Corticosteroid resistance in sepsis is influenced by microRNA-124–induced downregulation of...
8
Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Crit Care Med 2012 Vol. 40, No. 12 1 I nitiatives to improve care for venti- lated patients have been constrained by limitations of the ventilator- associated pneumonia (VAP) surveillance definition. The National Healthcare Safety Network definitions of Centers for Disease Control and Prevention (CDC) include clinically nuanced, subjective criteria such as “worsening gas exchange,” “change in the character of sputum,” and “new or progressive and persistent infiltrates” (Table 1)(1). Growing pressures to publicly report VAP rates have exposed three major shortcomings to these definitions: they correlate poorly with histology, they are highly subjective, and they are time- consuming and complicated to implement (2, 3). These limitations preclude meaningful benchmarking between institutions, complicate the evaluation of prevention initiatives, hamper the construction of an ideal prevention bundle, and raise questions about the authenticity of zero VAP rates (4–6). These shortcomings reflect the clini- cal challenge diagnosing VAP. A plethora of studies have documented poor correla- tion among clinical signs, microbiologi- cal cultures, radiographs, biochemical markers, and histological VAP (2, 7–15). From the Department of Population Medicine (MK, KK, RP), Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, MA; Department of Medicine (MK, DSY, RP), Brigham and Women’s Hospital, Boston, MA; Division of Healthcare Quality Promotion (SM), Centers for Disease Control and Prevention, Atlanta, GA; Department of Medicine and Department of Quality (AR), Northshore University Health System, Evanston, IL; Veterans Affairs Boston Healthcare System (JMS), Boston, MA; Department of Biomedical Informatics (RSE), University of Utah School of Medicine, Salt Lake City, UT; Department of Medical Informatics (RSE, JFL), Intermountain Healthcare, Salt Lake City, UT; Department of Medicine (YK, KS), The Ohio State University Medical Center, Columbus, OH. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (http://journals.lww. com/ccmjournal). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Supported by Prevention Epicenters Program of the Centers for Disease Control and Prevention. The authors have not disclosed any potential conflicts of interest. For information regarding this article, E-mail: [email protected] Copyright © 2012 by the Society of Critical Care Medicine and Lippincott Williams and Wilkins DOI: 10.1097/CCM.0b013e318260c6d9 Objectives: The subjectivity and complexity of surveillance defi- nitions for ventilator-associated pneumonia preclude meaningful internal or external benchmarking and therefore hamper quality improvement initiatives for ventilated patients. We explored the feasibility of creating objective surveillance definitions for venti- lator-associated pneumonia. Design: We identified clinical signs suitable for inclusion in objective definitions, proposed candidate definitions incorporating these objective signs, and then applied these definitions to retro- spective clinical data to measure their frequencies and associa- tions with adverse outcomes using multivariate regression models for cases and matched controls. Setting: Medical and surgical intensive care units in eight U.S. hospitals (four tertiary centers, three community hospitals, and one Veterans Affairs institution). Patients: Eight thousand seven hundred thirty-five consecutive episodes of mechanical ventilation for adult patients. Interventions: We evaluated 32 different candidate defini- tions composed of different combinations of the following signs: three thresholds for respiratory deterioration defined by sustained increases in daily minimum positive end-expiratory pressure or FIO 2 after either 2 or 3 days of stable or decreasing ventilator settings, abnormal temperature, abnormal white blood cell count, purulent pulmonary secretions defined by neutrophils on Gram stain, and positive cultures for pathogenic organisms. Measurements and Main Results: Ventilator-associated pneumonia incidence, attributable ventilator days, hospital days, and hospital mortality. All candidate definitions were significantly associated with increased ventilator days and hospital days, but only definitions requiring objective evidence of respiratory deterioration were significantly associated with increased hospital mortality. Significant odds ratios for hospi- tal mortality ranged from 1.9 (95% confidence interval 1.2–2.9) to 6.1 (95% confidence interval 2.2–17). Requiring additional clinical signs beyond respiratory deterioration alone decreased event rates, had little impact on attributable lengths of stay, and diminished sensitivity and positive predictive values for hospi- tal mortality. Conclusions: Objective surveillance definitions that include quantitative evidence of respiratory deterioration after a period of stability strongly predict increased length of stay and hospital mortality. These definitions merit further evaluation of their utility for hospital quality and safety improvement programs. (Crit Care Med 2012; 40:0–0) Objective surveillance definitions for ventilator-associated pneumonia Michael Klompas, MD, MPH; Shelley Magill, MD, PhD; Ari Robicsek, MD; Judith M. Strymish, MD; Ken Kleinman, ScD; R. Scott Evans, MS, PhD; James F. Lloyd, BS; Yosef Khan, MD, MPH; Deborah S. Yokoe, MD, MPH; Kurt Stevenson, MD, MPH; Matthew Samore, MD; Richard Platt, MD; for the CDC Prevention Epicenters Program
Transcript of Corticosteroid resistance in sepsis is influenced by microRNA-124–induced downregulation of...

Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Crit Care Med 2012 Vol. 40, No. 12 1
Initiatives to improve care for ventilated patients have been constrained by limitations of the ventilatorassociated pneumonia (VAP)
sur veillance definition. The National
Healthcare Safety Network definitions of Centers for Disease Control and Prevention (CDC) include clinically nuanced, subjective criteria such as “worsening gas exchange,” “change in
the character of sputum,” and “new or progressive and persistent infiltrates” (Table 1)(1). Growing pressures to publicly report VAP rates have exposed three major shortcomings to these definitions: they correlate poorly with histology, they are highly subjective, and they are timeconsuming and complicated to implement (2, 3). These limitations preclude meaningful benchmarking between institutions, complicate the evaluation of prevention initiatives, hamper the construction of an ideal prevention bundle, and raise questions about the authenticity of zero VAP rates (4–6).
These shortcomings reflect the clinical challenge diagnosing VAP. A plethora of studies have documented poor correlation among clinical signs, microbiological cultures, radiographs, biochemical markers, and histological VAP (2, 7–15).
