Cost-utility analysis of oral deferasirox versus infusional deferoxamine in transfusion-dependent...
8
TRANSFUSION PRACTICE Cost–utility analysis of oral deferasirox versus infusional deferoxamine in transfusion-dependent b-thalassemia patients Ali Keshtkaran, Mehdi Javanbakht, Sedigheh Salavati, Atefeh Mashayekhi, Mehran Karimi, and Bijan Nuri BACKGROUND: Deferasirox (DFX) is a novel iron chelator that has been shown to have similar efficacy and safety compared with deferoxamine (DFO) in patients with b-thalassemia. The aim of this study was to determine the cost utility of DFX versus DFO in b-thalassemia major patients from Iran’s society perspective. STUDY DESIGN AND METHODS: A Markov model has been developed to determine lifetime cost and quality-adjusted life-years (QALYs) of patients. To esti- mate the annual cost of each method, a cross-sectional study was conducted among two groups of patients who received DFO and DFX (n = 100 and n = 45, respectively). Also a time trade-off method was used to estimate the utility of two strategies. Finally a one-way and probabilistic sensitivity analysis was conducted to examine the strength of the results. RESULTS: Our base-case analysis showed that esti- mated total lifetime costs per patient for DFX and DFO were 47,029 international dollar ($Int) and $Int143,522, respectively, while the estimated total discounted QALYs per person were 12.28 and 7.76, respectively. Calculated incremental cost-effectiveness ratio showed that DSX is a dominant therapy and its estimated life- time net monetary benefit was $Int273,528. CONCLUSION: We conclude that the use of DFX instead of DFO represents a cost-effective use of resources for treatment of iron overload in patients with b-thalassemia from Iran’s society perspective. T halassemia is the most prevalent hereditary hematologic disorder in the world, particularly in Asia. 1,2 Severe b-thalassemia accounts for 50,000 to 100,000 deaths per year or 0.5% to 0.9% of all deaths of children under 5 years old in low- or middle-income countries. 3 Analysis of literature showed that approximately 80% of the annual live births with these conditions occur in low- and middle-income coun- tries where many of them have limited facilities. 4 Iran is geographically and epidemiologically in the middle of a stretch of land called the thalassemia belt. 5 Until now more than 25,000 affected individuals have been reported. A high prevalence of b-thalassemia occurs in the northern (Caspian Sea coast) and southern (Persian Gulf and Oman Sea coasts) areas of the country. The overall prevalence ranges approximately from 3 to 100 patients per 100,000 people in different provinces. 5,6 Annually a large amount of financial resources are allo- cated to these patients by the Iran health system. b-Thalassemia patients need repeated transfusions that result in iron overload in their parenchymal tissues and this iron overload, without iron chelation therapy, ABBREVIATIONS: DFO = deferoxamine; DFP = deferiprone; DFX = deferasirox; ICER = incremental cost-effectiveness ratio; $Int = international dollar; NMB = net monetary benefit; QALY(s) = quality-adjusted life-year(s); TTO = time trade-off. From the Health Economics Department, Health Care Management School, Shiraz University of Medical Sciences, Shiraz, Iran. Address reprint requests to: Mehdi Javanbakht, Health Management and Economics Research Center, School of Health Management and Information Sciences, Tehran University of Medical Sciences, PO Box 141765376, Tehran, Iran; e-mail: [email protected]. This study was supported partially by a Grant 323 from Shiraz University of Medical Sciences. Received for publication May 8, 2012; revision received September 14, 2012, and accepted September 26, 2012. doi: 10.1111/trf.12024 TRANSFUSION 2013;53:1722-1729. 1722 TRANSFUSION Volume 53, August 2013
Transcript of Cost-utility analysis of oral deferasirox versus infusional deferoxamine in transfusion-dependent...

