In situ proteomic analysis by MALDI imaging identifies ubiquitin and thymosin-β4 as markers of...
8
Original article In situ proteomic analysis by MALDI imaging identifies ubiquitin and thymosin-b4 as markers of malignant intraductal pancreatic mucinous neoplasms Vinciane Rebours a, b, * , Julie Le Faouder b , Samira Laouirem b , Mounya Mebarki b , Miguel Albuquerque b, c , Jean-Michel Camadro d, e , Thibaut Léger d , Philippe Ruszniewski a, b , Philippe Lévy a , Valérie Paradis b, c , Pierre Bedossa b, c , Anne Couvelard b, f a Pancreatology Department, Beaujon Hospital, AP-HP, Clichy, Paris-Diderot University, France b Inserm U773-CRB3, Paris-Diderot University, Paris, France c Pathology Department, Beaujon Hospital, AP-HP, Clichy, Paris-Diderot University, France d Mass Spectrometry Facility, Jacques Monod Institute, UMR7592, Paris-Diderot University e CNRS, Paris, France e Molecular and Cellular Pathology Program, Jacques Monod Institute, UMR7592, Paris-Diderot University e CNRS, Paris, France f Pathology Department, Bichat Hospital, AP-HP, Paris-Diderot University, France article info Article history: Received 10 August 2013 Received in revised form 6 December 2013 Accepted 9 December 2013 Keywords: MALDI Imaging mass spectrometry IPMN Pancreatic precancerous lesions Proteomics Biomarker hunting Ubiquitin Thymosin-b4 abstract Purpose: Intraductal pancreatic mucinous neoplasms (IPMN) are precancerous cystic lesions. The aim was to investigate the in situ IPMN proteome using MALDI (Matrix-Assisted Laser Desorption/Ionisation) imaging and to characterize biomarkers associated with the grade of dysplasia. Experimental design: Frozen human Branch duct -IPMN sections were selected according to dysplasia and proteomic analyses were performed by MALDI imaging to obtain mass spectra distribution. The most discriminating peaks were identified using tissue extraction and nanoLC-ESI-MS/MS. Identified peaks were validated in independent series of IPMN by immunochemistry on surgical specimens (tissue- microarrays (TMA), n ¼ 45) and endoscopic ultrasound fine-needle aspiration (EUS FNA) samples (n ¼ 25). Results: BD-IPMN samples with low (n ¼ 10) and high (n ¼ 10) grades of dysplasia were analyzed. Differential spectra of proteins were found in the two groups with significantly different intensities (n ¼ 15). The two peaks (intense in high grade IPMN) (m/z 8565 and 4747) were characterized as the monomeric ubiquitin (Mascot score ¼ 319.22) and an acetylated fragment of thymosin-b4 (2e42) (Omssa score ¼ 1.37 E9). Validation on TMA and EUS FNA samples confirmed that ubiquitin was overexpressed in high grade dysplasia (p ¼ 0.04 and p ¼ 0.0004). Thymosin-b4 expression was confirmed on TMA by immunohistochemistry on high grade IPMN (p ¼ 0.011). Conclusion: Ubiquitin and thymosin-b4 are overexpressed in IPMN with high grade dysplasia. Positive immunochemical staining on EUS-FNA material is a major argument in support of preventive resection. Copyright Ó 2013, IAP and EPC. Published by Elsevier India, a division of Reed Elsevier India Pvt. Ltd. All rights reserved. 1. Introduction Intraductal papillary mucinous neoplasms (IPMN) are precan- cerous intraepithelial pancreatic lesions that were first described in 1986 by Itai et al. [1] According to the World Health Organization (WHO) classification, IPMN are defined as abnormal proliferation of duct epithelium with mucus production involving the main pancreatic duct, the branch ducts (BD) or both, responsible for duct dilatation [2]. IPMN follow a sequential oncogenic course from low to high grade dysplasia then to invasive adenocarcinoma [3]. Abbreviations: IPMN, intraductal pancreatic mucinous neoplasms; WHO, World Health Organization; EUS, endoscopic ultrasound; MRCP, magnetic resonance cholangio-pancreatography; MALDI-TOF, matrix-assisted laser desorption/ionisa- tion e time of flight; nanoLC-ESI-MS/MS, nano liquid chromatography e electro- spray e tandem mass spectrometry; BD, branch duct; ACN, acetonitrile; TFA, trifluoroacetic acid; FNA, fine-needle aspiration; TMA, tissue micro array; NS, none significant. * Corresponding author. Pôle des Maladies de l’Appareil Digestif, Service de Pancréatologie, INSERM U773, Hôpital Beaujon, 100, boulevard du général Leclerc, 92110 Clichy Cedex, France. Tel.: þ33 (0) 1 40 87 52 25; fax: þ33 (0) 1 42 70 37 84. E-mail address: [email protected] (V. Rebours). Contents lists available at ScienceDirect Pancreatology journal homepage: www.elsevier.com/locate/pan 1424-3903/$ e see front matter Copyright Ó 2013, IAP and EPC. Published by Elsevier India, a division of Reed Elsevier India Pvt. Ltd. All rights reserved. http://dx.doi.org/10.1016/j.pan.2013.12.001 Pancreatology 14 (2014) 117e124
Transcript of In situ proteomic analysis by MALDI imaging identifies ubiquitin and thymosin-β4 as markers of...

