Exploratory associations with Tumor Necrosis Factor-α, disinhibition and suicidal endorsement after...
10
Exploratory associations with Tumor Necrosis Factor-a, disinhibition and suicidal endorsement after traumatic brain injury S.B. Juengst a , R.G. Kumar a , P.M. Arenth a , A.K. Wagner a,b,c,⇑ a Dept. Physical Medicine and Rehabilitation, University of Pittsburgh, United States b Center for Neuroscience, University of Pittsburgh, United States c Safar Center for Resuscitation Research, University of Pittsburgh, United States article info Article history: Received 7 March 2014 Received in revised form 1 May 2014 Accepted 8 May 2014 Available online xxxx Keywords: Brain injury Depression Inflammation Suicide Tumor Necrosis Factor-Alpha Disinhibition Impulsivity abstract Purpose: To examine the relationship of Tumor Necrosis Factor (TNF)-a to disinhibition and suicidal endorsement after traumatic brain injury (TBI). Participants: Adults with moderate to severe TBI (acute serum levels: n = 48, n = 543 samples; acute CSF levels: n = 37, n = 389 samples; chronic serum levels: n = 48, n = 326 samples). Main measures: TNFa levels (CSF, Serum) from time of injury to 12 months post-injury; Frontal Systems Behavior Scale – Disinhibition Subscale at 6 and 12 months post-injury; Patient Health Questionnaire at 6 and 12 months post-injury. Results: Participants with TBI had significantly higher CSF and serum TNFa levels than healthy controls (p < 0.05). Acute and chronic serum TNFa was significantly associated with disinhibition at 6 months post-injury (p = 0.009, p = 0.029 respectively), and 6 month disinhibition was associated with suicidal endorsement at both 6 and 12 months (p = 0.045, p = 0.033 respectively) and disinhibition at 12 months post-injury (p < 0.001). Conclusion: These preliminary data suggest a biological to behavioral pathway of suicidality after TBI, from TNFa to disinhibition to suicidal endorsement. Future investigation is warranted to validate these findings and clarify what biological mechanisms might underlie these relationships. Ó 2014 Elsevier Inc. All rights reserved. 1. Introduction Traumatic brain injury (TBI) induces many biological, cognitive, and behavioral changes that can result in poor functional and psy- chological outcomes. Among the more serious potential conse- quences is an increased risk for suicide. Individuals with TBI are 3–4 times more likely to die as a result of suicide than those in the general population (Harrison-Felix et al., 2009; Simpson and Tate, 2007; Teasdale and Engberg, 2001). A review of the literature suggests that most studies report suicidal ideation in over 10% of individuals after TBI, and suicidal ideation is associated with a 5 times higher likelihood of suicide attempt (Simpson and Tate, 2007). This increased risk persists for 15 years or longer after injury (Reeves and Laizer, 2012; Wasserman et al., 2008), suggesting that there are chronic contributing factors to this increased suicidal risk after TBI. Other symptomatic and behavioral risk factors for suicidality in the general population include depression (or other psychiatric disorder), aggression, poor cognitive inhibition, and impulsivity (Bertolote et al., 2003; Fountoulakis et al., 2004; Giegling et al., 2009; Lynch et al., 2004; Okusaga and Postolache, 2012). These risk factors are also observed among the long-term sequelae associated with TBI (Brown et al., 2011), providing a pos- sible explanation for the increased risk of suicidality after injury. Indeed, similar risk factors have been identified for suicidality after TBI, including depression, substance use, aggression, poor cogni- tion, and impulsivity (Brenner et al., 2009; Hesdorffer et al., 2009; Homaifar et al., 2012; Reeves and Laizer, 2012; Simpson and Tate, 2007; Wasserman et al., 2008). If suicidal risk after injury could be identified early, intensive tracking of suicidal ideation and other risk factors could be implemented, and suicidal risk might be reduced through screening and early intervention. However, inten- sive tracking of this nature is not feasible for all individuals who have sustained a TBI. Therefore, it is critical to identify not only which symptomatic and behavioral risk factors to track after injury, but also effective ways to determine, near the time of injury, who is at high risk for suicidal ideation and/or behavioral/symptomatic http://dx.doi.org/10.1016/j.bbi.2014.05.020 0889-1591/Ó 2014 Elsevier Inc. All rights reserved. ⇑ Corresponding author at: Dept. Physical Medicine and Rehabilitation, Univer- sity of Pittsburgh, 3471 Fifth Avenue, Suite 202, Pittsburgh, PA 15213, United States. Tel.: +1 412 648 6666; fax: +1 4126924354. E-mail address: [email protected] (A.K. Wagner). Brain, Behavior, and Immunity xxx (2014) xxx–xxx Contents lists available at ScienceDirect Brain, Behavior, and Immunity journal homepage: www.elsevier.com/locate/ybrbi Please cite this article in press as: Juengst, S.B., et al. Exploratory associations with Tumor Necrosis Factor-a, disinhibition and suicidal endorsement after traumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016/j.bbi.2014.05.020
Transcript of Exploratory associations with Tumor Necrosis Factor-α, disinhibition and suicidal endorsement after...

Brain, Behavior, and Immunity xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Brain, Behavior, and Immunity
journal homepage: www.elsevier .com/locate /ybrbi
Exploratory associations with Tumor Necrosis Factor-a, disinhibitionand suicidal endorsement after traumatic brain injury
http://dx.doi.org/10.1016/j.bbi.2014.05.0200889-1591/� 2014 Elsevier Inc. All rights reserved.
⇑ Corresponding author at: Dept. Physical Medicine and Rehabilitation, Univer-sity of Pittsburgh, 3471 Fifth Avenue, Suite 202, Pittsburgh, PA 15213, United States.Tel.: +1 412 648 6666; fax: +1 4126924354.
E-mail address: [email protected] (A.K. Wagner).
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations with Tumor Necrosis Factor-a, disinhibition and suicidal endorsemetraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016/j.bbi.2014.05.020
S.B. Juengst a, R.G. Kumar a, P.M. Arenth a, A.K. Wagner a,b,c,⇑a Dept. Physical Medicine and Rehabilitation, University of Pittsburgh, United Statesb Center for Neuroscience, University of Pittsburgh, United Statesc Safar Center for Resuscitation Research, University of Pittsburgh, United States
a r t i c l e i n f o a b s t r a c t
Article history:Received 7 March 2014Received in revised form 1 May 2014Accepted 8 May 2014Available online xxxx
Keywords:Brain injuryDepressionInflammationSuicideTumor Necrosis Factor-AlphaDisinhibitionImpulsivity
Purpose: To examine the relationship of Tumor Necrosis Factor (TNF)-a to disinhibition and suicidalendorsement after traumatic brain injury (TBI).Participants: Adults with moderate to severe TBI (acute serum levels: n = 48, n = 543 samples; acute CSFlevels: n = 37, n = 389 samples; chronic serum levels: n = 48, n = 326 samples).Main measures: TNFa levels (CSF, Serum) from time of injury to 12 months post-injury; Frontal SystemsBehavior Scale – Disinhibition Subscale at 6 and 12 months post-injury; Patient Health Questionnaire at 6and 12 months post-injury.Results: Participants with TBI had significantly higher CSF and serum TNFa levels than healthy controls(p < 0.05). Acute and chronic serum TNFa was significantly associated with disinhibition at 6 monthspost-injury (p = 0.009, p = 0.029 respectively), and 6 month disinhibition was associated with suicidalendorsement at both 6 and 12 months (p = 0.045, p = 0.033 respectively) and disinhibition at 12 monthspost-injury (p < 0.001).Conclusion: These preliminary data suggest a biological to behavioral pathway of suicidality after TBI,from TNFa to disinhibition to suicidal endorsement. Future investigation is warranted to validate thesefindings and clarify what biological mechanisms might underlie these relationships.
� 2014 Elsevier Inc. All rights reserved.
1. Introduction
Traumatic brain injury (TBI) induces many biological, cognitive,and behavioral changes that can result in poor functional and psy-chological outcomes. Among the more serious potential conse-quences is an increased risk for suicide. Individuals with TBI are3–4 times more likely to die as a result of suicide than those inthe general population (Harrison-Felix et al., 2009; Simpson andTate, 2007; Teasdale and Engberg, 2001). A review of the literaturesuggests that most studies report suicidal ideation in over 10% ofindividuals after TBI, and suicidal ideation is associated with a 5times higher likelihood of suicide attempt (Simpson and Tate,2007). This increased risk persists for 15 years or longer after injury(Reeves and Laizer, 2012; Wasserman et al., 2008), suggesting thatthere are chronic contributing factors to this increased suicidal riskafter TBI. Other symptomatic and behavioral risk factors for
suicidality in the general population include depression (or otherpsychiatric disorder), aggression, poor cognitive inhibition, andimpulsivity (Bertolote et al., 2003; Fountoulakis et al., 2004;Giegling et al., 2009; Lynch et al., 2004; Okusaga and Postolache,2012). These risk factors are also observed among the long-termsequelae associated with TBI (Brown et al., 2011), providing a pos-sible explanation for the increased risk of suicidality after injury.Indeed, similar risk factors have been identified for suicidality afterTBI, including depression, substance use, aggression, poor cogni-tion, and impulsivity (Brenner et al., 2009; Hesdorffer et al., 2009;Homaifar et al., 2012; Reeves and Laizer, 2012; Simpson and Tate,2007; Wasserman et al., 2008). If suicidal risk after injury couldbe identified early, intensive tracking of suicidal ideation and otherrisk factors could be implemented, and suicidal risk might bereduced through screening and early intervention. However, inten-sive tracking of this nature is not feasible for all individuals whohave sustained a TBI. Therefore, it is critical to identify not onlywhich symptomatic and behavioral risk factors to track after injury,but also effective ways to determine, near the time of injury, who isat high risk for suicidal ideation and/or behavioral/symptomatic
nt after

2 S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx
risk factors (e.g. depression, disinhibition) closely linked tosuicidality.
