirrunelveli Medical College,Tirunelveli- 627011.
DECLARATION
I, Dr.JAYALAKSHMI.D, MBBS., solemnly declare that the
Dissertation titled “SERUM βHCG AS A PREDICTOR OF
PREGNANCY INDUCED HYPERTENSION” had been prepared by me
under the expert guidance and supervision of Prof.Dr.MUTHU
PRABHA,MD.,(OG) Professor, Department of Obstetrics and Gynaecology,
Tirunelveli Medical College Hospital, Tirunelveli.
The dissertation is submitted to The Tamilnadu Dr. M.G.R. Medical
University, Chennai in partial fulfilment of the regulation for the award of
M.S. Degree (Branch VI) in Obstetrics and Gynaecology.
It was not submitted to the award of any degree/diploma to any
University either in part or in full previously.
Place: Tirunelveli.
Date:
Dr.JAYALAKSHMI.D, MBBS.,
POST GRADUATE,
M.S. (Obstetrics and Gynaecology),
Tirunelveli Medical College,
Tirunelveli.
ACKNOWLEDGEMENT
I am very much thankful to the Dean Dr. K.Sithy Athiya Munavarah,
Triunelveli Medical College Hospital, Tirunelveli, who has granted
permission to do this study in this institution,
I take this opportunity to express my deepest sense of gratitude to
professor Dr.MEENA, M.D., DGO., DNB., Head of the Department of
Obstetrics and Gynaecology, Tirunelveli Medical College Hospital,
Tirunelveli for encouraging me and rendering timely suggestions and guiding
me throughout the course of this study. I will be forever indebted to her for
her constant support.
I sincerely thank my professor Dr.RAMALAKSHMI, M.D.,(OG).,
Dr.SHEBA ROSATTE VICTOR,M.D.,(OG)., Dr.M.SUJATHA
ALAGESAN,M.D.,(OG), Dr.VALARMATHI,MD.,(OG).,
Dr.MALLIGA, MD.,(OG)., for their support and guidance.
I am very much thankful to professor Dr.M.Saradha,M.D., (Bio-
Chemistry), Head of Department of Bio-Chemistry for providing valuable
support and guiding through the study.
I am extremely thankful to my guide Dr.MUTHU PRABHA, M.D.,
(OG) for guiding me throughout the study.
I am extremely thankful to all my Assistant Professors of the
Department of Obstetrics and Gynaecology for their guidance and support
throughout my study period in this institution.
I thank Prof. P. Arumugam statistician for their useful inputs.
I wish to express my gratitude to my parents, my brother, my husband
and my son & my sister for their support throughout my study.

I also like to express my gratitude to my friends and colleagues who
have always been a source of love, support and encouragement.
I am very much thankful to all antenatal mothers of Tirunelveli
Medical College without whom this study would not have been possible.
Lastly, I am ever grateful to God for showering his blessing in making
me a part of this noble profession and allowing me to conduct this study and
finish it in time.
CONTENTS
S.No TITLES Page No
1. Introduction 1
2. Aim of the Study 2
3. Review of Literature 5
4. Materials and Methods 56
5. Result & Analysis 59
6. Discussion 86
7. Conclusion 87
8. Summary 89
9. Bibliography
10. Annexure
ABBREVIATIONS
GHT - Gestational Hypertension
LDH - lactate Dehydrogenase
DIC - Disseminated Intravascular Coagulation
APTT - Activated Partial Thromboplastin Time
ALT - Alanine Transaminase
AST - Aspartate Transaminase
DBP - Diastolic Blood Pressure
SBP - Systolic Blood Pressure
ACOG - American College of Obstetricians and Gynaecologists
HT - Hypertension
DM - Diabetes Mellitus
IV - Intra Venous
RCOG - Royal College of Obstetricians and Gynaecologists
MM - Millimetre
% - Percentage
PG - Prostaglandins
OP - Out Patient
dL - Deciliter
DNA - Deoxy Ribonucleic Acid
ML - Millilitre
IGF - Insulin like Growth Factor
IGFBP - Insulin Like Growth Factor Binding Protein
MG - Microgram
IUGR - Intra Uterine Growth restriction
LBW - Low Birth Weight
HCG - Human Chorionic Gonadotrophin
TVMCH - Tirunelveli Medical College Hospital
OPD - Out Patient Department
PIH - Pregnancy Induced Hypertension
BP - Blood Pressure
NICE - National Institute of Health and Clinical Excellence
SLE - Systemic Lupus Erythematosus
BMI - Body Mass Index
KG - Kilogram
M2 - Meter2
PE - Pedal Edema
FSH - Follicular Stimulating Hormone
LH - Luteinising Hormone
TGFβ - Transforming Growth Factor Beta
TSH - Thyroid Stimulating Hormone
HLA-G - Human Leukocyte Antigen-G
MIC - Million International Units
TH1 - ‘T’ Helper Cells 1
TH1 - ‘T’ Helper Cells 2
IL - Interleukin
1
INTRODUCTION
Hypertensive disorders affect 7-15% of 1all gestation and form deadly
triad with haemorrhage and infection2. About 16% of maternal deaths are due to
hypertensive disorders and half of these are preventable.
Hypertensive disorders are also responsible for perinatal mortality and
morbidity. Pre-eclampsia is a risk factor for still birth, IUGR, LBW, Preterm
delivery, Respiratory distress syndrome, and admission in neonatal intensive care
unit. Hypertensive disorders account for 8-10% of all preterm births.
A variety of biochemical and biophysical markers have been proposed for
predicting the development of preeclampsia in pregnancy. Chorionic villi is the
one that is needed for development of preeclampsia. Fetus is not an important
factor. Human chorionic gonadotropin is synthesized from syncitiotrophoblast in
chorionic villi. Incomplete trophoblastic invasion that is replacement of vascular
endothelial and muscular linings by endovascular trophoblast to enlarge the
vessel diameter is incomplete.
This study is conducted to predict gestational hypertension by using serum
beta HCG and thereby to follow up the risk patients and to reduce both maternal
and perinatal morbidity and mortality.
2
AIM OF THE STUDY
To find out the sensitivity of serum beta HCG in prediction of gestational
hypertension and its severity, thereby to follow up the at risk patients and to
prevent the development of Gestational hypertension and pre-eclampsia by
prophylactic measures and to prevent its complications.
3
ABSTRACT
BACKGROUND AND AIMS
Hypertensive disorders occur in 6 %- 8% of pregnancies and contribute
significantly to stillbirths and neonatal morbidity and mortality. They are one of
the leading cause of maternal mortality- accounting for almost 15% of such
deaths. Worldwide, over half a million women die each year because of
pregnancy-related causes, and 99% of these deaths occur in the developing
world.
A variety of biochemical and biophysical markers, have been proposed for
the purpose of predicting the development of preeclampsia in pregnancy.
Screening for these factors in the second trimester of pregnancy will help in early
detection of hypertensive disorders of pregnancy, thus enabling
1. Early identification of patients at risk of developing preeclampsia and
eclampsia.
2. Prophylactic medication to prevent hypertension or to reduce its severity.
3. Prophylactic proper antenatal care.
METHODS
A prospective study was done to determine the role of βhcg in 100
pregnant women in their second trimester (13-20) weeks, attending TVMCH
OPD.Routine antenatal investigations were done. 5 ml of venous blood sample
was collected and tests were carried out. Estimation of serum beta hcg level was
done by enzyme linked fluorescence immunoassay. In antenatal clinic, the
4
patients were followed up.Their frequency of visits are once in a month till 28
weeks, once in 15 days upto 34 weeks and weekly till delivery.
RESULTS
From the study it was found, women who have elevated βHCG values in
13-20 weeks are at increased risk of developing PIH. For any test to be used as a
screening tests it should have good sensitivity, specificity and positive predictive
value.In this study β hcg had Sensitivity – 71.4% , Specificity-87.1%.
CONCLUSION
While comparing patients with normal BP and pre eclampsia - βHCG
values are elevated in patients with pre eclampsia. The sensitivity and specificity
of βHCG are very low to be useful as a mass screening marker on its own and
therefore it should be combined with other serum markers and ultrasound
parameters like Doppler study of uterine vessels, which will help in
improving its role as a screening tool.
KEYWORDS : preeclampsia, hypertensive disorder of pregnancy, β
hcg,screening.
5
REVIEW OF LITERATURE
Yaron Y et al . Am J Obstet Gynecol 1999
A total of 60,040 patients underwent maternal serum screening of alpha
fetoprotein, beta HCG, Unconjugated estriol.There is a significant association
between PIH and increased serum alpha feto protein, increased serum beta HCG
and decreased unconjugated estriol.
Basirat z , et al . Saudi med J,2006
Case group : 40 term pregnant women with pre eclampsia.
Control group : 40 normal pregnancies.
Serum beta HCG is measured by Radio immune assay, and they concluded that
maternal serum beta HCG level in patients with pre eclampsia was higher than in
control group.
Preeti dubey ,kiran pandey ,sunita jain ,shilpi gupta
Prospective study(2009 - 2010) among 300 pregnant women with
gestational age between 14-24 weeks with singleton pregnancy was conducted.
They concluded that there is an association between serum HCG and the
subsequent development of pre-eclampsia.
Begum z , ARA I , TANIRA S , KEYA KA
Cross sectional case control study .A total of 74 pregnant patient with pre
eclampsia(patient were admitted in eclampsia ward in 2013) are included in this
study. 76 normotensive patients were taken as control. To identify the disease
early and to know the severity of disease βHCG is useful.
6
Sumitra yadav ,Namrata shrivastava, Sangeeta paneri,Preeti pawar (2013-
2014)
Prospective comparative study included 50 normotensive and 50 pre-
eclamptic women with gestational age of 28-40 weeks .Beta HCG is measured
by CMIA method (chemiluminescent micropartial immunoassay).They
concluded mean Beta HCG level tends to be significantly higher in pre-eclamptic
women as compared to normotensive pregnant women .
Tapas paul ,Jadab kishore phukan ,Kailash bhattacharyya (2016)
This study was conducted between 50 critically established cases of PIH
and 50 Normotensive women after 24 weeks of pregnancy.They concluded that
pregnant women with PIH have higher level of serum Beta HCG in comparison
to normotensive women.
7
GESTATIONAL HYPERTENSION
According to National High blood pressure working group and ACOG,
Hypertension in pregnancy is defined as systolic BP of 140 mm of Hg and
diastolic BP of 90 mm of Hg in a previously normotensive woman after 20
weeks of gestation,taken on two occasions 6 hours apart.3
Diastolic blood pressure is the disappearance of sounds (korotkoff
phase5). Blood pressure should be measured in sitting or in left lateral position
with the arm at the level of heart4. An appropriately sized cuff is used. If the BP
is high in one arm ,that arm is used for all BP recordings.
Classification of Hypertensive disorders5
Gestational hypertension :
Hypertension for first time during pregnancy.
No proteinuria
BP returns to normal before 12 weeks postpartum.
Pre eclampsia and eclampsia :
Hypertension diagnosed after 20 weeks gestation.
Proteinuria
May have other signs or symptoms of pre eclampsia
Eclampsia when accompanied by seizures that cannot be attributed to
other causes.
Preeclampsia superimposed on chronic hypertension :
New onset proteinuria in hypertensive women after 20 weeks gestation
8
A sudden increase in BP or proteinuria or thrombocytopenia in women
with hypertension and proteinuria before 20 weeks gestation.
Chronic hypertension :
Hypertension before pregnancy
Hypertension diagnosed before 20 weeks gestation, not attributed to
gestational trophoblastic disease or multiple pregnancy
Hypertension first diagnosed before 20 weeks gestation and persists
beyond 12 weeks postpartum
AS PER NICE GUIDELINES6
Mild gestational hypertension:
SBP of 140-149mm of Hg and DBP of 90-99mm of Hg.
Moderate gestational hypertension :
SBP of 150-159 mm of Hg and DBP of 100-109mm of Hg.
Severe gestational hypertension :
SBP of > 160mm of Hg and/ or DBP of >110 mm of Hg.
9
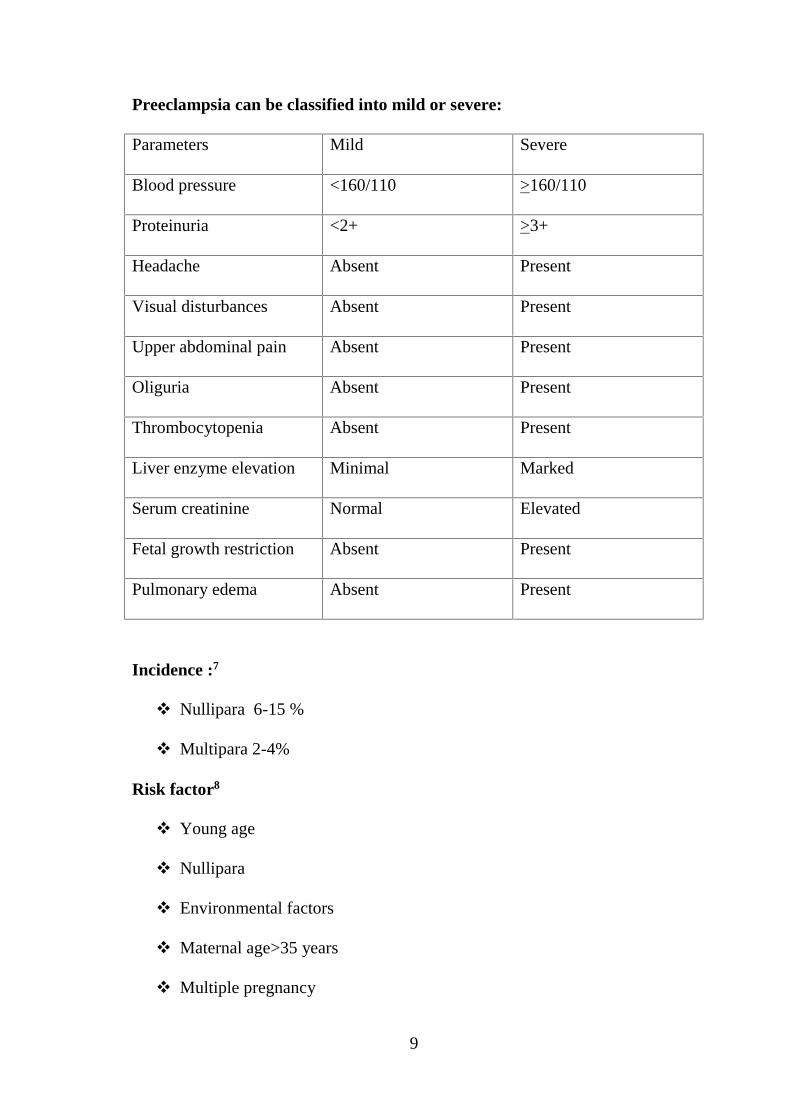
Preeclampsia can be classified into mild or severe:
Parameters Mild Severe
Blood pressure <160/110 >160/110
Proteinuria <2+ >3+
Headache Absent Present
Visual disturbances Absent Present
Upper abdominal pain Absent Present
Oliguria Absent Present
Thrombocytopenia Absent Present
Liver enzyme elevation Minimal Marked
Serum creatinine Normal Elevated
Fetal growth restriction Absent Present
Pulmonary edema Absent Present
Incidence :7
Nullipara 6-15 %
Multipara 2-4%
Risk factor8
Young age
Nullipara
Environmental factors
Maternal age>35 years
Multiple pregnancy
10
Molar pregnancy
Abnormal uterine artery Doppler at 18-24 weeks
High risk factor
Previous preeclampsia
Antiphospholipid antibody syndrome
Pre existing diabetes and or HT
Women with SLE
Chronic renal disease
Moderate risk factors
Multiple pregnancy
Primi
BMI >35 kg/m2
family history of pre eclampsia
maternal age >40 years
Inter pregnancy interval >10 years.
White coat hypertension
DBP >90 mm of hg in office , but <135/85 mm of hg at home (pickering
et al )
EtioPathogenesis 9
1) First time exposure to chorionic villi
2) Exposed to large amount of chorionic villi ,like twins,hydatiform mole.
3) Medical disorders in which endothelial cell activation and inflammation
may be present. ( diabetes, renal, cardiovascular diseases)
11
4) Genetic predisposition
5) Altered renin angiotensin aldosterone system (the refractoriness to
angiotensin 2 is lost).
Pre eclampsia- phenotypic expression
“Two stage disorder” – pre eclampsia theory10
Stage 1 :There is a defect in remodeling of endovascular trophoblast which leads
to stage 2 clinical syndrome.
Stage 2:Patient who were having pre existing Diabetes ,renal, cardiovascular
diseases.
Etiology:11
1) Abnormal trophoblastic invasion of uterine vessels.
2) Genetic factors
3) Inflammatory and angiogenic factors
4) Immunological intolerance between fetal and maternal tissues
12
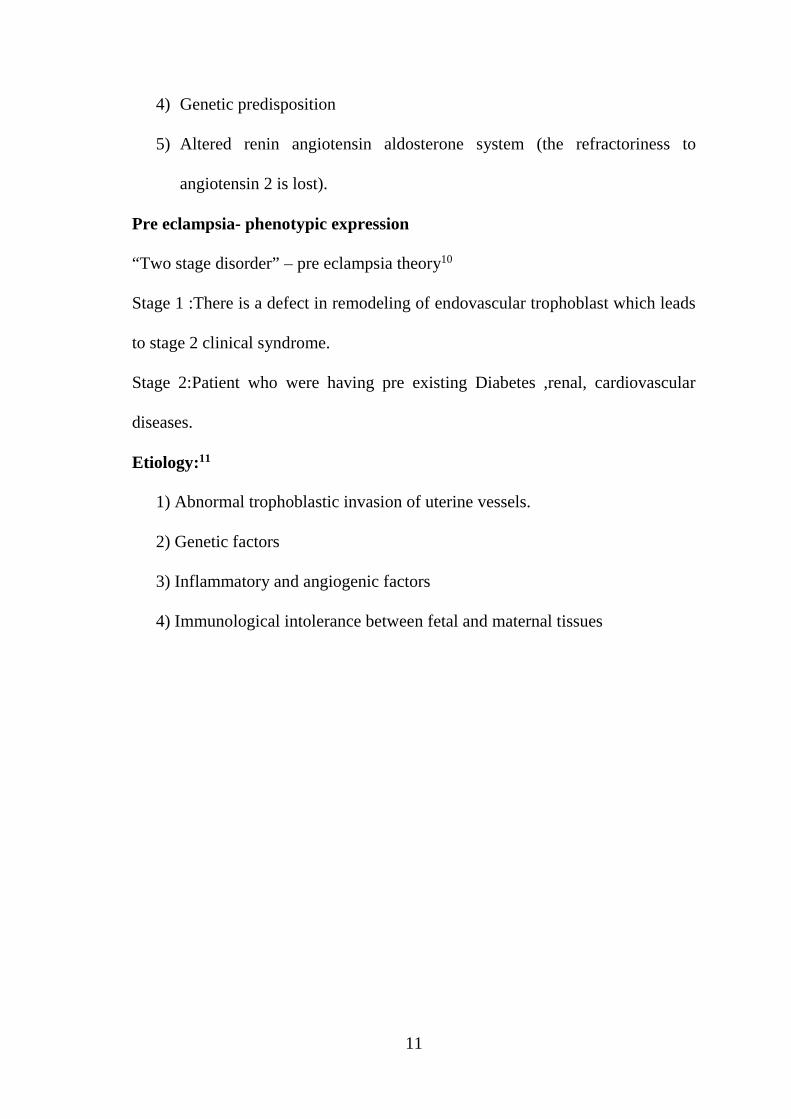
Figure 1: Pathogenesis of pre eclampsia :
Alterations in genetic ,immunological ,environmental factors lead to changes in
regulatory factors like OH/COMT Catechol O-Methyl Transferase /2ME
Methoxy Estradiol and Angiotensin Type 1 agonistic AutoAntibodies (AT1AA),
which results in impaired VEGF /PIGF and TGF-β signaling.- Ultimately leads
to systemic endothelial dysfunction and features of preeclampsia.
13
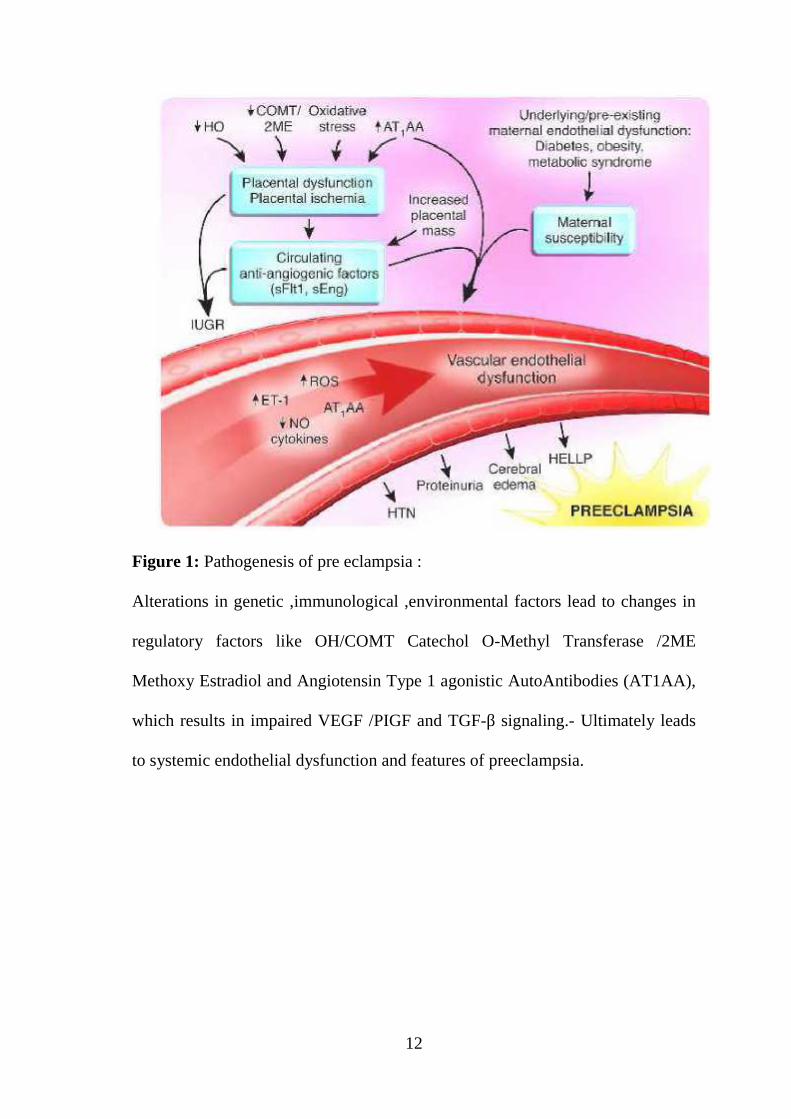
Trophoblastic invasion abnormality:12
Normal:
Replacement of Vascular endothelial cell and muscular linings by
Endovascular trophoblasts.
Abnormal:
Trophoblasts invade decidual vessels but not the myometrium vessels
which results in high resistance flow and a small diameter vessel.
Figure 2:
There is reduced trophoblastic invasion in pre eclampsia and (IUGR) intra
uterine growth restriction compared with normal pregnancy. Hence decreased
14
bloodflow in fetoplacental unit and results in FGR Foetal Growth Restriction.
There is also systemic endothelial dysfunction and development of preeclampsia.
Genetic Factors:13
Candidate genes: polymorphism of FAS, Hypoxia inducible factor -1
alpha protein , Interleukin -1 Beta, Lymophotoxin –alpha, Apo E,TGF –
Beta14,15,16
Gene associated with preeclampsia Function
Factor V(Leiden) Factor V Leiden
MTHFR gene (6771) Methylene Tetrahydrofolate reductase
NOS3 (Glu 298 ASP) Nitricoxide production in Endothelium
AGT (M235 T) Angiotensinogen
F2(I/D at Intron16) Prothrombin (Factor II)
Inflammatory and Angiogenic factors :17
There is reduced expression of HLA-G (immune suppressive human
leucocyte Antigen-G) in women destined to be pre-eclamptic.