lable at ScienceDirect
Pancreatology 14 (2014) 117e124
Contents lists avai
Pancreatology
journal homepage: www.elsevier .com/locate/pan
Original article
In situ proteomic analysis by MALDI imaging identifies ubiquitin andthymosin-b4 as markers of malignant intraductal pancreatic mucinousneoplasms
Vinciane Rebours a,b,*, Julie Le Faouder b, Samira Laouirem b, Mounya Mebarki b,Miguel Albuquerque b,c, Jean-Michel Camadro d,e, Thibaut Léger d,Philippe Ruszniewski a,b, Philippe Lévy a, Valérie Paradis b,c, Pierre Bedossa b,c,Anne Couvelard b,f
a Pancreatology Department, Beaujon Hospital, AP-HP, Clichy, Paris-Diderot University, Franceb Inserm U773-CRB3, Paris-Diderot University, Paris, Francec Pathology Department, Beaujon Hospital, AP-HP, Clichy, Paris-Diderot University, FrancedMass Spectrometry Facility, Jacques Monod Institute, UMR7592, Paris-Diderot University e CNRS, Paris, FranceeMolecular and Cellular Pathology Program, Jacques Monod Institute, UMR7592, Paris-Diderot University e CNRS, Paris, Francef Pathology Department, Bichat Hospital, AP-HP, Paris-Diderot University, France
a r t i c l e i n f o
Article history:Received 10 August 2013Received in revised form6 December 2013Accepted 9 December 2013
Keywords:MALDIImaging mass spectrometryIPMNPancreatic precancerous lesionsProteomicsBiomarker huntingUbiquitinThymosin-b4
Abbreviations: IPMN, intraductal pancreatic mucinHealth Organization; EUS, endoscopic ultrasound;cholangio-pancreatography; MALDI-TOF, matrix-assition e time of flight; nanoLC-ESI-MS/MS, nano liquidspray e tandem mass spectrometry; BD, branch dtrifluoroacetic acid; FNA, fine-needle aspiration; TMAsignificant.* Corresponding author. Pôle des Maladies de l’A
Pancréatologie, INSERM U773, Hôpital Beaujon, 100, b92110 Clichy Cedex, France. Tel.: þ33 (0) 1 40 87 52 2
E-mail address: [email protected] (V. R
1424-3903/$ e see front matter Copyright � 2013, IAhttp://dx.doi.org/10.1016/j.pan.2013.12.001
a b s t r a c t
Purpose: Intraductal pancreatic mucinous neoplasms (IPMN) are precancerous cystic lesions. The aimwas to investigate the in situ IPMN proteome using MALDI (Matrix-Assisted Laser Desorption/Ionisation)imaging and to characterize biomarkers associated with the grade of dysplasia.Experimental design: Frozen human Branch duct -IPMN sections were selected according to dysplasia andproteomic analyses were performed by MALDI imaging to obtain mass spectra distribution. The mostdiscriminating peaks were identified using tissue extraction and nanoLC-ESI-MS/MS. Identified peakswere validated in independent series of IPMN by immunochemistry on surgical specimens (tissue-microarrays (TMA), n ¼ 45) and endoscopic ultrasound fine-needle aspiration (EUS FNA) samples(n ¼ 25).Results: BD-IPMN samples with low (n ¼ 10) and high (n ¼ 10) grades of dysplasia were analyzed.Differential spectra of proteins were found in the two groups with significantly different intensities(n ¼ 15). The two peaks (intense in high grade IPMN) (m/z 8565 and 4747) were characterized as themonomeric ubiquitin (Mascot score ¼ 319.22) and an acetylated fragment of thymosin-b4 (2e42) (Omssascore ¼ 1.37 E�9). Validation on TMA and EUS FNA samples confirmed that ubiquitin was overexpressedin high grade dysplasia (p ¼ 0.04 and p ¼ 0.0004). Thymosin-b4 expression was confirmed on TMA byimmunohistochemistry on high grade IPMN (p ¼ 0.011).Conclusion: Ubiquitin and thymosin-b4 are overexpressed in IPMN with high grade dysplasia. Positiveimmunochemical staining on EUS-FNA material is a major argument in support of preventive resection.Copyright � 2013, IAP and EPC. Published by Elsevier India, a division of Reed Elsevier India Pvt. Ltd. Allrights reserved.
ous neoplasms; WHO, WorldMRCP, magnetic resonance
sted laser desorption/ionisa-chromatography e electro-
uct; ACN, acetonitrile; TFA,, tissue micro array; NS, none
ppareil Digestif, Service deoulevard du général Leclerc,5; fax: þ33 (0) 1 42 70 37 84.ebours).
P and EPC. Published by Elsevier I
1. Introduction
Intraductal papillary mucinous neoplasms (IPMN) are precan-cerous intraepithelial pancreatic lesions that were first described in1986 by Itai et al. [1] According to the World Health Organization(WHO) classification, IPMN are defined as abnormal proliferation ofduct epithelium with mucus production involving the mainpancreatic duct, the branch ducts (BD) or both, responsible for ductdilatation [2]. IPMN follow a sequential oncogenic course from lowto high grade dysplasia then to invasive adenocarcinoma [3].
ndia, a division of Reed Elsevier India Pvt. Ltd. All rights reserved.

V. Rebours et al. / Pancreatology 14 (2014) 117e124118
Because exocrine lesions account for 90% of pancreatic carcinomas,IPMN may be present in an estimated 5e10% of patients withpancreatic adenocarcinoma [4]. Preventive surgery is indicated forIPMN involving the main pancreatic duct due to the high risk ofmalignant transformation (5-year actuarial risk 63%) [5]. However,the management of BD-IPMN is still a matter of debate with anestimated risk of cancer varying between 3 and 18%. The recentinternational guidelines recommended preventive surgical resec-tion for lesions with mural nodules >5 mm, cyst size >30 mm,symptomatic lesions and positive cytology. New high-risk factorsthat have been proposed included a rapidly increasing cyst size andhigh grade atypia [6]. However, no specific morphological featureshave been correlated to the grade of dysplasia and avoiding ma-lignant transformation is still a difficult challenge. Proteomics is aninteresting approach for the characterization of cancer biomarkersby identifying proteins/peptides that are specifically expressed intissue extracts. Preliminary results from our group have shown thatproteomic analysis of the pancreatic mucus by surface-enhancedlaser desorption ionization time-of flight mass spectrometry canbe performed to determine candidate protein expression profilesand have confirmed that the carcinogenic process in IPMN isassociated with changes in the proteome with characteristic peaks[7]. Unfortunately, this approach does not take into account tissueheterogeneity unless careful microdissection of tumor cells is per-formed. MALDI IMS (matrix-assisted laser desorption ionizationimaging mass spectrometry) is a new approach that avoids thistechnical drawback [8]. A thin tissue section is collected on a targetslide and mass spectra are systematically recorded point by pointthroughout the tissue. Since this technology analyzes intact tissueavoiding the need for homogenization and purification, the spatialdistribution of the molecules within the tissue is preserved andthere is no risk of non-relevant pre-analytical protein alterations[9].