1.1. Disinhibition
While psychiatric disorders such as depression may be the mostrelevant risk factor for suicidality (Bertolote et al., 2003), this factoralone does not explain the multifold increase in suicidality riskafter TBI, compared to the general population. There is ample evi-dence that impulsivity and poor cognitive inhibition also contrib-ute to increased suicidality risk after TBI (Brenner et al., 2009;Hesdorffer et al., 2009; Homaifar et al., 2012; Reeves and Laizer,2012; Simpson and Tate, 2007; Wasserman et al., 2008). Disinhibi-tion, a broader term that incorporates impulsivity and poorcognitive inhibition, occurs frequently after TBI (Ciurli et al.,2011) and may be a candidate behavioral biomarker of increasedsuicidality risk in TBI compared to the general population. Preli-minary evidence suggests that disinhibition after TBI may be adirect consequence of the neurobiological processes – frontal lobedysfunction and white matter changes, axonal damage in mono-aminergic pathways – that occur after injury (Kim, 2002; Lux,2007; Yurgelun-Todd et al., 2011). Evidence linking disinhibitionto changes in white matter microstructure suggests a potentialinflammatory-induced neurobiological vulnerability to disinhibi-tion as a result of injury (Yurgelun-Todd et al., 2011). As such, earlyinflammatory profiles after TBI may serve as vulnerability bio-markers for disinhibition that could be determined near time ofinjury and could help identify those at greatest risk for developingdisinhibition.
1.2. Suicidality
There is increasing evidence that biological factors may contrib-ute to suicidality in other populations (Dombrovski et al., 2013;Fountoulakis et al., 2004; Lee et al., 2009; Matthews et al., 2012;McGirr et al., 2010; Saiz et al., 2011; Serafini et al., 2013; Steineret al., 2013), though it cannot be assumed that these biologicalmechanisms would contribute to suicidality after TBI; biologicalcontributors to depression, for example, may be different afterTBI than in the general population (Failla et al., 2013; Fann et al.,2009). Research specifically investigating neurobiological corre-lates of suicidality after TBI is limited. Furthermore, findings fromother populations do not explain the significantly higher suiciderisk observed after TBI. Some of the same increased inflammatorycytokines observed after TBI, such as Tumor Necrosis Factor (TNF)-a and IL-6, as well as glial cell activation, are associated with suici-dality in the general population (Serafini et al., 2013), regardless ofpsychiatric diagnosis (Steiner et al., 2013). Studies among veteranswith TBI suggest that thalamic dysfunction and enlargement andwhite matter degeneration may be radiographic biomarkers ofsuicidality (Lopez-Larson et al., 2013; Yurgelun-Todd et al.,2011), though identification of these biomarkers requires complexand costly neuroimaging. To date, no studies have assessed inflam-mation as a potential biomarker of suicidality after TBI.
1.3. TNFa
Several studies in the general population have demonstrated anassociation between suicidal ideation, attempt, or completion andTNFa levels (Janelidze et al., 2011; O’Donovan et al., 2013; Pandeyet al., 2012; Serafini et al., 2013) or TNFa gene polymorphisms(Kim et al., 2013; Omrani et al., 2009). TNFa, among other inflam-matory biomarkers, is produced as part of the inflammatory pro-cess that occurs early after TBI (Frugier et al., 2010; Namas et al.,2009; Woodcock and Morganti-Kossmann, 2013). Preliminarywork examining TNF antagonists in TBI found that they may be
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016
beneficial for improving depressive symptoms among those withhigh acute inflammatory biomarkers (Raison et al., 2013), suggest-ing a role for TNFa in post-traumatic depression, which is itself arisk factor for suicidality. Furthermore, TNFa, particularly in theCSF, has been linked to chronic microglial activation (Bennettet al., 2009) and white matter degeneration (Tarkowski et al.,2003), which reportedly contributes to disinhibition after TBI(Yurgelun-Todd et al., 2011), suggesting that TNFa may be a candi-date biomarker for both disinhibition and suicidality after TBI.
While these findings implicate TNFa as a potential candidatebiomarker for disinhibition and suicidality after TBI, this associa-tion has yet to be specifically investigated. Thus, the purpose of thisstudy was to assess a candidate biomarker for disinhibition andsuicidal endorsement after TBI, using the context of a Rehabilomicsframework (Wagner, 2011), which models relationships amongindividual biological and behavioral susceptibility, health condi-tion (TBI), and outcomes. Specifically, we investigated whetherTNFa measured acutely in CSF and serum, as well as chronicallyin serum, was associated with disinhibition and suicidal endorse-ment at 6 and 12 months post-injury. We hypothesized thatgreater disinhibition would be significantly associated with sui-cidal endorsement at both 6 and 12 months post-injury. Buildingon our previous work investigating inflammation and mood afterTBI (Juengst et al., 2014), we hypothesized that higher acute TNFalevels in the CSF would be associated with suicidal endorsement.We also explored how acute and chronic serum TNFa levels con-tributed to disinhibition and suicidal endorsement at 6 and12 months post-injury. Based on our findings, we propose a datadriven, conceptual pilot model for how this inflammatory cytokinemay influence disinhibition and suicidality.
2. Methods
2.1. Participants
Participants with moderate to severe TBI who survived their ini-tial injuries (n = 74) were recruited from a University-affiliatedLevel 1 Trauma Center, Neurotrauma Intensive Care Unit. Informedconsent was obtained from the designated proxy. Participantswere included in the study if they: (i) were between 16 and70 years old; (ii) had an initial GCS score 612; and (iii) had positivefindings on a head Computed Tomography (CT) scan consistentwith TBI. All study procedures were approved by our UniversityInstitutional Review Board.
As a comparison group, CSF samples from 15 healthy adult con-trols (n = 8 men, n = 7 women; median age 22 years) and serumsamples from 15 healthy adult controls (n = 6 men and n = 9women; median age 21 years), were collected. Control CSF wasobtained via lumbar puncture for research purposes. Controls werebetween 18 and 70 years old with no current or past history ofbrain injury, neurological disease, or bleeding disorder. For bothcontrols and participants with TBI, women were excluded if theywere pregnant, taking oral contraceptives, on hormone replace-ment therapy, or had any history of reproductive or endocrinedisorders.
2.2. CSF and serum TNFa collection
Acute CSF samples were collected up to 2 times daily (morningand evening) for up to six days after injury via an extraventriculardrain, initially placed as part of routine clinical care for individualswith severe TBI. CSF samples were stored at 4 �C until processingand were later centrifuged, aliquoted, and stored at �80 �C untilbatch analysis. Acute serum samples were collected as able (basedon stable medical state) each morning during the first week
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement after/j.bbi.2014.05.020

S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx 3
post-injury. Chronic serum samples were collected up to every twoweeks for six months post-injury, and another sample was col-lected at 12 months post-injury for participants with severe TBI.Upon collection and centrifugation, samples were aliquoted andstored at �80 �C until the time of assay. Serum and CSF TNFawas measured using a Luminex™ bead array assay (Millipore,Billerica, Massachusetts). The minimum detectable concentrationsreported for this Human, High-sensitivity assay—(catalog number:HSCYTO-60SK) is TNFa: 0.05 pg/ml. The intra-plate % coefficient ofvariance (CV) was 3.49%, while the inter-plate % CV was 3.78%.Inflammatory biomarker data generated from acute serum andCSF samples were scaled prior to analysis due to recognized vari-ability between assay kits and across sample plates. The scalingprocedure utilized both concentration standards (CS) and qualitycontrol (QC) samples duplicated across plates. Both CS and QCwere used such that the set of data was not shifted and the scalingprocess did not change the scale as a whole. Chronic serum sam-ples with levels that were undetectable (low) by the assay wereassigned values of 0.0001 pg/ml.
2.3. Demographic and injury data
Demographic and injury-related data were collected throughinterview with participants, family members, and through medi-cal chart review. Glasgow Coma Scale (GCS) scores for data anal-ysis were obtained by trained clinical ICU staff and represent thebest GCS score in the first 24 h post-injury. To characterize thecognitive impairment of participants, and to assess whether cog-nitive impairment differed by suicidality, overall cognitive impair-ment was assessed via neuropsychological test performance at 6and 12 months post-injury; this battery included the Trail MakingTest (TMT) A (Reitan, 1955), TMT B (Reitan, 1955), the ControlledOral Word Association (COWA) (Iverson et al., 1999), the Califor-nia Verbal Learning Test (CVLT) (Wiegner and Donders, 1999),the Stroop Interference Test (Strong et al., 2011), and the Delis-Kaplan Executive Function System-Verbal Fluency (Strong et al.,2011), representing multiple cognitive domains (speed of process-ing, memory, attention, executive function) affected by injury. Acognitive composite score was generated to represent overall cog-nition for each individual by averaging T-scores, normalized basedon age, sex, race, and years of education, across all completedtests. This method has been established previously as a reliablemethod of analyzing cognitive performance after brain injury(Green et al., 2008; Hart et al., 2005; Hartikainen et al., 2010;Wagner et al., 2012). Not all participants completed every testat 6 or 12 months, so composite scores were calculated only forthose who completed at least one test in each of the four differentcognitive domains.