From the Department of Population Medicine (MK, KK, RP), Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, MA; Department of Medicine (MK, DSY, RP), Brigham and Women’s Hospital, Boston, MA; Division of Healthcare Quality Promotion (SM), Centers for Disease Control and Prevention, Atlanta, GA; Department of Medicine and Department of Quality (AR), Northshore University Health System, Evanston, IL; Veterans Affairs Boston Healthcare System (JMS), Boston, MA; Department of Biomedical Informatics (RSE), University of Utah School of Medicine, Salt Lake City, UT; Department of Medical Informatics (RSE, JFL), Intermountain Healthcare, Salt Lake City, UT; Department of Medicine (YK, KS), The Ohio State University Medical Center, Columbus, OH.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text
and are provided in the HTML and PDF versions of this article on the journal’s Web site (http://journals.lww.com/ccmjournal).
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Supported by Prevention Epicenters Program of the Centers for Disease Control and Prevention.
The authors have not disclosed any potential conflicts of interest.
For information regarding this article, E-mail: [email protected]
Copyright © 2012 by the Society of Critical Care Medicine and Lippincott Williams and Wilkins
DOI: 10.1097/CCM.0b013e318260c6d9
Objectives: The subjectivity and complexity of surveillance defi-nitions for ventilator-associated pneumonia preclude meaningful internal or external benchmarking and therefore hamper quality improvement initiatives for ventilated patients. We explored the feasibility of creating objective surveillance definitions for venti-lator-associated pneumonia.
Design: We identified clinical signs suitable for inclusion in objective definitions, proposed candidate definitions incorporating these objective signs, and then applied these definitions to retro-spective clinical data to measure their frequencies and associa-tions with adverse outcomes using multivariate regression models for cases and matched controls.
Setting: Medical and surgical intensive care units in eight U.S. hospitals (four tertiary centers, three community hospitals, and one Veterans Affairs institution).
Patients: Eight thousand seven hundred thirty-five consecutive episodes of mechanical ventilation for adult patients.
Interventions: We evaluated 32 different candidate defini-tions composed of different combinations of the following signs: three thresholds for respiratory deterioration defined by sustained increases in daily minimum positive end-expiratory pressure or Fio2 after either 2 or 3 days of stable or decreasing ventilator settings,
abnormal temperature, abnormal white blood cell count, purulent pulmonary secretions defined by neutrophils on Gram stain, and positive cultures for pathogenic organisms.
Measurements and Main Results: Ventilator-associated pneumonia incidence, attributable ventilator days, hospital days, and hospital mortality. All candidate definitions were significantly associated with increased ventilator days and hospital days, but only definitions requiring objective evidence of respiratory deterioration were significantly associated with increased hospital mortality. Significant odds ratios for hospi-tal mortality ranged from 1.9 (95% confidence interval 1.2–2.9) to 6.1 (95% confidence interval 2.2–17). Requiring additional clinical signs beyond respiratory deterioration alone decreased event rates, had little impact on attributable lengths of stay, and diminished sensitivity and positive predictive values for hospi-tal mortality.
Conclusions: Objective surveillance definitions that include quantitative evidence of respiratory deterioration after a period of stability strongly predict increased length of stay and hospital mortality. These definitions merit further evaluation of their utility for hospital quality and safety improvement programs. (Crit Care Med 2012; 40:0–0)
Objective surveillance definitions for ventilator-associated pneumonia
Michael Klompas, MD, MPH; Shelley Magill, MD, PhD; Ari Robicsek, MD; Judith M. Strymish, MD; Ken Kleinman, ScD; R. Scott Evans, MS, PhD; James F. Lloyd, BS; Yosef Khan, MD, MPH; Deborah S. Yokoe, MD, MPH; Kurt Stevenson, MD, MPH; Matthew Samore, MD; Richard Platt, MD; for the CDC Prevention Epicenters Program

Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
2 Crit Care Med 2012 Vol. 40, No. 12
In the absence of accurate signs or tests, we are unlikely to be able to improve the accuracy of the surveillance definition. There is a significant potential, however, to improve the objectivity and efficiency of surveillance by shifting to a definition that can be defined quantitatively and electronically. Preliminary work in this direction suggests that objective definitions are feasible and can capture similar patients to those identified by traditional VAP surveillance (16–18).
Shifting to an objective electronic definition promises important benefits. An objective definition will make it possible to rigorously assess quality improvement initiatives without fear that apparent gains are due to observer bias rather than true advances in care. Objective definitions will also permit more meaningful comparisons between institutions if coupled with adequate casemix adjustments. Objectively determined differences in event rates between comparable institutions are more likely to help identify best practices and drive further improvements in care compared to subjective alternatives.
Given these pressing needs, we undertook an exploratory analysis of possible objective definitions for VAP. We hypothesized that clinically significant, objective surveillance definitions can be created, defining “clinically significant” as a complication statistically associated with increased length of stay and hospital mortality. We recognized from the outset that creating an objective definition is constrained by the absence of pathognomonic signs or tests for VAP. In the absence of criteria that can assure diagnostic accuracy, we chose to focus definition development instead on objectivity, practicality, efficiency, and most importantly, correlation with adverse outcomes. We reasoned that an objective and efficient surveillance definition closely linked to adverse outcomes will still be a substantial step forward even if it does not correlate perfectly with histological pneumonia. For the same reason, we intentionally focused on potential definitions amenable to electronic analysis to simplify data collection, increase consistency between observers and institutions, and facilitate the creation of automated surveillance systems. We did not attempt to develop new definitions for clinical care because the onus in clinical care is on sensitivity when diagnosing patients and specificity when managing patients whereas the onus in surveillance is on objectivity to facilitate reproducibility and comparisons over time and between institutions.
The candidate definitions explored in this article build upon prior work by the CDC Prevention Epicenters (16–18). The Epicenters demonstrated that establishing quantitative criteria for worsening oxygenation, purulent sputum, fever, and abnormal white blood cell counts makes surveillance faster, improves interobserver agreement, and predicts outcomes as well as conventional surveillance (17). The Epicenters’ definition, however, continued to require radiographic evidence of VAP and closely mirrored the structure and content of the current NHSN definitions of VAP. Retention of chest radiographs is problematic because they are subjective, nonspecific, and cannot be analyzed electronically (9, 19–22). We sought to extend the Epicenters’ work by evaluating alternative combinations of clinical signs and specifically excluding chest radiographs to render entirely objective definitions. We assessed clinical significance by calculating event rates and attributable ventilator length of stay, hospital length of stay, and hospital mortality for each candidate definition.
