Familial hyperinsulinism and pancreatic β-cell ATP-sensitive potassium channels
6
Kidney International, Vol. 57 (2000), pp. 803–808 Familial hyperinsulinism and pancreatic b-cell ATP-sensitive potassium channels NIDHI SHARMA,ANA CRANE,GABRIELA GONZALEZ,JOSEPH BRYAN, and LYDIA AGUILAR-BRYAN Departments of Medicine and Cell Biology, Baylor College of Medicine, Houston, Texas, USA Familial hyperinsulinism and pancreatic b-cell ATP-sensitive shows an increased glycemic response due to increased potassium channels. Familial hyperinsulinism, also known as glycogen storage in the liver. After the diagnosis of PHHI persistent hyperinsulinemic hypoglycemia of infancy (PHHI), has been established, immediate treatment is directed is a genetic disease characterized by mild to severe hypoglyce- towards the maintenance of euglycemia usually by con- mia in the presence of inappropriately high levels of insulin. tinuous administration of intravenous glucose at rates The recessive form is caused by mutations in the adenosine 59-triphosphate (ATP)-sensitive K 1 channel (K ATP channel) between 15 and 20 mg/kg/min. If hypoglycemia persists, present in the plasma membrane of pancreatic b-cells. This the second line of treatment is the administration of com- channel is formed by two subunits, the high-affinity sulfonyl- pounds that inhibit insulin secretion. Two compounds, urea receptor, SUR1, and K IR 6.2, a member of the inwardly diazoxide and somatostatin (octreotide), are widely used rectifying family of K 1 channels. K ATP channels regulate insulin [4]. If this clinical treatment fails to normalize glucose secretion by linking membrane excitability with glucose metab- olism. Approximately 50 mutations, in both channel subunits, levels a partial or subtotal pancreatectomy becomes the that abolish or alter the regulation of b-cell K ATP channels have treatment of choice [1]. Mild forms of the disease may go been identified in patients with the recessive form of PHHI. undiagnosed until eating habits change and an infant has less frequent meals and thus becomes hypoglycemic. Di- azoxide or octreotide for a few months may be sufficient Persistent hyperinsulinemic hypoglycemia of infancy to normalize glucose levels, and clinical remission of symp- (PHHI), also known as familial hyperinsulinism or nesi- toms with time has been observed [3]. In a follow-up dioblastosis (OMIM:256450), is an inherited disorder of study on patients who were treated clinically, Leibowitz glucose metabolism that presents in newborns and in- et al have shown that although patients appear to go into fants, and is mainly characterized by inappropriately high remission, the beta cell defect remains and a significant insulin levels in the presence of low levels of blood glu- number of these individuals become diabetic when they cose. PHHI was originally thought to be a relatively ho- reach puberty [5]. mogenous disorder, but over the last several years an The frequency of the recessive form of PHHI in the underlying heterogeneity has become clear [1]. It is now general population is low (1:50,000), but is reported to understood that PHHI can present with a quite variable be as high as 1:2500 in inbred populations with a high clinical picture, has at least two different histopathologic frequency of consanguineous marriages [6]. PHHI is ge- forms, can be inherited in either a recessive or dominant netically heterogeneous. Four genes have now been iden- manner, and can be caused by mutations in at least four tified to cause the disease, and in approximately 50% of genes [2]. the cases that have been screened for the known reces- From the clinical point of view, some patients present sive and dominant genes, the mutations have not been with severe hypoglycemia almost immediately after birth, identified. Two mild dominant forms of PHHI have been while others show mild hypoglycemia weeks or months described that are caused by mutations in the glucoki- after birth [3]. A biochemical diagnosis is based on ab- nase and glutamate dehydrogenase