2.4. Primary measures
Suicidal endorsement, or suicidality, was assessed by thePatient Health Questionnaire (PHQ)-9, a 9-question diagnosticsymptom questionnaire based on the DSM-IV criteria for MDD.The PHQ-9, validated for use after TBI (Fann et al., 2005), wasadministered to participants at 6 and 12 months after injury. Par-ticipants who endorsed a score of 1 or higher on question 9(thoughts that you would be better off dead, or of hurting yourself)were categorized as having suicidal endorsement. Use of single sui-cide items from broader depression scales has demonstrated valid-ity as a research measure of suicidal ideation (Desseilles et al.,2012). Furthermore, question 9 on the PHQ-9 is consistent withthe Self Directed Violence Classification System’s definition of sui-cidal ideation as ‘‘thoughts of engaging in suicidal behaviors wherethe individual has thoughts of suicide (a) without intent, (b) withan undetermined degree of suicidal intent, or (c) with some intent
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016/
(‘‘Self-Directed Violence Classification System,’’ n.d.)’’. The PHQ-9also served as a measure of depression status at 6 and 12 monthspost-injury. Participants were classified as having depression ifthey endorsed depressed mood or lack of interest and an overallminimum endorsement of 5 total symptoms on the PHQ-9 (Fannet al., 2005).
Disinhibition was assessed by the Frontal Systems BehaviorScale (FrSBe) Disinhibition Subscale, a valid and reliable tool forassessing behaviors associated with frontal lobe dysfunction(Carvalho et al., 2013; Niemeier et al., 2013). Specifically, theDisinhibition Subscale assesses behaviors characterized byimpulsivity and poor cognitive inhibition. Raw scores on thissubscale were converted to standardized T-scores normalized ina neurologically impaired population while controlling for age,sex, and education. For the purposes of this study, T-scores forself-reported disinhibition after injury were used. To improveinterpretability for when disinhibition was the independent vari-able in logistic regression models, the T-scores were divided by10 (1 SD), so that 1 unit change was equivalent to 1 SD.
TNFa levels (pg/mL) were measured in acute CSF, acute serum,and chronic serum. There were a total of 37 participants with acuteCSF TNFa samples (n = 389), 48 participants with acute serumTNFa samples (n = 543), and 42 participants with chronic serumTNFa samples (n = 326). Both acute CSF and acute serum TNFawere computed by averaging daily TNFa levels from the first weekafter injury. Chronic serum TNFa included the average TNFa levelsfrom 2 weeks to 5 months after injury and also included levels at6 months and 12 months post-injury.
2.5. Statistical analysis
Statistical analyses were performed using SPSS™ 20 and SAS™9.3. Means and medians were calculated to describe continuousvariables, and frequency measures were used to describecategorical variables. For all analyses, if the necessary normalityassumptions were not met, nonparametric tests were employed.Normality was assessed by plotting histograms and testing skew-ness. Independent sample t-tests or Mann Whitney-U tests wereconducted to assess differences in TNFa levels between those withand without suicidal endorsement and between participants withTBI and healthy controls. Spearman correlations were conductedto assess relationships between TNFa levels and disinhibition.For those relationships that were below the statistical threshold(p < 0.10) for between group comparisons, bivariate logistic regres-sion analyses were conducted to explore whether TNFa and/ordisinhibition predicted suicidal endorsement. Linear regressionanalyses were conducted to explore whether TNFa predicteddisinhibition at 6 and 12 months. To address the non-normal dis-tribution of TNFa levels, bootstrapping for both logistic and linearregression was performed using 1000 samples. As a resamplingmethod, bootstrapping is often used when parametric assumptions(e.g. normality) have not been met, as it creates a resamplingdistribution from the sample itself in cases where the populationdistribution is not known. There was no reason to suspect thatthe sample distribution for TNFa would be different from the TNFadistribution in the broader population with moderate to severe TBI.For regression models, a p < 0.05 was considered statisticallysignificant.
3. Results
3.1. Descriptive data
A total of 70 participants at 6 months post-injury and 74 par-ticipants at 12 months post-injury had measures of suicidal
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement afterj.bbi.2014.05.020

4 S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx
endorsement and at least one measure of TNFa levels. Amongthose, 42 participants and 48 participants had disinhibition dataat 6 and 12 months post-injury, respectively. Those with andwithout disinhibition data did not differ with regard to age, gen-der, injury severity, suicidality, or TNFa levels, with the exceptionof 6 month TNFa, which was higher among those with no disinhi-bition data (p < 0.05). Descriptive data for the sample by suicidalendorsement group are presented in Table 1. Suicidal endorse-ment groups did not differ at either 6 or 12 months post-injurywith regard to age, gender, race, injury severity, or cognitive per-formance. In this sample, while a current depressive episode wasa significant risk factor for suicidality, it was not necessary in allcases of suicide endorsement. TNFa levels also did not differ bydepression status, age, sex, or race (p > 0.05 for all comparisons;data not shown).
Participants with TBI (n = 37) had significantly higher medianCSF TNFa levels (p < 0.001) than healthy controls (n = 15), demon-strating a nearly 5-fold increase (see Table 2). This increase,compared to healthy controls, was even more dramatic for partici-pants with TBI who had suicidal endorsement, with a 12-foldincrease for those endorsing suicidality at 6 months and a 17-foldincrease for those endorsing suicidality at 12 months (see Table 2).Participants with TBI (n = 48) had significantly higher median acuteserum TNFa levels (p = 0.001) than healthy controls (n = 15),though the increase was not as large as what was observed acutelyin the CSF. In the first 5 months post-injury, participants with TBI(n = 48) had significantly higher chronic serum TNFa levels(p < 0.001) than controls (n = 15), demonstrating a 2-fold increase.This difference was also present at 6 months post-injury(p = 0.003). At 12 months post-injury, the difference did not achievestatistical significance (p = 0.054), but there was still a trendtowards higher serum TNFa levels among those with TBI comparedto healthy controls (see Table 2).
Table 1Demographic characteristics of study sample by suicidal endorsement (6 and 12 months).
6 Month
Suicidal endorsement(n = 14)
No suicidalendorsement (n = 56
Age (mean ± SD) 35.71 ± 15.02 32.96 ± 12.71Sex, Male, n (%) 11 (78.6) 43 (76.8)Race, White, n (%)) 13 (92.9) 51 (91.1)Glasgow Coma Scale (median) 7.00 7.00Current depression, n (%) 13 (92.90) 13 (23.20)Cognitive composite (mean ± SD) 40.07 + 7.32 39.13 + 8.73
6 month suicidal endorsement: GCS n = 13; cognitive composite n = 13.6 month no suicidal endorsement: GCS n = 50; cognitive composite n = 52.12 month suicidal endorsement: GCS n = 13; cognitive composite n = 11.2 month no suicidal endorsement: GCS n = 54; cognitive composite n = 49.
a Statistical significance at a = 0.05.
Table 2TNFa levels TBI compared to healthy controls.
TNFac TBI (Median) Control(Median)
p Median fol(TBI/Contro
Acute CSF levels 0.40 0.09 <0.001a 4.58Acute serum levels 7.90 5.89 0.001a 1.34
Chronic serums levels2 Weeks–5 Months 11.43 5.89 <0.001a 1.946 Months 8.47 5.89 0.003a 1.4312 Months 6.91 5.89 0.054b 1.17
TNF = Tumor Necrosis Factor; TBI = traumatic brain injury; CSF = cerebrospinal fluid; n/aa Statistical significance at a = 0.05.b Statistical significance at a = 0.10.c TNFa levels measured in pg/mL.
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016
3.2. Suicidal endorsement group comparisons
Disinhibition (FrSBe) scores at 6 and 12 months were comparedbetween suicidality groups using independent t-tests, and acuteand chronic TNFa levels were compared between suicidalitygroups using Mann–Whitney-U tests (Table 3). For both timepoints, those who endorsed suicidality had significantly higher lev-els of disinhibition than those who did not (p < 0.05); suicidalendorsers’ disinhibition scores were approximately 1.5 SD greaterthan those who did not endorse suicide. Also, the mean at bothtime points for those who did not endorse suicide fell within 1standard deviation of the normed average (T-scores have amean = 50, SD = 10), whereas those with suicidal endorsementhad disinhibition scores approximately 2 SD above average. Over-all, there were no statistically significant differences between sui-cidal endorsement groups at 6 or 12 months with regard to TNFalevels, though in both cases acute CSF TNFa showed a trendtowards statistical significance, where those endorsing suicidalityhad higher biomarker levels, and this variable met the thresholdfor inclusion in the regression models (p < 0.10).
