Correlation of α-thalassemia haplotype with detection of hemoglobin Bart's in cord blood by...
9
SCREENING Journal of the International Screening 3 (1994) 131-139 Society of Neonatal Screening Correlation of a-thalassemia haplotype with detection of hemoglobin Bart’s in cord blood by cellulose acetate or isoelectric focusing Ted Zwerdling”, Carmin D. Powell, Donald Rucknagel Department of Pediatrics, University of Cincinnati School of Medicine and the Children’s Hospital Research Foundation, and the Cincinnati Sickle Cell Center, Cincinnati, OH, USA Received 6 May 1993; revision accepted 19 May 1994 Introduction: Newborn screening for hemoglobinopathies is occurring in many locations in the United States. Commonly, liquid cord blood may be screened with either cellulose acetate (CAC) or isoelectric focusing (IEF) electrophoresis. The presence of hemoglobin Bart’s (y4), has been correlated with a-thalassemia, as defined by restriction fragment analysis. However, there are no data in the literature correlating the sensitivity of these two electrophoretic methods with the detection of thalassemic genotype. Methods: Random samples of liquid cord blood were collected initially, based on the presence of hemoglobin Bart’s on CAC and then compared with detection by IEF. A second set of samples was then chosen based on the absence of hemoglobin Bart’s on CAC. IEF was also performed. Restriction analysis of all samples was performed to determine cl-thalassemia or normal genotype. A total of 72 samples was analy:zed. Results: All patients with hemoglobin Bart’s on CAC had Bart’s detectable by IEF (n =2:1). Eighteen of these samples were consistent for homozygous a-thal-2, whereas three showed a heterozygous cl-thal-2 haplotype. In the second set of 51 samples without hemoglobm Bar-t’s on CAC, four samples were detected by IEF to have hemoglobin Bart’s. Among 47 samples without hemoglobin Bait’s by either method, ten were heterozygous for a-thal-2 haplotype, and the remaining 37 samples were normal. Discussion: Our data indicate that CAC and IEF are both accurate in the detection of hemoglobin Bart’s in persons who are a-thal-2 homozygous. For a-thal-2 heterozygous haplotype, IEF is more sensitive in determining the presence of hemoglobin Bart’s than CAC. However, neither method will detect the majority of this haplotype. We suggest more sophisticated molecular analysis for detection of a-thal-2 heterozygous genotype in at-risk populations. Keywords: Hemoglobin; a-Thalassemia; Electrophoresis; Newborn screening * Corresponding author: Hematology-Oncology Division, Children’s Hospital Medical Center, Elland and Bethesda Avenues, Cincinnati, OH 45229-2899, USA. 1994 Elsevier Science B.V. SSDZ 0925-6164(94)00010-6
Transcript of Correlation of α-thalassemia haplotype with detection of hemoglobin Bart's in cord blood by...

SCREENING Journal of the International
Screening 3 (1994) 131-139
Society of Neonatal Screening
Correlation of a-thalassemia haplotype with detection of hemoglobin Bart’s in cord blood by cellulose acetate or
isoelectric focusing
Ted Zwerdling”, Carmin D. Powell, Donald Rucknagel Department of Pediatrics, University of Cincinnati School of Medicine and the Children’s Hospital Research
Foundation, and the Cincinnati Sickle Cell Center, Cincinnati, OH, USA
Received 6 May 1993; revision accepted 19 May 1994
Introduction: Newborn screening for hemoglobinopathies is occurring in many locations in the United States. Commonly, liquid cord blood may be screened with either cellulose acetate (CAC) or isoelectric focusing (IEF) electrophoresis. The presence of hemoglobin Bart’s (y4), has been correlated with a-thalassemia, as defined by restriction fragment analysis. However, there are no data in the literature correlating the sensitivity of these two electrophoretic methods with the detection of thalassemic genotype. Methods: Random samples of liquid cord blood were collected initially, based on the presence of hemoglobin Bart’s on CAC and then compared with detection by IEF. A second set of samples was then chosen based on the absence of hemoglobin Bart’s on CAC. IEF was also performed. Restriction analysis of all samples was performed to determine cl-thalassemia or normal genotype. A total of 72 samples was analy:zed. Results: All patients with hemoglobin Bart’s on CAC had Bart’s detectable by IEF (n =2:1). Eighteen of these samples were consistent for homozygous a-thal-2, whereas three showed a heterozygous cl-thal-2 haplotype. In the second set of 51 samples without hemoglobm Bar-t’s on CAC, four samples were detected by IEF to have hemoglobin Bart’s. Among 47 samples without hemoglobin Bait’s by either method, ten were heterozygous for a-thal-2 haplotype, and the remaining 37 samples were normal. Discussion: Our data indicate that CAC and IEF are both accurate in the detection of hemoglobin Bart’s in persons who are a-thal-2 homozygous. For a-thal-2 heterozygous haplotype, IEF is more sensitive in determining the presence of hemoglobin Bart’s than CAC. However, neither method will detect the majority of this haplotype. We suggest more sophisticated molecular analysis for detection of a-thal-2 heterozygous genotype in at-risk populations.
