CXCR7 is induced by hypoxia and mediates glioma cell migration

ORIGINAL RESEARCH
Hypoxia Upregulates Estrogen Receptor b in Pulmonary ArteryEndothelial Cells in a HIF-1a–Dependent MannerAndrea L. Frump1*, Mona Selej1*‡, Jordan A. Wood1, Marjorie Albrecht1, Bakhtiyor Yakubov1, Irina Petrache1,2x, andTim Lahm1,2,3
1Division of Pulmonary, Critical Care, Sleep and Occupational Medicine, Department of Medicine, 2Richard L. Roudebush VA MedicalCenter, and 3Department of Cellular and Integrative Physiology, Indiana University School of Medicine, Indianapolis, Indiana
Abstract
17b-Estradiol (E2) attenuates hypoxia-induced pulmonaryhypertension (HPH) through estrogen receptor (ER)-dependenteffects, including inhibition of hypoxia-induced endothelial cellproliferation; however, the mechanisms responsible for this remainunknown. We hypothesized that the protective effects of E2 in HPHare mediated through hypoxia-inducible factor 1a (HIF-1a)-dependent increases in ERb expression. Sprague-Dawley rats andERa or ERb knockout mice were exposed to hypobaric hypoxiafor 2–3 weeks. The effects of hypoxia were also studied in primaryrat or human pulmonary artery endothelial cells (PAECs).Hypoxia increased expression of ERb, but not ERa, in lungs fromHPH rats as well as in rat and human PAECs. ERbmRNA timedependently increased in PAECs exposed to hypoxia. NormoxicHIF-1a/HIF-2a stabilization increased PAEC ERb, whereas HIF-1aknockdown decreased ERb abundance in hypoxic PAECs. In turn,ERb knockdown in hypoxic PAECs increased HIF-2a expression,suggesting a hypoxia-sensitive feedback mechanism. ERbknockdown in hypoxic PAECs also decreased expression of the HIFinhibitor prolyl hydroxylase 2 (PHD2), whereas ERb activationincreased PHD2 and decreased bothHIF-1a andHIF-2a, suggestingthat ERb regulates the PHD2/HIF-1a/HIF-2a axis during hypoxia.Whereas hypoxic wild-type or ERa knockout mice treated with E2demonstrated less pulmonary vascular remodeling and decreasedHIF-1a after hypoxia compared with untreated hypoxic mice, ERb
knockout mice exhibited increased HIF-2a and an attenuatedresponse to E2 during hypoxia. Taken together, our resultsdemonstrate a novel and potentially therapeutically targetablemechanismwhereby hypoxia, viaHIF-1a, increases ERb expressionand the E2-ERb axis targets PHD2, HIF-1a, and HIF-2a toattenuate HPH development.
Keywords: hypoxia-inducible factor 1a; hypoxia-induciblefactor 2a; pulmonary hypertension; prolyl hydroxylase 2; 17b-estradiol
Clinical Relevance
Our study has three important clinical implications. First, weidentify a novel and lung-specific estrogen receptor b responseto hypoxia that may explain the protective effects drivenby estrogen in hypoxia-induced pulmonary hypertension.This finding has potential therapeutic implications becausealthough hypoxia-induced pulmonary hypertension is oneof the most common forms of pulmonary hypertensionworldwide, no therapeutic options exist. Second, our resultsare the first to link estrogen receptor to the regulation ofhypoxia-inducible factor 2. Third, our results may help solvethe “estrogen paradox” in pulmonary arterial hypertension.
(Received in original form May 1, 2017; accepted in final form January 11, 2018 )
*These authors contributed equally to this work.‡Present address: Actelion Pharmaceuticals and University of California, San Francisco, San Francisco, California.xPresent address: National Jewish Health, Denver, Colorado.
Supported by VA Merit grant 1I01BX002042-01A2 (T.L.) and National Institutes of Health grants 5T32HL091816-05 (A.L.F.), NCATS 5TL1TR001107-02(A.L.F.), and R01HL077328 (I.P.).
Author Contributions: A.L.F., M.S., I.P. and T.L. designed experiments, analyzed and interpreted data, and wrote the manuscript. A.L.F., M.S., J.A.W., M.A.,B.Y., and T.L. performed experiments.
Correspondence and requests for reprints should be addressed to Tim Lahm, M.D., Walther Hall, C400, 980 W. Walnut Street, Indianapolis, IN 46202.E-mail: [email protected].
This article has a data supplement, which is accessible from this issue’s table of contents at www.atsjournals.org.
Am J Respir Cell Mol Biol Vol 59, Iss 1, pp 114–126, Jul 2018
Copyright © 2018 by the American Thoracic Society
Originally Published in Press as DOI: 10.1165/rcmb.2017-0167OC on February 2, 2018
Internet address: www.atsjournals.org
114 American Journal of Respiratory Cell and Molecular Biology Volume 59 Number 1 | July 2018

Pulmonary hypertension (PH) encompassesa heterogeneous group of pulmonaryvascular disorders characterized byincreased vasoconstriction and aberrantmuscularization of the pulmonary arteries(PAs) that lead to increased right ventricularafterload and, if left untreated, rightventricular failure and death (1–3). Severalforms of PH are characterized by sexualdimorphism. For example, hypoxia-induced PH (HPH), one of the mostcommon forms of PH worldwide (4–6),is less common and less severe in females(reviewed in Reference 7). On the otherhand, pulmonary arterial hypertension(PAH), a progressive vasculopathycharacterized by uncontrolled endothelialproliferation, obliterative PA lesions, andmarkedly elevated PA pressures, exhibits afemale/male ratio that ranges from 1.4 to4.1:1 (reviewed in Reference 7). Thesedisparate observations have been attributedto dichotomous and tissue-dependenteffects of 17b-estradiol (E2) and itsreceptors (estrogen receptor a [ERa] andERb). For example, although E2 may havedetrimental effects on the pulmonaryvasculature in the context of a BMPR2mutation (8, 9), it has favorable ER-dependent effects on pulmonary vasculartone and PA endothelial cell (PAEC)homeostasis in hypoxic conditions (10–13).Interestingly, E2’s vasculoprotectiveeffects on PAECs are not observed duringnormoxic conditions, indicating that E2exerts specific actions during hypoxia thatmay not be active during nonhypoxicconditions. Further studies of the specificeffects of hypoxia on E2 signaling in thepulmonary vasculature are therefore ofcrucial importance, as such investigationsmay 1) identify potential novel therapeutictargets for HPH and PH induced bychronic lung diseases, and 2) elucidatewhether alterations in the E2-ER axis—similarly to recently identified alterations inestrogen metabolism (14, 15)—contributeto the predisposition of females for PAH.Given our recently reported observationsof hypoxia-specific and ER-mediatedprotective E2 signaling in HPH (10, 16), weaimed to identify whether and how hypoxiaaffects ER expression and function in thepulmonary vasculature.
ERa and ERb (encoded by the genesEsr1 and Esr2, respectively) are proteinsthat belong to the nuclear-receptorsuperfamily of transcription factors andare expressed in both sexes (17, 18). Two
subtypes exist, both of which are expressedin the histologically normal lung, withERb purportedly being more abundantthan ERa (19–22). In addition todifferences in tissue expression patterns,the two ERs also differ in their biologicalfunctions (21–24). For instance, in thesetting of breast and prostate cancer,ERa mediates proproliferative effects andERb mediates antiproliferative signaling(25–28). Interestingly, ERb exhibitsrelevant effects in PAECs. Specifically,ERb mediates E2-induced increases inendothelial nitric oxide synthase activityand prostacyclin synthesis in fetal bovinePAECs (29, 30), and attenuates ERK1/2(p42/44 MAPK) activation in hypoxicrat PAECs (10). Administration of aselective ERb agonist replicates E2’sinhibitory effects on hypoxic pulmonaryvasoconstriction in isolated rat PA rings,and this effect is mediated in a nitricoxide– and endothelium-dependentmanner (13). Lastly, in a rat model ofHPH, E2-mediated decreases in pulmonaryvascular remodeling were attenuatedafter cotreatment with a selective ERbantagonist (10).
