Frequent β-catenin gene mutations in atypical polypoid adenomyoma of the uterus
8
Original contribution Frequent β-catenin gene mutations in atypical polypoid adenomyoma of the uterus ☆,☆☆ Hiroyuki Takahashi MD, PhD a , Tsutomu Yoshida MD, PhD a , Toshihide Matsumoto PhD a , Yoichi Kameda MD, PhD b , Yasuo Takano MD, PhD b , Yuki Tazo MD a , Hisako Inoue MD a , Makoto Saegusa MD, PhD a, ⁎ a Department of Pathology, Kitasato University School of Medicine, 1-15-1 Kitasato, Minami-ku, Sagamihara, Kanagawa 252-0374, Japan b Pathology Section, Kanagawa Cancer Center Research Institute, 1-1-2, Nakao, Asahi-ku, Yokohama 241-0815, Japan Received 22 April 2013; revised 3 June 2013; accepted 6 June 2013 Keywords: APA; β-Catenin; α-SMA; CD10; Cyclin D1; p21 waf1 Summary Atypical polypoid adenomyoma (APA) is an uncommon polypoid lesion of the uterus. To clarify the mechanism of its histogenesis, we examined the functional role of β-catenin, with reference to expression of p21 waf1 , cyclin D1, cyclin E, CD10, and α–smooth muscle actin (SMA), as well as cell proliferation, in 7 lesions. In the epithelial components, expression of nuclear β-catenin, p21 waf1 , and cyclin D1 was increased in a stepwise fashion from normal tissue through complex atypical hyperplasia and adenomyoma to APA lesions, particularly in squamous morular areas, whereas cell proliferation, as well as cyclin E expression, was significantly decreased in the latter. Similar findings were evident in the stromal lesions, with the exception of a case of nuclear β-catenin. In addition, coexpression of CD10 and α-SMA markers was observed in the stromal components in 3 APA cases, in line with the results of normal secretory endometrial and adenomyoma samples, suggesting that cells progress to myofibromatous cells in response to differentiation-promoting events. Finally, β-catenin gene (CTNNB1) mutations were detected in all APA cases, the single nucleotide substitutions being in the epithelial but not the stromal components. These findings suggest that activation of β-catenin signaling, probably secondary to the gene abnormalities, plays an important role in the formation of the complex epithelial architecture in APAs, leading to inhibition of cell proliferation through overexpression of p21 waf1 . In contrast, changes in the stromal cell phenotype may occur through a shift from CD10 to α- SMA immunopositivity, independent of CTNNB1 status. © 2014 Elsevier Inc. All rights reserved. 1. Introduction Atypical polypoid adenomyoma (APA), an uncommon focal and polypoid lesion of the uterus, is characterized by irregular structures of cytologically atypical endometrial epithelial components with squamous morula formation and prominent cellular smooth muscle stromal components [1,2]. Most patients with APAs are of reproductive age, nulliparous, ☆ Funding: This study was supported by a grant from the Ministry of Education, Culture, Sports, Science and Technology of Japan (Tokyo) (20590352). ☆☆ Conflict of interest: The authors declare no conflicts of interest. ⁎ Corresponding author. Department of Pathology, Kitasato University School of Medicine, 1-15-1 Kitasato, Minami-ku, Sagamihara, Kanagawa 252-0374, Japan. E-mail address: [email protected] (M. Saegusa). www.elsevier.com/locate/humpath 0046-8177/$ – see front matter © 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.humpath.2013.06.020 Human Pathology (2014) 45, 33–40