Keywords: Hemoglobin; a-Thalassemia; Electrophoresis; Newborn screening
* Corresponding author: Hematology-Oncology Division, Children’s Hospital Medical Center, Elland and Bethesda Avenues, Cincinnati, OH 45229-2899, USA.
1994 Elsevier Science B.V. SSDZ 0925-6164(94)00010-6

132 T. Zwerdling et al./Screening 3 (1994) 131-139
1. Introduction
Many states in the United States are routinely screening the hemoglobin of newborns by electrophoretic or chromatographic techniques to detect sickle cell anemia. With these methods, hemoglobinopathies that include the thalassemia syn- dromes will be detected in increasing numbers. This study was undertaken to assess
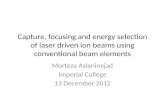
Fig. 1. Top: Configuration of cwglobin genes as they occur in the normal and thalassemic states. Shaded boxes indicate functional genes; unshaded boxes are non-functional. Bottom: Ploypeptide chain composi- tion of various hemoglobins.

T. Zwerdling et al./Screening 3 (1994) 131-139 133
the relative sensitivity of isoelectric focusing (IEF) and cellulose acetate (CAC) in the detection of a-thalassemia in African-American infants.
Hemoglobin is the predominant protein found in the cytoplasm of red blood cells and is composed of an iron containing heme moiety and two m- and two P-like heterodimer globin chains. Found on chromosomes 16 and 11 are clusters of genes encoding for the c1 and B; polypeptides chains, respectively (see Fig. 1, top). The expression of the globin genes is developmentally regulated and may be detected as different types of hemoglobin (see Fig. 1, bottom). For example, fetal hemoglobin (Hb F) is composed of two u and two y polypeptide chains. The proportion of fetal globin is high early in gestation and decreases progressively in the later stages of pregnanlcy. B-Chain synthesis is reciprocal to that of y, resulting in eventual replace- ment of Hb F (cl,y,) with Hb A (azbz). In addition to developmental regulation, the expression of a and B; genes are normally balanced with both polypeptide chains present in red blood cells in approximately equimolar amounts. In thalassemia, however, an imbalance in the synthesis of one of the chains exists, leading to a relative excess in the amount of the remaining normal chain. a-Thalassemia, most often re,sults when a deletion in all or part of the a-globin cluster has occurred, leaving some of the normally expressed P-like chains unpaired. In the newborn, unpaired y-chains form homopolymers known as Bart’s hemoglobin (y4) that are indicative of a-thalassemia. Four phenotypes are recognized, the severity determined by the number of alleles inactivated at the two a-globin loci. Since most often a-thalassemia is deletional in origin, it can easily be diagnosed by restriction analysis [ 11. Heretofore, a correlation has been shown between the phenotype based on hematologic characteristics and the proportion of Hb Bart’s measured by either cellulose acetate electrophoresis or column chromatography [2-41. Although numer- ous studiies correlating the proportion of Hb Bart’s with phenotype and serotype have been reported [ 5-101, we have found no investigations comparing IEF and CAC phenotype with the restriction genotype.