These findings implicate a uniquepathway of ER-dependent signaling duringhypoxia that inhibits pulmonary vascularremodeling. We sought to investigatewhether and how hypoxia affects ERexpression and function in vitro andin vivo. We demonstrate for the firsttime that hypoxia upregulates ERbexpression in isolated PAECs as wellas in the pulmonary vasculature, andthat this increase is dependent onhypoxia-inducible factor 1a (HIF-1a).Furthermore, we provide the first evidencedemonstrating that ERb decreases bothHIF-1a and HIF-2a in vitro and in vivo,and is necessary for E2’s vasculoprotectiveeffects in a murine model of HPH.This novel role of ERb in regulatingHIF-2a is of particular relevance becausedysregulated HIF-2a signaling has recentlybeen reported to be a potent driver of theformation of obliterative lesions in PH (31,32). Finally, we provide evidence that ERbstimulates expression of the HIF-ainhibitor prolyl hydroxylase 2 (PHD2) inPAECs, thus identifying attenuation ofHIF-1a and HIF-2a signaling as a novelmechanism of E2 action in the pulmonaryvasculature. Parts of this study havebeen previously reported in abstractform (33, 34).
Methods
Please refer to the data supplement fordetails regarding the materials and methodsused in this work.
Animal CareThe animal studies were approved bythe Indiana University School of MedicineInstitutional Animal Care and UseCommittee, and adhered to the NationalInstitutes of Health guidelines for the careand use of laboratory animals under theAnimal Welfare Act.
In Vivo StudiesThe HPH model has been describedpreviously (10). Male Sprague-Dawleyrats (Charles River) or wild-type (WT),Esr12/2, and Esr22/2 C57BL/6 mice(Jackson Laboratories) were exposed to 2–3weeks of hypobaric hypoxia, respectively.A subgroup of mice were treated with E2(75 mg/kg/d via subcutaneous pellets [10];Innovative Research of America) for theduration of hypoxia exposure.
In Vitro StudiesPrimary rat PAECs (from Drs. Troy Stevensand Diego Alvarez, University of SouthAlabama) or human PAECs (Lonza) wereexposed to hypoxia (1% O2) using anInvivO2 hypoxia workstation (Ruskinn,Inc.) as described previously (10). Controlcells of identical passage/confluence weregrown concomitantly under room-airconditions. To verify that no detectable oronly minimal amounts of E2 were presentin the culture media, E2 concentrationswere quantified via ELISA (Calbiotech)and by comparing levels with those fromE2-treated media (see Fig. E1 in the datasupplement). Cells were treated withdeferoxamine (DFO; 10–100 mM;Sigma-Aldrich) for 24 hours in roomair or with the selective ERb agonistdiarylpropionitrile (DPN; 1–100 nM; Tocris)for 48 hours at 1–5% O2. Cells were transfectedusing Lipofectamine 2000 with siHIF-1a orsiERb (ThermoFisher) for 24 hours andexposed to hypoxia for 24–48 hours.
ImmunocytochemistryRat or human PAECs were seeded ongelatin-coated coverslips and exposed toroom air or hypoxia. The EC phenotypewas confirmed (Figure E2). Primaryantibodies against ERa or ERb (1:200; Santa
ORIGINAL RESEARCH
Frump, Selej, Wood, et al.: Hypoxia and Estrogen Receptor b 115

Cruz) were used. Alexa Fluor 488 conjugatedanti-rabbit secondary antibody (1:200;ThermoFisher) and DAPI (ThermoFisher)mounting media were used. Ten fields perslide were taken using a Nikon microscopeat 403 . ER expression was quantified as theaverage megapixel intensity per numberof nuclei by ImageJ (National Institutesof Health).
ImmunohistochemistryLung sections were stained with ERa (1:500,Santa Cruz) or ERb (1:10; Dako) andquantified using Metamorph software.WT, Esr12/2, and Esr22/2 mouse lungswere stained for a-smooth muscle actin(1:500; Abcam). Quantification wasperformed as previously described (10).
Western BlottingTissue/cell lysis was performed as previouslydescribed (10). The following antibodieswere used: ERa (1:1,000; Santa Cruz), ERb(1:1,000; Santa Cruz), HIF-1a and HIF2-a
(1:1,000; Novus Biological), PHD2 (1:1,000;Abcam), and vinculin (1:5000; Calbiochem).Densitometry was performed via ImageJ.
Real-Time qRT-PCRTotal RNA was isolated from rat andhuman PAECs using the RNeasy Plus MiniKit (Qiagen), and 1 mg total RNA wasreverse transcribed using the iScript cDNAsynthesis kit (Bio-Rad). TaqMan geneexpression assays for Esr1, Esr2, and 18S(ThermoFisher; for assay IDs, see the datasupplement) were used. Changes inmRNA expression were determined bythe comparative CT (22ΔΔC
T) method andexpressed as the fold change comparedwith normoxic controls.
Statistical AnalysesResults are expressed as means 6 SEM.At least three independent experiments(run in duplicates) were performed for allin vitro studies. Statistical analyses wereperformed with GraphPad Prism 6 (La Jolla,
CA). Student’s t test or one-way ANOVA withTukey’s post hoc or Dunnett’s correction wereused when appropriate. Statistical significancewas accepted at P , 0.05.
Results
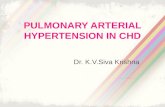
Hypoxia Increases ERb, but Not ERa,in Rat LungsOur previous studies in HPH rats suggestedthat hypoxia may upregulate ERb protein inthe pulmonary vasculature (10). To furtherinvestigate this finding, we evaluatedlung ERa and ERb protein expression inchronically hypoxic Sprague-Dawley rats byimmunohistochemistry and Western blot.Although 2 weeks of hypoxia tended todecrease lung ERa abundance (Figures 1A–1C), hypoxia robustly increased the lungexpression of ERb (Figures 1A and 1D–1E).ERb staining localized to PAECs, suggestingthat ERb is predominantly expressed inthese cells. The hypoxia-induced increase in
1.5
1.0
0.5
0.0
0.0Normoxia Hypoxia
Normoxia
Lung
ER
/ V
incu
linLu
ng E
R
/ Vin
culin
Hypoxia
*
0.12
0.14
0.16
0.18
0.20
Normoxia
ER
ERNegative ControlA
B
D
C
E
Vinculin
ER
ER
Vinculin
Hypoxia
Normoxia Hypoxia Normoxia Hypoxia
—66 kD
—120 kD
—56 kD
—120 kD
Normoxia Hypoxia
Figure 1. Hypoxia increases expression of estrogen receptor b (ERb), but not ERa, in the lung. (A) Representative immunohistochemistry images of lungsections from normoxic and hypoxic animals stained for ERa and ERb. Note the increase in ERb-positive cells (arrow) in pulmonary arteries from hypoxic rats.Positive staining for ERb was mainly present in endothelial cells, and there was no significant staining of smooth muscle cells. (B–E) Protein expression of(B) ERa and (D) ERb in whole-lung homogenates from rats exposed to 2 weeks of normoxia (fraction of inspired oxygen [FIO2
] 21%) or chronic hypobarichypoxia (Patm = 362 mm Hg; equivalent to 10% FIO2
). Quantification of (C) lung ERa and (E) ERb by densitometry is shown. Images were obtained at3 40 magnification. Scale bars = 50 mm; n = 4/group. Error bars in scatterplots are means 6 SEM. *P , 0.05 versus normoxia control by t test.
ORIGINAL RESEARCH
116 American Journal of Respiratory Cell and Molecular Biology Volume 59 Number 1 | July 2018

ERb was lung specific, as no increase wasnoted in the right ventricle (RV), leftventricle, or liver (Figure E3). In fact, ERbexpression was significantly decreased in theRV and liver, suggesting differential effectsof hypoxia on ERb expression in the lungversus other organ systems.