METHODS
We analyzed the classical clinical signs of VAP for their suitability for objective surveillance definitions (Table 2). We sought signs and investigations that are 1) routinely assessed on most patients on most days, 2) objective (quantitative rather than qualitative), and 3) electronically collectable (routinely recorded as structured data in electronic systems in hospitals with comprehensive electronic health record systems). An analysis of common clinical signs using these three criteria is presented in Table 2. The following signs met all three criteria: worsening oxygenation defined as a sustained increase in the daily minimum Fio2 after 2 or more days of stable or decreasing
daily minimum Fio2 or a sustained increase in the daily minimum positive endexpiratory pressure (PEEP) after 2 or more days of stable or decreasing daily minimum PEEP, fever, hypothermia, leukocytosis, leukopenia, purulent pulmonary secretions, and pathogenic cultures from pulmonary specimens.
We considered three different thresholds for respiratory deterioration: 1) rise in the daily minimum PEEP of ≥2 cm H2O or rise in the daily minimum Fio2 of ≥15 points sustained for at least 2 calendar days, 2) rise in the daily minimum PEEP of ≥3cm H2O or rise in the daily minimum Fio2 of ≥20 points sustained for at least 2 calendar days, and 3) rise in the daily minimum PEEP of ≥5 cm H2O or rise in the daily minimum Fio2 of ≥20 points sustained for at least 2 calendar days. All definitions of respiratory deterioration required evidence of stability prior to deterioration to identify trajectory changes in respiratory support rather than the continued evolution of preexisting respiratory disease. We evaluated two different thresholds for stability prior to respiratory deterioration: ≥2 days or ≥3 days of stable or decreasing daily minimum PEEP or daily minimum Fio2. We defined fever as temperature >38°C, hypothermia as temperature <36°C, leukocytosis as white blood cell count ≥12,000 cells/mm3, leucopenia as <4,000 cells/mm3, purulent pulmonary secretions as ≥25 neutrophils and ≤10 epithelial cells per low power field on Gram stain of endotracheal aspirate or bronchoalveolar lavage specimen, and pathogenic pulmonary specimen culture as recovery of any organism other than oral flora, Enterococcus species, coagulasenegative Staphylococcus species, or Candida species from endotracheal aspirate or bronchoalveolar lavage. We did not specify quantitative growth thresholds for cultures because these are not routinely calculated by many hospital laboratories and therefore of limited suitability for a generalizable surveillance definition.
We combined these signs to create candidate objective definitions for VAP (Table 3 and eTable I; see Supplemental Digital Content 1,
Table 1. Centers for Disease Control and Prevention’s clinical surveillance definition for ventilatorassociated pneumonia (PNU1)
Radiologic criteria (two or more serial radiographs with at least one of the following)
1. New or progressive and persistent infiltrate2. Consolidation3. Cavitation
Systemic criteria (at least one) 1. Fever (>38°C or >100.4°F)2. Leukopenia (<4,000 WBC/mm3) or leukocytosis (≥12,000 WBC/mm3)3. For adults ≥70 yrs old, altered mental status with no other
recognized cause
Pulmonary criteria (at least two) 1. New onset of purulent sputum, or change in character of sputum, or increased respiratory secretions, or increased suctioning requirements
2. Worsening gas exchange (e.g., desaturations, increased oxygen requirements, or increased ventilator demand)
3. New onset or worsening cough, or dyspnea, or tachypnea4. Rales or bronchial breath sounds
Patients must fulfill radiologic, systemic, and pulmonary criteria.

Jdivya 09/14/12 4 color fig(s); F# 08:16 Art: CCM203921
Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Crit Care Med 2012 Vol. 40, No. 12 3
http://links.lww.com/CCM/A489). We selected combinations that mirror classic clinical definitions for VAP such as purulent pulmonary secretions with or without a pathogenic culture, worsening oxygenation with purulent secretions, worsening oxygenation with systemic signs and purulent secretions, or worsening oxygenation with systemic signs and purulent secretions and pathogenic cultures.
Each candidate definition was evaluated for clinical significance using retrospective clinical data from eight hospitals (four academic hospitals, three community hospitals, and one Veterans Affairs tertiary hospital). Each participating hospital provided a minimum of 6 months of daily clinical data for every adult patient on mechanical ventilation during the study period. Clinical data included daily minimum PEEPs and Fio2s, minimum and maximum temperatures, minimum and maximum white blood cell counts, and endotracheal aspirate and bronchoalveolar lavage Gram stain and culture results. Patients’ comorbidities were derived from diagnosis and claims codes using the methods of Charlson et al (23) and Elixhauser et al (24). Six of the eight hospitals also provided Acute Physiology and Chronic Health Evaluation II scores from the day of intubation (or hospital admission day if intubated prior to arrival) when available.
We calculated incidence density, attributable ventilator days, attributable hospital length of stay, and attributable mortality for each candidate definition. The incidence density was defined as the event rate per 1,000 ventilator days. We designed this study using
standard surveillance principals which include all patients on mechanical ventilation regardless of the duration of ventilation, mode of ventilation, underlying conditions, or “do not resuscitate” status. We therefore included all such patients when calculating the size of the study population, the number of episodes of mechanical ventilation, and the total number of ventilator days. All candidate definitions, however, did require patients to be on the ventilator for at least 2 days. Patients were eligible for more than one VAP event per definition so long as the events were >10 days apart.