The aims of this study were to perform an in situ proteinprofiling of low and high grade dysplastic IPMN byMALDI imaging,to compare the peak intensity, to determine the relevant peakmarkers of high grade dysplasia, to identify the protein of interestand to validate these markers on pancreatic EUS-FNA.
2. Material and methods
2.1. Patients and tissue sample selection
IPMN tissue samples were collected from surgical specimens of20 patients operated on for branch duct IPMN from 2007 to 2009 inBeaujon Hospital, Clichy, France. Informed consent and institu-tional review board approval were obtained for all patients beforesurgery. All samples were stored at �80 �C until MALDI analysis. Atotal of 20 tissue samples were selected according to the grade ofdysplasia: low (n ¼ 10) and high grade dysplasia (n ¼ 10).
2.2. Tissue preparation for histology-directed MALDI IMS
Serial 10 mm sections were performed on a cryo-microtome foreach specimen. The two first sections were stained with haema-toxylin and eosin (H&E) and were analyzed by a pathologist (AC) toselect slides with relevant lesions. The two following sections offrozen specimens were thaw-mounted on a electrically conductiveindium-tin-oxide-coated glass slide (Bruker Daltonics, Bremen,Germany) forMALDI imaging analysis. The slides were immersed in70%, 70% and 100% isopropanol and dried using a vacuum. Tissuesections were directly covered with a matrix (sinapinic acid at aconcentration of 10 mg/mL in water/acetonitrile 40:60 (v/v) with0.2% trifluoroacetic acid (TFA); SigmaeAldrich (St Louis, MO, USA))
using an automatic sprayer (ImagePrep Station, Bruker Daltonics,Bremen, Germany).
2.3. Spectral acquisition
Acquisition was performed on an Autoflex III MALDI-TOF/TOF(Bruker Daltonics, Bremen, Germany) mass spectrometer equip-ped with a Smartbeam laser at a repetition rate of 200 Hz. TheFlexImaging v.2.1 software (Bruker Daltonics, Bremen, Germany)was used for image reconstruction. A positive ion linear detectionwas used for MALDI imaging, with masses ranging between m/z2000 and 20,000. Five hundred laser shots per position were ob-tained for selected area. Lateral resolution for MALDI-IMSwas set at100 mm. The software measured an average mass spectrumwith itscoordinates on the slice, at each position.
2.4. Data processing and statistical analysis
Baseline subtraction, normalization, peak detection, and spec-tral alignment were obtained with ClinProTools 2.2 software(Bruker Daltonics, Bremen, Germany). Signal intensities were usedfor all calculations and mass spectra were selected by assigningrepresentative areas of IPMN. The set of individual spectra of lowand high grade IPMN tissue samples were compared to generate alist of differentially expressed peaks. Comparison of peak intensitywas performed using the KruskalleWallis test for continuous data.
2.5. Identification process
2.5.1. Protein extraction from tissue sectionsThe most relevant protein peaks between high and low grade
dysplasia were considered to be identified. Ten sections of IPMNtissue (10 mm thick) were placed on a glass slide for proteinextraction. Extraction was performed with 20 mL of water/aceto-nitrile 40:60 (v/v) and 0.2% TFA. Supernatants were pooled, spin-dried (20,000 g, 2 min at 4 �C) and concentrated in a vacuumcentrifuge.
After the extract was desalted on a C18 Zip-Tip (Millipore,Bedford, MA, USA), the presence of the peak of interest was firstconfirmed using a MALDI target in the linear mode.
2.5.2. SDS-PAGE and bottom-up MS identification strategyProteins were separated on SDS-PAGE and relevant Coomassie-
blue-stained protein bands were excised, destained twice, dehy-drated in acetonitrile and dried for 10 min at 37 �C. Proteinreduction was performed by soaking the bands. Then proteinalkylation was performed in 55 mM iodoacetamide for 45 min inthe dark. The gel pieces were dehydrated and dried.
Tryptic digestion: Gel pieces were then rehydrated for 20 min at4 �C in digestion buffer (10 ng/mL trypsin, 25 mMNH4HCO3). Ten mLof 25 mM NH4HCO3 were added and samples were incubatedovernight at 37 �C. Gel pieces were re-extracted. Supernatants werepooled. Tryptic peptides were resuspended in 0.1% formic acid.
2.5.3. MS and MS/MS of tryptic digestTryptic peptides were analyzed by nano-LC/ESI-MS/MS using an
Easy nano-LC Proxeon system (Thermo Fisher Scientific, San Jose,CA, USA) connected to an LTQ Velos Orbitrap (Thermo Fisher Sci-entific, San Jose, CA, USA) mass spectrometer. A 2 cm long 5 mmparticle size C18 Easy column (Proxeon) was used for peptidepreconcentration. A 10 cm long 3 mm particle size C18 Easy column(Proxeon) was used for peptide separation. The peptide elutiongradient, using a constant flow of 300 nL/minwas from 95% solventA (water e 0.1% formic acid) to 25% solvent B (ACN, 0.1% formicacid) in 20 min, then to 45% B in 40 min and finally to 80% B in

V. Rebours et al. / Pancreatology 14 (2014) 117e124 119
10min. Peptides were analyzed in the orbitrap in full ion scanmodeat a resolution of 30,000 and a mass range of 400e1800 m/z.Fragments were obtained with a collision-induced dissociation(CID) activation with a collision energy of 40%, an activation Q of0.250 for 10 ms and an isolation width of 2 Da analyzed in the LTQ.Maximum injection timewas 100ms forMS in the Orbitrap cell and50 ms for MS/MS in the LTQ. MS/MS data were acquired in a datadependent mode inwhich the 20 most intense precursor ions wereisolated, with a dynamic exclusion of 20 s and an exclusion masswidth of 10 ppm.
