CV Lecture 7 - Fiziologiefiziologie.ro/en/2015-2016/lectures/Lecture 7_CV_2016.pdfthe heart pumps...
64
CV Lecture 7 CV system regulation
Transcript of CV Lecture 7 - Fiziologiefiziologie.ro/en/2015-2016/lectures/Lecture 7_CV_2016.pdfthe heart pumps...

CV Lecture 7
CV system regulation

Cardiovascular regulation
A. Local (intrinsic) regulation
B. Systemic (extrinsic) regulation
Heart activity
Vascular tone
CV Integration

LV
Cardiovascular ‘unit’
= R 8 π
. ηl r 4
= R ΔP F

A. Local/intrinsic regulation
Heart activity regulation
1. Ca2+ role
- Ca2+ homeostasis
- Ca2+ regulation factors
2. Frank-Starling low of the heart
3. Other +/- inotropic factors
Microcirculation regulation
1. Myogenic autoregulation
2. Metabolic factors, chemical messengers, endothelial factors
Atmospheric O2, angiogenesis...
B. Systemic regulation
Short-term regulation
- Nervous reflex regulation
Long-term regulation
Integrated regulation
- Humoral regulation
Short-term regulation
Long-term regulation

A. Local Regulation
Heart activity regulation 1. Ca2+ role
- Ca2+ homeostasis
- membrane transport systems for Ca2+
Calsequestrin
Sarcoplasmic reticulum
Ca2+ pump
Ca2+ channels Na+/Ca2+
exchanger
Na+/K+ pump Ca2+
pump
Phospholamban
(unphosphorilated)
(-)

Heart activity regulation
1. Ca2+ role Ca2+ regulation factors - sympathetic stimulation via β1 receptors cAMP PKA
phospholamban phosphorylation its inhibition on SERCA is
relieved upon phosphorylation ↓ [Ca2+]i lusitropic effect
& more Ca stored in SR +inotropic effect
L-type Ca Channels
- “garden-hose” effect: regulation by changes in coronary perfusion pressure
↑ [Ca2+]i
- ↑ heart rate – positive (Bowditch) staircase:
cumulative increase in [Ca2+]i ↑ contractility
- cardiac glycosides (digitalis):
inhibit Na/K pump, Na/Ca exchanger ↑ [Ca2+]i
- pH: intracell H+ competes with Ca2+ for binding on troponine complex
A. Local Regulation


T-tubule
Sarcoplasmic
reticulum
Sarcoplasmic
reticulum

Heart activity regulation
2. Frank-Starling low of the heart: within physiological limits, the heart pumps all the blood that returns to it
- Preload: the wall tension that corresponds to ED pressure venous return - skeletal mm pump & respiratory pump
- sympathetic constriction of veins
EDV - length of sarcomere at beginning of contraction - Afterload – blood pressure - total peripheral resistance
- Inotropic state of the heart
A. Local Regulation
2,2 µm 1,8 µm 2,8 µm

Frank-Starling law of the heart
The more blood there is in the ventricle at the beginning of contraction
(EDV), the greater the stroke volume will be. Stroke volume is
proportional to force.

A A’ A” B B’ B”
D” D’
E”
E’ E
D
Left Ventricular Volume
Left
Ven
tric
ula
r P
ressu
re
Frank-Starling law of the heart
normal
↑ EDV
↓ EDV
End-systolic pressure-volume relation

3. Inotropic factors:
- Extracellular Ca2+
- Adrenergic agonists activate through β1-receptors
G proteins AMPc PKA protein phosphorylation - Cardiac glycosides (digitalis) – Na/K-pump
- Increase in heart rate
- Ca channels blockers
- Extracellular Na+
Intracellular Ca2+
Negative
- Intracellular H+
- Extracellular Ca2+
- Extracellular Na+ Positive

Hormones effects on cardiac contractility
Circulating catecholamines from adrenal medulla, but rarely rise
sufficiently high to affect cardiac function appreciably.
Thyroid hormones enhance myocardial contractility (increase the rates
of calcium uptake and of ATP hydrolysis by the SR; increase protein
synthesis cardiac hypertrophy; increase myosin isoenzymes with
the greatest ATPase activity enhance myocardial contractility
substantially. In hyperthyroidism: tachycardia, high cardiac output,
palpitations, and arrhythmias.
Insulin enhances myocardial contractility, partially explained by the
concomitant increase of glucose transport into the myocardial cells.
Glucagon has potent positive inotropic and chronotropic effects on the
heart, mediated by activation of the adenylyl cyclase-cAMP system.