Attributable ventilator days, attributable hospital days, and attributable mortality were calculated by first matching each case patient to between one and five control patients. Patients were matched by hospital, unit type, Charlson score (<3 vs. ≥3), and duration of mechanical ventilation prior to VAP onset. We defined the date of VAP onset as the date of increased ventilator settings, but we matched control patients’ minimum duration of mechanical ventilation to cases’ second day of increased ventilator support because all candidate definitions of respiratory deterioration required at least 2 days of increased ventilator settings. We then applied negative binomial regression models to determine the ratio of ventilator days and hospital days postevent and logistic regression models to estimate the relative odds of hospital mortality in cases compared to controls. We used mixed effects models to account for matching. We assessed ventilator days from event date to extubation date and hospital days from event date to discharge date to focus on days potentially
attributable to VAP. Models were adjusted for hospital, unit type, age, sex, and Charlson score. Separate models were fitted for each potential definition (hence the same patient could serve as a case for some analyses and as a control in other analyses). We repeated all analyses among the subset of patients with Acute Physiology and Chronic Health Evaluation II scores wherein the Acute Physiology and Chronic Health Evaluation II score was added as a covariate to the regression models. If patients had more than one VAP event, all events >10 days apart were included in incidencedensity calculations but only the first event was included in the attributable length of stay and hospital mortality analyses. We conducted sensitivity analyses to assess whether the attributable mortality of selected definitions differed for surgical vs. medical patients. We also plotted the sensitivity and positive predictive values of selected definitions for hospital death to facilitate comparisons between the definitions.
We used SAS version 9.3 (SAS Institute, Cary, NC) for all analyses, including the application of candidate definitions. The study was reviewed and approved by the Institutional Review Board of each participating institution.
RESULTS
The eight study hospitals contributed data from 8,123 patients with 8,735 episodes of ventilation spanning a combined total of 50,324 ventilator days. Clinical characteristics of the population are presented in Table 4. Potential objective definitions of VAP, their event rates, and attributable ventilator days, hospital days, and hospital mortality are presented in Table 3 and eTable 1 (see Supplemental Digital Content 1, http://links.lww.com/CCM/A489). The definitions for respiratory deterioration in Table 3 are based on ≥2 days of stable respiratory status prior to deterioration, whereas those in eTable 1 (see Supplemental Digital Content 1, http://links.lww.com/CCM/A489) presume ≥3 days of stability prior to deterioration.
The incidence of VAP ranged from 26.3 events per 1,000 ventilator days with the least restrictive definition (purulent pulmonary secretions alone) to 0.2 events per 1,000 ventilator days with the most restrictive definition (highest threshold increase in ventilator settings after ≥3 days of stable settings + abnormal temperature or white blood cell count + purulent pulmonary secretions + positive pulmonary culture for pathogenic organism). All candidate definitions were significantly associated with increased ventilator days and hospital days compared to matched controls but only definitions requiring sustained evidence of respiratory
Table 2. Suitability of selected clinical signs of ventilatorassociated pneumonia for inclusion in an objective surveillance definition
Routine Objective Electronic
Radiographic infiltrates ✓Temperature ✓ ✓ ✓White blood cell count ✓ ✓ ✓Sputum quantity ✓Sputum quality ✓Sputum gram stain neutrophils ✓ ✓ ✓Cough ✓Dsypnea ✓Breath sounds ✓Mental status changes ✓Worsening oxygenation (rising Fio2) ✓ ✓ ✓Increasing ventilator support (rising positive endexpiratory pressure) ✓ ✓ ✓Pathogenic organisms from pulmonary secretions ✓ ✓ ✓Pao2/Fio2 ratioa +/− ✓ +/−Procalcitonin ✓ ✓
Definitions: 1) “Routine” defined as clinical signs or studies measured or ordered for most patients on most days. 2) “Objective” defined as data routinely measured using a quantitative or dichotomous scale. 3) “Electronic” defined as structured data elements routinely present in electronic form in hospitals with fullfeatured electronic medical record systems and amenable to electronic analysis with widely available software packages such as Excel, Access, and SAS without need for special analytic technologies such as natural language processing.
aPao2/Fio2 ratios were deemed not to meet “routine” and “electronic” criteria because some clinicians favor venous blood gases for some patients, and the Fio2 at the time Pao2 is measured is inconsistently recorded in electronic systems at present (not entered at all or entered as free text rather than as structured data easily amenable to electronic analysis).

Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
4 Crit Care Med 2012 Vol. 40, No. 12
deterioration were significantly associated with increased risk of hospital mortality. The only exceptions to this pattern were the most restrictive definitions, requiring all of sustained respiratory deterioration + abnormal temperature or white blood cell count + purulent pulmonary secretions + positive culture for a pathogenic organism. Hospital mortality odds ratios for these definitions were not significant. In general, requiring additional clinical signs beyond sustained respiratory
deterioration lowered event rates but did not meaningfully strengthen associations with adverse outcomes. Likewise, applying stricter thresholds for respiratory deterioration or requiring a baseline of ≥3 days of stable ventilator settings rather than ≥2 days lowered event rates but did not significantly magnify or diminish associations with length of stay and mortality. Covariates for the intermediate respiratory deterioration threshold definition are presented in eTable 2 (see Supplemental
Digital Content 1, http://links.lww.com/CCM/A489).
