In the name of God. A 23-years old β-thalassaemia major woman with resistant hypocalcemia.
68
In the name of God
-
Upload
stewart-richardson -
Category
Documents
-
view
220 -
download
5
Transcript of In the name of God. A 23-years old β-thalassaemia major woman with resistant hypocalcemia.
In the name of God
A 23-years old β-thalassaemia major woman with resistant hypocalcemia
Presentation of Case
ID:
A 23 years old woman known case of β-thalassaemia major, single, native and resident of Kahnooj city, Kerman province
Chief complaint:
Bone pain
Presentation of Case
Present illness:
The patient has regular Red Blood Cell Transfusion Program 2 times monthly. She uses Desferal (deferoxamine) almost regularly. She complain of bone pain since 5-6 days before admission. She also complain of paresthesia in perioral region, hands and feet. The symptoms had increased day by day.
Presentation of Case
Present illness (con.)
With these complains she was admited in emergency department in kahnooj.
On admissin, the lab evaluation showed a hypocalcemia.
She was treated with IV Ca- Gluconate.
Despite this treatment the serum Ca level didn’t increase and the patient experience a tonic colonic seizure. Because of resistant hypocalcemia she refered to afzalipoor hospital in Kerman.
Presentation of Case
Present illness (con.)
When she was admited in afzalipoor center she didn’t complain of bone pain and paresthesia.
The patient 3 years earlier with similar symptoms of bone pain, parestheisa, nausea, vomiting and a tonic colonic seizure was admitted.
She had a hypocalcemia and hyperphosohatemia.
Presentation of case
Present illness (con.)
At that time the patient was discharged with diagnosis of hypoparathyroidism and advised to follow up regularly prescribed drug:
Ca-forte, Caco3 and calcitriol.
Presentation of case
Present illness (con.)
She had no follow-up in the last three years but had been taking medicine almost regularly.
She had not any symptoms during this years until 1 month before recent admission that she had a emotional stress after which, she discontinue her drugs.
Presentation of Case
PMH :
• Thalacemia Major
• Primary amenorrhoea
• Short stature and growth failure (less than the 3rd percentile on growth charts)
• Perforated appendicitis 8 years ago
Presentation of Case
DH:
• Desferal 2 gr sc infuion daily,
• Caco3 1000 mg po TDS until 1 mounth before,
• Calcitriol 0.25 mg po BID until 1 mounth before,
FH: father and mother are not relatives
AH: non significant
PH: non significant
Presentation of CasePhysical Examination:
General appearance:
A young woman with chipmunk facial appearance that was not ill and toxic, the apparent age is not consistent with her chronological age with short stature
Vital signs:
BP: 90 / 60 PR: 100 RR: 16 T: 36.5 ;c (oral)
Weight: 45 Kg Height: 147 cm
BMI : 20.82
Presentation of Case
Head and Neck:
• pale conjunctiva
• prominent frontal bossing
• marked overgrowth of the maxillae
• Chvostek’s sign: negative
• No neck scar
• There is no evidence of candidiasis in mouth and pharynx mucusa
Presentation of Case
Chest:
• Heart: S1 S2 without any murmer
• Lungs: bilateral clear
• Breasts development: Tanner stage 3
• No growth of axillary hairs
