Farletuzumab, an anti-folate receptor α antibody, does not block binding of folate or anti-folates...
8
ORIGINAL ARTICLE Farletuzumab, an anti-folate receptor a antibody, does not block binding of folate or anti-folates to receptor nor does it alter the potency of anti-folates in vitro B. A. Kamen • A. K. Smith Received: 2 February 2012 / Accepted: 9 May 2012 / Published online: 27 May 2012 Ó Springer-Verlag 2012 Abstract Purpose Folate is a cofactor in the synthesis of purines and pyrimidines; folate analogs are potent cytotoxic drugs. Folate receptor alpha (FRa), a protein-mediating cellular accumulation of folate (and anti-folates), has limited expression in normal tissues and is overexpressed by numerous carcinomas. Limited distribution and high affinity for folic acid have resulted in the development of antibodies or the use of folic acid coupled to toxins or radionuclides as therapeutic and imaging agents. Farletuzumab is an anti- FRa antibody in clinical trials for ovarian and non-small cell lung cancers. Our goal was to evaluate the effect of far- letuzumab on binding and uptake of folates and anti-folates and the potency of anti-folates in vitro. Methods Direct binding and uptake of radiolabeled folates and anti-folates and the assessments of drug concentration of drug that inhibited cell growth 50 % (IC 50 ) in vitro in the presence or absence of antibody. Results Farletuzumab did not block membrane binding of radiolabeled folic acid, 5-methyltetrahydrofolate, pemetr- exed, and other anti-folates; folic acid blocked [ 95 %. Farletuzumab had a minimal effect on the cytoplasmic accumulation of 5-methyltetrahydrofolate or pemetrexed; folic acid had a considerable but variable effect on the different cell lines. As a single agent, farletuzumab did not affect cell viability or the IC 50 of pemetrexed and other anti-folates in vitro. Conclusions Farletuzumab does not block FRa binding of folates and anti-folates, minimally retards folate delivery via FRa-mediated transport, and minimally retards the growth of cells in vitro. Concomitant use of farletuzumab and pemetrexed is not contraindicated. Keywords Anti-folate Á Folate receptor Á Farletuzumab Á Pemetrexed Introduction Folate is a water-soluble vitamin, a cofactor in the synthesis of purines and pyrimidines [1]. The critical nature of these pathways has made them targets for anti-folates (folate ana- logs), drugs used as antibiotics, immunosuppressives, and anticancer agents. For example, methotrexate (MTX) has been a mainstay for patients with acute lymphoblastic leuke- mia for about 60 years and also remains one of the most commonly used disease-modifying antirheumatic drugs (DMARD). Concomitantly, with the empiric clinical suc- cesses, the study of folate and anti-folate transport and intra- cellular metabolism has led to a greater understanding of the mechanisms of resistance to anti-folates and subsequently, the development of newer agents which are either transported more robustly or are better substrates for folylpolyglutamate synthase [2]. One such drug is pemetrexed (Alimta Ò , Eli Lilly & Company), initially referred to as the multitargeted anti- folate because it inhibited three enzymes: thymidylate syn- thase, dihydrofolate reductase, and glycinamide ribonucleo- tide formyl transferase. It is approved for patients with mesothelioma and non-small cell lung cancer (NSCLC). A greater understanding of folate accumulation has also led to the development of agents that target a specific molecule on the membrane. Folate receptor a (FRa), one of the four members of the folate receptor family, has a high affinity for the natural, major serum folate, B. A. Kamen (&) Á A. K. Smith Cancer Institute of New Jersey, Robert Wood Johnson Medical School, 195 Little Albany Street, New Brunswick, NJ 80901, USA e-mail: [email protected] 123 Cancer Chemother Pharmacol (2012) 70:113–120 DOI 10.1007/s00280-012-1890-2
Transcript of Farletuzumab, an anti-folate receptor α antibody, does not block binding of folate or anti-folates...

ORIGINAL ARTICLE
Farletuzumab, an anti-folate receptor a antibody, does not blockbinding of folate or anti-folates to receptor nor does it alterthe potency of anti-folates in vitro
B. A. Kamen • A. K. Smith
Received: 2 February 2012 / Accepted: 9 May 2012 / Published online: 27 May 2012
� Springer-Verlag 2012
Abstract
Purpose Folate is a cofactor in the synthesis of purines and
pyrimidines; folate analogs are potent cytotoxic drugs.
Folate receptor alpha (FRa), a protein-mediating cellular
accumulation of folate (and anti-folates), has limited
expression in normal tissues and is overexpressed by
numerous carcinomas. Limited distribution and high affinity
for folic acid have resulted in the development of antibodies
or the use of folic acid coupled to toxins or radionuclides as
therapeutic and imaging agents. Farletuzumab is an anti-
FRa antibody in clinical trials for ovarian and non-small cell
lung cancers. Our goal was to evaluate the effect of far-
letuzumab on binding and uptake of folates and anti-folates
and the potency of anti-folates in vitro.