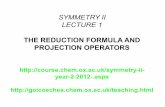
Blood gases affect the heart directly and indirectly
• Indirect effects - changes in PaO2 and PaCO2 of the blood perfusing the
brain and the peripheral chemoreceptors affect the heart through nervous
mechanisms.
Moderate degrees of hypoxia characteristically increase heart rate, cardiac
output, and myocardial contractility by increasing sympathetic nervous
activity (changes largely abolished by blocking β-adrenergic receptor)
Also, systemic increases in PaCO2 activate the sympatho-adrenal system.
• Direct effects - PaO2 of the blood perfusing the myocardium also
influences myocardial performance directly. The effect of hypoxia is
biphasic: moderate degrees are stimulatory and more severe degrees
are depressant.
Direct depressant effect of the increased PaCO2 on the heart: act
through reduced intracellular pH diminishes the influx of Ca2+ into the
cell via Ca channels, Na/Ca antiporter, decreases Ca2+ released from SR,
and affects myofilament sensitivity to Ca2+ directly.

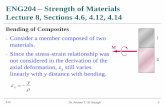
Effect of ischemia on left ventricular pressure and intracellular pH in an isolated
perfused rabbit heart.

LV
Cardiovascular ‘unit’
= R 8 π
. ηl r 4
= R ΔP F

A. Local/intrinsic regulation
Heart activity regulation
1. Ca2+ role
- Ca2+ homeostasis
- Ca2+ regulation factors
2. Frank-Starling low of the heart
3. Other +/- inotropic factors
Microcirculation regulation
1. Myogenic autoregulation
2. Metabolic factors, chemical messengers, endothelial factors
Atmospheric O2, angiogenesis...
B. Systemic regulation
Short-term regulation
- Nervous reflex regulation
Long-term regulation
Integrated regulation
- Humoral regulation
Short-term regulation
Long-term regulation

Φ = 1; F= 1ml/min
Φ = 2; F= 16ml/min
Φ = 4; F= 256ml/min
P=
100 m
mH
g
Microcirculation regulation
A. Local Regulation
l F
h
p
8
P r 4
D = Flow dependence on radius

100
75
50
25
0
Pre
ssu
re (
mm
Hg
)
art
eri
es
art
eri
ols
cap
ilari
es
vein
s
Effect of arteriolar vascular tone on arterial pressure
arteriolar dilation
normal
arteriolar constriction
A. Local regulation of microcirculation

Myogenic factors
Metabolic factors
Microcirculation regulation
A. Local Regulation - Short-term regulation
Chemical messengers, paracrines, endothelial
vasoactive factors

Myogenic factors
- stretch-activated nonselective cation channels…
Microcirculation regulation
A. Local Regulation - Short-term regulation
- myogenic autoregulation: vasoconstriction due to ↑ stretch
of wall when pressure ↑
- endothelins (ET): vasoconstrictor paracrines released
from endothelial cells as a response to stretch
Basal tone / tonic activity of vascular smooth mm,
independent on nervous system, related with intrinsic activity

-CO2, O2, H+/lactic ac, K+, ADP, adenosine (A rec–KATP channels
hyperpolarization), PGI2, NO…
-ATP (P2x rec = ligand-gated Ca channel), TxA2
Metabolic factors
Microcirculation regulation
A. Local Regulation - Short-term regulation
Chemical messengers, paracrines, endothelial
vasoactive factors
-Ach/bradykinine (NO), VIP, NE/E, histamine, serotonin
-ET (IP3&DAG, Ca2+)
-NO released by endothelial cells in response to shear stress
during rapid flow

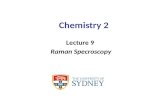
Function of cellular metabolism
0 1 2 3 4 5 6 7
Metabolic rate (x normal)
B
loo
d F
low
x n
orm
al
0 1
2 3 4
A. Local Regulation - Short-term regulation

Metabolic rate ↑
Production of CO2 ↑
CO2 tissue conc. ↑
Arteriolar smooth mm.
↑ Vasodilation
↓ Resistance
↑ Blood flow
↓ CO2 tissue conc.
Negative feed-back
Metabolic regulation: CO2 concentration effect
A. Local Regulation - Short-term regulation

Blood flow
Vasodilators: Vasoconstrictors:

Nitric Oxide (NO) - EDRF
- ↑[Ca2+]i
Ach, bradykinine
shear stress
- Free radical & Lipophilic gas with short half-life (5-10 sec)
- NO origin: endothelial, muscular, neuronal…
- Potent vasodilator, inhibit platelet adhesion & aggregation
- NO NO rec = soluble GC cGMP vasodil.
activation of Ca pump in the SR ↓ [Ca2+]i vasodil.
(+) eNOS L-arginine NO + L-citruline

Metabolic regulation of blood flow:
Hyperemia
1. Active Hyperemia 2. Reactive Hyperemia

.
A. Long-term regulation of microcirculation
Oxygen role
- altitudine: decreased atm. O2 , erythropoietin
- decreased conc. O2 in the incubator for
premature babies influence on angiogenesis
Angiogenesis stimulating growth factors – endothelial
derived growth factor (VEGF), fibroblastic GF…

Intrinsic versus extrinsic control of
vascular tone
Intrinsic Control
-Auto-regulation (capacity
to resist changes in flow
with pressure changes)
-Endothelium-mediated
regulation (act as a barrier
for vasoactive substances)
-Metabolic regulation
(generation of substances
with vasodilating activity
that are involved in
hyperemic responses)
Extrinsic control
- Sympathetic (Norepi.) –
Most important, fast reg.
-Parasympathetic (Causes
vasodilation) - Less important
-Humoral circulating factors
(catecholamines and non-
catecholamines) – long-term
regulation

B. Systemic Regulation
- Short-term regulation
Nervous reflex regulation
- Intermediate/Long-term regulation
- Integrated regulation
Humoral regulation
Renal-body fluid control system

B. Systemic Regulation

Nervous Regulation through ANS
= Cardiovascular reflexes – with fast response
- Regulation factors: arterial pressure, volume
changes, H+, O2, CO2 conc.
-Types of receptors:
1. arterial & cardiopulmonary mechanoreceptors:
baroreceptors & volum-receptors
2. chemoreceptors
- Correlations with humoral regulation: ADH,
ANP, suprarenal hormones

Cardiovascular Reflexes:
baro- & chemoreceptors reflexes

(-)
Vagal n.
Cardiovascular Nervous Regulation

Vasomotor center: 1. Vasoconstrictor area
2. Vasodilator area: inhibits 1.
3. Sensory area: bilaterally in the
tractus solitarus (NTS), receives
sensory nerves signals from the
circulatory system throught n. X
& IX; controls 1. & 2. reflex
control
4. Cardioinhibitor center dorsal
motor nc. vagal nerve

Autonomic Nervous Regulation
S and PS branches of the ANS influence HR and AV node conduction through antagonistic control
PS: 70/min -- SAN: intrinsic rate of 90-100/min -- S: >100/min (Ach, muscarinic rec) (NE, b1 rec)
S tone - increase HR, AV conduction and contractility (b1rec) - determine vc by a1rec (NE) and vd by b2 rec (E in heart, liver, skeletal mm – fight or flight response)
PS tone - decrease HR and AV conduction
- M rec (Ach) AC(-), Ach-regulated K channels…
- Ach NO vd
ANS fast responses: within 3 -5 sec. HR can increase 2x within 10-15 sec. AP can be doubled

Effects of sympathetic neural regulation on vascular tone
NE binds to α receptors constriction.
E binds to both β and α receptors, but more to β receptors dilation.

150
125
100
75
50
25
0
A
rte
ria
l p
ressu
re (
mm
Hg
)
0 5 10 15 20 min. Effect of total spinal anesthesia on the arterial pressure,
showing a marked decrease in pressure resulting from
loss of vasomotor tone (NE=norepinephrine)
NE inj.
Total spinal anesthesia

Effect of NE on contractility of the heart

Changes in heart rate evoked by stimulation (horizontal bars) of the
vagus (A) and sympathetic (B) nerves in an anesthetized dog.