Hypoxia Increases Expression ofERb, but Not ERa, in Primary Rat andHuman PAECsBecause ERb appeared to be primarilyexpressed in PAECs and upregulated underhypoxic conditions, we next evaluated theeffect of hypoxia on ER expression in
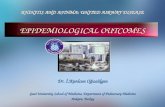
primary rat PAECs. Rat PAECs werecultured under hypoxic conditions (1% O2)for 4, 24, or 72 hours, and ER expressionwas evaluated by immunocytochemistry.As was observed in vivo, ERa was notsignificantly affected by hypoxia exposurecompared with normoxic controls (Figures2A and 2B). In contrast, hypoxia timedependently increased ERb proteincompared with normoxic controls (Figures2A and 2B). Interestingly, this hypoxia-induced increase in ERb expression wasaccompanied by a localization patternsuggestive of nuclear translocation (Figures2A and 2C). To investigate whether the
hypoxia-induced upregulation of ERb istranscriptionally regulated, we used real-time RT-PCR to quantify ERb mRNA. Asexpected, ERb mRNA was significantlyincreased in rat PAECs at 24 hours (butnot at the earlier time point of 16 h;Figure 2D), suggesting that the hypoxia-induced increase in ERb is mediated by atranscriptional mechanism. This increasewas specific to ERb, as similar increases inERa mRNA expression were not observed(Figure 2D).
To corroborate these findings, wecultured human primary PAECs underhypoxic conditions for 24 or 72 hours, and
30100
80
60
40
20
0
2.5
A
B C D
2.0
1.5
1.0
0.5
0.0
25
20
152
1
0
*
**
**
Rel
ativ
e E
R m
RN
A e
xpre
ssio
n (C
t)(F
old
chan
ge v
s. N
orm
oxia
)
Per
cent
of C
ells
with
ER
Co-
locl
aliz
ed w
ith D
AP
I
MP
I per
cel
l(F
old
chan
ge v
s. N
orm
oxia
)
Mer
geD
AP
I
Hypoxia
Normoxia 16 hrs 24 hrs
Hypoxia
Normoxia 24 hrs 72 hrs
Hypoxia
Normoxia 24 hrs 72 hrs
Normoxia Hypoxia24 hrs Hypoxia72 hrs Hypoxia24 hrs Hypoxia72 hrsER
ERER
ERER
ERER
NormoxiaER
Figure 2. Hypoxia increases expression of ERb, but not ERa, in cultured rat pulmonary artery endothelial cells (PAECs). (A) Representativeimmunocytochemistry images of PAECs at 24 and 72 hours of hypoxia (1% O2) versus normoxia. ERa (left three columns) and ERb (right threecolumns) are in green. Note the significant increase in ERb staining intensity in hypoxic cells, with a pattern of ERb staining suggestive of increasednuclear translocation (arrows). (B) Time course of hypoxia-induced expression of ERa (black bars) and ERb (gray bars) by immunocytochemistry.ERb expression was quantified by normalizing the megapixel intensity (MPI) by the number of cells (nuclei stained with DAPI) with ImageJ, and isexpressed as the fold change of MPI at 4, 24, and 72 hours versus MPI at corresponding normoxia time points. (C) ER nuclear translocation wasquantified as percent ER stain colocalized with DAPI. (D) ERa and ERb gene expression in rat PAECs measured by real-time qRT-PCR. Scale bars =10 mm. Data are from three independent experiments and are presented as means 6 SEM. *P , 0.05 versus normoxia control by one-way ANOVAwith post hoc Tukey’s test.
ORIGINAL RESEARCH
Frump, Selej, Wood, et al.: Hypoxia and Estrogen Receptor b 117

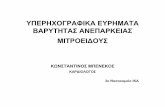
evaluated ERa and ERb expression byimmunocytochemistry and Western blot.As in the rat PAECs, hypoxia selectivelyand time dependently increased ERb(but not ERa) expression, with a trendtoward an increase at 24 hours and asignificant 25% increase at 72 hours(Figures 3A and 3B). As in the rat PAECs,immunocytochemistry studies suggestedthat the hypoxia-induced increase in ERbabundance was paralleled by a changein ERb’s cellular localization patternconsistent with translocation to the nucleus(Figures 3A and 3C). In fact, 80% of theERb-positive cells colocalized with DAPIat 24 hours, and this was maintained even
at 72 hours. Finally, we quantified thechanges in ERb expression using real-timeRT-PCR. Similar to what was observed withrat PAECs, ERb, but not ERa, mRNAwas significantly increased at 24 hours(but not at the earlier time point of 4 h;Figure 3D), suggesting that the hypoxia-induced increase in ERb is transcriptionallyregulated. Interestingly, we also observedhypoxic induction of ERb, but not ERa,protein in human pulmonarymicrovascular endothelial cells (PMVECs;Figure E4) and pulmonary smoothmuscle cells (data not shown) at 72 hours,indicating that the specific hypoxicregulation of ERb is relevant to multiple
cell types/phenotypes in the pulmonaryvasculature. Taken together, these dataindicate that hypoxia 1) selectively increasesERb mRNA and protein in culturedprimary PAECs, and 2) results in nucleartranslocation of ERb, suggesting that thisreceptor has biologically relevant effects inthe context of hypoxia.
Normoxic HIF-a Stabilization IsSufficient to Increase ERb in RatPAECsWe next sought to determine whether thehypoxia-induced increase in rat PAEC ERbexpression is driven by HIF-1a, a masterregulator of hypoxia-driven responses (35).
20100
80
60
40
20
0
B C D
1.5
1.0
0.5
0.0
15
10
5
0
****
*
Rel
ativ
e E
R
mR
NA
exp
ress
ion(
Ct)
(Fol
d ch
ange
vs.
Nor
mox
ia)
Per
cent
of C
ells
with
ER
Co-
locl
aliz
ed w
ith D
AP
I
MP
I per
cel
l(F
old
chan
ge v
s. N
orm
oxia
)
Hypoxia
Normoxia 16 hrs4 hrs 24 hrs
Hypoxia
Normoxia 24 hrs 72 hrs
Hypoxia
Normoxia 24 hrs 72 hrs
ERER
ERER
ERER
A
Mer
geD
AP
I
Normoxia Hypoxia24 hrs Hypoxia72 hrs Hypoxia24 hrs Hypoxia72 hrsER
NormoxiaER
Figure 3. Hypoxia increases expression of ERb, but not ERa, in primary human PAECs. (A) Representative immunocytochemistry images of humanPAECs at 24 and 72 hours of hypoxia (1% O2) versus normoxia. ERa (left three columns) or ERb (right three columns) are in green. Note a pattern of ERbstaining suggestive of increased nuclear translocation (arrows). (B) Time course of hypoxia-induced expression of ERa (black bars) and ERb (gray bars).ER expression was quantified by normalizing the MPI by the number of cells (nuclei stained with DAPI) with ImageJ, and is expressed as the fold change ofMPI at 4, 24, and 72 hours versus MPI at corresponding normoxia time points. (C) ER nuclear translocation was quantified as percent ER stain colocalizedwith DAPI. (D) ERa and ERb gene expression in rat PAECs measured by real-time qRT-PCR. Scale bars = 10 mm. Data are from three independentexperiments and are presented as means 6 SEM. *P , 0.05 versus normoxia control by one-way ANOVA with post hoc Tukey’s test.
ORIGINAL RESEARCH
118 American Journal of Respiratory Cell and Molecular Biology Volume 59 Number 1 | July 2018

We treated rat PAECs with the iron chelatorDFO, which leads to normoxic HIF-astabilization (Figures 4A and 4B). Indeed,DFO treatment (10 mM for 24 h) resulted ina robust 25% increase in ERb (Figures 4Aand 4D). DFO leads to stabilization ofHIF-2a and, similar to the case with HIF-1a,we detected the stabilization of HIF-2a inrat PAECs after DFO treatment (Figures 4Aand 4C), indicating that normoxic HIF-astabilization is sufficient to increase ERbexpression.
HIF-1a Is Necessary for the Hypoxia-induced Increase in ERb Expressionin Rat PAECsTo examine whether HIF-1a is necessaryfor the hypoxia-induced increase in ERb,we used siRNA directed against HIF-1a inrat PAECs grown under hypoxic conditions(Figures 5A and 5B). As expected, knockdownof HIF-1a attenuated the hypoxia-inducedincrease in ERb at 24 and 48 hours ofhypoxia (Figures 5A and 5C), suggestingthat HIF-1a indeed is necessary for hypoxiato increase ERb.