genes, respectively. normally high insulin levels in the presence of persisting Loss of function mutations in glucokinase have been hypoglycemia, low ketone bodies (a result of their sup- identified as a cause of maturity-onset diabetes of the pression by elevated insulin), and a glucagon test that young, MODY2 [7, 8]. Interestingly, a point mutation, V455 M, in glucokinase has now been identified as caus- ing one of the mild dominant forms of PHHI. This muta- Key words: insulin, potassium channel, sulfonylurea receptor, pan- creas. tion produces an enzyme with a K m that is ,65% lower in comparison with wild-type glucokinase (2.9 mmol/L vs. 2000 by the International Society of Nephrology 803
Transcript of Familial hyperinsulinism and pancreatic β-cell ATP-sensitive potassium channels

Kidney International, Vol. 57 (2000), pp. 803–808
Familial hyperinsulinism and pancreatic b-cell ATP-sensitivepotassium channels
NIDHI SHARMA, ANA CRANE, GABRIELA GONZALEZ, JOSEPH BRYAN, andLYDIA AGUILAR-BRYAN
Departments of Medicine and Cell Biology, Baylor College of Medicine, Houston, Texas, USA
Familial hyperinsulinism and pancreatic b-cell ATP-sensitive shows an increased glycemic response due to increasedpotassium channels. Familial hyperinsulinism, also known as glycogen storage in the liver. After the diagnosis of PHHIpersistent hyperinsulinemic hypoglycemia of infancy (PHHI), has been established, immediate treatment is directedis a genetic disease characterized by mild to severe hypoglyce-
towards the maintenance of euglycemia usually by con-mia in the presence of inappropriately high levels of insulin.tinuous administration of intravenous glucose at ratesThe recessive form is caused by mutations in the adenosine
59-triphosphate (ATP)-sensitive K1 channel (KATP channel) between 15 and 20 mg/kg/min. If hypoglycemia persists,present in the plasma membrane of pancreatic b-cells. This the second line of treatment is the administration of com-channel is formed by two subunits, the high-affinity sulfonyl- pounds that inhibit insulin secretion. Two compounds,urea receptor, SUR1, and KIR6.2, a member of the inwardly
diazoxide and somatostatin (octreotide), are widely usedrectifying family of K1 channels. KATP channels regulate insulin[4]. If this clinical treatment fails to normalize glucosesecretion by linking membrane excitability with glucose metab-
olism. Approximately 50 mutations, in both channel subunits, levels a partial or subtotal pancreatectomy becomes thethat abolish or alter the regulation of b-cell KATP channels have treatment of choice [1]. Mild forms of the disease may gobeen identified in patients with the recessive form of PHHI. undiagnosed until eating habits change and an infant has
less frequent meals and thus becomes hypoglycemic. Di-azoxide or octreotide for a few months may be sufficient
Persistent hyperinsulinemic hypoglycemia of infancy to normalize glucose levels, and clinical remission of symp-(PHHI), also known as familial hyperinsulinism or nesi- toms with time has been observed [3]. In a follow-updioblastosis (OMIM:256450), is an inherited disorder of study on patients who were treated clinically, Leibowitzglucose metabolism that presents in newborns and in- et al have shown that although patients appear to go intofants, and is mainly characterized by inappropriately high remission, the beta cell defect remains and a significantinsulin levels in the presence of low levels of blood glu- number of these individuals become diabetic when theycose. PHHI was originally thought to be a relatively ho- reach puberty [5].mogenous disorder, but over the last several years an The frequency of the recessive form of PHHI in theunderlying heterogeneity has become clear [1]. It is now general population is low (1:50,000), but is reported tounderstood that PHHI can present with a quite variable be as high as 1:2500 in inbred populations with a highclinical picture, has at least two different histopathologic frequency of consanguineous marriages [6]. PHHI is ge-forms, can be inherited in either a recessive or dominant netically heterogeneous. Four genes have now been iden-manner, and can be caused by mutations in at least four tified to cause the disease, and in approximately 50% ofgenes [2]. the cases that have been screened for the known reces-