Transcript of Frequent β-catenin gene mutations in atypical polypoid adenomyoma of the uterus

www.elsevier.com/locate/humpath
Human Pathology (2014) 45, 33–40
Original contribution
Frequent β-catenin gene mutations in atypical polypoidadenomyoma of the uterus☆,☆☆
Hiroyuki Takahashi MD, PhDa, Tsutomu Yoshida MD, PhDa,Toshihide Matsumoto PhDa, Yoichi Kameda MD, PhDb, Yasuo Takano MD, PhDb,Yuki Tazo MDa, Hisako Inoue MDa, Makoto Saegusa MD, PhDa,⁎
aDepartment of Pathology, Kitasato University School of Medicine, 1-15-1 Kitasato, Minami-ku, Sagamihara,Kanagawa 252-0374, JapanbPathology Section, Kanagawa Cancer Center Research Institute, 1-1-2, Nakao, Asahi-ku, Yokohama 241-0815, Japan
Received 22 April 2013; revised 3 June 2013; accepted 6 June 2013
E(2
S2
0h
Keywords:APA;β-Catenin;α-SMA;CD10;Cyclin D1;p21waf1
Summary Atypical polypoid adenomyoma (APA) is an uncommon polypoid lesion of the uterus. Toclarify the mechanism of its histogenesis, we examined the functional role of β-catenin, with referenceto expression of p21waf1, cyclin D1, cyclin E, CD10, and α–smooth muscle actin (SMA), as well as cellproliferation, in 7 lesions. In the epithelial components, expression of nuclear β-catenin, p21waf1, andcyclin D1 was increased in a stepwise fashion from normal tissue through complex atypical hyperplasiaand adenomyoma to APA lesions, particularly in squamous morular areas, whereas cell proliferation, aswell as cyclin E expression, was significantly decreased in the latter. Similar findings were evident inthe stromal lesions, with the exception of a case of nuclear β-catenin. In addition, coexpression of CD10and α-SMA markers was observed in the stromal components in 3 APA cases, in line with the results ofnormal secretory endometrial and adenomyoma samples, suggesting that cells progress tomyofibromatous cells in response to differentiation-promoting events. Finally, β-catenin gene(CTNNB1) mutations were detected in all APA cases, the single nucleotide substitutions being in theepithelial but not the stromal components. These findings suggest that activation of β-catenin signaling,probably secondary to the gene abnormalities, plays an important role in the formation of the complexepithelial architecture in APAs, leading to inhibition of cell proliferation through overexpression ofp21waf1. In contrast, changes in the stromal cell phenotype may occur through a shift from CD10 to α-SMA immunopositivity, independent of CTNNB1 status.© 2014 Elsevier Inc. All rights reserved.
☆ Funding: This study was supported by a grant from the Ministry ofducation, Culture, Sports, Science and Technology of Japan (Tokyo)0590352).☆☆ Conflict of interest: The authors declare no conflicts of interest.⁎ Corresponding author. Department of Pathology, Kitasato University
chool of Medicine, 1-15-1 Kitasato, Minami-ku, Sagamihara, Kanagawa52-0374, Japan.E-mail address: [email protected] (M. Saegusa).
