Geographic diversity and temporal trends of antimicrobial resistance in Streptococcus pneumoniae in...
7
424 NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003 ARTICLES Streptococcus pneumoniae is a leading cause of bacteremia, sinusi- tis, otitis media, bacterial meningitis and bacterial pneumonia worldwide 1,2 . An increasing prevalence of S. pneumoniae strains resistant to important anti-pneumococcal drugs, including β-lac- tams and macrolides, has been observed in both developing and developed countries 3 . In the United States, the proportion of penicillin-resistant S. pneumoniae strains increased from 21% of tested isolates in 1995 to 24% in 1998 (ref. 4), and the propor- tion of macrolide-resistant strains increased from 10.6% in 1995 to 20.4% in 1999 (refs. 5, 6). Use of antimicrobial agents is highly correlated with the increase in resistance of S. pneumoniae to β-lactams and macrolides 7–10 . Differential use of antimicrobial agents may be responsible for some of the observed regional and seasonal differences in the proportions of resistance 11 . The proportions of resistance to various classes of antimicro- bial agents vary substantially both among countries 3,4,12–14 and among regions within countries 5,13–16 . The ABCs, a collabora- tion between the CDC and several health departments and universities participating in the Emerging Infections Program (EIP) network, collects population-based data through active surveillance of invasive pneumococcal infections at 8 sites around the US, covering approximately 21 million people. All of the collected isolates are tested for antimicrobial susceptibil- ity and, since 1998, serotyped 17 . In the US in 1998, the propor- tion of penicillin resistance varied among the ABCs sites from 14.7% in New York State to 35.1% in Tennessee. Similar varia- tion exists in the proportions of isolates resistant to ery- thromycin and in the proportions dually resistant to penicillin and erythromycin (a macrolide). Pneumococci are classified into approximately 90 serotypes, defined by their capsular polysaccharides. Worldwide, resistance to penicillin, ery- thromycin and, to some extent, other antibiotic classes is largely confined to a limited number of serotypes, most no- tably serotypes 6A, 6B, 9V, 14, 19A, 19F and 23F 4,13 . There are at least two possible mechanistic explanations for the observed geographic differences in the proportions of resis- tance. Different geographic sites may have differential selection pressures for resistance (mechanism 1). If such differential selec- Geographic diversity and temporal trends of antimicrobial resistance in Streptococcus pneumoniae in the United States ALTHEA W. MCCORMICK 1 , CYNTHIA G. WHITNEY 2 , MONICA M. FARLEY 3 , RUTH LYNFIELD 4 , LEE H. HARRISON 5 , NANCY M. BENNETT 6 , WILLIAM SCHAFFNER 7 , ARTHUR REINGOLD 8 , JAMES HADLER 9 , PAUL CIESLAK 10 , MATTHEW H. SAMORE 11 & MARC LIPSITCH 1 1 Department of Epidemiology, Harvard School of Public Health, Boston, Massachusetts, USA 2 Active Bacterial Core surveillance and Emerging Infections Program Network, Centers for Disease Control and Prevention, Atlanta, Georgia, USA 3 Emory Department of Medicine, Emory University, Atlanta, Georgia, USA 4 Minnesota Emerging Infections Program, Minnesota Department of Health, Minneapolis, Minnesota, USA 5 Department of International Health, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, USA 6 Monroe County Health Department, Rochester, New York, USA 7 Vanderbilt University School of Medicine, Vanderbilt Medical Center, Nashville, Tennessee, USA 8 School of Public Health, University of California, Berkeley, California, USA 9 Connecticut Emerging Infections Program, Connecticut Department of Public Health, Hartford, Connecticut, USA 10 Oregon Emerging Infections Program, Department of Human Services, Health Services, Office of Disease Prevention and Epidemiology, Portland, Oregon, USA 11 Department of Medicine, University of Utah School of Medicine, Salt Lake City, Utah, USA Correspondence should be addressed to M.L.; e-mail: [email protected] Published online 3 March 2003; doi:10.1038/nm839 Resistance of Streptococcus pneumoniae to antibiotics is increasing throughout the United States, with substantial variation among geographic regions. We show that patterns of geographic variation are best explained by the intensity of selection for resistance, which is reflected by dif- ferences between the proportions of resistance within individual serotypes, rather than by dif- ferences between the frequencies of particular serotypes. Using a mathematical transmission model, we analyzed temporal trends in the proportions of singly and dually resistant organisms and found that pneumococcal strains resistant to both penicillin and erythromycin are increas- ing faster than strains singly resistant to either. Using the model, we predict that by 1 July 2004, in the absence of a vaccine, 41% of pneumococci at the Centers for Disease Control and Prevention (CDC)’s Active Bacterial Core surveillance (ABCs) sites, taken together, will be dually resistant, with 5% resistant to penicillin only and 5% to erythromycin only. © 2003 Nature Publishing Group http://www.nature.com/naturemedicine
Transcript of Geographic diversity and temporal trends of antimicrobial resistance in Streptococcus pneumoniae in...

424 NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003
ARTICLES
Streptococcus pneumoniae is a leading cause of bacteremia, sinusi-tis, otitis media, bacterial meningitis and bacterial pneumoniaworldwide1,2. An increasing prevalence of S. pneumoniae strainsresistant to important anti-pneumococcal drugs, including β-lac-tams and macrolides, has been observed in both developing anddeveloped countries3. In the United States, the proportion ofpenicillin-resistant S. pneumoniae strains increased from 21% oftested isolates in 1995 to 24% in 1998 (ref. 4), and the propor-tion of macrolide-resistant strains increased from 10.6% in 1995to 20.4% in 1999 (refs. 5, 6). Use of antimicrobial agents ishighly correlated with the increase in resistance of S. pneumoniaeto β-lactams and macrolides7–10. Differential use of antimicrobialagents may be responsible for some of the observed regional andseasonal differences in the proportions of resistance11.
