Comparison of 1α-hydroxycholecalciferol and 25 ... · Comparison of la-hydroxycholecalciferol and...
9
Kidney International, Vol. 15 (1979), pp. /96 —204 Comparison of la-hydroxycholecalciferol and 25-hydroxy- cholecalciferol in the treatment of renal osteodystrophy: Greater effect of 25-hydroxycholecalciferol on bone mineralization ALBERT FOURNIER, PHILIPPE BORDIER, JEAN GUERIS, JEAN Luc SEBERT, PIERRE MARIE, CHRISTINE FERRIERE, JEANINE BEDROSSIAN, AND HECTOR F. DELUCA Service de Néphrologie et Clinique IVlédicale B, Centre Hospitalier Universitaire d'Amiens; André Lichwitz Research Unit of the Institut National de Ia Sante et de la Recherche Tvlédicale (Hôpital Lariboisière), Clinique Médicale Néphrologique, Hópital Broussias, Paris, and Department of Biochemistry, College of Agricultural and Life Science, University of Wisconsin, Madison, Wisconsin Comparison of la-hydroxycholecalciferol and 25-hydroxy- cholecalciferol in the treatment of renal osteodystrophy: Greater effect of 25-hydroxycholecalciferol on bone mineralization. A com- parison was made of the biochemical and osseous effects of in- OH vitamin D3 and 25-OH vitamin D3 in uremic men on chronic hemodialysis. Two groups of patients dialyzed in the same center were matched for their plasma concentrations of calcium (Pca), phosphate (P0), immunoreactive parathyroid hormone (PIPTH), 25-OH vitamin D (P2Hfl), their serum alkaline phosphatase (Alk. Pase), and their degree of osteomalacia as assessed on bone histomorphometry. The first group received la-OH-D3 for 2 to 9 months at a mean daily dosage of 1 to 2 zg, and the second group received 25-OH-D3 for ito 6 months at a mean daily dos- age of 50 to 100 rig. The la-OH-D3 therapy was more effective than the 25-OH-D3 therapy was in increasing the P( X P0 prod- uct, in decreasing the serum Alk. Pase and the percent of osteo- blastic surface (OB). On the other hand, 25-OH-D3 therapy ini- tially increased bone formation and was more effective than was the la-OH-D3 in increasing the mineralization front (MF). In one patient, in which the MF did not increase after 9 months of la-OH-D3, it increased from 34.0 to 44.6% after addition of 25-OH- D3. Increased serum calcium occurred earlier with la-OH-D than it did with 25-OH-D3 (2 vs. 8 weeks), and reversal of hyper- calcemia was more rapid after withholding treatment with la- OH-D3 than it was with 25-OH-D3 (1 vs. 4 weeks). It is concluded that (1) large dosages of 25-OH-D3, rather than "physiologic" dos- ages of la-OH-D3, induce more effectively bone mineralization in spite of a smaller increase of the P. x Pm), product and may be therefore a better treatment for a renal osteomalacia; (2) the more rapid reversal of hypercalcemia induced by la-OH-D3, however, makes the use of this tatter less hazardous than that of 25-OH-D3. Comparison du la-hydroxycholécalciférol et du 25-hydroxy- cholécalciférol dans le traitement de l'ostéodystrophie rénale: Ef- Received for publication July 25, 1977 and in revised form August II, 1978. 0085-2538/79/0015-0196 $01.80 © 1979 by the International Society of Nephrology 196 ficacité supérieure de 25-hydroxycholécatciférol sur Ia minéralisa- tion de l'os. On a compare les effets osseux et biochimiques de Ia la-OH-vitamine D3 et de Ia la-25-OH vitamine D3 sur deux groupes de matades uremiques en hémodialyse chronique. Les deux groupes étaient dialyses dans le méme centre et étaient comparables au depart en ce qui concerne leurs concentrations plasmatiques de calcium (Pea), de phosphore (P0) d'hormone parathyroidienne immunoréactive (PIPTH), de 25-OH vitamine D (P2oHD,) teurs phosphatases alcalines sériques et leur degré d'ostéomalacie appréciée par histomorphométrie. Le premier groupe a recu de Ia la-OH-D3 pendant 2 to 9 mois a Ia dose journalière moyenne de 1 a 2 rg et le second groupe a recu de la 25-OH-D3 pendant 1 a 6 mois ?t Ia dose journalière moyenne de 50 a 100 g. La la-OH-D3 a été plus efficace que Ia 25-OH-D dans l'augmentation du produit phosphocalcique, Ia diminution des phosphatases alcalines et de Ia surface ostëoblastique. A I'opposé Ia 