Presentation of Case
Abdomen:
• Midline surgery scar
• Hepatomegaly
liver span measured 20 cm in the midclavicular line
• Spleenomegaly:
13 cm below the left costal margin
Presentation of Case
Extremities:
• No edema or cyanosis
• Bone pain : tenderness in extremities
• There is no muscle weakness
• The forces are normal
• Trousseau’s sign: Negative
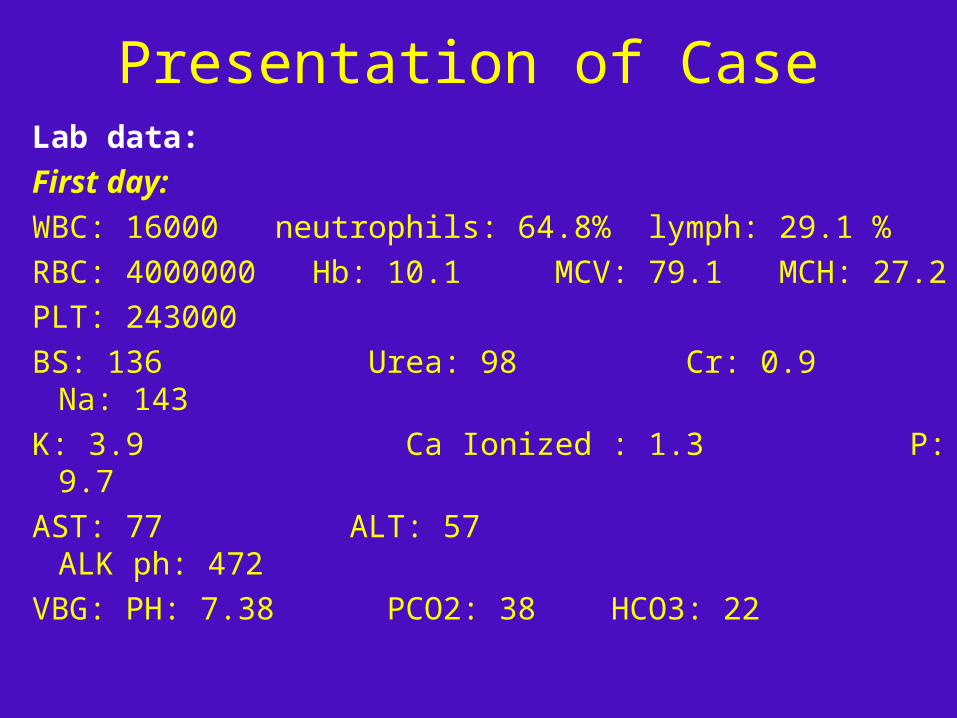
Presentation of CaseLab data:
First day:
WBC: 16000 neutrophils: 64.8% lymph: 29.1 %
RBC: 4000000 Hb: 10.1 MCV: 79.1 MCH: 27.2
PLT: 243000
BS: 136 Urea: 98 Cr: 0.9 Na: 143
K: 3.9 Ca Ionized : 1.3 P: 9.7
AST: 77 ALT: 57 ALK ph: 472
VBG: PH: 7.38 PCO2: 38 HCO3: 22
Presentation of case
ECG:
Prolonged QT interval
Echocardiography
• Ejection fraction: 45 - 50%
• Pulmonary artery pressure: 40 – 45 mm Hg
• LV diastolic dysfunction grade 1
• Mild LV systolic dysfunction
Presentation of case
Abdominopelvic sonography:Liver shows enlarged size (270 mm) with normal echo pattern.
Biliary tree and portal system are normal in diameter.
Gallblader shows normal size and wall thikness and contains some stone with maximum diameter of 7 mm.
Spleenomegaly is evident (190 mm).
Both kidneys shows normal size and echo pattern without evidence of stone or hydronephrosis.
Bladder shows normal wall thickness without any filling defect and stone.
Uterus shows small size. No adenexal pathology is evident.
The problem:
hypocalcemia
CALCIUM HOMEOSTASIS
• Calcium in the blood is transported:bound to plasma proteins (about 45 percent),
notably albuminbound to small anions such as phosphate and
citrate (about 15 percent)in the free or ionized state (about 40 percent)
• Only the ionized calcium is metabolically active
CALCIUM HOMEOSTASIS
Normal serum range
• Total serum calcium:
between 8.5 and 10.5 mg/dL
• Ionized calcium:
4.65 to 5.25 mg/dL
Causes of hypocalcemia
Major causes
• Low PTH (hypoparathyroidism)
• High PTH (secondary hyperparathyroidism in response to hypocalcemia)
• Drugs
• Disorders of magnesium metabolism
Causes of hypocalcemia
Low PTH (hypoparathyroidism) Genetic disorders
• Abnormal parathyroid gland development
• Abnormal PTH synthesis
• Activating mutations of calcium-sensing receptor (autosomal dominant hypocalcemia or sporadic isolated hypoparathyroidism)
Causes of hypocalcemia
Low PTH (hypoparathyroidism) (con.)Post-surgical (thyroidectomy,
parathyroidectomy, radical neck dissection) Autoimmune
• Autoimmune polyglandular syndrome type 1 (associated with chronic mucocutaneous candidiasis and primary adrenal insufficiency)
• Isolated hypoparathyroidism due to activating antibodies to calcium-sensing receptor
Causes of hypocalcemia
Low PTH (hypoparathyroidism) (con.)Infiltration of the parathyroid gland
(hemochromatosis, iron overload , Wilson's disease, granulomatous, metastases)
Radiation-induced destruction parathyroid glandsHungry bone syndrome
(post parathyroidectomy) HIV infection
Causes of hypocalcemia
High PTH (secondary hyperparathyroidism in response to hypocalcemia)
Vitamin D deficiency or resistance
Multiple causes Parathyroid hormone resistance
Pseudohypoparathyroidism
Hypomagnesemia Renal disease
Causes of hypocalcemia
High PTH (secondary hyperparathyroidism in response to hypocalcemia) (con.)