From the clinical point of view, some patients present sive and dominant genes, the mutations have not beenwith severe hypoglycemia almost immediately after birth, identified. Two mild dominant forms of PHHI have beenwhile others show mild hypoglycemia weeks or months described that are caused by mutations in the glucoki-after birth [3]. A biochemical diagnosis is based on ab- nase and glutamate dehydrogenase genes, respectively.normally high insulin levels in the presence of persisting Loss of function mutations in glucokinase have beenhypoglycemia, low ketone bodies (a result of their sup- identified as a cause of maturity-onset diabetes of thepression by elevated insulin), and a glucagon test that young, MODY2 [7, 8]. Interestingly, a point mutation,
V455 M, in glucokinase has now been identified as caus-ing one of the mild dominant forms of PHHI. This muta-Key words: insulin, potassium channel, sulfonylurea receptor, pan-
creas. tion produces an enzyme with a Km that is ,65% lowerin comparison with wild-type glucokinase (2.9 mmol/L vs. 2000 by the International Society of Nephrology
803

Sharma et al: Familial hyperinsulinism and KATP channels804
8.4 mmol/L). This better binding of glucose to glucoki- gene to the short arm of chromosome 11 (11p15.1). Thisnase results in insulin release at a lower blood glucose location was within the region where previous familyconcentration [9]. The second dominant form of PHHI studies by Ben Glaser, Heddy Landau, Alan Permutt [17,presents with asymptomatic hyperammonemia and hy- 18] and Pamela Thomas [19] had localized the gene(s) forpoglycemia [1]. Five mutations in the glutamate dehy- the recessive form of PHHI. Subsequent studies showeddrogenase gene have been identified that give this pheno- that the SUR1 and KIR6.2 genes were clustered in thistype [10]. These dominant forms of PHHI respond to region (Fig. 1). This cluster has been completely se-treatment with diazoxide indicating KATP channels are quenced and is available as part of the sequence of thefunctional. The recessive and most common form of the chromosome 11p14.3 PAC clone, pDJ239b22 (Genbankdisease is caused by mutations in SUR1 and KIR6.2, the accession #s AC003969 & U90583). This clone contains asubunits of the pancreatic b-cell ATP-sensitive K1 considerable amount of flanking sequence, which shouldchannel. facilitate investigation of the regulatory sequences that
From the histopathologic point of view, PHHI was control expression of these genes. The region specifyinginitially thought to result from nesidioblastosis following both genes spans ,90 Kb of DNA. SUR1 (OMIMthe report by Brown and Young of neoformation of 600509) encodes the high affinity sulfonylurea receptorislets in the pancreas of a newborn patient with severe (1581 or 1582 amino acids) [20]. The intronless KCNJ11hypoglycemia [11]. Nesidioblastosis was used to identify gene encoding the 390 amino acid inward rectifier, KIR6.2the disorder over the next decade, and it was not until (OMIM 600937), is 4900 base pairs 39 of the end of thethe early 1980s that Jaffe, Hashida and Yunis [12] and SUR1 gene [21]. A preliminary identification of the basalRahier et al [13], using specific staining techniques and promoter sequences is available [22]. We have comparedby studying age-matched controls, determined that nesi- the structure of the SUR1-KIR6.2 gene cluster with thedioblastosis was present in both hypoglycemic and con- SUR2-KIR6.1 gene cluster elsewhere [23].trol groups. Following these observations and confirma- A definitive connection between the recessive form oftion of the lack of specificity of nesidioblastosis, others PHHI and KATP channels was made by Dunne et al, whohave identified nesidioblastosis in diseases like MEN1, demonstrated the absence of ATP-sensitive K1 channelpancreatitis and cystic fibrosis. activity in the b-cells of a patient homozygous for a