25-OH-D3 entraina une augmentation initiale de la formation osseuse et a été plus efficace que Ia la-OH-D3 dans l'augmentation du front de minéralisation (FM). Chez un mal- ade, le FM qui n'avait pas augmenté aprés 9 mois de la-OH-D3, s'accrut de 34,0% a 44,6% après addition de 25-OH-D3. L'augmentation de Ia calcémie est survenue plus rapidement avec la la-OH-D3 qu'avec la 25-OH-D3 (2 semaines contre 8 se- maines) et Ia correction de l'hypercalcemie a éte plus rapide après l'arrêt de Ia la-OH-D3 qu'après arrét de la 25-OH-D3 (I se- maine contre 4 semaines). En conclusion (1) de fortes doses de 25-OH-D3 sont plus efficaces que des doses physiologiques" de la-OH-D3 pour augmenter la minéralisation osseuse en dépit d'une moindre augmentation du produit phosphocalcique et pourraient ainsi représenter un meilleur traitement de l'ostéomalacie rénale; (2) la correction plus rapide de l'hypercaicemie induite par la la-OH-D3 rend cependant l'usage de cette dernière moms dangereux que celui de Ia 25-OI-T-D3. In patients on chronic hemodialysis, radiologic renal osteodystrophy has become less frequent [1, 2] due to a better control of calcium and phosphate homeostasis by means of phosphate binders, oral calcium supplements, high dialysate calcium, and more frequent dialysis with deionized water. Com-
Transcript of Comparison of 1α-hydroxycholecalciferol and 25 ... · Comparison of la-hydroxycholecalciferol and...

Kidney International, Vol. 15 (1979), pp. /96 —204
Comparison of la-hydroxycholecalciferol and 25-hydroxy-cholecalciferol in the treatment of renal osteodystrophy:
Greater effect of 25-hydroxycholecalciferolon bone mineralization
ALBERT FOURNIER, PHILIPPE BORDIER, JEAN GUERIS, JEAN Luc SEBERT, PIERRE MARIE,CHRISTINE FERRIERE, JEANINE BEDROSSIAN, AND HECTOR F. DELUCA
Service de Néphrologie et Clinique IVlédicale B, Centre Hospitalier Universitaire d'Amiens; André Lichwitz ResearchUnit of the Institut National de Ia Sante et de la Recherche Tvlédicale (Hôpital Lariboisière), Clinique Médicale
Néphrologique, Hópital Broussias, Paris, and Department of Biochemistry, College of Agricultural and Life Science,University of Wisconsin, Madison, Wisconsin
Comparison of la-hydroxycholecalciferol and 25-hydroxy-cholecalciferol in the treatment of renal osteodystrophy: Greatereffect of 25-hydroxycholecalciferol on bone mineralization. A com-parison was made of the biochemical and osseous effects of in-OH vitamin D3 and 25-OH vitamin D3 in uremic men on chronichemodialysis. Two groups of patients dialyzed in the same centerwere matched for their plasma concentrations of calcium (Pca),phosphate (P0), immunoreactive parathyroid hormone (PIPTH),25-OH vitamin D (P2Hfl), their serum alkaline phosphatase(Alk. Pase), and their degree of osteomalacia as assessed onbone histomorphometry. The first group received la-OH-D3 for2 to 9 months at a mean daily dosage of 1 to 2 zg, and the secondgroup received 25-OH-D3 for ito 6 months at a mean daily dos-age of 50 to 100 rig. The la-OH-D3 therapy was more effectivethan the 25-OH-D3 therapy was in increasing the P( X P0 prod-uct, in decreasing the serum Alk. Pase and the percent of osteo-blastic surface (OB). On the other hand, 25-OH-D3 therapy ini-tially increased bone formation and was more effective than wasthe la-OH-D3 in increasing the mineralization front (MF). In onepatient, in which the MF did not increase after 9 months ofla-OH-D3, it increased from 34.0 to 44.6% after addition of 25-OH-D3. Increased serum calcium occurred earlier with la-OH-Dthan it did with 25-OH-D3 (2 vs. 8 weeks), and reversal of hyper-calcemia was more rapid after withholding treatment with la-OH-D3 than it was with 25-OH-D3 (1 vs. 4 weeks). It is concludedthat (1) large dosages of 25-OH-D3, rather than "physiologic" dos-ages of la-OH-D3, induce more effectively bone mineralizationin spite of a smaller increase of the P. x Pm), product and maybe therefore a better treatment for a renal osteomalacia; (2) themore rapid reversal of hypercalcemia induced by la-OH-D3,however, makes the use of this tatter less hazardous than that of25-OH-D3.