ERb Decreases HIF-2a and IncreasesPHD2 in Rat PAECsTo determine whether ERb in turn affectsHIF-1a expression during hypoxia, we used
siRNA directed against ERb. Interestingly,knockdown of ERb during hypoxia resultedin decreased expression of HIF-1a at 24 (butnot 48) hours of hypoxia exposure (Figures5A and 5B), suggesting that HIF-1a istime dependently under the control of ERb.We next assessed whether the HIF-a familymember HIF-2a is regulated by ERb.Although HIF-2a was decreased after24 hours of ERb knockdown, we noted asignificant 30% increase in HIF-2a protein48 hours after ERb knockdown (Figures 5Aand 5D), suggesting that ERb regulates andtime dependently decreases HIF-2a. BecausePHD2 is a major inhibitor of HIF-a (bymediating HIF-a degradation) (36), we nextsought to identify whether ERb also affectsPHD2 expression. Indeed, knockdown ofERb during hypoxia resulted in 50%decreased expression of PHD2 at both24 and 48 hours (Figures 5A and 5E),indicating that ERb regulates PHD2expression. We corroborated these findingsby treating hypoxic rat PAECs for 48 hourswith the ERb-selective agonist DPN(Figure 6). We noted a dose-dependentincrease in PHD2 expression in cells treatedwith 100 nM of DPN (Figures 6A and 6B),indicating that, indeed, ERb increases PHD2expression in rat PAECs. We also observeddose-dependent decreases in HIF-1a
(Figures 6A and 6C) and HIF-2a (Figures6A and 6D) expression in cells treated withDPN. Given the potential inactivation ofPHD2 in severe hypoxic conditions (37), wealso tested the effect of DPN on PHD2,HIF-1a, and HIF-2a expression under lesssevere hypoxic conditions (5% O2; Figure E5).Similar to our observations at 1% O2, weobserved a dose-dependent increase inPHD2 expression (Figures E5A and E5B), adecrease in HIF-2a expression (Figures E5Aand E5D), and a trend toward decreasedHIF-1a expression (Figures E5A and E5C).In summary, these data suggest that inhypoxic rat PAECs, HIF-1a increases ERb,and that ERb in turn decreases HIF-2aand increases its inhibitor, PHD2. The datafor DPN, but not those for siERb, suggestthat ERb may also decrease HIF-1a. Thisdiscrepancy may be due to a compensatoryupregulation of ERa or other factors afterERb knockdown, or it may indicate a time-dependent differential effect of ERb onHIF-1a expression.
ERb Is Necessary for E2 to AttenuateHypoxia-induced Pulmonary VascularRemodeling and Decrease LungHIF-1a and HIF-2a ExpressionTo corroborate our findings in vivo, wetreated Esr12/2 or Esr22/2 mice (mice
Veh
ER
/ Vin
culin
(Fol
d ch
ange
vs
Veh
icle
)
10 M
*
100 M
DFO
2.0
1.5
1.0
0.5
0.0Veh
HIF
-2
/ V
incu
lin(F
old
chan
ge v
s V
ehic
le)
*
10 M 100 M
DFO
1.5
1.0
0.5
0.0
Veh 10 M 100 M
DFOA
B C D
— 120 kD
— 118 kD
— 56 kD
— 120 kD
HIF-1
HIF-2
ER
Vinculin
Veh
HIF
-1
/ V
incu
lin(F
old
chan
ge v
s V
ehic
le)
*
10 M 100 M
DFO
1.5
1.0
0.5
0.0
Figure 4. Hypoxia-inducible factor 1a (HIF-1a) stabilization under normoxic conditions increases ERb expression in cultured rat PAECs. Effects oftreatment with deferoxamine (DFO; 10 or 100 mM for 24 h) or vehicle (veh; H2O) on HIF-1a (A and B), HIF-2a (A and C), and ERb (A and D) expression areshown in representative Western blots (A) and densitometry (B–D) from three independent experiments. Data are means6 SEM. *P, 0.05 versus vehiclecontrol using one-way ANOVA with post hoc Tukey’s test.
ORIGINAL RESEARCH
Frump, Selej, Wood, et al.: Hypoxia and Estrogen Receptor b 119

containing germline null mutationsfor ERa or ERb, respectively) and WTmice with E2 (75 mg/kg/day [10]),and exposed them to 3 weeks of hypoxia
(Patm = 362 mm Hg). An additional groupof untreated WT mice were placed inhypoxia to serve as controls. As previouslynoted in chronically hypoxic rats, compared
with hypoxic WT controls, E2 treatment inWT mice significantly decreased hypoxia-induced pulmonary vascular remodeling by40% (Figures 7A and 7B). Importantly, this
*
^
^ ^
^ ^
^^
^ ^ ^
^
^
^
^
1.5
HIF
-1
/ V
incu
lin(F
old
chan
ge v
s N
orm
oxia
)
Nor
mox
ia
Scr
Scr
siH
IF-1
siH
IF-1
siE
R
siE
R
Nor
mox
ia
Scr
Con
trol
Scr
Con
trol
siH
IF-1
siH
IF-1
siE
R
siE
R
1.0
0.5
0.0
* *
24 hrs Hypoxia 48 hrs Hypoxia
24 hours Hypoxia 48 hours Hypoxia
*
2.0E
R
/ Vin
culin
(Fol
d ch
ange
vs
Nor
mox
ia)
Nor
mox
ia
Scr
Scr
siH
IF-1
siH
IF-1
siE
R
siE
R
1.0
1.5
0.5
0.0
*
* *
24 hrs Hypoxia 48 hrs Hypoxia
3
HIF
-2
/ V
incu
lin(F
old
chan
ge v
s N
orm
oxia
)
Nor
mox
ia
Scr
Scr
*
siH
IF-1
siE
R
2
1
0
3
PH
D2
/ Vin
culin
(Fol
d ch
ange
vs
Nor
mox
ia)
2
1
0
siE
R
*
siH
IF-1
*
*
24 hrs Hypoxia 48 hrs Hypoxia
Nor
mox
ia
Scr
Scr
*
siH
IF-1
siE
R
*
siH
IF-1
*
siE
R
*
24 hrs Hypoxia 48 hrs Hypoxia
HIF-1
A
B C
D E
HIF-2
PHD2
ER
Vinculin
— 120 kD
— 118 kD
— 56 kD
— 120 kD
— 46 kD
Figure 5. HIF-1a and ERb regulate HIF-2a and prolyl hydroxylase 2 (PHD2) expression in hypoxic rat PAECs. (A) Western blot and (B–E) densitometry of HIF-1a(B), ERb (C), HIF-2a (D), and PHD2 (E) protein expression after knockdown of HIF-1a or ERb by siRNA. Scrambled control oligos were used as negative control.Cells were grown for 24 or 48 hours under hypoxic conditions (1% O2). Data represent three independent experiments and are expressed as means 6 SEM.*P , 0.05 versus scrambled control; ^P , 0.05 versus normoxic control using one-way ANOVA with post hoc Tukey’s test. Scr = scrambled.
ORIGINAL RESEARCH
120 American Journal of Respiratory Cell and Molecular Biology Volume 59 Number 1 | July 2018

reduction in pulmonary vascularremodeling was observed in E2-treatedEsr12/2, but not Esr22/2, mice (Figures 7Aand 7B), suggesting that ERb is requiredfor E2 to attenuate hypoxia-inducedpulmonary vascular remodeling. Contraryto our hypothesis, PHD2 was not affectedby E2 or loss of ERa or ERb (Figures 7Cand 7D), suggesting that PHD2 is not solelyregulated by E2-ER signaling. Alternatively,it is possible that E2-ER–mediated changesin PHD2 expression in PAECs in vivo werenot captured at the time point investigated,or were masked by surrounding tissue inwhole-lung homogenates. On the otherhand, E2 treatment in hypoxic WT micetended to decrease lung HIF-1a and HIF-2a expression (Figures 7C, 7E, and 7F),and in the case of HIF-1a, resulted in asignificant 50% decrease in E2-treatedEsr12/2 mice (where E2 signaling occursthrough ERb; Figures 7C and 7E).However, E2 did not lower HIF-1aabundance in Esr22/2 mice (where E2signaling occurs through ERa; Figures 7Cand 7E). In parallel, E2 treatment led toincreased HIF-2a expression in Esr22/2
mice (Figures 7C and 7F). This suggeststhat ERb is required for E2 to decreaseHIF-2a and HIF-1a expression. However,
in the latter case, this effect can only occur inthe absence of ERa, indicating that 1) ERahas effects opposite to those of ERb andactually increases HIF-1a, and 2) ERa andERb compete with each other for E2 binding.Taken together, these studies demonstratethat ERb is required for E2 to attenuatehypoxia-induced pulmonary vascularremodeling, is necessary for E2 to decreaselung HIF-a expression, and preventsincreases in lung HIF-2a expression.