T R A N S F U S I O N P R A C T I C E
Cost–utility analysis of oral deferasirox versus infusionaldeferoxamine in transfusion-dependent b-thalassemia patients
Ali Keshtkaran, Mehdi Javanbakht, Sedigheh Salavati, Atefeh Mashayekhi, Mehran Karimi, and
Bijan Nuri
BACKGROUND: Deferasirox (DFX) is a novel ironchelator that has been shown to have similar efficacyand safety compared with deferoxamine (DFO) inpatients with b-thalassemia. The aim of this study wasto determine the cost utility of DFX versus DFO inb-thalassemia major patients from Iran’s societyperspective.STUDY DESIGN AND METHODS: A Markov modelhas been developed to determine lifetime cost andquality-adjusted life-years (QALYs) of patients. To esti-mate the annual cost of each method, a cross-sectionalstudy was conducted among two groups of patientswho received DFO and DFX (n = 100 and n = 45,respectively). Also a time trade-off method was used toestimate the utility of two strategies. Finally a one-wayand probabilistic sensitivity analysis was conducted toexamine the strength of the results.RESULTS: Our base-case analysis showed that esti-mated total lifetime costs per patient for DFX and DFOwere 47,029 international dollar ($Int) and $Int143,522,respectively, while the estimated total discountedQALYs per person were 12.28 and 7.76, respectively.Calculated incremental cost-effectiveness ratio showedthat DSX is a dominant therapy and its estimated life-time net monetary benefit was $Int273,528.CONCLUSION: We conclude that the use of DFXinstead of DFO represents a cost-effective use ofresources for treatment of iron overload in patients withb-thalassemia from Iran’s society perspective.
Thalassemia is the most prevalent hereditaryhematologic disorder in the world, particularlyin Asia.1,2 Severe b-thalassemia accounts for50,000 to 100,000 deaths per year or 0.5% to 0.9%
of all deaths of children under 5 years old in low- ormiddle-income countries.3 Analysis of literature showedthat approximately 80% of the annual live births withthese conditions occur in low- and middle-income coun-tries where many of them have limited facilities.4
Iran is geographically and epidemiologically in themiddle of a stretch of land called the thalassemia belt.5
Until now more than 25,000 affected individuals havebeen reported. A high prevalence of b-thalassemia occursin the northern (Caspian Sea coast) and southern (PersianGulf and Oman Sea coasts) areas of the country. Theoverall prevalence ranges approximately from 3 to 100patients per 100,000 people in different provinces.5,6
Annually a large amount of financial resources are allo-cated to these patients by the Iran health system.
b-Thalassemia patients need repeated transfusionsthat result in iron overload in their parenchymal tissuesand this iron overload, without iron chelation therapy,
ABBREVIATIONS: DFO = deferoxamine; DFP = deferiprone;
DFX = deferasirox; ICER = incremental cost-effectiveness ratio;
$Int = international dollar; NMB = net monetary benefit;
QALY(s) = quality-adjusted life-year(s); TTO = time trade-off.
From the Health Economics Department, Health Care
Management School, Shiraz University of Medical Sciences,
Shiraz, Iran.
Address reprint requests to: Mehdi Javanbakht, Health
Management and Economics Research Center, School of Health
Management and Information Sciences, Tehran University of
Medical Sciences, PO Box 141765376, Tehran, Iran; e-mail:
This study was supported partially by a Grant 323 from
Shiraz University of Medical Sciences.
Received for publication May 8, 2012; revision received
September 14, 2012, and accepted September 26, 2012.
doi: 10.1111/trf.12024
TRANSFUSION 2013;53:1722-1729.
1722 TRANSFUSION Volume 53, August 2013

increases the iron burden of the body, leading to a growingimpairment of the heart, liver, and endocrine glands.7-9
Since humans have no physiologic mechanisms to elimi-nate iron from their bodies, iron chelation therapy hasbeen recommended for transfusion-dependent patientswith iron overload.10 Deferoxamine (DFO) is the standardtreatment for iron overload that is administered in a sub-cutaneous or intravenous infusion for 8 to 12 hours, 5 to 7days a week using a portable pump.11-13 In recent years,oral deferasirox (DFX) has also been represented as amethod of treatment for iron overload. DFX is a once-dailyoral chelation agent and it has shown efficacy in reducinghepatic injuries and the iron burden of the body.14-16 InIran DFO has been a licensed treatment and in 2008 DFXwas also allowed to be prescribed for b-thalassemiapatients.
Recent clinical evidence has demonstrated that DFXin the recommended doses of 20 to 30 mg/kg/day has anefficacy similar to that of DFO at equivalent doses in thecontrol of chronic iron overload.7,17,18 The main differencebetween them is in the mode of administration andmechanism of action that can lead to poor or high com-pliance with different subsequent impacts on quality oflife.
Although thalassemia mostly affects developingcountries, there is limited knowledge of cost and effective-ness of its treatments; therefore, we designed this studyto determine the cost utility of DFX versus DFO, whichare the most commonly used iron-chelating therapies inIran.
