GRK2 blockade with βARKct is essential for cardiac β2-adrenergic receptor signaling towards...
10
RESEARCH Open Access GRK2 blockade with βARKct is essential for cardiac β 2 -adrenergic receptor signaling towards increased contractility Norma C Salazar 1 , Ximena Vallejos 1 , Ashley Siryk 1 , Giuseppe Rengo 2 , Alessandro Cannavo 2 , Daniela Liccardo 2 , Claudio De Lucia 2 , Erhe Gao 3 , Dario Leosco 2 , Walter J Koch 3 and Anastasios Lymperopoulos 1* Abstract Background: β 1 - and β 2 –adrenergic receptors (ARs) play distinct roles in the heart, e.g. β 1 AR is pro-contractile and pro-apoptotic but β 2 AR anti-apoptotic and only weakly pro-contractile. G protein coupled receptor kinase (GRK)-2 desensitizes and opposes βAR pro-contractile signaling by phosphorylating the receptor and inducing beta-arrestin (βarr) binding. We posited herein that GRK2 blockade might enhance the pro-contractile signaling of the β 2 AR subtype in the heart. We tested the effects of cardiac-targeted GRK2 inhibition in vivo exclusively on β 2 AR signaling under normal conditions and in heart failure (HF). Results: We crossed β 1 AR knockout (B1KO) mice with cardiac-specific transgenic mice expressing the βARKct, a known GRK2 inhibitor, and studied the offspring under normal conditions and in post-myocardial infarction (MI). βARKct expression in vivo proved essential for β 2 AR-dependent contractile function, as β 2 AR stimulation with isoproterenol fails to increase contractility in either healthy or post-MI B1KO mice and it only does so in the presence of βARKct. The main underlying mechanism for this is blockade of the interaction of phosphodiesterase (PDE) type 4D with the cardiac β 2 AR, which is normally mediated by the actions of GRK2 and βarrs on the receptor. The molecular “brake” that PDE4D poses on β 2 AR signaling to contractility stimulation is thus “released”. Regarding the other beneficial functions of cardiac β 2 AR, βARKct increased overall survival of the post-MI B1KO mice progressing to HF, via a decrease in cardiac apoptosis and an increase in wound healing-associated inflammation early (at 24 hrs) post-MI. However, these effects disappear by 4 weeks post-MI, and, in their place, upregulation of the other major GRK in the heart, GRK5, is observed. Conclusions: GRK2 inhibition in vivo with βARKct is absolutely essential for cardiac β 2 AR pro-contractile signaling and function. In addition, β 2 AR anti-apoptotic signaling in post-MI HF is augmented by βARKct, although this effect is short-lived. Keywords: Cardiac β 2 –adrenergic receptor, Pro-contractile signaling, Post-myocardial infarction survival, GRK2 inhibition, GRK5 * Correspondence: [email protected] 1 Department of Pharmaceutical Sciences, Laboratory for the Study of Neurohormonal Control of the Circulation, Nova Southeastern University College of Pharmacy, Fort Lauderdale, FL 33328, USA Full list of author information is available at the end of the article © 2013 Salazar et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Salazar et al. Cell Communication and Signaling 2013, 11:64 http://www.biosignaling.com/content/11/1/64
-
Upload
anastasios -
Category
Documents
-
view
213 -
download
1
Transcript of GRK2 blockade with βARKct is essential for cardiac β2-adrenergic receptor signaling towards...

RESEARCH Open Access
GRK2 blockade with βARKct is essential forcardiac β2-adrenergic receptor signaling towardsincreased contractilityNorma C Salazar1, Ximena Vallejos1, Ashley Siryk1, Giuseppe Rengo2, Alessandro Cannavo2, Daniela Liccardo2,Claudio De Lucia2, Erhe Gao3, Dario Leosco2, Walter J Koch3 and Anastasios Lymperopoulos1*
Abstract
Background: β1- and β2–adrenergic receptors (ARs) play distinct roles in the heart, e.g. β1AR is pro-contractile andpro-apoptotic but β2AR anti-apoptotic and only weakly pro-contractile. G protein coupled receptor kinase (GRK)-2desensitizes and opposes βAR pro-contractile signaling by phosphorylating the receptor and inducing beta-arrestin(βarr) binding. We posited herein that GRK2 blockade might enhance the pro-contractile signaling of the β2ARsubtype in the heart. We tested the effects of cardiac-targeted GRK2 inhibition in vivo exclusively on β2AR signalingunder normal conditions and in heart failure (HF).
Results: We crossed β1AR knockout (B1KO) mice with cardiac-specific transgenic mice expressing the βARKct, aknown GRK2 inhibitor, and studied the offspring under normal conditions and in post-myocardial infarction (MI).βARKct expression in vivo proved essential for β2AR-dependent contractile function, as β2AR stimulation withisoproterenol fails to increase contractility in either healthy or post-MI B1KO mice and it only does so in thepresence of βARKct. The main underlying mechanism for this is blockade of the interaction of phosphodiesterase(PDE) type 4D with the cardiac β2AR, which is normally mediated by the actions of GRK2 and βarrs on the receptor.The molecular “brake” that PDE4D poses on β2AR signaling to contractility stimulation is thus “released”. Regardingthe other beneficial functions of cardiac β2AR, βARKct increased overall survival of the post-MI B1KO miceprogressing to HF, via a decrease in cardiac apoptosis and an increase in wound healing-associated inflammationearly (at 24 hrs) post-MI. However, these effects disappear by 4 weeks post-MI, and, in their place, upregulation ofthe other major GRK in the heart, GRK5, is observed.
Conclusions: GRK2 inhibition in vivo with βARKct is absolutely essential for cardiac β2AR pro-contractile signalingand function. In addition, β2AR anti-apoptotic signaling in post-MI HF is augmented by βARKct, although this effectis short-lived.
Keywords: Cardiac β2–adrenergic receptor, Pro-contractile signaling, Post-myocardial infarction survival,GRK2 inhibition, GRK5
* Correspondence: [email protected] of Pharmaceutical Sciences, Laboratory for the Study ofNeurohormonal Control of the Circulation, Nova Southeastern UniversityCollege of Pharmacy, Fort Lauderdale, FL 33328, USAFull list of author information is available at the end of the article
© 2013 Salazar et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.