There is increased amount of serum antiangiogenic factor (e.g:sFLT-1 is
on chromosome -13) in women with risk for preeclampsia. Hence women
with Trisomy 13 fetus have high risk for preeclampsia.18
Th1 (Pro inflammatory Cytokines) lymphocytes activity is increased &
Th 2 (anti inflammatory Cytokines) activity is decreased.19,20
15
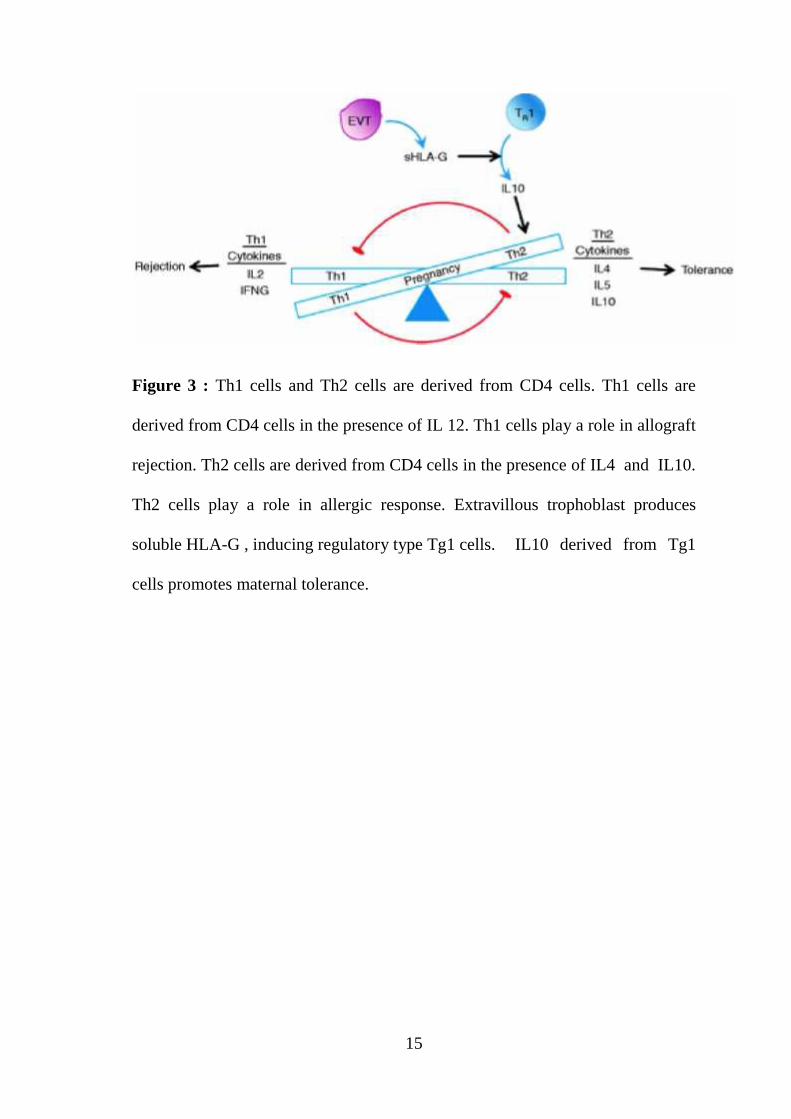
Figure 3 : Th1 cells and Th2 cells are derived from CD4 cells. Th1 cells are
derived from CD4 cells in the presence of IL 12. Th1 cells play a role in allograft
rejection. Th2 cells are derived from CD4 cells in the presence of IL4 and IL10.
Th2 cells play a role in allergic response. Extravillous trophoblast produces
soluble HLA-G , inducing regulatory type Tg1 cells. IL10 derived from Tg1
cells promotes maternal tolerance.
16
Immunological cause:21
Maternal immune system develops immune tolerance to fetal and
placental antigens by blocking antibodies. These blocking antibody sites are
impaired in women with high risk for preeclampsia.
Pathogenesis:
1. Vasoconstriction22
Vasoconstriction and resistance to flow are increased in response to
endothelial activation which leads to Hypertension
2. Increased response to vasopressor 23,24,25,26
Normal pregnant women—develop refractoriness to vasopressor
Preeclampsia predisposed individual –have increased sensitivity to
vasopressor.
3. Prostaglandins27,28
In preeclampsia predisposed individual prostacyclin (PGI2) level deceases,
and (TXA2) Thromboxane A2 level increases - leads to increased sensitivity
to infused vasopressor.
4. Nitric oxide29
Nitric oxide synthesis inhibition mimics the picture of preeclampsia by means
of increased mean arterial pressure and reduced heart rate.
17
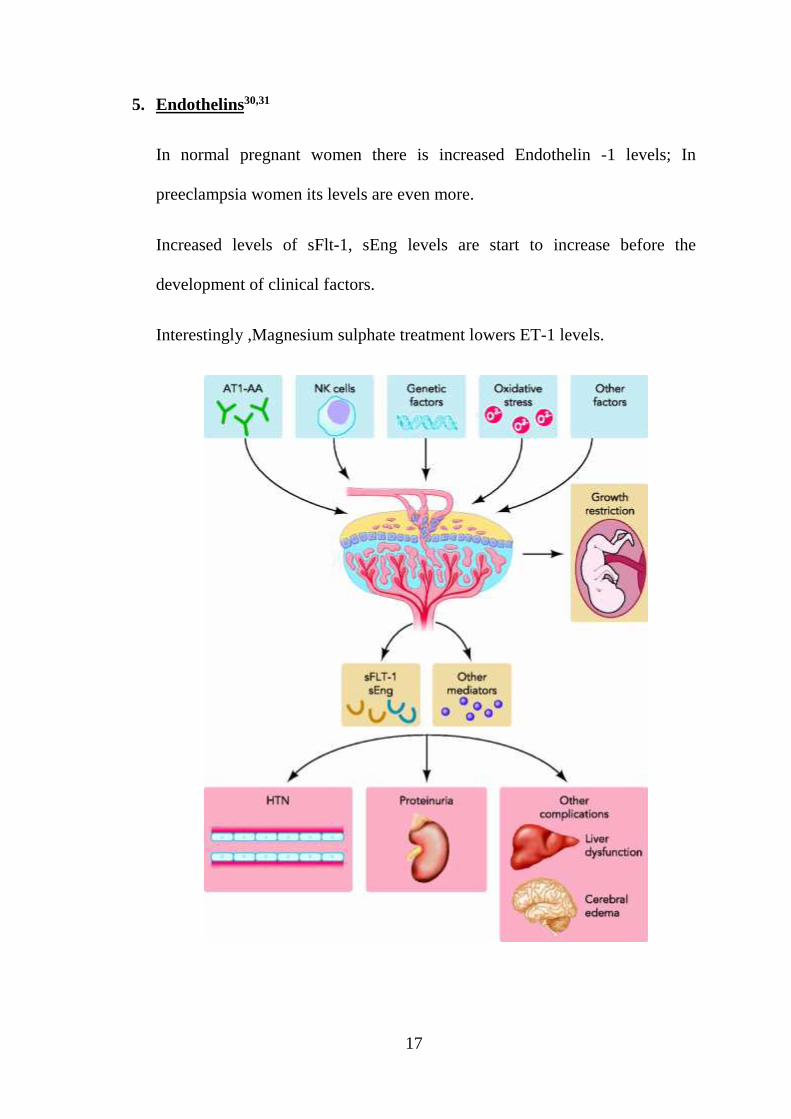
5. Endothelins30,31
In normal pregnant women there is increased Endothelin -1 levels; In
preeclampsia women its levels are even more.
Increased levels of sFlt-1, sEng levels are start to increase before the
development of clinical factors.
Interestingly ,Magnesium sulphate treatment lowers ET-1 levels.
18
Pathophysiology
Cardio vascular system:32
Peripheral resistance is increased and cardiac output is decreased
Ventricular function is normal (or) Hyperdynamic.
Pulmonary oedema due to alveolar endothelial & epithelial leak,
accompanied by decreased oncotic pressure due to low serum albumin.
Blood Volume:33
Usually in GHT, normal blood volume is maintained
In preeclampsia –women have decreased blood volume
Coagulation Abnormalities 34,35
Thrombocytopenia
LDH levels are elevated
Schistocytosis, spherocytosis, reticulocytosis in peripheral blood.
Elevated liver enzymes (because of hepato cellular necrosis).
Fibronectin level is elevated36
19
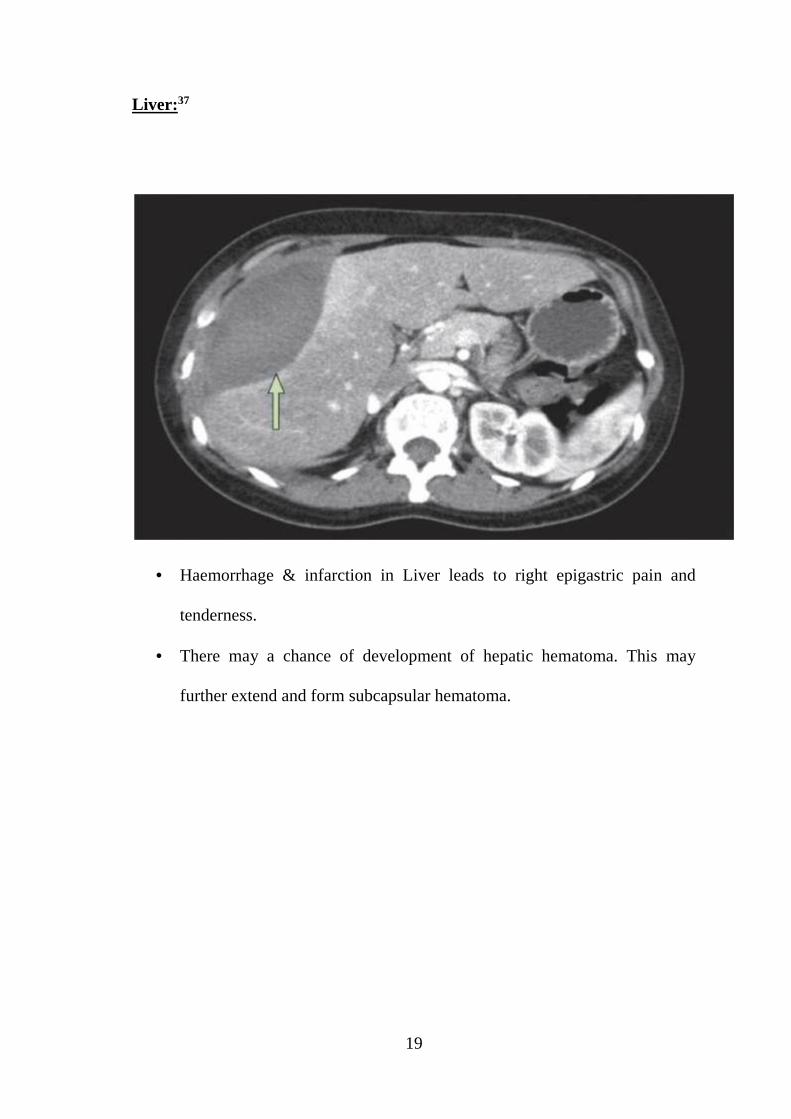
Liver:37
Haemorrhage & infarction in Liver leads to right epigastric pain and
tenderness.
There may a chance of development of hepatic hematoma. This may
further extend and form subcapsular hematoma.
20
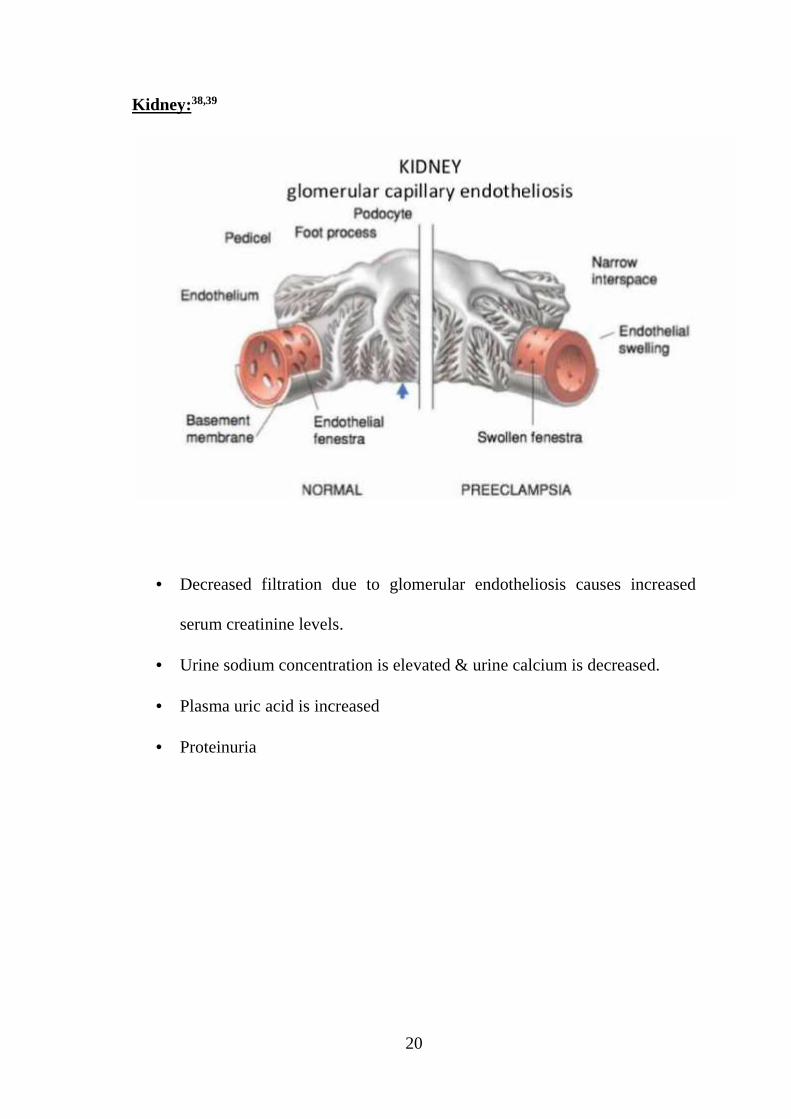
Kidney:38,39
Decreased filtration due to glomerular endotheliosis causes increased
serum creatinine levels.
Urine sodium concentration is elevated & urine calcium is decreased.
Plasma uric acid is increased
Proteinuria
21
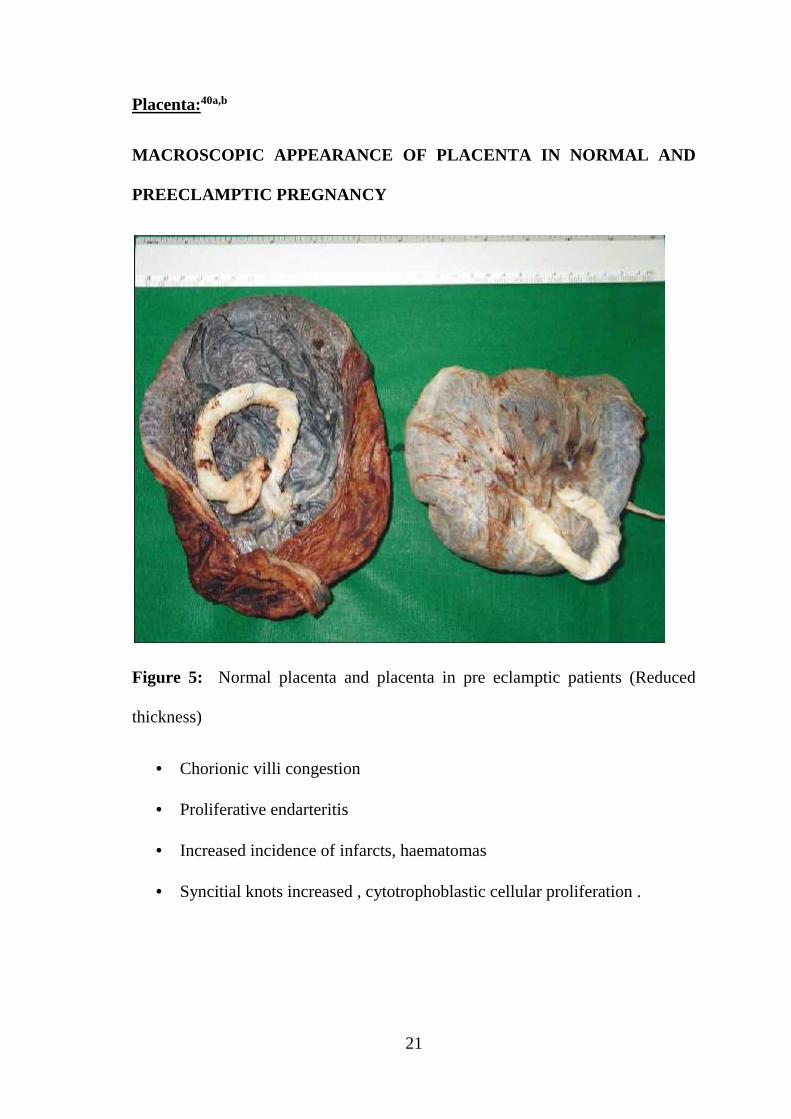
Placenta:40a,b
MACROSCOPIC APPEARANCE OF PLACENTA IN NORMAL AND
PREECLAMPTIC PREGNANCY
Figure 5: Normal placenta and placenta in pre eclamptic patients (Reduced
thickness)
Chorionic villi congestion
Proliferative endarteritis
Increased incidence of infarcts, haematomas
Syncitial knots increased , cytotrophoblastic cellular proliferation .

22
MICROSCOPIC APPEARANCE OF PLACENTA
Figure 6 :Increased levels of syncytial knots in placeta of the patient with pre
eclampsia.
Brain:41,42
There is vasoconstriction of cerebral vessels due to autoregulation which
leads to cytotoxic oedema. When this fails—leads to vasodilatation and
vasogenic oedema.
Foci of infarction may be seen
Cerebral haemorrhage may be seen with chronic hypertension with
eclampsia
23
MRI should be performed in severe hypertensive disease of pregnancy
with complications.43
Management:44a
Evaluation
Urine examination – proteinuria
Hb% increased
Platelet – decreased
Peripheral smear – schistioscytes
INR, APTT- increased (in DIC) – This is done if platelet count and LDH
are abnormal.44b
Serum Creatinine –higher
ALT, AST, LDH, Bilirubin – higher
Albumin-lower
Fundus examination
Pre conceptional advice:
Angiotensin converting enzyme inhibitors, Atenolol, Statins, Thiazides
should be discontinued because of teratogenic effect.
Antepartum Management45a
According to NICE45b guidelines women with at least one high and two
moderate risk factors of preeclampsia should be given 75mg of aspirin
from 12 weeks of pregnancy till the delivery of the baby
24
Reduced physical activity
Regular blood pressure monitoring & ante natal visit (weekly or two
weekly)
Anti-hypertensive therapy
According to NICE guidelines ,women with mild to moderate HT with
comorbid condition –start antihypertensives.
Admission is advised in women with preeclampsia and complication
Out patient management if the disease does not worsen
Criteria for home management of mild preeclampsia.
Ability to comply with recommendations
DBP < 100 mm Hg
SBP < 150 mm Hg
Normal laboratory tests and no maternal symptoms
Reassuring fetal status with appropriate growth
Urine protein of 1 g or less in 24 hours.
Intrapartum management:46,47
Hourly Blood pressure monitoring
Aim is to maintain diastolic BP at or below 110mmHg and Systolic BP at
or below 160mmHg.
Mild hypertension with severe disease or organ dysfunction- start Anti
Hypertensives. Women with mild to moderate HT with co-morbid
condition- Treat with Anti Hypertensives.
25
Eclampsia prophylaxis given in women with severe preeclampsia or
impending eclampsia
Continuous fetal heart monitoring
Vaginal delivery should be considered except for obstetric indications
In case of poor bishop score, induction should be done with
prostaglandins
Ergometrin should be avoided; Active management of third stage of
labour (AMTSL) should be followed.
Indication for caesarean delivery:
Timing of Delivery(ACOG)
The outcome of Labour induction > 37 weeks in mild preeclampsia, was
better compared to expectant management (Koopmans et al 2009)
For women with controlled HT (With drugs)- 37 to 39 weeks
With severe HT -36 to 37 weeks.
Treatment of Hypertension:
SOGC Guidelines (2008) suggest that with Anti-hypertensive therapy 48
Hypertensive women without comorbid conditions should have DBP
between 80-105 mmHg
Hypertensive women with comorbid conditions (DM, Renal disease)
should have SBP 130-139 mm of Hg and DBP 80-89mm of Hg
In patients with severe HT, maintain SBP of 140 -150mm of Hg and DBP
of 90-100mm of Hg.
26
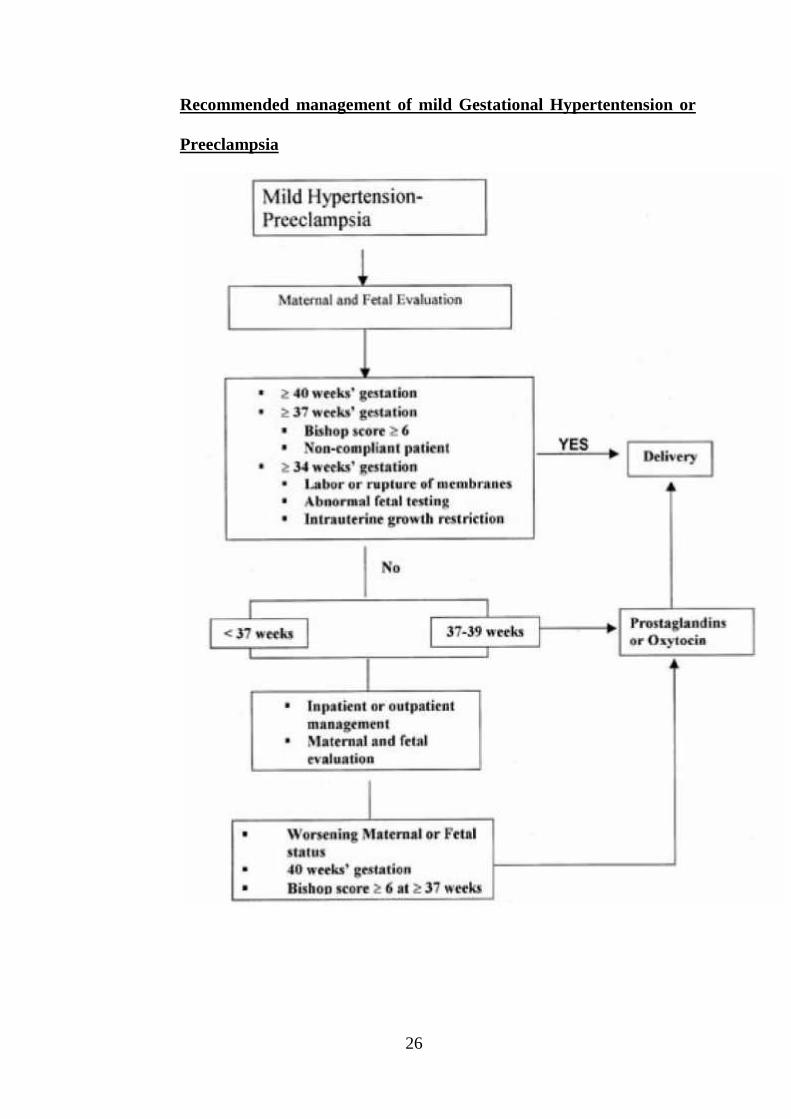
Recommended management of mild Gestational Hypertentension or
Preeclampsia
27
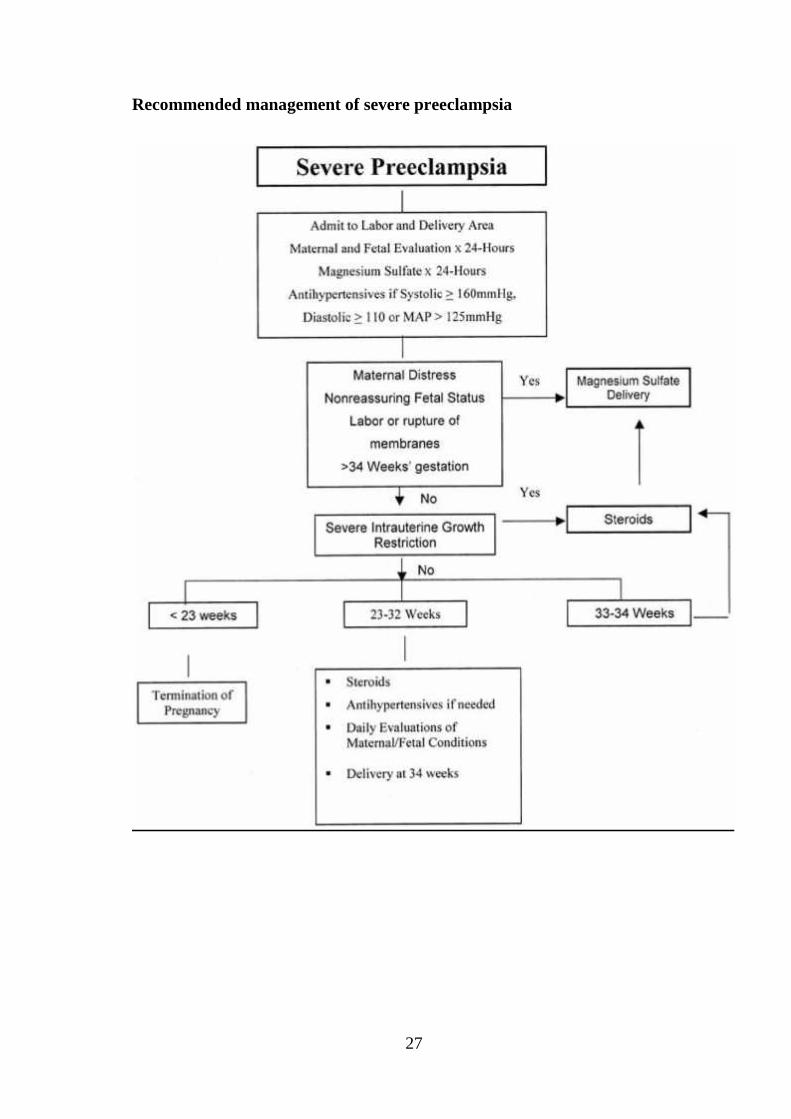
Recommended management of severe preeclampsia
28
DRUGS
1. LABETALOL-- Adrenoceptor blocker ; 100-400 mg bd- tds (maximum
of 1200mg/day) . Side effects – postural Hypotension, tiredness
2. METHYL DOPA --Centrally acting alpha adrenergic agonist ; 250 -
500mg tds-qid(maximum of 2g/day). Side effects – headache, dizziness,
hypotension .