Methods Direct binding and uptake of radiolabeled folates
and anti-folates and the assessments of drug concentration of
drug that inhibited cell growth 50 % (IC50) in vitro in the
presence or absence of antibody.
Results Farletuzumab did not block membrane binding of
radiolabeled folic acid, 5-methyltetrahydrofolate, pemetr-
exed, and other anti-folates; folic acid blocked [95 %.
Farletuzumab had a minimal effect on the cytoplasmic
accumulation of 5-methyltetrahydrofolate or pemetrexed;
folic acid had a considerable but variable effect on the
different cell lines. As a single agent, farletuzumab did not
affect cell viability or the IC50 of pemetrexed and other
anti-folates in vitro.
Conclusions Farletuzumab does not block FRa binding of
folates and anti-folates, minimally retards folate delivery
via FRa-mediated transport, and minimally retards the
growth of cells in vitro. Concomitant use of farletuzumab
and pemetrexed is not contraindicated.
Keywords Anti-folate � Folate receptor � Farletuzumab �Pemetrexed
Introduction
Folate is a water-soluble vitamin, a cofactor in the synthesis of
purines and pyrimidines [1]. The critical nature of these
pathways has made them targets for anti-folates (folate ana-
logs), drugs used as antibiotics, immunosuppressives, and
anticancer agents. For example, methotrexate (MTX) has
been a mainstay for patients with acute lymphoblastic leuke-
mia for about 60 years and also remains one of the most
commonly used disease-modifying antirheumatic drugs
(DMARD). Concomitantly, with the empiric clinical suc-
cesses, the study of folate and anti-folate transport and intra-
cellular metabolism has led to a greater understanding of the
mechanisms of resistance to anti-folates and subsequently, the
development of newer agents which are either transported
more robustly or are better substrates for folylpolyglutamate
synthase [2]. One such drug is pemetrexed (Alimta�, Eli Lilly
& Company), initially referred to as the multitargeted anti-
folate because it inhibited three enzymes: thymidylate syn-
thase, dihydrofolate reductase, and glycinamide ribonucleo-
tide formyl transferase. It is approved for patients with
mesothelioma and non-small cell lung cancer (NSCLC).
A greater understanding of folate accumulation has also
led to the development of agents that target a specific
molecule on the membrane. Folate receptor a (FRa), one
of the four members of the folate receptor family, has a
high affinity for the natural, major serum folate,
B. A. Kamen (&) � A. K. Smith
Cancer Institute of New Jersey, Robert Wood Johnson
Medical School, 195 Little Albany Street,
New Brunswick, NJ 80901, USA
e-mail: [email protected]
123
Cancer Chemother Pharmacol (2012) 70:113–120
DOI 10.1007/s00280-012-1890-2

5-methyltetrahydrofolate (Kd * 10-9 M), and an even
greater affinity for folic acid (Kd * 10-12 M). It also binds
pemetrexed and, to a much lesser extent, MTX [3]. FRa has
a limited normal tissue distribution and is overexpressed by
a number of carcinomas [4]. This specificity, affinity, and
limited tissue distribution have led to using folic acid
coupled to toxins or radionuclides and the development of
antibodies as therapeutic or imaging agents [5].
Farletuzumab, an anti-FRa antibody (Ab), is currently in
multiple clinical trials for women with ovarian cancer and,
more recently, in NSCLC [6, 7]. Pemetrexed is indicated for
the treatment for NSCLC and mesothelioma and has shown
some activity in patients with ovarian cancer [8, 9]. If far-
letuzumab and anti-folates are to be used concomitantly, it is
important to know the effect of the antibody on folate and
anti-folate binding and accumulation as well as potency of
the latter in FRa? tumors. Previously, it has been shown
that farletuzumab mediates antibody-dependent cellular
cytotoxicity (ADCC) and complement-dependent cytotoxic-
ity (CDC) and has some effects on the growth of a Chinese
Hamster Ovary (CHO) cell line transfected with FRa (CHO-
FR) when grown in low folate, but its effects on folate uptake
and toxicity in human cell lines naturally expressing FRa have
not been reported [10]. Here, we show that, in several cell
lines, naturally expressing FRa farletuzumab did not block
binding of folic acid, 5-methyltetrahydrofolate, pemetrexed,
and other anti-folates and only minimally altered FRa-medi-
ated folate uptake and cell growth in vitro. Moreover, the
concentration of drug that inhibited cell growth 50 % (IC50) of
MTX, aminopterin, and pemetrexed (PMX) in vitro were not
significantly affected by the same Ab concentration that
mediated ADCC and CDC [10]. As important controls, we
found that (a) exogenous folate in the medium did decrease
PMX potency, and (b) functionally disabling FRa by satu-
rating with low-dose folic acid decreased PMX accumulation
but not cytotoxicity. This latter point confirms that FRa is not
the major transport system for pemetrexed or folates. This is in
agreement with the work of others [11, 12].