Computation: Data were processed with Proteome Discoverer1.3 software (Thermo Fisher scientific) coupled to an in-houseMascot search server (Matrix Science, Boston, MA, USA; version2.3.02). The mass tolerance was set at 10 ppm for precursor ionsand 0.6 Da for fragments. Met-oxidation and Cys-carbamidomethylation were selected as variable modifications.The maximum number of missed cleavages was limited to 2 fortrypsin digestion. MSeMS data were searched against the Swis-sProt database. A threshold of 1% was chosen for this rate.
2.5.4. Top-down MS identification strategyBefore performing the nano-LC/ESI-MS/MS measurement of
intact proteins, the Agilent Human 14 Multiple Affinity RemovalSpin Cartridge was used to remove 14 high-abundant proteins fromthe tissue extract, according to themanufacturer’s instructions. Thedepleted sample was desalted and concentrated with Agilent SpinConcentrators (5000 Molecular Weight Cut-off) first, then in avacuum centrifuge and controlled in MALDI MS.
Accurate mass determination was performed by nano-LC/ESI-MS using an Easy nano-LC Proxeon system (Thermo Fisher Scien-tific, San Jose, CA, USA) connected to an LTQ Velos Orbitrap (ThermoFisher Scientific, San Jose, CA, USA) mass spectrometer. MS and MS/MS spectra were acquired on an Orbitrap analyser at resolutionmode R ¼ 30,000 and 7500 for MS and MS/MS analyses, respec-tively. From an inclusion list, the two most intense charge states ofprecursor ions were fragmented, using CID fragmentation mode at35% relative resonant activation energy for 10msec and an isolationwidth of 1Da. Maximum injection times were 100 ms in MS and200 ms in MS/MS.
MS/MS spectra were then submitted to the server http://ytat2.ijm.univ-paris-diderot.fr/Biomarkers/with the correspondingbiomarker algorithm (Mestivier et al., submitted) by entering themonoisotopic mass of the marker with an error mass of 0.1Da andusing the following parameters: database NCBI nr, taxonomy Homosapiens, whole protein. The algorithm did not identify the peakwithm/z 4745.44, indicating the presence of a post-translational modi-fication. However, manual interpretation of the fragmentationspectrum clearly indicated a sequence tag (QEKNPL) which, whenblasted to the NCBI-nr protein database, returned beta-thymosinswith a high score. A new search was performed with variablemodifications comprising Met-oxidation, N-terminal acetylationand Lysine acetylation.
2.6. Identification validation
The identification was validated by immunohistochemical ana-lyses on an independent series of IPMN (including high and lowgrades of dysplasia) obtained from pancreatic surgical specimensincluded in tissue microarrays (TMA) and from EUS-FNA materialincluded in cell blocks.
2.6.1. Immunohistochemical analysis2.6.1.1. Patients and material. a/Forty five formalin-fixed, paraffin-embedded IPMN were included in 3 tissue microarray (TMA)blocks. The 45 IPMN were retrieved from 45 patients undergoing
surgery for BD, main-duct or mixed IPMN and followed up atBeaujon Hospital. The construction of the tissue microarrays wasperformed using a tissue arrayer (Beecher Instruments, SilverSpring, MD, USA) and each tumor specimenwas represented by five1-mm cores on the tissue microarray. The arrayed IPMN wereclassified into 2 groups (high (n ¼ 24) or low (n ¼ 21) gradedysplasia) according to the WHO pathological criteria [2]. b/Pancreatic EUS-FNA of cystic fluid from 25 patients with BD-IPMNof high (n ¼ 18) or low grade (n ¼ 7) dysplasia were analyzed. Allsamples were selected when surgical specimens were available tostrictly confirm the IPMN grade. All patients presented BD-IPMN,the main pancreatic duct was considered as normal. Mural nodeswere found in 2/7 and 13/18 patients with low and high dysplasia,respectively. The size of the lesions were >30 mm in 6/7 and 12/18patients with low and high dysplasia, respectively. The materialconsisting in minimal 1 ml liquid and floating cells was fixed informalin, centrifuged and mixed by vortexing with a reagent(Shandon, CytoBlock�, Thermo, USA). The pellet (corresponding tothe floating cells) was included in paraffin cell-blocks. c/Two con-trol groups of patients with mucinous cystic neoplasms (MCN)(n¼ 20) and serous cystic neoplasms (SCN) (n¼ 20) were analyzed.The MCN group was composed by 10 cases with low grade ofdysplasia and 10 cases with high grade of dysplasia. Surgicalspecimens of MCN and SCN were formalin-fixed and paraffin-embedded.
2.6.1.2. Techniques. Three-micrometer sections were obtained ofeither TMA-blocks or cell-blocks. The slides were immunolabeledwith rabbit polyclonal antiubiquitin antibody (1:100, Dako, USA) orThymosin-b4 (1:300, LifeSpan BioSciences, USA). Immunohisto-chemistry was performed with an automated immunohistochem-ical stainer according to the manufacturer’s guidelines(Streptavidine-peroxidase with an automate Ventana, Benchmark,USA). Immunostaining was performed after the slides were dew-axed and rehydrated. Antigen retrieval was conducted by pre-treatment at a high temperature. PBS was substituted for theprimary antibody and used as a negative control.
2.6.1.3. Evaluation of the staining. Ubiquitin and thymosin-b4stainings were evaluated in a blinded manner by a pathologist,expert in pancreatic disorders (AC). A score (0e300) was calculatedbymultiplying the intensity (negative, 0; weak, 1; moderate, 2; andstrong, 3) and the percentage of stained cells (0%e100%). Thepattern of expression (cytoplasmic, membranous, or nuclear) wasnoted. For TMA analysis, all cores were evaluated separately and amean score of the 5 cores representing each IPMN was given.
2.7. Statistical analysis
General characteristics were expressed as medians and rangesor percentages. Comparison of data were performed using theKruskalleWallis test for continuous data and the Chi2 test orFisher’s exact test for categorical data. Datawere analyzed with SAS9.1 statistical software for Windows (SAS Institute Inc., Cary, NC,USA). All statistical tests were two-sided; p < 0.05 was consideredto be statistically significant.