Comparison du la-hydroxycholécalciférol et du 25-hydroxy-cholécalciférol dans le traitement de l'ostéodystrophie rénale: Ef-
Received for publication July 25, 1977and in revised form August II, 1978.
0085-2538/79/0015-0196 $01.80© 1979 by the International Society of Nephrology
196
ficacité supérieure de 25-hydroxycholécatciférol sur Ia minéralisa-tion de l'os. On a compare les effets osseux et biochimiques de Iala-OH-vitamine D3 et de Ia la-25-OH vitamine D3 sur deuxgroupes de matades uremiques en hémodialyse chronique. Lesdeux groupes étaient dialyses dans le méme centre et étaientcomparables au depart en ce qui concerne leurs concentrationsplasmatiques de calcium (Pea), de phosphore (P0) d'hormoneparathyroidienne immunoréactive (PIPTH), de 25-OH vitamine D(P2oHD,) teurs phosphatases alcalines sériques et leur degréd'ostéomalacie appréciée par histomorphométrie. Le premiergroupe a recu de Ia la-OH-D3 pendant 2 to 9 mois a Ia dosejournalière moyenne de 1 a 2 rg et le second groupe a recu de la25-OH-D3 pendant 1 a 6 mois ?t Ia dose journalière moyenne de50 a 100 g. La la-OH-D3 a été plus efficace que Ia 25-OH-Ddans l'augmentation du produit phosphocalcique, Ia diminutiondes phosphatases alcalines et de Ia surface ostëoblastique. AI'opposé Ia 25-OH-D3 entraina une augmentation initiale de laformation osseuse et a été plus efficace que Ia la-OH-D3 dansl'augmentation du front de minéralisation (FM). Chez un mal-ade, le FM qui n'avait pas augmenté aprés 9 mois de la-OH-D3,s'accrut de 34,0% a 44,6% après addition de 25-OH-D3.L'augmentation de Ia calcémie est survenue plus rapidementavec la la-OH-D3 qu'avec la 25-OH-D3 (2 semaines contre 8 se-maines) et Ia correction de l'hypercalcemie a éte plus rapideaprès l'arrêt de Ia la-OH-D3 qu'après arrét de la 25-OH-D3 (I se-maine contre 4 semaines). En conclusion (1) de fortes doses de25-OH-D3 sont plus efficaces que des doses physiologiques" dela-OH-D3 pour augmenter la minéralisation osseuse en dépitd'une moindre augmentation du produit phosphocalcique etpourraient ainsi représenter un meilleur traitement del'ostéomalacie rénale; (2) la correction plus rapide del'hypercaicemie induite par la la-OH-D3 rend cependant l'usagede cette dernière moms dangereux que celui de Ia 25-OI-T-D3.