The proportions of resistance to various classes of antimicro-bial agents vary substantially both among countries3,4,12–14 andamong regions within countries5,13–16. The ABCs, a collabora-tion between the CDC and several health departments anduniversities participating in the Emerging Infections Program
(EIP) network, collects population-based data through activesurveillance of invasive pneumococcal infections at 8 sitesaround the US, covering approximately 21 million people. Allof the collected isolates are tested for antimicrobial susceptibil-ity and, since 1998, serotyped17. In the US in 1998, the propor-tion of penicillin resistance varied among the ABCs sites from14.7% in New York State to 35.1% in Tennessee. Similar varia-tion exists in the proportions of isolates resistant to ery-thromycin and in the proportions dually resistant to penicillinand erythromycin (a macrolide). Pneumococci are classifiedinto approximately 90 serotypes, defined by their capsularpolysaccharides. Worldwide, resistance to penicillin, ery-thromycin and, to some extent, other antibiotic classes islargely confined to a limited number of serotypes, most no-tably serotypes 6A, 6B, 9V, 14, 19A, 19F and 23F4,13.
There are at least two possible mechanistic explanations forthe observed geographic differences in the proportions of resis-tance. Different geographic sites may have differential selectionpressures for resistance (mechanism 1). If such differential selec-
Geographic diversity and temporal trends of antimicrobialresistance in Streptococcus pneumoniae in the United States
ALTHEA W. MCCORMICK1, CYNTHIA G. WHITNEY2, MONICA M. FARLEY3, RUTH LYNFIELD4, LEE H. HARRISON5, NANCY M. BENNETT6, WILLIAM SCHAFFNER7, ARTHUR REINGOLD8,
JAMES HADLER9, PAUL CIESLAK10, MATTHEW H. SAMORE11 & MARC LIPSITCH1
1Department of Epidemiology, Harvard School of Public Health, Boston, Massachusetts, USA2Active Bacterial Core surveillance and Emerging Infections Program Network,
Centers for Disease Control and Prevention, Atlanta, Georgia, USA3Emory Department of Medicine, Emory University, Atlanta, Georgia, USA
4Minnesota Emerging Infections Program, Minnesota Department of Health, Minneapolis, Minnesota, USA5Department of International Health, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, USA
6Monroe County Health Department, Rochester, New York, USA7Vanderbilt University School of Medicine, Vanderbilt Medical Center, Nashville, Tennessee, USA
8School of Public Health, University of California, Berkeley, California, USA9Connecticut Emerging Infections Program, Connecticut Department of Public Health, Hartford, Connecticut, USA
10Oregon Emerging Infections Program, Department of Human Services, Health Services, Office of Disease Prevention and Epidemiology, Portland, Oregon, USA
11Department of Medicine, University of Utah School of Medicine, Salt Lake City, Utah, USACorrespondence should be addressed to M.L.; e-mail: [email protected]
Published online 3 March 2003; doi:10.1038/nm839
Resistance of Streptococcus pneumoniae to antibiotics is increasing throughout the United States,with substantial variation among geographic regions. We show that patterns of geographicvariation are best explained by the intensity of selection for resistance, which is reflected by dif-ferences between the proportions of resistance within individual serotypes, rather than by dif-ferences between the frequencies of particular serotypes. Using a mathematical transmissionmodel, we analyzed temporal trends in the proportions of singly and dually resistant organismsand found that pneumococcal strains resistant to both penicillin and erythromycin are increas-ing faster than strains singly resistant to either. Using the model, we predict that by 1 July 2004,in the absence of a vaccine, 41% of pneumococci at the Centers for Disease Control andPrevention (CDC)’s Active Bacterial Core surveillance (ABCs) sites, taken together, will be duallyresistant, with 5% resistant to penicillin only and 5% to erythromycin only.
D-nm839.qxd 3/13/03 1:42 PM Page 424
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003 425
ARTICLES
tion were operative, it could have two possible effects on thepneumococcal population: areas of higher selection pressuremight have greater proportions of isolates from serotypes thattend to be resistant (mechanism 1a); or areas of higher selectionpressure might have a greater proportion of resistance withineach serotype although they have serotype distributions similarto those in areas of lower selection pressure (mechanism 1b). Analternative mechanism not involving differential selection pres-sures for resistance is that certain resistant clones of S. pneumo-niae might be widely disseminated in some regions but not inothers (mechanism 2). Worldwide, a small number of multi-re-sistant clones have shown remarkable success, not only in com-petition with drug-sensitive clones, but in competition withother singly and multi-resistant pneumococci18, suggesting thatfactors besides antibiotic resistance may be partly responsible forthe success of these clones.
We sought to distinguish between mechanisms 1 and 2. Ifmechanism 1b were the cause of the geographic variation, thenwe would expect that the proportions of resistance should showconsistent (highly correlated) patterns across different serotypes;areas with high levels of resistance in one serotype should alsohave high levels of resistance in most other serotypes10. By con-trast, if mechanism 2 were operative, such consistency acrossserotypes would not be expected. Each of the defined multi-resistant clones would be restricted to one or a small number ofserotypes18. Therefore, differential success of one or a few multi-resistant clones would result in elevated proportions of resis-tance in one or a few serotypes in those areas where the clonesspread successfully, but not in geographical correlations in theresistant proportions across a large number of serotypes.
We also tested whether geographic variation in the resistantproportions reflects differences in serotype composition (mecha-nism 1a), or variation in the resistant proportions within indi-vidual serotypes (mechanism 1b). First, to test the importance ofgeographic differences in serotype distribution, we statisticallyeliminated these differences by calculating standardized resis-tant proportions for each site, using the population’s averageserotype distribution but each site’s own serotype-specific resis-
tant proportions. If mechanism 1a alone were operative, thisstandardization would remove site-to-site variation in the resis-tant proportions. By contrast, if mechanism 1b alone were oper-ative, the standardized resistant proportions for each site shouldbe the same as the crude resistant proportions for that site, pre-serving site-to-site variation.