Loss of calcium from the circulation • Hyperphosphatemia
• Tumor lysis
• Acute pancreatitis
• Osteoblastic metastases
• Acute respiratory alkalosis
• Sepsis or acute severe illness
• Surgery
Causes of hypocalcemiaDrugs Inhibitors of bone resorption (bisphosphonates,
calcitonin), especially in vitamin D deficiency Cinacalcet Calcium chelators (EDTA, citrate, phosphate) Foscarnet (due to intravascular complexing with
calcium) Phenytoin (due to conversion of vitamin D to inactive
metabolites) Fluoride poisoning Chemotherapy (Cisplatin is probably most common)
Causes of hypocalcemia
Disorders of magnesium metabolism
• Hypomagnesemia can reduce PTH secretion or cause PTH resistance and is therefore associated with normal, low, or high PTH levels
• Severe hypermagnesemia, a very rare disorder, can also cause hypocalcemia, by suppressing the secretion of PTH
Diagnostic approach to hypocalcemia
The first step is measurement of the serum albumin concentration. Calcium in serum is bound to proteins, principally albumin. As a result, the total serum calcium concentration in patients with low or high serum albumin levels may not accurately reflect the physiologically important ionized (or free) calcium concentration.
Diagnostic approach to hypocalcemia
Each 1 g/dL reduction in the serum albumin concentration will lower the total calcium concentration by approximately 0.8 mg/dL without affecting the ionized calcium concentration and therefore without producing any symptoms or signs of hypocalcemia.
Diagnostic approach to hypocalcemia
• It is important to verify with repeat measurement (ionized calcium or total serum calcium corrected for albumin)
• Determine the blood PH,
It is important to note that the affinity of calcium for albumin is increased in the presence of alkalosis
Acidosis reducing calcium-albumin binding and alkalosis, enhancing it
Diagnostic approach to hypocalcemia
CLINICAL EVALUATION
• The etiology of hypocalcemia may be obvious from the clinical history
• A history of head and neck surgery (thyroid, parathyroid, or radical neck surgery for head and neck cancer) or the presence of a neck scar suggests postsurgical hypoparathyroidism.
Diagnostic approach to hypocalcemia
CLINICAL EVALUATION
• A family history of hypocalcemia suggests:genetic causepolyglandular autoimmune syndrome type I
• History of Chronic hypocalcemiaAn activating mutation of the calcium sensing
receptor pseudohypoparathyroidism
Diagnostic approach to hypocalcemia
CLINICAL EVALUATION
• The presence of chronic mucocutaneous candidiasis and adrenal insufficiency suggests a polyglandular syndrome
Diagnostic approach to hypocalcemia
CLINICAL EVALUATION
• Other causes of hypocalcemia that may be apparent from the history, physical examination, and routine laboratory data:
Acute or chronic kidney disease Acute pancreatitis Rhabdomyolysis Marked increases in tissue breakdown with the release
of phosphate from cells, as occurs in the tumor lysis syndrome
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION• Serum PTH concentrations
• Creatinin
• Phosphate
• Magnesium
• Vitamin D metabolites
• Other tests that may be helpful:
serum alkaline phosphatase, serum amylase, and 24-hour urinary excretion of calcium and magnesium
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
• Among the tests that may be helpful in defining the etiology of hypocalcemia, measurement of serum intact parathyroid hormone is the most valuable and should be performed in all patients with hypocalcemia
• Other tests should be performed selectively, based upon the patient's history and physical examination
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Serum PTH concentrations
• Can be interpreted correctly only when serum calcium is measured simultaneously
• The serum PTH concentration varies with the cause of the hypocalcemia
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Serum PTH concentrations
• Hypoparathyroidism:
Serum PTH is reduced or inappropriately normal
• Acute or chronic kidney disease, vitamin D deficiency, and pseudohypoparathyroidism: Serum PTH is elevated
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Serum PTH concentrations
• Hypomagnesemia or autosomal dominant hypocalcemia, a rare disorder characterized by an activating mutation in the calcium-sensing receptor gene : Serum PTH is typically normal or low
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Magnesium
• Hypomagnesemia is serum magnesium concentration below 0.8 meq/L (1 mg/dL)
• Hypomagnesemia causes hypocalcemia by inducing PTH resistance or deficiency.