3. Results
3.1. Patients and samples
Twenty samples from patients with BD-IPMN were selected,collected and analyzed by MALDI imaging. Low and high gradedysplasia was identified in 10 and 10 samples, respectively. The sexratio was 1/1 (10 women (50% with high grade dysplasia) and 10

Table 1Putative biomarkers detected according to the grade of dysplasia.
m/z Type of dysplasiagrade withrelevant intensityexpression
Intensityexpression inHG area
Intensity expressionin LG area
p
4747 High grade 3.57 1.62 0.00378958 High grade 1.1 0.76 0.00373329 High grade 5.75 3.05 0.0099747 High grade 1.02 0.72 0.0099443 High grade 0.96 0.75 0.01057775 High grade 1.61 0.96 0.01358565 High grade 1.3 0.99 0.013611,188 High grade 0.77 0.58 0.01577176 High grade 2.14 1.02 0.01853222 High grade 4.68 2.86 0.02929554 High grade 1.05 0.67 0.0372398 Low grade 1.24 3.68 0.00092471 Low grade 1.85 4.46 0.0032598 Low grade 2.56 3.81 0.01572529 Low grade 3.25 11.03 0.0185
m/z, mass/charge.HG, High grade.LG, Low grade.
V. Rebours et al. / Pancreatology 14 (2014) 117e124120
men (50% with high grade dysplasia)). Patients in the low gradedysplasia group were operated on due to morphological features ofinvasive carcinoma on in 7 patients (the presence of mural nodules,n ¼ 2; a lesion >30 mm, n ¼ 7) or recurrent acute pancreatitis in 3patients. In the high grade dysplasia group, surgical resection wasperformed because of mural nodules in all patients. The patients’median age at surgerywas 68[53e76] and 62[45e78] (NS) years oldin the low and high grade dysplasia group, respectively.
Surgical procedures were enucleation in 6 patients with lowgrade dysplasia, left pancreatectomy in 2 and 5 patients with lowand high dysplasia, respectively and whipple procedures in 2 and 5patients with low and high dysplasia, respectively. IPMN of themain pancreatic duct was never found in all surgical specimens. Thephenotype of BD-IPMN was gastric in all cases of low gradedysplasia (n ¼ 10/10) and was gastric (n ¼ 1), pancreatic (n ¼ 2) orintestinal (n ¼ 7) in cases of high grade of dysplasia. In the surgicalspecimens, no concomitant invasive lesion (pancreatic adenocar-cinoma) was found. No patient developed pancreatic adenocarci-noma a part from the IPMN lesions after resection (median follow-up after surgical resection: 2 years [1-2]).
3.2. Mass spectral profiling
The median number of spectra acquired by MALDI imaging persample was 1038 [269e2428], representing cell populations ofIPMN, high or low grade dysplasia. The spectra were processed,and multiple spectra were averaged to generate one peak list pertissue sample. Peptide signals in the m/z 2000e20,000 range weredetected. The average spectra of patients with high and low gradedysplasia are represented in Fig. 1. The list of significantly differentintensity expression masses is summarized in Table 1. 11 and 4
Fig. 1. Average spectra expressed in high (red
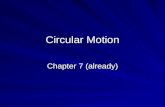
peaks were over expressed in areas of high and lowgrade dysplasia,respectively. Expression of the relevant peak m/z 4747 by MALDIimaging is shown in Fig. 2.
3.3. Identification process
Two of the most discriminating peaks, m/z 8565 and 4747,which were more intense in high grade IPMN were selected foridentification.
) and low (green) grade of dysplasia area.

Fig. 2. Optical image (A) and Ion intensity maps (B,C) of the relevant mass (m/z 4747) in an area of high (pink circle) and low grade (green circle) IPMN.
V. Rebours et al. / Pancreatology 14 (2014) 117e124 121
Tissue extracts were first analyzed by MALDI MS. The MALDITOF spectrum in the linear mode provided the m/z of 8565 and4747.
The human Polyubiquitin (P0CG47, MW ¼ 25.7 KDa) with aMascot score of 319.22, a sequence coverage of 77.29% and 7assigned peptides was identified based on analysis of an adequatelyexcised band from SDS-PAGE by the bottom-up approach using a
Fig. 3. Ubiquitin identification: CID fragmentation spectrum of the 762.392þ (MHþ ¼ 15
MASCOT database search engine. Thus m/z 8565 corresponded tothe monomeric ubiquitin (76 aa, nominal mass 8560 Da) (Fig. 3).
The mono-isotopic molecular weight of MHþ ¼ 4745.44 Da wasobtained by deconvolution of the nano-LC/ESI-MS spectrum by topdown analysis. The MS/MS spectrum was submitted to theBiomarkers@IJM server and resulted in the identification of anacetylated fragment of the thymosin-b4 (2e42) (ID: TIB4_HUMAN,
23.78) precursor ion selected in the LC-ESI/MSMS separation of the tryptic digest.

V. Rebours et al. / Pancreatology 14 (2014) 117e124122
P62328, MHþ ¼ 4745.417) with a very high confidence score(Omssa: E-value: 1.37 E-9, P-value: 5.74 E-16) (Fig. 4).
3.4. Identification validation
3.4.1. Immunohistochemical analysis (Fig. 5)
- Ubiquitin: expressionwas nuclear or cytoplasmic. Ubiquitinwasexpressed in all types of IPMN phenotype. On TMA samples, themedian nuclear and cytoplasmic staining scores of Ubiquitinwere 101 [0e257] and 69 [0e270] in high and low gradedysplasia, respectively, (p ¼ 0.04). On EUS FNA samples, nuclearpositivity was observed in high grade IPMN in 94% of the sam-ples versus 14% (p ¼ 0.0004). The median high and low gradeexpression scores were 80 [15e240] and 0 [0e60], respectively.Sensitivity, specificity, positive and negative predictive valueswere 94, 86, 94 and 86%, respectively. On SCN samples, themedian expression score was 300 [200e300]; on MCN samplesthe median high and low grade expression scores were 250[120e300] and 100 [50e300], respectively (p ¼ 0.024).