046-8177/$ – see front matter © 2014 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.humpath.2013.06.020
1. Introduction
Atypical polypoid adenomyoma (APA), an uncommonfocal and polypoid lesion of the uterus, is characterized byirregular structures of cytologically atypical endometrialepithelial components with squamous morula formation andprominent cellular smooth muscle stromal components [1,2].Most patients with APAs are of reproductive age, nulliparous,

Table
Clin
icop
athlog
ical
find
ings
in7APAs,2AMs,10
CAHs,and11
norm
alendo
metrium
samples
Case
Age
(y)
Treatment
Morule
CTNNB1
Nu-β-cateninLIs
p21
waf1LIs
Cyclin
D1LIs
Cycin
ELIs
Ki-67
LIs
CD10
+
Nucleotides
Amino
acid
Epithelium
Strom
aEpithelium
Strom
aEpithelium
Strom
aEpithelium
Strom
aEpithelium
Strom
aStrom
a⁎
Gla
Mo
Gla
Mo
Gla
Mo
Gla
Mo
Gla
Mo
APA-1
34Curettage
+TCT37
TTT
Ser→
Phe
839
.45.4
1.1
41.5
3642
.735
.936
.21.7
2.8
00.8
1.1
1.5
+APA-2
40Curettage
+TCT37
TGT
Ser→
Cys
10.4
48.8
5.8
1.5
28.8
17.5
3066
.935
.30.8
0.3
017
.51.2
2.4
−APA-3
43Hysterectom
y+
TCT33
TGT
Ser→
Cys
547
.94.9
0.7
2.5
3236
.676
.19.1
10
0.3
201.8
1.5
+APA-4
44Curettage
+TCT37
GCT
Ser→
Ala
55.3
61.3
13.2
1.9
1.3
7.6
19.9
36.7
30.3
6.1
*0
9.5
0.8
1.6
+APA-5
38Curettage
+TCT33
TTT
Ser→
Phe
12.2
57.5
3.8
1940
.351
.481
.862
.538
.1*
**
29.7
1.1
3.1
−APA-6
37Curettage
+GAC32
CAC
Asp→
His
1319
5.8
18.8
*25
5036
.418
.12.5
*0.9
302.8
1.5
−APA-7
46Hysterectom
y+
GAC32
TAC
Asp→
Tyr
10.5
16.1
1.4
9.5
55.6
0.6
17.2
54.4
1.7
9.6
40.2
010
.75
2.6
−AM-1
42Polyp
ectomy
−Wild
0*
1.1
2.8
*8.1
15.2
*8.6
22.1
*0.3
3.2
*0
+AM-2
34Polyp
ectomy
−Wild
8.3
*0
0.8
*4.1
10.7
*17
.26.5
*0
1.8
*0
+CAH
(n=10
)44
.6±
7.0
Curettage
−Wild
8.5±
5.9
*4.9±
3.5
7.4±
7.7
*1.6±
1.8
14.6
±10
.8*
5.2±
5.9
27.8
±27
.9*
0.5±
0.6
31.7
±23
.9*
10.8
±12
.6+
Normal
(P)
(n=11
)41
±9.1
Biopsy
−NE
5.8±
1.9
*3.3±
2.2
6.1±
8.3
*1.6±
1.0
20.1
±8.5
*10
.4±
8.8
11.8
±12
.1*
3.7±
3.2
36.8
±13
.6*
34.2
±19
.1+
Abb
reviations:CAH,complex
atyp
ical
hyperplasia;
NE,no
tevaluable;
Nu,
nuclear;*,
morethan
50%
CD10
-positive
cells
instromal
lesion
;no
rmal
(P),no
rmal
proliferativeendo
thelium.
34 H. Takahashi et al.
and premenopausal, with an age range of 21 to 53 years(median, 39.7 years) [2,3]. The lesions frequently developin the lower uterine segments [2,4]. In some cases,curettage samples obtained from the lesions may beresponsible for misidentification as an invasive carcinomabecause of the presence of dense proliferation of smoothmuscle cells [2].
Previous studies have demonstrated conflicting resultsregarding the biological behavior of APAs. For example, areview of 136 APA cases indicated that 30% had residual orrecurrent tumors after local excision by curettage and that therisk of coexistent endometrial hyperplasia or carcinoma wasapproximately 9%, indicating a potentially high risk ofmalignant disease [5]. In contrast, others have found that thelesions appeared to be histologically and biologically benign,as suggested by DNA ploidy studies and Ki-67 immunohis-tochemical staining [4,6]. Interestingly, several riskfactors for APAs, including obesity, hormone replacementtherapy, and prolonged estrogenic stimulation, arecommon to patients with endometrial hyperplasia andcarcinoma [2,7], indicating the possibility of coexistence ofthese lesions [8-10].