Discussion
Our studies reveal that ERb, but not ERa, isupregulated in hypoxic rat lung, culturedhypoxic rat and human conduit PAECs,and PMVECs. We show for the first timethat HIF-a chemical stabilization with DFOis sufficient to induce ERb expression andthat knockdown of HIF-1a by siRNAreduces ERb expression in hypoxic PAECs,identifying that the hypoxia-inducedincrease in ERb expression occurs via aHIF-a–dependent mechanism. Additionally,we provide novel evidence suggestingthat HIF-2a is downregulated and PHD2is upregulated by ERb in vitro. siRNAdirected against ERb leads to the robust
upregulation of HIF-2a and downregulationof PHD2 in hypoxic PAECs, and treatmentwith the ERb agonist DPN upregulatesPHD2 expression and decreases HIF-1a andHIF-2a in a dose-dependent manner. Lastly,we demonstrate that ERb is necessary for E2to attenuate hypoxia-induced pulmonaryvascular remodeling, decrease lung HIF-1a,and prevent increases in HIF-2a expression.However, the decrease in HIF-1a in vivoonly occurred in the absence of ERa. Takentogether, these novel data implicate ERbas a mediator of protective E2 signaling inthe hypoxic pulmonary vasculature. Aschematic of the putative interaction amonghypoxia, ERb, HIF-1a, HIF-2a, and PHD2in the pulmonary vasculature is providedin Figure E6.
HPH is prevalent globally; it affectsmillions of people living at high altitude andmillions of patients afflicted with a widespectrum of chronic lung disease andsleep-disordered breathing (5). HPH ischaracterized by significant pulmonaryvascular remodeling that may culminate inright ventricular failure and death (4, 38).Although it occurs much more frequentlythan PAH (39), no specific treatment forHPH exists. In fact, therapeutics used forPAH frequently worsen oxygenation in
0.0Veh 1 nM 1 M10 nM
DPN
*
100 nM
0.5
1.0
1.5
2.0
PH
D2
/ Vin
culin
(Fol
d ch
ange
vs
Veh
icle
Con
trol
)
0.0Veh 1 nM 1 M10 nM
DPN
* *
100 nM
0.5
1.0
1.5H
IF-1
/ V
incu
lin(F
old
chan
ge v
s V
ehic
le C
ontr
ol)
DPN
Veh 1 nM 1 M10 nM 100 nM
0.0Veh 1 nM 1 M10 nM
DPN
*
100 nM
0.5
1.0
1.5
HIF
-2
/ V
incu
lin(F
old
chan
ge v
s V
ehic
le C
ontr
ol)
— 120 kD
— 118 kD
— 120 kD
— 46 kD
HIF-1
HIF-2
Vinculin
PHD2
A
B C D
Figure 6. Selective ERb agonism with diarylpropionitrile (DPN) dose dependently increases PHD2 and decreases HIF-1a and HIF-2a in cultured ratPAECs. (A) Representative Western blots showing the effects of DPN (1, 10, or 100 nM, or 1 mM) or vehicle (DMSO) on PHD2 protein expressionduring hypoxia (1% O2; 48 h). (B–D) The protein expression of PHD2 (B), HIF-1a (C), and HIF-2a (D) was quantified with densitometry. Data represent themean 6 SEM from three independent experiments. *P , 0.05 versus vehicle control using one-way ANOVA with post hoc Dunnett’s test.
ORIGINAL RESEARCH
Frump, Selej, Wood, et al.: Hypoxia and Estrogen Receptor b 121

HPH (40–42), indicating a need for noveltherapeutic approaches to HPH. Severalclinical and preclinical studies haveidentified that female sex confers aprotective phenotype during acute or
chronic hypoxia exposure (reviewed inReference 7). For example, in multiplespecies, females exhibit less hypoxicpulmonary vasoconstriction and areprotected from HPH. These effects have
been linked to vasodilator andantiproliferative effects of E2 (7). Forexample, pregnancy attenuates hypoxicpulmonary vasoconstriction, ovariectomyworsens HPH, and E2 repletion attenuates
0.5
0.4
0.3
0.2
0.1PH
D2
/ Vin
culin
0.0WT WT
+ E2Esr1-/-
+ E2Esr2-/-
+ E2
80
70
60
50
% V
esse
l Wal
l Are
a
40WT WT
+ E2Esr1-/-
+ E2Esr2-/-
+ E2
0.6
0.4
0.2
HIF
-1
/ V
incu
lin
0.0WT
*
* * #
WT+ E2
Esr1-/-
+ E2Esr2-/-
+ E2
1.5
1.0
0.5
HIF
-2
/ V
incu
lin
0.0WT
*#
WT+ E2
Esr1-/-
+ E2Esr2-/-
+ E2
HIF-1
HIF-2
Vinculin
PHD2
— 120 kD
— 118 kD
— 120 kD
— 46 kD
+ E2
Hypoxia WT
Hypoxia WT Hypoxia WT + E2 Hypoxia Esr1-/- + E2 Hypoxia Esr2-/- + E2
Hypoxia WT Hypoxia Esr1-/- Hypoxia Esr2-/-
A
B
C
D E F^
Figure 7. ERb is necessary for E2-mediated attenuation of hypoxic pulmonary vascular remodeling and HIF-1a and HIF-2a expression in mice. (A) Representativeimmunohistochemical images of lung sections stained for smooth muscle actin from untreated wild-type (WT) (solid circles), E2-treated WT (solid squares),E2-treated Esr12/2 (solid triangles), and E2-treated Esr22/2 (solid inverted triangles) mice exposed to chronic hypobaric hypoxia (Patm = 362 mmHg; equivalent to10% FIO2
; 3 wk). Note the decrease in vascular wall thickness (arrowheads) in E2-treated WT and Esr12/2 mice, but not in E2-treated Esr22/2 mice compared toWT controls. Scale bars = 50 mm. (B) Quantification of the wall thickness of small- and medium-sized pulmonary arteries (less than 200 mM). (C) PHD2, HIF-2a,and HIF-1a protein expression in mouse lung homogenates from WT, E2-treated WT, E2-treated Esr12/2, and E2-treated Esr22/2 mice exposed to chronichypobaric hypoxia. (D–F) Expression levels of lung PHD2, HIF-2a, and HIF-1a quantified by densitometry; n = 4–5 per group. Scatterplots include means6 SEM.*P , 0.05 versus WT; #P , 0.05 versus WT 1 E2; ^P , 0.05 versus Esr12/2 (one-way ANOVA with post hoc Tukey’s test). E2 = 17b-estradiol.
ORIGINAL RESEARCH
122 American Journal of Respiratory Cell and Molecular Biology Volume 59 Number 1 | July 2018

HPH (reviewed in References 7 and 43).A better understanding of the effects of E2and its receptors in the hypoxic pulmonaryvasculature could provide the rationaleand basis for future studies focused ondeveloping novel therapeutic strategies forHPH.
We previously demonstrated thatE2 attenuates HPH via an ER-dependentmechanism (10), and recently expandedupon that finding by discovering an ER-dependent genome in lungs from HPH rats(16). Of note, our previous data showedthat E2 exerts specific antiproliferativeeffects during hypoxia that are not evidentduring normoxia (10). For example, E2-ERdependently decreased bromodeoxyuridineuptake and vascular endothelial growthfactor secretion in hypoxic rat PAECs, butnot in PAECs grown in room air. Ourcurrent data expand upon these findingsand suggest that hypoxia-enabled increasesin ERb expression may allow for E2 to exertits hypoxia-specific effects. Such a findingmay explain why E2 has consistently beenshown to be protective in hypoxia modelsof PH, whereas its effects in other types ofPH have been less consistent (reviewed inReference 7).