Salazar et al. Cell Communication and Signaling 2013, 11:64http://www.biosignaling.com/content/11/1/64

BackgroundDespite recent advances in prevention and managementof heart disease, death due to post-myocardial infarction(MI) heart failure (HF) continues to rise and new treat-ments are needed [1]. β1- and β2–adrenergic receptors(ARs) are the main stimulatory receptors of cardiacfunction but are now known to play clearly distinct rolesin cardiac physiology and pathology [2-5]. For instance,cardiomyocyte contraction is readily stimulated byβ1ARs but not β2ARs and β1AR signaling is generallyconsidered pro-apoptotic whereas β2AR signaling anti-apoptotic in the heart [2-5]. These differences might beexplained by differences in the signaling complexes as-sembled by activation of these two βARs: β1AR forms acomplex with phosphodiesterase (PDE) 4D8 directlywhen inactive, and agonist binding dissociates it [6,7].Additionally, β1AR does not readily bind the receptoradapter proteins beta-arrestins (βarrs) following itsagonist-promoted phosphorylation by G protein coupledreceptor kinases (GRKs), the most prominent membersof which in the heart are GRK2 and −5 [8-11]. In con-trast, β2AR recruits another PDE variant upon its agonistactivation, PDE4D5, via its interaction with βarrs follow-ing its GRK-dependent phosphorylation [6,7,12-16]. PDErecruitment to the receptor’s signaling complex plays acrucial role in compartmentalizing the cyclic adenosinemonophosphate (cAMP) signal and thereby tightlyregulating βAR-stimulated contractility [7]. It has beenpostulated that this PDE4D5 recruitment to the agonist-activated cardiac β2AR poses a “brake” on the β2AR cAMPsignaling’s ability to stimulate contractility [6,7,13,15]. Bycontrast, agonist-promoted dissociation of PDE from theβ1AR underlies the more “diffuse” and more powerful atstimulating contraction signaling of this βAR subtype[6,7]. Of note, cardiac β2AR signaling has been reported tobecome more “diffuse” and decompartmentalized, i.e. toadopt a β1AR-like signaling pattern, in a rat model of HF,which might underlie cardiac β2AR dysfunction inHF [17].On the other hand, cardiac β2AR can switch its signaling
from Gs protein-mediated to Gi/o protein-mediated, whichis believed to underlie its anti-apoptotic effects and is afeature cardiac β1ARs lack [18-24]. Finally, the interactionsof the β2AR with the βarrs, which require prior receptorphosphorylation by GRKs, can have pleiotropic effects incardiac myocytes, such as inhibition of apoptosis/pro-motion of survival by promoting extracellular signal-regulated kinase (ERK) signaling [25] and inhibition ofinflammation by blocking the pro-inflammatory trans-cription factor nuclear factor-kappaB (NF-κB) [26,27], acrucial mediator of major pro-inflammatory cytokine ex-pression, such as tumor necrosis factor-alpha (TNF-α)and interleukin-1 and −6 (IL-1 & -6) [28-30]. These βarr-dependent signaling effects may also play some part in the
well known and described anti-apoptotic and other benefi-cial in post-MI HF effects of cardiac β2AR.Cardiac GRK2 is a major negative regulator of βAR pro-
contractile signaling [8-11]. By desensitizing both β1- andβ2ARs, i.e. terminating their G protein-mediated signalingthrough cAMP, it dramatically reduces cardiac inotropicand adrenergic reserves, and since it is markedly elevatedin HF, its blockade represents an attractive therapeuticstrategy for heart disease treatment [8-11,31-35]. Giventhat GRK2 can block the pro-contractile and other benefi-cial signaling of cardiac β2AR in HF, and also that its ac-tion on β2AR induces recruitment of βarrs with all theiraforementioned myriad effects on this receptor’s signaling,we hypothesized, in the present study, that cardiac GRK2blockade in vivo might enhance β2AR signaling post-MI.In order to study the effects of GRK2 blockade specificallyon this subtype’s signaling, without any interference by thequalitatively different β1AR signaling, we utilized the β1ARknockout (B1KO) mice [36], which we crossed with miceoverexpressing the known GRK2 inhibitor mini-geneβARKct (or GRK2ct) specifically in cardiac myocytes [32].After breeding the offspring to homozygosity, we studiedthem both under normal conditions (i.e. healthy, sham-operated animals) and after surgically induced MI to induceHF. We found that GRK2 inhibition in vivo is absolutelynecessary for the β2AR to be capable of increasing contract-ility. In addition, β2AR anti-apoptotic signaling post-MI isaugmented by βARKct, but only acutely.
ResultsβARKct restores cardiac β2AR-dependent pro-contractilesignaling by reducing the interaction of PDE4D with thereceptorWe developed the hybrid transgenic line βARKct/B1KOby crossing the B1KO mice with the βARKct transgenicmice, which express βARKct only in cardiomyocytes.The βARKct/B1KO’s breed normally, without any grossabnormalities and present no overt cardiovascular orother phenotype (data not shown). Three-month-oldmale mice were chosen to undergo surgical MI in orderto induce HF and were studied alongside age-matchedmale homozygous B1KO’s (without βARKct expression),which served as the control group.Since GRK2 is a major (negative) regulator of cardiac
βAR-dependent contractility in vivo, and the β2AR stimu-lates contractility only very weakly, we first examined thecardiac function parameters of these mice, both in shamand post-MI groups. Echocardiography revealed that theB1KO mice display significantly decreased ejection frac-tion compared to control wild type (WT) mice, both undernormal conditions (sham groups) and at 4 weeks post-MI,as expected since the β1AR is the major βAR subtype inthe heart stimulating contractility (Table 1) [8]. Notably,βARKct overexpression led to significant augmentation of
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 2 of 10http://www.biosignaling.com/content/11/1/64

the ejection fraction of the B1KO mice, up to the levels ofWT mice, again both in normal and in 4 week post-MImice (Table 1), while, as already known from our studiesin the past [10,11,32,33], βARKct significantly augmentscontractility of the WT mice, as well (Table 1). Import-antly, when the mice underwent in vivo cardiac cathe-terization to measure their hemodynamic responses toisoproterenol stimulation (a standard βAR full agonist),B1KO mice, remarkably, completely failed to show any in-crease in contractility (as measured by the +dP/dtmax LVpressure elevation parameter), even at the highest concen-tration of isoproterenol challenge (Max. Iso, Table 1). Incontrast, the hybrid βARKct/B1KO mice showed verygood contractile responses to isoproterenol, both in thesham (healthy) conditions and in post-MI HF (Table 1).As expected, the other two mouse lines, i.e. WT andβARKct, were responsive to βAR stimulation, with the HFanimals in these groups showing somewhat reduced re-sponses compared to their sham counterparts and theβARKct line displaying much more robust responses com-pared to the WT group (Table 1). These results stronglyindicate that cardiac GRK2 is a major opposing force forthe β2AR pro-contractile function and only when its activ-ity is blocked (e.g. in the presence of βARKct) is the car-diac β2AR capable of promoting contractility in responseto agonist stimulation.To identify the main signaling mechanism underlying
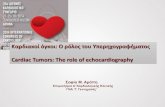
this dramatic effect of βARKct on cardiac β2AR-dependent contractiity, we examined the levels ofPDE4D interaction with the β2AR in cardiac membranesof these mice in vivo. As shown in Figures 1A and 1B,the interaction of cardiac β2AR with both the PDE4D3and -D5 isoforms is significantly reduced in βARKct/
B1KO mouse hearts compared to control B1KO hearts,an effect that might enable βARKct to enhance cardiacβ2AR-dependent pro-contractile signaling in vivo.