3.3. TNFa levels and disinhibition
Correlations between TNFa levels and disinhibition wereassessed with spearman correlations (Table 4). Acute serum TNFalevels were inversely associated with 12 month disinhibition(r = �0.520, p = 0.027) and achieved borderline significance with6 month disinhibition (r = �0.470, p = 0.057). In contrast, chronicserum TNFa levels, averaged across 2 weeks to 5 months post-injury, were positively correlated with 6 month disinhibitionscores (r = 0.459, p = 0.008). Six-month TNFa levels demonstratedtrends (p < 0.10) in relation to 6 and 12 month disinhibition, wherehigher levels were associated with greater disinhibition. Of note,
12 Month
)p-Value Suicidal endorsement
(n = 13)No suicidalendorsement (n = 61)
p-Value
0.487 33.54 ± 16.03 34.31 ± 13.06 0.8530.599 10 (76.9) 47 (77.00) 0.6220.655 12 (92.30) 55 (90.20) 0.6440.123 7.00 7.00 0.612<0.001a 9 (69.23) 14 (23.00) 0.002a
0.722 40.62 + 7.18 40.92 + 8.33 0.912
d changel)
TBI with suicidal endorsement(TBI-S) 6, 12 months
Median fold change(TBI-S/Control) 6, 12 months
1.08, 1.50 12.00, 16.676.61, 8.33 1.12, 1.41
12.90, 10.17 2.19, 1.7410.26, 10.11 1.74, 1.72n/a, 7.77 n/a, 1.32
= not applicable. The bolded values are correct and represent p-values < 0.05.
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement after/j.bbi.2014.05.020

Table 4Spearman correlations for TNFa levels and disinhibition (6 and 12 months).
6 Month disinhibition 12 Month disinhibition
n r p n r p
Acute CSF TNFac 16 �0.240 0.371 22 �0.209 0.350Acute serum TNFac 17 �0.470 0.057b 18 �0.520 0.027a
Chronic serum TNFac
2 Weeks–5 months 32 0.459 0.008a 37 0.126 0.4586 Months 19 0.395 0.094b 19 0.393 0.096b
12 Months – – – 21 0.333 0.141
TNF = Tumor Necrosis Factor; CSF = cerebrospinal fluid.a Statistical significance at a = 0.05.b Statistical significance at a = 0.10.c TNFa levels measured in pg/mL.
Table 3TNFa levels and disinhibition by suicidal endorsement (6 and 12 months).
6 Months post-injury 12 Months post-injury
n Suicidalendorsement
n No suicidalendorsement
p n Suicidalendorsement
n No suicidalendorsement
p
Disinhibition (Mean ±SD) 8 69.75 ± 11.51 34 53.03 ± 18.80 0.030a 9 72.67 ± 16.88 39 54.08 ± 17.08 0.005a
Acute CSF TNFa (median)c 8 1.08 24 0.40 0.056b 6 1.50 27 0.41 0.084Acute serum TNFa (median)c 8 6.61 26 7.90 0.543 6 8.33 31 7.42 0.711
Chronic serum TNFa (median)c
2 Weeks–5 months 9 12.90 35 11.28 0.375 11 10.17 37 12.35 0.7416 Months 6 10.26 20 7.36 0.224 6 10.11 23 7.51 0.55412 Months – – – – – 3 7.77 23 6.70 0.758
TNF = Tumor Necrosis Factor. The bolded values are correct and represent p-values < 0.05.a Statistical significance at a = 0.05.b Statistical significance at a = 0.10.c TNFa levels measured in pg/mL.
S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx 5
these results indicate that lower acute serum TNFa levels wereassociated with higher disinhibition, whereas higher TNFa levelsin the chronic serum were associated with higher disinhibition.
3.4. Logistic and linear regressions: Suicidal endorsement, TNFa levels,& disinhibition
To assess predictors of suicidal endorsement at 6 and12 months, logistic regression analyses were conducted includingTNFa levels or disinhibition that met the a priori threshold ofp < 0.10 in the group comparison or correlation analyses. Logisticregression results are presented in Table 5. Acute CSF TNFa lev-els significantly predicted suicidal endorsement at 12 months(OR = 3.224, p = 0.014), with an area under the curve (AUC) of 0.73.
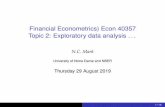
Most notably, disinhibition at 6 months was a significant pre-dictor of suicidal endorsement at both 6 and 12 months, and disin-hibition at 12 months significantly predicted suicidal endorsementat 12 months. Specifically, for every 1 SD increase in disinhibition(t-score change of 10 points), individuals had 1.8 times (6 months)or 1.9 times (12 months) the odds of endorsing suicide. Fig. 1depicts disinhibition scores by suicidal endorsement. While thesample size is not sufficient to conduct statistical analyses, thesedata suggest that those who do not endorse suicide have disinhibi-tion scores within a normal range, while those who endorse suicidehave disinhibition scores nearly 2 SD above the mean. Further,these findings suggest that those who endorse suicide at both 6and 12 months post-injury may exhibit even higher levels of disin-hibition (>2 SD above the mean).
While serum TNFa levels did not predict suicidal endorsement,linear regression indicated that they were predictive of disinhibi-tion. Specifically, acute serum TNFa significantly predicted both6 and 12 month disinhibition scores, and average TNFa levels from2 weeks to 5 months post-injury significantly predicted 6 month
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016/
disinhibition (see Table 6). Interestingly, lower acute serum TNFaand higher chronic serum TNFa levels predicted higher disinhibi-tion scores. This finding suggests that serum TNFa levels mayreflect a temporally dynamic pathology with regard to blood brainbarrier (BBB) integrity when transitioning from the acute to thechronic phase after injury.
Finally, 6 month disinhibition strongly predicted 12 month dis-inhibition, suggesting that this behavioral consequence of injurypersists over time.
4. Discussion
Individuals with TBI have a significantly higher risk for suicidal-ity than the general population, potentially as a result of theincreased risk for both depression and disinhibition after injury.While depression is a known risk factor for suicidality, it doesnot explain fully the higher suicidality risk that is observed afterTBI. Understanding the underlying mechanisms for this increasedsuicidality risk could aid in early identification of those in needof closer monitoring and inform early intervention approachesfor suicidal endorsement. There is no research to date specificallyexamining how biofluid biomarkers of any kind might contributeto risk for suicidal endorsement after TBI, and there is no researchexamining how biofluid biomarkers contribute to disinhibitionafter TBI. While this study is a pilot exploration with a relativelysmall sample size, our findings suggest that serum TNFa is a poten-tial candidate biomarker for disinhibition, which in turn is a signif-icant risk factor for suicidal endorsement after TBI. While TNFawas not associated with depression status in our sample, acuteCSF TNFa was a risk factor for suicidal endorsement at 12 monthspost-injury. The link between disinhibition and increased risk forsuicidality in this study is consistent with previous research amongindividuals with psychiatric disorders, (Burton et al., 2011;
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement afterj.bbi.2014.05.020

Table 5Logistic regression models.
6 Month suicidal endorsement n = 32 12 Month suicidal endorsement n = 33AUC = 0.73 AUC = 0.73
Odds ratio 95% CI p-Value Odds ratio 95% CI p-Value
Acute CSF TNFa 1.936 0.719–5.214 0.172 3.224 1.039–10.006 0.014a,b
6 Month suicidal endorsement n = 42 12 Month suicidal endorsement n = 43AUC = 0.76 AUC = 0.78
Odds ratio 95% CI p-Value Odds ratio 95% CI p-Value
Disinhibitionc (6 months) 1.764 1.012–3.075 0.045a 1.925 1.056–3.508 0.033a
12 month suicidal endorsement n = 48AUC = 0.76
Odds ratio 95% CI p-Value Odds ratio 95% CI p-Value
Disinhibitionc (12 months) – – – 1.896 1.142–3.147 0.013a
Note: Selected models were run based on group comparison differences with p < .10.AUC = Area under the curve; TNF = Tumor Necrosis Factor; CSF = Cerebrospinal fluid.
a Statistical significance at a = 0.05.b Bootstrapping was performed with 1000 samples.c Disinhibition t-scores were divided by 10 (the standard deviation for t-scores) prior to inclusion in the logistic regression models. Therefore, a 1 unit change in
disinhibition indicates a change of 1 standard deviation.
Table 6Linear regression models.
6 Month disinhibition 12 Month disinhibitionn = 17 n = 33RAdj
2 = .150 RAdj2 = .244
b 95% CI p-Value b 95% CI p-Value
Acute serum TNFa �1.570 �2.589, �0.478 0.009a,b �2.246 �3.890, �.767 0.009a,b
6 Month disinhibitionn = 32RAdj
2 = .107
b 95% CI p-Value
Chronic TNFa (2 weeks–5 months) 1.153 0.473–2.433 0.029a,b – – –
6 Month disinhibition 12 Month disinhibitionn = 19 n = 19RAdj
2 = .054 RAdj2 = .031
b 95% CI p-Value b 95% CI p-Value
Chronic TNFa (6 months) 1.088 �0.050 to 3.202 0.200b 0.787 �0.148, 1.555 0.10b
12 Month disinhibitionn = 34RAdj
2 = .394
b 95% CI p-Value
Disinhibition** (6 months) – – – 0.661 .377, .946 <0.001a
Note: Selected models were included based on correlations with p < .10.TNF = Tumor Necrosis Factor; CSF = Cerebrospinal fluid; RAdj
2 = Adjusted R squared.a Statistical significance at a = 0.05.b Bootstrapping was performed with 1000 samples.
6 S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx
Giakoumatos et al., 2013; Lynch et al., 2004; Richard-Devantoyet al., 2012a,b), adolescents (Pan et al., 2011), and individuals withTBI (Homaifar et al., 2012), supporting the examination of disinhi-bition, in addition to depression, when assessing suicide risk.