Second, we statistically removed site-to-site variation in the re-sistant proportions within each serotype and calculated stan-dardized resistant proportions for each site, using thepopulation’s average resistant proportions within a serotype, buteach site’s own serotype distribution. This standardizationshould have the opposite effect from the previous one, removingdifferences caused by mechanism 1b but preserving differencescaused by mechanism 1a.
Pneumococcal resistance to both β-lactams and macrolides isincreasing in the US4. To understand the reasons for this increaseand to predict future trends, we developed a mathematicalmodel of the transmission of susceptible, singly and dually resis-tant pneumococci. Under assumptions described in theMethods, the model predicts the shape of the curve describingchanges in the prevalence of each of these pneumococcal typesover time. We have fitted this model to subsets of ABCs datafrom 1996 to 1999 and used these fitted curves to predict trendsin resistance from 2000 to 2004.
Geographic variation is consistent across serotypesTo determine whether geographic differences in the proportionsof resistance were replicated across different serotypes, we firstcalculated the proportions resistant to penicillin, erythromycinor both for each of the eight most common serotypes in countiesof eight sites present in the 1998–1999 data set (Table 1). Usingthese values, the Spearman correlation coefficient for each pairof serotypes was calculated to form a correlation matrix. Wefound a significantly positive sum of the correlations observedbetween serotypes by site in the proportions resistant to ery-thromycin (P < 0.001), penicillin (P < 0.01) and both (P < 0.001).The significant association of site with resistant proportions indifferent serotypes supports the hypothesis that differences inselection pressure account for geographic variation in the pro-portions of resistance.
Source of geographic variation in resistant proportionWhen the resistant proportions in each site were standardized toreflect the population’s average serotype composition, standard-ized proportions remained almost identical to crude proportions(Table 2, second column of each section). This pattern was con-sistent when applied to penicillin resistance, erythromycin resis-tance or dual resistance. This indicates that geographicdifferences in serotype composition contribute little to geo-graphic differences in the resistant proportion. On the otherhand, standardized proportions reflecting the population’s aver-age resistant proportions within each serotype showed almostno geographic variation; in other words, removing geographicdifferences in resistant proportions within each serotype re-moved the geographic differences in resistance (Table 2, third
�SXS
�DXD
�PXP
(uS + τP + τE )S
uDD
(uE + τP)E
�E XE
(uP + τE )PX
S
E
D
P
+ τP + τE
E + τP
( + τE
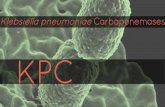
Fig. 1 Model of pneumococcal transmission (described in Methods). X,uncolonized host; S, strains susceptible to both penicillin and erythromycin;P, strains resistant to penicillin only; E, strains resistant to erythromycinonly; D, strains resistant to both penicillin and erythromycin; β, transmis-sion rate constant; u, clearance rate; τP, effective rate of treatment with β-lactam; τE, effective rate of treatment with macrolide.
D-nm839.qxd 3/13/03 1:42 PM Page 425
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

426 NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003
ARTICLES
column of each section). Again, patterns were similar amongpenicillin, erythromycin and dual resistance. These patternswere quantified by the regression of crude and standardized re-sistant proportions (see Methods). Regression slopes for the firststandardization were near one, whereas the slopes for the secondstandardization were near zero and rejected the null hypothesisof no effect (Table 2).
These findings indicate that differential selection pressures invarious geographic areas have resulted in geographic variationin the proportions of resistance, and that this variation is dueprimarily to differences in the resistant proportions in eachserotype. Thus, the findings reject the hypothesis that differen-tial success of a few clones explains differences in resistance, andthey also reject the hypothesis that differential selection pres-sure results in significant shifts in pneumococcal populations to-ward a greater representation of the highly resistant serotypes.
Dynamics of resistance: model predictionsTo characterize temporal trends in resistance, we fit ABCs resis-tance data to a multinomial logistic regression based on a modelof transmission of four classes of pneumococci: susceptible topenicillin and erythromycin, resistant to penicillin only, resis-tant to erythromycin only and dually resistant to penicillin anderythromycin (Fig. 1).
Dynamic patternsOverall penicillin resistance increased from 21.7% in 1996 to26.6% in 1999, and erythromycin resistance increased from10.8% to 20.2%. We hypothesized that strains resistant to bothclasses of antibiotics would increase in frequency faster thanstrains resistant to either class alone. To determine the relativerates of increase of dually and singly resistant strains, we fit thedata to a multinomial logistic regression versus time (Fig. 2),based on the transmission model described in the Methods. Theproportion of strains resistant to penicillin only decreased be-tween 1996 and 1999, with a multinomial coefficient of–0.068/year (95% confidence –0.11 to –0.022), whereas the pro-portion of strains resistant to erythromycin only increased veryslowly, with a coefficient of 0.13/year (95% confidence 0.041 to0.22). Only dually resistant strains increased substantially be-tween 1996 and 1999, with a multinomial coefficient of0.25/year (95% confidence 0.2 to 0.29). These results suggestthat under current usage patterns of antimicrobial agents, strainsresistant to both penicillin and erythromycin have a substantialfitness advantage over singly resistant strains.
Dynamics and predictionsWe extrapolated the multinomial logistic regression to predictthe proportion of penicillin-only, erythromycin-only and dually
Table 1 Percentage of resistant isolates from serotypes 4, 14, 6A, 6B, 9V, 19A, 19F and 23F, at 8 sites.