MATERIALS AND METHODS
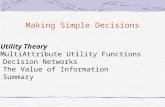
Study designThis study is an economic evaluation conducted from theviewpoint of Iran’s society. A Markov model has beendeveloped to determine the cost utility of DFX comparedwith DFO therapies in b-thalassemia patients. We used themodel to calculate lifetime costs, life-years, and quality-adjusted life-years (QALYs) of each strategy. The incre-mental cost-effectiveness of DFX versus DFO therapy wascalculated and defined in terms of the ratio of the differ-ence in lifetime costs to the difference in QALYs. Theexpected costs and consequences of two strategies werecompared using a lifetime time horizon (modeling withinpatient’s life expectancy). We used 5 and 3% annual dis-count rate to discount future costs and QALYs, respec-tively. It has been shown that cardiac disease is a majorcause of deaths in patients with transfusion-dependentb-thalassemia.19 Therefore, we constructed our Markovmodel with tree health status: b-thalassemia withoutcardiac complication, b-thalassemia with a cardiac com-plication, and death (Fig. 1). We assumed that transitionsbetween health status occurred annually20,21 and theirprobabilities were derived from previous studies (Table 1).
CostsIn this study, both direct and indirect cost of the treatmentfor iron overload was considered. Using a randomizedsampling method, 45 and 100 subjects were recruitedfrom patients who received DFX and DFO, respectively. To
Fig 1. Structure of Markov model.
COST UTILITY OF DEFERASIROX VS. DEFEROXAMINE
Volume 53, August 2013 TRANSFUSION 1723

estimate annual medical costs, medical records of thesubjects were used to extract the drug dosage and otherresources that they received over a year. Direct medicalcost included drug, pump, and transfusion kit cost in theDFO group and drug cost in the DFX group. Finallythe annual medical cost was calculated by multiplying themean annual utilized medical resource by the cost of everyunit of drug and medical equipment in two groups. Theannual cost for treatment of cardiac complication wasderived from a study that has been conducted in Iran.According to the previous study there are no significantdifferences in rates of serious adverse events between twogroups,22 although patients in DFX group reportedadverse events such as nausea, rash, diarrhea, nonseriousabdominal pain, and vomiting more than those whoreceived DFO. Since prescribed drugs for treatment of theside effects were registered in patients’ medical records,we estimated annual cost using each patient’s medicalrecord and price of each medication. Since some of theindirect costs such as time cost of patients for blood trans-fusion and consulting with medical staff are the same inthe two groups, only extra indirect cost in DFO group hasbeen estimated. Therefore, transfusion time cost has beenincluded in indirect cost. To estimate this cost mean timeof transfusion in weeks has been asked from patients in
the DFO group and then annual indirect cost was esti-mated using the human capital approach. To have aninternational perspective the costs were converted fromIranian Rials (IRR) into international dollars ($Int), basedon purchasing power parities, which is a method of mea-suring the relative purchasing power of the currencies ofdifferent countries over the same types of goods and ser-vices, by eliminating the differences in price levelsbetween countries.
UtilityA time trade-off (TTO) method was employed to deter-mine the utility associated with receiving an oral or a slowsubcutaneous iron chelator with taking into account pres-ence or absence of cardiac complication. The US panel oncost-effectiveness suggested that the patients tend toexaggerate in evaluating the utility of their conditions.23
Therefore, we conducted a TTO exercise in a sample of 40nurses to elicit utility values for different modes of admin-istration of chelation therapy.
Transitions probabilityThe cardiac complication probabilities derived from twostudies.24,25 These studies provided a cardiac complication
TABLE 1. Base-case values for the model variablesInput variables Value 95% CI References
Dosage prescribedDFO mg/kg/day for 5 days of each week 40.8* (37.1-44.4) CalculatedDFX mg/kg/day every day of the week 24.7* (22.5-26.9) Calculated
Annual cost ($Int)DFO
Drug 6,575.4* (5,953.7-7,197.2) CalculatedPump 85.1 (83.1-87.1) CalculatedInfusion kit 330.8 (310.3-351.2) CalculatedSide effects 6.1* (5.8-6.4) CalculatedTransfusion time 4,525.0 (4,695.3-5,106.8) CalculatedTotal DFO 11,692.8 (10,849-12,536.3)
DFXDrug 3,803.2* (3,451.7-4,154.6) CalculatedSide effects 11.2* (10.3-12.9) CalculatedTotal DFX 3,814.8 (3,462.9-4,165.9)Cardiac complication cost 353 (289-416) Javanbakht et al.33
Utility valuesb-Thalassemia with DFO 0.56 (0.49-0.63) Calculatedb-Thalassemia with DFX 0.82 (0.78-0. 86) Calculatedb-Thalassemia with DFO and a cardiac complication 0.42 (0.38-0.46) Calculatedb-Thalassemia with DFX and a cardiac complication 0.70 (0.67-0.73) Calculated
Transition probabilitiesFrom b-thalassemia to thalassemia with a cardiac complication (DFO) 0.0199 Borgna-Pignatti et al.,24
Ladis et al.25
From b-thalassemia to thalassemia with a cardiac complication (DFX) 0.0104 Pennell et al.34
From b-thalassemia to death Varies Borgna-Pignatti et al.,9
Ladis et al.,25
Pourmalek et al.26
From b-thalassemia with a cardiac complication to death Varies Pourmalek et al.,26
Chouliaras et al.27
* These estimates are based on the mean prescribed dosages of DFX and DFO among studied subjects.