In patients on chronic hemodialysis, radiologicrenal osteodystrophy has become less frequent [1,2] due to a better control of calcium and phosphatehomeostasis by means of phosphate binders, oralcalcium supplements, high dialysate calcium, andmore frequent dialysis with deionized water. Com-

la-OH-D3 and 25-OH-D3 in renal osteodystrophy 197
plete reversal of the histologic lesions of osteitisfibrosa or osteomalacia, or both, has rarely beenachieved, however [2—4]. Therefore, administrationof vitamin D has been used in combination with theabove measures. Variable results have been report-ed either with parent vitamin D [5-7] and its hepaticmetabolite 25-hydroxycholecalciferol (25-OH-D3)[4, 8—101, or with its hormonal metabolite la,25-hy-droxycholecalciferol (la,25(OH)2-D3) [11—15], or itsanalogue, 1 a-hydroxycholecalciferol (1c-OH-D3)[16—24]. Surprisingly, the effect of la,25(OH)2D3and of la-OH-D3 on renal osteomalacia has notbeen consistently seen even with long-term studies,whereas reduction of increased levels of plasma im-munoreactive parathyroid hormone (iPTH) and re-versal of osteitis fibrosa have been usual exceptin cases of autonomous hyperparathyroidism [14,23, 24]. This lack of effect of la,25(OH)2D3 in somecases of renal osteomalacia unrelated to phosphatedepletion [14], together with some observations ofnormal osteoid volume and mineralization front inanephric patients [3], with complete absence ofla,25(OH)2D3 [25, 26], suggests that la,25(OH)2D3may not be the metabolite solely responsible formineralization of the osteoid tissue. This hypothesisis further supported by the recent study of Bordieret a! [27] on the comparative effectiveness of 25-OH-D3, la,25(OH)2D3, and 24, 25(OH)2D3 in adultvitamin-D-deficient man. This study showed that25-OH-D3 in large doses was more effective thanwere its two metabolites in remineralizing osteoidtissue and that only a combined treatment ofla,25(OH)2D3 and 24, 25(OH)2D3 led to the returnof the mineralization front to normal. This led us tocompare treatment of renal osteomalacia with largedoses of 25-OH-D3 or with "physiologic" doses ofla-OH-D3.
Methods
la-OH-D3 protocol. Four uremic patients onchronic hemodialysis (age range, 27 to 50 years)were given 4 jsg of 1a-OH-D at each dialysis, threetimes per week, during 8 to 9 weeks. In one of thesepatients, la-OH-D3 was given again, after 2 monthsof discontinuation, at each dialysis at a dosage of 4pg for 2 months and then at 2 sg for 5 months.Aluminum hydroxide was given at a constant dos-age of 3 to 9 glday throughout the study.
25-OH-D3 protocol. 25-OH-D3 was given to sixuremic patients on chronic hemodialysis (age range,28 to 56 years). Five of them received 200 g ateach dialysis, three times per week, for 1 to 4months. The last patient received only 100 jig of 25-
OH-D3 at each dialysis, three times a week, for 6months. Aluminum hydroxide was given at a con-stant dose of 0 to 6 g/day throughout the study. Acombination of 1a-OH-D and 25-OH-D3 was givento the patient who previously had received la-OH-D3 for 9 months. At each dialysis, he at first re-ceived 2 jig of la-OH-D3 and 100 jig of 25-OH-D3for 1 month, and then he received 1 jig of la-OH-D3and 50 jig of 25-OH-D3 for 5 months.
Dialysis technique and other therapeutic mea-sures. The patients were dialyzed for 6 hours, threetimes a week, with a 1-rn2 cuprophane dialyzer anda dialysate containing 7.0 mg/dl of calcium and 1.9mg/dl of magnesium after preparation with softenedwater. The diet of each patient had approximately80 g of protein, 1.2 g of phosphorus, and I g of cal-cium. No patient received previously vitamin D ororal calcium supplement. None of the patients wereon anticonvulsant therapy.