Materials and methods
Materials
Radiolabeled compounds (5-methyltetrahydrofolic acid
[3H-MTHF], folic acid [3H-FA], and pemetrexed [3H-PMX])
were obtained from Moravek Biochemicals. The specific
activity of these compounds varied from batch to batch and
ranged from 10,000 to 40,000 DPM/pmole. They were puri-
fied by high-performance liquid chromatography (HPLC)
when the non-specific background was[5 %.
Roswell Park Memorial Institute (RPMI) folic acid-free
medium was from Invitrogen #27016-021 and fetal bovine
serum (FBS) was purchased from Gibco�. All other com-
pounds for buffers (e.g., Tris, saline) were purchased from
commercial sources such as Sigma. Pemetrexed, commer-
cially available, was supplied by our Pharmacy and ami-
nopterin and MTX purchased from Sigma. Farletuzumab
was provided by Morphotek, Inc.
Cell lines
IGROV-1, MA104, JAR, BeWo, HK2, and CHO cells
(both transfected with FRa and parent) were maintained in
RPMI folic acid-free medium containing 10 % FBS, with
20 pmol/ml fresh 5-methyltetrahydrofolate added to stock
flasks only at time of split (approximately weekly), so that
the final concentration of reduced folate in the medium of
experimental cells was 5 nM, with the exception of CHO
parent, which required additional folate in experimental
plates as well for adequate growth [13–16].
Folate and anti-folate uptake
Cells were grown in RPMI without folic acid with 10 %
FBS and Penicillin and Streptomycin until the desired level
of confluence was reached. Typically, T25 flasks were
seeded with 0.2 million cells each in 3–5 ml media. For
multi-well plates, approximately 1.5 million cells from
stock flask were diluted with 50 ml growth medium
(30,000 cells/ml) and then plated at: 2 ml/well for 6-well
plates, 1 ml/well for 12-well plates, 0.5 ml/well for 24-well
plates, 0.25 ml/well for 48-well plates, or 0.1 ml/well for
96-well plates (yielding final plating density of approxi-
mately 7,000–9,000 cells/cm2). On the day of an experi-
ment, the media were aspirated and cells rinsed once with
Hanks Balanced Salt Solution (HBSS).
For assessing vitamin or drug accumulation, the growth
media were replaced with incubation media (either HBSS
or RPMI without folate or FBS) and the desired 3H-labeled
compound as indicated in each experiment. To control for
non-specific uptake, a flask or well of each condition/
concentration was incubated with a 200–5009 excess of
non-labeled compound. To harvest, cells were chilled on
ice, the media aspirated, and plates were washed 39 with
large volumes of ice-cold phosphate-buffered saline (PBS).
Freeze–thaw (FT) buffer (10 mM Tris, 1 % beta mercap-
toethanol) and 0.5 lM MTHF were added in the same
volume as initial incubation, and the flasks or plates were
frozen flat at -80 �C for at least 15 min to lyse the cells
(plates are wrapped in plastic wrap first to deter evapo-
ration; flasks caps are tightened). The cells were then
thawed on ice, scraped with a plastic cell scraper, and
collected into microcentrifuge tubes along with a FT
buffer rinse. Tubes were then centrifuged at 1009g for
20 min at 4 �C, and the supernatant carefully removed.
114 Cancer Chemother Pharmacol (2012) 70:113–120
123

The entire supernatant (intracellular uptake) was aspirated
and counted for radioactivity. The pellet, representing
membrane-bound compound, was also subjected to analy-
sis by liquid scintillation counting after solubilizing in
0.1 N NaOH. These techniques are detailed in our previous
reports [14–16].
Folic acid binding to folate receptor (AL and AR)
Direct binding
3H-folic acid was added to the incubation medium. At the
end of incubation, the cells were chilled on a bed of ice, the
media aspirated, and cells washed 39 with large volumes
of ice-cold PBS. Acid saline (pH 3.5 with acetic acid) was
added (same volume as 3H incubation), and the flask or
plate rocked for 30 s. The acid wash was collected into
scintillation vials, and the cells rinsed with PBS (about
5–10 s) and that wash added to the first. This represents the
surface-bound ligand referred to as the acid-labile (AL)
fraction. The radioactivity remaining with the acid-resis-
tant (AR) cells was determined either by trypsinizing the
cells and collecting them with a rinse or by solubilizing the
cells with 0.1 N NaOH. At least one of the non-specific
wells was collected by trypsinization, so that a cell count
could be done (if growth conditions or experimental
treatment was likely to have changed the final cell count,
then one well from each condition was counted). These
techniques are detailed in our previous efforts [14–16].