KESHTKARAN ET AL.
1724 TRANSFUSION Volume 53, August 2013

probability, which was converted into an annual risk ofhaving cardiac complications. For b-thalassemia patientswithout cardiac disease, we estimated the risk of death bymultiplying Iranian age-specific mortality by a relative riskof 3.9.20,21,26 Annual probability of death in thalassemiapatients with cardiac disease was estimated, using datafrom a cohort study of thalassemia patients who werefollowed up to determine the risk of cardiac-relateddeath.27
Statistical analysisThe mean estimates of the TTO responses and annual costfor both DFO and DFX were compared after checking fornormality using the Kolmogorov-Smirnov test. Withregard to nonnormality in the distribution of TTOresponses, the nonparametric Wilcoxon signed-rank sta-tistical test was used to determine if a statistical differenceexists between two groups. The Mann-Whitney test wasused to determine any difference in costs of two strategies.Also 95% confidence intervals (CIs) were calculated usingthe bias-corrected accelerated percentile bootstrappingmethod for cost and utility.
For base-case analysis the Markov model was simu-lated to calculate the expected proportion of patients whowould develop iron overload–related cardiac disease, theexpected costs of each strategy, life-years, QALYs, incre-mental cost-effectiveness ratio (ICER), and net monetarybenefit (NMB). Since the ICER has poor statistical proper-ties within the range of values relevant to this study, wealso calculated the NMB by assigning a monetary value toa unit of effectiveness (ceiling rate [CR]) and multiplying itby the net number of units of effectiveness achieved.The ceiling rate represents the maximum amount thatsociety would be willing to pay for the incrementalimprovement in health. According to the World HealthOrganization guideline, medical interventions with a cost-effectiveness of less than three times gross domesticproduct per capita per QALY are generally considered tobe cost-effective.28,29
Finally, we conducted a determinis-tic one-way sensitivity analysis to deter-mine the strength of the results, and itsresults are presented by a tornadodiagram. We also conducted a probabi-listic sensitivity analysis to determinethe effect of all variable uncertaintysimultaneously within the model usingMonte Carlo simulation. We assignedbeta-distributions for transition prob-abilities and utility variables andgamma-distributions for costs. Allmodels and simulation were con-structed with computer software(Treeage, http://www.treeage.com/).
RESULTS
Base-case analysisTo estimate the utility of the two methods, 40 nurses wereinterviewed. A total of 50% of the respondents werefemale, 40% of them were in the 20- to 30-year age group,32% aged 31 to 40 years, and 28% aged 40 years and older.The mean utilities of patients who received DFO and DFXwith cardiac complication were 0.42 (95% CI, 0.38-0.46)and 0.70 (95% CI, 0.67-0.73) and without cardiac compli-cations were 0.56 (95% CI, 0.49-0.63) and 0.82 (95%CI, 0.86-0.78), respectively. The mean utility of thepatients in the DFX group was significantly higher thanDFO in both conditions (p < 0.001).
The main characteristics of subjects that wererecruited to estimate annual cost were as follows in theDFO and DFX groups, respectively: approximately 49 and45% were female, the mean � SD ages were 16 � 7.2 and18 � 8.6 years, and the mean weights were 36 � 13and 38 � 11.4 kg. Table 1 shows the mean daily prescribeddosage and annual costs per patient for each strategy. TheMann-Whitney test showed that there was a significantdifference in the annual costs between two groups(p < 0.0001).
Our base-case analysis showed the estimated totallifetime costs of using DFX and DFO per patients were$Int47,029 and $Int143,522, respectively, while the esti-mated total discounted QALYs per person were 12.28 and7.76, respectively (Table 2). The additional clinical ben-efits and expected lifetime cost saving of DFX was 4.52QALYs and $Int96,493.18 per patient. The average cost-effectiveness ratios of DFX and DFO were $Int3826.9 and$Int18,475.6. The ICER results showed that DFX is a domi-nant alternative and its estimated lifetime NMB was$Int273,528.