Blood samples were taken before the first dialysisof the week throughout the vitamin-D therapy andalso 1 month before and after. Plasma calcium (Pca)and phosphate (P04) were measured by autoanalyz-er. Plasma iPTH (P1) was determined every 2weeks with a modification of the method of ArnaudTsao, and Littledike [28, 29] and with the GP1 Mantibody, which recognizes the C terminal region ofthe molecule. It is expressed in nanograms of pro-tein of parathyroid adenoma culture medium permilliliter (normal range, 4 to 8 ng). All samples ofeach patient were measured at the end of the studyin the same assay. The intraassay variability was6%, and that of the interassay was 14%.
Plasma levels of 25-OH-D were measured in thefour patients before their treatment with la-OH-D3and in four out of the six patients before and at theend of their 25-OH-D3 treatment. The competitiveprotein-binding assay of Ferriere, Gueris, and Mi-ravet [30], derived from that of Belsey, DeLuca,and Potts, Jr. [31] was used. This assay recog-nizes not only 25-OH-D3 but also 25-OH-D2 and24, 25(OH)2D [32]. The normal mean SD is 14.34.2 nglml.
Transilial bone biopsies were performed as pre-viously described [33] in all patients, with their in-formed consent, the first one before treatment andthe other at the end of the ito 6 months of therapy.In one patient, four bone biopsies were taken: thefirst one before la-OH-D3, the second one after 2months of la-OH-D3, the third one after 9 monthsof la-OH-D3, the fourth after 6 months of a combi-nation of la-OH-D3 and 25-OH-D3. Serial undecal-cified sections, 5- to 6-ji thick, were obtained and

198 Fournier et al
Table 1. Comparison of the initial status of the two groups4
Differencela-OH-D3 (N = 4) 25-OH-D.3 (N = 6) (Wilcoxon)
Dialysis duration, months 7 to 24 1 to 15 NSAnephric state incidence 1 2 NSDurationof anephric state, months 12 6 to 11 NSClinical or radiologic symptoms 0 0 NSAluminum hydroxide, g/day 3 to 9 0 to 6 NSPca, mg/lOOml 8.6 to 10.1 8.8 to 10.2 NSPpo,mg/l00ml 3.5 to 6.5 4.0 to 6.1 NSPiPTH, ng/ml 33 to 46 23 to 144 NSSerum Alk. Pase, King Armstrong U 6 to 45 6 to 16 NSP250HD, nglml 1.8 to 10.8 1.3 to 42.0 NSOsteoblastic surface,
%total cancellous bone surface 5.7 to 21.0 4.1 to 15.6 NSOsteoid volume,
%total cancellous bone tissue 5.8 to 26.3 3.7 to 15.0 NSOsteoid surface,
% total cancellous bone surface 15 to 57 11 to 70 NSMineralization front,
%total osteoid surface 14 to 33 10.7 to 21.9 NSOsteoclast count per mm2 0.6 to 1.4 0.08 to 0.96 0.05Osteoclastic resorption surface,
% total cancellous bone surface 1.2 to 2.7 0.4 to 2.4 NS
Abbreviations used are: P, plasma concentration of; Ca, calcium; P04, phosphate; iPTH, immunoreactive parathyroid hormone; 25-OH-D, 25-hydroxycholecalciferol; 5, serum concentration of; Alk. Pase, alkaline phosphatase.
stained with Toluidine blue. The following parame-ters were measured (normal means SD are givenin parentheses): osteoclast count, expressed innumber per square millimeter of bone section (0.37
0.07 mm2); osteoclastic resorption surface, ex-pressed in percent of total cancellous bone surface(0.48 0.2%); osteoblastic surface, that is, theosteoid surface covered with an active osteoblastlayer, expressed in percent of the total cancellousbone surface (4.9 1.4%); osteoid volume, ex-pressed in percent of the volume of cancellous bonetissue (4.1 1.0%); osteoid surface, expressed inpercent of the total cancellous bone surface (14.83.0%); mineralization front labeled by methylchlor-tetracycline, expressed in percent of the osteoidsurface (63.3 4.5%). The methylchlortetracyclinewas given 2 days before the biopsy was performed.Each measurement was made on ten sections ran-domly chosen from the core of the biopsy speci-men, and a mean value was obtained, with the intra-biopsy variation expressed as the SEM. This permit-ted individual assessment of the significance of thechanges obtained during the course of treatment.