β-Catenin is a multifunctional protein involved inE-cadherin–mediated cell-cell adhesion, acting as a down-stream effector in the Wnt signaling pathway [11-13]. Wepreviously demonstrated that mutations in exon 3 of thegene were frequent in endometrial carcinomas withsquamous morular differentiation, suggesting that thenuclear accumulation is an initial signal for an inductionof the process, leading to inhibition of cell proliferationthrough overexpression of p21waf1 [14-16]. Given that thetrans-differentiation toward the squamous morular pheno-type is common in APAs [2], we hypothesized a role for β-catenin signaling in its histogenesis. To test this idea, weinvestigated alterations in β-catenin status with reference toexpression of several cell cycle– and stromal-relatedmolecules and cell proliferation in APAs, as well asnormal, complex atypical hyperplasia (CAH) and adeno-myoma (AM) lesions.
2. Materials and methods
2.1. Cases
We reviewed uterine tumor samples obtained by curettageor hysterectomy from the patient records of KitasatoUniversity Hospital and Kanagawa Cancer Center Hospitalbetween 1990 and 2012. According to the criteria describedby Longacre et al [2], tumors were designated as APAs ifthey featured localized polypoid proliferation of irregularglands with various degrees of squamous morular differen-tiation and cellular smooth muscle or hybrid smooth muscle/fibrous stroma. In curettage samples, we used CD10immunoreactivity patterns to distinguish APAs from

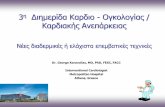
Fig. 1 Serial sections of APA. Hematoxylin and eosin (HE) staining and IHC for β-catenin, p21waf1, cyclin D1, cyclin E, Ki-67, CD10, andα-SMA. Boxes with solid outlines enclose both squamous morules (arrows in H&E panel) and stromal lesions and are magnifiedin lower panels. Note focal Ki-67 immunoreactivity in glandular components (arrow). Original magnifications ×100 (upper panels);×400 (lower panels).
35CTNNB1 mutations in APA
myoinvasive endometrioid carcinomas, as described byOhishi and colleagues [17], referred for clinical examinationssuch as imaging studies. Briefly, CD10-positive stromal cellsimmediately surrounding the irregular glands (fringelikestaining pattern) were frequently evident in myoinvasiveendometrioid carcinoma; but such findings were relativelyrare in APAs. Finally, a total of 7 APA cases were selectedfor this study. In addition, 19 biopsy samples of normalendometrial tissue (11 in the proliferative and 8 in the latesecretory phase), 10 curettage samples of CAH withoutsquamous morules, and 2 polypectomy specimens of AMswere investigated (Table 1). All tissues were routinely fixedin 10% formalin and embedded in paraffin.
This study was approved by the Kitasato UniversityMedical Ethics Committee (B12-95).
2.2. Immunohistochemistry staining
Immunohistochemistry (IHC) examination was per-formed using a combination of microwave-oven heatingand polymer immunocomplex (Envision; DAKO, Copenha-gen, Denmark) methods, as described previously [14-16].Antibodies to β-catenin (clone 14; BD Bioscience, San Jose,CA), α-SMA (clone 1A4; DAKO), CD10 (clone 56C6;Leica Microsystems, Wetzlar, Germany), Ki-67 (MIB-1;DAKO), cyclin D1 (SP4; DAKO), cyclin E (HE12; BDBioscience), and p21waf1 (SX118; DAKO) were used.
For evaluation of IHC results, tumor lesions weresubdivided into glandular and stromal components. Todetermine labeling indices (LIs) for nuclear β-catenin,
p21waf1, cyclin D1, cyclin E, and Ki-67, immunopositivenuclei were counted in at least 500 cells in 3 randomlyselected fields in each of the 2 phenotypes, as describedpreviously [15]. The LI values for cytoplasmic α-SMAimmunopositivity in normal endometrial stromal cellswere examined in a similar manner. In addition, caseswere defined as positive for CD10 immunostaining when50% of the stroma lesions in APAs were stained ineach section.