3. NIFEDIPINE -- calcium channel blockers ; 10-20mg bd. Side effects-
Hypotension, head ache, and nasal congestion .
4. HYDRALAZINE- i.v boluses ; starting at 5mg and increasing by 5mg
every 20 minutes upto 20 mg.49
CORTICOSTEROIDS:
Women with preeclampsia before 34 weeks should have steroids for fetal
lung maturity.
12 mg of Betamethasone given in 24 hours apart as2 doses .(RCOG –
2010) 50
Complications:
Maternal:
1. Eclampsia
2. Cerebro vascular Accident (May occur due to intracerebral haemorrhage )
3. Placental abruption
4. HELLP Syndrome51
29
Haemolysis
Abnormal peripheral smear (schistocytes, burr cells
LDH> 600 U/L
Bilirubin >1.2 mg/dl
Elevated Liver Enzymes
AST > 70 U/L
LDH> 600 U/L
Low Platelet count
Platelet count < 100 000 /mm3
5. Pulmonary oedema with or without acute left ventricular failure
6. Acute Renal failure
7. Micro angiopathic haemolytic Anaemia.
8. Disseminated intravascular coagulation (DIC)
9. Drug related side effects
Foetal:
1. Intra uterine fetal growth restriction
2. Oligohydramnios
3. Prematurity (more likely to be iatrogenic in preeclampsia due to
termination in severe Preeclampsia, Eclampsia, Abruption)
4. Antepartum and intrapartum asphyxia mostly due to poor placental blood
flow, maternal hypoxia induced by Eclampsia (or) sedative effect by
anticonvulsant
30
5. Intra uterine death
6. Fetal side effects of antihypertensive drugs.
Eclampsia:
Eclampsia is defined as the development of seizures that can not be
attributed to other causes and/ or unexplained coma during pregnancy or
puerperium in a woman with pre-eclampsia
Maternal mortality in Eclampsia is 1 to 5 %
Perinatal mortality occurs in about 5-12% of the cases.52
Impending Eclampsia:
It is suggested in women with following signs and symptoms
Headache (occipital or frontal)
Blurring of vision
Epigastric pain and or right upper quadrant pain
Nausea/ vomiting
Oliguria
Laboratory evidence of disseminated intra vascular coagulation
It presents as generalised tonic-clonic convulsions and or coma in a pre-
eclamptic woman.
Management:53,53a,b,c
Magnesium sulphate is for prevention and treatment.
31
Clearing the airways, oral suctioning, oxygen
Controlling the blood pressure
Delivering the baby
MAGNESIUM SULPHATE
Loading dose: 4g of 20% magnesium sulphate is given i.v slowly over 5
minutes, followed by 10 g of 50% magnesium suphate solution, one half (5g)
i.m injected deeply into each gluteal region.
Maintenance dose:5 g magnesium sulphate (50% solution) every 4 hours into
alternate buttock intramuscularly.
Monitor:
Respiratory rate
Patellar reflexes
Urinary output before giving repeat doses.
In case of magnesium toxicity give 1 g calcium gluconate (10 ml of 10%
solution) i.v slowly
DELIVERY
In case of preeclampsia – must be delivered with in 24 hours
In case of Eclampsia – with in 12 hours in a patient who has Convulsions.
If the cervix is favourable – Amniotomy or labour induction with PG, Oxytocin
If the cervix is unfavourable & fetus is alive – caesarean section
32
Risk of recurrence:54
In women with GHT:
GHT-16 to 17%
Pre-eclampsia- 2 to 7 %
In women with Pre-eclampsia
GHT-13-53%
Pre-eclamplsia-16%
In women with Eclampsia or HELLP
Preeclampsia -25 to 55 %
PREDICTION AND PREVENTION
SCREENING TESTS FOR PREECLAMPSIA
I. Alteration in the function of placental perfusion and resistance in vessels
Mean arterial blood pressure
Doppler ultrasound
Roll over test
Angiotensin infusion test
Isometric exercise test
Platelet angiotension II binding
Platelet calcium response to arginine vasopressin
Renin
33
24-hours Ambulatory blood pressure monitoring
II.Alteration in the function of Fetoplacental unit
Human chorionic gonadotrophin
Alpha fetoprotein
Inhibin A
Pregnancy-associated plasma protein A – decreased
Estriol
III. Alteration in the function of Renal parameters
Elevated Serum uric acid
Increased Microalbuminuria
Kallikrein in urine
Elevated Microtransferrinuria
IV.Alteration in the function of Endothelial & oxidant stress
Fibronectin-elevated
Endothelin-elevated
Thromboxane-elevated
Homocysteine-elevated,
The various predictors can be broadly classified as non laboratory methods and
laboratory methods.
34
NON LABORATORY METHODS:
1. History : High risk factors associated with preeclampsia includes
· Primigravida
· Extremes of maternal age
· Obesity
· Multifetal gestation
· Prior pregnancy complicated by preeclampsia
· Ethnicity.
2. Provocative pressor tests: These tests are based on increased vascular
sensitivity to vasopressor stimuli in women those destined to be hypertensive
during pregnancy
a. Angiotensin II infusion test- Talledo et al.1968
This test is done between 28-30 weeks
An increase in the diastolic BP more than 20 mmHg during the Angiotensin
infusion predicts preeclampsia with a sensitivity of 90% , specificity of 87%,
positive predictive value of 78% in high risk population
Disadvantage:
· Difficulty to do as a mass screening procedure.
· Time consuming
· Expensive
· Unreliable
35
b. Roll over Test-Grant et al
This test is done between 28-32 weeks of pregnancy. First the blood
pressure is recorded with the patient in left lateral position. An increase in
diastolic BP of more than 20mmHg, when the patient lies on the supine
position is regarded as positive test.
Sensitivity - 0-88%
Specificity - 5-95%
Positive predictive value - 0-93%
This test is of no clinical use due to gross variation in results.
c. Isometric handgrip test: Dagani et al.55
This test is done between 28-32 weeks of gestation.
Suggested a threshold increase of 20mmHg in diastolic BP when patient
Squeezes a hand ball for 3 minutes
Sensitivity 81%
Specificity 96%
Positive predictive value 81%
d. Mean Arterial pressure:
Page and Christians on suggested that patients with mean arterial pressure
more than 90 mmHg in second trimester are at high risk for pre-eclampsia. But
predictive value vary greatly.
36
Doppler USG: Campbell and associates
Doppler velocimetry of uterine umbilical vessels can predict pre-
eclampsia as early as 18 weeks. There is a characteristic notching of diastolic
waveform, suggesting increased peripheral resistance due to impaired
trophoblastic invasion of spiral arterioles in patients with risk to develop pre-
eclampsia. It is not useful for screening pregnant women -Bowel and colleagues
(1993)
Sensitivity 78%
Positive predictive value 28%
LABORATORY TESTS :
Fetal placental unit – endo crine dysfunction
HCG, Alpha Fetoprotein , Estriol ,PAPPA, inhibin A , activin A,
Placental protein 13 , Corticotropin releasing hormone .
Markers of endothelial dysfunction
Serum fibronectin
Plasminogen activator inhibitors,cell adhesion molecules, serum
thrombomodulin,endothelin-1
coagulation factors and platelets
serum uric acid
Atrial natriuretic peptide, Haematocrit.
37
Urinary assays:
a. Microalbuminuria
b. Urinary calcium excretion56
c. Urinary calcium / creatinine ratio57
d. Urine kallikrien / creatinine ratio
e. Fasting urine albumin/ creatinine ratio
Proteinuria
Proteinuria means protein levels in urine of >150 mg/day.
In O.P settings, Dipstick method is used.
False positive results with
1. Hematuria
2. Drugs like penicillin ,sulphanamides
3. Pus,semen and vaginal secretions.
False negative reports in
1. Diluted urine
2. Other nonalbumin or LMW protein
The results are graded as
negative (less than 10 mg per dL),
Trace (10 to 20 mg per dL),
1+ (30 mg per dL),
2+ (100 mg per dL),
3+ (300 mg per dL)
4+ (1,000 mg per dL).
38
This method preferentially detects albumin and it is less sensitive to globulins
or parts ofglobulins (heavy or light chains or Bence Jones proteins).
Angiogenic factors
Decrease in proangiogenic factors like vascular endothelial growth factors
(VEGF) and placental growth factors (PlGF)
Increase in antiangiogenic factors like sFlt -1 and sEng
Cell free fetal DNA: 58,59
Fetal maternal cell trafficking is increased in pregnancies complicated by
preeclmpsia. Conde concluded that cell free-fetal DNA quantification is
not yet useful for prediction of preeclampsia.
Serum uric acid:
Serum uric acid concentration is raised in preeclampsia due to decreased
clearance. Serum level correlates with disease severity and fetal outcome.
The rise in serum levels occurs relatively late in the course of the disease. Hence
not reliable as a predictor. Sensitivity ranged from 0-55% and specificity 77-
95%. Raised serum uric acid is probably better regarded not as a predictive,
diagnostic or specific feature of preeclampsia, but as a sensitive indicator of
impaired renal function.
39
SERUM FIBRONECTION:
Fibronectin is a glycoprotein that has a important role in cellular
adhesions, migration, phagocytosis and homeostasis. It is a component of
connective tissue and basement membrane. Following endothelial injury, it is
released from endothelial cells and extracellular matrix into circulation.
Cellular fibronectin levels of> 3.8 ug/mL within 22 to 26 weeks of gestation was
proposed to be helpful in the early detection of preeclampsia in primigravida.
Sensitivity, specificity and positive & negative predictive values were
inconsistent among different studies. Systemic review concluded that neither
cellular nor total fibronectin was clinically useful to predict
PIH.
Hyperhomocysteinemia:
Homocysteine causes oxidative stress and endothelial cell dysfunction and
it is found to be elevated in preeclampsia. Although women with elevated serum
homocysteine levels at 14-16 weeks of pregnancy had a 3 – 4 fold risk of
developing preeclampsia, 80 it has not shown consistent results.
Serum inhibin A activin A:
Their role in etiology of preeclampsia is not clear. They are secreted by
trophoblast cells of placenta, levels peak at 8 weeks and then declines to rise
again at term. They have a formation of placental bed in invasion of trophoblast.
Maternal serum levels are increased between 13-18 weeks in patients who later
develop preeclampsia.
40
Alpha-Fetoprotein (AFP):
Origin from ,
i. Yolk sac
ii. Fetal liver
iii. Gastro intestinal tract
Maternal serum AFP increases until 30 weeks of gestation.there is a association
between high maternal AFP and preeclampsia or GHT have been demonstrated
in several studies. In fetal serum AFP reaches a peak value of 3mg/ml at 12
weeks of gestation and declines thereafter.
Pregnancy Associated Plasma Protein – A (PAPP-A):
IGF have a role in regulation of fetal growth. PAAP-A is a protease for
IGFBP1 and IGFBP2. Hence ,
Low level of PAPP-A
Elevated IGFBP1 and IGFBP2
Low level of IGF
IGF have also role in trophoblastic invasion of deciduas by controlling the
uptake of glucose and aminoacids.
Low maternal PAPP-A at 10-14 weeks
Marker of inadequate placentation
Associated with GHT and FGR
41
Angiogenic and antiangiogenic factors:
Several proangiogenic and antiangiogenic substances are involved in
placental vascular development. Factors like Vascular Endothelial Growth Factor
(VEGF) placental growth factor (PLGF) are decreased in preeclampsia. This
difference is consistently not seen in early pregnancy. Study demonstrated that
placental growth factor is not a good marker for subsequent development of
severe preeclampsia. Excessive amounts of antiangiogenic factors are stimulated
by worsening hypoxia at the uteroplacental interface. Trophoblastic tissue of
women destined to develop preeclampsia over produces at least 2 antiangiogenic
peptides that enter the maternal circulation.
i. Soluble Fms – like tyrosine kinase (sFlt-1) is a receptor for placental
growthfactor (PLGF) and Vascular Endothelial Growth Factor (VEGF).
ii. Soluble endoglin (sEng) is a placental derived molecule that blocks
iii. Endoglin, a co-receptor for TGFB. It inhibits binding of TGFB to
endothelial receptors and results in decreased endothelial nitric oxide
dependent vasodilatation. The cause of placental overproduction of
antiangiogenic proteinss remains enigma.
iv. Soluble endoglin and soluble fms like tyrosine kinase 1 (SFlt-1) are
increased prior to onset of clinical disease. Until better substantiated, their
clinical usefulness is not recommended,
URINE TESTS
A number of investigators have evaluated the potential value of
microalbuinuria as a predictive test. Microalbuminuric phase precedes clinical
42
proteinuric phase. The developmentof a radioimmunoassay for albumin has
made it possible to detect microalbuminuria in women who have not yet
developed proteinuria as demonstrated by clinical methods.87 Pregnant women
with mircoalbuminuria (> 12.04 ugm/ml) at 16-22 weeks are at risk of
developing hypertensive disorder Sensitivity 9% and specificity 29% with poor
predictive value.
Urinary calcium excretion:
Hypocalciuria occurs early and persists throughout the pregnancy affected
with preeclampsia. Taufield et al measured 24 hours urinary calcium excretion
and found lower total and fractional excretion in women with preeclampsia as
compared to normotensive pregnant women.
Urinary calcium creatinine ratio:
Rodrigtiez et al compared the microalbuminuria and calcium creatinine as
predictive test.
Microalbuminuria ≥11µg/ml
Calcium creatinine ratio≤0.04µg/ml
They concluded Calcium creatinine ratio is superior to microalbuminuria. But
still large number of studies are required.
Urinary Kallikreins excretion:
Kallikreins are proteases with indirect vasomotor effects mediated by
kinins and by the renin-angiotensin system. Urinary Kallikreins excretion has
been shown to increase in normotensive pregnancy, whereas in preeclampsia
reduced levels as compared to non-pregnant subjects have been found.
43
In Millar et al study, the ratio between inactive urinary Kallikreins and urinary
creatinine concentrations at 16-20 weeks as predictor test to diagnose
preeclampsia. This test does not have any significant sensitivity and specificity.
But have some prognostic significant in development of PIH.
Difficulties with assay techniques have impeded assessment of Kallikrein-kinin
system in PIH.
Microtransferrinuria :
Urinary microtransferrin levels in pregnant women who subsequently
developed severe PE and eclampsia were significantly higher than those of the
pregnant women who remained normotensive. With sensitivity 93.5%,
specificity 65%, it can be a potential predictor of preeclampsia.
As of ACOG (2004), there is no clinically useful screening test to predict
the development of preeclampsia. Further, prospective longitudinal studies are
needed.
44
Prevention
There is a considerable literature devoted to the prevention of
preeclampsia. However, there is some controversy over whether or not
prevention of preeclampsia per se is a worthy goal, rather than the prevention of
the complications of preeclampsia.
Primary prevention
Primary prevention though best, is possible only when the exact etiology
is known. Primary prevention is possible to some extent by modification of some
of the risk factors. As the disease process more common in nulliparous women or
in mutliparous women with change of partners, it is recommended to have
pregnancies with low risk men, to stay with same partner and to have children at
an age when the endothelium is still able to cope with the inflammatory stress
associated with the pregnancy state. Prevention &/or effective control of
obesity could significantly result in the frequency of preeclampsia.
Similarly women with diabetes, chronic hypertension, renal and other
medical disorders should have their primary condition under control before
attempting conception. However it applies only to minority of patients.
Secondary prevention
The basic requirements for secondary prevention are
1) knowledge of pathophysiological mechanisms
2) availability of screening methods
3) means of intervention and modification of the pathophysiology.
45
None of the 3 criteria are available for effective secondary prevention.
Many screening tests suffer from poor sensitivity and specificity.
Non pharmacological interventions
1. Bed rest
2. Life style changes
3. Regular physical activity
Nutritional interventions
1. Dietary sodium restriction
2. Dietary protein and energy intake
3. Control of obesity.
4. Change in dietary habits
5. Fist oil-some studies have shown beneficial effects of omega-3 fatty
acids in the prevention of preeclampsia. The large European multicentre
Fish Oil supplementation. Trial (FOTIP) concluded that fish oils are
unlikely to beneficial in prevention of preeclampsia.
6. Alcohol intake.
7. Arginine supplementation – found to be beneficial but it was an
isolated study.
8. Japanese Herbal medicine Toki-shakuyuku-san (TS) – may be
beneficial in the
treatment and prevention of preeclampsia.
46
Pharmacological Interventions
1 Antihypertensive drugs.
2 Diuretics
3 Zinc supplementation.
4 Magnesium
5 Folic acid and other B vitamins – there is no scientific data that any of B
vitamins are beneficial in the prevention of preeclampsia.
6 Low dose aspirin: Low dose aspirin 50-150mg/day therapy during
pregnancy selectively inhibits platelet thromboxane A2 (TX-A2)
biosynthesis with minimal effects on prostacyclin. Largest trial to date is
CLASP (collaborative low dose aspirin) study. Overall the use of low
dose aspirin was associated with 12% reduction in the incidence of
preeclampsia (non significant) and it reduced the incidence of preterm
delivery (19.7% v/s 22.3% in placebo group). Aspirin treated women has
slightly higher risk of abruptio placentae (STATISTICALLY NOT
SIGNIFICANT). Meta analysis of antiplatelet agents for the prevention of
preeclampsia did not find difference between treatment and control group.
The results of available trials do not support the widespread and routine
prophylactic or therapeutic use of aspirin therapy for women judged to be
at risk for preeclampsia. The only group where low dose aspirin may be
justified is in women at risk of developing early onset preeclampsia.
7 Heparin and low dose aspirin – for only women with anti phospholipids
antibody syndrome and not for routine recommendation.
47
8 Calcium supplementation – There is inverse relation between calcium
intake and the frequency of preeclampsia. The largest trial conducted
(2g/day supplementation) by Levind did not find any benefit. However
Cochrane review observed a modest reduction in preeclampsia and the
effect was greatest in high risk women with low calcium intake.
9 Nitric oxide (NO) donors – NO synthesis is impaired in preeclampsia.
10 The data on effects of NO donors in prevention of preeclampsia are
limited and conflicting. A large multicentric trial is currently underway.
11 Antioxidants – Various antioxidants like Vitamin C, E, Iycopene,
selenium, N-acetylcysteine and garlic are used in many studies with
encouraging results. However the Cochrane review 2008 finds that
antioxidant supplementation may not affect risk of preeclampsia or
clinical outcomes (level 2 evidence).
Diet:60,61
Low salt diet
Calcium and fish oil containing foods
Exercise:
Cardiovascular drugs:
Diuretics
antihypertensive drugs
Anti-oxidants62,63,64
Vitamin C, Vitamin E, Vitamin D
48
Anti-thrombotic agents:65,66
Low dose Aspirin
Aspirin/ Dipyridamole
Aspirin + Heparin
Aspirin + Ketanserin
HUMAN CHORIONIC GONADOTROPIN
Human chorionic gonadotropin is a glycoprotein a peptide frame
work to which carbohydrate side chains are attached.
Half-life – 24 to 36 hours
Alpha (92 amino acids)
HCG consists of -2 subunits
Beta (145 amino acids)
These 2 subunits are linked by disulphide bonds
α subunit is identical to –FSH,LH,TSH
β subunit is unique and specificity in immunoassay is attributed to the molecular
and carbohydrate differences in β subunit
In β subunit, there is a unique carboxy terminal tail piece of 23 amino
acids groups that allow production of highly specific immunologic assays.
Molecular weight :36000 Daltons .
49
Biosynthesis of HCG:
1) α subunit originates from one single gene on chromosome 6
50
2) β subunit originates from 8 separate genes for beta subunits of different
glycoprotein hormone on chromosome 19.
3) Secreted by trophoblasts
Before 5 weeks syncytiotrophoblasts and cytotrophoblasts produce HCG.
Later produced exclusively by syncytiotrophoblasts.
It acts via plasma membrane LH-HCG receptors
Regulation of HCG synthesis:
HCG Secretion is probably regulated by
1. Placental GnRH (Gonadotrophin releasing hormone) and CRH
(corticotropic releasing hormone)
2. Activin, Endorphin, inhibin
3. Butylated cyclic AMP
4. Interleukin 1, and interleukin 6
5. Transforming growth factor ( TGF- Beta )
6. Fibroblast growth factor
7. Tumour necrosis factor (TNF)
Exact mechanism by which regulation occurs is not known
51
Clearance:
Renal clearance accounts for 30% of HCG clearance.
Remaining is likely cleared by metabolism in liver
Molecular forms in plasma and urine
HCG exists in multiple forms
Intact HCG
Hyperglycosylated HCG
Nicked HCG
Free subunits
HCG concentration in serum:
HCG concentration is approximately 100 IU/L at time of expected but
missed menses. The maximum level of about 1,00,000 IU/L in maternal
circulation is reached at 8-10 weeks gestation. HCG levels decrease to about
10,000 -20,000 IU/L by 18-20 weeks of gestation and remain at that level until
delivery.