Recent observations have identified at least two histo- mutation in exon 35 that resulted in truncation of SUR1pathologic forms of PHHI: focal and diffuse [14]. The in the second nucleotide binding fold [24]. The patientfocal form is described by the presence of a well defined was not responsive to diazoxide, requiring continuousarea within normal pancreatic tissue showing b-cells with infusion of glucose (18 mg/kg/min) to remain euglycemic.enlarged nuclei and increased cytoplasmic volume. En- Subtotal (95%) pancreatectomy did not significantly re-larged cells with similar morphology, indicative of in- duce insulin levels and removal of 99% of the pancreascreased metabolic and secretory activity, are widely scat- was necessary to control hypoglycemia. Electrical re-tered throughout the pancreas in the diffuse form of cording from isolated b-cells from this patient failed toPHHI. The differentiation of these two types is impor- show KATP channel activity while voltage-gated Ca21
tant as the focal form of the disease, present in ,30 to channels were spontaneously active. As in the five infants50% of cases that require surgery, responds well to par- studied earlier [25], b-cell cytosolic Ca21 levels were ele-tial rather than total pancreatectomy with the patient vated beyond control cell values (83 vs. 115 nmol/L) andbecoming euglycemic after removal of the hyperplastic this elevation was assumed to initiate insulin secretion.lesion. Considerable effort is being directed at under- A parallel mutation engineered into hamster SUR1 failedstanding the origin of the focal form of PHHI. SUR1 to generate KATP channel activity when cotransfected intoand KIR6.2 map to a region of chromosome 11, where COS cells with wild-type KIR6.2. Biochemical studies onother genes show loss of heterozygosity as a result of
the parallel mutation showed the truncated receptor was“imprinting.” In some cases of the recessive form of
produced and retained high affinity sulfonylurea bindingPHHI, loss of heterozygosity appears to result from a lossactivity. Preliminary results indicate that the truncatedof the maternal allele through a somatic deletion. PHHIreceptor is able to associate with and cophotolabel KIR6.2.can result when apparent homozygosity is achieved by
For the KIR6.2 gene, three mutations have been identi-combination of this imprinting effect with a genomicfied that cause PHHI (Fig. 2). Thomas, Ye and Lightnermutation in either of the paternal SUR1 alleles. At thisfirst reported a KIR6.2 mutation, a leu→pro change,time, no mutations in KIR6.2 have been found that reachL147P, near the extracellular side of the second trans-the homozygous state by this mechanism [15, 16].membrane helix (M2), to cause PHHI [26]. This mutationwas identified in a child of Iranian origin, the progeny
MUTATIONS IN SUR1 AND KIR6.2 of a first cousin marriage. Diagnosis of PHHI was basedon an insulin level of .30 mU/mL with a glucose levelThe first suggestion that the recessive form of PHHI
might be a channelopathy was the mapping of the SUR1 ,30 mg/dL and a requirement of .15 mg glucose kg/min

Sharma et al: Familial hyperinsulinism and KATP channels 805
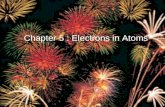
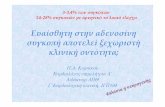
Fig. 1. Human SUR1-KIR6.2 gene cluster. The 39 exons of the SUR1 gene are represented by the numbered light and dark boxes. The numbersabove each exon indicate the exon size in base pairs. NBF1 and NBF2 mark the nucleotide binding folds and their corresponding Walker A andB motifs. The intronless KIR6.2 lies 39 of SUR1 as shown.
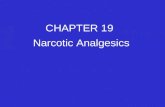
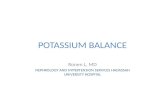
Fig. 2. Human KIR6.2 gene mutations. A sche-matic representation of KIR6.2 in the plasmamembrane positioning the three known muta-tions. The M1 and M2 identify the transmem-brane helices. The H5 region identifies the K1
selective pore. (Figure modified from [2]; usedwith permission).