2.3. Mutation analysis of CTNNB1 gene
Six serial 10-μm paraffin-wax sections were reviewedmicroscopically; and areas with tumor lesions weremicrodissected, carefully avoiding contamination withnon-APA tissue. Tumor areas containing epithelial andstromal components were microdissected separately in 3APA cases. Genomic DNA was extracted using aQIAamp DNA FFPE Tissue Kit (Qiagen, Tokyo,Japan). A 148–base pair fragment of exon 3 of the β-catenin gene (CTNNB1) was amplified by heminestedpolymerase chain reactions using the following primers:common forward, 5′-ATTTGATGGAGTTGGACATGG-3′; outer reverse, 5′-TGTTCTTGAGTGAAGGACTGA-3′;and inner reverse, 5′-TCTTCCTCAGGATTGCCTT-3′.Water was used instead of template DNA as a negativecontrol for each examination. The polymerase chainreaction products were sequenced using BigDye Termi-nators v1.1 Cycle Sequencing Kit (Life TechnologiesJapan, Tokyo, Japan) and analyzed with an ABI PRISM

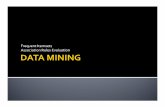
Fig. 2 Nuclear LIs for several markers investigated in epithelial (A) and stromal (B) components of APAs. Data are shown as means ±SDs. Nu, nuclear; P, normal proliferative endometrium; H, complex atypical hyperplasia; Gla, glandular components; Mo, squamousmorular lesions.
36 H. Takahashi et al.
3130 genetic analyzer (Perkin-Elmer Japan, Yokohama,Japan) according to the manufacturers’ protocols.
2.4. Statistical analysis
Comparative data were analyzed using the Mann-Whitney U test. The cutoff for statistical significance wasP b .05.
3. Results
3.1. Immunohistochemical findings
Examples of immunoreactivity for β-catenin, p21waf1,cyclin D1, cyclin E, Ki-67, CD10, and α-SMA in bothepithelial and stromal components of APAs are illustrated inFig. 1. Nuclear accumulations of β-catenin, p21waf1, andcyclin D1, as well as cytoplasmic CD10 immunoreactivity,were frequently observed in epithelial components,including squamous morular lesions, in contrast to theless intense immunoreactivity for cyclin E and Ki-67.Distinct immunopositivities for p21waf1 and cyclin D1, butnot for nuclear β-catenin, cyclin E, and Ki-67, wereevident in the myofibromatous stromal components. Inaddition to diffuse and strong immunoreaction for α-SMA,focal and weak CD10 immunopositivity was observed in thestroma of 3 cases (Table 1).
In the epithelial components, the average LI values fornuclear β-catenin, as well as p21waf1 and cyclin D1, showedstepwise increases from normal proliferative endometriumthrough CAH and AM to APA lesions, particularly insquamous morular areas, whereas the LIs of both Ki-67 and
cyclin E were significantly decreased in APAs, with theexception of the squamous morular APA lesions (Fig. 2A).In the stromal components, significantly higher LI values forp21waf1 and cyclin D1 were evident in APAs than in normal,CAH, or AM lesions, whereas the LIs of Ki-67, as well ascyclin E, were decreased in stepwise fashion from normaltissue to APA lesions. There was no significant difference innuclear β-catenin LIs (Fig. 2B).
In normal endometrial stromal components with strongCD10 immunoreactivity, significantly higher α-SMA LIswere observed in the secretory than in the proliferative phase(Fig. 3A and B). In 2 AM cases, strong α-SMA and weakCD10 immunopositivity were common in stromal compo-nents (Fig. 3C), supporting an earlier report that such lesionsconsist of endometrial-type stroma and smooth muscles, withthe latter predominant [18].
3.2. Mutation analysis of CTNNB1
Sequence analysis of exon 3 of CTNNB1 revealedheterozygous substitution mutations in all 7 APA cases(Table 1). Of these cases, 3 also demonstrated single-nucleotide substitutions in the epithelial but not the stromalcomponents (Fig. 4A), in contrast to absence of the genemutations in AM and CAH (Fig. 4B and Table 1).