Statistical methods. Comparison of groups wasmade using the nonparametric test of Wilcoxon fornonpaired data. The theoretical advantage of theWilcoxon test is that it does not imply a normal dis-
tribution as does Student's t test. Therefore, whenit is used, range of values and not means have beentabulated [34]. Comparison of paired data was madewith Student's paired t test, because the paired Wil-coxon test requires at least six paired data, and thisnumber was not reached in the la-OH-D3 group.The regression calculations were made using a pro-grammed computer.
Results
Comparison of the initial status of the two thera-peutic groups. Table 1 shows that there was no sig-nificant difference between the two groups initiallyas regards the dialysis duration, the incidence andduration of the anephric state, the clinical or radio-logic symptoms, the dose of aluminum hydroxide,Pca, P04, PiPTH, and PZ0H..D, the serum alkalinephosphatase (SAlk. Pase), osteoblastic surface, osteoidvolume, osteoid surface, and mineralization front.The mineralization front was below the lower limitof normal (<50%) in all cases, whereas the osteoidvolume was above upper limit of normal (9%) in twoout of the three patients of the la-OH-D3 group andin four out of the six patients treated with 25-OH-D3. Thus, both groups were comparable as regardsthe severity of osteomalacia and their vitamin-Dstatus. In spite of comparable PIPTH levels, the

1 a-OH-D,3 and 25-O1I-D3 in renal osteodystrophy 199
Table 2. Comparison of the biological effects of the two vitamin D sterolsa
osteoclast count was higher (P = 0.05) in the liz-OH-D3 group, but no significant difference wasfound in the active resorption surface.
Treatment duration. The duration of treatmentwas comparable: from 2 to 9 months in the la-OH-D3-treated group and 1 to 6 months in the 25-OH-D3-treated group. Although no plasma concentration of1 ,25(OH)2D3 was available to assess the complianceof the patients to the la-OH-D3 administration,measurements of P25_OHD showed that 25-OH-D3was effectively taken since the concentrations in-creased from an initial range of 1.3 to 42.0 ng/mlto 25 to 302 ng/ml.
Comparison of the biochemical and histologic ef-fects of Icx-OH-D3 with those of 25-OH-D3. Table 2describes the range and significance of the changesproduced by the two vitamin D compounds. It alsoillustrates the significance of the difference in theresponses induced by the two sterols. Both com-pounds equally increased PCa. With 1aOHD3, Pp04increased in three patients (that is, in four therapeu-tic periods) and decreased in one patient, whereaswith 25-OH-D3 it increased in three patients and de-creased in three. The difference between the twogroups as regards the hyperphosphatemic effectwas not significant. The Pca x P04 product was in-creased more with lct-OH-D3 than it was with25-OH-D3 (P = 0.05). PIPTH was decreased equally(—9% to —70%) with the treatments, but remainedabove normal in all patients. With la-OH-D3,
SAlk. Pase decreased in three patients and increasedin two, whereas with 25-OH-D3 it increased in fourpatients and decreased in one. The difference in re-sponse of alkaline phosphatase to the two com-pounds was significant (P < 0.05).
Osteoblastic surface showed changes parallel tothose of SALk. Pase with la-OH-D3, it decreased inthree patients and did not change in two. With25-OH-D3, osteoblastic surface increased signifi-cantly in four patients, decreased in one patient,and did not change in another one. The differencebetween the two treatments was significant (P <0.05).
Osteoid volume did not change significantly in ei-ther of the two groups. When individual patientstreated with Ia-OH-D3 were considered, osteoidvolume (which for technical reason was not eval-uated in one patient), decreased in two patients andthree therapeutic periods, but did not change in an-other one with a normal initial value. With 25-OH-D3, osteoid volume decreased in three patients, didnot change in two others, and increased in anotherone, so that after treatment it remained elevated intwo patients. No significant difference between thetwo groups was observed. Similarly, osteoid sur-face did not change significantly with either drug.