Penicillin-resistant isolatesNumber of
4 14 6A 6B 9V 19A 19F 23F strainsCalifornia 6.8 18.4 25.0 29.4 22.6 65.0 22.2 19.2 231Connecticut 0.63 27.1 52.5 27.1 67.4 64.1 26.3 36.4 842Georgia 3.8 53.7 57.9 54.8 62.5 45.8 42.4 62.0 1,254Maryland 0.0 15.9 20.4 28.7 44.6 76.3 21.3 41.2 880Minnesota 1.3 30.9 14.0 38.7 69.6 42.4 44.3 32.3 601New York 0.0 14.9 33.3 23.1 55.6 54.6 17.4 27.3 261Oregon 1.9 44.7 20.0 25.0 58.5 60.0 33.3 21.7 270Tennessee 1.1 79.6 24.0 61.9 74.4 84.2 54.1 58.9 507Total 787 1,367 357 532 590 229 432 552 4,846
Erythromycin-resistant isolatesNumber of
4 14 6A 6B 9V 19A 19F 23F strainsCalifornia 0 22.5 10.0 23.5 12.9 10.0 22.2 15.4 231Connecticut 0.63 18.8 45.8 18.8 5.4 15.4 18.8 18.2 842Georgia 6.3 59.0 57.0 47.6 12.5 40.7 36.4 34.7 1,254Maryland 0.73 20.2 3.7 23.2 10.2 13.2 13.8 26.3 880Minnesota 1.3 36.5 10.0 35.5 39.1 9.1 27.9 16.1 601New York 0 14.9 27.8 18.0 3.7 9.1 8.7 0 261Oregon 1.9 17.1 20.0 15.6 39.0 40.0 25.0 8.7 270Tennessee 1.1 81.8 24.0 50.8 15.9 36.8 43.2 14.3 507Total 787 1,367 357 532 590 229 432 552 4,846
Penicillin- and erythromycin-resistant isolatesNumber of
4 14 6A 6B 9V 19A 19F 23F strainsCalifornia 0 12.2 10.0 23.5 12.9 10.0 11.1 11.5 231Connecticut 0 8.7 42.4 15.3 5.4 12.8 17.5 14.1 842Georgia 3.8 50.6 56.2 46.8 11.7 30.5 33.1 32.7 1,254Maryland 0 14.2 3.7 17.6 8.4 13.2 12.5 24.6 880Minnesota 1.3 25.8 8.0 30.7 39.1 6.1 26.2 16.1 601New York 0 10.5 27.8 7.7 3.7 9.1 8.7 0 261Oregon 1.9 13.2 10.0 6.3 39.0 40.0 25.0 4.4 270Tennessee 1.1 78.8 20.0 46.0 13.4 31.6 43.2 10.7 507Total 787 1,367 357 532 590 229 432 552 4,846
D-nm839.qxd 3/13/03 1:42 PM Page 426
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003 427
ARTICLES
Fig. 2 Actual and predicted proportions ofresistance. a–e, Points represent averages fortime periods from 1 January to 31 Decemberof the next year; curves represent fitted multi-nomial logistic regressions. Shown are propor-tions for all counties and all serotypes (a);counties in Georgia (b); counties in Georgiaand only serotypes present in the heptavalentconjugate vaccine (c); counties in Minnesota(d); and counties in Minnesota and onlyserotypes in the heptavalent conjugate vaccine (e). The symbols repre-sent the actual proportion of strains resistant to both erythromycin andpenicillin (�), penicillin only (�) and erythromycin only (�). The lines
resistant strains in the years after 1999 (Fig. 2a). The predictionsshow strains resistant to penicillin only decreasing from 13.7% to5.3%, strains resistant to erythromycin only increasing from2.4% to 4.6% and dually resistant strains increasing from 8.6% to40.6%, from 1 July 1996 to 1 July 2004. These predictions assumethat selective pressures (such as use of antimicrobial agents andvaccination status) remain constant from 1999 onward.
Increasing use of the heptavalent pneumococcal conjugatevaccine (PCV), approved in the US in February 2000, will violateour assumption of constant selection pressures. Because the vac-cine is expected to reduce the incidence of infection with theserotypes included in the vaccine, and because those serotypesare among the types with the highest proportions of resistanceto both β-lactams and macrolides, it is likely that the vaccinewill reduce the frequency of resistant pneumococcal infectionsmore than that of susceptible ones19. Although vaccine use is ex-pected to reduce the proportion of all infections caused by vac-cine-type pneumococci, it should not change the proportion ofresistance within serotypes (except perhaps indirectly by reduc-ing antibiotic use).
To test the model prospectively, we require predictions thatwill hold even if vaccine uptake changes over time. Predictionsof trends in resistance for vaccine serotypes alone should not beaffected by changes in serotype composition resulting from in-creased use of the vaccine. Such predictions were possible onlyfor Georgia and Minnesota, the two sites for which serotype in-formation was available for the full period from 1 January 1996to 31 December 1999 (Fig. 2b–e). For both sites, the proportionsof strains resistant to penicillin only and erythromycin only de-crease between 1996 and 2004 in the vaccine serotypes andacross all serotypes, while the proportions of dually resistantstrains increases.