Doubling time approximately 3 days (1.4 to 3.5 days)
Levels are elevated in : multiple gestation
Down’s syndrome fetus
Gestational trophoblastic disease
52
Decreased levels seen in:
Ectopic pregnancy
Impending miscarriage
Functions of HCG:
Supports corpus luteum of pregnancy till placenta takes over
Stimulates fetal leydig cells to produce testosterone
May promote uterine muscle relaxation and vasodilatation
Promotes secretion of relaxin by corpus luteum
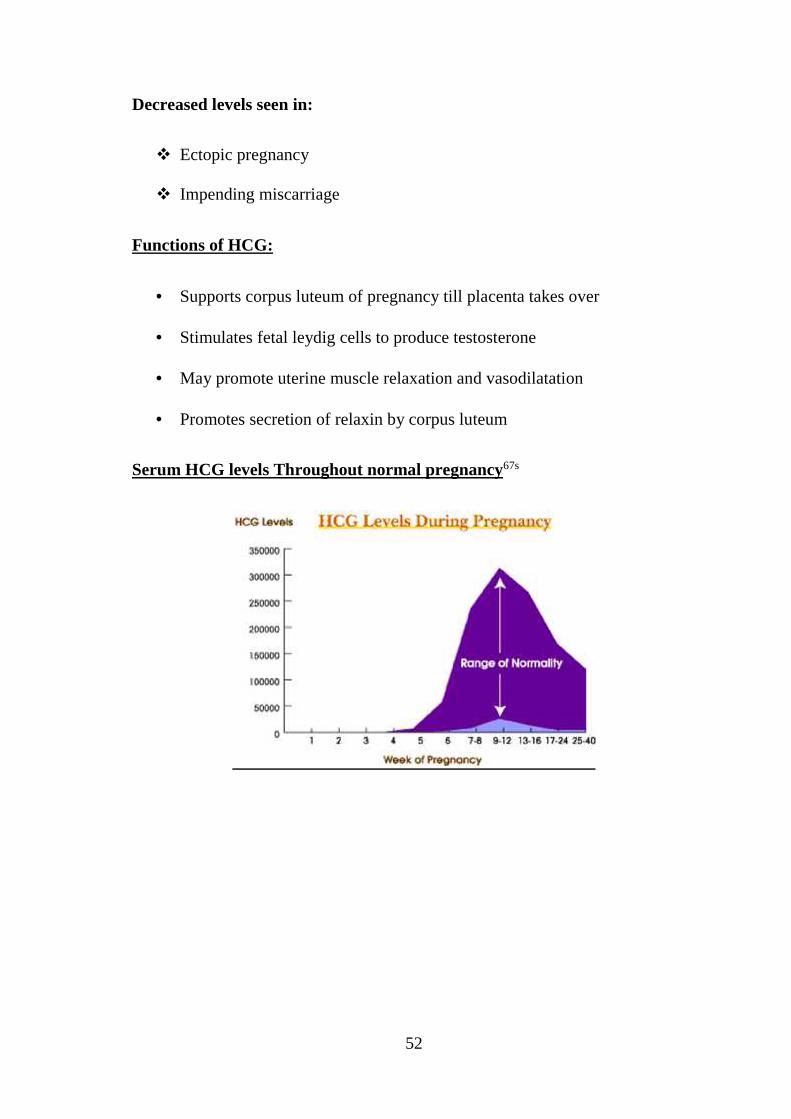
Serum HCG levels Throughout normal pregnancy67s
53
3 weeks LMP : 5-50 m IU/ml
4 weeks LMP : 5-426 m IU/ml
5 weeks LMP : 18-7340 m IU/ml
6 weeks LMP : 1080-56500 m IU/ml
7-8 weeks LMP : 7650 -229,000 m IU/ml
9-12 weeks LMP : 25700-2,88,000 m IU/ml
13-16 weeks LMP : 13,300-2,54,000 m IU/ml
17-19 weeks LMP : 4,060 -1,65,400 m IU/ml
25-40 weeks LMP : 3640-117,000 m IU/ml
Non pregnant females < 5 m IU/ml
Numerous different assays for quantitative estimation of HCG have been
developed that differ in methodology (Radio- immunoassay, Enzyme
immunoassay,Fluorescent immunoassay), sensitivity and specificity.68
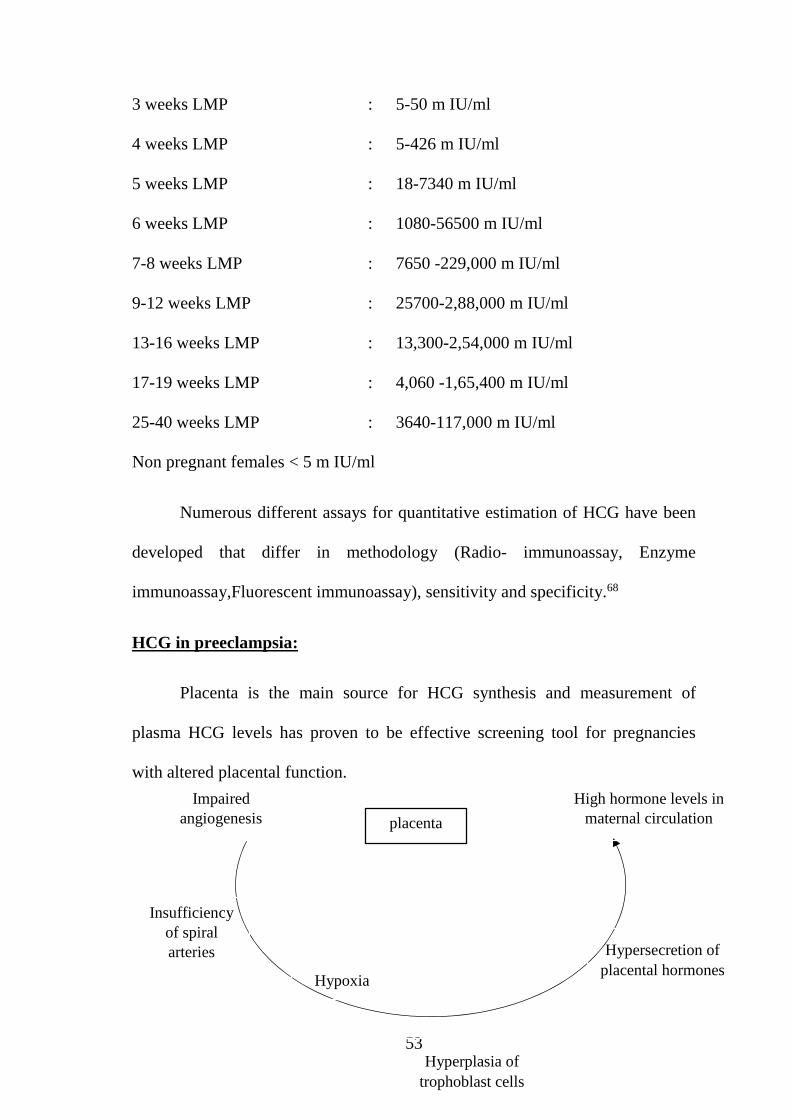
HCG in preeclampsia:
Placenta is the main source for HCG synthesis and measurement of
plasma HCG levels has proven to be effective screening tool for pregnancies
with altered placental function.
placenta
Impairedangiogenesis
High hormone levels inmaternal circulation
Insufficiencyof spiralarteries Hypersecretion of
placental hormones
Hyperplasia oftrophoblast cells
Hypoxia
54
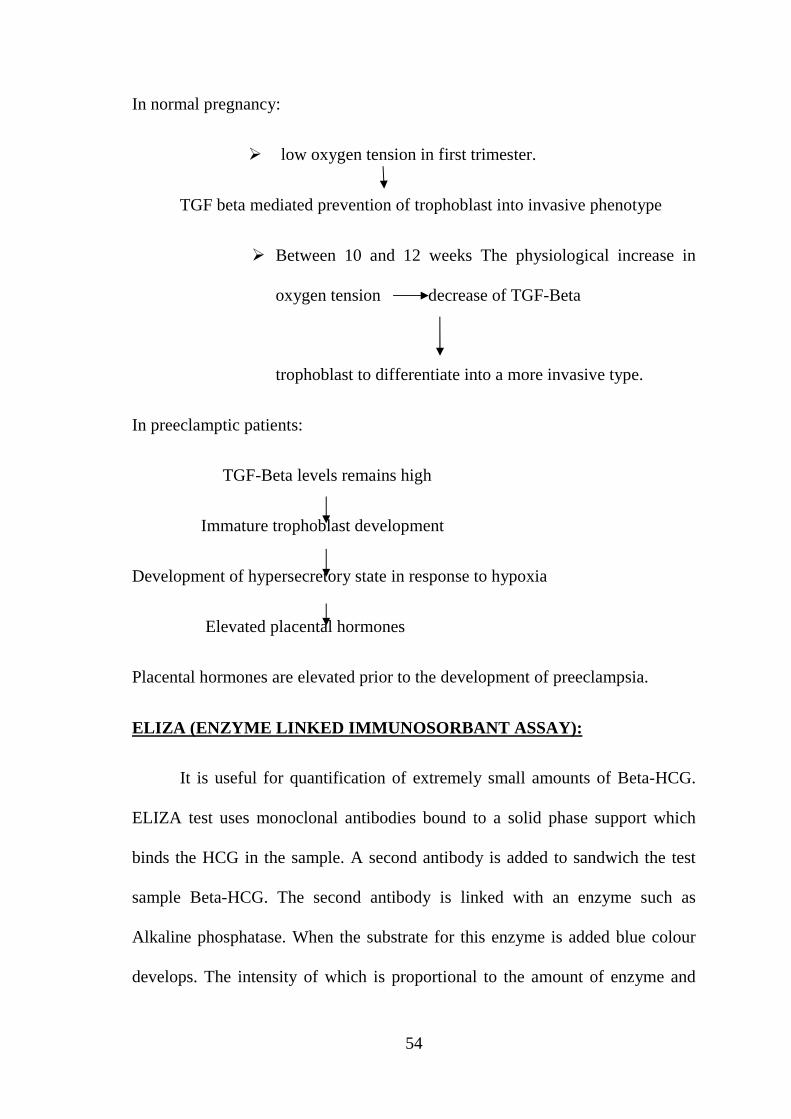
In normal pregnancy:
low oxygen tension in first trimester.
TGF beta mediated prevention of trophoblast into invasive phenotype
Between 10 and 12 weeks The physiological increase in
oxygen tension decrease of TGF-Beta
trophoblast to differentiate into a more invasive type.
In preeclamptic patients:
TGF-Beta levels remains high
Immature trophoblast development
Development of hypersecretory state in response to hypoxia
Elevated placental hormones
Placental hormones are elevated prior to the development of preeclampsia.
ELIZA (ENZYME LINKED IMMUNOSORBANT ASSAY):
It is useful for quantification of extremely small amounts of Beta-HCG.
ELIZA test uses monoclonal antibodies bound to a solid phase support which
binds the HCG in the sample. A second antibody is added to sandwich the test
sample Beta-HCG. The second antibody is linked with an enzyme such as
Alkaline phosphatase. When the substrate for this enzyme is added blue colour
develops. The intensity of which is proportional to the amount of enzyme and
55
thus to the amount of second antibody bound. This in turn is a function of the
amount of Beta-HCG in the test sample. The sensitivity of the test is 25-50
mU/ml.
56
METHODOLOY
INTRODUCTION
The primary aim of antenatal care is to achieve a healthy mother and
healthy baby .Nowadays there are many investigations and treatment modalities
are available. Although advances in antenatal care, Hypertensive disorder in
pregnancy contribute to increased maternal mortality and morbidity and thereby
accounts for increased perinatal morbiditiy and mortality. Major causes of
maternal mortality includes haemorrhage, sepsis, hypertension, obstructed
labour abortion and other conditions.
Placentation abnormality is one of the main event in disease
formation.There is immunological changes in trophoblast which leads to
secretory response. This is seen as rise seen in β hcg levels. This study was
conducted to find out the association between β hcg and development of GHT.
AIM
To test the hypothesis that women with high serum beta-HCG levels in
early pregnancy are at higher risk of developing PIH.
METHODS
Serum beta-HGC estimation was done by ELISA method in 100 women
between 13 and 20 weeks of gestation, selected randomly for this study from
Aug2014 to Jul2015.
57
INCLUSION CRITERA
Pregnant women with
1. Non proteinuric
2. Normotensive
3. Primi/Multi gravida
4. Singleton
5. Gestational age 13-20 weeks as determined by last menstrual period or
ultrasound scan.
EXCLUSION CRITERIA
Chronic hypertension.
Molar Pregnancy.
Diabetes mellitus.
Anomalous foetus.
Multiple pregnancy.
METHODS
All the women were subjected to detailed history regarding age, parity,
past obstetric history, medical history, and family history. Height, weight, blood
pressure were measured.
Routine antenatal investigation was done. 5 ml of venous blood sample
was collected andtests were carried out. Estimation of serum β hcg level was
done by enzyme linked fluorescence immunoassay.
58
The cases were followed up in antenatal clinic and were examined 4
weekly till 28 weeks, fortnightly upto 34 weeks and thereafter weekly till
delivery. At every visit, blood pressure was recorded and urine was examined for
albumin.PIH included gestational hypertension and preeclampsia. Gestational
hypertension was defined as blood pressure _ 140/90 mmHg on two occasions at
least 6 hours apart after 20 weeks of gestation. Preeclampsia was defined as
gestational hypertension and proteinuria of atleast 1 + on dipstick. The patients
who developed preeclampsia were followed till 6 weeks after delivery.
59
RESULTS AND ANALYSIS
Data analysis and interpretation:
The data were analysed and interpreted according to the type of variables.
The continuous variables were analysed in terms of mean and interpreted by
student’s t test. The discontinuous variables were described in terms of
percentages and interpreted by χ2 (Chi-square) test. The cut point for prediction
of βHCG as an indicator of PIH was done by ROC curve approach. The level of
significance was fixed as 5% and the P-values less than or equal to 0.05 (P≤0.05)
were considered as statistically significant.
Results:
Similarity of study subjects:
The study subjects namely normal and PIH mothers were compared in
terms of their age, SBP and DBP at the time of Ante- natal registration.
60
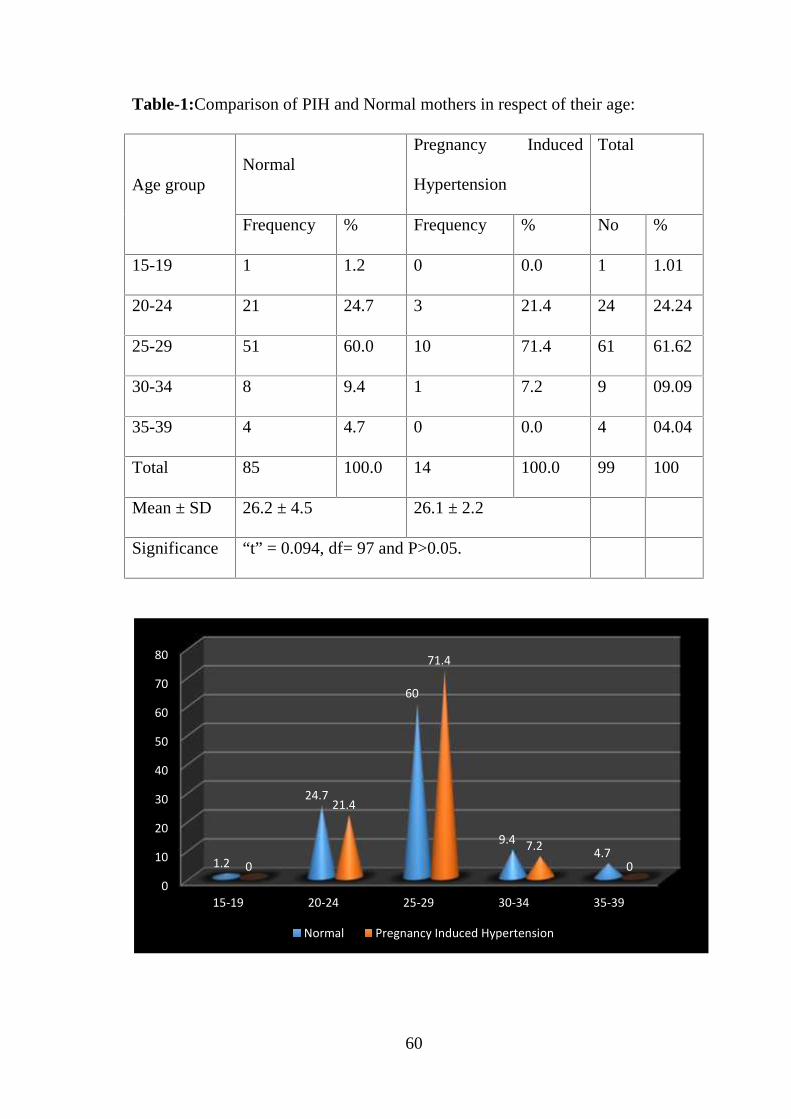
Table-1:Comparison of PIH and Normal mothers in respect of their age:
Age groupNormal
Pregnancy Induced
Hypertension
Total
Frequency % Frequency % No %
15-19 1 1.2 0 0.0 1 1.01
20-24 21 24.7 3 21.4 24 24.24
25-29 51 60.0 10 71.4 61 61.62
30-34 8 9.4 1 7.2 9 09.09
35-39 4 4.7 0 0.0 4 04.04
Total 85 100.0 14 100.0 99 100
Mean ± SD 26.2 ± 4.5 26.1 ± 2.2
Significance “t” = 0.094, df= 97 and P>0.05.
0
10
20
30
40
50
60
70
80
15-19 20-24 25-29 30-34 35-39
1.2
24.7
60
9.44.7
0
21.4
71.4
7.20
Normal Pregnancy Induced Hypertension
61
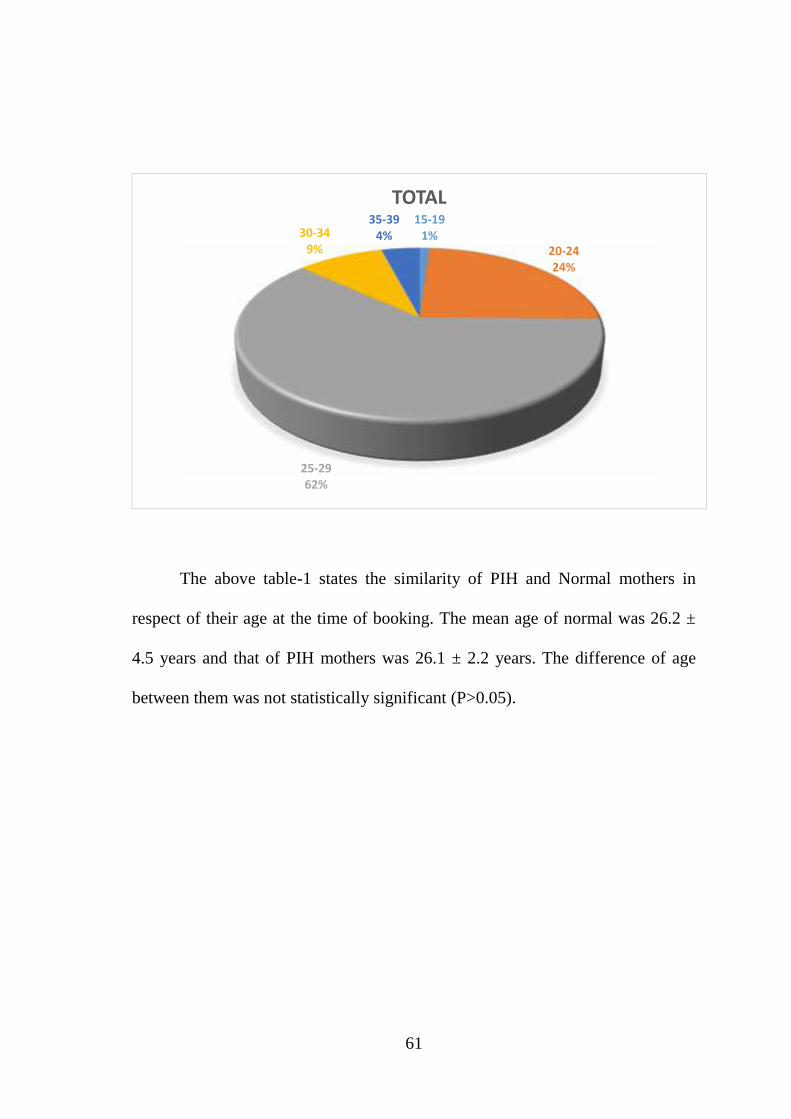
The above table-1 states the similarity of PIH and Normal mothers in
respect of their age at the time of booking. The mean age of normal was 26.2 ±
4.5 years and that of PIH mothers was 26.1 ± 2.2 years. The difference of age
between them was not statistically significant (P>0.05).
15-191%
20-2424%
25-2962%
30-349%
35-394%
TOTAL
62
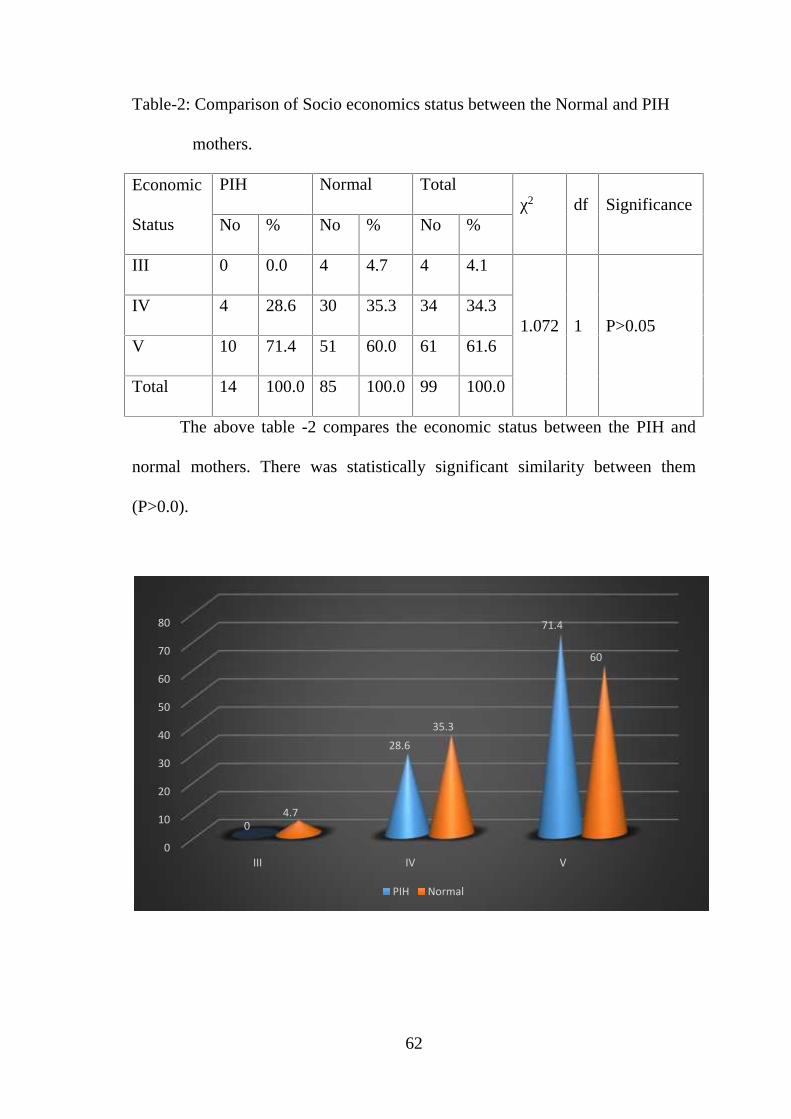
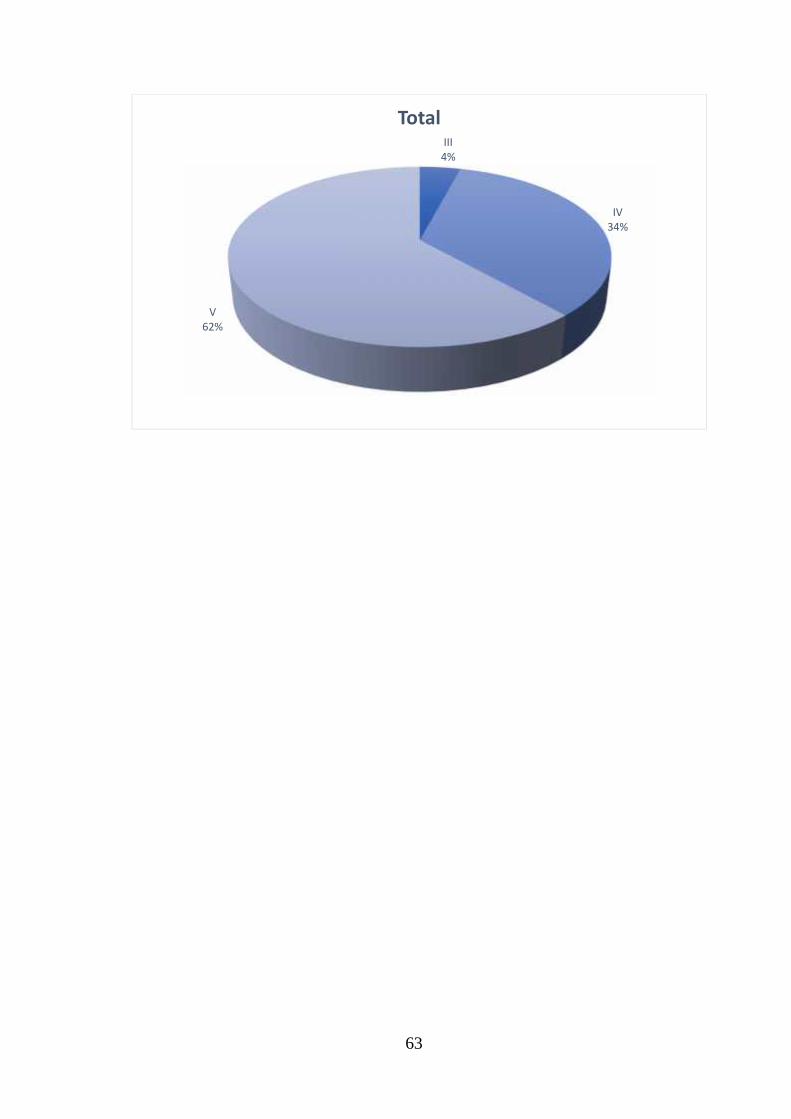
Table-2: Comparison of Socio economics status between the Normal and PIH
mothers.
Economic
Status
PIH Normal Totalχ2 df Significance
No % No % No %
III 0 0.0 4 4.7 4 4.1
1.072 1 P>0.05IV 4 28.6 30 35.3 34 34.3
V 10 71.4 51 60.0 61 61.6
Total 14 100.0 85 100.0 99 100.0
The above table -2 compares the economic status between the PIH and
normal mothers. There was statistically significant similarity between them
(P>0.0).