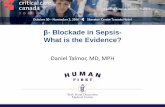
βARKct and cardiac β2AR-dependent anti-apoptotic/inflammatory signalingNext, we examined the impact of βARKct expression onthe other major aspect of cardiac β2AR signaling, anti-apoptosis/cardiac survival. Post-MI βARKct/B1KO micedisplay markedly better survival post-MI compared to theirB1KO counterparts (Figure 2A). Kaplan-Meier survivalcurves indicated that at 4 weeks post-MI, a significant(~70%) of βARKct/B1KO’s are still alive, compared toonly ~40% of B1KO’s at the same time point post-MI(Figure 2A). In addition, cardiac apoptosis is found signifi-cantly decreased very early (at 24 hrs) post-MI in theβARKct/B1KO hearts compared to control B1KO hearts(Figure 2B) but similar between the two groups at 4 weekspost-MI (Figure 2B), indicating that this reduction in post-MI apoptosis induced by βARKct is short-lived. Asfor post-MI cardiac inflammation in the two animalgroups, levels of the major pro-inflammatory cytokinesTNFα(Figure 2C), IL-6 (Figure 2D) and IL-1β (Figure 2E)are significantly increased in the hearts of βARKct/B1KOmice, compared to control B1KO hearts at 24 hrs post-MI,indicating increased wound (infarct) healing-associated in-flammation. By 4 weeks post-MI however, levels of all thesethree cytokines (TNFα, IL-6, IL-1β) in βARKct/B1KOhearts have returned to the levels of 24-hour post-MIB1KO hearts (data not shown), indicating that also the ef-fect of βARKct on post-MI inflammation is short-lived.To identify potential signaling mechanisms underlying
these effects of βARKct on apoptosis and inflammation
Table 1 In vivo cardiac functional parameters
Parameter WT-Sham
βARKct-Sham
B1KO-Sham
βARKct/ B1KO-Sham
WT-MI βARKct-MI
B1KO-MI βARKct/ B1KO-MI
Infarct size (% LV free wall) N/A N/A N/A N/A 41±1.2 42±2.2 40±2.6 43±3.0
FS (%) 41.4±1.3 48.3±2.8^ 36.7±2.6^ 41.3±2.4# 18.6±2.2 23.7±1.3+ 11.0±1.4+ 19.0±2.4*
EF (%) 72.0±1.0 78.0±2.0^ 67.0±2.4^ 72.0±2.0# 37.5±3.0 45.3±2.4+ 23.7±2.5+ 38.5±4.2*
Basal HR (min–1) 385±12 402±37 402±27 383±23 392±12 408±10 391±8 389±13
Basal LV +dP/dtmax
(mm Hg/s)4692±363 6835±637^ 3572±287^ 4576±375# 3512±220 4900±172+ 2576±155+ 3549±231*
Basal LV –dP/dtmin
(mm Hg/s)−4568±452 −6714±536^ −3269±296^ −4782±286# −3515±246 −4620±203+ −2592±233+ −3471±194*
Max. Iso-HR (min–1) 557±36 515±40 405±28^ 393±14^ 509±24 581±17+ 399±11+ 413±20+
Max. Iso-LV +dP/dtmax
(mm Hg/s)8825±644 13547±476^ 3611±286^ 9041±528# 5641±431 9419±601+ 2639±139+ 5628±419*
Max. Iso-LV–dP/dtmin
(mm Hg/s)−7210±430 −8837±491^ −3199±279^ −6344±364# −5880±303 −6948±277+ −2605±251+ −5548±382*
Cardiac parameter values of three-month-old wild type (WT, i.e. C57/B6), βARKct, B1KO and βARKct/B1KO mice measured at 4 weeks after MI or sham operation(Sham). LV +dP/dtmax maximal first derivative of LV pressure rise, LV –dP/dtmin minimal first derivative of LV pressure fall, HR heart rate, FS, fractional shortening,EF ejection fraction, LV Left ventricular, N/A Not applicable, Max. Iso dose: 333 ng/kg body weight. #, p<0.05, vs. B1KO-Sham; *, p<0.05, vs. B1KO-MI; ^, p<0.05,vs. WT-Sham; +, p<0.05, vs. WT-MI; n=7 mice/group. One-way ANOVA with Bonferroni test was performed among groups. Data are presented as mean ± SEM.