4. Discussion
The present study provides evidence for frequentmutations of CTNNB1 in epithelial but not stromalcomponents of APAs, in line with results showing highnuclear β-catenin accumulation, particularly in squamous

Fig. 3 Expression of α-SMA and CD10 in stroma of normal endometrium and AM. A, Normal proliferative (left) and latesecretory (right) endometrial tissues; H&E staining (upper panels) and IHC staining for α-SMA (lower). Note apparentimmunoreactivity for α-SMA immunoreactivity in stromal cells in late secretory phase (stromal lesions indicated by arrow aremagnified in the inset), in contrast to the immunoreaction in vessel walls only (arrow) in the proliferative phase (originalmagnifications ×200; inset, ×400). B, α-SMA LI values in proliferative (Proli) and late secretory (Late Sec) stromal components.Data are shown as means ± SDs. C, Serial sections of AM case. H&E staining (left) and IHC staining for CD10 (middle) andα-SMA (right). Original magnification ×100.
37CTNNB1 mutations in APA
morular lesions. Considering the absence of mutations inAM and CAH cases, it is suggested that activation of β-catenin signaling, probably by the gene abnormalities, isessential for establishment of the architecturally character-istic glandular components. This conclusion may besupported by our previous findings of a functional role ofthe signaling during trans-differentiation toward the morularphenotype of endometrial carcinoma cells [14-16].
In contrast to our present data, an earlier report revealedcytoplasmic and nuclear accumulation of β-catenin in 5 of 6APAs, despite the absence of gene mutations [19]. Althoughwe are unable to provide an explanation for the discrepantresults, it is possible that there were differences in themicrodissection of the paraffin-embedded tissues because thepresence of stromal components not having the mutationsappeared to be false-negative results. In addition, it ispossible that CTNNB1-mutated tumor cells escaped detec-tion because of smaller numbers or heterogeneous distribu-tion in the lesions.
An important finding was that p21waf1 was over-expressed in both the epithelial and stromal componentsof APAs, in line with the significant decrease in cell
proliferation. In general, p21waf1 is considered to inhibitcell-cycle progression primarily through inhibition ofcyclin-dependent kinase 2 [20], allowing us to speculatethat its overexpression may be key in the modulation ofcell proliferation in APA lesions. In addition, it appearsthat CTNNB1 abnormalities serve as a regulator of the cellkinetics in epithelial but not stromal components throughinduction of p21waf1 expression, as the nuclear accumula-tion was demonstrated to be secondary to activation of thep14ARF/p53/p21waf1 pathway [15].
As unexpected results in this study, overexpression of thecyclin D1 gene (CCND1), a target of β-catenin signaling,was observed in both components, with a tendency todemonstrate an inverse relationship to cell proliferation. Ingeneral, G1 cyclins, including cyclin D1, Cdk4, andp16INK4A, are considered nonessential for completion ofmost normal cell division cycles, as overexpressed G1cyclins do not as a rule increase net cell proliferation, despiteaccelerating G1 to S progression [21]. In fact, frequentcoexpression of nuclear β-catenin, cyclin D1, and p16INK4A
has been demonstrated at invasive fronts with low prolifer-ation rates in colorectal adenocarcinomas [22]. Together with

Fig. 4 Sequence analysis of exon 3 of CTNNB1 in APA and AM. A, Case APA-3. Note heterozygous substitution mutation (arrows)in total and epithelial samples (upper panel), in line with nuclear β-catenin accumulation, whereas such mutations are not evident instromal samples (lower left, dotted arrow). B, Case AM-2. No mutations in hot spots (indicated by C33, C37, C41, and C45) in exon 3 ofCTNNB1 (upper panel). IHC staining for β-catenin (lower). Note absence of nuclear β-catenin immunoreactivity in glandular components, incontrast to strong membranous immunoreaction. Boxes with solid outlines that enclose a gland are magnified in the insets; originalmagnifications ×100; inset ×400.