CV Nervous Regulation
Cardio-inhibitory
activity
NTS
n. IX
Vagus n
Dorsal nc of the Vag n + Nc. Ambiguus
-
CV stim. activity Vagus n – PS preggl. fb.
Adrenal medulla
S postggl. fb.
venules
arterioles
Spinal cord Arterial
baroreceptors

• Baroreceptors /stretch/pressorec.
– are pressure sensitive neurons in the aortic arch and carotid sinus.
– fast (sec.) response to decreased arterial pressure (AP) by concomitantly: - decreasing cardioinhibitory activity - increasing both cardio-acceleratory activity and the vasoconstrictor center
(all in the medulla oblongata)
arterio&venoconstriction
stimulation of the heart: increased HR and contraction
Baroreceptor Reflex

Baroreceptor Reflex

Imp
uls
es/ sec.
fro
m c
aro
tid
sin
us n
n.
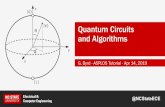
0 80 160 240 mmHg
AP effect on carotid baroreceptors response
Baroreceptors response in arterial pressure changes
Max rate at
180 mmHg
Obs: aortic barorec operate
at press 30 mmHg higher

http://cvphysiology.com/Blood%20Pressure/BP012.htm
The “resetting” of the baroreceptors may
attenuate their potency as a control system for
correcting disturbances that tend to change
arterial pressure for longer than a few days at a
time.
Baroreceptors tend to reset in 1-2 days to the
pressure level to which they are exposed.
Ex: if the arterial pressure rises from 100 mmHg
to 160 mmHg, a very high rate of baroreceptor
impulses are at first transmitted. During the next
few minutes, the rate of firing diminishes
considerably; then it diminishes much more
slowly during the next 1-2 days, at the end of
which time the rate of firing will have returned to
nearly normal despite the fact that the mean
arterial pressure still remains at 160 mm Hg.
Conversely, when the arterial pressure falls to a
very low level, the baroreceptors at first transmit
no impulses, but gradually, over 1-2 days, the
rate of baroreceptor firing returns toward the
control level.


150
125
100
75
50
25
0 A
rte
ria
l P
res
su
re (m
m H
g)
2 4 6 8 10 12 min.
Sino-carotidian reflex effect on AP
Carotid arteries
occlusion
Carotid a.
reperfusion
Both vagal nerves blocked

The Baroreceptors Attenuate Blood Pressure
Changes During Changes in Body Posture.
The ability of the baroreceptors to maintain relatively
constant arterial pressure in the upper body is
important when a person stands up after having been
lying down.
Immediately on standing, the arterial pressure in the
head and upper part of the body tends to fall, and
marked reduction of this pressure could cause loss of
consciousness. However, the falling pressure at the
baroreceptors elicits an immediate reflex, resulting in
strong sympathetic discharge throughout the body that
minimizes the decrease in pressure in the head and
upper body.

The Valsalva manoeuvre & the baroreceptor reflex
The patient breathes out forcefully against a closed larynx
- "straining" an increased intrathoracic pressure
decreased venous return, cardiac output and a fall in
blood pressure reduced baroreceptor discharge to the
vasomotor centre peripheral vasoconstriction, and an
increase in heart rate (normal response).



Atrial sensory receptors regulate cardiac and renal function
Bainbridge Reflex
Bainbridge (1915): infusions of blood or saline solution increased the
heart rate, regardless of whether the infusions did or did not raise
the arterial blood pressure; the effect was abolished by cutting both
vagi.
Sensory receptors in both atria, located principally in the venoatrial
junctions, influence heart rate. Their distention sends impulses centrally
in the vagi. The efferent impulses are carried by S and PS fibers to the
SA node.
Stimulation of the atrial receptors also increases urine flow (reduced
secretion of vasopressin/antidiuretic hormone, reduction in renal
sympathetic nerve activity, and the release of atrial natriuretic peptide,
from the atrial tissues in response to atrial contraction and stretch).
Increased venous return stimulates atrial mechanoreceptors which:
– Directly stimulates the SA node to increase its firing rate
– Stimulates the cardioacceleratory center in the medulla oblongata
which causes an increase in sympathetic output to the heart.

Intravenous infusions of blood or electrolyte solutions tend to increase
heart rate via the Bainbridge reflex and to decrease heart rate via the
baroreceptor reflex.
The actual change in heart rate induced by such infusions is the result
of these two opposing reflex actions.
Bainbridge reflex

Ventricular sensory receptors affect cardiac function
in a reflex way
Sensory receptors located in the ventricular endocardium initiate
reflex effects similar to those elicited by the arterial baroreceptors
diminishes heart rate and peripheral vascular resistance.
The receptor discharge pattern parallels the changes in ventricular
pressure. Impulses originating in these receptors are transmitted to
the medulla oblongata via the vagus nerves.
Other sensory receptors in the epicardial regions of the ventricles,
are stimulated by various mechanical and chemical stimuli, but their
physiological functions are not clear.