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 3 of 10http://www.biosignaling.com/content/11/1/64

in post-MI B1KO hearts, we examined protein levels ofthe major anti-apoptotic mediator Bcl-2 [37] and levelsof activation of the crucial pro-inflammatory transcrip-tion factor NFκB. Bcl-2 was found significantly up-regulated in βARKct/B1KO hearts compared to controlB1KO hearts at 24 hrs post-MI (Figures 3A and 3B), in-dicating enhanced cellular survival/inhibition of apop-tosis. However, at 4 weeks post-MI, Bcl-2 protein wasvirtually undetectable in the hearts of both mouse lines(Figure 3C), which is consistent with the phenotypicfinding of the short-lived inhibition of apoptosis in theheart by βARKct (Figure 2B). In addition, NFκB activa-tion appears also markedly elevated in βARKct/B1KOhearts compared to control B1KO hearts at 24 hrs post-MI (Figures 3A and 3B), indicating enhanced cardiac in-flammation. For NFκB to get activated, its inhibitoryIκBα subunit must be phosphorylated and subsequentlytargeted for proteasomal degradation to release the tran-scriptionally active subunits of the complex [28-30].Thus, increased phosphorylation of IκBα and decreasedlevels (increased degradation) of total IκBα in the hybrid
transgenic hearts at 24 hrs post-MI (Figures 3A and 3B)suggest increased NFκB activation compared to B1KOhearts. Finally, blotting for βARKct in these hearts con-firmed the robust expression of this GRK2 inhibitor inthe hearts of βARKct/B1KO’s, which, of course, was ab-sent from the hearts of B1KO mice (Figure 3A).
GRK5 and cardiac β2AR-dependent signalingApart from GRK2, the other major cardiac GRK thatcan phosphorylate and desensitize β2ARs, and thus op-pose β2AR pro-contractile and anti-apoptotic signaling,is GRK5 [8-10]. As shown in Figure 3D, cardiac post-MIGRK5 levels are initially (at 24 hrs post-MI) similar be-tween the two groups, as is the case also in the healthy,sham-operated groups (data not shown). By 4 weekspost-MI however, a significant up-regulation (~2-foldincrease) of GRK5 is observed in βARKct/B1KO heartscompared to control B1KO hearts (Figure 3D), indicat-ing that GRK2 inhibition with βARKct leads to a com-pensatory up-regulation of GRK5 over time.
Figure 1 β2AR-PDE4D interaction in the heart. Co-immunoprecipitation (co-IP) followed by western blotting in cardiac extracts from normal(sham) B1KO and βARKct/B1KO (CT/B1KO) mice to measure the β2AR-PDE4D interaction in the heart. Representative immunoblots are shown in(A), and the amounts of the co-immunoprecipitated PDE4D isoforms, as measured by densitometry and normalized with the amount of β2ARpulled down in the co-IP, are shown in (B). *, p<0.05, vs. B1KO; n=4 independent experiments (i.e. performed on 4 different hearts from eachmouse line). IP: Immunoprecipitation, IB: Immunoblotting.
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 4 of 10http://www.biosignaling.com/content/11/1/64

Figure 2 (See legend on next page.)
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 5 of 10http://www.biosignaling.com/content/11/1/64

DiscussionThe present study reports for the first time, to ourknowledge, that cardiac GRK2 is an endogenous “stum-bling block” that normally prevents β2AR signaling fromstimulating contractility, mainly because it promotes
association of this βAR subtype with PDE4D in theheart, a major molecular “brake” on cardiac β2AR-dependent contractility [6,7,15]. Thus, only when cardiacGRK2 is blocked (e.g. with βARKct) is the β2AR capableof promoting cardiac contractility. Obviously, several
(See figure on previous page.)Figure 2 Survival, cardiac apoptosis and inflammation post-MI. (A) Kaplan-Meier survival curves of the 4 groups of mice of the study:sham-operated (Sham) and post-MI (MI) B1KO and βARKct/B1KO mice. p=0.011 between MI B1KO and MI βARKct/B1KO; n=15 mice/group for sham,37 mice/group for MI mice. (B) Apoptotic cell death at 24 hrs and at 4 weeks (wks) post-MI in the two transgenic (B1KO and CT/B1KO) lines, asmeasured by TUNEL performed in the border zone of the infarct. No difference in rate of apoptosis in the remote zone at either post-MI time pointwas found (data not shown). **, p<0.05, vs. B1KO 24 hrs, n=6 mice/group. (C-E) Levels of pro-inflammatory cytokines TNFα (C), IL-6 (D), and IL-1β (E),measured via ELISA in serum of intra-cardiac blood from B1KO and βARKct/B1KO (CT/B1KO) mice at 24 hrs post-MI. *, p<0.05, n=5 mice/group.
Figure 3 Levels of cardiac Bcl-2, NFκB activity and GRK5 post-MI. (A-B) Western blotting in total cardiac extracts from 24 hr post-MI B1KOand βARKct/B1KO (CT/B1KO) mice for βARKct, Bcl-2, phospho-IκBα (pIκBα), and total IκBα. Representative blots are shown in (A), including blotsfor glyceraldehyde 3-phosphate dehydrogenase (GAPDH) as loading control for each protein tested, and densitometric quantitation, normalizedwith GAPDH as control and expressed as % of B1KO levels, of 4 independent experiments done in duplicate, is shown in (B). *, p<0.05, vs. B1KO.(C) Western blotting for Bcl-2 protein in total cardiac extracts from 4 week post-MI B1KO and βARKct/B1KO (CT/B1KO) mice. Representative blotsfrom 4 independent experiments done in duplicate are shown, including GAPDH as loading control and h9c2 cell extract as positive control(input) for Bcl-2. Bcl-2 was virtually undetectable in either group at 4 weeks post-MI. (D) Western blotting for GRK5 in total cardiac extracts fromB1KO and βARKct/B1KO (CT/KO) mice at 24 hrs and at 4 weeks (wks) post-MI. Representative blots of 4 independent experiments done induplicate, with GAPDH as loading control, are shown on top, and densitometric quantitation on bottom. *, p<0.05, vs. all other groups.
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 6 of 10http://www.biosignaling.com/content/11/1/64

signaling mechanisms/pathways are at play, the pre-sent study has identified the following two: 1) βARKct, byblocking GRK2, reduces the uncoupling of β2AR withthe classical pro-contractile Gs protein-adenylyl cyclase-cAMP-PKA signaling pathway (Figure 4), and 2) GRK2blockade reduces the interaction of β2AR with βarrs,which scaffold on themselves various isoforms of PDE4D(mainly PDE4D3 and PDE4D5) (Figure 4). PDE4D causesdegradation of the local cAMP signals produced byactivated β2AR, which are essential for stimulation ofcontractility, and thus it weakens these pro-contractilesignals hampering β2AR-stimulated contractility [6,7,15].By indirectly reducing the βarr-PDE4D interactionwith the cardiac β2AR, βARKct releases the “brake”PDE4D poses on this receptor’s pro-contractile signal-ing and enhances its capacity to stimulate contractility(Figure 4).