Cytotoxicity
Cells were plated in 96-well plates in 100 ll growth media
(RPMI without folic acid, with 10 % FBS and Pen-Strep) at
3,000 cells/well. Cells were usually allowed to settle and
attach before additives or treatments were begun (generally
2–4 h). Antibody and/or folate was added in a 50 ll volume
at 49 concentration to appropriate wells. Drug or further
treatments were added in additional 50 ll (also 49), and
cells were allowed to grow as indicated in experiment.
Phenazine methosulfate (PMS)-activated MTS (Promega)
was added to wells (usually 25–30 ll/well) and incubated for
2–4 h. Absorbance at 490 nm was read on a plate reader and
the IC50 calculated from the maximum and minimum read-
ings for each set of conditions. A media/MTS control was
subtracted as background. All cell lines had been adapted to
grow in folic acid-free medium with 10 % FBS, with no
additional folate added except as indicated.
Analysis
All experimental points shown here were done at least in
triplicate and repeated at least twice on separate days. In
order to account for non-specific binding and uptake, folic
acid or 5MTHF at 200–500 times the radiolabeled com-
pound was also included in each experiment. This back-
ground was generally \5 % of total counts or the
radiolabeled compound was purified before using. The data
are plotted showing the 95 % confidence limits using Prism
IV (Graph Pad, San Diego California).
Results
Farletuzumab does not block binding of folic acid
to FRa
FRa, a glycosyl phosphatidyl inositol (GPI) linked pro-
tein, is clustered in lipid rafts on the membrane and
cycles between a surface (acid labile) and internalized,
but still membrane-bound, compartment (acid-resistant)
[13]. To begin the assessment of potential effects of far-
letuzumab on FRa function/cellular location, we first
CHO-FR cells
0 1 10 1000
100002000030000400005000060000700008000090000
Farletuzumab (ug/ml)
DP
M B
ou
nd
/105 c
ells
control 1 10 1000
2500
5000
7500
10000 MA104 Cells
Farletuzumab (ug/ml)
DP
M B
ou
nd
/105 c
ells
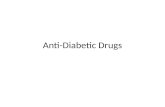
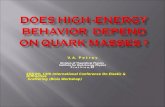
Fig. 1 Farletuzumab has little effect on the steady-state distribution
of FRa bound folic acid: CHO-FR and Ma104 cells were incubated
for 2 h with 10 nM 3H-folic acid at 37�, and then the cells were
processed to determine the surface binding (acid labile, AL) and
internal pool (acid-resistant, AR) using an acid buffer wash as
detailed in ‘‘Materials and methods.’’ The open bars are the AL and
the closed bars the AR pool of bound 3H-folic acid. Farletuzumab
was added 2 h before the 3H-folic acid and remained in the medium
for the entire incubation
Cancer Chemother Pharmacol (2012) 70:113–120 115
123

compared the binding of 10 nM 3H-folic acid by MA104
cells (monkey kidney proximal tubule cell) and CHO cell
transfected with FRa (CHO-FR). The former was the
initial model for FRa-mediated folate transport and the
latter the cell line used to initially characterize far-
letuzumab effects in vitro [10, 13–15]. Using up to a 109
greater concentration than what was used in cytotoxicity
studies previously reported [10], farletuzumab had little
effect on folic acid binding (Fig. 1). Confirming an earlier
report [13], the CHO-FR cells bind 6–7 times more folic
acid than MA104 cells, and the ratio of the AL/AR pool
is approximately 4:1, that is, the majority of the receptor
was in the external pool, whereas in the MA104 cell the
ratio was approximately 1.5:1. To more thoroughly study
the effects of the Ab, we studied the binding of folic acid
by the naturally overexpressing IGROV-1 cells. Binding
was essentially complete by 2 h, and the ratio of AL/AR
was about 4:1 (Fig. 2a). Importantly, even at 6 h, there is
no significant cytoplasmic accumulation of folic acid
(solid circle at 6 h time point). Folic acid has such a great
affinity for FRa that at this low, but saturating, concen-
tration, it is not released into the cytoplasm of the cell;
therefore, it is an excellent marker of membrane binding
[13]. Cells in Fig. 2b (IGROV-1), c (HK2), and d (JAR)
show that farletuzumab does not block binding of 3H-folic
acid, as total membrane radioactivity (AL ? AR) was
similar in controls and Ab-treated cells. The JAR cells
have an AL/AR ratio similar to the IGROV-1 cells
(*4:1) and other malignant cell lines, such as KB, HCT8,
and SKOV, which we have studied (data not shown)
while the HK2 is similar to the MA104 cells (1.5:1). Why
cancer cells and cells transfected with FRa have the
majority of the receptor on the external surface while the
nonmalignant cells have a more equal distribution is not
known. Interestingly, treating MA104 cells with phorbol
myristic acid (PMA) externalizes the majority of the
receptor, and PMA has no effect on malignant cells [21].