to maintain euglycemia. Substitution of this proline into coexpressed with wild-type SUR1, KIR6.2W91R failed toM2 abolishes KATP channel activity when it is engineered produce active channels.into KIR6.2 and expressed with wild-type SUR1. It is not Fifty mutations in the SUR1 gene have been identifiedclear if KIR6.2L147P can fold correctly and assemble with in PHHI patients. These mutations can be divided intoSUR1, as we have been unable to show co-photolabeling two main groups based on the severity of the diseasewith 125I-iodoazidoglibenclamide (Aguilar-Bryan, unpub- (Fig. 3). Point mutations that result in amino acid substi-lished data). tutions can produce mild forms of the disorder, while
Nestorowicz et al described a nonsense mutation in nonsense mutations or those that alter splice sites andKIR6.2 that truncated the protein after 12 amino acids, result in truncation of the receptor are associated withY12X [27]. The patient was homozygous for this muta- severe cases.tion. When Y12X was engineered into KIR6.2, as ex-pected for a 12 residue peptide that is missing all of the
THE G1479R MUTATION IS AN EXAMPLE OFelements required to form the K1 channel pore, it didTHE MILD FORMnot form a functional channel when coexpressed with
Studies on cells expressing the G1479R missense mu-wild-type SUR1.tant of SUR1, identified in a patient with a mild case ofSharma and Aguilar-Bryan have identified a thirdfamilial hyperinsulinism, suggests adenosine 59-diphos-KIR6.2 mutant, a trp→arg change, W91R, near the exter-phate (ADP) rather than ATP is the physiologic regulatornal side of M1 (unpublished data). This mutation wasof KATP channels [28]. This mutation in NBF2 was identi-identified in a newborn, the product of a first cousinfied by Dr. Ann Nestorowicz in Dr. Alan Permutt’s labo-marriage of Palestinian descent. Clinical treatment withratory in a patient of Iraqi and Moroccan Jewish extrac-diazoxide and somatostatin was not successful and a par-tion diagnosed with PHHI by Drs. Heddy Landau andtial pancreatectomy was performed at two weeks of age;
a second resection was necessary four weeks later. When Benjamin Glaser (Hebrew University, Hadassah Medi-

Sharma et al: Familial hyperinsulinism and KATP channels806
Fig. 3. Human SUR1 gene mutations. A schematic representation of SUR1 and the SUR1 gene is shown. The receptor is on the top with thepredicted transmembrane domains (shaded boxes) and nucleotide binding folds illustrated for reference. The gene structure is given below. Theapproximate positions of mutations within exons are shown, while the mutations within introns are given in italics at the bottom of the graphic(figure modified from [2]; used with permission).
cal Center, Jerusalem). The patient is a compound het- TRUNCATIONS OF SUR1 MAY RESULT INDEFECTIVE TRAFFICKING OF KATPerozygote, with the G1479R allele on one chromosomeCHANNEL SUBUNITSand a second, unidentified allele on the other. In excised
membrane patches MgADP antagonizes the inhibitory A number of mutations identified with severe casesof PHHI cause truncation of the receptor. As noted aboveaction of ATP on KATP channels. In the G1479R channelsfor the exon 35 mutation reconstitution of the engineeredthis antagonizing action is strongly reduced [28]. Co-mutant receptor with wild-type KIR6.2 does not produceexpression of SUR1G1479R with wild-type KIR6.2 producesactive KATP channels. The reason for this failure is notK1 channels that are inhibited by ATP 42, or MgATP,clear. We have looked at recombinant receptors engi-in excised patches with nearly the same IC50 as native orneered with smaller truncations (one example with 49wild-type reconstituted channels; however, these channelsamino acids truncated from the SUR1 C-terminus is shown
are poorly activated by MgADP [28]. The SUR1G1479R/ in Fig. 4) in order to determine whether smaller deletionsKIR6.2 channels are also poorly activated by conditions can be tolerated without loss of channel function. 86Rb1
of metabolic inhibition that strongly activate wild-type efflux data (Fig. 4A) show that deletion of 49 aminochannels. We have concluded that in PHHI b-cells the acids from the C-terminus of SUR1 reduces channelG1479R channels are blocked by ATP and apparently activity to background levels equivalent to that observedfail to respond to fluctuations in ADP. The result implies with SUR1 or KIR6.2 alone [21]. Comparison of the pho-
tolabeling pattern of the SUR1DC49 receptor with andthat fluctuations of [ATP]i alone are not sufficient towithout KIR6.2 indicates the truncated receptors havetrigger insulin secretion in either the recombinant chan-not undergone maturation. This result suggests that trun-nels during metabolic inhibition or in PHHI patients andcation of the C-terminus of SUR1 interferes with traf-indicate ADP is a critical factor. Approximately 25% officking of the channel complex to the plasma membrane.the mutations identified in recessive cases of PHHI ap-
pear to have lost this stimulatory response to ADPSUMMARY[2, 29]. Patients with these SUR1 mutations usually re-
spond well to a high carbohydrate diet, diazoxide or It is now understood that mutations in SUR1 andKIR6.2 can result in the loss of KATP channel activity inoctreotide treatment.