Geographic variation in temporal trendsIn the static analysis it was evident that there were geographicdifferences in the proportions resistant to each class of antimi-crobials. We sought to determine whether those sites with highproportions of resistance in 1999 were already high in 1996, orwhether resistance increased faster in these sites from 1996 to1999, or both. The proportions of resistance and the rates of in-
00.10.20.30.40.50.60.70.80.91.0
1996
1997
1998
1999
2000
2001
2002
2003
2004
Year
Prop
ortio
n re
sist
anta
00.10.20.30.40.50.60.70.80.91.0
1996
1997
1998
1999
2000
2001
2002
2003
2004
Year
Prop
ortio
n re
sist
antb
00.10.20.30.40.50.60.70.80.91.0
1996
1997
1998
1999
2000
2001
2002
2003
2004
Year
Prop
ortio
n re
sist
antc
00.10.20.30.40.50.60.70.80.91.0
1996
1997
1998
1999
2000
2001
2002
2003
2004
YearPr
opor
tion
resi
stan
td
00.10.20.30.40.50.60.70.80.91.0
1996
1997
1998
1999
2000
2001
2002
2003
2004
Year
Prop
ortio
n re
sist
ante
represent the predicted proportion of strains resistant to both ery-thromycin and penicillin (solid), penicillin only (dashed) and ery-thromycin only (dotted).
Table 2 Crude and standardized proportions resistant to penicillin, erythromycin and both.
Penicillin-resistant Erythromycin-resistant Penicillin- anderythromycin-resistant
State Number Crude Std-1a Std-2b Crude Std-1a Std-2b Crude Std-1a Std-2b
of isolates
California 380 0.14 0.14 0.17 0.082 0.10 0.054 0.058 0.073 0.079Connecticut 1,301 0.21 0.23 0.17 0.11 0.12 0.11 0.076 0.089 0.092Georgia 1,743 0.36 0.33 0.19 0.30 0.26 0.14 0.27 0.23 0.12Maryland 1,254 0.21 0.18 0.20 0.11 0.10 0.12 0.085 0.081 0.098Minnesota 1,032 0.22 0.23 0.17 0.19 0.19 0.13 0.14 0.14 0.11New York 407 0.16 0.18 0.17 0.066 0.076 0.11 0.049 0.060 0.091Oregon 448 0.21 0.23 0.16 0.13 0.13 0.11 0.098 0.10 0.085Tennessee 841 0.36 0.39 0.16 0.26 0.28 0.11 0.23 0.26 0.086Regression slope 0.91 0.041 0.82 0.12 0.84 0.07295% confidence 0.58 to –0.16 to 0.63 to –0.036 to 0.64 to –0.016 tointerval 1.25 0.24 1.02 0.27 1.03 0.16
aStd-1, standardization removing effects of serotype composition. bStd-2, standardization removing site-specific differences in resistant proportion for each serotype. Regressionslopes are for standardized versus crude resistant proportions.
D-nm839.qxd 3/13/03 1:42 PM Page 427
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

428 NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003
ARTICLES
crease in resistance (Table 3) show that most regions with highproportions of resistance in 1999 were already high by 1996, butwere not those with the highest rates of increase in resistanceduring the period, especially for single resistance.
DiscussionResistance in S. pneumoniae has been increasing worldwide, withsome areas developing resistance faster than others. Our analy-ses show that variation in the recent (1998–1999) proportions ofstrains resistant to β-lactams and macrolides, between geo-graphic sites in the US, is best explained by geographic variationin selection pressure for resistance, rather than by clonal dynam-ics. The effect of these selective differences has been primarily tochange the proportions of resistance within individualserotypes, rather than to shift the balance in ‘high-resistance’areas in favor of serotypes in which high proportions of isolatesare resistant.
These inferences have been made without regionally and tem-porally specific data on the use of antimicrobial agents. Suchdata would be valuable in determining the extent to which thegeographic differences in the rate of increase of resistance in theUS are correlated with antimicrobial use. Nevertheless, ourtestable predictions, which distinguish between mechanisms forgeographic differences in resistance, provide evidence that site-to-site differences in the proportions of resistant strains arelargely attributable to regional differences in the selective pres-sures favoring those strains. Besides antimicrobial agents, otherfactors that may be causing these differences include day care at-
tendance, prevalence of immunodeficiencies, and other risk fac-tors for resistance20.
We expected that strains of pneumococci resistant to morethan one widely used drug would be increasing at a faster ratethan singly resistant strains, because they would be unaffectedby treatment with a wider variety of antibiotics. This predictionwas confirmed in the case of penicillin and erythromycin resis-tance; dually resistant strains are increasing much faster thanstrains resistant to either drug alone. Resistance to erythromycinis increasing among both penicillin-susceptible and penicillin-resistant strains of pneumococci. However, the rate of this in-crease is much faster among penicillin-resistant pneumococci.Resistance to penicillin is increasing only among erythromycin-resistant strains and is decreasing among erythromycin-suscepti-ble strains.
We used a simple model of transmission of susceptible, singlyresistant and dually resistant pneumococci21 to predict the shapeof the curves describing the changes in frequencies of each ofthese types over time. We fit ABCs data to a multinomial logisticregression, based on the model. We then extrapolated the pro-portions of resistance of the different classes out to 2004, usingthe model, for the pneumococcal population as a whole and forserotypes included in the heptavalent conjugate vaccine. We pre-dict that by 1 July 2004, 41% of pneumococci, in all ABCs sitestaken together, will be dually resistant, with 5% resistant to peni-cillin only and 5% to erythromycin only. For Georgia andMinnesota, two sites for which long-term serotype data wereavailable, we considered resistance only in those serotypes in-
Table 3 Changes in resistance over time, by site.