There does appear to be a small decrease in binding of3H-folic acid-resistant (AR) compartment (Fig. 2c, d) and
slight increase in the acid-labile fraction in Fig. 2b. We
speculate that these small differences in the distribution of
FRa on the membrane may be a result of the fact that
compartmentalization of a GPI-anchored protein affected
by the bulk of the protein attached to the lipid anchor [17].
0 1 2 3 4 5 60
50000
100000
150000
200000
250000AAL
AR
Hours
dp
m/w
ell
0 1 2 3 4 5 6 70
100000
200000
300000B
Hours
dp
m/w
ell
0 1 2 3 4 5 6 70
2000
4000
6000
8000
10000
12000C
Hours
dp
m/w
ell
0 1 2 3 4 50
10000
20000
30000
40000D
Hours
dp
m/w
ell
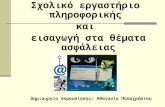
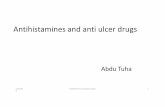
Fig. 2 Time course of 3H-folic acid binding to membrane in naturally
expressing FRa human cell lines in the presence and absence of
farletuzumab: Cells (IGROV-1, ovarian cancer), JAR (choriocarci-
noma) and HK2(human kidney epithelial cells) were incubated with
10 nM 3H-folic acid at 37� for the times indicated, and then surface
membrane binding (i.e., acid labile, AL) and the internalized membrane
fraction (i.e., acid-resistant, AR) were determined. a The time course to
the saturation of the receptor pool and the lack of cytoplasmic folic acid
(solid circle at 6 h) accumulation in IGROV-1 cells. b (IGROV-1);
c (HK2) and d (JAR) Farletuzumab (10 lg/ml) added 2 h before 3H-
folic acid had no significant effect on the binding of 3H-folic acid or the
distribution of the receptor in the AL or AR compartment. Solid line is
AL and dotted lines are AR. Squares = control; Triangles = sample
with Ab
116 Cancer Chemother Pharmacol (2012) 70:113–120
123

0 1 2 3 40
10000
20000
30000
40000
50000A
Hours
dp
m/w
ell
0 30 60 90 120
0
5000
10000
15000
20000
25000
30000C
min
dp
m/w
ell
0 1 2 3 40
2000
4000
6000
8000
10000
12000B
Hours
dp
m/w
ell
0 30 60 90 120
0
500
1000
1500
2000
2500D
min
dp
m/w
ell
0 2 4 6 80
20
40
60
80
100
+ Folic Acid
+ Ab (10ug)
+ Ab (50ug)
E
Time (hours)
% m
ax u
pta
ke
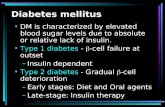
Fig. 3 Total membrane binding and cytoplasmic accumulation of3H-MTHF and 3H-PMX in the presence or absence of farletuzumab or
folic acid: a (IGROV-1 cells) and b (HK2 cells) incubated with 3H-
MTHF (20 nM) and c (IGROV-1) and d (HK2 cells) with 3H-PMX
(50 nM). e 3 H-MTHF uptake in the presence of either 10 or 50 ug/ml
Ab or 5 nM folic acid normalized to control. In a–d, Farletuzumab
(10 lg/ml) or folic acid (5 nM) when present was added 2 h before
vitamin or drug. Squares = control; Triangles = farletuzumab; Circles =
folic acid. Solid line = cytoplasmic uptake; dashed line = membrane
binding. a–d 95 % Confidence limits
Cancer Chemother Pharmacol (2012) 70:113–120 117
123

The Ab (160,000 kD) would add significant mass to the
approximately 40 kD FRa. This observation and the
potential effect on FRa cycling (and other proteins that
may also be in the same lipid raft) are under further study
and will be discussed below and in greater detail
elsewhere.