Since the other major beneficial effect of cardiac β2ARsignaling in vivo is inhibition of apoptosis (promotion ofsurvival), we also tested the effects of cardiac GRK2blockade in vivo on this aspect of β2AR signaling in thecontext of post-MI HF progression. We found that earlyon after MI, cardiac GRK2 blockade with βARKct alsodramatically augments β2AR anti-apoptotic signaling, aswell as its pro-infarct healing inflammatory signaling, inthe heart. This results in significant reduction in all-cause mortality (marked increase in animal survival inthe first 4 weeks post-MI), and reduced cellular apop-tosis in the post-MI heart, compared to B1KO mice withunopposed cardiac GRK2 activity. Thus, βARKct en-hances not only cardiac contractility, but also cardiacsurvival stimulated by the β2AR, which further rein-forces its validity as an attractive therapeutic strategy topotentiate cardiac β2AR signaling and function in post-MI
Figure 4 Schematic illustration of the signaling pathways discussed in the present study that are elicited by β2AR activation in cardiacmyocytes and are affected by GRK2 inhibition with βARKct. CA: Catecholamine; AC: Adenylyl cyclase; ATP: adenosine triphosphate. See textfor details and all other molecular acronym descriptions.
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 7 of 10http://www.biosignaling.com/content/11/1/64

HF. Of course, enhancement of the anti-apoptotic signalingof other cardio-protective receptors that are also GRK2substrates by βARKct cannot be ruled out and is, in fact,quite likely to have contributed to the observed cardiacapoptosis phenotype of βARKct/B1KO mice. However,βARKct’s cardio-protective and anti-apoptotic effects havebeen shown to be β2AR-dependent, since selective block-ade of this receptor in cardiac myocytes abolishes βARKct-mediated anti-apoptotic effects [38]. On the other hand,effects of βARKct on β2AR-dependent pro-angiogeneticsignaling, which plays an important role in peri-infarct HFprogression [39], cannot be ruled out either. Nevertheless,it becomes quite clear from our current data that βARKctaugments β2AR contractile function without negatively af-fecting its anti-apoptotic one, but rather actually preservingand further enhancing this β2AR function, as well.However, this augmentation of anti-apoptotic signaling
is short-lived: by 4 weeks post-MI, cardiac cellular apop-tosis has returned to the 24-hour post-MI B1KO heartlevels. This might be related to the nature of cardiac β2ARpro-survival signaling; β2AR can have remarkably differenteffects in the heart depending on its expression levels andon time [40,41]. Cardiac β2AR is known to be beneficial(i.e. promoting survival) at low levels of overexpressionand in the first few months of life in mice, but whenoverexpressed at extremely high levels in murine hearts orlater on in the mouse’s life, these animals do not surviveand die of severe cardiac complications [40]. Mechanistic-ally, cardiac β2AR anti-apoptotic signaling is known toproceed mainly through the Gi/o protein signaling pathway[20-23], to which it is capable of switching following itsphosphorylation by PKA [42]. GRK2 blockade by βARKctcan increase this signaling by a) decreasing the pathway’sβarr-mediated desensitization, i.e. increasing the couplingof Gi/o proteins with the β2AR, and b) by increasing thePKA-dependent switching of β2AR signaling from Gs toGi/o proteins thanks to the increase of β2AR signaling viathe Gs protein-cAMP-PKA (the pro-contractile) pathwayit also causes, discussed above (Figure 4). With regards tothe pro-inflammatory signaling of cardiac β2AR, βarrs areknown to scaffold and stabilize the inhibitory IκBα subunitof NFκB, thereby prohibiting NFκB activation [26,27].GRK2 blockade with βARKct decreases βarr interactionwith the β2AR thereby “releasing” the inhibitory effect ofβarrs on NFκB activation (Figure 4). Thus, NFκB activa-tion and the subsequent pro-inflammatory cytokine pro-duction are enhanced (Figure 4). Indeed, NFκB activationand inflammatory cytokine levels were found significantlyelevated in βARKct/B1KO hearts compared to B1KOhearts without GRK2 inhibition at 24 hrs post-MI.Meanwhile however, βARKct also causes upregulation
of the other major cardiac GRK, GRK5, in the first fewweeks post-MI. This is also probably due to the enhancedNFκB activation (Figure 4), since NFκB can cause
upregulation of GRK5 in cardiomyocytes [43]. Import-antly, and given that GRK5 elevation is generally consid-ered detrimental for the heart [8-10], this finding mightexplain, at least in part, the aforementioned switching ofcardiac β2AR signaling from beneficial (anti-apoptotic)early in life of transgenic mice or at low levels of receptorexpression to detrimental (pro-apoptotic) later on in thelifespan of these mice or at very high levels of cardiacβ2AR overexpression [41]. Of note, GRK5 has also beenreported to bind (via its non-catalytic, N-terminal domain)to, and stabilize IκBα, thereby inhibiting NFκB activity inseveral tissues, including the heart [44]. Therefore, ourpresent findings strongly indicate that a negative feedbackloop might exist in the heart, in which NFκB inducesGRK5 expression, and GRK5 can subsequently suppressNFκB activation (Figure 4).
ConclusionsIn summary, the present study reports that cardiacGRK2 inhibition with βARKct in vivo is absolutely es-sential for the cardiac β2AR subtype’s pro-contractilefunction, all the while preserving and augmenting thisreceptor’s beneficial anti-apoptotic/pro-survival and pro-infarct healing signaling pathways post-MI, early on afterthe cardiac insult. However, the effects of βARKct onthe latter signaling modalities are transient due (in part)to compensatory elevation of cardiac GRK5 over time.
MethodsExperimental animals and surgical proceduresThe animals in this study were handled according to ani-mal welfare regulations and protocols approved by the au-thors’ Institutional Review Boards. Genetically engineered,8- to 12-wk-old β1AR KO (B1KO) (on C57/B6 back-ground) [36] and the offspring of their cross with Mini-27mice, expressing the βARKct (or GRK2ct) transgene underthe alpha-myosin heavy chain gene promoter [32], wereused for this study. Mice were anesthetized with a mixtureof ketamine (100 mg/kg) and xylazine (2.5 mg/kg). Ani-mals were placed in the supine position on a heated oper-ation board and a midline cervical incision was made toexpose the trachea. Following successful endotrachealintubation, the cannula was connected to a rodent ventila-tor. The entire left ventricle (i.e. both infarct and non-infarct zones) were used for subsequent histological andbiochemical assays. Myocardial infarction was performedas previously described [35].