Lower acute serum TNFa levels were associated with both 6 and12 month disinhibition, while higher chronic serum TNFa levelspredicted disinhibition at 6 months. While disinhibition is posi-tively associated with suicidality, to our knowledge, there are noreports of how inflammation may directly influence a disinhibitedbehavioral state, making this finding a potentially interesting onebeyond the context of suicidality and TBI. For example, individualswith Down Syndrome have been reported to have a lifetime eleva-tion in TNFa (Wilcock and Griffin, 2013) and be at risk for exhibit-ing a disinhibited behavioral state (Ball et al., 2010). Another
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016
condition that is commonly associated with behavioral disinhibi-tion is post-traumatic stress disorder (PTSD) (Casada and Roache,2005; Myers et al., 2012), which, like TBI, has been associated withhigher levels of TNFa (Gill et al., 2008; Gola et al., 2013; Hammadet al., 2012; von Känel et al., 2007). TNFa and disinhibition maytherefore be pertinent biomarkers for populations at risk for PTSDand suicidality, such as a military population (James et al., 2014;Wisco et al., 2014).
Higher TNFa levels have been found to be associated with suici-dality in other populations (Janelidze et al., 2011; Martinez et al.,2012; Tonelli et al., 2008), and suicidality is associated with higherdisinhibition (Brenner et al., 2009; Hesdorffer et al., 2009;Homaifar et al., 2012; Reeves and Laizer, 2012; Simpson andTate, 2007; Wasserman et al., 2008). This literature is consistent
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement after/j.bbi.2014.05.020

S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx 7
with our finding of associations between higher chronic TNFalevels and higher disinhibition, but may contrast with our findingthat low acute serum TNFa levels correlate with higher disinhibi-tion. One potential explanation for this temporal difference inthe directionality of these serum associations is that, in TBI, acuteserum TNFa levels may be lower among those with moredisinhibition as a result of peripheral TNFa (serum) transit intothe CNS (CSF) through a compromised BBB; therefore, lower acuteserum TNFa may reflect the contribution of peripheral TNFa to themulti-fold increase in CSF TNFa observed with TBI compared tocontrols (Pan and Kastin, 2002) (see Table 2). As TNFa is a proin-flammatory mediator that initiates and perpetuates inflammatorysignaling pathways (Ghirnikar et al., 1998; Woodcock andMorganti-Kossmann, 2013), this multifold elevation of TNFa inthe CNS may, in turn, contribute to the chronic inflammatory statethat has been demonstrated after TBI (Johnson et al., 2013).
Those with TBI demonstrated a nearly 5-fold increase in CSFTNFa levels compared to controls, and those with TBI plus suicidalendorsement had a 12 to 17-fold increase in CSF TNFa compared tocontrols. Preliminary evidence in the MDD population indicatesthat plasma TNFa is elevated in the context of depression(Himmerich et al., 2008), and higher CSF TNFa concentrations areassociated with greater suicidal ideation and poor treatmentresponse (Martinez et al., 2012). Higher CSF TNFa levels amongthose who endorsed suicide may indicate more BBB damage and/or a stronger CNS inflammatory response to injury than thosewho did not endorse suicide. The literature (An et al., 2013)indicates that brain injury triggers both central and peripheralinflammation, with peripheral macrophages, neutrophils, and lym-phocytes entering the brain and CNS activation of the peripheralimmune system. Further, this CNS-induced peripheral immune sys-tem activation results as a direct consequence of BBB breakdownafter injury and occurs in the presence of TNFa (An et al., 2013).Additional research is required to assess whether CSF levels remainhigher among individuals with TBI than controls in the chronicphase after injury.
Fig. 1. Mean disinhibition scores (t-scores), as measured by the Frontal Systems BehavioThese groups included those who did not endorse at either 6 or 12 months (‘‘None’’), tendorsed at 12 months but not 6 months (‘‘12-month only’’), and those who endorsed astandard deviations (SD) from the normalized mean (t-scores have a mean of 50, SD ofendorsers are presented in Table 3.
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016/
While chronic CSF TNFa levels were not available, serum TNFalevels did remain elevated among individuals with TBI, comparedto healthy controls, over the first 5 months post-injury. As theBBB integrity is repaired, and the peripheral TNFa transit into theCNS is slowed, chronic serum TNFa levels may become even moreelevated post-injury; this concept is consistent with our findingsthat suggest a larger fold change between TBI participants andhealthy controls in the chronic compared to the acute serum. Giventhe impracticality of obtaining CSF samples among individualswith less severe injuries or in the chronic phase after TBI, identify-ing a peripheral biomarker (i.e. via serum) that reflects chronic CNSinflammatory status is critical.
TNFa has been implicated specifically in BBB degradation afterinjury through its role in increasing microglia activation (Dilgerand Johnson, 2008; Morganti-Kossmann et al., 2007) and its down-stream effects on white matter degeneration (Tarkowski et al.,2003; Yurgelun-Todd et al., 2011). The CNS inflammatory response,when physiologically intact, may be neuroprotective when injuryinduced perturbations are mild or transient. However, if thisinflammatory response becomes maladaptive, such as can occurafter significant TBI or repetitive mild TBI observed commonly inmilitary populations exposed to active combat, it can pathologicallypersist for years after injury (Johnson et al., 2013) and result in pooroutcomes (Felger and Lotrich, 2013; Loane and Byrnes, 2010) As anearly inflammatory cascade initiator, TNFa is critical to microglialactivation (Bennett et al., 2009; Dilger and Johnson, 2008;Morganti-Kossmann et al., 2007) and the long-term perpetuationof neuroinflammation (Johnson et al., 2013). Previous research indi-cates that individuals with TBI may not differ from controls withregard to microglial activation acutely, but they do demonstrateincreased microglial density and activation beginning two weeksafter injury and lasting for years (Johnson et al., 2013). Future workmight also explore other markers known to be elevated after TBI,such as S100B, which is elevated acutely after TBI (Goyal et al.,2013) and has shown promise as a biomarker for mood disordersthrough its association with glial activation (Schroeter et al., 2013).
r Scale (FrSBe) Disinhibition subscale, are presented by suicidal endorsement group.hose who endorsed at 6 months but not 12 months (‘‘6-month only’’), those whot both 6 and 12 months (‘‘Both 6 and 12 months’’). Hashed lines represent 1 and 210). Statistical analysis comparing disinhibition scores in suicide endorsers to non-
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement afterj.bbi.2014.05.020

8 S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx
This work may have broader implications for understandingdisinhibition as a behavioral link between neurobiology and suici-dality. While we assessed the contribution of TNFa to disinhibition,it remains unclear whether a disinhibited state might contribute toincreased inflammation as well, creating a biological to behavioralfeedback loop. With larger sample sizes, the role of disinhibitionas a mediating factor linking TNFa to depression and suicidalitycan be directly tested. TNFa may have been more sensitive to disin-hibition as it is a continuous measure, unlike suicidality and depres-sion which were both dichotomous outcomes in this study. HigherTNFa levels may be associated with greater depressive symptomburden, rather than simply a diagnosis of depression; in this case,individuals with minor depression (categorized in our sample asnot having a current depressive episode) may have higher TNFathan those with no depressive symptoms, despite being categorizedin the same group. Longitudinal studies could assess the temporalpatterns between inflammatory markers and behavioral (disinhibi-tion) and psychological (depression, suicidality) outcomes. Finally,future work will need to confirm TNFa as a biomarker of both dis-inhibition and suicidal endorsement in TBI, assess the contributionof TNFa and disinhibition to suicidality in the presence and absenceof depression, and delineate how these biological mechanisms mapto TBI-specific pathology.
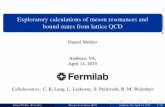
While further analysis with a larger sample is required tovalidate these findings, this work represents an effectiveRehabilomics-based (Wagner, 2011) pilot study linking bothbiological and behavioral biomarkers to a multifactorial complica-tion (suicidality) for which individuals with TBI are particularlysusceptible. The current report is limited by a small sample sizeand an inability to perform robust repeated measures, multivariateanalyses, and mediational analyses. However, these data present astriking pattern that suggests a biological to behavioral pathway tosuicidal endorsement after TBI (Fig. 2). Confirmatory studies arerequired to assess these potential biological mechanisms, to estab-lish TNFa as a biomarker of disinhibition, and to establish bothTNFa and disinhibition as markers of suicidality. This would enableearly screening and identification of those at risk for persistentbehavioral (disinhibition) and emotional (depression) problemsthat lead to eventual suicidality. Inflammatory markers other thanTNFa have been linked to suicidality in the general population(Currier and Mann, 2008; Mandelli and Serretti, 2013; Serafini
Fig. 2. This conceptual model is based on associations found in the logistic andlinear regressions. Solid lines indicate statistically significant relationships(p < 0.05) and hashed lines represent trending relationships (p < 0.20). Up anddown arrows associated with TNFa represent the direction of the relationship (e.g.higher CSF TNFa is associated with suicidal endorsement; lower serum TNFa isassociation with higher disinhibition). TNF = Tumor Necrosis Factor; CSF = cerebro-spinal fluid. Of note, depression status is not represented in this model, but is acritical component to consider when assessing suicidal endorsement.
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016
et al., 2013), and future work may consider how these and othernon-inflammatory markers associated with suicidality in thegeneral population influence suicidality after TBI.