Folic acid, but not farletuzumab, blocks binding
of 5-methyltetrahydrofolate and pemetrexed
and also decreases cytoplasmic accumulation
of these ligands more than Ab
As shown in Fig. 2a, FRa has such a great affinity for folic
acid (Kd * 10-12 M) compared with the natural serum
folate, 5-MTHF, that it does not accumulate to any sig-
nificant degree under low physiological concentrations
(e.g., 10–20 nM) because it is not released from the
receptor and is a very poor substrate for the reduced folate
carrier (Kt * 100–200 lM). Therefore, to more com-
pletely assess the effect of farletuzumab on FRa-mediated
vitamin or drug transport, we measured membrane binding
and cytoplasmic accumulation of the natural serum folate,
MTHF, and PMX in the presence of Ab and/or folic acid.
The latter will block binding to FRa; therefore, uptake of
any substrate under these conditions is a measure of non-
FRa-mediated uptake, likely the ubiquitous and well-
described RFC or PCFT [18, 19]. Similar to the lack of the
effect of farletuzumab on binding of 3H-folic acid by FRashown in Figs. 1 and 2, we observed no significant effect
on total membrane binding of either 3H-MTHF or3H-PMX, whereas folic acid pre-incubation blocked
[95 % binding of both ligands (dashed lines in Fig. 3).
Cytoplasmic accumulation of 3H-MTHF and 3H-PMX was
minimally blocked by farletuzumab under the conditions
tested (triangles, solid lines Fig. 3). However, folic acid
blocked 34 and 23 % of MTHF uptake and 93 and 53 % of
PMX in IGROV-1 and HK2 cells, respectively. Similar
results for 3H-MTHF were seen when confluent MA104
and CHO cells were studied, although the inhibition of3H-PMX was more in the 50 % range, not [90 % as seen
for the IGROV-1 cells. The accumulation of MTHF and
PMX when FRa is blocked with folic acid shows that other
transport mechanisms for vitamin and drug uptake are
active to varying degrees in all the lines studied. The
importance, or lack thereof, of FRa in log-phase growth of
MA104 cells has been previously shown by us and further
highlights that FRa function on normal epithelial cells such
as in the kidney and choroid plexus [15, 16] is to help
package and conserve folate under the conditions of folate
deficiency [20] and, in general, is not likely critical for
folate uptake in a proliferative cell.
The slightly decreased FRa-mediated uptake of 3H-MTHF
in the presence of farletuzumab is in agreement with the
data in Fig. 2, which allowed the suggestion that receptor
cycling may be altered since ligand binding is not. This is
more completely shown in Fig. 3e, in which the effects
of two concentrations of farletuzumab or folic acid on3H-MTHF cytoplasmic accumulation were studied over an
extended time in IGROV-1 cells. As seen, by 8 h, the total
accumulation of MTHF in the presence of farletuzumab
was equivalent to the control cells and only about 80 %
maximum in the presence of folic acid. To see whether this
attenuated rate of delivery was critical to the cell (since it
was not the major pathway for uptake of MTHF), we more
completely evaluated the effect of Ab on cell proliferation
1 10 1000.00
0.25
0.50
0.75
1.00control
1ug/ml Ab
10ug/ml Ab
A
5methyltetrahydrofolate (nM)
MT
S (
abs
@ 4
90 n
M)
1 10 100
0.0
0.5
1.0
1.5control
1ug/ml Ab
10ug/ml Ab
B
5methyltetrahydrofolate (nM)
MT
S (
abs
@ 4
90 n
m)
1 10 1000.00
0.25
0.50
0.75
1.00 control
1ug/ml Ab
10ug/ml Ab
C
5-methyltetrahydrofolate (nM)
MT
S (
abs
@ 4
90 n
m)
Fig. 4 Three-day growth of cells in the presence of farletuzumab and
increasing concentrations of 5-methyltetrahydrofolate. a Ma104 cells,
b CHO-FR cells, and c IGROV-1 cells. All cells were plated in
96-well plate in RPMI (folic acid-free ?5 % FBS, day 0). On day 1, 1 or
10 lg/ml farletuzumab was added in addition to increasing concentra-
tions of 5-MTHF. After 3 days, MTS was added (30 ll/0.5 ml) and
incubated *1 h and then absorbance was read at 490 nm
118 Cancer Chemother Pharmacol (2012) 70:113–120
123

in vitro as earlier work did show some growth inhibition of
CHO cells transfected with FRa when grown in low folate
for 96 h [10]. The growth of CHO-FR, MA104, and
IGROV-1 cells grown in the presence of Ab and increasing
MTHF for 3 days is shown in Fig. 4. Figure 4a, b shows
that farletuzumab at best may minimally result in some
growth retardation in the MA104 and CHO-FR cells (as
already reported for CHO-FR) that was abrogated as
5-MTHF was increased. IGROV-1 cells were unaffected
(Fig. 4c). This supports the concept that the decreased/
delayed delivery of 5-MTHF in the presence of far-
letuzumab seen in Fig. 3 does not likely cause much
growth arrest.