- Thymosin-b4: expression was cytoplasmic. Thymosin-b4expression was confirmed on high grade IPMN included in tis-sue microarrays. The expression was found in all types of IPMNphenotypes. On TMA samples, the median cytoplasmic stainingscores of thymosin- b4 were 140 [100e250] and 80 [20e200] inhigh and low grade dysplasia, respectively, (p ¼ 0.0011).Immunohistochemical positivity was observed in high gradeIPMN in 70% of the TMA samples versus 29% in low grade IPMN(p¼ 0.013). Sensitivity, specificity and negative predictive valueswere 70%, 71% and 67%, respectively. On SCN samples, thethymosin-b4 expression score was negative in all cases; on MCNsamples the median high and low grade expression scores were180 [100e250] and 50 [0e140], respectively (p ¼ 0.005).
4. Discussion
Proteomic analysis of high and low grade IPMN by MALDI im-aging showed specific peaks of protein expression according to thegrade of dysplasia. Fifteen putative peaks were found: two of thepeaks that were expressed in high grade dysplasia (m/z: 8565 and4747) were identified as themonomeric ubiquitin and an acetylatedfragment of the thymosin-b4. Validation of these peaks was per-formed on independent series, by immunohistochemistry on sur-gically resected IPMN included in tissue microarrays and on EUS
Fig. 4. Thymosin-b4 identification: CID fragmentation spectrum of the 792.086þ (MHþ ¼slices.
FNA samples. According to these methods of validation, theexpression of ubiquitin was higher in high grade IPMN (94% versus14%, p ¼ 0.0004). Strong expression of thymosin-b4 was confirmedin high grade IPMN on tissue micro arrays (p ¼ 0.011).
Follow up of patients with BD-IPMN remains a challenge.Invasive criteria for resection of BD-IPMN in internationalconsensus guidelines are a lesion >30 mm, the presence of muralnodule and positive cytology [6]. A rapid increase in cyst size wasrecently added as a possible criteria for resection [10,11]. Althoughthe usefulness of these criteria has been validated [12,13], no spe-cific morphological criteria have been shown to be well correlatedto the grade of dysplasia and the rapid progression of small BD-IPMN into invasive carcinoma has be observed despite closeannual follow up. On the other hand, the frequency of malignancyin operated BD-IPMN was only between 6.3 and 51% in recentstudies and invasive IPMN represent 1.4%e36.7% of the patients[5,14e16]. It has been suggested that the criteria of size >3 cmcould be a less important predictive marker of malignancy than thepresence of a mural nodule or positive cytology. This highlights theneed for more precise tools for the diagnosis and follow up of thisentity.
Several studies have examined the potential role of cyst fluidanalysis, proteomics, gene expression, and microRNA as accuratepredictive biomarkers to distinguish cysts with a malignant po-tential from the large majority of others that do not progress. Re-ports have mentioned pancreatic juice cytology and fluid levels oftumors markers [17,18]. CEA (>800 ng/mL) and CA 72.4 (>40 U/mL)levels have been shown to have a good negative predictive value inthe preoperative differential diagnosis of benign versus malignantIPMN (96%). Similarly, somatic KRAS gene mutations in cyst fluidDNA paired with a loss of heterozygosity were highly predictive ofmalignancy in pancreatic cysts [19,20]. cDNAmicroarray analysis tocharacterize gene expression profiles demonstrated expressionchange in more than half of IPMN. Deregulated microRNA expres-sion in pancreatic cyst fluid of miR-21, miR-221, and miR-17-3p wassignificantly higher in mucinous versus non-mucinous cysts [21].Although numerous chemical and molecular parameters have beenanalyzed in cyst fluid to increase the specificity of the diagnosis ofcarcinoma in IPMN, none has been found to be specific.
In this study we used the in situ proteomic approach to searchfor new biomarkers of dysplasia in IPMN to obtain a more accuratepicture of cell physiopathology. MALDI imaging was pertinent dueto the marked heterogeneity of tissue samples in IPMNs, whichcontain a limited number of epithelial cells in close associationwith
4744) precursor ion selected in the MSMS separation of protein extracted from tissue

Fig. 5. Immunohistochemical expression of Ubiquitin (AeB) and Thymosin-b4 (CeD) on low (AeC) or high (BeD) grade IPMN included in tissue microarrays. Ubiquitin is notdetected on this low grade IPMN (A), but is strongly detected, mainly in the nucleus and also in the cytoplasm of most tumor cells in this high grade IPMN (B). Original magnification�20 objective; immunostaining counterstained with haematoxylin. Thymosin-b4 is not detected in tumor cells in this low grade IPMN (C). It is strongly detected in high grade IPMN(D), mainly in the cytoplasm of tumor cells. Original magnification �20 objective; immunostaining counterstained with haematoxylin.
V. Rebours et al. / Pancreatology 14 (2014) 117e124 123
a significant amount of fibrous tissue. Only MALDI imaging coulddetect markers that were specifically expressed by epithelial cells,which could not have been identified if proteomic analysis hadbeen performed from protein extracted from the tissue by con-ventional procedures. Even selective microdissection did not pro-vide enough material to run classical 2D-gels.
Monomeric ubiquitin was identified as a putative biomarker ofhigh grade dysplasia expressed in IPMN. Ubiquitin is a conservedregulatory protein that is tagged to proteins as a signal for pro-teasome degradation and has been involved in the control ofmultiple cellular processes including cell cycle control, transcrip-tion regulation, DNA damage repair and endocytosis. Ubiquitinmetabolism enzymes feature prominently as either oncogenes ortumor suppressors in several cancers and many signaling/regula-tory pathways relevant to cancer [22]. The role of ubiquitin hasalready been described in non-pancreatic cancers, especially E3ubiquitin ligases, which clearly contribute to the development ofcancer. There are very few studies on the role of the ubiquitinsystem in pancreatic diseases. One study on pancreatic cancer hasshown that the ubiquitin-proteasome pathway mediates gelsolinprotein downregulation and the status of ubiquitinated gelsolinwas correlated with invasion criteria, including lymph node me-tastases [23]. Recently exomic DNA sequences were obtained fromthe neoplastic epithelium of resected pancreatic cysts. NumerousRNF43 inactivating mutations, a gene coding for a protein withintrinsic E3 ubiquitin ligase activity, were found in IPMN [24].