Sharma et al: Familial hyperinsulinism and KATP channels 807
pancreatic b-cells and cause a recessive form of PHHI.These results emphasize the important role of ionicmechanisms in control of insulin secretion. Efforts tounderstand how individual mutations result in loss ofchannel activity provide insight into the molecular mech-anism(s) of regulation of this family of channels andtheir expression on the cell surface.
ACKNOWLEDGMENTS
This work was supported by grants from the American DiabetesAssociation (ADA) to Dr. Aguilar-Bryan, and NIH grants DK44311,DK50750, and DK52771 to Dr. J. Bryan. Dr. Aguilar-Bryan is a T.C.Chao Scholar. We thank Li-Zhen Song for technical assistance, andother members of the Baylor group for encouragement.
Reprint requests to Lydia Aguilar-Bryan, M.D., Ph.D., Division ofEndocrinology, Baylor College of Medicine, One Baylor Plaza 537E,Houston, TX 77030, USA.E-mail: [email protected]
REFERENCES
1. Stanley CA: Hyperinsulinism in infants and children. PediatricClinics North Am 44:363–374, 1997
2. Aguilar-Bryan L, Bryan J: The molecular biology of ATP-sensi-tive potassium channels. Endocrine Rev 20:101–135, 1999
3. Permutt MA, Nestorowicz A, Glaser B: Familial hyperinsulin-ism: An inherited disorder of spontaneous hypoglycemia in neo-nates and infants. Diabetes Rev 4:347–355, 1996
4. Glaser B, Hirsch HJ, Landau H: Persistent hyperinsulinemichypoglycemia of infancy: Long-term octreotide treatment withoutpancreatectomy. J Pediatr 123:644–650, 1993
5. Leibowitz G, Glaser B, Higazi AA, Salameh M, Cerasi E, Lan-dau H: Hyperinsulinemic hypoglycemia of infancy (nesidi-oblastosis) in clinical remission: High incidence of diabetes mellitusand persistent b-cell dysfunction at long-term follow-up. J ClinEndo Metab 80:386–392, 1995
6. Mathew PM, Young JM, Abu-Osba YK, Mulhern BD, HamoudiS, Hamadan JA, Sa’di AR: Persistent neonatal hyperinsulinism.Clin Pediatr (Phila) 27:148–151, 1988
7. Stoffel M, Patel P, Lo YM, Hattersley AT, Lucassen AM,Page R, Bell JI, Bell GI, Turner RC, Wainscoat JS: Missenseglucokinase mutation in maturity-onset diabetes of the young andmutation screening in late-onset diabetes. Nat Genet 2:153–156,1992
8. Velho G, Froguel P: Genetic determinants of non-insulin-depen-dent diabetes mellitus: Strategies and recent results. Diabetes Me-tabolism 23:7–17, 1997
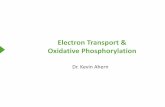
Fig. 4. Comparison of channel activity and [125I]-iodoazidoglibenclam-ide labeling of wild-type and truncated SUR1/KIR6.2 complexes. (A)Relative KATP channel activity was measured by 86Rb1 efflux as describedpreviously [21, 30]. The wild-type channels (h) show a robust effluxupon metabolic poisoning, while the SUR1DC49/KIR6.2 channels (s)show no activity above background. (B) Pattern of [125I]-iodoazidoglibe-nclamide photolabeling of membranes isolated from COSm6 trans-fected, as described in Clement et al [30], with the indicated plasmids.The mature, complex glycosylated form of SUR1 associated with surfaceexpression of active channels [30; reviewed in 23] is present when SUR1,but not SUR1DC49, is coexpressed with wild-type KIR6.2. Similarly,cophotolabeling of KIR6.2, indicative of coassembly of SUR1 and KIR6.2[30; reviewed in 23] is observed when both SUR1 and SUR1DC49 arecoexpressed with KIR6.2. The immature, core glycosylated form of SUR1is present in both the SUR1 and SUR1DC49 samples. The 1 and 2 lanesindicate the presence or absence of 1 mmol/L unlabeled glibenclamide toshow specificity of labeling of SUR1 and KIR6.2.