Currently, the recommended management for suicidal endorse-ment includes: (1) detection, reduction and management of suicidalideation and behaviors; (2) treatment of comorbid mood disorders,substance abuse, and cognitive impairment; and (3) counseling orpsychotherapy (Reeves and Laizer, 2012). For those with TBI andsuicidal endorsement, this management approach should addressneurological, psychological, and psychosocial factors, such asneurobiological changes, mood symptoms, and social/familysupports. The specific approach for these factors should include aproactive assessment of suicidal ideation and should focus on treat-ing mental health problems with pharmacotherapy, neuropsycho-social treatments, and psychosocial support (Kuehn, 2009). Iffuture work corroborates TNF-a and disinhibition as markers forsuicidality after TBI, personalized rehabilitation screening andtreatment trajectories may be considered as strategies to improvecommunity based outcomes and better serve those at increased riskfor suicidality by providing early interventions and preventativemeasures and identifying those who require more intensive track-ing, follow-up, and intervention. While speculative, modulators ofTNFa, like omega-3 fatty acids and TNFa inhibitors, may be benefi-cial (Colin et al., 2003; Krügel et al., 2013).
Acknowledgments
This work was supported in part by: CDC: R49 CCR 323155,DOD: W81XWH-071-0701, the University of Pittsburgh’s Women’sStudies Faculty Research Fund (Amy Wagner); NIDRRH133A120087 and the UPMC Rehabilitation Institute (AmyWagner & Shannon Juengst). The authors would like to acknowledgeand thank the University of Pittsburgh Cancer Institute and theirLuminex Facility for assay performance. Special thanks to Dr. AnnaLokshin and John Snyder for input on data scaling for inflammatorymarkers.
References
An, C., Shi, Y., Li, P., Hu, X., Gan, Y., Stetler, R.A., et al., 2013. Molecular dialogsbetween the ischemic brain and the peripheral immune system: dualistic rolesin injury and repair. Prog. Neurobiol. http://dx.doi.org/10.1016/j.pneurobio.2013.12.002.
Ball, S.L., Holland, A.J., Watson, P.C., Huppert, F.A., 2010. Theoretical exploration ofthe neural bases of behavioural disinhibition, apathy and executive dysfunctionin preclinical Alzheimer’s disease in people with Down’s syndrome: potentialinvolvement of multiple frontal-subcortical neuronal circuits. J. Intell. Disab.Res.: JIDR 54 (4), 320–336. http://dx.doi.org/10.1111/j.1365-2788.2010.01261.x.
Bennett, M.R., Farnell, L., Gibson, W.G., 2009. P2X7 regenerative-loop potentiationof glutamate synaptic transmission by microglia and astrocytes. J. Theor. Biol.261 (1), 1–16. http://dx.doi.org/10.1016/j.jtbi.2009.07.024.
Bertolote, J.M., Fleischmann, A., De Leo, D., Wasserman, D., 2003. Suicide and mentaldisorders: do we know enough? Br. J. Psych.: J. Mental Sci. 183, 382–383.
Brenner, L.A., Homaifar, B.Y., Adler, L.E., Wolfman, J.H., Kemp, J., 2009. Suicidalityand veterans with a history of traumatic brain injury: precipitants events,protective factors, and prevention strategies. Rehabil. Psychol. 54 (4), 390–397.http://dx.doi.org/10.1037/a0017802.
Brown, A.W., Moessner, A.M., Mandrekar, J., Diehl, N.N., Leibson, C.L., Malec, J.F.,2011. A survey of very-long-term outcomes after traumatic brain injury amongmembers of a population-based incident cohort. J. Neurotrauma 28 (2), 167–176. http://dx.doi.org/10.1089/neu.2010.1400.
Burton, C.Z., Vella, L., Weller, J.A., Twamley, E.W., 2011. Differential effects ofexecutive functioning on suicide attempts. J. Neuropsych. Clin. Neurosci. 23 (2),173–179. http://dx.doi.org/10.1176/appi.neuropsych.23.2.173.
Carvalho, J.O., Ready, R.E., Malloy, P., Grace, J., 2013. Confirmatory factor analysis ofthe Frontal Systems Behavior Scale (FrSBe). Assessment 20 (5), 632–641. http://dx.doi.org/10.1177/1073191113492845.
Casada, J.H., Roache, J.D., 2005. Behavioral inhibition and activation inposttraumatic stress disorder. J. Nerv. Ment. Dis. 193 (2), 102–109.
Ciurli, P., Formisano, R., Bivona, U., Cantagallo, A., Angelelli, P., 2011.Neuropsychiatric disorders in persons with severe traumatic brain injury:prevalence, phenomenology, and relationship with demographic, clinical, and
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement after/j.bbi.2014.05.020

S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx 9
functional features. J. Head Trauma Rehabil. 26 (2), 116–126. http://dx.doi.org/10.1097/HTR.0b013e3181dedd0e.
Colin, A., Reggers, J., Castronovo, V., Ansseau, M., 2003. Lipids, depression andsuicide. L’Encéphale 29 (1), 49–58.
Currier, D., Mann, J.J., 2008. Stress, genes and the biology of suicidal behavior. Psych.Clin. North America 31 (2), 247–269. http://dx.doi.org/10.1016/j.psc.2008.01.005.
Desseilles, M., Perroud, N., Guillaume, S., Jaussent, I., Genty, C., Malafosse, A.,Courtet, P., 2012. Is it valid to measure suicidal ideation by depression ratingscales? J. Affect. Disord. 136 (3), 398–404. http://dx.doi.org/10.1016/j.jad.2011.11.013.
Dilger, R.N., Johnson, R.W., 2008. Aging, microglial cell priming, and the discordantcentral inflammatory response to signals from the peripheral immune system. J.Leukoc. Biol. 84 (4), 932–939. http://dx.doi.org/10.1189/jlb.0208108.
Dombrovski, A.Y., Szanto, K., Clark, L., Reynolds, C.F., Siegle, G.J., 2013. Rewardsignals, attempted suicide, and impulsivity in late-life depression. JAMA Psych.(Chicago, Ill.). http://dx.doi.org/10.1001/jamapsychiatry.2013.75.
Failla, M.D., Burkhardt, J.N., Miller, M.A., Scanlon, J.M., Conley, Y.P., Ferrell, R.E.,Wagner, A.K., 2013. Variants of SLC6A4 in depression risk following severe TBI.Brain Injury: [BI] 27 (6), 696–706. http://dx.doi.org/10.3109/02699052.2013.775481.
Fann, J.R., Bombardier, C.H., Dikmen, S., Esselman, P., Warms, C.A., Pelzer, E., et al.,2005. Validity of the Patient Health Questionnaire-9 in assessing depressionfollowing traumatic brain injury. J. Head Trauma Rehabil. 20 (6), 501–511.
Fann, J.R., Hart, T., Schomer, K.G., 2009. Treatment for depression after traumaticbrain injury: a systematic review. J. Neurotrauma 26 (12), 2383–2402. http://dx.doi.org/10.1089/neu.2009.1091.
Felger, J.C., Lotrich, F.E., 2013. Inflammatory cytokines in depression:neurobiological mechanisms and therapeutic implications. Neuroscience 246,199–229. http://dx.doi.org/10.1016/j.neuroscience.2013.04.060.
Fountoulakis, K.N., Iacovides, A., Fotiou, F., Nimatoudis, J., Bascialla, F., Ioannidou, C.,et al., 2004. Neurobiological and psychological correlates of suicidal attemptsand thoughts of death in patients with major depression. Neuropsychobiology49 (1), 42–52. http://dx.doi.org/10.1159/000075338.
Frugier, T., Morganti-Kossmann, M.C., O’Reilly, D., McLean, C.A., 2010. In situdetection of inflammatory mediators in post mortem human brain tissue aftertraumatic injury. J. Neurotrauma 27 (3), 497–507. http://dx.doi.org/10.1089/neu.2009.1120.
Ghirnikar, R.S., Lee, Y.L., Eng, L.F., 1998. Inflammation in traumatic brain injury: roleof cytokines and chemokines. Neurochem. Res. 23 (3), 329–340.
Giakoumatos, C.I., Tandon, N., Shah, J., Mathew, I.T., Brady, R.O., Clementz, B.A.,Keshavan, M.S., 2013. Are structural brain abnormalities associated withsuicidal behavior in patients with psychotic disorders? J. Psych. Res. 47 (10),1389–1395. http://dx.doi.org/10.1016/j.jpsychires.2013.06.011.
Giegling, I., Olgiati, P., Hartmann, A.M., Calati, R., Möller, H.-J., Rujescu, D., Serretti,A., 2009. Personality and attempted suicide. Analysis of anger, aggression andimpulsivity. J. Psych. Res. 43 (16), 1262–1271. http://dx.doi.org/10.1016/j.jpsychires.2009.04.013.
Gill, J., Vythilingam, M., Page, G.G., 2008. Low cortisol, high DHEA, and high levels ofstimulated TNF-alpha, and IL-6 in women with PTSD. J. Trauma. Stress 21 (6),530–539. http://dx.doi.org/10.1002/jts.20372.
Gola, H., Engler, H., Sommershof, A., Adenauer, H., Kolassa, S., Schedlowski, M.,Kolassa, I.-T., 2013. Posttraumatic stress disorder is associated with anenhanced spontaneous production of pro-inflammatory cytokines byperipheral blood mononuclear cells. BMC Psych. 13, 40. http://dx.doi.org/10.1186/1471-244X-13-40.
Goyal, A., Failla, M.D., Niyonkuru, C., Amin, K., Fabio, A., Berger, R.P., Wagner, A.K.,2013. S100b as a prognostic biomarker in outcome prediction for patients withsevere traumatic brain injury. J. Neurotrauma 30 (11), 946–957. http://dx.doi.org/10.1089/neu.2012.2579.