Thymosin-b4 belongs to the family of actin-binding poly-peptides that promote or inhibit actin assembly and sequester actinmonomers within the cell [25]. It has many functions including:repairing injured tissues and an anti-inflammatory action in
monocyte/macrophages, to mediate angiogenesis [26e28].Thymosin-b4 has been shown to be involved in metastatic pro-gression inmelanoma, non-small cell lung cancer and other cancers[29,30]. Its over expression causes additional actin sequestration, aless rigid cytoskeleton, and allows more motility in the cell [31,32].In normal pancreatic tissue, thymosin-b4 distribution is mainlyobserved in islet cells [33]. In pancreatic cancer cells lines, overexpression of thymosin-b4 mRNA was found with increasedsecretion of proinflammatory cytokines such as IL-6, IL-8 and MCP-1 in a single series [34]. No data are available for IPMN but ourresults suggest that it is involved in the malignant transformationof IPMN. This hypothesis was indirectly strengthened by the recentresults of proteomic analysis of PanIN lesions. Thymosin-beta 4 wasfound significantly increased in sera of mice with PanIN lesions[35]. Ubiquitin and Thymosin-beta 4 proteins were already detec-ted in MALDI imaging approaches for others tumors. It revealedtheir potential main role in the oncogenesis process in general butthese findings revealed their high prevalence and main abundancein tissues in general. It means that these results have to be inter-pretedwith caution. A real risk of overlap between other pancreatic(or non-pancreatic) tumoral lesions exists in patients with BD-IPMN. This could be a difficulty to develop blood analysis withrelevant specificity in these patients. To confirm the specificity andthe sensitivity of positive immunochemical analysis on EUS-FNAsamples, a prospective study would have to be conducted.
This study demonstrates a profiling and imaging strategy fol-lowed by protein identification and validation to detect andvalidate biomarkers for IPMN dysplasia grade. Positive immuno-chemical staining for ubiquitin and thymosin-b4 on EUS-FNAsamples could provide strong support for preventive resection.

V. Rebours et al. / Pancreatology 14 (2014) 117e124124
Because of the limitations of morphological procedures, systematicevaluation of ubiquitin and thymosin-b4 by ELISA in mucus andblood could become a tool to monitor patients with branch ductIPMN.
Grant support
This study was supported by the French Association for CancerResearch (ARC, Association pour la Recherche sur le Cancer).
Author’s contribution
Dr Vinciane Rebours: Study design and concept, acquisition ofthe data, data analysis, statistical analysis and manuscript drafting.
Dr Julie Le Faouder: Acquisition of the data, data analysis.Samira Laouirem, Mounya Mebarki, Miguel Albuquerque, Thi-
baut Léger and Dr Jean-Michel Camadro: Acquisition of the data,MS data analysis.
Pr Philippe Ruszniewski: Critical revision and Manuscriptdrafting.
Pr Valérie Paradis and Pr Philippe Lévy: Critical revision.Pr Pierre Bedossa: Study design and critical revision.Pr Anne Couvelard: Study design, acquisition of the data, critical
revision and manuscript drafting.
Conflicts of interest
No conflicts of interest exist.
Acknowledgment
Authors are grateful to all members of the pathology Unit ofBeaujon Hospital (Tissuthèque de l’hôpital Beaujon), especiallyBrigitte Boulangé, Nathalie Colnot, Sylvie Mosnier and OlivierBoucher.
References
[1] Itai Y, Ohhashi K, Nagai H, Murakami Y, Kokubo T, Makita K, et al. “Ductec-tatic” mucinous cystadenoma and cystadenocarcinoma of the pancreas.Radiology 1986;161(3):697e700.
[2] Klöppel G, Solcia E, Capella C, Sobin IH. International histological typing oftumors of the exocrine pancreas; 1996.
[3] Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores-Saavedra J, Biankin AV,et al. An illustrated consensus on the classification of pancreatic intraepithelialneoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol2004;28(8):977e87.
[4] Shi C, Klein AP, Goggins M, Maitra A, Canto M, Ali S, et al. Increased prevalenceof precursor lesions in Familial pancreatic cancer patients. Clin Cancer Res2009;15(24):7737e43.
[5] Lévy P, Jouannaud V, O’Toole D, Couvelard A, Vullierme MP, Palazzo L, et al.Natural history of intraductal papillary mucinous tumors of the pancreas:actuarial risk of malignancy. Clin Gastroenterol Hepatol 2006;4(4):460e8.
[6] Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, et al.,International Association of Pancreatology. International consensus guidelines2012 for the management of IPMN and MCN of the pancreas. Pancreatology2012 MayeJun;12(3):183e97.
[7] Corcos O, Couvelard A, Dargère D, Sauvanet A, Hammel P, Paradis V, et al.Proteomic assessment of markers for malignancy in the mucus of intraductalpapillary mucinous neoplasms of the pancreas. Pancreas 2012;41(2):169e74.
[8] Stoeckli M, Chaurand P, Hallahan DE, Caprioli RM. Imaging mass spectrom-etry: a new technology for the analysis of protein expression in mammaliantissues. Nat Med 2001;7(4):493e6.
[9] Fournier I, Day R, Salzet M. Direct analysis of neuropeptides by in situ MALDI-TOF mass spectrometry in the rat brain. Neuro Endocrinol Lett 2003;24(1e2):9e14.
[10] Kang MJ, Jang JY, Kim SJ, Lee KB, Ryu JK, Kim YT, et al. Cyst growth ratepredicts malignancy in patients with branch duct intraductal papillarymucinous neoplasms. Clin Gastroenterol Hepatol 2011;9(1):87e93.
[11] Rautou PE, Lévy P, Vullierme MP, O’Toole D, Couvelard A, Cazals-Hatem D,et al. Morphologic changes in branch duct intraductal papillary mucinousneoplasms of the pancreas: a midterm follow-up study. Clin GastroenterolHepatol 2008;6(7):807e14.
[12] Nagai K, Doi R, Ito T, Kida A, Koizumi M, Masui T, et al. Single-institutionvalidation of the international consensus guidelines for treatment of branchduct intraductal papillary mucinous neoplasms of the pancreas.J Hepatobiliary Pancreat Surg 2009;16(3):353e8.