38 H. Takahashi et al.
the evidence of cyclin D1 expression in squamous morularlesions lacking cell proliferative activity within endometrialcarcinomas [15], its overexpression may contribute to celldifferentiation rather than to proliferation. Second, theobserved overexpression of cyclin E in the squamousmorular lesions was unexpected, as E-type cyclins induceprogression through the G1 phase of the cell cycle [23].Given the evidence that β-catenin coactivates liverreceptor homolog 1 effects on the cyclin E promoter [24],it is likely that β-catenin signaling also contributes tocyclin E expression through interaction with other transcrip-tion factors.
There is a rapidly growing body of evidence that APAshave a hybrid myofibromatous stroma with admixturesof smooth muscle, collagenous fibrous tissue, and normalendometrial stroma, indicating the histogenesis as myofi-bromatous metaplasia of normal endometrial stromal cells[2,17,25]. In this study, coexpression of CD10 and α-SMAwas evident in stromal components in 3 of the 7 APAs.Similar findings were observed in 2 AM cases. Togetherwith the evidence of changes in α-SMA immunopositivity
in normal endometrial stroma during the menstrual cycle,it appears that established cells progress to myofibromatouscells in response to differentiation-promoting events,probably hormonal effects, leading to a shift from CD10 toα-SMA immunophenotypes.
Previously, a concept of “APA with low malignantpotential (APA-LMP),” which shows a high risk for localrecurrence and infiltration into myometrium, has beenproposed [2]. Although the number of cases in our serieswas small, it was impressive that both components showedsignificantly decreased cell proliferation, implying thatmost APAs can be categorized as benign or at least low-grade malignant lesions. Further studies on this point clearlyare warranted.
Together, our observations suggest a model for estab-lishment and maintenance of epithelial and stromal parts ofAPAs (Fig. 5). A combination of β-catenin signaling andoverexpression of p21waf1 may be necessary for formation ofthe architectural complexity of the glandular components,leading to inhibition of cell proliferation. In contrast,changes in the cell phenotype through a shift from CD10

Fig. 5 Schematic representation of possible histogenesis of epithelial and stromal components of APA.
39CTNNB1 mutations in APA
to α-SMA immunopositivity may occur during myofibro-matous formation in the stromal components, independent ofCTNNB1 status.
In conclusion, our data clearly demonstrate differentmechanisms for the histogenesis of the epithelial and stromalcomponents of APAs.
References
[1] Mazur MT. Atypical polypoid adenomyomas of the endometrium. AmJ Surg Pathol 1981;5:473-82.
[2] Longacre T, Chung MH, Rouse RV, et al. Atypical polypoidadenomyofibromas (atypical polypoid adenomyomas) of the uterus.Am J Surg Pathol 1996;20:1-20.
[3] Young RH, Treger T, Scully RE. Atypical polypoid adenomyoma ofthe uterus: a report of 27 cases. Am J Clin Pathol 1986;86:139-45.
[4] Fukunaga M, Endo Y, Ushigome S, et al. Atypical polypoidadenomyomas of the uterus. Histopathology 1995;27:35-42.
[5] Heatley MK. Atypical polypoid adenomyoma: a systematic review ofthe English literature. Histopathology 2006;48:609-10.
[6] Kuwashima Y, Uehara T, Kurosumi M, et al. Atypical polypoidadenomyomas of the uterus in a very old woman: report of a case withimmunohistochemical characterization of its stromal components andproliferative status. Eur J Gynaecol Oncol 1995;16:115-9.
[7] Clement PB, Young RH. Atypical polypoid adenomyomas of the uterusassociated with Turner’s syndrome: a report of three cases, including areview of ‘estrogen-associated’ endometrial neoplasm and neoplasmsassociated with Turner’s syndrome. Int J Gynecol Pathol 1987;71:141-4.