Green, R.E., Colella, B., Hebert, D.A., Bayley, M., Kang, H.S., Till, C., Monette, G., 2008.Prediction of return to productivity after severe traumatic brain injury:investigations of optimal neuropsychological tests and timing of assessment.Arch. Phys. Med. Rehabil. 89 (12 Suppl), S51–S60. http://dx.doi.org/10.1016/j.apmr.2008.09.552.
Hammad, S.M., Truman, J.-P., Al Gadban, M.M., Smith, K.J., Twal, W.O., Hamner, M.B.,2012. Altered blood sphingolipidomics and elevated plasma inflammatorycytokines in combat veterans with post-traumatic stress disorder. Neurobiol.Lipids 10, 2.
Harrison-Felix, C.L., Whiteneck, G.G., Jha, A., DeVivo, M.J., Hammond, F.M., Hart,D.M., 2009. Mortality over four decades after traumatic brain injuryrehabilitation: a retrospective cohort study. Arch. Phys. Med. Rehabil. 90 (9),1506–1513. http://dx.doi.org/10.1016/j.apmr.2009.03.015.
Hart, T., Whyte, J., Kim, J., Vaccaro, M., 2005. Executive function and self-awarenessof ‘‘real-world’’ behavior and attention deficits following traumatic brain injury.J. Head Trauma Rehabil. 20 (4), 333–347.
Hartikainen, K.M., Waljas, M., Isoviita, T., Dastidar, P., Liimatainen, S., Solbakk, A.-K.,Ohman, J., 2010. Persistent symptoms in mild to moderate traumatic braininjury associated with executive dysfunction. J. Clin. Exp. Neuropsychol. 32 (7),767–774. http://dx.doi.org/10.1080/13803390903521000.
Hesdorffer, D.C., Rauch, S.L., Tamminga, C.A., 2009. Long-term psychiatricoutcomes following traumatic brain injury: a review of the literature. J.Head Trauma Rehabil. 24 (6), 452–459. http://dx.doi.org/10.1097/HTR.0b013e3181c133fd.
Himmerich, H., Fulda, S., Linseisen, J., Seiler, H., Wolfram, G., Himmerich, S.,Pollmächer, T., 2008. Depression, comorbidities and the TNF-alpha system. Eur.
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016/
Psych.: J. Assoc. Eur. Psychiatr. 23 (6), 421–429. http://dx.doi.org/10.1016/j.eurpsy.2008.03.013.
Homaifar, B.Y., Brenner, L.A., Forster, J.E., Nagamoto, H., 2012. Traumatic braininjury, executive functioning, and suicidal behavior: a brief report. Rehabil.Psychol. 57 (4), 337–341. http://dx.doi.org/10.1037/a0030480.
Iverson, G.L., Franzen, M.D., Lovell, M.R., 1999. Normative comparisons for thecontrolled oral word association test following acute traumatic brain injury.Clin. Neuropsychol. 13 (4), 437–441. http://dx.doi.org/10.1076/1385-4046(199911)13:04;1-Y;FT437.
James, L.M., Strom, T.Q., Leskela, J., 2014. Risk-taking behaviors and impulsivityamong veterans with and without PTSD and mild TBI. Mil. Med. 179 (4), 357–363. http://dx.doi.org/10.7205/MILMED-D-13-00241.
Janelidze, S., Mattei, D., Westrin, Å., Träskman-Bendz, L., Brundin, L., 2011. Cytokinelevels in the blood may distinguish suicide attempters from depressed patients.Brain Behav. Immun. 25 (2), 335–339. http://dx.doi.org/10.1016/j.bbi.2010.10.010.
Johnson, V.E., Stewart, J.E., Begbie, F.D., Trojanowski, J.Q., Smith, D.H., Stewart, W.,2013. Inflammation and white matter degeneration persist for years after asingle traumatic brain injury. Brain: J. Neurol. 136 (Pt 1), 28–42. http://dx.doi.org/10.1093/brain/aws322.
Juengst, S.B., Kumar, R.G., Failla, M.D., Goyal, A., Wagner, A.K., 2014. Acuteinflammatory biomarker profiles predict depression risk following moderateto severe traumatic brain injury. J. Head Trauma Rehabil. http://dx.doi.org/10.1097/HTR.0000000000000031.
Kim, E., 2002. Agitation, aggression, and disinhibition syndromes after traumaticbrain injury. NeuroRehabilitation 17 (4), 297–310.
Kim, Y.-K., Hong, J.-P., Hwang, J.-A., Lee, H.-J., Yoon, H.-K., Lee, B.-H., Na, K.-S., 2013.TNF-alpha -308G>A polymorphism is associated with suicide attempts in majordepressive disorder. J. Affect. Disord. 150 (2), 668–672. http://dx.doi.org/10.1016/j.jad.2013.03.019.
Krügel, U., Fischer, J., Radicke, S., Sack, U., Himmerich, H., 2013. Antidepressanteffects of TNF-a blockade in an animal model of depression. J. Psych. Res. 47 (5),611–616. http://dx.doi.org/10.1016/j.jpsychires.2013.01.007.
Kuehn, B.M., 2009. Soldier suicide rates continue to rise: military, scientists work tostem the tide. JAMA: J. Am. Med. Assoc. 301(11), 1111, 1113. doi:http://dx.doi.org/10.1001/jama.2009.342.
Lee, R., Petty, F., Coccaro, E.F., 2009. Cerebrospinal fluid GABA concentration:relationship with impulsivity and history of suicidal behavior, but notaggression, in human subjects. J. Psych. Res. 43 (4), 353–359. http://dx.doi.org/10.1016/j.jpsychires.2008.04.004.
Loane, D.J., Byrnes, K.R., 2010. Role of microglia in neurotrauma. Neurotherapeutics:J. Am. Soc. Exp. NeuroTher. 7 (4), 366–377. http://dx.doi.org/10.1016/j.nurt.2010.07.002.
Lopez-Larson, M., King, J.B., McGlade, E., Bueler, E., Stoeckel, A., Epstein, D.J.,Yurgelun-Todd, D., 2013. Enlarged thalamic volumes and increased fractionalanisotropy in the thalamic radiations in veterans with suicide behaviors.Frontiers Psych. 4, 83. http://dx.doi.org/10.3389/fpsyt.2013.00083.
Lux, W.E., 2007. A neuropsychiatric perspective on traumatic brain injury. J. Rehabil.Res. Dev. 44 (7), 951–962.
Lynch, T.R., Cheavens, J.S., Morse, J.Q., Rosenthal, M.Z., 2004. A model predictingsuicidal ideation and hopelessness in depressed older adults: the impact ofemotion inhibition and affect intensity. Aging Mental Health 8 (6), 486–497.http://dx.doi.org/10.1080/13607860412331303775.
Mandelli, L., Serretti, A., 2013. Gene environment interaction studies in depressionand suicidal behavior: an update. Neurosci. Biobehav. Rev. 37 (10 Pt 1), 2375–2397. http://dx.doi.org/10.1016/j.neubiorev.2013.07.011.
Martinez, J.M., Garakani, A., Yehuda, R., Gorman, J.M., 2012. Proinflammatory and‘‘resiliency’’ proteins in the CSF of patients with major depression. Depress.Anxiety 29 (1), 32–38. http://dx.doi.org/10.1002/da.20876.
Matthews, S., Spadoni, A., Knox, K., Strigo, I., Simmons, A., 2012. Combat-exposedwar veterans at risk for suicide show hyperactivation of prefrontal cortex andanterior cingulate during error processing. Psychosom. Med. 74 (5), 471–475.http://dx.doi.org/10.1097/PSY.0b013e31824f888f.
McGirr, A., Diaconu, G., Berlim, M.T., Pruessner, J.C., Sablé, R., Cabot, S., Turecki, G.,2010. Dysregulation of the sympathetic nervous system, hypothalamic–pituitary–adrenal axis and executive function in individuals at risk forsuicide. J. Psych. Neurosci.: JPN 35 (6), 399–408. http://dx.doi.org/10.1503/jpn.090121.
Morganti-Kossmann, M.C., Satgunaseelan, L., Bye, N., Kossmann, T., 2007.Modulation of immune response by head injury. Injury 38 (12), 1392–1400.http://dx.doi.org/10.1016/j.injury.2007.10.005.
Myers, C.E., Vanmeenen, K.M., Servatius, R.J., 2012. Behavioral inhibition and PTSDsymptoms in veterans. Psych. Res. 196 (2–3), 271–276. http://dx.doi.org/10.1016/j.psychres.2011.11.015.
Namas, R., Ghuma, A., Hermus, L., Zamora, R., Okonkwo, D.O., Billiar, T.R., Vodovotz,Y., 2009. The acute inflammatory response in trauma/hemorrhage andtraumatic brain injury: current state and emerging prospects. Libyan J. Med. 4(3), 97–103. http://dx.doi.org/10.4176/090325.
Niemeier, J.P., Perrin, P.B., Holcomb, M.G., Nersessova, K.S., Rolston, C.D., 2013.Factor structure, reliability, and validity of the Frontal Systems Behavior Scale(FrSBe) in an acute traumatic brain injury population. Rehabil. Psychol. 58 (1),51–63. http://dx.doi.org/10.1037/a0031612.