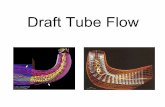
Sensitivities and positive predictive values for hospital death for selected definitions are displayed in Figure 1. Definitions requiring changes in ventilator settings alone or ventilator changes with an abnormal temperature or white blood cell count had the best combinations of sensitivity and positive predictive values. Requiring purulent sputum with or without positive cultures substantially
Table 3. Incidence densities and attributable outcomes for potential objective definitions for ventilatorassociated pneumonia
Models Without APACHE II Scores Models With APACHE II Scores
Ventilator Associated
Pneumonias per 1,000 Ventilator
Days
Excess Ventilator Day
Ratioa
Excess Hospital Day
Ratiob
Mortality Odds Ratio
Excess Ventilator Day
Ratioa
Excess Hospital
Day Ratiob
Mortality Odds Ratio
Purulent pulmonary secretions 26.3 1.7 (1.6–1.8) 1.2 (1.1–1.3) 1.0 (0.8–1.3) 1.6 (1.4–1.8) 1.3 (1.2–1.4) 1.1 (0.8–1.5) + Positive culture for pathogen 11.3 1.9 (1.7–2.1) 1.3 (1.2–1.4) 1.0 (0.8–1.2) 1.7 (1.4–1.9) 1.3 (1.1–1.4) 1.0 (0.7–1.4)
Rise in daily minimum PEEP of ≥2 cm H2O or Fio2 of ≥15 points sustained for ≥2 days after ≥2 days stable or decreasing values
15.6 2.1 (1.9–2.2) 1.3 (1.2–1.4) 1.8 (1.4–2.2) 1.8 (1.6–2.0) 1.3 (1.2–1.5) 2.9 (2.0–4.2)
+ Abnormal temperature or WBC count 14.7 2.0 (1.9–2.2) 1.3 (1.2–1.4) 1.9 (1.5–2.3) 1.7 (1.5–1.9) 1.3 (1.2–1.5) 2.7 (1.8–4.0) + Purulent secretions 5.4 1.7 (1.5–1.9) 1.3 (1.2–1.4) 1.6 (1.2–2.3) 1.5 (1.3–1.8) 1.3 (1.2–1.5) 1.9 (1.2–2.9) + (abnormal temperature or WBC count)
AND purulent secretions5.2 1.6 (1.4–1.8) 1.2 (1.1–1.4) 1.8 (1.3–2.5) 1.6 (1.3–1.8) 1.3 (1.1–1.5) 2.1 (1.3–3.3)
+ (abnormal temperature or WBC count) AND purulent secretions AND pathogenic culture
1.7 1.5 (1.2–1.8) 1.3 (1.1–1.6) 0.8 (0.5–1.5) 1.5 (1.2–1.9) 1.4 (1.1–1.7) 0.9 (0.4–2.0)
Rise in daily minimum PEEP of ≥3 cm H2O or Fio2 of ≥20 points sustained for ≥2 days after ≥2 days stable or decreasing values
12.0 2.0 (1.8–2.1) 1.2 (1.1–1.3) 1.9 (1.5–2.3) 1.9 (1.7–2.1) 1.4 (1.2–1.5) 2.4 (1.6–3.6)
+ Abnormal temperature or WBC count 11.4 2.0 (1.8–2.1) 1.4 (1.3–1.6) 1.7 (1.4–2.2) 1.9 (1.6–2.1) 1.4 (1.2–1.5) 2.1 (1.4–3.3) + Purulent secretions 3.9 1.6 (1.4–1.9) 1.2 (1.1–1.4) 1.4 (1.0–2.2) 1.7 (1.4–2.0) 1.3 (1.1–1.5) 1.6 (1.0–2.7) + (abnormal temperature or WBC count)
AND purulent secretions3.7 1.7 (1.5–1.9) 1.3 (1.1–1.4) 1.5 (1.0–2.2) 1.6 (1.3–1.9) 1.3 (1.1–1.5) 2.2 (1.3–3.7)
+ (abnormal temperature or WBC count) AND purulent secretions AND pathogenic culture
0.6 1.7 (1.2–2.4) 1.6 (1.2–2.2) 0.7 (0.2–2.0) 1.9 (0.9–3.8) 2.4 (0.8–7.1) 0.1 (0.0–2.3)
Rise in daily minimum PEEP of ≥5 cm H2O or Fio2 of ≥20 points sustained for ≥2 days after ≥2 days stable or decreasing values
8.4 1.8 (1.7–2.0) 1.2 (1.1–1.3) 1.8 (1.4–2.4) 1.7 (1.5–2.0) 1.3 (1.1–1.5) 3.1 (1.9–5.1)
+ Abnormal temperature or WBC count 7.9 1.9 (1.7–2.1) 1.2 (1.1–1.3) 2.0 (1.5–2.6) 1.7 (1.5–2.0) 1.3 (1.1–1.5) 3.2 (1.9–5.3) + Purulent secretions 2.4 1.5 (1.3–1.8) 1.2 (1.1–1.4) 2.0 (1.3–3.3) 1.6 (1.2–1.9) 1.3 (1.0–1.5) 3.1 (1.6–6.0) + (abnormal temperature or WBC count)
AND purulent secretions2.3 1.7 (1.4–1.9) 1.3 (1.1–1.4) 2.0 (1.3–3.3) 1.5 (1.2–1.9) 1.7 (1.4–2.1) 2.5 (1.3–4.9)
+ (abnormal temperature or WBC count) AND purulent secretions AND pathogenic culture
0.5 1.9 (1.3–2.8) 1.9 (1.4–2.6) 0.5 (0.1–1.6) 2.3 (1.1–4.9) 2.5 (1.3–4.9) 0.1 (0.0–4.1)
APACHE, Acute Physiology and Chronic Health Evaluation; PEEP, positive endexpiratory pressure; WBC, white blood cell.Cases matched to controls on the basis of hospital, unit type, Charlson score, and duration of mechanical ventilation prior to ventilatorassociated
pneumonia (VAP) onset. Outcomes models adjusted for hospital, unit, age, sex, Charlson score, duration of mechanical ventilation prior to VAP onset, and APACHE II score when available (only six of the eight participating hospitals were able to provide APACHE II scores). Numbers in parentheses are 95% confidence intervals. eTable 1 (see Supplemental Digital Content 1, http://links.lww.com/CCM/A489) presents event rates and attributable outcomes for the same definitions but presumes ≥3 days of stable or improving ventilator settings prior to respiratory deterioration.
aRatio of ventilator days from VAP to extubation in cases vs. matched controls; bratio of hospital days from VAP to hospital discharge in cases vs. matched controls.

Jdivya 09/14/12 4 color fig(s); F# 08:16 Art: CCM203921
Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Crit Care Med 2012 Vol. 40, No. 12 5
decreased both sensitivity and positive predictive values for hospital death.