• Serum magnesium should be measured in any patient with hypocalcemia in whom the cause is not obvious
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Phosphate• Persistent hypocalcemia and hyperphosphatemia
is, in the absence of kidney disease or increased tissue breakdown, virtually diagnostic of either hypoparathyroidism (PTH deficiency) or pseudohypoparathyroidism (PTH resistance)
• It is due to loss of the stimulatory effect of PTH on urinary phosphate excretion
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Phosphate
• A low serum phosphate concentration with excess PTH secretion and hypocalcemia means:
secondary hyperparathyroidism (and some abnormality in vitamin D intake or metabolism)
low dietary phosphate intake
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Vitamin D metabolites • Vitamin D deficiency increases PTH secretion by
causing hypocalcemia (due to the reduction in intestinal calcium absorption) and, to a lesser degree, by removing the normal inhibitory effect of calcitriol on PTH production.
• Vitamin D deficiency also diminishes intestinal phosphate absorption. Excess PTH enhances phosphate excretion and lowers the serum phosphate.
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Vitamin D metabolites • Measurement of serum 25-hydroxyvitamin D
(25OHD, calcidiol) provides more information about vitamin D deficiency than does measurement of serum 1,25-dihydroxyvitamin D (calcitriol) because the hypocalcemia-induced increase in PTH secretion stimulates renal 1,25-dihydroxyvitamin D production (in patients without underlying renal insufficiency).
Diagnostic approach to hypocalcemia
LABORATORY EVALUATION (con.)
Vitamin D metabolites