Sharma et al: Familial hyperinsulinism and KATP channels808
9. Glaser B, Kesavan P, Heyman M, Davis E, Cuesta A, Buchs 19. Thomas PM, Cote GJ, Hallman DM, Mathew PM: Homozygositymapping of the gene for familial persistent hyperinsulinemic hypo-A, Stanley CA, Thornton PS, Permutt MA, Matschinsky FM,
Herold K: Familial hyperinsulinism caused by an activating glu- glycemia of infancy to chromosome 11p. Am J Hum Genet 56:416–421, 1995cokinase mutation. N Engl J Med 338:226–230, 1998
10. Stanley CA, Lieu YK, Hsu BY, Burlina AB, Greenberg CR, 20. Aguilar-Bryan L, Nichols CG, Wechsler SW, Clement JP IV,Boyd AE III, Gonzalez G, Herrera-Sosa H, Nguy K, Bryan J,Hopwood NJ, Perlman K, Rich BH, Zammarchi E, Poncz M:
Hyperinsulinism and hyperammonemia in infants with regulatory Nelson DA: Cloning of the beta cell high-affinity sulfonylureareceptor: A regulator of insulin secretion. Science 268:423–426,mutations of the glutamate dehydrogenase gene. N Engl J Med
338:1352–1357, 1998 199521. Inagaki N, Gonoi T, Clement JP IV, Namba N, Inazawa J, Gon-11. Brown RE, Young RB: A possible role for the exocrine pancreas
in the pathogenesis of neonatal leucine-sensitive hypoglycemia. zalez G, Aguilar-Bryan L, Seino S, Bryan J: Reconstitution ofIKATP: An inward rectifier subunit plus the sulfonylurea receptor.Am J Dig Dis 15:65–72, 1970
12. Jaffe R, Hashida Y, Yunis EJ: Pancreatic pathology in hyperinsu- Science 270:1166–1170, 199522. Ashfield R, Ashcroft SJ: Cloning of the promoters for the beta-linemic hypoglycemia of infancy. Lab Invest 42:356–365, 1980
13. Rahier J, Falt K, Muntefering H, Becker K, Gepts W, Falkmer cell ATP-sensitive K-channel subunits Kir6.2 and SUR1. Diabetes47:1274–1280, 1998S: The basic structural lesion of persistent neonatal hypoglycaemia
with hyperinsulinism: Deficiency of pancreatic D cells or hyperac- 23. Aguilar-Bryan L, Clement JP IV, Gonzalez G, Kunjilwar K,Babenko A, Bryan J: Towards understanding the assembly andtivity of B cells? Diabetologia 26:282–289, 1984
14. Goossens A, Gepts W, Saudubray JM, Bonnefont JP, Nihoul structure of KATP channels. Physiol Rev 78:227–245, 199824. Dunne MJ, Kane C, Shepherd RM, Sanchez JA, James RFL,F, Heitz PU, Kloppel G: Diffuse and focal nesidioblastosis. A
clinicopathological study of 24 patients with persistent neonatal Johnson PRV, Aynsley-Green A, Lu S, Clement IVJP, LindleyKJ, Seino S, Aguilar-Bryan L: Familial persistent hyperinsulin-hyperinsulinemic hypoglycemia. Am J Surg Pathol 13:766–775,
1989 emic hypoglycemia of infancy and mutations in the sulfonylureareceptor. N Engl J Med 336:703–706, 199715. de Lonlay P, Fournet J, Rahier J, Gross-Morand M, Poggi-