State Percent penicillin-resistant (rank)a Rate of increase in resistance(95% confidence interval) (rank)a
1 Jan–31 Dec 1996 1 Jan–31 Dec 1999California 7.2 (7) 7.0 (7) –0.052 (–0.28 to 0.17) (4)Connecticut 14.1 (3) 14.0 (1) 0.027 (–0.071 to 0.12) (3)Georgia 18.1 (2) 9.5 (4) –0.20 (–0.30 to –0.10) (7)Maryland 11.1 (4) 10.5 (2) 0.13 (–0.091 to 0.12) (1)Minnesota 9.0 (6) 7.3 (6) –0.056 (–0.19 to 0.080) (5)Oregon 9.6 (5) 9.0 (5) 0.051 (–0.14 to 0.24) (2)Tennessee 18.3 (1) 10.4 (3) –0.17 (–0.30 to –0.036) (6)
State Percent erythromycin-resistant (rank)a Rate of increase in resistancea
(95% confidence interval) (rank)a
1 Jan–31 Dec 1996 1 Jan–31 Dec 1999California 5.5 (1) 2.5 (6) –0.28 (–0.64 to 0.074) (7)Connecticut 1.8 (5) 4.8 (2) 0.33 (0.11 to 0.54) (2)Georgia 4.0 (3) 3.4 (4) 0.023 (–0.15 to 0.20) (5)Maryland 1.0 (6) 2.4 (7) 0.19 (–0.056 to 0.44) (3)Minnesota 4.0 (2) 5.3 (1) 0.18 (–0.015 to 0.38) (4)Oregon 0.5 (7) 3.6 (3) 0.40 (–0.033 to 0.84) (1)Tennessee 2.9 (4) 2.8 (5) –0.018 (–0.30 to 0.26) (6)
State Percent penicillin- and Rate of increase in resistanceerythromycin-resistant (rank)a (95% confidence interval) (rank)a
1 Jan–31 Dec 1996 1 Jan–31 Dec 1999California 4.4 (4) 6.0 (7) 0.15 (–0.13 to 0.43) (6)Connecticut 3.4 (7) 10.1(5) 0.38 (0.23 to 0.53) (1)Georgia 16.7 (2) 28.1 (1) 0.21 (0.13 to 0.29) (5)Maryland 4.0 (6) 8.3 (6) 0.24 (0.10 to 0.39) (4)Minnesota 5.2 (3) 16.5 (3) 0.36 (0.23 to 0.49) (3)Oregon 4.3 (5) 13.0 (4) 0.38 (0.14 to 0.61) (2)Tennessee 16.7 (1) 26.2 (2) 0.13 (0.014 to 0.24) (7)aRank of 1 = most resistance or largest rate of increase in resistance
D-nm839.qxd 3/13/03 1:42 PM Page 428
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003 429
ARTICLES
cluded in the vaccine. By 1 July 2004, we predict that in Georgia,65% of the vaccine-type pneumococci will be dually resistant(Georgia overall, 55% dually resistant), and that in Minnesota67% of the strains included in the vaccine will be dually resistant(Minnesota overall, 53% dually resistant). We did not considerthe possibility of penicillin- or erythromycin-resistant strainsconverting to dual resistance because acquisition of resistance bya strain is rare relative to transmission of dually resistant strains22.
The method for generating these predictions has the impor-tant strength of being based on a mechanistic (transmission-dynamic) model. However, it also has several limitations.Ideally, one would like to estimate parameters of the underly-ing transmission model (such as use of antimicrobial agents,duration of colonization with pneumococci and differences intransmissibility between susceptible and resistant strains) inde-pendently, and use these estimates to predict changes in theproportions of resistant pneumococci. This was not possiblebecause geographically specific antimicrobial use data were notavailable, nor were independent estimates of the effects of var-ious types of resistance on pneumococcal fitness (transmissibil-ity)23. Instead, the functional form (multinomial logisticregression with time as a co-variate) was specified by the trans-mission model, and the parameters for that function were ob-tained by curve fitting. The following assumptions are requiredto obtain the predicted functional form. (i) Selective pressurefor each type of resistance remains constant over time; selec-tive pressure is determined by use of antimicrobial agents andthe fitness cost of resistance. (ii) Different pneumococcalstrains are interchangeable; in other words, the only factor in-fluencing a strain’s expected prevalence in a given year is its re-sistance pattern. (iii) The model is designed for carriedpneumococci, whereas our data set (as with nearly all largepneumococcal data sets) includes only pneumococci causinginvasive disease. Strictly, therefore, the model should only bepredictive of disease isolates if the disease strains are randomlysampled from the carriage population. Although these assump-tions, like any modeling assumptions, are only approximationsof reality, the limited data that are available are consistent withassumption (i). Data from the CDC’s National (Hospital)Ambulatory Medical Care Survey show that β-lactam andmacrolide use remained nearly stable in the US from 1996 to199924–26. Data collected over the coming years will tell howstrongly departures from the remaining assumptions influencethe predictive validity of the model.
An improved understanding of the factors responsible for geographic variations in resistance patterns will help in the de-sign and evaluation of measures to slow the increase in resis-tance to clinically important antibiotics. Predictions of trendsin resistance serve several purposes. They may be used in plan-ning, to estimate the lifespan of existing drugs. They may serveas a baseline for evaluating interventions, such as vaccinationor changes in antimicrobial use, that are expected to reduce therate of increase of resistance and (optimistically) to reduce theabsolute proportions of resistance in the pneumococcal popula-tion. Predictions that can be tested with prospective data serveas a means of testing the adequacy of our understanding (as for-malized in a model) of the reasons for the current rate of in-crease of resistance. Further progress will require integration ofindependent estimates of model parameters, especially region-ally specific antibiotic use, into the predictions.
Our findings indicate that geographic differences in selectionpressures between sites in the United States are responsible for
significant differences in the proportions of resistance to twomajor classes of antibiotics, and that rapid increases in the pro-portions of resistance (and especially multiple resistance) areexpected to continue. We hope that the conjugate vaccine forchildren will reverse this trend and that better vaccines foradults will soon be available. These findings underline the ur-gency of limiting the unnecessary use of antimicrobial agentsand of finding new agents that will be effective against multi-re-sistant strains.