We report herein correlation between the a-thalassemia genotype based on restric- tion analysis of DNA and the presence of Hb Bart’s on both CAC and IEF electrophoreses of the newborn’s hemoglobin. We also report the relative sensitivities of detecting Hb Bart’s in these two electrophoretic screening methods. Our data indicate that CAC will miss most heterozygotes with single gene deletions and that IEF will detect only about 40% of these. These data have implications for accurate diagnosis as well as genetic counselling of at-risk populations.
2. Me&ads
Sample collection As part of an ongoing screening program of African-American newborns, cord
blood was collected in EDTA anti-coagulant during a 3-month period in 1990. A total of 1412 samples were processed. The samples were subjected to electrophoresis within 10 days of arrival in the laboratory.

134 T. Zwerdling et al.lScreening 3 (1994) 131-139
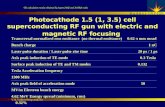
Sample selection Inasmuch as the frequency of a-thalassemia is low, an efficient two-tiered sampling
method (see Fig. 2) was employed whereby the upper and lower tails of the distribu- tion of Hb Bart’s were examined. The first group consisted of the initial 21 consecu- tive samples with Hb Bart’s present on CAC electrophoresis. If the presence of Hb Bart’s was detected on CAC, an IEF gel was prepared and scanned (see below). A second group of 51 samples from African-American infants was then examined. These samples were chosen based on the absence of Hb Bart’s on stained CAC gels. IEF gels were then prepared for these samples. Race was determined by parental declaration on the birth certificate. Southern blot analysis was performed on all 72 samples.
Electrophoresis Liquid cord blood anticoagulated with EDTA was examined by standard methods
for CAC and IEF. Standards for hemoglobin were obtained from Helena Laboratories (Beaumont, TX) or have been accumulated by our laboratory over time. Hb Bart’s was identified by matching electrophoretic migration with those of the standards, and by electrophoresis on CAC at pH 7.1. [ 111.
72 Samples
CAC e CAC @
,/ ‘\,l
IEF e IEF @
/^\,
IEF @
47 4 21
Ii A 10 37 4 18 3 01- cg aa
c1- CL- a- aa
1 E
k C T R 0
R 0 R E S I S
J :: 1 P Y
i
Fig. 2. Results of 72 samples analyzed for the presence @ or absence Q of Hb Bart’s and correlation with haplotype. See text for details.

T Zwerdling et al./Screening 3 (1994) 131-139 135
Cellulose acetate electrophoresis The procedure was performed according to the manufacturer’s instruction (Helena
Laboratories, Beaumont, TX) at pH 8.6. Briefly, 1 drop of cord blood was placed into 5 (drops of hemolyzing solution. Five ul of hemolysate were loaded onto the cellulose acetate membrane and electrophoresed at 450 V for 15 min at room temperature. The membrane was stained with Ponceau S stain for 5 min, destained with acetic acid, and finally cleared with acetic acid and ethanol. After the staining, the gel was scanned at 525 nm on a CLINISCAN II (Helena Laboratories) densito- meter to determine the per cent Hb Bart’s.
Isoelectric focusing According to the manufacturer’s instructions (Isolab Inc., RESOLVE Hb kit), an
hemolysate of 25 ul of whole blood was made. Sample hemoglobin was adjusted to between 10 and 20 mg/ml. Three pl of this solution were added to a pre-cooled gel which was then run at 15 W (constant power) for 40 min at 5°C. The gel was then spectrophotometrically scanned. Initially, scanning was performed at 415 nm, but this was found to give a high background and, subsequently, 545 nm was used. After densitometry, the gel was fixed with 10% TCA and stained with o-dianisidine/H,O, .