• In vitamin D deficiency, serum 25OHD is low whereas 1,25-dihydroxyvitamin D is typically normal or high.
• In hypoparathyroidism may have normal serum 25OHD and low 1,25-dihydroxyvitamin D concentrations
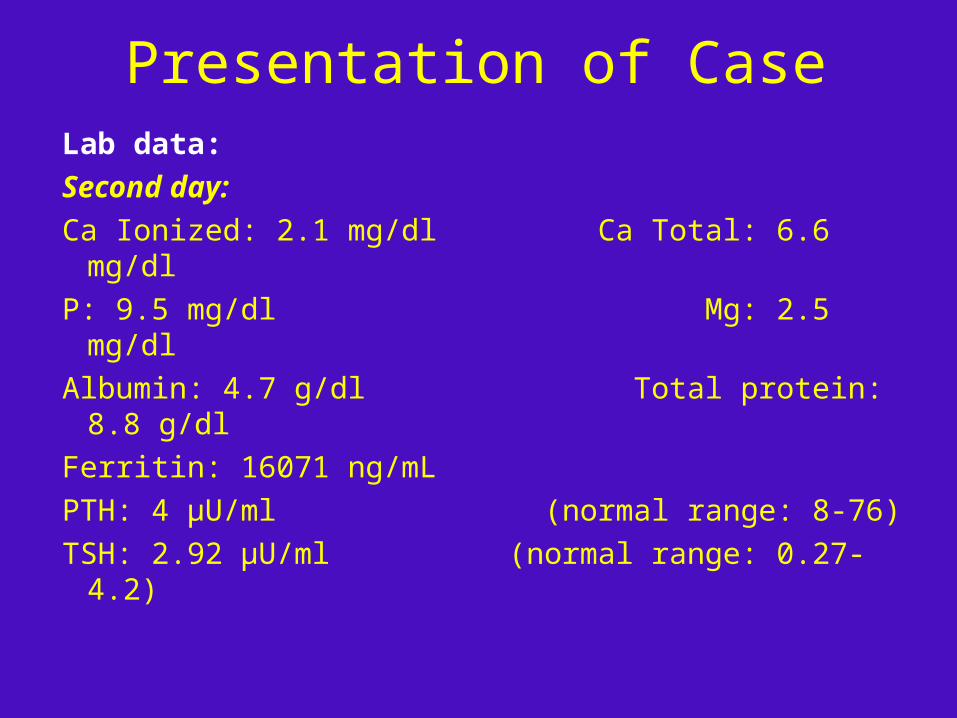
Presentation of Case
Lab data:
Second day:
Ca Ionized: 2.1 mg/dl Ca Total: 6.6 mg/dl
P: 9.5 mg/dl Mg: 2.5 mg/dl
Albumin: 4.7 g/dl Total protein: 8.8 g/dl
Ferritin: 16071 ng/mL
PTH: 4 µU/ml (normal range: 8-76)
TSH: 2.92 µU/ml (normal range: 0.27- 4.2)
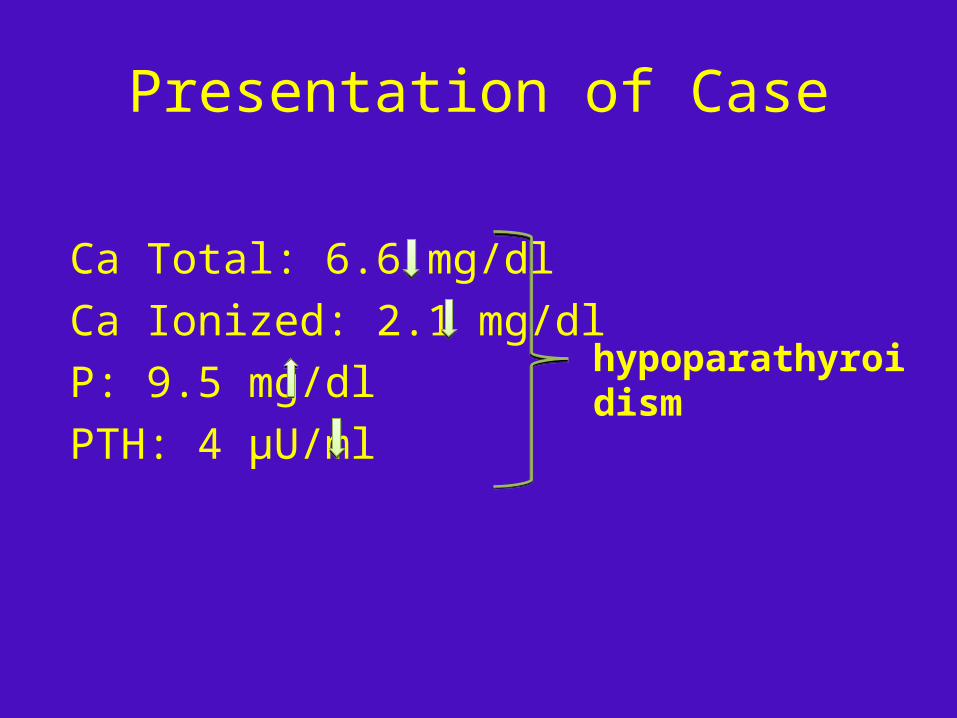
Presentation of Case
Ca Total: 6.6 mg/dl
Ca Ionized: 2.1 mg/dl
P: 9.5 mg/dl
PTH: 4 µU/ml
hypoparathyroidism
β-thalassaemia major and hypocalcemia
• Beta-thalassemia major, a hereditary hemoglobin disorder and is characterized by a decreased synthesis of the β-globin chain.
• Regular blood transfusions and chelation therapy have considerably prolonged survival in thalassemic patients.
β-thalassaemia major and hypocalcemia
• Despite a significant increase in the lifespan of these patients, many endocrine abnormalities such as growth failure, hypogonadism, diabetes mellitus, hypothyroidism develop due to an iron overload.
• Hypoparathyroidism is thought to be a rarer complication, usually, but not always, accompanied by hypocalcemia.
β-thalassaemia major and hypocalcemia
• Osteoporosis represents an important cause of morbidity in the thalassemic population.
• Although the main role is played by hypogonadism and bone marrow expansion, the etiology of this bone disease is multifactorial (hormonal deficiency, increased iron stores, desferrioxamine toxicity)
β-thalassaemia major and hypocalcemia
• In addition, calcium and vitamin D deficiency associated with hypoparathyroidism are also implicated in osteoporosis.