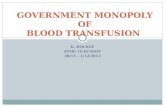
Sensitivity analysisOne-way sensitivity analysis results are shown in Fig. 2.The mean annual costs and utility of DFO and DFX were
TABLE 2. Results of base-case analysisOutcome measure DFX DFO Difference
Life-yearsNot discounted 19.2 19.15 0.05Discounted 14.46 14.43 0.03
QALYsNot discounted 16.29 10.26 6.03Discounted 12.28 7.76 4.52
Discounted costs ($Int)Total 47,029 143,522 96,493.18
ACER (Cost/QALY) ($Int) 3,826.9 18,475.6ICER DFX vs. DFO (DCost/DQALY) DominantNMB (DQALY ¥ Ceiling ratio - Dcost) ($Int) 273,528.1
ACER = average cost-effectiveness ratio.
COST UTILITY OF DEFERASIROX VS. DEFEROXAMINE
Volume 53, August 2013 TRANSFUSION 1725

changed in a sequence to the upper and lower limits at0.95% CI. Moreover, the discount rate of cost and effec-tiveness was changed from 0 to 6 and 10% change in thebaseline transition probabilities was tested, while theother variables were held constant. The results showedthat the NMB was relatively insensitive to changes in tran-sition probabilities in two strategies, annual cost andutility of each strategy with presence of cardiac complica-tion, although the NMB was sensitive to the chosen dis-count rate and utility of each strategy without cardiaccomplication.
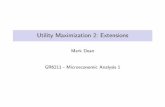
Figure 3 shows the results of probabilistic sensitivityanalysis. We simulated 10,000 sets of utility, transitionprobability, and cost estimates for each strategy by simul-taneously sampling from assigned probability distribu-tions of the variables. Expected lifetime costs and QALYsfor each strategy were calculated for each simulation andresult showed in 97% of iterations DFX was optimal strat-egy. In other words, DFX was estimated to have a lower
total lifetime cost and greater effectiveness than DFO;thus, DFX is a cost-saving alternative for DFO from Iran’ssociety perspective.
DISCUSSION
Due to limited resource in health systems worldwide,demand for economic evaluation of health care programs,especially pharmaceuticals, is steadily increasing.30 Iran’shealth care system is in charge of medical care financing formore than 25,000 Iranian b-thalassemia patients; hence,the necessity of efficient resource allocation is obvious. Thestudies that were conducted around the world with thepurpose of comparing the effectiveness of DFX with DFOshowed their similarity in decreasing the iron burden of thebody, declining the serum ferritin level in the blood, andaffecting the balance of the body iron. Furthermore, thestudies have validated the effectiveness, safety, and accept-ability of DFX as a new oral medicine.7,14,16,18
Fig. 2. Results of one-way sensitivity analysis (tornado diagram). ( ) Upper; ( ) lower.
KESHTKARAN ET AL.
1726 TRANSFUSION Volume 53, August 2013

The TTO exercise results revealed that the mean utili-ties of using DFX and DFO, when patients have not hadcardiac complications, were 0.82 and 0.56, respectively.Karnon and colleagues22 and Delea and colleagues31 alsoadopted the TTO method in their studies. The first studyestimated the utilities of using DFX and DFO to be 0.84and 0.66, and the second one, 0.85 and 0.57, respectively.
Further studies were also conducted to compareamount of patients’ satisfaction in both methods. Cappel-lini and coworkers32 conducted a study to evaluate thepatients’ satisfaction with two methods and concludedthat 92% of the patients treated with DFX and 50% of thosetreated with DFO were satisfied at the fourth week of thetreatment and 96.9% of those patients who have used DFOexpressed that they would prefer DFX.
We concluded that the annual cost of patients whoused DFO was higher than DFX. In accordance with thisstudy, in a study by Karnon and colleagues22 the annualcost of DFX (£12,787) was also lower than DFO (£14,356),where considered costs were drug and pump costs, cost ofthe injection equipment, and those costs related to the sideeffects of each medicine.