DISCUSSION
Meaningful surveillance is indispensible for rigorous quality improvement programs. Surveillance helps define the extent of the problem, gauges the effectiveness of current improvement efforts, and informs the need to introduce or modify prevention efforts. The subjectivity of current VAP surveillance definitions has limited their utility to monitor and improve quality. In this article, we demonstrate the feasibility of creating objective VAP definitions that can be electronically applied to routine clinical data. The capacity to electronically apply these definitions is proof of their objectivity and reproducibility. Just as importantly, selected objective definitions are significantly associated with increased
ventilator days, hospital days, and hospital mortality. These features make them promising tools for quality improvement programs.
Definitions with criteria for respiratory deterioration were most strongly associated with adverse outcomes, particularly mortality. Purulent pulmonary secretions alone, with or without a pathogenic culture, were associated with increased ventilator days and hospital days but not increased mortality. By contrast, respiratory decompensation defined by an increase in the daily minimum PEEP or Fio2 after a period of stable or decreasing daily minimum PEEP or Fio2 strongly predicted increased ventilator days, hospital days, and hospital mortality. These changes are likely more than simply markers of severity of illness because by definition they are only flagged by a change in respiratory trajectory from stability or improvement to sustained deterioration.
Strikingly, selecting stricter thresholds for respiratory deterioration or adding systemic signs (abnormal temperature or white blood cell count), purulent secretions, and/or pathogenic cultures to worsening oxygenation diminished apparent VAP rates but had little impact on attributable outcomes. Indeed, requiring positive cultures for pathogenic organisms weakened the association between respiratory deterioration and mortality to the point that it was no longer statistically significant. These findings are consistent with previous studies demonstrating that most clinical signs do little to improve clinical certainty about the presence or absence of VAP (25).
The paradoxical weakening of the association between respiratory deterioration and mortality in definitions requiring pathogenic cultures may have been due to their low frequencies and consequent loss of power, but this finding does mirror previous work noting poorer outcomes among culturenegative VAP patients compared to culturepositive patients (26). Possible reasons for this are manifold. Negative bacterial cultures may be due to difficult to culture and less treatable organisms such as viruses and fungi, prior antibiotic exposure (which in turn is a possible marker for severity of illness), or undiagnosed noninfectious conditions, such as pulmonary emboli, hypersensitivity reactions, cryptogenic organizing pneumonia, or cancers. Failure or delay in recognizing and treating these alternative conditions may account
for increased mortality in this subgroup. Conversely, positive cultures for pathogenic organisms likely facilitate better outcomes by helping affirm an infectious etiology for the patient’s decompensation and guiding the appropriate choice of antimicrobials. We did not collect suitable data in this study to indicate which of these factors might have accounted for the higher attributable mortality we observed among culturenegative patients.
The clear and consistent association between the objective definitions evaluated in this article and increased length of stay and mortality bespeak their clinical significance but their correlation with histological pneumonia, clinically diagnosed pneumonia, or antibiotic starts is unknown. Prior qualitative analyses of patients that meet either objective or conventional surveillance definitions suggest that both flag similar sets of complications in similar proportions, primarily pneumonia, acute respiratory distress syndrome, pulmonary edema, and atelectasis (16). This is consistent with the extensive literature showing that patients clinically diagnosed with pneumonia actually have a range of underlying diagnoses that may or may not include pneumonia (2, 25, 27). These include diffuse alveolar damage, acute respiratory distress syndrome, pulmonary edema, pulmonary hemorrhage, hypersensitivity reactions, contusion, atelectasis, pulmonary infarction, and others (15, 19, 28). Objective definitions are likely similar to current clinical diagnosis and surveillance definitions in this regard.
The poor specificity of clinical signs for VAP and consequent tendency of all VAP definitions to flag a range of underlying conditions have prompted CDC to propose a new paradigm for ventilatorassociated event surveillance (29, 30). CDC convened a working group of representatives from U.S. critical care, nursing, respiratory therapy, infectious disease, and healthcare epidemiology societies to inform the development of a new surveillance definition for VAP. The working group recommended shifting the focus of surveillance from pneumonia alone to complications of mechanical ventilation in general, defined as sustained deteriorations in ventilator settings after a period of stable or improving settings (specifically ≥2 days of stable or decreasing daily minimum PEEP or Fio2 followed by a rise in daily minimum PEEP of ≥3 cm H2O or rise
Table 4. Patient characteristics
Frequency, n = 8735
Male 4976 (57.3%)Age group, n (%) <40 611 (7.0) 40–59 2252 (25.9) 60–79 4005 (46.1) ≥80 1824 (21.0)Age (mean ± sd) 65.4 ± 15.9Intensive care unit type, n (%) Cardiovascular 942 (10.8) Medical 1221 (14.0) Neuroscience 242 (2.8) Surgical 1254 (14.4) Mixed 5052 (57.8)Comorbidities, n (%) Chronic lung disease 2035 (23.3) Congestive heart failure 2451 (28.1) Myocardial infarction 1770 (20.3) Valvular disease 1298 (14.9) Peripheral vascular disease 917 (10.5) Neurological disease 1327 (15.2) Renal failure 1404 (16.1) Liver disease 328 (3.8) Acquired immunodeficiency
syndrome25 (0.3)
Lymphoma 212 (2.4) Solid cancers 1047 (12.0) Diabetes mellitus 2499 (28.6) Obesity 642 (7.4) Alcohol abuse 515 (5.9) Depression 875 (10.0)Acute Physiology and Chronic
Health Evaluation II Score (median, IQR)
16 (13–19)
Ventilator length of stay (median days, IQR)
3.0 (2.0–7.0)
Hospital length of stay (median days, IQR)
12.0 (7.0–20.0)
Hospital mortality 1843 (21.1%)
IQR, interquartile range.

Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
6 Crit Care Med 2012 Vol. 40, No. 12
in daily minimum Fio2 ≥20 points sustained for ≥2 calendar days). Shifting the focus of surveillance in this direction more accurately describes what can and cannot be discerned using surveillance definitions and emphasizes the importance of preventing all complications in mechanically ventilated patients, not just pneumonia. Our work affirms that this paradigm is a strong predictor of adverse outcomes. Our findings that inflammatory signs, purulent secretions, and pathogenic cultures add little in terms of attributable length of stay or mortality and substantially decrease sensitivity and positive predictive values for hospital death further affirm the wisdom of surveillance for respiratory deterioration in general rather than pneumonia in particular.