0
10
20
30
40
50
60
70
80
III IV V
0
28.6
71.4
4.7
35.3
60
PIH Normal
63
III4%
IV34%
V62%
Total
64
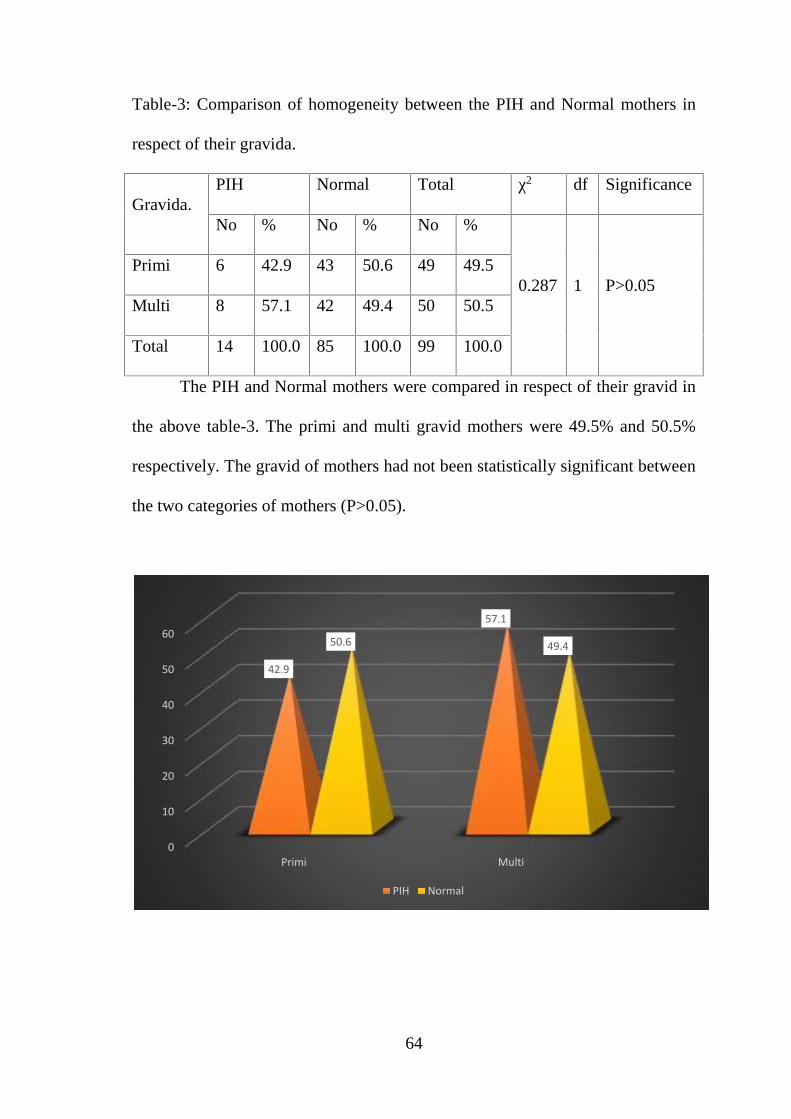
Table-3: Comparison of homogeneity between the PIH and Normal mothers in
respect of their gravida.
Gravida.PIH Normal Total χ2 df Significance
No % No % No %
0.287 1 P>0.05Primi 6 42.9 43 50.6 49 49.5
Multi 8 57.1 42 49.4 50 50.5
Total 14 100.0 85 100.0 99 100.0
The PIH and Normal mothers were compared in respect of their gravid in
the above table-3. The primi and multi gravid mothers were 49.5% and 50.5%
respectively. The gravid of mothers had not been statistically significant between
the two categories of mothers (P>0.05).
0
10
20
30
40
50
60
Primi Multi
42.9
57.1
50.6 49.4
PIH Normal
65
49%51%
Total
Primi
Multi
66
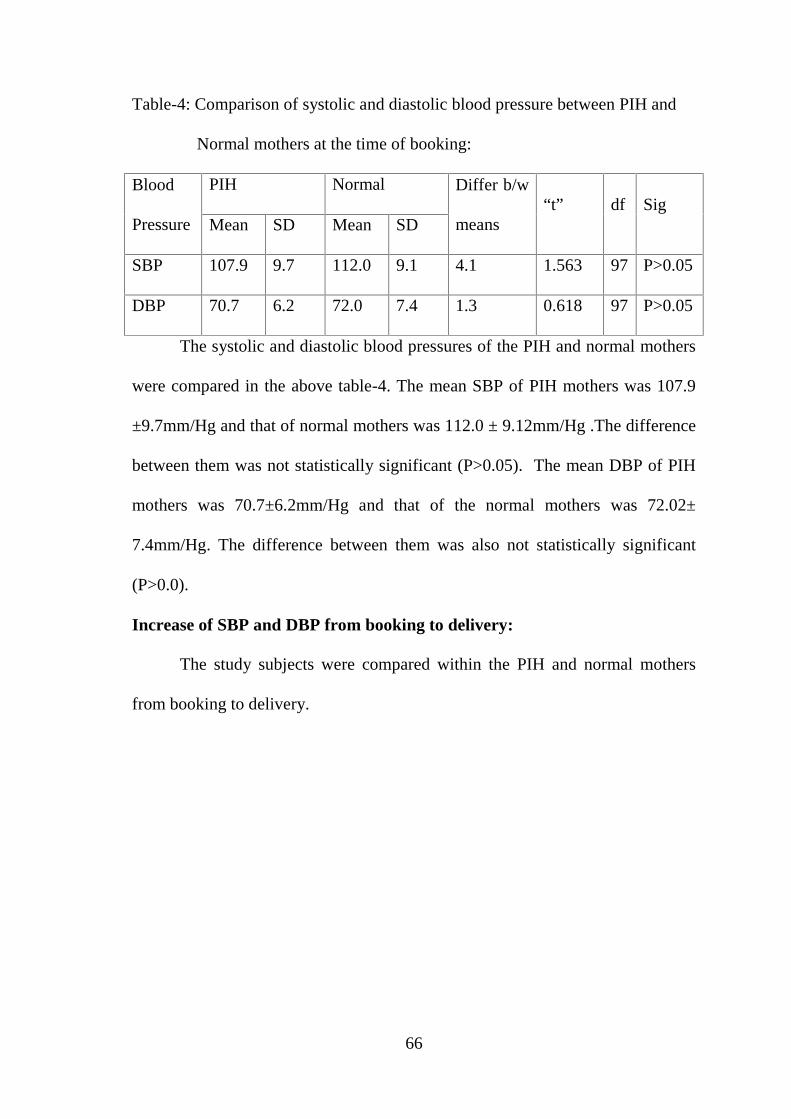
Table-4: Comparison of systolic and diastolic blood pressure between PIH and
Normal mothers at the time of booking:
Blood
Pressure
PIH Normal Differ b/w
means“t” df Sig
Mean SD Mean SD
SBP 107.9 9.7 112.0 9.1 4.1 1.563 97 P>0.05
DBP 70.7 6.2 72.0 7.4 1.3 0.618 97 P>0.05
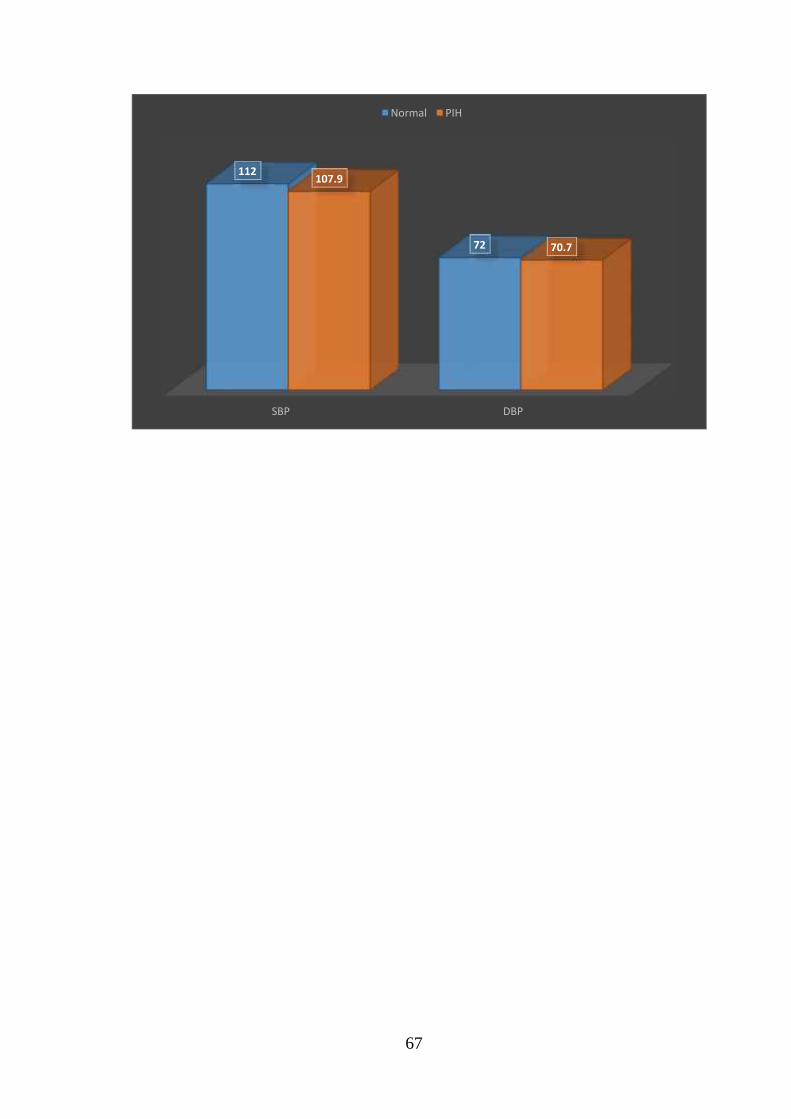
The systolic and diastolic blood pressures of the PIH and normal mothers
were compared in the above table-4. The mean SBP of PIH mothers was 107.9
±9.7mm/Hg and that of normal mothers was 112.0 ± 9.12mm/Hg .The difference
between them was not statistically significant (P>0.05). The mean DBP of PIH
mothers was 70.7±6.2mm/Hg and that of the normal mothers was 72.02±
7.4mm/Hg. The difference between them was also not statistically significant
(P>0.0).
Increase of SBP and DBP from booking to delivery:
The study subjects were compared within the PIH and normal mothers
from booking to delivery.
67
SBP DBP
112
72
107.9
70.7
Normal PIH
68
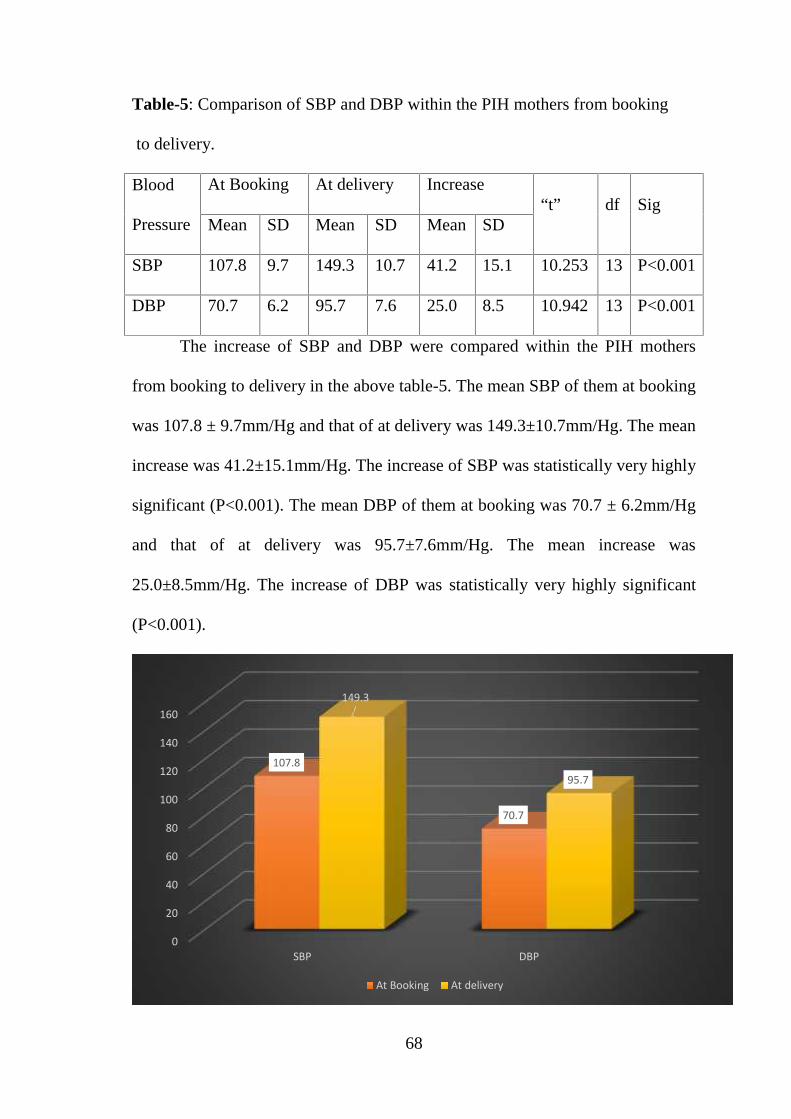
Table-5: Comparison of SBP and DBP within the PIH mothers from booking
to delivery.
Blood
Pressure
At Booking At delivery Increase“t” df Sig
Mean SD Mean SD Mean SD
SBP 107.8 9.7 149.3 10.7 41.2 15.1 10.253 13 P<0.001
DBP 70.7 6.2 95.7 7.6 25.0 8.5 10.942 13 P<0.001
The increase of SBP and DBP were compared within the PIH mothers
from booking to delivery in the above table-5. The mean SBP of them at booking
was 107.8 ± 9.7mm/Hg and that of at delivery was 149.3±10.7mm/Hg. The mean
increase was 41.2±15.1mm/Hg. The increase of SBP was statistically very highly
significant (P<0.001). The mean DBP of them at booking was 70.7 ± 6.2mm/Hg
and that of at delivery was 95.7±7.6mm/Hg. The mean increase was
25.0±8.5mm/Hg. The increase of DBP was statistically very highly significant
(P<0.001).
0
20
40
60
80
100
120
140
160
SBP DBP
107.8
70.7
149.3
95.7
At Booking At delivery
69
0
20
40
60
80
100
120
SBP DBP
112
72
116.4
74.6
At Booking At delivery
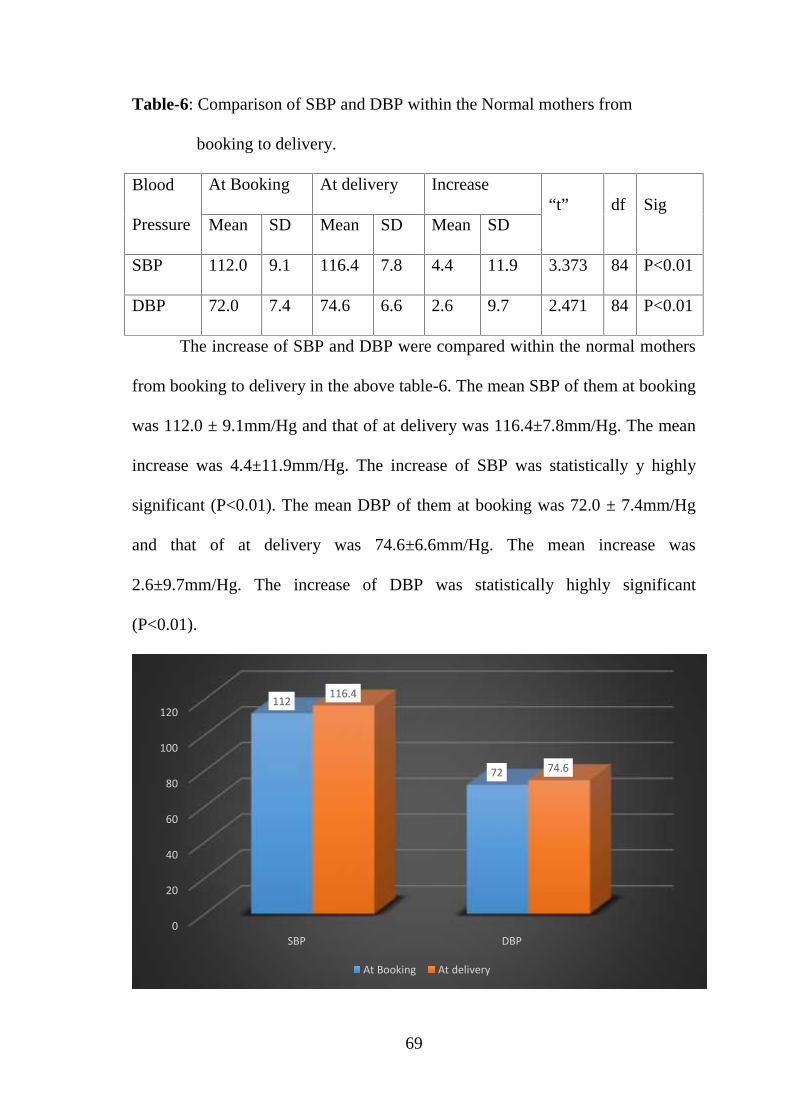
Table-6: Comparison of SBP and DBP within the Normal mothers from
booking to delivery.
Blood
Pressure
At Booking At delivery Increase“t” df Sig
Mean SD Mean SD Mean SD
SBP 112.0 9.1 116.4 7.8 4.4 11.9 3.373 84 P<0.01
DBP 72.0 7.4 74.6 6.6 2.6 9.7 2.471 84 P<0.01
The increase of SBP and DBP were compared within the normal mothers
from booking to delivery in the above table-6. The mean SBP of them at booking
was 112.0 ± 9.1mm/Hg and that of at delivery was 116.4±7.8mm/Hg. The mean
increase was 4.4±11.9mm/Hg. The increase of SBP was statistically y highly
significant (P<0.01). The mean DBP of them at booking was 72.0 ± 7.4mm/Hg
and that of at delivery was 74.6±6.6mm/Hg. The mean increase was
2.6±9.7mm/Hg. The increase of DBP was statistically highly significant
(P<0.01).
70
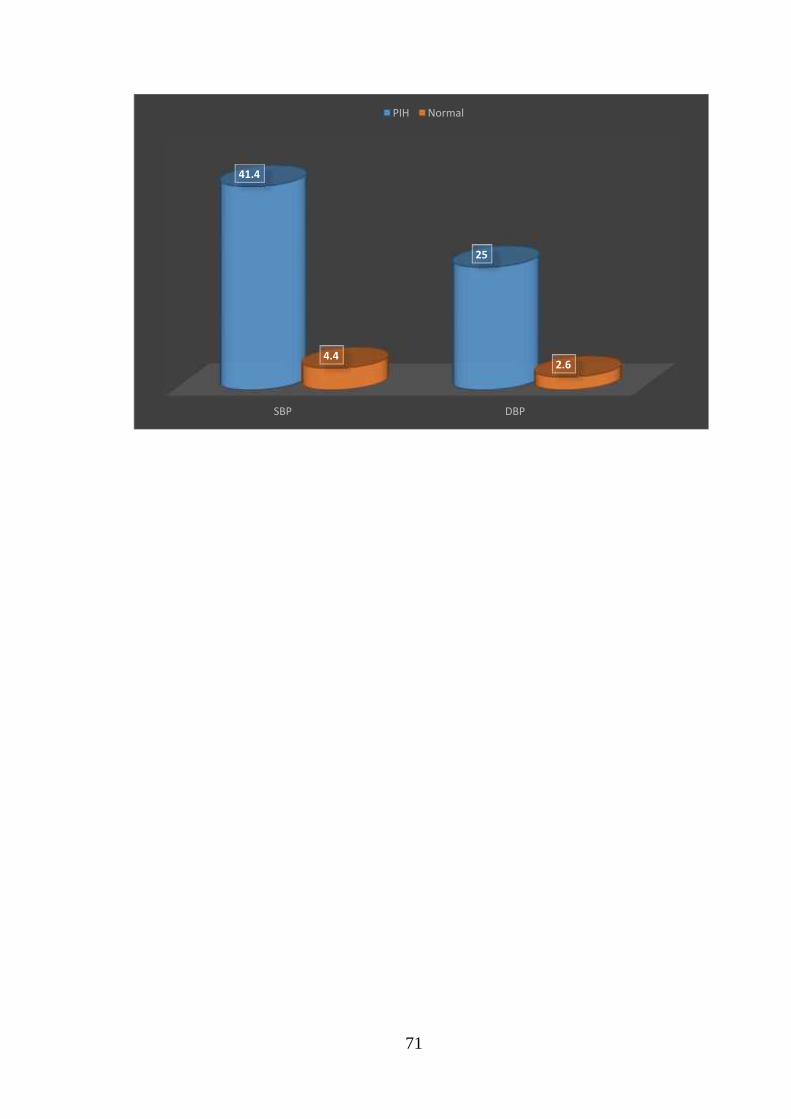
Table-7:Comparison of Increased SBP and DBPbetween PIH and Normal
mothers:
Blood
Pressure
PIH Normal Differ
b/w
means
“t” df SigMean SD Mean SD
SBP 41.4 15.1 4.4 11.9 37.0 10.385 97 P<0.001
DBP 25.0 8.5 2.6 9.7 22.4 8.167 97 P<0.001
The increase of SBP and DBP between the PIH and normal mothers was
compared in the above table-7. The mean increase of SBP of PIH mothers was
41.4±15.1mm/Hg. The mean increase of SBP of Normal mothers was
4.4±11.9mm/Hg. The difference between them was statistically very highly
significant (P<0.001). Similarly, the DBP mean increase of PIH mothers was
25.0±8.5mm/Hg. The mean increase of DBP of Normal mothers was
2.6±9.7mm/Hg. The difference between them was statistically very highly
significant (P<0.001).
Increase of Urine albumin from booking to delivery:
The incidence of urine albumin was found in the booking status in both
groups. But at delivery there was an incidence of urine albumin in both groups.
71
SBP DBP
41.4
25
4.42.6
PIH Normal
72
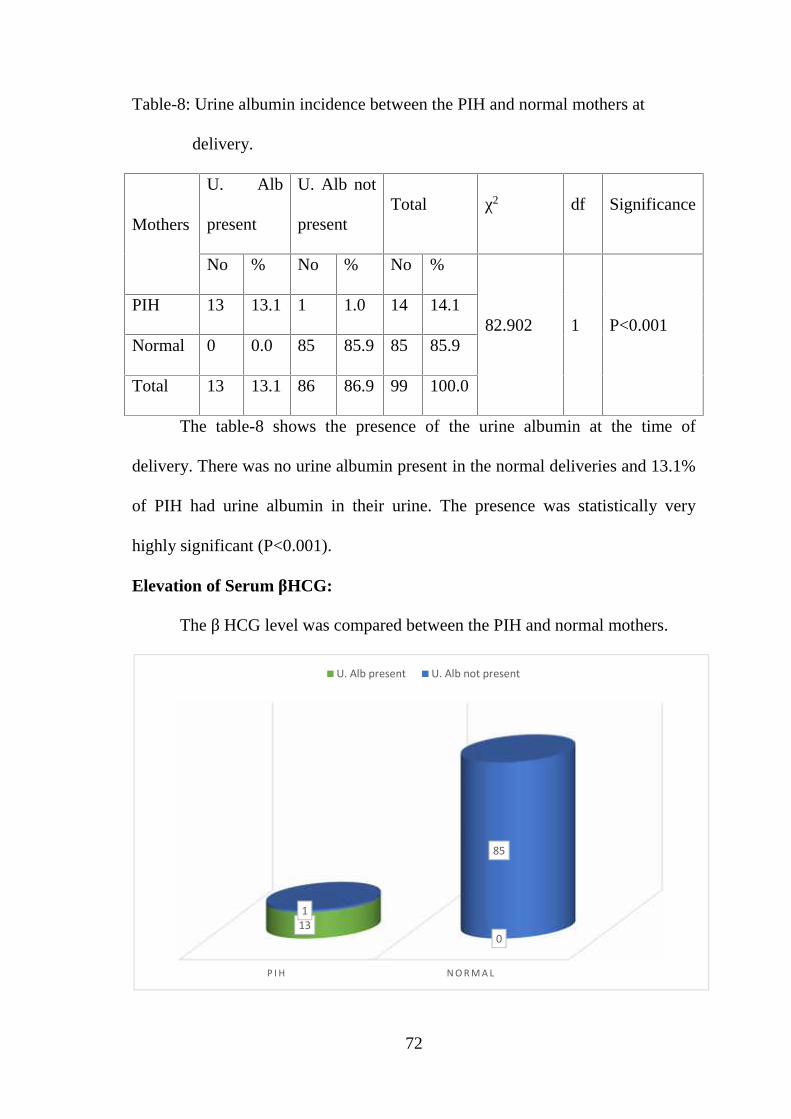
Table-8: Urine albumin incidence between the PIH and normal mothers at
delivery.