The findings of the economic evaluation resultingfrom the comparison between DFX and DFO revealed thatthe cost utility of DFX is higher than that of DFO. Indeed,DFX is the dominant choice compared to DFO with a
lower mean in the lifetime costs and a higher mean in theQALY gained. The calculated NMB showed that receivingDFX instead of DFO will save $Int273,528 for each patientin their lifetime for Iran’s society. Karnon and colleagues22
investigated cost utility of DFX compared to DFO from theUK National Health Services viewpoint. Their resultsrevealed that DFO was dominated by DFX, which is inagreement with our finding. They concluded that inpatients with a mean weight of 62 kg, the incremental costper QALY gained was €3775. Delea and colleagues31
carried out another study from the US Health Care Systemperspective. They used a Markov model with a 50-yeartime horizon and found that DFX caused an additional 4.5QALYs gained per patient at a cost of $US126,018; thus thecost of each additional QALY gained was $US28,255. In adetailed assessment, Kim and Kim10 investigated the timecost of DFX and DFO for patients with iron overload inSouth Korea. It was shown that the drug cost of DFX wasmore than that of DFO but the other costs related to DFOsuch as pump and injection materials were higher; hence,the DFX was dominant and resulted in a saving of$US3197 per 2.63 QALYs gained for each patient. Luan-gasanatip and coworkers20 conducted another study toevaluate the cost-effectiveness of DFO, deferiprone (DFP),and DFX from Thailand’s society perspective. In contrastwith our study, they found that using DFP is cost-saving
Fig. 3. Results of probabilistic sensitivity analysis (each point represents the difference in costs and QALYs for DFX vs. DFO in a
single simulation). WTP = willingness to pay.
COST UTILITY OF DEFERASIROX VS. DEFEROXAMINE
Volume 53, August 2013 TRANSFUSION 1727

compared to DFO, while using DFX is not cost-effectivewhen compared with either DFO or DFP.
Although using local cost and utility data in our analy-sis has made our results more applicable in local healthpolicy making, nonetheless there are several limitations ofour study that merit consideration in interpreting results.First, due to lack of local data, we obtained transitionprobabilities from the international literature. These vari-ables may therefore be different in Iranian patients.Second, only transfusion time cost was included in indi-rect cost, while other cost such as productivity lost due todisability in two groups may be different. Nevertheless,with regard to similarity of efficacy and safety of DFO andDFX it seems that this limitation is likely to be minor.Third, we did not consider the different compliance ratesbetween two methods. This may have led to an underes-timation of the benefits of an oral regimen compared withsubcutaneous infusion.20
In conclusion, DFX is a novel iron chelator that hasbeen shown to have similar efficacy and safety comparedwith DFO with a considerable improvement in the conve-nience and saving in injection time of patients withb-thalassemia. The results of the cost–utility analysis ofDFX versus DFO showed that DFX is a dominant therapyfor patients with iron overload from Iran’s societyperspective.
ACKNOWLEDGMENTS
The authors acknowledge the assistance of the whole centers and
people involved in the study.
CONFLICT OF INTEREST
The authors have declared that no competing interests exist.
REFERENCES
1. Fucharoen S, Winichagoon P. Haemoglobinopathies in
southeast Asia. Indian J Med Res 2011;134:498-506.
2. Weatherall DJ. The challenge of thalassemia for the devel-
oping countries. In: Vichinsky EP, editor. Cooley’s anemia
eighth symposium. Ann NY Acad Sci 2005;1054:11-7.
3. Weatherall D, Akinyanju O, Fucharoen S, Olivieri N, Mus-
grove P. Inherited disorders of hemoglobin. In: Jamison DT,
Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB,
Jha P, Mills A, Musgrove P, editors. Disease control priori-
ties in developing countries. New York: Oxford University
Press; 2006. p. 663-80.
4. Weatherall DJ. The challenge of haemoglobinopathies in
resource-poor countries. Br J Haematol 2011;154:736-44.
5. Abolghasemi H, Amid A, Zeinali S, Radfar MH, Eshghi P,
Rahiminejad MS, Ehsani MA, Najmabadi H, Akbari MT,
Afrasiabi A, Akhavan-Niaki H, Hoorfar H. Thalassemia in
Iran: epidemiology, prevention, and management. J Pediatr
Hematol Oncol 2007;29:233-8.
6. Rahimi Z, Muniz A, Akramipour R, Tofieghzadeh F, Moza-
fari H, Vaisi-Raygani A, Parsian A. Haplotype analysis of
beta thalassemia patients in Western Iran. Blood Cells Mol
Dis 2009;42:140-3.
7. Cappellini MD, Cohen A, Piga A, Bejaoui M, Perrotta S,
Agaoglu L, Aydinok Y, Kattamis A, Kilinc Y, Porter J, Capra
M, Galanello R, Fattoum S, Drelichman G, Magnano C, Ver-
issimo M, Athanassiou-Metaxa M, Giardina P, Kourakli-
Symeonidis A, Janka-Schaub G, Coates T, Vermylen C,
Olivieri N, Thuret I, Alberti D et al. A phase 3 study of
deferasirox (ICL670), a once-daily oral iron chelator, in
patients with beta-thalassemia. Blood 2006;107:3455-62.