If ERb signaling can be protective inthe pulmonary vasculature, this raises thepossibility that alterations in ERb signalingmay contribute to the female predominancenoted in PAH. Of note, SNPs in ESR22/2
have been associated with LV structuraldifferences in women with hypertension(44) and with increased arterial stiffness inFramingham Offspring Study participants(45). This suggests that genetic alterationsin ESR22/2 could also contribute toabnormalities in the pulmonary vasculature.Alternatively, in the absence of hypoxia-enabled increases in ERb expression, E2’sprotective signaling pathways may not beengaged, allowing for the development ofpulmonary vascular disease, especially in thecontext of otherwise predisposing conditionsfor PAH development (e.g., geneticabnormalities and environmental exposures).
To the best of our knowledge, ourstudies are the first to implicate HIF-1aas a regulator of ERb in PAECs. Giventhat HIF-1a is a key regulator of hypoxia-mediated effects, this finding is not entirelysurprising. Our findings are consistent withresults from studies in HEK293 cells, whichdemonstrated that HIF-1a transcriptionallyactivates ERb expression in the absence ofE2, and the addition of E2 did not further
enhance the upregulation of ERb (46).Subsequent studies in other cell types havelinked HIF-1a to the induction of ERbindependently of E2 (47–49). For instance,in human ER-positive breast cancer cells,hypoxia stimulated ERb expression andreduced ERa expression (48), whereas inhuman stromal cells isolated from patientswith endometriosis, hypoxia stronglyinduced ERb (47), both in the absenceof E2. Additionally, steroid receptorcoactivator-1 and CREB-binding proteincomprise part of the HIF-1a transcriptionalcoactivator complex and can promote ERbtranscription in the absence of E2 (49).Building on these observations, weperformed PROMO and TRANSFACin silico promoter analyses, which identifiedtwo putative HIF-1a binding sites in theESR2 promoter (Ensembl ENSG00000140009)to be validated in future studies.Interestingly, we did not observe asignificant increase in ERb mRNAexpression until 16 hours (human PAECs)or 24 hours (rat PAECs) after hypoxia. Oneexplanation for this slow upregulation isthat because ERb expression is regulated bymultiple coactivators and corepressors,there may be a transcriptional repressorcomplex at the ERb promoter upon thefirst, acute induction of HIF-1a due tohypoxia that is not present at a later,chronic hypoxia time point. Finally, wecannot completely rule out that the traceamounts of E2 detected in rat PAEC media(Fig. E1; likely arising as a result ofendogenous PAEC E2 synthesis viaaromatase [50]) activated ERb. However,this seems unlikely, as no E2 was detectedin human PAEC media, yet hypoxiaincreased ERb expression and induced itstranslocation in this cell type as well.Together, these data suggest that ERb,independently of the presence of E2, isencoded by a hypoxia-responsive gene.
The finding that ERb in turn regulatesHIF-1a and HIF-2a in vitro andin vivo reveals a novel and potentiallytherapeutically targetable mechanism ofaction in the hypoxic pulmonaryvasculature that may explain in part why E2attenuates HPH and why females areprotected against the development of HPH.This putative negative-feedback loop ofERb on HIF-a likely occurs via directbinding of HIF-1a to ERb, followed by thenuclear translocation of ERb and bindingto estrogen response elements of targetgenes. Interestingly, at least one study has
shown that the ERb protein is able to binddirectly to HIF-1a (46). Alternatively,hypoxia could indirectly facilitate ERbnuclear translocation via direct activation ofERb by a HIF-1a–induced growth factor,e.g., epidermal growth factor (51). Thenegative-feedback mechanism we identifiedis consistent with data from the oncologyliterature, which demonstrates that ERbinhibits HIF-1a transcriptional activity andpromotes its proteasome degradation inprostate cancer cells (52). On the otherhand, to the best of our knowledge, we arenot aware of any prior data demonstratingthat ERb decreases HIF-2a. This is ofparticular importance because dysregulatedHIF-2a signaling has been linked to theformation of obliterative pulmonaryvascular lesions in PH (32). However, theeffects of ERb on HIF-1a and HIF-2awere not clear-cut. At 24 hours of ERbknockdown, both HIF-1a and HIF-2a weredecreased rather than increased, suggestinga time dependence of ERb effects on thesetranscription factors. In addition, ERbknockdown did not lead to increased HIF-1a at the 48-hour time point. Thisphenomenon may be explained by competingeffects of ERa and ERb on HIF expression:ERa (or another, as yet unidentified factor)may compensate for the loss of ERb andrepress HIF-a. On the other hand, thefinding that selective ERb activationdecreased both HIF-1a and HIF-2a clearlyindicates that ERb exerts inhibitory effectson these mediators.
The in vivo effects of E2 and ERb onHIF-a were complex. E2 did notstatistically significantly decrease HIF-1a inhypoxic WT rats (even though there was atrend), and a significant decrease occurredonly in E2-treated Esr12/2 mice. Althoughthis could be the result of a type II error, itmay also suggest that ERa increasesHIF-1a. Specifically, ERa and ERb mayhave opposing effects on HIF-1a in vivo,allowing ERb to decrease HIF-1a onlyin the absence of ERa. Such a paradigmwould be consistent with the knownproproliferative effects of ERa in prostatecancer (28) and in PA smooth muscle cells(53). An alternative hypothesis is that theabsence of ERa increases the abundance ofE2 at ERb, thus driving a more prominentERb signal. This would suggest that ERaand ERb compete with each other forbinding to E2. Such a scenario is likely,given that in the absence of ERb there is noincrease in HIF-1a (Figures 7C and 7F).
ORIGINAL RESEARCH
Frump, Selej, Wood, et al.: Hypoxia and Estrogen Receptor b 123

Similarly, E2 did not statisticallysignificantly decrease HIF-2a in vivo, yet,again, there was a trend. In contrast toHIF-1a, HIF-2a markedly increased inE2-treated Esr22/2 mice. This indicatesthat ERb exerts inhibitory effects onHIF-2a and suggests that ERa and ERbmay have opposing effects on HIF-2ain vivo, with ERa exerting stimulatoryeffects and ERb preventing this increase.
Our data suggest that the inhibitoryeffect of ERb on HIF-1a and HIF-2amay be mediated by PHD2. PHDshydroxylate HIF-1a and HIF-2a, leading tovon Hippel–Lindau protein-dependentubiquitination and rapid proteasomaldegradation (35). Three main isoformsexist, with PHD2 being the most prominentisoform (36). Interestingly, we found thatERb induces PHD2 in hypoxic PAECs.This may, in turn, downregulate HIF-1aand HIF-2a. This finding is supportedby recently published data from prostateepithelial cells demonstrating that ERbpromotes HIF-1a degradation byincreasing PHD2 transcription and byidentifying an estrogen response element inthe PHD2 promoter (52). Given the recentreport that PHD2 expressed in PAECsprotects against PAH development (32),our identification of PHD2 as a target ofERb is of particular interest, as it suggests anovel mechanism whereby E2 attenuatesHPH development.
ERb may also inhibit HIF-1a andHIF-2a through PHD2-independentmechanisms. For example, ERb was shownto inhibit HIF-1a transcriptional activity viadownregulation of ARNT (HIF-1b) (54). Inanother study, ERb was shown to destabilizeHIF-1a protein via proteasomal degradation(55). It is possible that similar mechanismsregulate ERb’s effects on HIF-1a in thehypoxic pulmonary vasculature. Futurestudies will focus on identifying the exactmolecular mechanisms of ERb-mediatedattenuation of HIF-1a and HIF-2a in thehypoxic lung and in hypoxic PAECs.