MethodsData. We analyzed invasive pneumococcal isolates from the ABCs27 col-lection, collected by active population-based surveillance at sites in theUnited States between 1996 and 1999. For each analysis, we includedonly isolates from counties under surveillance for the entire time frameconsidered. Intermediate and highly resistant strains (penicillin mini-mum inhibitory concentration ≥0.12 µg/ml; erythromycin minimum in-hibitory concentration ≥0.5 µg/ml)28 were grouped as resistant andconsidered together.
Statics. To determine whether sites with high proportions of resistancewere consistently high across all serotypes, we calculated Spearman rankcorrelation coefficients for the resistant proportions by site, for each pairof serotypes from the eight most common serotypes in the collection,producing a symmetric 8 × 8 matrix of correlation coefficients C. Eachrow and column corresponds to a serotype, and each entry cij representsthe correlation by site between the resistant proportions of serotypes iand j. Nonrandom overall correlation was assessed by permutation testsusing the sum of C as a test statistic. In this permutation test, the null dis-tribution of the sum of C was approximated by computing test statisticsfor 1,000 matrices, obtained by permuting the resistant proportions ofeach serotype randomly by site. This analysis included 7,406 isolates from1998 and 1999, the years for which all sites had serotype data.
For the same 2-year interval, we analyzed by standardization the effectsof serotype composition and resistant proportions within serotypes ongeographic differences in the proportions of resistance. Crude resistantproportions were calculated for each geographic site, and 2 differentmethods were used to calculate the standardized values for each of thesesites, using the following formula:
where Ri is the standardized resistant proportion for site i. For the stan-dardization to remove the effects of serotype composition, pj is the pop-ulation’s proportion of isolates that are serotype j, and rij is the resistantproportion among isolates of serotype j at site i. For the standardizationto remove the site-specific differences in the resistant proportion ofeach serotype, pj is the population’s resistant proportion among isolatesof serotype j, and rij is the proportion of isolates from site i that areserotype j.
We used inverse-variance weighted linear regression to examine the re-lationship between the standardized and crude resistant proportions foreach geographic area. The slope of this regression should be 1 if the stan-dardizing factor has no effect on geographic differences in the propor-tions of resistance, and 0 if the standardizing factor is completelyresponsible for the differences. Intermediate regression slopes indicatethat some, but not all, of the inter-site variations in resistance are ex-plained by the standardizing factor.
Dynamics. To analyze changes in resistance over time, we generalized apreviously published mathematical model of competition between resis-tant and susceptible strains of S. pneumoniae in a closed host popula-tion21. The state variables in the model represent the frequencies of 5types of hosts: uncolonized (X) or colonized with a strain that is suscepti-ble to both penicillin and erythromycin (S), penicillin-resistant (P), ery-thromycin-resistant (E) or resistant to both penicillin and erythromycin(D). Parameter subscripts follow the same convention. The model as-sumes that each individual can only carry one strain at a given time. The
Ri = Σ pj rijj
D-nm839.qxd 3/13/03 1:42 PM Page 429
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

430 NATURE MEDICINE • VOLUME 9 • NUMBER 4 • APRIL 2003
ARTICLES
following differential equations describe the rates, with respect to time, atwhich individuals move between states:
βi represents the transmission rate constant and ui the clearance rate.This model also considers that an individual can be treated with a β-lactamat an ‘effective rate’ (incidence of treatment with each antibiotic × proba-bility that such treatment clears colonization with pneumococci susceptibleto that antibiotic) of τP, or a macrolide at an effective rate of τE.
Assuming that X stays approximately constant over time, this model pre-dicts that the changes in the proportion of S (the reference group), P, E andD can be described by a multinomial logistic regression, with the 4 strainsas the outcomes and time as a co-variate. We calculated the rates of in-crease of P, E or D compared with S, using 12,989 isolates, for counties withdata from 1 January 1996 to 31 December 1999. Rates of increase de-scribed in the text represent the coefficient of time in this regression foreach strain relative to S; because of the properties of multinomial regres-sion, the sign of this coefficient need not be the same as the sign of thechange in frequency of the corresponding strain. Assuming that the rate ofincrease will remain constant, the regression predicted the future propor-tion of resistance for each group and determined whether dually resistantstrains were more successful than singly resistant strains. A multinomial lo-gistic regression stratified by site was performed to determine whether siteswith the greatest prevalence of resistance in 1996 had rates of increase inresistance that were faster or slower than those sites that had smaller pro-portions of resistance in 1996.
AcknowledgmentsThis work was supported by a National Institutes of Health grant AI48935 toM.L. and by an Ellison Foundation New Scholar Award in Global InfectiousDiseases to M.L. We thank S. McCoy and E. Zell for compiling antimicrobialuse data and J. Robins for helpful suggestions.
Competing interests statementThe authors declare that they have no competing financial interests.
RECEIVED 7 OCTOBER 2002; ACCEPTED 24 JANUARY 2003
1. Hausdorff, W.P., Bryant, J., Paradiso, P.R. & Siber, G.R. Which pneumococcalserogroups cause the most invasive disease: implications for conjugate vaccine for-mulation and use, part I. Clin. Infect. Dis. 30, 100–121 (2000).
2. Prevention of pneumococcal disease: recommendations of the Advisory Committeeon Immunization Practices (ACIP). MMWR Recomm. Rep. 46, 1–24 (1997).
3. Baquero, F. Pneumococcal resistance to β-lactam antibiotics: a global geographic
overview. Microb. Drug Resist. 1, 115–20 (1995).4. Whitney, C.G. et al. Increasing prevalence of multidrug-resistant Streptococcus pneu-
moniae in the United States. N. Engl. J. Med. 343, 1917–1924 (2000).5. Geographic variation in penicillin resistance in Streptococcus pneumoniae—selected
sites, United States, 1997. MMWR Morb. Mortal. Wkly Rep. 48, 656–661 (1999).6. Hyde, T.B. et al. Macrolide resistance among invasive Streptococcus pneumoniae iso-
lates. JAMA 286, 1857–1862 (2001).7. Garcia-Rey, C., Aguilar, L., Baquero, F., Casal, J. & Dal-Re, R. Importance of local vari-
ations in antibiotic consumption and geographical differences of erythromycin andpenicillin resistance in Streptococcus pneumoniae. J. Clin. Microbiol. 40, 159–164(2002).