8. Goldberg SL. Novel treatment options for transfusional iron
overload in patients with myelodysplastic syndromes. Leuk
Res 2007;31 Suppl 3:S16-22.
9. Borgna-Pignatti C, Cappellini MD, De Stefano P, Del
Vecchio GC, Forni GL, Gamberini MR, Ghilardi R, Origa R,
Piga A, Romeo MA, Zhao H, Cnaan A. Survival and compli-
cations in thalassemia. Ann N Y Acad Sci 2005;1054:40-7.
10. Kim J, Kim Y. A time-cost augmented economic evaluation
of oral deferasirox versus infusional dereroxmine for
patients with iron overload in South Korea. Value Health
2009;12 Suppl 3:S78-81.
11. Pathare A, Taher A, Daar S. Deferasirox (Exjade) signifi-
cantly improves cardiac T2* in heavily iron-overloaded
patients with beta-thalassemia major. Ann Hematol 2010;
89:405-9.
12. Miyazawa K, Ohyashiki K, Urabe A, Hata T, Nakao S, Ozawa
K, Ishikawa T, Kato J, Tatsumi Y, Mori H, Kondo M, Tanigu-
chi J, Tanii H, Rojkjaer L, Omine M. A safety, pharmacoki-
netic and pharmacodynamic investigation of deferasirox
(Exjade, ICL670) in patients with transfusion-dependent
anemias and iron-overload: a Phase I study in Japan. Int J
Hematol 2008;88:73-81.
13. Jabbour E, Garcia-Manero G, Taher A, Kantarjian HM. Man-
aging iron overload in patients with myelodysplastic syn-
dromes with oral deferasirox therapy. Oncologist 2009;14:
489-96.
14. Vichinsky E, Onyekwere O, Porter J, Swerdlow P, Eckman J,
Lane P, Files B, Hassell K, Kelly P, Wilson F, Bernaudin F,
Forni GL, Okpala I, Ressayre-Djaffer C, Alberti D, Holland J,
Marks P, Fung E, Fischer R, Mueller BU, Coates T; Defera-
sirox in Sickle Cell Investigators. A randomised comparison
of deferasirox versus deferoxamine for the treatment of
transfusional iron overload in sickle cell disease. Br J Hae-
matol 2007;136:501-8.
15. Metzgeroth G, Dinter D, Schultheis B, Dorn-Beineke A,
Lutz K, Leismann O, Hehlmann R, Hastka J. Deferasirox in
MDS patients with transfusion-caused iron overload—a
phase-II study. Ann Hematol 2009;88:301-10.
16. Taher A, Cappellini MD, Vichinsky E, Galanello R, Piga A,
Lawniczek T, Clark J, Habr D, Porter JB. Efficacy and safety
of deferasirox doses of >30 mg/kg per day in patients with
transfusion-dependent anaemia and iron overload. Br J
Haematol 2009;147:752-9.
KESHTKARAN ET AL.
1728 TRANSFUSION Volume 53, August 2013

17. Maggio A, Filosa A, Vitrano A, Aloj G, Kattamis A, Ceci A,
Fucharoen S, Cianciulli P, Grady RW, Prossomariti L, Porter
JB, Iacono A, Cappellini MD, Bonifazi F, Cassarà F,
Harmatz P, Wood J, Gluud C. Iron chelation therapy in
thalassemia major: a systematic review with meta-analyses
of 1520 patients included on randomized clinical trials.
Blood Cells Mol Dis 2011;47:166-75.
18. Piga A, Galanello R, Forni GL, Cappellini MD, Origa R,
Zappu A, Donato G, Bordone E, Lavagetto A, Zanaboni L,
Sechaud R, Hewson N, Ford JM, Opitz H, Alberti D. Ran-
domized phase II trial of deferasirox (Exjade, ICL670), a
once-daily, orally-administered iron chelator, in compari-
son to deferoxamine in thalassemia patients with transfu-
sional iron overload. Haematologica 2006;91:873-80.
19. Borgna-Pignatti C, Rugolotto S, De Stefano P, Zhao H, Cap-
pellini MD, Del Vecchio GC, Romeo MA, Forni GL, Gam-
berini MR, Ghilardi R, Piga A, Cnaan A. Survival and
complications in patients with thalassemia major treated
with transfusion and deferoxamine. Haematologica 2004;
89:1187-93.