Travert F, Foussier V, Bonnefont J, Brusset M, Brunelle F, 25. Kane C, Shepherd RM, Squires PE, Johnson PR, James RF,Milla PJ, Aynsley-Green A, Lindley KJ, Dunne MJ: Loss ofRobert J, Nihoul-Fekete CJS, Junien C: Somatic deletion of the
imprinted 11p15 region in sporadic persistent hyperinsulinemic functional KATP channels in pancreatic beta-cells causes persistenthyperinsulinemic hypoglycemia of infancy. Nat Med 2:1344–1347,hypoglycemia of infancy is specific of focal adenomatous hyperpla-
sia and endorses partial pancreatectomy. J Clin Invest 100:802–807, 199626. Thomas P, Ye Y, Lightner E: Mutations of the pancreatic islet1997
16. Verkarre V, De Fournet JC, Lonlay P, Gross-Morand MS, inward rectifier also lead to familial persistent hyperinsulinemichypoglycemia of infancy. Hum Mol Genet 5:1809–1812, 1996Devillers M, Rahier J, Brunelle F, Robert JJ, Nihoul-Fekete
C, Saudubray JM, Junien C: Paternal mutation of the sulfonylurea 27. Nestorowicz A, Inagaki N, Gonoi T, Schoor KP, Wilson BA,Glaser B, Landau H, Stanley CA, Thornton PS, Seino S, Per-receptor (SUR1) gene and maternal loss of 11p15 imprinted genes
lead to persistent hyperinsulinism in focal adenomatous hyperpla- mutt MA: A nonsense mutation in the inward rectifier potassiumchannel gene, Kir6.2, is associated with familial hyperinsulinism.sia. J Clin Invest 102:1286–1291, 1998
17. Glaser B, Chiu KC, Anker R, Nestorowicz A, Landau H, Ben- Diabetes 46:1743–1748, 199728. Nichols CG, Shyng SL, Nestorowicz A, Glaser B, ClementBassat H, Shlomai Z, Kaiser N, Thornton PS, Stanley CA,
Spielman RS, Gogolin-Ewens K, Cerasi E, Baker L, Rice J, JP IV, Gonzalez G, Aguilar-Bryan L, Permutt MA, BryanJ: Adenosine diphosphate as an intracellular regulator of insulinDonis-Keller H, Permutt MA: Familial hyperinsulinism maps to
chromosome 11p14–15.1, 30 cM centromeric to the insulin gene. secretion. Science 272:1785–1787, 199629. Shyng SL, Ferrigni T, Shepard JB, Nestorowicz A, Glaser B,Nat Genet 7:185–188, 1994
18. Glaser B, Chiu KC, Liu L, Anker R, Nestorowicz A, Cox NJ, Permutt MA, Nichols CG: Functional analyses of novel mutationsin the sulfonylurea receptor 1 associated with persistent hyperinsu-Landau H, Kaiser N, Thornton PS, Stanley CA, Cerasi E,
Baker L, Donis-Keller H, Permutt MA: Recombinant mapping linemic hypoglycemia of infancy. Diabetes 47:1145–1151, 199830. Clement JP IV, Kunjilwar K, Gonzalez G, Schwanstecher M,of the familial hyperinsulinism gene to an 0.8 cM region on chromo-
some 11p15.1 and demonstration of a founder effect in Ashkenazi Panten U, Aguilar-Bryan L, Bryan J: Association and stoichiom-etry of KATP channel subunits. Neuron 18:827–838, 1997Jews. Hum Mol Genet 4:879–886, 1995