Our study has several limitations.First, although our in vitro data robustlyidentify PHD2 as a target of ERb, we didnot detect any changes in PHD2 expressionin Esr12/2 or Esr22/2 mice treated withE2. Although it is possible that PHD2 isnot regulated by E2-ERb signaling in vivo,we consider it more likely that E2-ERb–mediated changes in PHD2 expression inPAECs in vivo were not captured at thetime point investigated, or were maskedby surrounding tissue in whole-lunghomogenates. This is supported by theobservation that the effects we noted onHIF-1a and HIF-2a were robust in vitro aswell as in vivo. Second, our in vitro studiesused a severe level of hypoxia (1% O2). Thissevere level of hypoxia can inhibit PHD2activity at least acutely (at 4 h), but perhapsnot chronically (36, 37, 56), which couldbe a source of variability in our data;however, we were able to corroborate ourDPN findings using less severe hypoxicconditions (5% O2), during which PHD2should be active (Figure E3). Second, in ourstudies we used in vitro rat and humanprimary cells, and conducted in vivo studiesin rats and mice; however, it should benoted we did not use human cells for allstudies. Future investigations will focus onexpanding upon these mechanisms inhuman PAECs and PMVECS, and inpatients with HPH under less severehypoxic conditions. Third, although weconfirmed that hypoxia upregulates ERb inseveral cell types and in two species, we didnot corroborate our mechanistic studies inhuman cells. We did, however, confirm therelevance of this signaling pathway in vivo,making the rat PAEC studies relevant.Mechanistic studies dissecting the interplayamong HIFs, PHD, and ERb in PAECsfrom healthy donors and patients with PHare currently ongoing in our laboratory.To eliminate potentially confoundingeffects of estrogens or the estrous cycle onER expression, we performed the currentstudy in male animals, and therefore do
not provide information on ER expressionin hypoxic females. Similarly, ourcommercially obtained human PAECs andPMVECs were derived from male donors.Studies in females are currently underway,and a sex-specific comparison of ERexpression will be the focus of futureinvestigations. Lastly, our studies focusedon hypoxia-induced changes in thepulmonary vasculature and are thereforerelevant for HPH and WHO group 3 PH,but cannot necessarily be extrapolated toPAH. Given that HIF-1a, HIF-2a, andfemale sex play major roles in PAHdevelopment, the cross-talk among HIF-1a,HIF-2a, E2, and ERb in this disease needsto be explored further. The protective ERbsignaling noted in hypoxia may be lost oraltered in PAH.
In summary, we provide the firstevidence of a novel HIF-1a–dependenthypoxia pathway that induces ERb, but notERa, in PAECs and PMVECs. We show thatthe hypoxia-induced upregulation of ERbis specific to the lung and pulmonaryvasculature, as evidenced by the decreasein ERb expression in the hypoxic RV andliver. We demonstrate that ERb inducesexpression of the HIF-a inhibitor PHD2 anddecreases HIF-1a and HIF-2a expressionin vitro. In vivo, ERb prevents increases inHIF-2a and is necessary for E2 to decreaselung HIF-1a and hypoxia-induced pulmonaryvascular remodeling. Harnessing thesepathways may facilitate the development ofspecific therapeutic strategies for patientswith HPH and WHO group 3 PH, forwhom there are no pharmacologicaltreatment options, and help unravel the“estrogen paradox” in PAH. n
Author disclosures are available with the textof this article at www.atsjournals.org.
Acknowledgment: The authors thank Dr.Robert G. Presson, Jr., for equipment support,Ms. Crystal Sorg and Mr. John Fierst for technicalassistance, and Drs. Angelia Lockett and KellySchweitzer for technical advice.
References
1. Rabinovitch M. Molecular pathogenesis of pulmonary arterialhypertension. J Clin Invest 2012;122:4306–4313.
2. Tuder RM, Stacher E, Robinson J, Kumar R, Graham BB. Pathology ofpulmonary hypertension. Clin Chest Med 2013;34:639–650.
3. Tuder RM, Archer SL, Dorfmuller P, Erzurum SC, Guignabert C,Michelakis E, et al. Relevant issues in the pathology and pathobiologyof pulmonary hypertension. J Am Coll Cardiol 2013;62(25, Suppl):D4–D12.
4. Stenmark KR, Fagan KA, Frid MG. Hypoxia-induced pulmonary vascularremodeling: cellular and molecular mechanisms. Circ Res 2006;99:675–691.
5. Seeger W, Adir Y, Barbera JA, Champion H, Coghlan JG, Cottin V, et al.Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol2013;62(25, Suppl):D109–D116.
6. Bartsch P, Gibbs JSR. Effect of altitude on the heart and the lungs.Circulation 2007;116:2191–2202.
7. Lahm T, Tuder RM, Petrache I. Progress in solving the sex hormoneparadox in pulmonary hypertension. Am J Physiol Lung Cell MolPhysiol 2014;307:L7–L26.
ORIGINAL RESEARCH
124 American Journal of Respiratory Cell and Molecular Biology Volume 59 Number 1 | July 2018

8. Dempsie Y, Nilsen M, White K, Mair KM, Loughlin L, Ambartsumian N,et al. Development of pulmonary arterial hypertension in mice over-expressing S100A4/Mts1 is specific to females. Respir Res 2011;12:159.
9. Fessel JP, Chen X, Frump A, Gladson S, Blackwell T, Kang C, et al.Interaction between bone morphogenetic protein receptor type 2 andestrogenic compounds in pulmonary arterial hypertension. Pulm Circ2013;3:564–577.
10. Lahm T, Albrecht M, Fisher AJ, Selej M, Patel NG, Brown JA, et al. 17b-Estradiol attenuates hypoxic pulmonary hypertension via estrogenreceptor-mediated effects. Am J Respir Crit Care Med 2012;185:965–980.
11. Lahm T, Patel KM, Crisostomo PR, Markel TA, Wang M, Herring C,et al. Endogenous estrogen attenuates pulmonary artery vasoreactivityand acute hypoxic pulmonary vasoconstriction: the effects of sex andmenstrual cycle. Am J Physiol Endocrinol Metab 2007;293:E865–E871.
12. Ventetuolo CE, Ouyang P, Bluemke DA, Tandri H, Barr RG, Bagiella E,et al. Sex hormones are associated with right ventricular structureand function: the MESA-right ventricle study. Am J Respir Crit CareMed 2011;183:659–667.
13. Lahm T, Crisostomo PR, Markel TA, Wang M, Wang Y, Tan J, et al.Selective estrogen receptor-alpha and estrogen receptor-b agonistsrapidly decrease pulmonary artery vasoconstriction by a nitric oxide-dependent mechanism. Am J Physiol Regul Integr Comp Physiol2008;295:R1486–R1493.
14. Austin ED, Cogan JD, West JD, Hedges LK, Hamid R, Dawson EP,et al. Alterations in oestrogen metabolism: implications for higherpenetrance of familial pulmonary arterial hypertension in females. EurRespir J 2009;34:1093–1099.
15. White K, Johansen AK, Nilsen M, Ciuclan L, Wallace E, Paton L, et al.Activity of the estrogen-metabolizing enzyme cytochrome P450 1B1influences the development of pulmonary arterial hypertension.Circulation 2012;126:1087–1098.
16. Frump AL, Albrecht ME, McClintick JN, Lahm T. Estrogen receptor-dependent attenuation of hypoxia-induced changes in the lunggenome of pulmonary hypertension rats. Pulm Circ 2017;7:232–243.
17. Mangelsdorf DJ, Thummel C, Beato M, Herrlich P, Schutz G, Umesono K,et al. The nuclear receptor superfamily: the second decade. Cell 1995;83:835–839.
18. Beato M, Herrlich P, Schutz G. Steroid hormone receptors: manyactors in search of a plot. Cell 1995;83:851–857.
19. Mollerup S, Jørgensen K, Berge G, Haugen A. Expression of estrogenreceptors a and b in human lung tissue and cell lines. Lung Cancer2002;37:153–159.
20. Fasco MJ, Hurteau GJ, Spivack SD. Gender-dependent expression ofa and b estrogen receptors in human nontumor and tumor lungtissue. Mol Cell Endocrinol 2002;188:125–140.
21. Krege JH, Hodgin JB, Couse JF, Enmark E, Warner M, Mahler JF, et al.Generation and reproductive phenotypes of mice lacking estrogenreceptor b. Proc Natl Acad Sci USA 1998;95:15677–15682.
22. Couse JF, Lindzey J, Grandien K, Gustafsson JA, Korach KS. Tissuedistribution and quantitative analysis of estrogen receptor-a (ERa)and estrogen receptor-b (ERb) messenger ribonucleic acid in thewild-type and ERa-knockout mouse. Endocrinology 1997;138:4613–4621.