20. Luangasanatip N, Chaiyakunapruk N, Upakdee N, Wong P.
Iron-chelating therapies in a transfusion-dependent thalas-
saemia population in Thailand: a cost-effectiveness study.
Clin Drug Investig 2011;31:493-505.
21. Delea T, Sofrygin O, Thomas S, Baladi JF, Phatak P, Coates
TD. PHM1 cost-effectiveness of once-daily oral chelation
therapy with deferasirox versus infusional deferoxamine in
transfusion-dependent thalassemia patients. Value Health
2006;9:A143.
22. Karnon J, Tolley K, Oyee J, Jewitt K, Ossa D, Akehurst R.
Cost-utility analysis of deferasirox compared to standard
therapy with desferrioxamine for patients requiring iron
chelation therapy in the United Kingdom. Curr Med Res
Opin 2008;24:1609-21.
23. Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB.
Recommendations of the panel on cost-effectiveness in
health and medicine. JAMA 1996;276:1253-8.
24. Borgna-Pignatti C, Cappellini MD, De Stefano P, Del
Vecchio GC, Forni GL, Gamberini MR, Ghilardi R, Piga A,
Romeo MA, Zhao H, Cnaan A. Cardiac morbidity and mor-
tality in deferoxamine- or deferiprone-treated patients with
thalassemia major. Blood 2006;107:3733-7.
25. Ladis V, Chouliaras G, Berdoukas V, Moraitis P, Zannikos K,
Berdoussi E, Kattamis C. Relation of chelation regimes to
cardiac mortality and morbidity in patients with thalas-
saemia major: an observational study from a large Greek
Unit. Eur J Haematol 2010;85:335-44.
26. Pourmalek F, Abolhassani F, Naghavi M, Mohammad K,
Majdzadeh R, Holakouie Naeini K, Fotouhi A. Direct esti-
mation of life expectancy in the Islamic Republic of Iran in
2003. East Mediterr Health J 2009;15:76-84.
27. Chouliaras G, Yiannoutsos CT, Berdoukas V, Ladis V.
Cardiac related death in thalassaemia major: time trend
and risk factors in a large Greek unit. Eur J Haematol 2009;
82:381-7.
28. Tan-Torres Edejer T, Baltussen R, Adam T, Hutubessy R,
Acharya A, Evans DB, Murray CJ, editors. Making choices in
health: WHO guide to cost-effectiveness analysis. Geneva:
World Health Organization; 2003. p. 329.
29. Stinnett AA, Mullahy J. Net health benefits: a new
framework for the analysis of uncertainty in cost-
effectiveness analysis. Med Decis Making 1998;18(2 Suppl):
S68-80.
30. Blumenschein K, Johannesson M. Incorporating quality of
life changes into economic evaluations of health care: an
overview. Health Policy 1996;36:155-66.
31. Delea TE, Sofrygin O, Thomas SK, Baladi JF, Phatak PD,
Coates TD. Cost effectiveness of once-daily oral chelation
therapy with deferasirox versus infusional deferoxamine in
transfusion-dependent thalassaemia patients—US health-
care system perspective. Pharmacoeconomics 2007;25:329-
42.
32. Cappellini MD, Bejaoui M, Agaoglu L, Porter J, Coates T,
Jeng M, Lai ME, Mangiagli A, Strauss G, Girot R, Watman N,
Ferster A, Loggetto S, Abish S, Cario H, Zoumbos N, Vichin-
sky E, Opitz H, Ressayre-Djaffer C, Abetz L, Rofail D, Baladi
JF. Prospective evaluation of patient-reported outcomes
during treatment with deferasirox or deferoxamine for iron
overload in patients with b-thalassemia. Clin Ther 2007;29:
909-17.
33. Javanbakht M, Baradaran HR, Mashayekhi A, Haghdoost
AA, Khamseh ME, Kharazmi E, Sadeghi A. Cost-of-illness
analysis of type 2 diabetes mellitus in Iran. Plos ONE 2011;
6:e26864.
34. Pennell DJ, Porter JB, Cappellini MD, El-Beshlawy A, Chan
LL, Aydinok Y, Elalfy MS, Sutcharitchan P, Li CK, Ibrahim
H, Viprakasit V, Kattamis A, Smith G, Habr D, Domokos G,
Roubert B, Taher A. Efficacy of deferasirox in reducing and
preventing cardiac iron overload in beta-thalassemia.
Blood 2010;115:2364-71.
COST UTILITY OF DEFERASIROX VS. DEFEROXAMINE
Volume 53, August 2013 TRANSFUSION 1729