Folate concentration, but not farletuzumab, decreases
the potency of pemetrexed in vitro
The potency of PMX and several other anti-folates with a
lower affinity for FRa was assessed in the presence of low
and physiological folate concentrations in vitro. In the
presence of increasing amount of folate, the IC50 for PMX
increased but the presence of farletuzumab did not make
any difference (Fig. 5). Specifically, as the folate content
was increased from 5 to 50 nM, the potency of PMX
decreased by as much as 15-fold for IGROV-1 cells
(Fig. 5a) and *twofold for MA104 cells (Fig. 5b). The
potency of PMX against CHO-FR cells was also not altered
by farletuzumab (IC50 2 nM), but overall growth rate was
stimulated by increasing 5-MTHF (data not shown). In this
regard, to confirm the absence of any ‘‘off-site effects,’’ we
also found that farletuzumab had no effect on the potency
of PMX in a receptor-negative cell line (CHO parent), and
the IC50 of PMX for CHO cells transfected with FRa and
the parent line was the same. This is more evidence that
FRa is not important in PMX potency. Finally, as a further
indication that FRa was not overly important with regard
to anti-folate cytotoxicity, we also tested MTX and
aminopterin, two very potent anti-folates with a very low
affinity for FRa, compared to MTHF and PMX. We
found that the IC50 was not altered by farletuzumab (IC50
values of *5 and 0.1 nM for MTX and aminopterin,
respectively).
Discussion
Since PMX is currently approved for patients with can-
cers that may express FRa, it was important to know if
farletuzumab interfered with its potency. Overall, the
results here provide more evidence that (a) FRa is not
the major transport route for intracellular accumulation of
physiological folates or PMX, and (b) that farletuzumab,
an anti-FRa antibody has no significant effect on folate or
anti-folate accumulation or potency (in the case of the
drug). These results support previous studies that PMX
potency is not affected by the presence or absence of the
receptor [11, 12]. Moreover, since folic acid is routinely
prescribed when patients are receiving PMX, the results
here confirm that the potency of PMX may be decreased,
but this is balanced by the need to maintain adequate
folate stores to minimize toxicity, that is maintain accept-
able efficacy.
Farletuzumab has been shown to be active via ADCC
and CDC [10] by targeting FRa as a unique antigen on the
tumor cell and because it has little effect on anti-folate
accumulation or potency, supporting the concept that anti-
folates and antibody can be used together if both agents
have activity as single agents is supported.
More studies of the Ab effect on FRa cycling and dis-
tribution in lipid rafts as a GPI-anchored protein may yield
interesting insights from a cell biology view of membrane
integrity and function, but for now we conclude that far-
letuzumab, although targeting FRa, is not functioning as an
anti-folate.
0 10 20 30 40 500
2
4
6
8
10
12
14B
5-methyltetrahydrofolate (nM)
PM
X IC
50 (
nM)
0 10 20 30 40 500
5
10
15
20
25
30
35A
5-methyltetrahydrofolate (nM)
PM
X IC
50 (
nM)
Fig. 5 Folate but not
farletuzumab decreases the
potency of pemetrexed:
IGROV-1 cells (a) and Ma104
Cells (b) were grown in the
presence of 10 lg/ml antibody,
or just increasing folate without
Ab, for 72 h along with
increasing PMX (10-10–10-7
M). The addition of folate
increased the IC50 from *2 to
*30 nM for IGROV-1 cells
and from *7 to *13 nM for
Ma104 cells, whereas the Ab
had no significant effect
Cancer Chemother Pharmacol (2012) 70:113–120 119
123

Acknowledgments The authors acknowledge medical writing
assistance by Robyn Boyle, RPh under the direction of the authors as
well as financial assistance provided by Morphotek.
Conflict of interest Barton Kamen is now a consultant for Mor-
photek, Inc. Angela Smith reports no conflicts of interest. The authors
have full control of all primary data.