Work is now needed to determine the clinical correlates of events flagged by objective definitions. Better understanding of the association between objective definitions and clinical impressions, risk factors, antimicrobial usage, and concomitant diagnoses (e.g., pulmonary edema, atelectasis, thromboembolic disease, sepsis, and abdominal catastrophes) is needed to inform the interpretation of event rates and the development of prevention strategies. It remains to be seen whether existing ventilator care bundles can prevent objectively defined events or whether bundles will need to be expanded to better target pulmonary edema, atelectasis, barotrauma, the acute respiratory distress syndrome, and other
complications of mechanical ventilation in addition to pneumonia.
Future evaluations should also consider how variability in clinical practice patterns impacts case rates for these definitions. Parameters to consider include differences in ventilator management strategies, different clinical thresholds to send pulmonary specimens for culture, routine vs. ondemand Gram staining of pulmonary specimens, and the impact of preferential use of endotracheal aspirates vs. bronchoalveolar lavage Gram stains and/or cultures to evaluate possible respiratory infections. There is a room to consciously or subconsciously “game” these definitions by varying these practices, particularly the definitions that require purulent sputum and/or positive cultures. This is another argument in favor of focusing external reporting on definitions that require respiratory deterioration alone. The fact that respiratory deterioration is contingent upon either a PEEP or Fio2 increase should decrease temptation to selectively manipulate one of these parameters rather than the other to manage hypoxemia. Some might still be tempted to tolerate sustained hypoxemia to limit PEEP and Fio2 increases. If so, the thresholds for significant changes in PEEP and Fio2 might need to be lowered and/or the current decision to exclude Pao2/Fio2 ratios from surveillance algorithms revisited. No surveillance definition is likely to be completely free of risk of gaming. Objective surveillance
for respiratory deterioration alone at least mitigates the problem of surveyor subjectivity.
The incidence densities of ventilatorassociated events captured by objective definitions fall within the general range of VAP rates currently reported to NHSN of CDC (31). The most liberal definition (purulent sputum only) generated an incidence density of 26.3 events per 1,000 ventilator days, a rate substantially higher than current medians. By contrast, the strictest objective definition (highest threshold for respiratory deterioration, abnormal temperature and white blood cell count, purulent sputum, and pathogenic pulmonary culture) yielded only 0.2 events per 1,000 ventilator days, a rate well below the 50th percentile of VAP rates reported to CDC. The intermediate respiratory deterioration definition corresponding to CDC’s proposed new definition for ventilatorassociated conditions generated an incidence density of 12.0 events per 1,000 ventilator days. This is higher than most VAP rates currently reported to NHSN, but this definition explicitly seeks more than just VAP. Furthermore, the appropriateness of using current NHSN rates to benchmark objectively determined rates is unclear given the susceptibility of current definitions to gaming and the increasing disconnect between clinical and surveillance pneumonia rates (32).
The generalizability of objective surveillance methods for widespread,
Figure 1. Sensitivity and positive predictive values for hospital death among selected objective definitions for ventilatorassociated pneumonia. WBC, white blood cell count; fever/WBC, abnormal temperature or white blood cell count; PEEP, positive endexpiratory pressure.

Jdivya 09/14/12 4 color fig(s); F# 08:16 Art: CCM203921
Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Crit Care Med 2012 Vol. 40, No. 12 7
prospective use also requires further evaluation. Our success applying this method to large numbers of patients drawn from diverse hospitals, including both medical and surgical patients and both community and academic institutions, augurs well. All the data elements included in our definitions are routinely recorded by clinical staff on a daily basis and almost all are routinely stored in electronic medical record systems with the possible exception of daily minimum PEEP and Fio2. Nonetheless, it should be straightforward for respiratory therapists or other staff to routinely tabulate these data on bedside charts or in electronic spreadsheets or databases that can then be analyzed manually or with electronic macros and/or statistical code that could be distributed by public health agencies. An Excel spreadsheet that automatically applies a selection of these definitions is available as an online supplement to serve as an example for readers (see Supplemental Digital Content 2, http://links.lww.com/CCM/A546).
Our estimates of attributable lengths of stay and mortality should be tempered by limitations of our study. Retrospective matching of controls to cases can bias the control population towards being healthier (because the controls did not develop VAP) or sicker (if the controls die before they can develop VAP) compared to cases. We attempted to adjust for these possibilities by matching controls to cases on multiple parameters. We also used multivariate regression models to adjust for additional confounders. Some important confounders, however, were not available to us such as reason for admission, recent surgery, and history of trauma.
CONCLUSIONS
In sum, we demonstrate the feasibility of creating objective surveillance definitions for mechanically ventilated patients that can be electronically applied to routinely collectable electronic data. These definitions strongly predict increased ventilator days, hospital days, and hospital mortality. In particular, surveillance for deteriorating ventilator settings after a period of stability or improvement is a potent predictor of adverse outcomes. Requiring concurrent temperature or white blood cell abnormalities, purulent secretions, and pathogenic pulmonary cultures has little impact on attributable
ventilator days or hospital days and paradoxically weakens the association between respiratory deterioration and hospital mortality. Surveillance for ventilatorassociated complications in general rather than pneumonia per se sidesteps the limited accuracy of clinical definitions for VAP and broadens the focus of quality improvement from pneumonia alone to additional morbid complications in mechanically ventilated patients. The strong association between this surveillance paradigm and adverse patient outcomes, its objectivity and efficiency, and its emphasis on tracking all complications in patients on mechanical ventilation rather than pneumonia alone makes it a better candidate for benchmarking within and between institutions (presuming adequate risk adjustment) and therefore a more useful metric to identify best practices and catalyze improved care for ventilated patients. This definition now merits evaluation of its utility in hospital quality and safety improvement programs.