O’Donovan, A., Rush, G., Hoatam, G., Hughes, B.M., McCrohan, A., Kelleher, C.,Malone, K.M., 2013. Suicidal ideation is associated with elevated inflammationin patients with major depressive disorder. Depress. Anxiety 30 (4), 307–314.http://dx.doi.org/10.1002/da.22087.
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement afterj.bbi.2014.05.020

10 S.B. Juengst et al. / Brain, Behavior, and Immunity xxx (2014) xxx–xxx
Okusaga, O., Postolache, T.T., 2012. Toxoplasma gondii, the immune system, andsuicidal behavior. In: Dwivedi, Y. (Ed.), The Neurobiological Basis of Suicide. CRCPress, Boca Raton, FL, <http://www.ncbi.nlm.nih.gov/books/NBK107197/>.
Omrani, M.D., Bushehri, B., Bagheri, M., Salari-Lak, S., Alipour, A., Anoshae, M.-R.,Massomi, R., 2009. Role of IL-10 -1082, IFN-gamma +874, and TNF-alpha -308genes polymorphisms in suicidal behavior. Arch. Suicide Res.: Official J. Int.Acad. Suicide Res. 13 (4), 330–339. http://dx.doi.org/10.1080/13811110903266418.
Pan, W., Kastin, A.J., 2002. TNFalpha transport across the blood-brain barrier isabolished in receptor knockout mice. Exp. Neurol. 174 (2), 193–200. http://dx.doi.org/10.1006/exnr.2002.7871.
Pan, L.A., Batezati-Alves, S.C., Almeida, J.R.C., Segreti, A., Akkal, D., Hassel, S., et al.,2011. Dissociable patterns of neural activity during response inhibition indepressed adolescents with and without suicidal behavior. J. Am. Acad. ChildAdolesc. Psych. 50 (6). http://dx.doi.org/10.1016/j.jaac.2011.03.018, 602–611.e3.
Pandey, G.N., Rizavi, H.S., Ren, X., Fareed, J., Hoppensteadt, D.A., Roberts, R.C.,Dwivedi, Y., 2012. Proinflammatory cytokines in the prefrontal cortex ofteenage suicide victims. J. Psych. Res. 46 (1), 57–63. http://dx.doi.org/10.1016/j.jpsychires.2011.08.006.
Raison, C.L., Rutherford, R.E., Woolwine, B.J., Shuo, C., Schettler, P., Drake, D.F., et al.,2013. A randomized controlled trial of the tumor necrosis factor antagonistinfliximab for treatment-resistant depression: the role of baseline inflammatorybiomarkers. JAMA Psych. (Chicago, Ill.) 70 (1), 31–41. http://dx.doi.org/10.1001/2013.jamapsychiatry.4.
Reeves, R.R., Laizer, J.T., 2012. Traumatic brain injury and suicide. J. Psychosoc. Nurs.Ment. Health Serv. 50 (3), 32–38. http://dx.doi.org/10.3928/02793695-20120207-02.
Reitan, R.M., 1955. The relation of the trail making test to organic brain damage. J.Consult. Psychol. 19 (5), 393–394.
Richard-Devantoy, S., Gorwood, P., Annweiler, C., Olié, J.-P., Le Gall, D., Beauchet, O.,2012a. Suicidal behaviours in affective disorders: a deficit of cognitiveinhibition? Can. J. Psych. Rev. Can. Psych. 57 (4), 254–262.
Richard-Devantoy, S., Jollant, F., Kefi, Z., Turecki, G., Olié, J.P., Annweiler, C., Le Gall,D., 2012b. Deficit of cognitive inhibition in depressed elderly: a neurocognitivemarker of suicidal risk. J. Affect. Disord. 140 (2), 193–199. http://dx.doi.org/10.1016/j.jad.2012.03.006.
Saiz, P.A., García-Portilla, P., Paredes, B., Corcoran, P., Arango, C., Morales, B., Bobes,J., 2011. Role of serotonergic-related systems in suicidal behavior: data from acase-control association study. Prog. Neuropsychopharmacol. Biol. Psych. 35(6), 1518–1524. http://dx.doi.org/10.1016/j.pnpbp.2011.04.011.
Schroeter, M.L., Sacher, J., Steiner, J., Schoenknecht, P., Mueller, K., 2013. SerumS100B represents a new biomarker for mood disorders. Curr. Drug Targets.
Self-Directed Violence Classification System, n.d. United States Department ofVeteran Affairs. <http://www.mirecc.va.gov/visn19/education/nomenclature.asp> (retrieved 27.01.14).
Serafini, G., Pompili, M., Elena Seretti, M., Stefani, H., Palermo, M., Coryell, W.,Girardi, P., 2013. The role of inflammatory cytokines in suicidal behavior: asystematic review. Eur. Neuropsychopharmacol.: J. Eur. CollegeNeuropsychopharmacol. http://dx.doi.org/10.1016/j.euroneuro.2013.06.002.
Please cite this article in press as: Juengst, S.B., et al. Exploratory associations wtraumatic brain injury. Brain Behav. Immun. (2014), http://dx.doi.org/10.1016
Simpson, G., Tate, R., 2007. Suicidality in people surviving a traumatic brain injury:prevalence, risk factors and implications for clinical management. Brain Injury:[BI] 21 (13–14), 1335–1351. http://dx.doi.org/10.1080/02699050701785542.
Steiner, J., Gos, T., Bogerts, B., Bielau, H., Drexhage, H.A., Bernstein, H.-G., 2013.Possible impact of microglial cells and the monocyte-macrophage system onsuicidal behavior. CNS Neurol. Disord.: Drug Targets 12 (7), 971–979.
Strong, C.-A.H., Tiesma, D., Donders, J., 2011. Criterion validity of the Delis-KaplanExecutive Function System (D-KEFS) fluency subtests after traumatic braininjury. J. Int. Neuropsychol. Soc.: JINS 17 (2), 230–237. http://dx.doi.org/10.1017/S1355617710001451.
Tarkowski, E., Tullberg, M., Fredman, P., Wikkelsö, C., 2003. Correlation betweenintrathecal sulfatide and TNF-alpha levels in patients with vascular dementia.Dement. Geriatr. Cogn. Disord. 15(4), 207–211. doi:68780.
Teasdale, T.W., Engberg, A.W., 2001. Suicide after traumatic brain injury: apopulation study. J. Neurol. Neurosurg. Psych. 71 (4), 436–440.
Tonelli, L.H., Stiller, J., Rujescu, D., Giegling, I., Schneider, B., Maurer, K., Postolache,T.T., 2008. Elevated cytokine expression in the orbitofrontal cortex of victims ofsuicide. Acta Psychiatr. Scand. 117 (3), 198–206. http://dx.doi.org/10.1111/j.1600-0447.2007.01128.x.
Von Känel, R., Hepp, U., Kraemer, B., Traber, R., Keel, M., Mica, L., Schnyder, U., 2007.Evidence for low-grade systemic proinflammatory activity in patients withposttraumatic stress disorder. J. Psych. Res. 41 (9), 744–752. http://dx.doi.org/10.1016/j.jpsychires.2006.06.009.
Wagner, A.K., 2011. Rehabilomics: a conceptual framework to drive biologicsresearch. PM&R: J. Injury, Function, Rehabil. 3 (6 Suppl. 1), S28–S30. http://dx.doi.org/10.1016/j.pmrj.2011.04.013.
Wagner, A.K., Brett, C.A., McCullough, E.H., Niyonkuru, C., Loucks, T.L., Dixon, C.E.,Berga, S.L., 2012. Persistent hypogonadism influences estradiol synthesis,cognition and outcome in males after severe TBI. Brain Injury: [BI] 26 (10),1226–1242. http://dx.doi.org/10.3109/02699052.2012.667594.
Wasserman, L., Shaw, T., Vu, M., Ko, C., Bollegala, D., Bhalerao, S., 2008. An overviewof traumatic brain injury and suicide. Brain Injury: [BI] 22 (11), 811–819. http://dx.doi.org/10.1080/02699050802372166.
Wiegner, S., Donders, J., 1999. Performance on the California verbal learning testafter traumatic brain injury. J. Clin. Exp. Neuropsychol. 21 (2), 159–170. http://dx.doi.org/10.1076/jcen.21.2.159.925.
Wilcock, D.M., Griffin, W.S.T., 2013. Down’s syndrome, neuroinflammation, andAlzheimer neuropathogenesis. J. Neuroinflam. 10, 84. http://dx.doi.org/10.1186/1742-2094-10-84.
Wisco, B.E., Marx, B.P., Holowka, D.W., Vasterling, J.J., Han, S.C., Chen, M.S., et al.,2014. Traumatic brain injury, PTSD, and current suicidal ideation among Iraqand Afghanistan U.S. Veterans. J. Trauma. Stress. http://dx.doi.org/10.1002/jts.21900.
Woodcock, T., Morganti-Kossmann, M.C., 2013. The role of markers of inflammationin traumatic brain injury. Frontiers Neurol. 4, 18. http://dx.doi.org/10.3389/fneur.2013.00018.
Yurgelun-Todd, D.A., Bueler, C.E., McGlade, E.C., Churchwell, J.C., Brenner, L.A.,Lopez-Larson, M.P., 2011. Neuroimaging correlates of traumatic brain injuryand suicidal behavior. J. Head Trauma Rehabil. 26 (4), 276–289. http://dx.doi.org/10.1097/HTR.0b013e31822251dc.
ith Tumor Necrosis Factor-a, disinhibition and suicidal endorsement after/j.bbi.2014.05.020