References
1. Fox JT, Stover PJ (2008) Folate-mediated one-carbon metabo-
lism. In: Litwack G (ed) Vitamins and hormones: folic acid and
folates (vol 79). Elsevier, Philadelphia, pp 1–29
2. Kamen BA, Cole P, Bertino JR (2006) Chemotherapeutic agents:
folic acid antagonists. In: Holland JF, Frei E, Bast RC, Kufe DW,
Morton DL, Weichselbaum RR (eds) Cancer medicine. Williams
and Wilkins, Philadelphia, pp 648–660
3. Westerhof GR, Schornagel JH, Kathmann I et al (1995) Carrier-
and receptor mediated transport of folate antagonists targeting
folate-dependent enzymes: correlates of molecular-structure and
biological activity. Mol Pharmacol 48:459–471
4. Elnakat H, Ratnam M (2004) Distribution, functionality and gene
regulation of folate receptor isoforms: implications in targeted
therapy. Adv Drug Deliv Rev 56:1067–1084
5. Leamon CP, Reddy JA (2004) Folate-targeted chemotherapy.
Adv Drug Deliv Rev 56:1127–1141
6. Konner JA, Bell-McGuinn KM, Sabbatini P, Hensley ML, Tew
WP, Pandit-Taskar N, Vander Els N, Phillips MD, Schweizer C,
Weil SC, Larson SM, Old LJ (2010) Farletuzumab, a humanized
monoclonal antibody against folate receptor alpha, in epithelial
ovarian cancer: a phase I study. Clin Cancer Res 16:5288–5295
7. Spannuth WA, Sood AK, Coleman RL (2010) Farletuzumab in
epithelial ovarian carcinoma. Expert Opin Biol Ther 10:431–437
8. Miller DS, Blessing JA, Krasner CN, Mannel RS, Hanjani P,
Pearl ML, Waggoner SE, Boardman CH (2009) Phase II evalu-
ation of pemetrexed in the treatment of recurrent or persistent
platinum-resistant ovarian or primary peritoneal carcinoma: a
study of the Gynecologic Oncology Group. J Clin Oncol
27:2686–2691
9. Tomao F, Panici PB, Frati L, Tomao S, Federica et al (2009)
Emerging role of pemetrexed in ovarian cancer. Expert Rev
Anticancer Ther 9:1727–1735
10. Ebel W, Routhier EL, Foley B, Jacob S, McDonough JM, Patel
RK, Turchin HA, Chao Q, Kline JB, Old LJ, Phillips MD,
Nicolaides NC, Sass PM, Grasso L (2007) Preclinical evaluation
of MORAb-003, a humanized monoclonal antibody antagonizing
folate receptor-alpha. Cancer Immun 7:1–8
11. Chattopadhyay S, Wang Y, Zhao R, Goldman ID (2004) Lack of
impact of the loss of constitutive folate receptor alpha expression,
achieved by RNA Interference, on the activity of the new gen-
eration antifolate pemetrexed in HeLa cells. Clin Cancer Res
10:7986–7993
12. Nutt JE, Razak AR, O’Toole K, Black F, Quinn AE, Calvert AH,
Plummer ER, Lunec J (2010) The role of folate receptor alpha
(FRalpha) in the response of malignant pleural mesothelioma to
pemetrexed-containing chemotherapy. Br J Cancer 102:553–560
13. Kamen BA, Smith AK (2004) A review of folate receptor alpha
cycling and 5-methyltetra-hydrofolate accumulation with an
emphasis on cell models in vitro. Adv Drug Deliv Rev 56:1085–
1097
14. Kamen BA, Capdevilla A (1986) Receptor-mediated folate
accumulation is regulated by the cellular folate content. Proc Natl
Acad Sci USA 83:5983–5987
15. Kamen BA, Wang MT, Streckfuss AJ, Peryea X, Anderson RGW
(1988) Delivery of folates to the cytoplasm of MA104 cells is
mediated by a surface membrane receptor that recycles. J Biol
Chem 263:13602–13609
16. Kamen BA, Wang M-T, Johnson C, Anderson RGW (1989)
Regulation of the cytoplasmic accumulation of 5-Methyltetra-
hydrofolate in MA104 cells is independent of folate receptor
regulation. J Clin Invest 84:1379–1386
17. Nichols B (2009) Endocytosis of lipid-anchored proteins:
excluding GEECs from the crowd. J Cell Biol 186:457–459
18. Zhao R, Qiu A, Tsai E, Jansen M, Akabas MH, Goldman ID
(2008) The proton-coupled folate transporter: impact on
pemetrexed transport and on antifolates activities compared with
the reduced folate carrier. Mol Pharmacol 74:854–862
19. Zhao R, Matherly LH, Goldman ID (2009) Membrane trans-
porters and folate homeostasis: intestinal absorption and transport
into systemic compartments and tissues. Expert Rev Mol Med
11:e4. doi:10.1017/S1462399409000969
20. Birn H, Spiegelstein O, Christensen EI, Finnell RH (2005) Renal
tubular reabsorption of folate mediated by folate binding protein
1. J Am Soc Nephrol 16:608–615
21. Lewis CM, Smith AK, Nguyen C, Kamen BA (1998) PMA alters
folate receptor distribution in the plasma membrane and increases
the rate of 5-methyltetrahydrofolate delivery in mature MA104
cells. Biochim Biophys Acta 1401:157–169
120 Cancer Chemother Pharmacol (2012) 70:113–120
123