Mothers
U. Alb
present
U. Alb not
presentTotal χ2 df Significance
No % No % No %
82.902 1 P<0.001PIH 13 13.1 1 1.0 14 14.1
Normal 0 0.0 85 85.9 85 85.9
Total 13 13.1 86 86.9 99 100.0
The table-8 shows the presence of the urine albumin at the time of
delivery. There was no urine albumin present in the normal deliveries and 13.1%
of PIH had urine albumin in their urine. The presence was statistically very
highly significant (P<0.001).
Elevation of Serum βHCG:
The β HCG level was compared between the PIH and normal mothers.
P I H N O R M A L
130
1
85
U. Alb present U. Alb not present
73
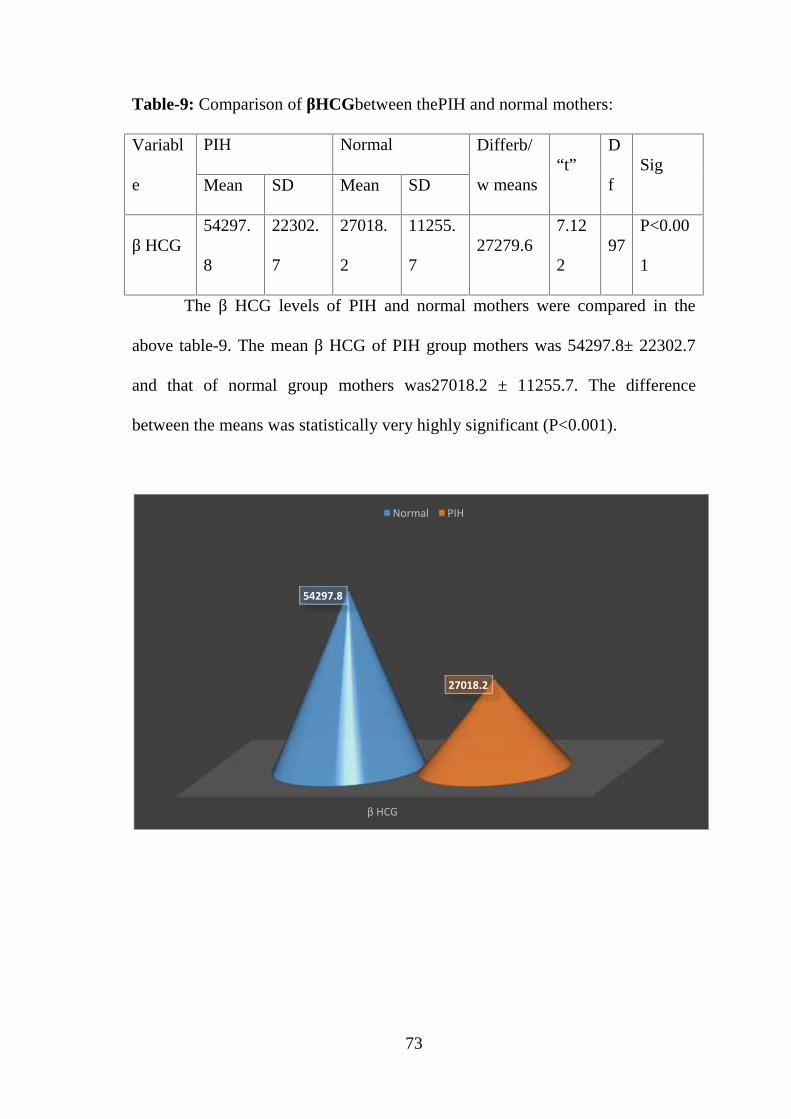
Table-9: Comparison of βHCGbetween thePIH and normal mothers:
Variabl
e
PIH Normal Differb/
w means“t”
D
fSig
Mean SD Mean SD
β HCG54297.
8
22302.
7
27018.
2
11255.
727279.6
7.12
297
P<0.00
1
The β HCG levels of PIH and normal mothers were compared in the
above table-9. The mean β HCG of PIH group mothers was 54297.8± 22302.7
and that of normal group mothers was27018.2 ± 11255.7. The difference
between the means was statistically very highly significant (P<0.001).
β HCG
54297.8
27018.2
Normal PIH
74
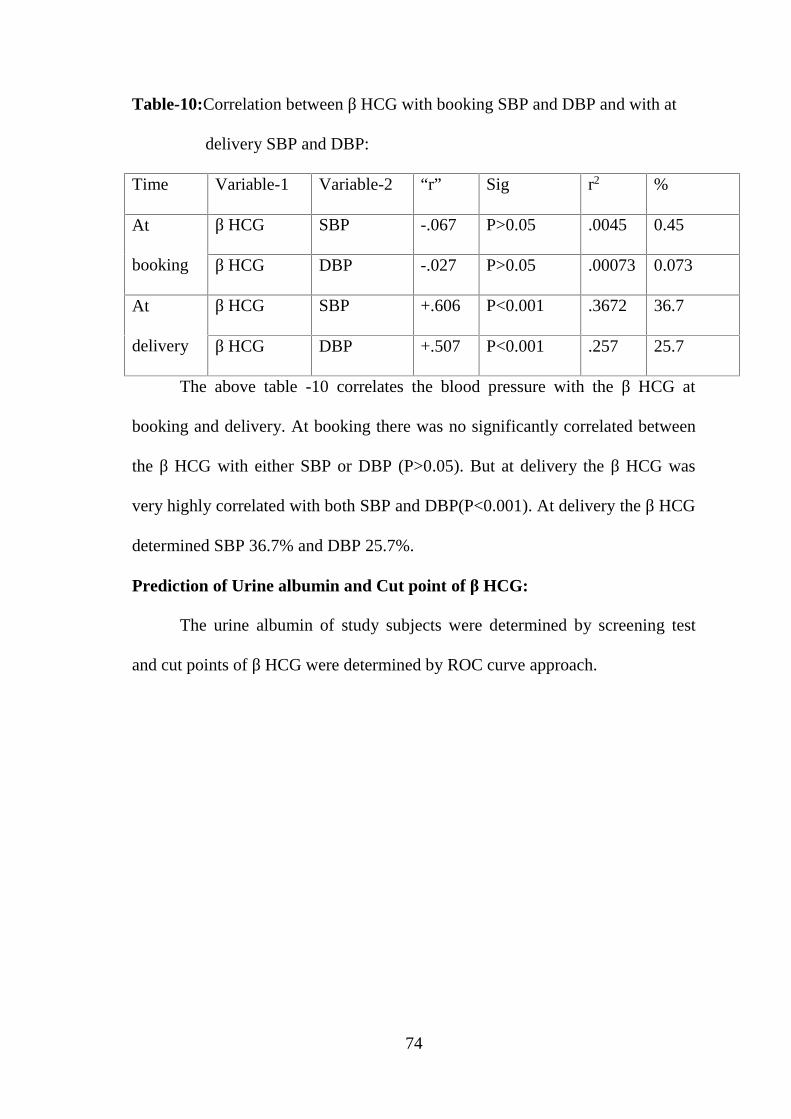
Table-10:Correlation between β HCG with booking SBP and DBP and with at
delivery SBP and DBP:
Time Variable-1 Variable-2 “r” Sig r2 %
At
booking
β HCG SBP -.067 P>0.05 .0045 0.45
β HCG DBP -.027 P>0.05 .00073 0.073
At
delivery
β HCG SBP +.606 P<0.001 .3672 36.7
β HCG DBP +.507 P<0.001 .257 25.7
The above table -10 correlates the blood pressure with the β HCG at
booking and delivery. At booking there was no significantly correlated between
the β HCG with either SBP or DBP (P>0.05). But at delivery the β HCG was
very highly correlated with both SBP and DBP(P<0.001). At delivery the β HCG
determined SBP 36.7% and DBP 25.7%.
Prediction of Urine albumin and Cut point of β HCG:
The urine albumin of study subjects were determined by screening test
and cut points of β HCG were determined by ROC curve approach.
75
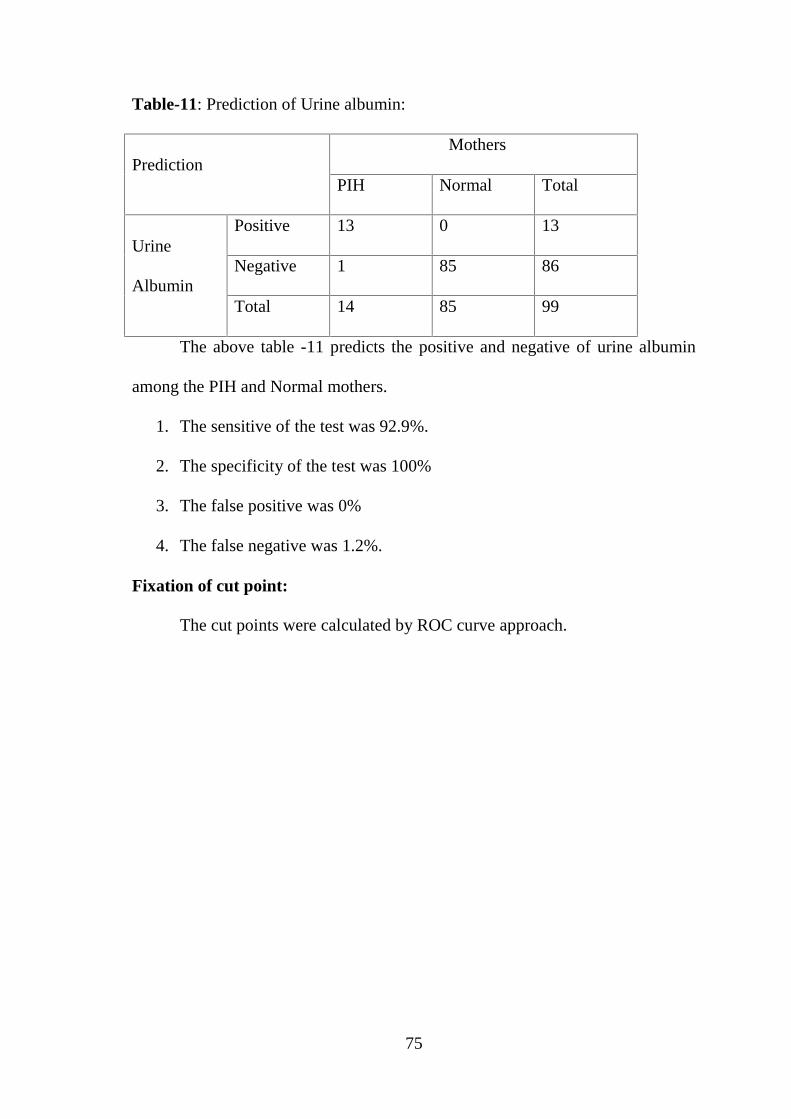
Table-11: Prediction of Urine albumin:
PredictionMothers
PIH Normal Total
Urine
Albumin
Positive 13 0 13
Negative 1 85 86
Total 14 85 99
The above table -11 predicts the positive and negative of urine albumin
among the PIH and Normal mothers.
1. The sensitive of the test was 92.9%.
2. The specificity of the test was 100%
3. The false positive was 0%
4. The false negative was 1.2%.
Fixation of cut point:
The cut points were calculated by ROC curve approach.
76
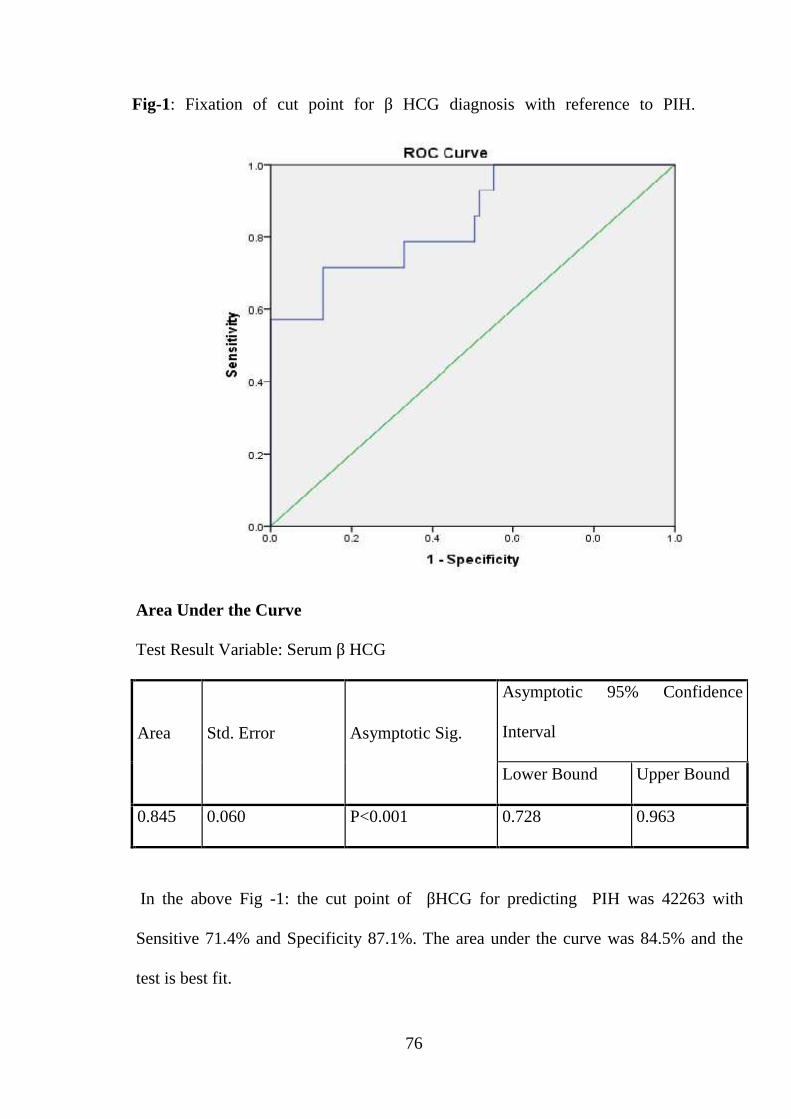
Fig-1: Fixation of cut point for β HCG diagnosis with reference to PIH.
Area Under the Curve
Test Result Variable: Serum β HCG
Area Std. Error Asymptotic Sig.
Asymptotic 95% Confidence
Interval
Lower Bound Upper Bound
0.845 0.060 P<0.001 0.728 0.963
In the above Fig -1: the cut point of βHCG for predicting PIH was 42263 with
Sensitive 71.4% and Specificity 87.1%. The area under the curve was 84.5% and the
test is best fit.
77
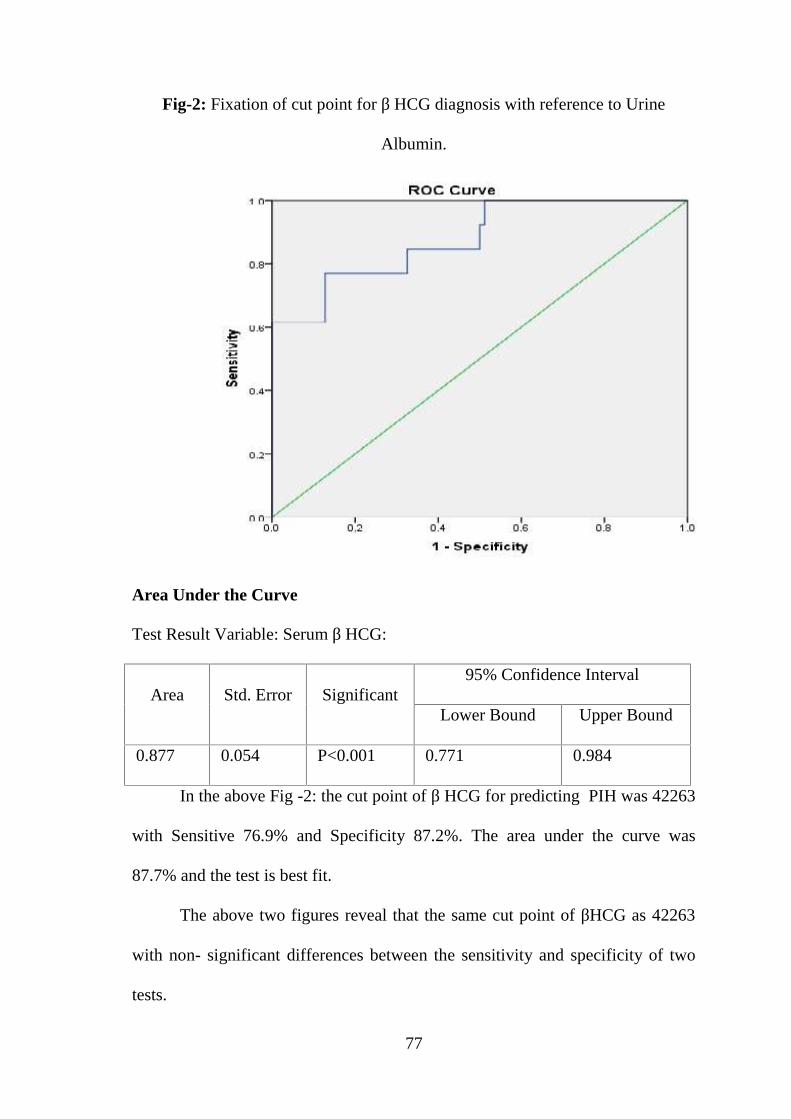
Fig-2: Fixation of cut point for β HCG diagnosis with reference to Urine
Albumin.
Area Under the Curve
Test Result Variable: Serum β HCG:
Area Std. Error Significant95% Confidence Interval
Lower Bound Upper Bound
0.877 0.054 P<0.001 0.771 0.984
In the above Fig -2: the cut point of β HCG for predicting PIH was 42263
with Sensitive 76.9% and Specificity 87.2%. The area under the curve was
87.7% and the test is best fit.
The above two figures reveal that the same cut point of βHCG as 42263
with non- significant differences between the sensitivity and specificity of two
tests.
78
Maternal outcome of study subjects:
The maternal outcomes of subjects namely PIH and normal mothers were
compared in the following tables.
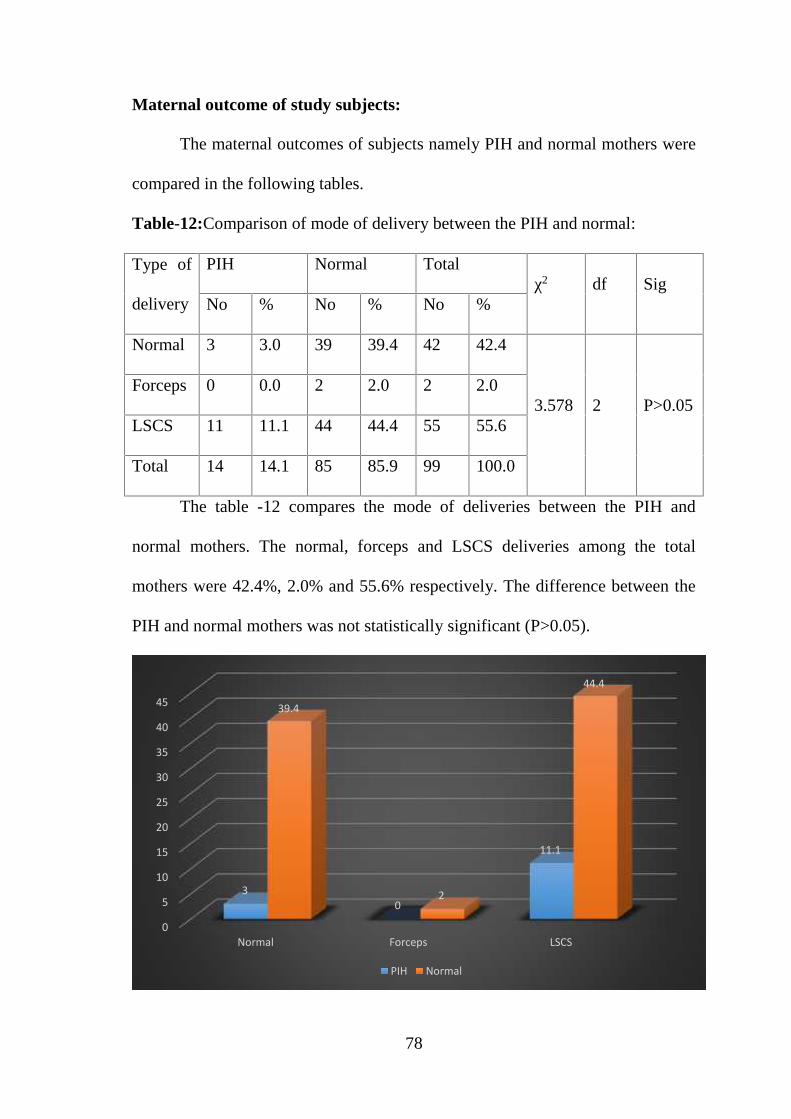
Table-12:Comparison of mode of delivery between the PIH and normal:
Type of
delivery
PIH Normal Totalχ2 df Sig
No % No % No %
Normal 3 3.0 39 39.4 42 42.4
3.578 2 P>0.05Forceps 0 0.0 2 2.0 2 2.0
LSCS 11 11.1 44 44.4 55 55.6
Total 14 14.1 85 85.9 99 100.0
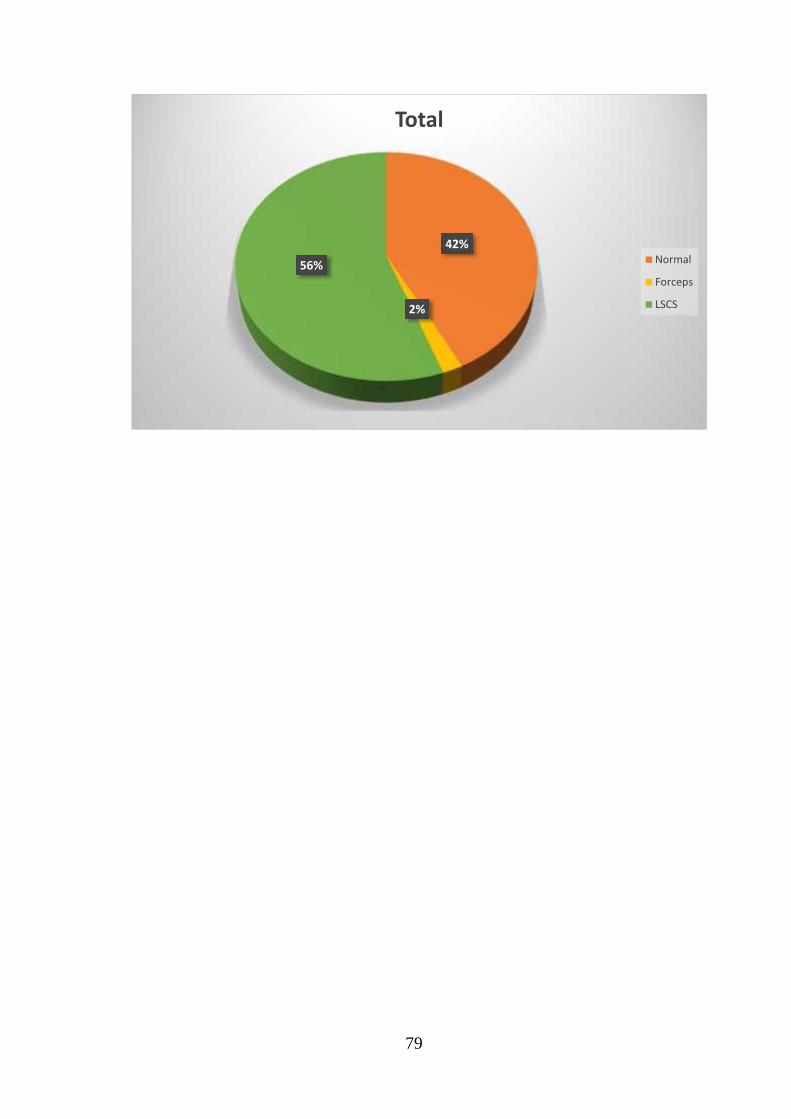
The table -12 compares the mode of deliveries between the PIH and
normal mothers. The normal, forceps and LSCS deliveries among the total
mothers were 42.4%, 2.0% and 55.6% respectively. The difference between the
PIH and normal mothers was not statistically significant (P>0.05).