Echocardiography & in vivo hemodynamicsTransthoracic echocardiography was performed with alinear 30-MHz transducer (VeVo 770 High ResolutionImaging System, VisualSonics, Toronto, ON, Canada), as
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 8 of 10http://www.biosignaling.com/content/11/1/64

described [35]. In vivo hemodynamic analysis was alsoperformed as previously described [35].
In situ TUNEL stainingHeart specimens were fixed with 10% neutral bufferedformalin, embedded in paraffin, and sectioned at 5-μmthickness. DNA fragmentation was detected in situ indeparaffinized sections using the ApopTag Kit (Intergene)and according to manufacturer’s instructions, as describedpreviously [45]. The total number of nuclei was deter-mined by manual counting of DAPI-stained nuclei in sixrandom fields per section. All terminal deoxynucleotidyltransferase-mediated dUTP nick end-labeling (TUNEL)-positive nuclei were counted in each section.
Co-immunoprecipitation and western blottingCardiac extracts were prepared in 20 mM Tris pH 7.4,137 mM NaCl, 1% Nonidet P-40, 20% glycerol, 10 mMPMSF, 1 mM Na3VO4, 10 mM NaF, 2.5 μg/ml aprotinin,and 2.5 μg/ml leupeptin. Protein concentration was thendetermined and equal amounts of protein per sample wereloaded on SDS-PAGE gels for electrophoretic separation,as described previously [46]. For β2AR-PDE4D co-immunoprecipitation experiments, β2AR was immuno-precipitated with an anti-mouse β2AR antibody (sc-9042,Santa Cruz), immobilized on Protein A-sepharose beads(Invitrogen), prior to SDS-PAGE/western blotting. TotalIκBα and phospho-IκBα were detected by using anti-IκBα(sc-1643, Santa Cruz) and anti-phosphoIκBα at Ser-32(sc-7977, Santa Cruz) antibodies, Bcl-2, GRK5, GRK2/βARKct and GAPDH, with antibodies sc-492, sc-565,sc-562, and sc-25778, respectively (all from Santa Cruz),and PDE4D (various isoforms) with the PD4-401APantibody (FabGennix). Immunoblots were revealed byenhanced chemiluminescence (ECL, Amersham Biosci-ences) and visualized in the FluorChem E Digital Dark-room (Cell Biosciences). Densitometry was performedwith the AlphaView software (Cell Biosciences) in the lin-ear range of signal detection (on non-saturated bands).
Cytokine measurements via ELISAPro-inflammatory cytokines TNFα, IL-6 and IL-1β weremeasured in serum obtained from left ventricular blood,immediately prior to heart excision and animal euthaniz-ing, via multiplexed ELISA, as described [47,48]. Theassay was performed using the Mouse Cytokine ELISAProfiling Kit (EA-1091, Signosis), according to the man-ufacturer’s instructions.
Statistical analysesData are generally expressed as mean ± SEM. Unpaired 2-tailed Student’s t test and one- or two-way ANOVA withBonferroni test were generally performed for statistical
comparisons, unless otherwise indicated. For all tests, ap value of <0.05 was generally considered to be significant.
AbbreviationsβAR: Beta-adrenergic receptor; B1KO: β1AR knockout; GRK: G protein-coupledreceptor kinase; βARKct: Beta-adrenergic receptor kinase (GRK2) carboxylterminal fragment; βarr: Beta-arrestin; PDE: Phosphodiesterase; MI: Myocardialinfarction; HF: Heart failure; NFκB: Nuclear factor-kappaB; IκBα: Inhibitor ofnuclear factor-kappaB alpha subunit; cAMP: 3′-5′ adenosine monophosphate(cyclic adenosine monophosphate); WT: Wild type; PKA: Protein kinase A;Gs: Stimulatory G protein; Gi/o: Inhibitory or other G protein; TNFα: Tumornecrosis factor alpha; IL: Interleukin; TUNEL: Terminal deoxynucleotidyltransferase-mediated dUTP nick-end labeling; Bcl-2: B-cell lymphoma 2;LV: Left ventricular; ELISA: Enzyme-linked immunosorbent assay.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsNCS, XV, AS, GR, AC, DLic, CDL, and EG performed research. DLeos assistedwith writing of the paper. WJK supervised the project, provided funding forthe research and assisted with writing of the paper. AL conceived andsupervised the project, designed research, provided funding for it, and wrotethe paper. All authors have read and approved the final manuscript.
AcknowledgmentsThis work was supported in part by a Scientist Development Grant from theAmerican Heart Association (AHA #09SDG2010138, National Center) and aNova Southeastern University’s Health Professions Division (HPD) ResearchGrant (to AL), and NIH grants R37 HL061690, R01 HL085503, P01 HL075443(Project 2) and P01 HL091799 (to WJK).
Author details1Department of Pharmaceutical Sciences, Laboratory for the Study ofNeurohormonal Control of the Circulation, Nova Southeastern UniversityCollege of Pharmacy, Fort Lauderdale, FL 33328, USA. 2Division of Cardiology,Department of Internal Medicine, Cardiovascular Sciences and Immunology,University “Federico II”, Naples, Italy. 3Center for Translational Medicine,Temple University, Philadelphia, PA 19140, USA.
Received: 27 June 2013 Accepted: 23 August 2013Published: 28 August 2013
References1. Tamargo J, López-Sendón J: Novel therapeutic targets for the treatment
of heart failure. Nat Rev Drug Disc 2011, 10:536–555.2. Xiang Y, Kobilka BK: Myocyte adrenoceptor signaling pathways. Science
2003, 300:1530–1532.3. Xiao RP, Zhu W, Zheng M, Chakir K, Bond R, Lakatta EG, Cheng H:
Subtype-specific beta-adrenoceptor signaling pathways in the heartand their potential clinical implications. Trends Pharmacol Sci 2004,25:358–365.
4. Devic E, Xiang Y, Gould D, Kobilka B: Beta-adrenergic receptor subtype-specificsignaling in cardiac myocytes from beta(1) and beta(2) adrenoceptorknockout mice. Mol Pharmacol 2001, 60:577–583.