Isolation of DNA DNA was isolated by standard means [ 11. Red blood cells were removed from
the cord blood samples by hypotonic lysis. The remaining cells were then incubated with Proteinase K (final concentration, 0.15 ug/ul), SDS (0.5% final concentration), and NaCl (0.1 M final concentration) overnight at 37°C. This material was then mixed with an equal volume of buffered phenol and shaken for 30 min at room temperature. The aqueous and phenol phases were separated and the procedure repeate’d. An equal volume of chloroform/isoamylalcohol (24: 1) was then mixed with the aqueous phase and again shaken at room temperature for 30 min. The aqueous phase was separated and placed in a fresh microtube. DNA was precipitated with one-half volume 7.5 M ammonium acetate and 2 volumes of isopropanol for 1 h at 0°C. The DNA pellet was separated by spooling, washed with 70% ethanol, and dried under vacuum. The pellet was resuspended in Tris/EDTA, and the concen- tration determined by absorbance at 260 mn.
Southern analysis Ten ltg of DNA samples were digested with restriction endonucleases, BamHI and
BgZII, overnight in appropriate buffer at 37°C. The next day a 0.8% agarose gel was prepared, and the entire sample electrophoresed in TAE buffer. DNA was denatured in the gel using 1.5 M NaCl and 0.5 M NaOH, and then neutralized to pH 8.0. Overnight transfer to nitrocellulose membrane in 20 x SSC was followed by baking at 80°C for 1 h under vacuum. Meanwhile, 50 ng of an a-globin cDNA probe (pIW101) labelled by random priming with 32P was prepared. The nitrocellulose filter was pre-hybridized at 68°C for 1 h, and then incubated with probe in hybridiza- tion media overnight. Non-bound probe was removed under stringent conditions

136 T. Zwerdling et al./Screening 3 (1994) 131-139
(washes with 1 x SSC, 0.1% SDS). The filter was autoradiographed for 48 h at -70°C. Results of the autoradiogram were then scored for a-thalassemia. With BumHI digestion, a 14 kb fragment is expected with four genes present. In a-thalassemia-2 heterozygotes (single deletion), an abnormal 10 kb fragment is seen along with the 14 kb normal band. Homozygotes for the single gene deletion have only the 10 kb band. Using BgZII, normally two bands are seen which are 7 kb and 12 kb in size. In the single 3.7 kb deletion, an additional 15 kb band is present. Homozygotes have only the 15 kb band. In the 4.5 kb (leftward) deletion, the 12 kb band is diminished in intensity in heterozygotes and absent in homozygotes.
3. Results
Among the 21 samples with Hb Bart’s on CAC electrophoresis selected for further study, all had Hb Bart’s by IEF and an abnormal Southern blot analysis (Fig. 2). Eighteen restriction analyses were consistent for homozygosity for the a-thal-2 haplotype and three samples showed a restriction pattern consistent with a heterozygous c.+thal-2 haplotype.
In the second tier of the study, 51 samples without Hb Bart’s on CAC electrophore- sis were further studied. Among these samples, four were detected by IEF to have Hb Bart’s (Fig. 2). These four samples were heterozygous for cl-thal-2 haplotype by Southern analysis. Among 47 samples without Hb Bart’s by either IEF or CAC, ten were heterozygous a-thal-2 by Southern analysis; the remaining 37 samples showed all four cl-globin genes to be present. Thus, by CAC 18% of heterozygotes were detected; by IEF, the proportion detected was 41%.
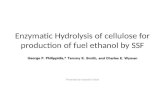
The mean proportion of Hb Bart’s in the three heterozygotes in which Bart’s was visible by CAC electrophoresis was 1.5% (range 1.3-1.8%). The mean proportion of Hb Bart’s in the seven heterozygotes that were detected by IEF was 1.7% (range 1.3-2.3%). In the 18 homozygotes, the mean proportion of Hb Bart’s by CAC was 4.6% (range 2.3-6.3%); by IEF 5.8% (range 3.8-10%) (Fig. 3).