0
5
10
15
20
25
30
35
40
45
Normal Forceps LSCS
30
11.1
39.4
2
44.4
PIH Normal
79
42%
2%
56%
Total
Normal
Forceps
LSCS
80
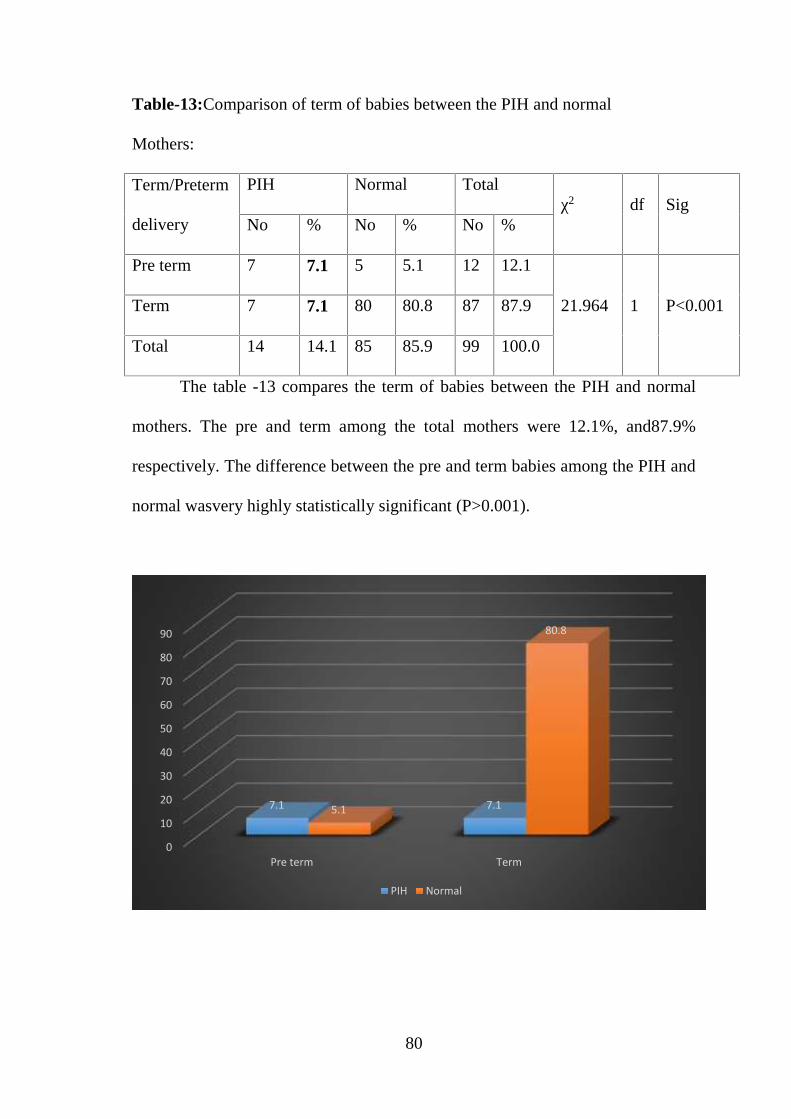
Table-13:Comparison of term of babies between the PIH and normal
Mothers:
Term/Preterm
delivery
PIH Normal Totalχ2 df Sig
No % No % No %
Pre term 7 7.1 5 5.1 12 12.1
21.964 1 P<0.001Term 7 7.1 80 80.8 87 87.9
Total 14 14.1 85 85.9 99 100.0
The table -13 compares the term of babies between the PIH and normal
mothers. The pre and term among the total mothers were 12.1%, and87.9%
respectively. The difference between the pre and term babies among the PIH and
normal wasvery highly statistically significant (P>0.001).
0
10
20
30
40
50
60
70
80
90
Pre term Term
7.1 7.15.1
80.8
PIH Normal
81
12%
88%
Total
Pre term
Term
82
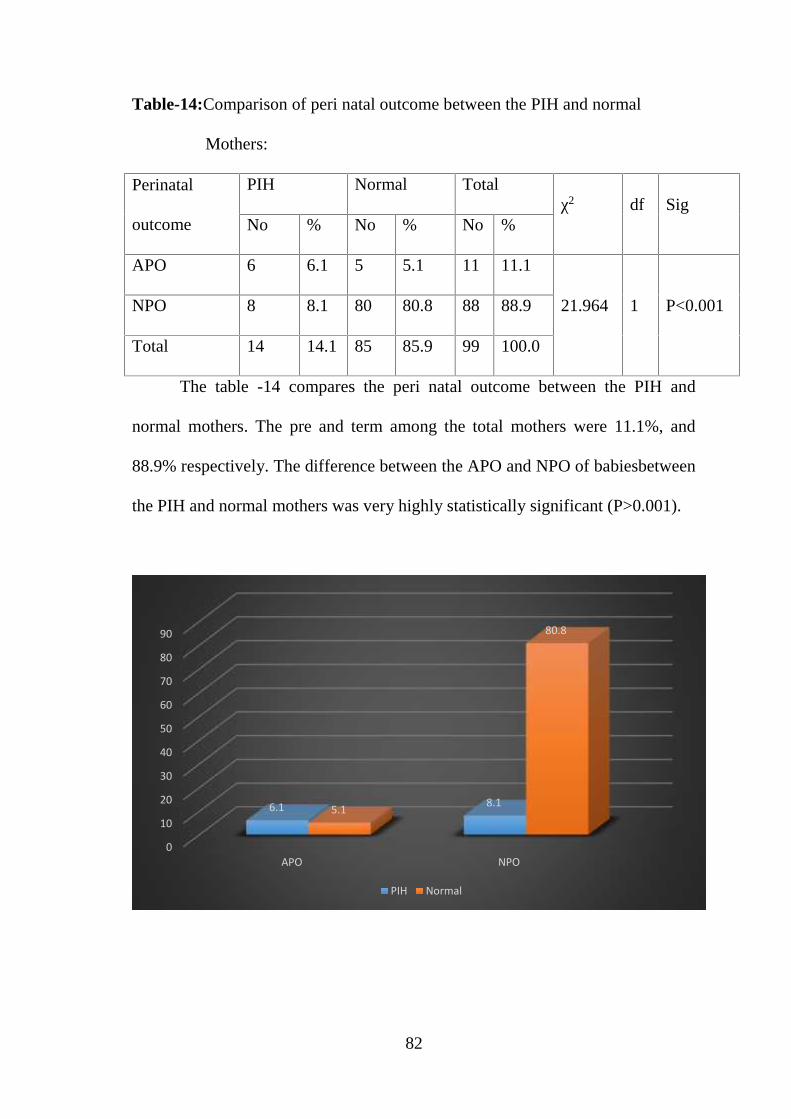
Table-14:Comparison of peri natal outcome between the PIH and normal
Mothers:
Perinatal
outcome
PIH Normal Totalχ2 df Sig
No % No % No %
APO 6 6.1 5 5.1 11 11.1
21.964 1 P<0.001NPO 8 8.1 80 80.8 88 88.9
Total 14 14.1 85 85.9 99 100.0
The table -14 compares the peri natal outcome between the PIH and
normal mothers. The pre and term among the total mothers were 11.1%, and
88.9% respectively. The difference between the APO and NPO of babiesbetween
the PIH and normal mothers was very highly statistically significant (P>0.001).
0
10
20
30
40
50
60
70
80
90
APO NPO
6.1 8.15.1
80.8
PIH Normal
83
11%
89%
Total
APO
NPO
84
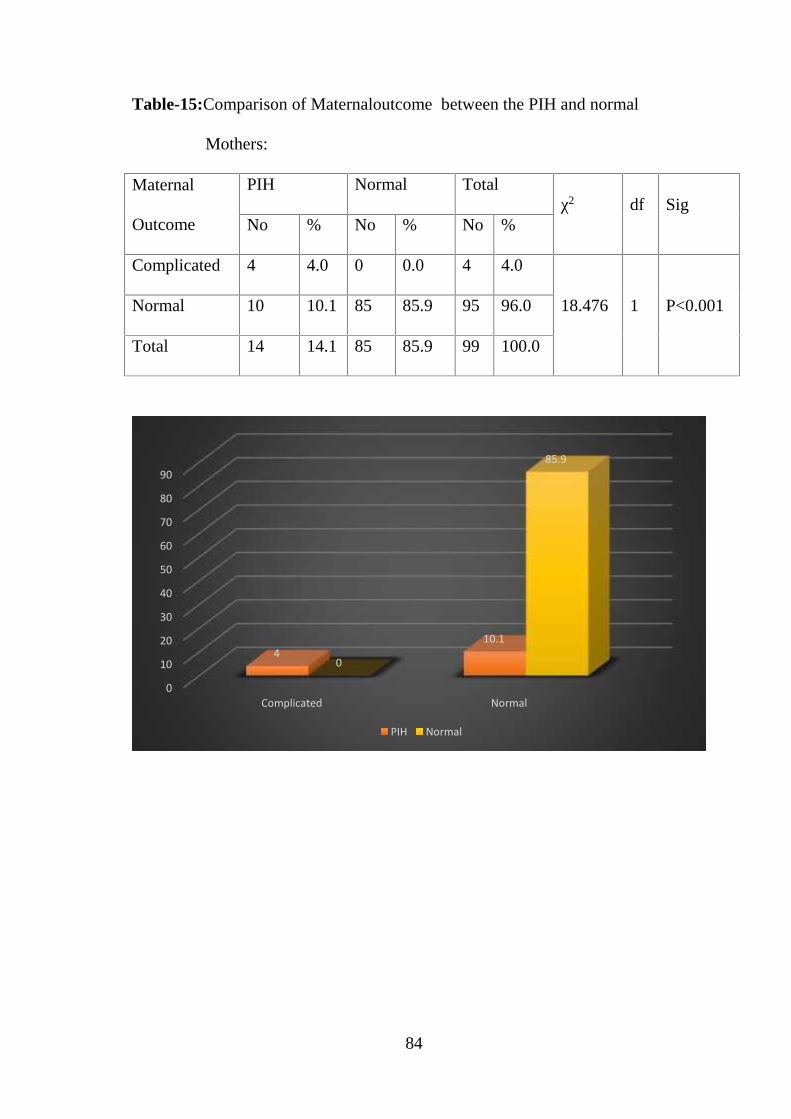
Table-15:Comparison of Maternaloutcome between the PIH and normal
Mothers:
Maternal
Outcome
PIH Normal Totalχ2 df Sig
No % No % No %
Complicated 4 4.0 0 0.0 4 4.0
18.476 1 P<0.001Normal 10 10.1 85 85.9 95 96.0
Total 14 14.1 85 85.9 99 100.0
0
10
20
30
40
50
60
70
80
90
Complicated Normal
410.1
0
85.9
PIH Normal
85
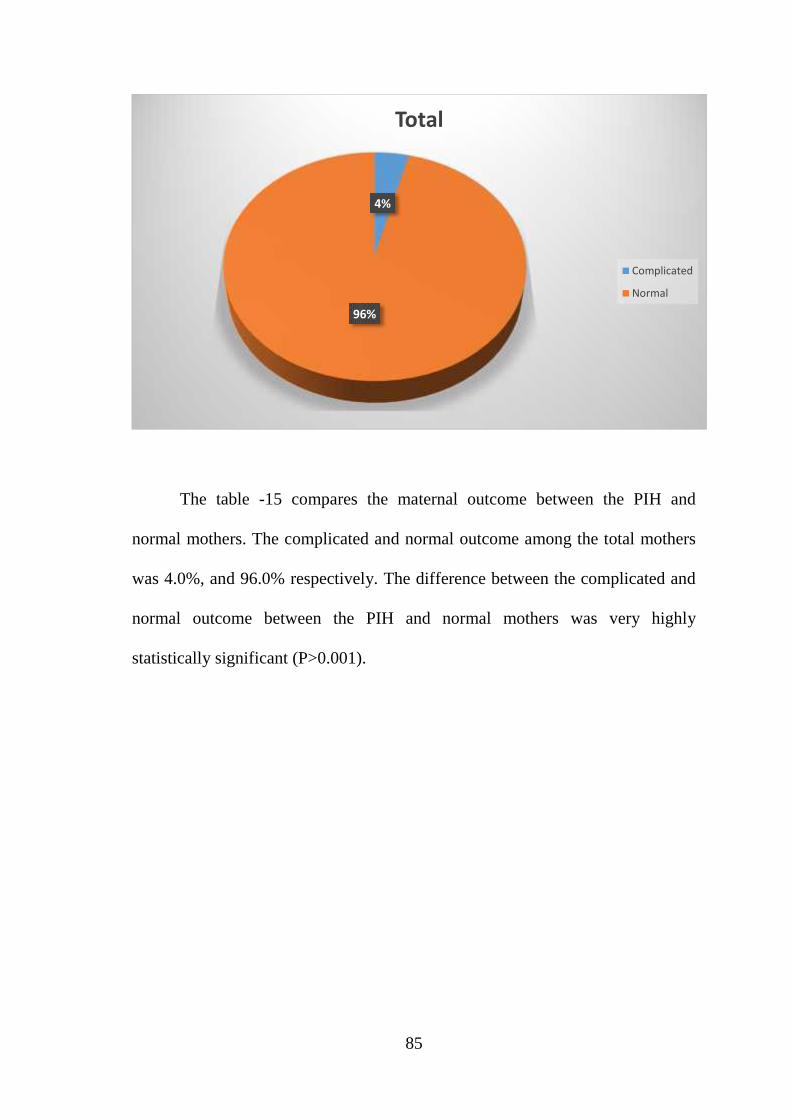
The table -15 compares the maternal outcome between the PIH and
normal mothers. The complicated and normal outcome among the total mothers
was 4.0%, and 96.0% respectively. The difference between the complicated and
normal outcome between the PIH and normal mothers was very highly
statistically significant (P>0.001).
4%
96%
Total
Complicated
Normal
86
DISCUSSION
1. The PIH and normal mothers of study were not differed in respect of
their demographic, economic, gravid status and blood pressure level at
the time of booking was not significantly differed.
2. The increase of β HCG among the PIH mothers was significantly
greater than the counterpart of normal mothers.
3. The urine albumin all subject was nil at the booking and the same was
present among the PIH cases.
4. The cut points β HCG by ROC curve.
5. The maternal outcome by means of mode of delivery was not
significant.
6. The number of preterm babies and abnormal perinatal outcome was
significantly more in PIH mothers than the normal mothers.
7. The maternal complications among the PIH mothers were significantly
more than the normal mothers.
The prediction of PIH through β HCG which is simple procedure will help
the mothers early detection and treatment.
87
CONCLUSION
This study was done to examine the possibility of using serum beta hcg to
predict PIH.
100 pregnant women between 13-20 weeks gestation with singleton
pregnancy were selected randomly and serum β hcg were estimated.
Regular follow up of the cases was done till delivery.
Patients who have elevated β hcg levels, in second trimester are at
increased risk of developing PIH.
The mean β HCG of PIH group mothers was 54297.8± 22302.7 and that
of normal group mothers was27018.2 ± 11255.7. The difference between
the means was statistically very highly significant (P<0.001).
For any test to be used as a screening tests it should have good sensitivity,
specificity and positive predictive value.
This study had Sensitivity – 71.4% ,Specificity –87.1% .
Hence instead of single serum marker, it is advised to do multiple serum
analysis, such as AFP, uterine artery Doppler (bilateral notching), along
with βhcg, which has the potential to minimize unwarranted
inconvenience and morbidity and mortality associated with false positive
results.
According to RCOG ,2008 NICE GUIDELINES ,further research using large
prospective studies should be conducted into the effectiveness and cost
effectiveness of using alpha fetoprotein ,beta human chorionic gonadotropin ,

88
fetal DNA in maternal blood and uterine artery dopplers ,or potentially a
combination of these ,to detect women at risk of developing preeclampsia.
89
SUMMARY
This study was done to examine the possibility of using serum beta hcg to
predict PIH.
100 pregnant patients were included in the study between 13-20 weeks of
getational age with singleton pregnancy.
Regular follow up of the cases was done till delivery.
Systolic, diastolic, mean blood pressure at the time of booking between
PIH and normotensive patients did not vary significantly.
From this study we found that βhcg levels were elevated in patients
having preeclampsia,compared with patients who remained normotensives
throughout pregnancy, but while significant effects reported in this study are too
modest compared with natural variability and also sensitivity and positive
predictive value of βhcg are too low to be useful as mass screening marker on its
own and therefore it should be combined with other serum markers and
ultrasound parameters like Doppler study of uterine vessels, which will help in
improving its role as a screening tool.
BIBLIOGRAPHY
1. James PR, Nelson-Piercy. Management of Hypertension before,during, and after
pregnancy. Heart. 2004;90:1499-1504
2. Khan KS,Wojdyla D,Say L et al.WHO analysis of causes of maternal death: a
systematic review. Lancet.2006;367:1066-1074.
3. American College of obstetricians &Gynaecologists. Diagnosis and Management of
preeclampsia and Eclampsia. Practice Bulletin No.22. Washington. DC: ACOG,
January 2002
4. Brown MA, Reiter L, et al. Measuring blood pressure in pregnant women: a comparison
of direct and indirect methods. Am J Obstet Gynecol. 1994;171:661-667 5)
5. NHBPEP (National High Blood Pressure Education program) workingDroup on High
Blood pressure. Report of the National High Blood Pressure in Education program
working Group in High Blood pressure in pregnancy. Am J obstetGynecol
2000:183:SI-22
6. National Institute of Health and Clinical excellence. 2010.Hypertension in pregnancy.
The management of hypertensive disorders during pregnancy.CG no 107. London:
National Institute of Health and Clinical excellence.
7. Hauth JC,Ewell MG, Levine RL, et al.Pregnancy outcome in healthy nulliparous
women who subsequently developed hypertension. Obstet Gynecol.2000;95:24-48.
8. Sibai B, Dekker G, Kupferminc M: Preeclampsia. Lancet. 2005;365:785-799
9. Williams Obstetrics 24 th edition. 731-735.
10. Redman CWG, Sargent IL, Roberts JM. Immunology of abnormal pregnancy and
preeclampsia. In Lindheimer MD, Robers JM, Cunningham FG (eds). Cheley’s
Hypertensive disorders of pregnancy, 3rd ed. New York:Elseiver,2009:129
11. Lindheimer MD, Taylor RN, Cunningham FG, et al: Introduction,
history,controversies, and definitions. In Taylor RN, Roberts JM, Cunningham FG
(eds): Chesley’s Hypertensive Disorders in Pregnancy, 4th ed, Amsterdam, Academic
Press, 2014
12. Fisher S, Roberts JM: The placenta in normal pregnancy and preeclampsia. In Taylor
RN, Roberts JM, Cunningham FG (eds): Chesley’s Hypertensive Disorders in
Pregnancy, 4th ed. Amsterdam, Academic Press, 2014
13. Borowski K, Kair L, Zeng S, et al: Lack of association of FAS gene and
preeclampsia.Abstract No 706. Presented at the 29th Annual Meeting of theSociety for
Maternal-Fetal Medicine, January 26–31, 2009
14. Buurma AJ, Turner RJ, Driessen JH, et al: Genetic variants in pre-eclampsia:level,
urinary excretion and metabolic productionof cGMP during gestation in rats. Am J
Physiol 257:R847, 1989
15. Staines-Urias E, Paez MC, Doyle P, et al: Genetic association studies in
preeclampsia:systematic meta-analyses and field synopsis. Int J Epidemiol41(6):1764,
2012
16. Ward K, Taylor RN: Genetic factors in the etiology of preeclampsia. In Taylor RN,
Roberts JM, Cunningham FG (eds): Chesley’s Hypertensive Disorders
17. Loisel DA, Billstrand C, Murray K, et al: The maternal HLA-G 1597 DC null mutation
is associated with increased risk of pre-eclampsia and reduced HLA-G expression
during pregnancy in African-American women. Mol Hum Reprod 19(3):144, 2013
18. Bdolah Y, Palomaki GE, Yaron Y, et al: Circulating angiogenic proteins in trisomy 13.
Am J Obstet Gynecol 194(1):239, 2006
19. Redman CW, Tannetta DS, Dragovic RA, et al: Review: does size matter? Placental
debris and the pathophysiology of pre-eclampsia. Placenta 33(Suppl):S48, 2012
20. Redman CW, Sargent IL, Taylor RN: Immunology of abnormal pregnancy and
preeclampsia. In Taylor RN, Roberts JM, Cunningham FG (eds): Chesley’s
Hypertensive Disorders in Pregnancy, 4th ed. Amsterdam, Academic Press, 2014
21. Erlebacher A: Immunology of the maternal-fetal interface. Annu Rev Immunol 31:387,
2013
22. Hinselmann H:Die Eklampsie. Bonn, F Cohen, 1924
23. Karim R, Assali NS: Pressor response to angiotensin in pregnant and nonpregnant
women. Am J Obstet Gynecol 82:246, 1961
24. Raab W, Schroeder G, Wagner R, et al: Vascular reactivity and electrolytes innormal
and toxemic pregnancy. J Clin Endocrinol 16:1196, 1956
25. Talledo OE, Chesley LC, Zuspan FP: Renin-angiotensin system in normal andtoxemic
pregnancies, 3. Differential sensitivity to angiotensin II and norepinephrinein toxemia
of pregnancy. Am J Obstet Gynecol 100:218, 1968
26. Gant NF, Chand S, Worley RJ, et al: A clinical test useful for predicting the
development of acute hypertension in pregnancy. Am J Obstet Gynecol120:1, 1974
27. Davidge S, de Groot C, Taylor RN: Endothelial cell dysfunction and oxidative stress.
In Taylor RN, Roberts JM, Cunningham FG (eds): Chesley’s Hypertensive Disorders
in Pregnancy, 4th ed. Amsterdam, Academic Press, 2014
28. Spitz B, Magness RR, Cox SM: Low-dose aspirin. I. Effect on angiotensin II pressor
responses and blood prostaglandin concentrations in pregnant women sensitive to
angiotensin II. Am J Obstet Gynecol 159(5):1035, 1988
29. Conrad KP, Vernier KA: Plasma level, urinary excretion and metabolic production of
cGMP duringgestation in rats.Am J Physiol257:R 847, 1989
30. Ajne G, Wolff K, Fyhrquist F, et al: Endothelin converting enzyme (ECE) activity in
normal pregnancy and preeclampsia. Hypertens Pregnancy 22:215, 2003
31. Sagsoz N, Kucukozkan T: The effect of treatment on endothelin-1 concentration and
mean arterial pressure in preeclampsia and eclampsia. Hypertens Pregnancy 22:185,
2003
32. Williams Obstetrics 24th edition 736-738.
33. Silver HM, Seebeck M, Carlson R: Comparison of total blood volume in normal,
preeclamptic, and non-proteinuric gestational hypertensive pregnancy by simultaneous
measurement of redblood cell and plasma volumes. Am J Obstet Gynecol 179:87, 1998
34. Heilman L, Rath W, Pollow K. Hemostatic abnormalities in patients with severe
preeclampsia. Clin Appl Thromb Hemost 2007;13:285
35. Cunningham FG, Lowe T,Guss S et al. Erythrocyte morphology in women with severe
pre eclampsia and eclampsia.Am J Obstet Gynecol 1985;153:358
36. Brubaker DB, Ross MG, Marinoff D: The function of elevated plasma fibronectin in
preeclampsia. Am J Obstet Gynecol 166:526, 1992
37. Calson KL, Bader CL: Ruptured subcapsular liver hematoma in pregnancy: a case
report of nonsurgical management.Am J Obstet Gynecol 190:558,2004
38. Lindheimer MD. Conrad K, Karumanchi SA :Renal physiology and disease in
pregnancy. In Alpern RJ, Hebert SC (eds): Seldin and Giebisch’s The Kidney:
Physiology and Pathophysiology, 4th ed. New York, Elsevier,2008a, p2339
39. Taufield PA, Ales KL, Resnick LM, et al: Hypocalciuria in preeclampsia. N Engl J Med
316:715, 1987
40. a) Majumdar S, Dasgupta H, Bhattacharya K, Bhattacharya A. A study of placenta in
normal and hypertensive pregnancies. J Anat Soc India 2005;54(2): 1-9.
40. b)DiFederico E, Genbacev O, Fisher SJ: Preeclampsia is associated with widespread
apoptosis of placental cytotrophoblasts within the uterine wall. Am J Pathol 155:293, 1999
41. Trommer BL, Homer D, Mikhael MA: Cerebral vasospasm and eclampsia.Stroke
19:326, 1988
42. Hauser RA, Lacey DM, Knight MR: Hypertensive encephalopathy. Arch Neuro
45:1078, 1988
43. Topuz S, Kalelioglu I, Iyibozkurt AC, Akhan S,Has R, Tunaci M, Ibrahimoglu L.
Cranial imaging spectrum in hypertensive disease of pregnancy, Clin Exp Obstet
Gynecol 2008: 35(3):194-97
44. a)Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia.