5. Bernstein D, Fajardo G, Zhao M, Urashima T, Powers J, Berry G, Kobilka BK:Differential cardioprotective/cardiotoxic effects mediated by beta-adrenergicreceptor subtypes. Am J Physiol Heart Circ Physiol 2005, 289:H2441–H2449.
6. Xiang Y, Naro F, Zoudilova M, Jin SL, Conti M, Kobilka B: Phosphodiesterase4D is required for beta2 adrenoceptor subtype-specific signaling incardiac myocytes. Proc Natl Acad Sci USA 2005, 102:909–914.
7. Richter W, Day P, Agrawal R, Bruss MD, Granier S, Wang YL, Rasmussen SG,Horner K, Wang P, Lei T, Patterson AJ, Kobilka B, Conti M: Signaling frombeta1- and beta2-adrenergic receptors is defined by differentialinteractions with PDE4. EMBO J 2008, 27:384–393.
8. Rockman HA, Koch WJ, Lefkowitz RJ: Seven-transmembrane-spanningreceptors and heart function. Nature 2002, 415:206–212.
9. Rengo G, Lymperopoulos A, Koch WJ: Future g protein-coupled receptortargets for treatment of heart failure. Curr Treat Options Cardiovasc Med2009, 11:328–338.
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 9 of 10http://www.biosignaling.com/content/11/1/64

10. Belmonte SL, Blaxall BC: G protein coupled receptor kinases astherapeutic targets in cardiovascular disease. Circ Res 2011, 109:309–319.
11. Rengo G, Lymperopoulos A, Leosco D, Koch WJ: GRK2 as a novel genetherapy target in heart failure. J Mol Cell Cardiol 2011, 50:785–792.
12. Baillie GS, Sood A, McPhee I, Gall I, Perry SJ, Lefkowitz RJ, Houslay MD:beta-Arrestin-mediated PDE4 cAMP phosphodiesterase recruitmentregulates beta-adrenoceptor switching from Gs to Gi. Proc Natl Acad SciUSA 2003, 100:940–945.
13. Houslay MD, Adams DR: PDE4 cAMP phosphodiesterases: modularenzymes that orchestrate signalling cross-talk, desensitization andcompartmentalization. Biochem J 2003, 370:1–18.
14. De Arcangelis V, Liu R, Soto D, Xiang Y: Differential association ofphosphodiesterase 4D isoforms with beta2-adrenoceptor in cardiacmyocytes. J Biol Chem 2009, 284:33824–33832.
15. Fischmeister R, Castro LR, Abi-Gerges A, Rochais F, Jurevicius J, Leroy J,Vandecasteele G: Compartmentation of cyclic nucleotide signaling in theheart: the role of cyclic nucleotide phosphodiesterases. Circ Res 2006,99:816–828.
16. Conti M, Beavo J: Biochemistry and physiology of cyclic nucleotidephosphodiesterases: essential components in cyclic nucleotide signaling.Annu Rev Biochem 2007, 76:481–511.
17. Nikolaev VO, Moshkov A, Lyon AR, Miragoli M, Novak P, Paur H, Lohse MJ,Korchev YE, Harding SE, Gorelik J: Beta2-adrenergic receptor redistribution inheart failure changes cAMP compartmentation. Science 2010, 327:1653–1657.
18. Chesley A, Lundberg MS, Asai T, Xiao RP, Ohtani S, Lakatta EG, Crow MT:The beta(2)-adrenergic receptor delivers an antiapoptotic signal tocardiac myocytes through G(i)-dependent coupling tophosphatidylinositol 3′-kinase. Circ Res 2000, 87:1172–1179.
19. Patterson AJ, Zhu W, Chow A, Agrawal R, Kosek J, Xiao RP, Kobilka B:Protecting the myocardium: a role for the beta2 adrenergic receptor inthe heart. Crit Care Med 2004, 32:1041–1048.
20. Xiao RP, Avdonin P, Zhou YY, Cheng H, Akhter SA, Eschenhagen T,Lefkowitz RJ, Koch WJ, Lakatta EG: Coupling of beta2-adrenoceptor to Giproteins and its physiological relevance in murine cardiac myocytes.Circ Res 1999, 84:43–52.
21. Zhu W, Zeng X, Zheng M, Xiao RP: The enigma of beta2-adrenergicreceptor Gi signaling in the heart: the good, the bad, and the ugly.Circ Res 2005, 97:507–509.
22. Hasseldine AR, Harper EA, Black JW: Cardiac-specific overexpression ofhuman beta2 adrenoceptors in mice exposes coupling to both Gs andGi proteins. Br J Pharmacol 2003, 138:1358–1366.
23. Communal C, Singh K, Sawyer DB, Colucci WS: Opposing effects of beta(1)- and beta(2)-adrenergic receptors on cardiac myocyte apoptosis: roleof a pertussis toxin-sensitive G protein. Circulation 1999, 100:2210–2212.
24. Zhu WZ, Zheng M, Koch WJ, Lefkowitz RJ, Kobilka BK, Xiao RP: Dualmodulation of cell survival and cell death by beta(2)-adrenergicsignaling in adult mouse cardiac myocytes. Proc Natl Acad Sci USA 2001,98:1607–1612.
25. DeWire SM, Ahn S, Lefkowitz RJ, Shenoy SK: Beta-arrestins and cellsignaling. Annu Rev Physiol 2007, 69:483–510.
26. Witherow DS, Garrison TR, Miller WE, Lefkowitz RJ: beta-Arrestin inhibitsNF-kappaB activity by means of its interaction with the NF-kappaBinhibitor IkappaBalpha. Proc Natl Acad Sci USA 2004, 101:8603–8607.
27. Gao H, Sun Y, Wu Y, Luan B, Wang Y, Qu B, Pei G: Identification ofbeta-arrestin2 as a G protein-coupled receptor-stimulated regulator ofNF-kappaB pathways. Mol Cell 2004, 14:303–317.
28. Valen G, Yan ZQ, Hansson GK: Nuclear factor kappa-B and the heart. J AmColl Cardiol 2001, 38:307–314.
29. Valen G: Signal transduction through nuclear factor kappa B inischemia-reperfusion and heart failure. Basic Res Cardiol 2004, 99:1–7.