[13] Sai JK, Suyama M, Kubokawa Y, Watanabe S, Maehara T. Pancreatic-duct-lavage cytology in candidates for surgical resection of branch-duct intraductalpapillary mucinous neoplasm of the pancreas: should the InternationalConsensus Guidelines be revised? Gastrointest Endosc 2009;69(3 Pt 1):434e40.
[14] Sadakari Y, Ienaga J, Kobayashi K, Miyasaka Y, Takahata S, Nakamura M, et al.Cyst size indicates malignant transformation in branch duct intraductalpapillary mucinous neoplasm of the pancreas without mural nodules.Pancreas 2010;39(2):232e6.
[15] Kim SC, Park KT, Lee YJ, Lee SS, Seo DW, Lee SK, et al. Intraductal papillarymucinous neoplasm of the pancreas: clinical characteristics and treatmentoutcomes of 118 consecutive patients from a single center. J HepatobiliaryPancreat Surg 2008;15(2):183e8.
[16] Kawamoto S, Lawler LP, Horton KM, Eng J, Hruban RH, Fishman EK. MDCT ofintraductal papillary mucinous neoplasm of the pancreas: evaluation of fea-tures predictive of invasive carcinoma. AJR Am J Roentgenol 2006;186(3):687e95.
[17] Maire F, Voitot H, Aubert A, Palazzo L, O’Toole D, Couvelard A, et al. Intraductalpapillary mucinous neoplasms of the pancreas: performance of pancreaticfluid analysis for positive diagnosis and the prediction of malignancy. Am JGastroenterol 2008;103(11):2871e7.
[18] Yamaguchi K, Nakamura M, Shirahane K, Kawamoto M, Konomi H, Ohta M,et al. Pancreatic juice cytology in IPMN of the pancreas. Pancreatology2005;5(4e5):416e21.
[19] Khalid A, McGrath KM, Zahid M, Wilson M, Brody D, Swalsky P, et al. The roleof pancreatic cyst fluid molecular analysis in predicting cyst pathology. ClinGastroenterol Hepatol 2005;3(10):967e73.
[20] Khalid A, Zahid M, Finkelstein SD, LeBlanc JK, Kaushik N, Ahmad N, et al.Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report ofthe PANDA study. Gastrointest Endosc 2009;69(6):1095e102.
[21] Ryu JK, Matthaei H, Dal Molin M, Hong SM, Canto MI, Schulick RD, et al.Elevated microRNA miR-21 levels in pancreatic cyst fluid are predictive ofmucinous precursor lesions of ductal adenocarcinoma. Pancreatology2011;11(3):343e50.
[22] Clague MJ, Urbe S. Ubiquitin: same molecule, different degradation pathways.Cell 2010;143(5):682e5.
[23] Ni XG, Zhou L, Wang GQ, Liu SM, Bai XF, Liu F, et al. The ubiquitin-proteasomepathway mediates gelsolin protein downregulation in pancreatic cancer. MolMed 2008;14(9e10):582e9.
[24] Wu J, Jiao Y, Dal Molin M, Maitra A, de Wilde RF, Wood LD, et al. Whole-exome sequencing of neoplastic cysts of the pancreas reveals recurrent mu-tations in components of ubiquitin-dependent pathways. Proc Natl Acad Sci US A 2011;108(52):21188e93.
[25] Hertzog M, van Heijenoort C, Didry D, Gaudier M, Coutant J, Gigant B, et al.The beta-thymosin/WH2 domain; structural basis for the switch from inhi-bition to promotion of actin assembly. Cell 2004;117(5):611e23.
[26] Goldstein AL, Hannappel E, Kleinman HK. Thymosin beta4: actin-sequesteringprotein moonlights to repair injured tissues. Trends Mol Med 2005;11(9):421e9.
[27] Young JD, Lawrence AJ, MacLean AG, Leung BP, McInnes IB, Canas B,et al. Thymosin beta 4 sulfoxide is an anti-inflammatory agents gener-ated by monocytes in the presence of glucocorticoids. Nat Med1999;5(12):1424e7.
[28] Sosne G, Szliter EA, Barrett R, Kernacki KA, Kleinman H, Hazlett LD. Thymosinbeta 4 promotes corneal wound healing and decreases inflammation in vivofollowing alkali injury. Exp Eye Res 2002;74(2):293e9.
[29] Hardesty WM, Kelley MC, Mi D, Low RL, Caprioli RM. Protein signatures forsurvival and recurrence in metastatic melanoma. J Proteomics 2011;74(7):1002e14.
[30] Ji P, Diederichs S, Wang W, Böing S, Metzger R, Schneider PM, et al. MALAT-1,a novel noncoding RNA, and thymosin beta4 predict metastasis and survivalin early-stage non-small cell lung cancer. Oncogene 2003;22(39):8031e41.
[31] Nummela P, Yin M, Kielosto M, Leaner V, Birrer MJ, Holtta E. Thymosin beta4is a determinant of the transformed phenotype and invasiveness of S-ade-nosylmethionine decarboxylase-transfected fibroblasts. Cancer Res2006;66(2):701e12.
[32] Liu CR, Ma CS, Ning JY, You JF, Liao SL, Zheng J. Differential thymosin beta 10expression levels and actin filament organization in tumor cell lines withdifferent metastatic potential. Chin Med J (Engl) 2004;117(2):213e8.
[33] Nemolato S, Cabras T, Cau F, Fanari MU, Fanni D, Manconi B, et al. Differentthymosin Beta 4 immunoreactivity in foetal and adult gastrointestinal tract.PLoS One 2010;5(2):e9111.
[34] Zhang Y, Feurino LW, Zhai Q, Wang H, Fisher WE, Chen C, et al. Thymosin Beta4 is overexpressed in human pancreatic cancer cells and stimulates proin-flammatory cytokine secretion and JNK activation. Cancer Biol Ther2008;7(3):419e23.
[35] Grüner BM, Hahne H, Mazur PK, Trajkovic-Arsic M, Maier S, Esposito I, et al.MALDI imaging mass spectrometry for in situ proteomic analysis of preneo-plastic lesions in pancreatic cancer. PLoS One 2012;7(6):e39424.