4. Discussion
Various a-thalassemia syndromes are determined by the number of cl-globin genes that are functional. Accordingly, loss of a single allele (heterozygous cL-thalassemia-2) is the silent carrier state which has few hematologic manifestations. The homozygous state for this haplotype is hematologically equivalent to a-thalassemia-1, in which both genes on chromosome 16 are deleted or one is deleted and the other non- functional. Compound heterozygotes lacking three genes have Hemoglobin H disease. This genotype has severe clinical consequences and would be expected to have 30% Hb Bart’s at birth. Homozygotes for cl-thalassemia-1 have fetal hydrops and produce only Hb Bart’s (Fig. 1).
Approx. 30% of African-Americans are heterozygous for the a-thalassemia-2 haplotype, and the frequency of the homozygous state is approx. 2.6% [3]. Silent

i? Zwerdling et al./Screening 3 (1994) 131-139 137
% Bart’s X IEF
Fig. 3. Linear regression of the proportion of Hb Bart’s as measured by CAC and IEF. Filled squares indicate heterozygous a-thal-2; dotted squares indicate homozygous a-thal-2. RZ=0.66.
carriers or heterozygotes for a-thalassemia-2 have been reported to have approx. 1 to 2% Hb Bart’s at birth, usually determined by CAC electrophoresis or chromato- graphy [2-41. Dash et al. [2] have reported finding as little as 0.25% Hb Bart’s using IEF; the number of false-negative results was unknown. However, we were unable to find any comparative studies in the literature that correlated genotype with both CAC and IEF. Zhao et al. [ 121 reported on a large number of cord blood results from Ch.ina. Using a discontinuous electrophoresis system, one of ten negative controls was found to have heterozygous a-thalassemia-2 genotype.
Our study was designed to compare the sensitivity of CAC and IEF for screening purposes. Our strategy for these experiments was to initially correlate the value of Hb Bart’s present in modest amounts on CAC with that determined by IEF. A second group, chosen because no Hb Bart’s was detectable on CAC, was designed to determine the relative threshold for detection of the two methods. IEF proved to be more sensitive with Hb Bart’s detectable in four samples not found by CAC. We then correlated haplotype with electrophoresis results and found that haplotyping was more sensitive than either IEF or CAC in the detection of the heterozygotes for a-thalassemia-2. Because of the way this study was designed, the data cannot be extrapolated to the universe of all heterozygotes for a-thal-2. Nevertheless, in this study, 41% of those patients with deletions of one a-globin gene had Hb Bart’s by IEF, whjile only 18% of the same group were demonstrable by CAC. A possible reason for this finding is based on differences inherent in the two techniques. IEF separates proteins based on charge in a pH gradient gel. The protein is focused at the isoelectric point in the gel, all of the material being in a narrow band increasing the chance of detection. CAC membranes also separate proteins on the basis of charge, blut the protein bands tend to diffuse, decreasing the band intensity below a threshold of detection.
While these data clearly indicate that IEF is more sensitive than CAC, in nearly 60% of heterozygotes for a-thalassemia-2 the presence of Hb Bart’s is still undetected.

138 T. Zwerdling et al./Screening 3 (1994) 131-139
In mass newborn screening programs, the initial IEF electrophoresis is performed by applying a maximum number of samples using smaller volumes than were employed in this study. Under those circumstances, it is unlikely that a significantly larger proportion of a-thal-2 heterozygotes can be detected. It is not clear whether chromatographic techniques will improve the ability to detect the presence of Hb Bart’s.
The sensitivity of CAC and IEF, in the detection of hemoglobin Bart’s, will also depend on whether liquid or dried blood samples are used. Papadea et al. [lo] have recently reported that liquid cord blood samples are superior for the detection of hemoglobin Bart’s in infants with presumptive one gene deletion a-thalassemia. In 1239 occurrences of hemoglobin Bart’s, detected either by CAC or IEF, nearly two- thirds were observed in cord blood. The cord blood samples were evaluated by CAC. Dried blood samples, having been analyzed by IEF, were found to show the presence of hemoglobin Bart’s in only one-third. However, in 101 dried blood samples, in which the level of hemoglobin Bart’s assessed by high performance liquid chromatography (HPLC) and IEF suggested two-gene deletion a-thalassemia, none were detected by CAC electrophoresis of liquid cord samples. These authors suggest that HPLC and liquid cord blood analysis should be undertaken in screening programs with interest in the detection of hemoglobin Bart’s.