8. Diekema, D.J., Brueggemann, A.B. & Doern, G.V. Antimicrobial-drug use andchanges in resistance in Streptococcus pneumoniae. Emerg. Infect. Dis. 6, 552–556(2000).
9. Doern, G. Antimicrobial use and the emergence of antimicrobial resistance withStreptococcus pneumoniae in the United States. Clin. Infect. Dis. 33 (suppl. 3),S187–S192 (2001).
10. Jones, M. Relationship between antibiotic resistance in Streptococcus pneumoniaeand that in Haemophilus influenzae: evidence for common selective pressure.Antimicrob. Agents Chemother. 46, 3106–3107 (2002).
11. McEllistrem, M. et al. Distribution of penicillin-nonsusceptible pneumococcal clonesin the Baltimore metropolitan area and variables associated with drug resistance.Clin. Infect. Dis. 34, 704–707 (2002).
12. Scott, J.A. et al. Serotype distribution and prevalence of resistance to benzylpenicillinin three representative populations of Streptococcus pneumoniae isolates from thecoast of Kenya. Clin. Infect. Dis. 27, 1442–1450 (1998).
13. Fenoll, A., Jado, I., Vicioso, D., Perez, A. & Casal, J. Evolution of Streptococcus pneu-moniae serotypes and antibiotic resistance in Spain: update (1990 to 1996). J. Clin.Microbiol. 36, 3447–3454 (1998).
14. Pihlajamaki, M. et al. Macrolide-resistant Streptococcus pneumoniae and use of an-timicrobial agents. Clin. Infect. Dis. 33, 483–488 (2001).
15. Arason, V.A. et al. Do antimicrobials increase the carriage rate of penicillin resistantpneumococci in children? Cross sectional prevalence study. BMJ 313, 387–391(1996).
16. de Neeling, A.J., Overbeek, B.P., Horrevorts, A.M., Ligtvoet, E.E. & Goettsch, W.G.Antibiotic use and resistance of Streptococcus pneumoniae in the Netherlands duringthe period 1994-1999. J. Antimicrob. Chemother. 48, 441–444 (2001).
17. Schuchat, A. et al. Active Bacterial Core surveillance of the Emerging InfectionsProgram Network. Emerg. Infect. Dis. 7, 92–99 (2001).
18. McGee, L. et al. Nomenclature of major antimicrobial-resistant clones ofStreptococcus pneumoniae defined by the Pneumococcal Molecular EpidemiologyNetwork. J. Clin. Microbiol. 39, 2565–2571 (2001).
19. Black, S. et al. Efficacy, safety and immunogenicity of heptavalent pneumococcalconjugate vaccine in children. Northern California Kaiser Permanente Vaccine StudyCenter Group. Pediatr. Infect. Dis. J. 19, 187–195 (2000).
20. Schrag, S.J., Beall, B. & Dowell, S.F. Limiting the spread of resistant pneumococci:biological and epidemiologic evidence for the effectiveness of alternative interven-tions. Clin. Microbiol. Rev. 13, 588–601 (2000).
21. Lipsitch, M. The rise and fall of antimicrobial resistance. Trends Microbiol. 9, 438–444(2001).
22. Lipsitch, M. Interpreting results from trials of pneumococcal conjugate vaccines: astatistical test for detecting vaccine-induced increases in carriage of nonvaccineserotypes. Am. J. Epidemiol. 154, 85–92 (2001).
23. Andersson, D.I. & Levin, B.R. The biological cost of antibiotic resistance. Curr. Opin.Microbiol. 2, 489–493 (1999).
24. National Ambulatory Medical Care Survey: 1993-1999 Summary. (National Centerfor Health Statistics, Centers for Disease Control and Prevention Hyattsville,Maryland, 2001).
25. National Hospital Ambulatory Medical Care Survey: 1993-1999 OutpatientDepartment Summary. (National Center for Health Statistics, Centers for DiseaseControl and Prevention, Hyattsville, Maryland, 2001).
26. National Hospital Ambulatory Medical Care Survey: 1993-1999 EmergencyDepartment Summary (National Center for Health Statistics, Centers for DiseaseControl and Prevention, Hyattsville, Maryland, 2001).
27. Robinson, K.A. et al. Epidemiology of invasive Streptococcus pneumoniae infections inthe United States, 1995-1998: opportunities for prevention in the conjugate vaccineera. JAMA 285, 1729–1735 (2001).
28. Methods for dilution of antimicrobial susceptibility tests for bacteria that grow aero-bically. Approved Standard NCCLS Document M7-A5 (National Committee forClinical Laboratory Standards, Wayne, Pennsylvania, 2000).
dXdt
= – �sXS + (us + τE + τp)S – �PXP + (uP + τE)P – �EXE + (uE + τp)E
– �DXD + uDD
dSdt
= �sXS – (us + τE + τp)S
dPdt
= �PXP – (uP + τE)P
dEdt
= �EXE – (uE + τp)E
dDdt
= �DXD – uDD
D-nm839.qxd 3/13/03 1:42 PM Page 430
©20
03 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine







![ο υπέροχος κόσμος του National geographic [66]](https://static.fdocument.org/doc/165x107/55b84ee9bb61eb5b488b47dc/-national-geographic-66.jpg)
![ο υπέροχος κόσμος του National geographic [65]](https://static.fdocument.org/doc/165x107/55b84fc3bb61ebc5028b458f/-national-geographic-65.jpg)