REFERENCES
1. Horan TC, Andrus M, Dudeck MA: CDC/NHSN surveillance definition of health careassociated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008; 36:309–332
2. Tejerina E, Esteban A, FernándezSegoviano P, et al: Accuracy of clinical definitions of ventilatorassociated pneumonia: Comparison with autopsy findings. J Crit Care 2010; 25:62–68
3. Klompas M: Interobserver variability in ventilatorassociated pneumonia surveillance. Am J Infect Control 2010; 38:237–239
4. Klompas M, Platt R: Ventilatorassociated pneumonia—The wrong quality measure for benchmarking. Ann Intern Med 2007; 147:803–805
5. Bonten MJ: Healthcare epidemiology: Ventilatorassociated pneumonia: Preventing the inevitable. Clin Infect Dis 2011; 52:115–121
6. Klompas M: Ventilatorassociated pneumonia: Is zero possible? Clin Infect Dis 2010; 51:1123–1126
7. Chastre J, Viau F, Brun P, et al: Prospective evaluation of the protected specimen brush for the diagnosis of pulmonary infections in ventilated patients. Am Rev Respir Dis 1984; 130:924–929
8. Rouby JJ, Martin De Lassale E, Poete P, et al: Nosocomial bronchopneumonia in the critically ill. Histologic and bacteriologic aspects. Am Rev Respir Dis 1992; 146:1059–1066
9. Wunderink RG, Woldenberg LS, Zeiss J, et al: The radiologic diagnosis of autopsyproven
ventilatorassociated pneumonia. Chest 1992; 101:458–463
10. Torres A, elEbiary M, Padró L, et al: Validation of different techniques for the diagnosis of ventilatorassociated pneumonia. Comparison with immediate postmortem pulmonary biopsy. Am J Respir Crit Care Med 1994; 149(2 Pt 1):324–331
11. Papazian L, Thomas P, Garbe L, et al: Bronchoscopic or blind sampling techniques for the diagnosis of ventilatorassociated pneumonia. Am J Respir Crit Care Med 1995; 152(6 Pt 1): 1982–1991
12. Kirtland SH, Corley DE, Winterbauer RH, et al: The diagnosis of ventilatorassociated pneumonia: A comparison of histologic, microbiologic, and clinical criteria. Chest 1997; 112:445–457
13. Papazian L, AutilloTouati A, Thomas P, et al: Diagnosis of ventilatorassociated pneumonia: An evaluation of direct examination and presence of intracellular organisms. Anesthe-siology 1997; 87:268–276
14. Fàbregas N, Ewig S, Torres A, et al: Clinical diagnosis of ventilator associated pneumonia revisited: Comparative validation using immediate postmortem lung biopsies. Thorax 1999; 54:867–873
15. Petersen IS, Aru A, Skødt V, et al: Evaluation of pneumonia diagnosis in intensive care patients. Scand J Infect Dis 1999; 31:299–303
16. Klompas M, Khan Y, Kleinman K, et al; CDC Prevention Epicenters Program: Multicenter evaluation of a novel surveillance paradigm for complications of mechanical ventilation. PLoS ONE 2011; 6:e18062
17. Klompas M, Kleinman K, Khan Y, et al; CDC Prevention Epicenters Program: Rapid and reproducible surveillance for ventilatorassociated pneumonia. Clin Infect Dis 2012; 54:370–377
18. Klompas M, Kleinman K, Platt R: Development of an algorithm for surveillance of ventilatorassociated pneumonia with electronic data and comparison of algorithm results with clinician diagnoses. Infect Control Hosp Epidemiol 2008; 29:31–37
19. Meduri GU, Mauldin GL, Wunderink RG, et al: Causes of fever and pulmonary densities in patients with clinical manifestations of ventilatorassociated pneumonia. Chest 1994; 106:221–235
20. WinerMuram HT, Rubin SA, Ellis JV, et al: Pneumonia and ARDS in patients receiving mechanical ventilation: Diagnostic accuracy of chest radiography. Radiology 1993; 188: 479–485
21. Albaum MN, Hill LC, Murphy M, et al: Interobserver reliability of the chest radiograph in communityacquired pneumonia. PORT Investigators. Chest 1996; 110: 343–350
22. Loeb MB, Carusone SB, Marrie TJ, et al: Interobserver reliability of radiologists’ interpretations of mobile chest radiographs for

Copyright (c) Society of Critical Care Medicine and Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
8 Crit Care Med 2012 Vol. 40, No. 12
nursing homeacquired pneumonia. J Am Med Dir Assoc 2006; 7:416–419
23. Charlson ME, Pompei P, Ales KL, et al: A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis 1987; 40:373–383
24. Elixhauser A, Steiner C, Harris DR, et al: Comorbidity measures for use with administrative data. Med Care 1998; 36:8–27
25. Klompas M: Does this patient have ventilatorassociated pneumonia? JAMA 2007; 297: 1583–1593
26. Muscedere JG, McColl C, Shorr A, et al: Canadian Critical Care Trials Group: Determinants of outcome in patients with a clinical
suspicion of ventilatorassociated pneumonia. J Crit Care 2008; 23:41–49
27. ReaNeto A, Youssef NC, Tuche F, et al: Diagnosis of ventilatorassociated pneumonia: A systematic review of the literature. Crit Care 2008; 12:R56
28. Marquette CH, Copin MC, Wallet F, et al: Diagnostic tests for pneumonia in ventilated patients: Prospective evaluation of diagnostic accuracy using histology as a diagnostic gold standard. Am J Respir Crit Care Med 1995; 151:1878–1888
29. Magill SS, Fridkin SK: Improving surveillance definitions for ventilatorassociated pneumonia in an era of public reporting and
performance measurement. Clin Infect Dis 2012; 54:378–380
30. Centers for Disease Control and Prevention: Improving surveillance for ventilator associated events in adults. Available at: http://www.cdc.gov/nhsn/PDFs/vae/CDC_VAE_CommunicationsSummaryforcompliance_20120313.pdf. Accessed April 26, 2012
31. Dudeck MA, Horan TC, Peterson KD, et al: National Healthcare Safety Network (NHSN) report, data summary for 2009, deviceassociated module. Am J Infect Control 2011; 39:349–367
32. Klompas M: Is a ventilatorassociated pneumonia rate of zero really possible? Curr Opin Infect Dis 2012; 25:176–182