[8] Horita A, Kurata A, Komatsu K, et al. Coexistent atypical polypoidadenomyoma and complex atypical endometrial hyperplasia in theuterus. Diagn Cytopathol 2010;38:527-32.
[9] Sugiyama T, Ohta S, Nishida T, et al. Two cases of endometrialadenocarcinoma arising from atypical polypoid adenomyoma. Gyne-col Oncol 1998;71:141-4.
[10] Fukuda M, Sakurai N, Yamamoto Y, et al. Case of atypicaladenomyoma that possibly underwent a serial progression fromendometrial hyperplasia to carcinoma. J Obstet Gynecol Res2011;5:468-71.
[11] Ozawa M, Baribault H, Kemler R. The cytoplasmic domain of the celladhesion molecule uvomorulin associates with three independentproteins structurally related in different species. EMBO J 1989;8:1711-7.
[12] Kemler R. From cadherins to catenins: cytoplasmic proteininteractions and regulation of cell adhesion. Trends Genet 1993;9:317-21.
[13] Gumbiner B. Signal transduction by β-catenin. Curr Opin Cell Biol1997;7:634-40.
[14] Saegusa M, Okayasu I. Frequent nuclear β-catenin accumulationand associated mutations in endometrioid-type endometrial andovarian carcinomas with squamous differentiation. J Pathol 2001;194:59-67.
[15] Saegusa M, Hashimura M, Kuwata T, et al. β-Catenin simultaneouslyinduces activation of the p53-p21WAF1 pathway and overexpressionof cyclin D1 during squamous differentiation of endometrialcarcinoma cells. Am J Pathol 2004;164:1739-49.
[16] Saegusa M, Hashimura M, Kuwata T, et al. A functional role of Cdx inβ-catenin signaling during transdifferentiation in endometrial carcino-mas. Carcinogenesis 2007;28:1885-92.
[17] Ohishi Y, Kaku T, Kibayashi H, et al. CD10 immunostainingdistinguishes atypical polypoid adenomyofibroma (atypical polypoidadenomyoma) from endometrial carcinoma invading the myometrium.HUM PATHOL 2008;39:1446-53.
[18] Gilks CB, Clement PB, Hart WR, et al. Uterine adenomyomasexcluding atypical polypoid adenomyomas and adenomyomas ofendocervical type: a clinicopathologic study of 30 cases of anunderemphasized lesion that may cause diagnostic problems with briefconsideration of adenomyomas of other female genital tract sites. Int JGynecol Pathol 2000;19:195-205.
[19] Ota S, Catasus L, Matias-Guiu X, et al. Molecular pathology of atypicalpolypoid adenomyoma of the uterus. HUM PATHOL 2003;34:784-8.
[20] Abbas T, Dutta A. p21 in cancer: intricate networks and multipleactivities. Nat Rev Cancer 2009;9:400-14.

40 H. Takahashi et al.
[21] Quelle DE, Ashmun RA, Shurtleff SA, et al. Overexpression of mouseD-type cyclins accelerates G1 phase in rodent fibroblasts. Genes Dev1993;7:1559-71.
[22] Jung A, Schrauder M, Oswald U, et al. The invasion front ofhuman colorectal adenocarcinomas shows co-localization of nuclearβ-catenin, cyclin D1, and p16INK4A and is a region of low proliferation.Am J Pathol 2001;159:1613-7.
[23] Sherr CJ. Cancer cell cycles. Cell 1996;274:1672-7.[24] Botrugno OA, Fayard E, Annicotte J-S, et al. Synergy between LRH-1
and β-catenin induces G1 cyclin-mediated cell proliferation. Mol Cell2004;15:499-509.
[25] Horita A, Kurata A, Maeda D, et al. Immunohistochemicalcharacteristics of atypical polypoid adenomyoma with specialreference to h-caldesmon. Int J Gynecol Pathol 2010;30:64-70.