The presence of small amounts of Hb Bart’s in cord blood does not presage significant hematologic disorder. It does signal the potential for more serious anemias, namely, Hb H disease or Bart’s/hydrops fetalis among subsequent offspring. Thus, haplotyping of parents may be desirable, although expensive and not readily available. Although small, this study suggests that the break point between deletion of one and two c1 genes is between two and three per cent Bart’s. This is of some value in genetic counseling.
In summary, we report that IEF is more sensitive than standard CAC in the detection of Hb Bart’s and have correlated this with genotype. More sophisticated molecular analysis is needed to determine silent mutations. While IEF is a better method than standard CAC electrophoresis, it’s sensitivity is still poor and many cases will go undetected. These data have implications for diagnosis, patient care, and genetic counseling.
Acknowledgements
The authors appreciate the technical assistance of Linda Leslie, Ramona DuBose, Paula Pietryga, and Dorothy Elsaesser. The authors also wish to acknowledge the typing assistance of Donna Accorinti, and Sandi Jones in preparation of this manuscript. This work was funded by USPHS-HL-16008.
References
[l] Ausubel FM, Brent R, Kingston RE, Moore DD, Smith JA, Editors. Current protocols in molecular biology. New York: Green Publishing Associates, 1987; 2.9.

T. Zwerdling et al./Screening 3 (1994) 131-139 139
[2] Daslh S, Vashist K, Sehgal S, Devi S, Verma A. Isoelectric focusing for the measurement of hemoglobin levels in cord blood and detection of CL thalassemia. Indian J Med Res 1987; 62-66.
[3] Dozy AM, Kan YW, Embury SH, et al. c+Globin gene organization in Blacks precludes the severe form of a-thalassemia. Nature 1979; 280: 605-607.
[4] Henson JB, Carver JR, Wilson JB, Huisman TH. Carboxymethyl-cellulose microchromatography for rhe quantitation of hemoglobin (gamma 4) and its use in the detection of the a-thalassemia conditions. J Chromatogr 1980; 198: 443-448.
[5] Higgs DR, Lamb J, Aldridge BE, et al. Inadequacy of Hb Bart’s as an indicator of cx thalassemia (letter). Br J Haematol 1982; 51: 177-178.
[6] Hig8s DR, Pressley L, Clegg JB, et al. Detection of a thalassemia in Negro infants. Br J Haematol 1980; 46: 39946.
[7] Hig8s DR, Pressley L, Clegg JB, Weatherall DJ, Serjeant GR. a-thalassemia in Black populations. The Johns Hopkins Journal 1980; 146: 300-310.
[8] Ohene-Frempong K, Rappaport E, Atwater J, Schwartz E, Surrey S. Alpha-gene deletions in black newborn infants with Hb Bart’s. Blood 1980; 56: 931-933.
[9] Serjeant BE, Forbes M, Williams LL, Serjeant GR: Screening cord bloods for detection of sickle cell (disease in Jamaica. Clin Chem 1974; 20: 666-67.
[lo] Papadea C, F&man JR, Kuehnert RS, Platt AF. Comparison of liquid and dried blood for neonatal hemoglobinopathy screening: laboratory and programmatic issues. Pediatrics 1994; 93: 427.
[ 1 l] Schmidt RA, Brossius E. Basic laboratory methods of hemoglobinopathy detection. US Dept. HEW, PHS Center Disease Control, Atlanta, GA, 1976.
[12] Zhao W, Zhang J, Wang NS, Peng P. The relationship between Hb Bart’s in cord blood and the deletions of u globin genes. Hemoglobin 1988; 12: 519-527.