30. Rothwarf DM, Karin M: The NF-kappa B activation pathway: a paradigm ininformation transfer from membrane to nucleus. Sci STKE 1999, 1999:RE1.
31. Ungerer M, Böhm M, Elce JS, Erdmann E, Lohse MJ: Altered expression ofbeta-adrenergic receptor kinase and beta 1-adrenergic receptors in thefailing human heart. Circulation 1993, 87:454–463.
32. Koch WJ, Rockman HA, Samama P, Hamilton RA, Bond RA, Milano CA,Lefkowitz RJ: Cardiac function in mice overexpressing the β-adrenergicreceptor kinase or a βARK inhibitor. Science 1995, 268:1350–1353.
33. Rockman HA, Choi DJ, Akhter SA, Jaber M, Giros B, Lefkowitz RJ, Caron MG, Koch WJ:Control of myocardial contractile function by the level of β-adrenergicreceptor kinase 1 in gene-targeted mice. J Biol Chem 1998, 273:18180–18184.
34. Matkovich SJ, Diwan A, Klanke JL, Hammer DJ, Marreez Y, Odley AM,Brunskill EW, Koch WJ, Schwartz RJ, Dorn GW 2nd: Cardiac-specific ablationof G-protein receptor kinase 2 redefines its roles in heart developmentand β-adrenergic signaling. Circ Res 2006, 99:966–1003.
35. Raake PW, Vinge LE, Gao E, Boucher M, Rengo G, Chen X, DeGeorge BR Jr,Matkovich S, Houser SR, Most P, Eckhart AD, Dorn GW 2nd, Koch WJ: Gprotein- coupled receptor kinase 2 ablation in cardiac myocytes beforeor after myocardial infarction prevents heart failure. Circ Res 2008,103:413–422.
36. Rohrer DK, Desai KH, Jasper JR, Stevens ME, Regula DP Jr, Barsh GS, Bernstein D,Kobilka BK: Targeted disruption of the mouse beta1-adrenergic receptorgene: developmental and cardiovascular effects. Proc Natl Acad Sci USA1996, 93:7375–7380.
37. Whelan RS, Kaplinskiy V, Kitsis RN: Cell death in the pathogenesis of heartdisease: mechanisms and significance. Annu Rev Physiol 2010, 72:19–44.
38. Brinks H, Boucher M, Gao E, Chuprun JK, Pesant S, Raake PW, Huang ZM,Wang X, Qiu G, Gumpert A, Harris DM, Eckhart AD, Most P, Koch WJ: Levelof G protein-coupled receptor kinase-2 determines myocardial ischemia/reperfusion injury via pro- and anti-apoptotic mechanisms. Circ Res 2010,107:1140–1149.
39. Santulli G, Cipolletta E, Sorriento D, Del Giudice C, Anastasio A, Monaco S,Maione AS, Condorelli G, Puca A, Trimarco B, Illario M, Iaccarino G: CaMK4gene deletion induces hypertension. J Am Heart Assoc 2012, 1:e001081.
40. Dorn GW 2nd, Tepe NM, Lorenz JN, Koch WJ, Liggett SB: Low- and high- leveltransgenic expression of beta2-adrenergic receptors differentially affectcardiac hypertrophy and function in Galphaq-overexpressing mice.Proc Natl Acad Sci USA 1999, 96:6400–6405.
41. Liggett SB, Tepe NM, Lorenz JN, Canning AM, Jantz TD, Mitarai S, Yatani A,Dorn GW 2nd: Early and delayed consequences of beta(2)-adrenergicreceptor overexpression in mouse hearts: critical role for expressionlevel. Circulation 2000, 101:1707–1714.
42. Daaka Y, Luttrell LM, Lefkowitz RJ: Switching of the coupling of thebeta2-adrenergic receptor to different G proteins by protein kinase A.Nature 1997, 390:88–91.
43. Islam KN, Koch WJ: Involvement of nuclear factor κB (NF-κB) signalingpathway in regulation of cardiac G protein-coupled receptor kinase 5(GRK5) expression. J Biol Chem 2012, 287:12771–12778.
44. Sorriento D, Santulli G, Fusco A, Anastasio A, Trimarco B, Iaccarino G:Intracardiac injection of AdGRK5-NT reduces left ventricular hypertrophyby inhibiting NF-kappaB-dependent hypertrophic gene expression.Hypertension 2010, 56:696–704.
45. Yoo B, Lemaire A, Mangmool S, Wolf MJ, Curcio A, Mao L, Rockman HA:Beta1-adrenergic receptors stimulate cardiac contractility and CaMKIIactivation in vivo and enhance cardiac dysfunction following myocardialinfarction. Am J Physiol Heart Circ Physiol 2009, 297:H1377–H13786.
46. Lymperopoulos A, Rengo G, Funakoshi H, Eckhart AD, Koch WJ: AdrenalGRK2 upregulation mediates sympathetic overdrive in heart failure.Nat Med 2007, 13:315–323.
47. Scott NJ, Cameron VA, Raudsepp S, Lewis LK, Simpson ER, Richards AM,Ellmers LJ: Generation and characterization of a mouse model of themetabolic syndrome: apolipoprotein E and aromatase double knockoutmice. Am J Physiol Endocrinol Metab 2012, 302:E576–E584.
48. Hu Y, Zhang H, Lu Y, Bai H, Xu Y, Zhu X, Zhou R, Ben J, Xu Y, Chen Q: ClassA scavenger receptor attenuates myocardial infarction-inducedcardiomyocyte necrosis through suppressing M1 macrophage subsetpolarization. Basic Res Cardiol 2011, 106:1311–1328.
doi:10.1186/1478-811X-11-64Cite this article as: Salazar et al.: GRK2 blockade with βARKct is essentialfor cardiac β2-adrenergic receptor signaling towards increasedcontractility. Cell Communication and Signaling 2013 11:64.
Salazar et al. Cell Communication and Signaling 2013, 11:64 Page 10 of 10http://www.biosignaling.com/content/11/1/64
![Ca2+ Entry (SOCE) Contributes to Muscle Contractility in ... · physiological role in young and aged skeletal muscle. We found that reagents that prevent [Ca2+] o entry reduce contractile](https://static.fdocument.org/doc/165x107/5fbbf98d4e86af3f2a7e3a76/ca2-entry-soce-contributes-to-muscle-contractility-in-physiological-role.jpg)