β-thalassaemia major and hypocalcemia
• Hypoparathyroidism usually develops after first decade. All patients over the age of 12 years should have calcium and phosphate levels checked at least every 6 months. If these are abnormal, parathyroid hormone level should be measured.
• Hypoparathyroidism should be managed as per endocrine standards.
Treatment
Calcium
• The treatment of hypocalcemia varies with its severity and the underlying cause.
• Patients with hypocalcemia who are severely symptomatic (carpopedal spasm, tetany, seizures, decreased cardiac function, or prolonged QT interval) require rapid correction of calcium levels with IV calcium therapy. IV calcium therapy in asymptomatic patients with an acute decrease in serum corrected calcium to ≤7.5 mg/dL (1.9 mmol/L) should be done.
Treatment
• Calcium (con.)
• Intravenous calcium is NOT warranted as initial therapy for asymptomatic hypocalcemia in patients with impaired renal function in whom correction of hyperphosphatemia and of low circulating 1,25-dihyroxyvitamin D are usually the primary goals.
Treatment
Calcium (con.)
• For those with milder symptoms of neuromuscular irritability (paresthesias) and corrected serum calcium concentrations greater than 7.5 mg/dL (1.9 mmol/L), initial treatment with oral calcium supplementation is sufficient. If symptoms do not improve with oral supplementation, intravenous calcium infusion is required.
• To effectively treat hypocalcemia in patients with concurrent magnesium deficiency, hypomagnesemia should be corrected first.
Treatment
Vitamin D
• When hypoparathyroidism (transient or permanent) or vitamin D deficiency are the cause of hypocalcemia, administration of intravenous calcium is only transiently effective (as long as the infusion continues), and oral calcium may not be well absorbed. In these cases, successful management requires the addition of vitamin D, which often permits a lower dose of calcium supplementation.
Treatment
Vitamin D (con.)• For the initial management of patients with
hypoparathyroidism, vitamin D supplementation in addition to calcium is recommend . Calcitriol is the vitamin D metabolite of choice because it does not require renal activation, it has a rapid onset of action (hours), and a shorter half-life. Other acceptable options include alfacalcidol, vitamin D (ergocalciferol or cholecalciferol), or dihydrotachysterol
Treatment
Vitamin D (con.)
• In individuals with hypocalcemia due to vitamin D deficiency, vitamin D repletion is recommend. Nutritional deficiency (25OHD <20 ng/mL [50 nmol/L]) requires initial treatment with 50,000 units of vitamin D2 or D3 orally once per week for six to eight weeks, and then 800 to 1000 international units of vitamin D3 daily thereafter.
Treatment
Permanent hypoparathyroidism • In patients with permanent hypoparathyroidism, the
goals of therapy are to relieve symptoms, to raise and maintain the serum calcium concentration in
the low-normal range (eg, 8.0 to 8.5 mg/dL [2.0 to 2.1 mmol/L]),
to avoid hypercalciuria (maintain 24-hour urinary calcium below 300 mg).
Treatment
• Permanent hypoparathyroidism (con.)
• All patients with permanent hypoparathyroidism require adequate calcium intake (1.0 to 1.5 g elemental calcium daily).
Treatment
Permanent hypoparathyroidism (con.)• Along with calcium supplementation, calcitriol rather
than recombinant human parathyroid hormone (PTH) is suggested.
• The long-term safety of recombinant PTH has not been established.
• In addition, recombinant PTH is much more expensive than standard therapy with calcitriol.
• However, in patients with refractory hypercalciuria, PTH is a reasonable option.
Treatment
Permanent hypoparathyroidism (con.)
• The initial treatment of hypercalciuria in patients with hypoparathyroidism is reducing the dose of calcium and vitamin D. Some patients will require the addition of thiazide diuretics.
Treatment of the case
• Amp Calcium gluconate 6 gr IV infusion q 6 hours
decrease to 10 gr daily after 1 week
• Tab Caco3 1 gr po QID
• Pearl Calcitriol 0.25 mg po TDS
• Cap Sevelamer 800 mg po daily
Lab data on discharge
Ca ionized: 4 mg/dl
Ca total : 8.1 mg/dl
P : 4.4 mg/dl
Prescription on discharge
• Tad Caco3 1 gr po TDS
• Pearl calcitriol 0.25 mg TDS
• Eff Tad Calcium forte 500 BID

Thanks for your attention