Chemoreceptor reflexes
- Stim. of chemoreceptors by decreased O2, pH and increased CO2
- The chemosensitive cells are located in the 2 mm sized chemoreceptor
organs (two carotid bodies, one of which lies in the bifurcation of each
common carotid artery, and usually one to three aortic bodies adjacent to
the aorta).
- The chemoreceptors excite nerve fibers that, along with the baroreceptor
fibers, pass through Hering’s nerves and the vagus nerves into the
vasomotor center of the brain stem.
- Each carotid or aortic body is supplied with an abundant blood flow
through a small nutrient artery, so the chemoreceptors are always in
close contact with arterial blood and sense arterial pressure falls below a
critical level, when they become stimulated .
- The signals transmitted from the chemoreceptors excite the vasomotor
center, and this response elevates the arterial pressure back toward
normal.
- Chemoreceptor reflex is not a powerful arterial pressure controller until
the arterial pressure falls below 80 mm Hg becomes important at the
lower pressures to prevent further decreases in arterial pressure.


CNS ischemic response: control of arterial pressure by
the brain’s vasomotor center in response to diminished
brain blood flow
When blood flow to the vasomotor center in the lower brain stem becomes
decreased severely enough to cause nutritional deficiency/cerebral ischemia,
the vasoconstrictor and cardioaccelerator neurons in the vasomotor center
respond directly to the ischemia and become strongly excited.
When this excitation occurs, the systemic arterial pressure often rises to a
level as high as the heart can possibly pump.
This effect is believed to be caused by failure of the slowly flowing blood to
carry CO2 away from the brain stem vasomotor center stimulate
sympathetic vasomotor nervous control areas.
The ischemic effect on vasomotor activity can elevate MAP dramatically (up
to 250 mm Hg) for as long as 10 minutes. The degree of sympathetic
vasoconstriction caused by intense cerebral ischemia is often so great that
some of the peripheral vessels become totally or almost totally occluded.
The kidneys often entirely cease their production of urine because of renal
arteriolar constriction in response to the sympathetic discharge.
CNS ischemic response is an emergency pressure control system, a
powerful activator of the sympathetic vasoconstrictor system !

Cushing Reaction to Increased Pressure Around the Brain - a
special type of CNS ischemic response that results from increased
pressure of the cerebrospinal fluid around the brain in the cranial vault.
-cerebrospinal fluid pressure rises to equal the arterial pressure, it
compresses the whole brain, as well as the arteries in the brain, and
cuts off the blood supply to the brain initiates a CNS ischemic
response arterial pressure rise to a level higher than the
cerebrospinal fluid pressure blood flows once again into the vessels
of the brain to relieve the brain ischemia -> the blood pressure comes
to a new equilibrium level slightly higher than the cerebrospinal fluid
pressure, thus allowing blood to begin to flow through the brain again.
The Cushing reaction helps protect vital centers of the brain from loss
of nutrition if the cerebrospinal fluid pressure ever rises high enough to
compress the cerebral arteries.

Long-term Humoral Regulation 1) Vasoactive substances released in the blood/proximity of vascular
smooth mm effect on AP & local blood flow
Biogenic amines:
-E (MSR, a1R–vc, b2R-vd, b1R-↑HR & contractility)
-serotonin (local vc)
-histamine (local vd)
Peptides:
-Angiotensin II (vc) - AT1A rec
-Endothelins (the most powerful vc)
-ANP (vd)
-Kinins (vd): bradykinins
- Vasopressine/ADH (vc. at high level)
Prostaglandins:
-vd: PGI2, PGE2; vc: TxA2
Nitric oxide (vd)
2) Non-vasoactive substances effective circulating volume: kidney,
by regulating total-body Na content effect on MAP, CO
Renin-ANG II-aldosterone axis, AVP, ANP
B. Systemic Regulation

Renin-ANG II-aldosterone axis



Factors that affect cardiac output

Integrated regulation
Filling time
Filling pressure
Vasc compliance
preload
contractility
afterload
EDV ESV Intrinsic
Regul Extrinsic
Regul
CO Total Peripheral
Resistance
Systemic
Reg
Local
Reg
Stroke
Volume HR
MAP
Humoral
factors
ANS
Venous return
- Regulation ?