Obstet Gynaecol. 2003:102:181-192
44-b) Barron WM, Heckerling P, Hibbard JU, et al. Reducing unnecessary coagulation
testing in hypertensive disorders of pregnancy. Obstet Gynecol. 1999;94:364-370.
45. a) The management of hypertensive disorders during pregnancy. NICE clinical
guideline 107, January 2011. National Institute of Clinical Excellence
45-b)American College of Obstetricians and Gynecologists: Antepartum fetal surveillance.
Practice Bulletin No. 9, October 1999, Reaffirmed 2012 a meta-analysis. Hum Reprod
Update 19(3):289, 2013
46. American College of Obstetricians and Gynecologists. Diagnosis and Management of
Preeclampsia and Eclampsia. Practice Bulletin No.33.Washington, DC:ACOG,
January 2002
47. Royal College of obstetricians and Gynaecologists. The management of severe pre-
eclampsia/ eclampsia. Evidence Based Clinical Guide line No 10 (A) . London: RCOG
Press: 2006, Reviewed in 2010
48. SOGC practice Guideline No. 206, March 2008. Diagnosis, evaluation and
management of hypertensive disorders os pregnancy, J obstetGynecol can. Vol 30(3),
Supplement 1.
49. Magee LA.Cham C,Waterman EJ, et al. Hydralazine for treatment of severe
hypertension in pregnancy: a meta –analysis. Brit Med.J 2003-327:955
50. RCOG.2010.Greentop Guideline No .7.Antenatal corticosteroids to reduce neonatal
morbidity and mortality.
51. Sibai BM. The HELLP syndrome: much also about nothing?. JOG 1990; 162:311-316.
52. Sibai BM: Diagnosis Differential diagnosis and management of eclampsia. Obstet
Gynecol. 2005: 105:402-410
53. Managing eclampsia. Educational material for teachers of midwifery. World Health
Organization 2008.
53a) Magpie Triaj Collaborative Group: Do Women with pre-eclampsia, and their babies,
benefilt from magnesium sulfate? The Magpie Trial: A randomized Placebo-controlled trial
Lancet 2002:359 1877-1890.
53b) Eclampsia Trial collaborative Group whichanticonulsant for women with eclampsia?
Eclampsia? Evidence from the collaborative eclampsia trial Lancet. 1995-345: 1455-1462
53c) SibaiBM.Magnesiua. Sutfate is the ideal anticonvulsant in pre-eclampsia- eclampsia
Am J obstetGynaecol 1990:162:1141-1145
54. National Institute of Health and Clinical Excellence.2010. Hypertension in pregnancy.
The management of hypertensive disorders during pregnancy. CG no 107.London:
National Institute of Health and Clinical Excellence.
55. Kaur D, saini AS, kaurA, et al Evaluatioin of isometic exercise (hand –grip test) as a
predictor of PIH J obsterGynecol India 2003:53: 115-117
56. Kar J. ShrivastavaK.Mishra RK. et al Role of urinary calcium creatinine ratio
inpredicting pregnancy induced hypertension. J obstet Gyncol India 2002;52(2):39-41
57. Desai P.Malik S. Serum urinary calcium creatinine ratio in predicting pregnancy
induced hypertension How useful? J Obstet Gynecol India 2001;51(4):61-63
58. Holzgreve W, Ghezzi F, Di Naro E, et al: Disturbed fetomaternal cell traffic in
preeclampsia. Obstet Gynecol 91:669, 1998
59. Conde-Agudelo A, Romero R,Roberts JM :Tests to predict pre eclampsia.In Taylor RN
, Roberts JM, Cunningham FG(eds): Chesley’s Hypertensive Disorders in
Pregnancy,4th ed.Amsterdam, Academic Press,2014
60. Levin RJ Hauth JC ,Curet LB, et al Trial of calcium to prevent preeclampsia. N Engl J
Med 1997:337:69-79
61. Atallah An Hofmeyr GJ Duley L. Calcium supplementation during pregnancy for
preventing hypertensive disorders and related problems. Cochrane database sys
Rev.2002 issue I CD001059 DOI: 10.1002/14651858 CD001059
62. Roberts JM speer P.Antioxidant therapy to prevent preeclampsia. Semin Nephrol.
2004;24:557-564
63. Chappell LC. Seede. PT.Briley AL et al Effects of antioxidants on the occurrence of
preeclampsia in women at increased risk; a randomized trial Lancet 1999;354:810-816
64. Beazley D, AhokasR, Livngston J,et.al Vitamin C and E Supplementaion in women at
high risk for preeclampsia: a double blind placbo –controlled trial. AM J obstet Gynecol
2005;192:520-521
65. Duley L, Henderson-Smart DJ, King KM . Antiplatelet agents for preventing pre
eclampsia and its complications. Cochrane Data based Sys Rev 2007;issue 4;
CD0046549.DOI: 10.1002/14681858.CD004659.
66. Askie Lm, Henderson smart DJ.stewart LA Antiplatelet agents for the prevention of
preeclampsia: A meta-annalysis of individual data. Lancet 2007;369:179-180
67. Braunstein GD, Rasor J. Serum human chorionic gonadotropin levels throughout
normal pregnancy. AJOG 1976;126:678-81
68. Reis et al. Hormones and gestational diseases. Endocrine Reviews 2002
April;23(2):230-257.
69. Clinical gynecologic endocrinology and infertility. Leon Speroff. 9th Edition.
70. Lee SM, Romero R, Lee YJ, et al: Systemic inflammatory stimulation by microparticles
derived from hypoxic trophoblast as a model for inflammatory response in
preeclampsia. Am J Obstet Gynecol 207(4):337.e1, 2012
71. Nelson DB, Ziadie MS, McIntire DD, et al: Placental pathology suggesting that
preeclampsia is more than one disease. Am J Obstet Gynecol 210:66.e1, 2014
72. Ness RB, Roberts JM: Heterogeneous causes constituting the single syndrome of
preeclampsia: a hypothesis and its implications. Am J Obstet Gynecol 175(5):1365,
1996
73. Wang Y, Zhao S, Loyd, et al: Increased urinary excretion of nephrin, podocalyxin,and
ig-h3 in women with preeclampsia. Am J Physiol Renal Physiol302(9):F1084, 2012b
SaudanP.Brown MA. Buddie ML. et al Does gestational hypertension become pre-
eclampsia? Br.JobstetGyncol. 1998: 105:1177-1184.
74. Crowther CA. Bowmeester AM, Ashurt HM. Does admission to the hospital for bed
rest prevent disease progression or improve fetal outcome in pregnancy complicate by
nonptroteinuric hypertension? Br.JobsterGynecol 1992-99-13-17.
75. Rayburn WF: Self blood pressure monitoring during pregnancy. Am J obstet Gynecol.
1984:148:159-161.
76. Lowe SA.Brown MA, Dekker GA.et al Guidelines for the management of hypertensive
disorders of pregnancy 2008. Society of obstetric Medicine of Ausrtalia and New
Zealand Aust N ZJ obstetGynecol 2009:49:242-246.
77. Abalos E, DuleyL.Steyn DW, et al. Antihypertensive drug therapy for mild to moderate
by hypertension during pregnancy Cochrane. Database Meyer NL. Mercer BM.
Friedman SA, et al urihary dipstick protein: a poor predictor of absent or severe
proteinuria. Am J obstetGynaecol 1994:170:137-41
78. Durnwald CP. Mercer B.A prospective comparison of total Protein/ preeclampsia Am
J obstetGynaecol. 2003:189:848-852
79. Koopmans CM BijlengaD.Groen H, et al. Induction of labour versus expectant
monitioring for gestational hypertension or mild preeclampsia srandomized controlled
trial Lancet : 2009:37:979-88
80. Paulino VG, Osvaldo RT, andres CM et al Expectant management of severe
preeclampsia remote from term: the MEXPRE Latin Study a rendomizwd, multiceter
clinical trial Am J obsterGynecol 2013:209:425-425
81. Sibai BM, Barton JR:Expectant management of sverepreedlampsia remote from term:
patient selection treatment and delivery indication Am J obstet Gynecol. 2007:196:514-
516
82. Blackwell Sc. Redman ME, Tominson M.et. alLabor induction for the preterm severe
preeclamptic patient: is it worth the effirtJ MatenFetal Med . 2001:10:305-311
83. Satyanarayan K.sawhney H.vashta Associationbetween sec ond trimesterhCG levels
and pregnancy induced hypertension J obstetGunecolindia 2001:51(5):85-86
84. Desai P.PaoS.Predictive Value of raised of raised mindrtimester beta-Hcg in preg nancy
induced hypertension. J obstetGunecolindia. 2002:52(1): 68-70
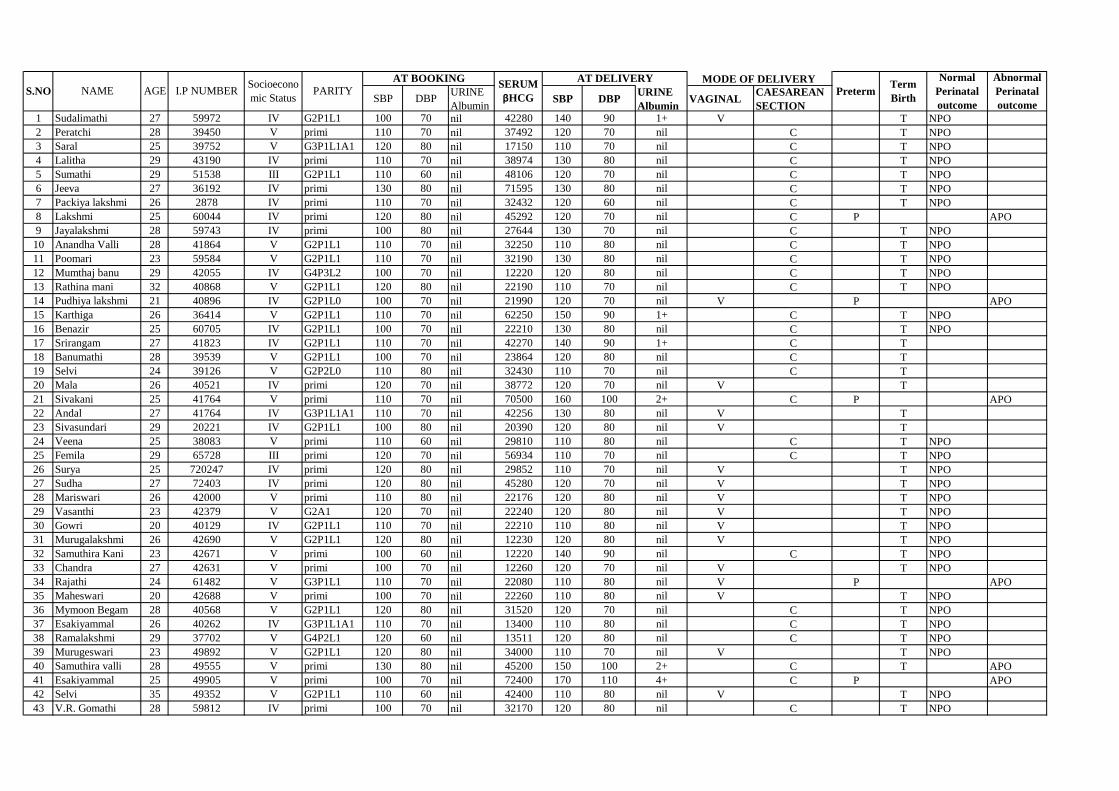
SBP DBPURINE
AlbuminSBP DBP
URINE
AlbuminVAGINAL
CAESAREAN
SECTION1 Sudalimathi 27 59972 IV G2P1L1 100 70 nil 42280 140 90 1+ V T NPO
2 Peratchi 28 39450 V primi 110 70 nil 37492 120 70 nil C T NPO
3 Saral 25 39752 V G3P1L1A1 120 80 nil 17150 110 70 nil C T NPO
4 Lalitha 29 43190 IV primi 110 70 nil 38974 130 80 nil C T NPO
5 Sumathi 29 51538 III G2P1L1 110 60 nil 48106 120 70 nil C T NPO
6 Jeeva 27 36192 IV primi 130 80 nil 71595 130 80 nil C T NPO
7 Packiya lakshmi 26 2878 IV primi 110 70 nil 32432 120 60 nil C T NPO
8 Lakshmi 25 60044 IV primi 120 80 nil 45292 120 70 nil C P APO
9 Jayalakshmi 28 59743 IV primi 100 80 nil 27644 130 70 nil C T NPO
10 Anandha Valli 28 41864 V G2P1L1 110 70 nil 32250 110 80 nil C T NPO
11 Poomari 23 59584 V G2P1L1 110 70 nil 32190 130 80 nil C T NPO
12 Mumthaj banu 29 42055 IV G4P3L2 100 70 nil 12220 120 80 nil C T NPO
13 Rathina mani 32 40868 V G2P1L1 120 80 nil 22190 110 70 nil C T NPO
14 Pudhiya lakshmi 21 40896 IV G2P1L0 100 70 nil 21990 120 70 nil V P APO
15 Karthiga 26 36414 V G2P1L1 110 70 nil 62250 150 90 1+ C T NPO
16 Benazir 25 60705 IV G2P1L1 100 70 nil 22210 130 80 nil C T NPO
17 Srirangam 27 41823 IV G2P1L1 110 70 nil 42270 140 90 1+ C T
18 Banumathi 28 39539 V G2P1L1 100 70 nil 23864 120 80 nil C T
19 Selvi 24 39126 V G2P2L0 110 80 nil 32430 110 70 nil C T
20 Mala 26 40521 IV primi 120 70 nil 38772 120 70 nil V T
21 Sivakani 25 41764 V primi 110 70 nil 70500 160 100 2+ C P APO
22 Andal 27 41764 IV G3P1L1A1 110 70 nil 42256 130 80 nil V T
23 Sivasundari 29 20221 IV G2P1L1 100 80 nil 20390 120 80 nil V T
24 Veena 25 38083 V primi 110 60 nil 29810 110 80 nil C T NPO
25 Femila 29 65728 III primi 120 70 nil 56934 110 70 nil C T NPO
26 Surya 25 720247 IV primi 120 80 nil 29852 110 70 nil V T NPO
27 Sudha 27 72403 IV primi 120 80 nil 45280 120 70 nil V T NPO
28 Mariswari 26 42000 V primi 110 80 nil 22176 120 80 nil V T NPO
29 Vasanthi 23 42379 V G2A1 120 70 nil 22240 120 80 nil V T NPO
30 Gowri 20 40129 IV G2P1L1 110 70 nil 22210 110 80 nil V T NPO
31 Murugalakshmi 26 42690 V G2P1L1 120 80 nil 12230 120 80 nil V T NPO
32 Samuthira Kani 23 42671 V primi 100 60 nil 12220 140 90 nil C T NPO
33 Chandra 27 42631 V primi 100 70 nil 12260 120 70 nil V T NPO
34 Rajathi 24 61482 V G3P1L1 110 70 nil 22080 110 80 nil V P APO
35 Maheswari 20 42688 V primi 100 70 nil 22260 110 80 nil V T NPO
36 Mymoon Begam 28 40568 V G2P1L1 120 80 nil 31520 120 70 nil C T NPO
37 Esakiyammal 26 40262 IV G3P1L1A1 110 70 nil 13400 110 80 nil C T NPO
38 Ramalakshmi 29 37702 V G4P2L1 120 60 nil 13511 120 80 nil C T NPO
39 Murugeswari 23 49892 V G2P1L1 120 80 nil 34000 110 70 nil V T NPO
40 Samuthira valli 28 49555 V primi 130 80 nil 45200 150 100 2+ C T APO
41 Esakiyammal 25 49905 V primi 100 70 nil 72400 170 110 4+ C P APO
42 Selvi 35 49352 V G2P1L1 110 60 nil 42400 110 80 nil V T NPO
43 V.R. Gomathi 28 59812 IV primi 100 70 nil 32170 120 80 nil C T NPO
Normal
Perinatal
outcome
Abnormal
Perinatal
outcome
AT DELIVERY
AGE PretermTerm
BirthNAMES.NO
SERUM
βHCGPARITYI.P NUMBER
AT BOOKINGSocioecono
mic Status
MODE OF DELIVERY
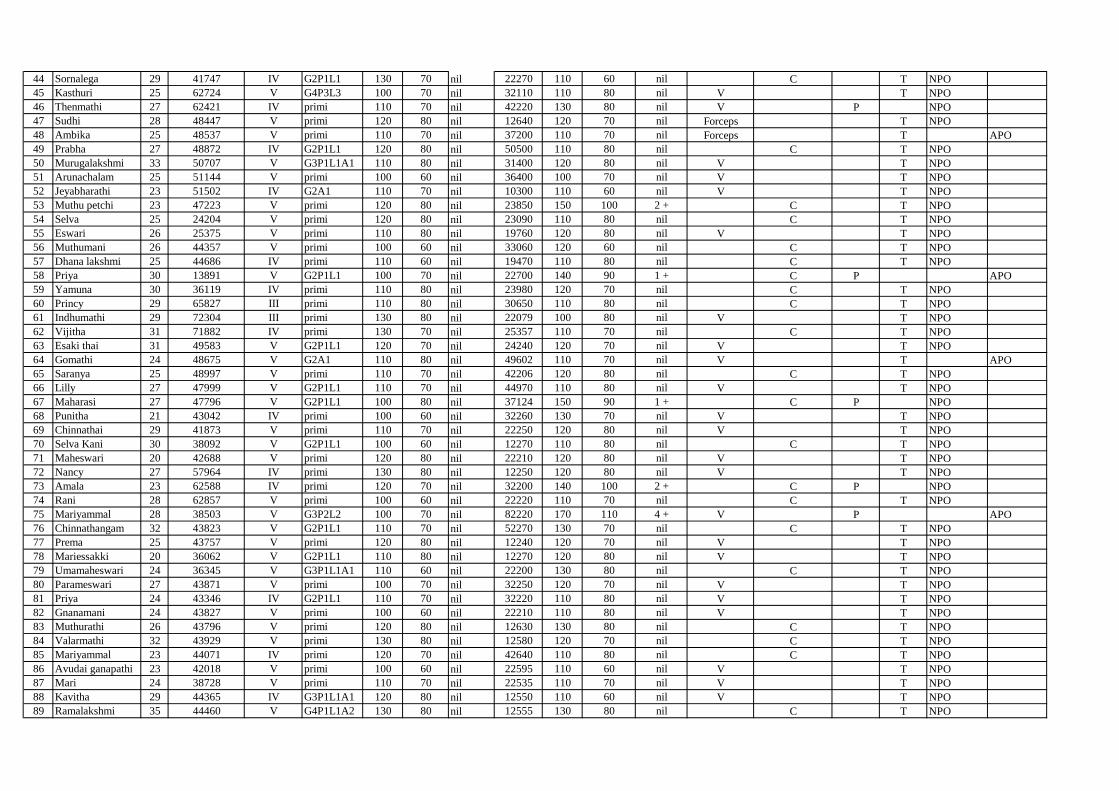
44 Sornalega 29 41747 IV G2P1L1 130 70 nil 22270 110 60 nil C T NPO
45 Kasthuri 25 62724 V G4P3L3 100 70 nil 32110 110 80 nil V T NPO
46 Thenmathi 27 62421 IV primi 110 70 nil 42220 130 80 nil V P NPO
47 Sudhi 28 48447 V primi 120 80 nil 12640 120 70 nil Forceps T NPO
48 Ambika 25 48537 V primi 110 70 nil 37200 110 70 nil Forceps T APO
49 Prabha 27 48872 IV G2P1L1 120 80 nil 50500 110 80 nil C T NPO
50 Murugalakshmi 33 50707 V G3P1L1A1 110 80 nil 31400 120 80 nil V T NPO
51 Arunachalam 25 51144 V primi 100 60 nil 36400 100 70 nil V T NPO
52 Jeyabharathi 23 51502 IV G2A1 110 70 nil 10300 110 60 nil V T NPO
53 Muthu petchi 23 47223 V primi 120 80 nil 23850 150 100 2 + C T NPO
54 Selva 25 24204 V primi 120 80 nil 23090 110 80 nil C T NPO
55 Eswari 26 25375 V primi 110 80 nil 19760 120 80 nil V T NPO
56 Muthumani 26 44357 V primi 100 60 nil 33060 120 60 nil C T NPO
57 Dhana lakshmi 25 44686 IV primi 110 60 nil 19470 110 80 nil C T NPO
58 Priya 30 13891 V G2P1L1 100 70 nil 22700 140 90 1 + C P APO
59 Yamuna 30 36119 IV primi 110 80 nil 23980 120 70 nil C T NPO
60 Princy 29 65827 III primi 110 80 nil 30650 110 80 nil C T NPO
61 Indhumathi 29 72304 III primi 130 80 nil 22079 100 80 nil V T NPO
62 Vijitha 31 71882 IV primi 130 70 nil 25357 110 70 nil C T NPO
63 Esaki thai 31 49583 V G2P1L1 120 70 nil 24240 120 70 nil V T NPO
64 Gomathi 24 48675 V G2A1 110 80 nil 49602 110 70 nil V T APO
65 Saranya 25 48997 V primi 110 70 nil 42206 120 80 nil C T NPO
66 Lilly 27 47999 V G2P1L1 110 70 nil 44970 110 80 nil V T NPO
67 Maharasi 27 47796 V G2P1L1 100 80 nil 37124 150 90 1 + C P NPO
68 Punitha 21 43042 IV primi 100 60 nil 32260 130 70 nil V T NPO
69 Chinnathai 29 41873 V primi 110 70 nil 22250 120 80 nil V T NPO
70 Selva Kani 30 38092 V G2P1L1 100 60 nil 12270 110 80 nil C T NPO
71 Maheswari 20 42688 V primi 120 80 nil 22210 120 80 nil V T NPO
72 Nancy 27 57964 IV primi 130 80 nil 12250 120 80 nil V T NPO
73 Amala 23 62588 IV primi 120 70 nil 32200 140 100 2 + C P NPO
74 Rani 28 62857 V primi 100 60 nil 22220 110 70 nil C T NPO
75 Mariyammal 28 38503 V G3P2L2 100 70 nil 82220 170 110 4 + V P APO
76 Chinnathangam 32 43823 V G2P1L1 110 70 nil 52270 130 70 nil C T NPO
77 Prema 25 43757 V primi 120 80 nil 12240 120 70 nil V T NPO
78 Mariessakki 20 36062 V G2P1L1 110 80 nil 12270 120 80 nil V T NPO
79 Umamaheswari 24 36345 V G3P1L1A1 110 60 nil 22200 130 80 nil C T NPO
80 Parameswari 27 43871 V primi 100 70 nil 32250 120 70 nil V T NPO
81 Priya 24 43346 IV G2P1L1 110 70 nil 32220 110 80 nil V T NPO
82 Gnanamani 24 43827 V primi 100 60 nil 22210 110 80 nil V T NPO
83 Muthurathi 26 43796 V primi 120 80 nil 12630 130 80 nil C T NPO
84 Valarmathi 32 43929 V primi 130 80 nil 12580 120 70 nil C T NPO
85 Mariyammal 23 44071 IV primi 120 70 nil 42640 110 80 nil C T NPO
86 Avudai ganapathi 23 42018 V primi 100 60 nil 22595 110 60 nil V T NPO
87 Mari 24 38728 V primi 110 70 nil 22535 110 70 nil V T NPO
88 Kavitha 29 44365 IV G3P1L1A1 120 80 nil 12550 110 60 nil V T NPO
89 Ramalakshmi 35 44460 V G4P1L1A2 130 80 nil 12555 130 80 nil C T NPO
90 Baby 28 43180 V G4P1L0A2 110 60 nil 72575 150 90 1+ V P APO
91 Santhabeula 27 44766 V primi 100 60 nil 23635 110 60 nil V T NPO
92 Mahalakshmi 29 35587 V G2P1L1 110 70 nil 32585 120 70 nil C T NPO
93 Packia thai 25 43719 V G2P1L1 120 70 nil 22600 100 80 nil V T NPO
94 Sakunthala 25 64962 IV primi 120 80 nil 12530 120 80 nil C T NPO
95 Arumugakani 35 64336 V G3P1L0A1 100 80 nil 32600 100 70 nil C P T NPO
96 Thangamani 25 44814 IV G2P1L1 100 70 nil 12595 140 90 1+ C T NPO
97 Rajeswari 23 44819 V G2P1L1 110 60 nil 17300 120 70 nil C T NPO
98 Kaleeswari 19 43958 V primi 120 80 nil 15200 120 60 nil C T NPO
99 Sankarammal 37 44172 V G2P1L1 110 70 nil 24400 110 80 nil C T NPO
100 Mariyammal 24 45295 IV G3P2L2 100 60 nil 19670 110 80 nil C T NPO