23. Gustafsson JA. Estrogen receptor b—a new dimension in estrogenmechanism of action. J Endocrinol 1999;163:379–383.
24. Katzenellenbogen BS, Katzenellenbogen JA. Estrogen receptortranscription and transactivation: Estrogen receptor a and estrogenreceptor b: regulation by selective estrogen receptor modulatorsand importance in breast cancer. Breast Cancer Res 2000;2:335–344.
25. Paruthiyil S, Parmar H, Kerekatte V, Cunha GR, Firestone GL, Leitman DC.Estrogen receptor beta inhibits human breast cancer cell proliferationand tumor formation by causing a G2 cell cycle arrest. Cancer Res2004;64:423–428.
26. Platet N, Cathiard AM, Gleizes M, Garcia M. Estrogens and theirreceptors in breast cancer progression: a dual role in cancerproliferation and invasion. Crit Rev Oncol Hematol 2004;51:55–67.
27. McPherson SJ, Hussain S, Balanathan P, Hedwards SL, Niranjan B,Grant M, et al. Estrogen receptor-b activated apoptosis in benignhyperplasia and cancer of the prostate is androgen independent andTNFa mediated. Proc Natl Acad Sci USA 2010;107:3123–3128.
28. Slusarz A, Jackson GA, Day JK, Shenouda NS, Bogener JL, Browning JD,et al. Aggressive prostate cancer is prevented in ERaKO mice andstimulated in ERbKO TRAMP mice. Endocrinology 2012;153:4160–4170.
29. Chambliss KL, Yuhanna IS, Anderson RG, Mendelsohn ME, Shaul PW.ERbeta has nongenomic action in caveolae. Mol Endocrinol 2002;16:938–946.
30. Sherman TS, Chambliss KL, Gibson LL, Pace MC, Mendelsohn ME,Pfister SL, et al. Estrogen acutely activates prostacyclin synthesis inovine fetal pulmonary artery endothelium. Am J Respir Cell Mol Biol2002;26:610–616.
31. Kapitsinou PP, Rajendran G, Astleford L, Michael M, Schonfeld MP,Fields T, et al. The endothelial prolyl-4-hydroxylase domain2/hypoxia-inducible factor 2 axis regulates pulmonary arterypressure in mice. Mol Cell Biol 2016;36:1584–1594.
32. Dai Z, Li M, Wharton J, Zhu MM, Zhao Y-Y. PHD2 deficiency inendothelial cells and hematopoietic cells induces obliterativevascular remodeling and severe pulmonary arterial hypertension inmice and humans through HIF-2a. Circulation 2016;133:2447–2458.
33. Selej MW, Wood J, Lockett AD, Albrecht M, Schweitzer K, Petrache I,et al. Hypoxia increases expression of estrogen receptor (ER)-bin vivo and in vitro. Am J Resp Crit Care Med 2013;187:A2257.
34. Selej MLA, Albrecht M, Petrache I, Lahm T. Hypoxia increases estrogenreceptor b expression in cultured rat pulmonary artery endothelialcells. Am J Respir Crit Care Med 2012;185:A4817.
35. Semenza GL. Oxygen sensing, homeostasis, and disease. N Engl JMed 2011;365:537–547.
36. Semenza GL. HIF-1, O(2), and the 3 PHDs: how animal cells signalhypoxia to the nucleus. Cell 2001;107:1–3.
37. Semenza GL. Regulation of oxygen homeostasis by hypoxia-induciblefactor 1. Physiology (Bethesda) 2009;24:97–106.
38. Pak O, Aldashev A, Welsh D, Peacock A. The effects of hypoxia on thecells of the pulmonary vasculature. Eur Respir J 2007;30:364–372.
39. Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M,Denton CP, et al. Updated clinical classification of pulmonaryhypertension. J Am Coll Cardiol 2009;54(1, Suppl):S43–S54.
40. Ghofrani HA, Wiedemann R, Rose F, Schermuly RT, Olschewski H,Weissmann N, et al. Sildenafil for treatment of lung fibrosis andpulmonary hypertension: a randomised controlled trial. Lancet 2002;360:895–900.
41. Stolz D, Rasch H, Linka A, Di Valentino M, Meyer A, Brutsche M, et al. Arandomised, controlled trial of bosentan in severe COPD. Eur RespirJ 2008;32:619–628.
42. Blanco I, Gimeno E, Munoz PA, Pizarro S, Gistau C, Rodriguez-RoisinR, et al. Hemodynamic and gas exchange effects of sildenafil inpatients with chronic obstructive pulmonary disease and pulmonaryhypertension. Am J Respir Crit Care Med 2010;181:270–278.
43. Austin ED, Lahm T, West J, Tofovic SP, Johansen AK, Maclean MR,et al. Gender, sex hormones and pulmonary hypertension. Pulm Circ2013;3:294–314.
44. Peter I, Shearman AM, Vasan RS, Zucker DR, Schmid CH, Demissie S,et al. Association of estrogen receptor beta gene polymorphismswith left ventricular mass and wall thickness in women. Am JHypertens 2005;18:1388–1395.
45. Peter I, Kelley-Hedgepeth A, Huggins GS, Housman DE, MendelsohnME, Vita JA, et al. Association between arterial stiffness andvariations in oestrogen-related genes. J Hum Hypertens 2009;23:636–644.
46. Lim W, Cho J, Kwon HY, Park Y, Rhyu M-R, Lee Y. Hypoxia-induciblefactor 1 a activates and is inhibited by unoccupied estrogen receptorb. FEBS Lett 2009;583:1314–1318.
47. Wu M-H, Lu C-W, Chang F-M, Tsai S-J. Estrogen receptor expressionaffected by hypoxia inducible factor-1a in stromal cells from patientswith endometriosis. Taiwan J Obstet Gynecol 2012;51:50–54.
48. Wolff M, Kosyna FK, Dunst J, Jelkmann W, Depping R. Impact ofhypoxia inducible factors on estrogen receptor expression in breastcancer cells. Arch Biochem Biophys 2017;613:23–30.
ORIGINAL RESEARCH
Frump, Selej, Wood, et al.: Hypoxia and Estrogen Receptor b 125

49. Tremblay A, Giguere V. Contribution of steroid receptor coactivator-1and CREB binding protein in ligand-independent activity of estrogenreceptor b. J Steroid Biochem Mol Biol 2001;77:19–27.
50. Mair KM, Wright AF, Duggan N, Rowlands DJ, Hussey MJ, Roberts S,et al. Sex-dependent influence of endogenous estrogen in pulmonaryhypertension. Am J Respir Crit Care Med 2014;190:456–467.
51. Curtis SW, Washburn T, Sewall C, DiAugustine R, Lindzey J, Couse JF,et al. Physiological coupling of growth factor and steroid receptorsignaling pathways: estrogen receptor knockout mice lack estrogen-like response to epidermal growth factor. Proc Natl Acad Sci USA1996;93:12626–12630.
52. Mak P, Chang C, Pursell B, Mercurio AM. Estrogen receptor b sustainsepithelial differentiation by regulating prolyl hydroxylase 2 transcription.Proc Natl Acad Sci USA 2013;110:4708–4713.
53. Wright AF, Ewart MA, Mair K, Nilsen M, Dempsie Y, Loughlin L, et al.Oestrogen receptor alpha in pulmonary hypertension. CardiovascRes 2015;106:206–216.
54. Lim W, Park Y, Cho J, Park C, Park J, Park YK, et al. Estrogen receptorbeta inhibits transcriptional activity of hypoxia inducible factor-1through the downregulation of arylhydrocarbon receptor nucleartranslocator. Breast Cancer Res 2011;13:R32.
55. Mak P, Leav I, Pursell B, Bae D, Yang X, Taglienti CA, et al. ERbimpedes prostate cancer EMT by destabilizing HIF-1a and inhibitingVEGF-mediated snail nuclear localization: implications for Gleasongrading. Cancer Cell 2010;17:319–332.
56. Ginouves A, Ilc K, Macıas N, Pouyssegur J, Berra E. PHDs overactivationduring chronic hypoxia “desensitizes” HIFaand protects cells fromnecrosis. Proc Natl Acad Sci USA 2008;105:4745–4750.
ORIGINAL RESEARCH
126 American Journal of Respiratory Cell and Molecular Biology Volume 59 Number 1 | July 2018