Mineralization front increased significantly in twopatients but did not change in two therapeutic peri-ods of 2 months with la-OH-D3. Therapy with lct-OH-D3 for 7 additional months in one patient did
Changes with la-OH-D3 (N = 5)b Changes with 25-OH-D (N = 6)' Difference1-OH-D vs. 25-OH-D
(P, nonpairedSignificancec SignificanceRange (paired test) Range (paired test) Wilcoxon test)
P,mg/100ml + 0.5 to + 1.8 <0.05(7) + 0.2 to + 1.7 <0.05(7) NSPpo, mg/lOOm! — 1.3 to + 2.5 NS(47,1\) — 1.5 to + 2.2 NS(3/,3\) NSPca X P0 — 4.2 to + 28.7 <0.05(7) —12.8 to 20.2 NS(37,3\) 0.05PIpTH,%ofcontrolvalue — 9 to — 70 <0.05(\) —23 to — 70 <0.05(\) NSAlk. Pase,KingAr,nstrong U —30 to + 5 NS(3\,27) —13 to + 16 <0.05(7) <0.05Osteoblastic surface,
%cancellous bone surface —11.5 to + 0.5 NS(3\,2) — 5.1 to + 9.8 <0.05(7) <0.05Osteoid volume,
% total cancellous bone tissue —13 to + 1.1 N5(3\ ,1s-) — 8.2 to 7 NS(3\ ,2, I \) NSOsteoid surface,
%totalcancel!ousbonesurface 11 to + 4 NS(3\,2-*) — 6 to + 6 NS(5-,17) NSMineralization front,
%osteoid surface 0 to + 7 <0.05(27.3*) + 9 to + 22 <0.05(67) <0.05Osteoclast count per mm2 —11 to + 0.2 NS(4\,1) — 0.5 to + 0.5 NS(2\,3-*,17) NSOsteoclastic resorption — 1.8 to + 0.4 NS(3\,2-) — 1 to + 0.6 NS(2\,3,17) NS
See Table 1 for abbreviations used.One patient is considered with two therapeutic periods.Group or individual variations are given in parentheses: 7, increase; \, decrease; -*, no change.

200 Fournier et a!
not induce any increase in mineralization front (Fig.1). With 25-OH-D3, mineralization front increasedsignificantly in the six patients, so that the increasewith 25-OH-D3 was significantly greater than it waswith la-OH-D3. This greater effect is further illus-trated by the significant increase of mineralizationfront from 34% to 44.6% observed in the patient ofFig. 1, 6 months after addition of 25-OH-D3 at lowdosages (50 cg and then 25 tg/day), whereas icr-OH-D3 was decreased to 1 cg and then to 0.5 jig!day. This increase in mineralization front was asso-ciated with a small decrease of the calcium phos-phate product from 54.4 to 51.5.
Osteoclast count did not change significantly, ei-ther with la-OH-D3 or with 25-OH-D3. When thepatients treated with lcr-OH-D3 were considered in-
60 dividually, osteoclast count, which was initially elevated in the four patients, decreased in three pa
5.0 tients (that is, after four therapeutic periods) ant00, .
did not change in one patient. With 25-OH-D34.0 osteoclast count decreased in two patients with mi
tial increased surface, did not change in three pa
0tients with initial normal count, and increased itone patient with initial normal count. The differenct
40 between the two groups was not significant.Osteoclastic resorption surface did not chang
significantly either with la-OH-D3 or with 25-OH60 D3. When the individual patients were considered
osteoclastic resorption surface, which was initiall340 ci increased in all four patients treated with la-OH-D:
decreased in two patients (that is, after three thera20 peutic periods) and did not change in two others, s20 that after treatment, it remained elevated in two pa10 tients. With 25-OH-D3, it decreased in two patient
k with initial increased surface, did not change itOtt
0 three others with initial normal surface, and increased in another one with initial normal surfaceThe difference between the two groups was not significant.
• 25-OH-03 A lca-OH--D3
Patient 4 with lca-OH-D3o Patient 4 with addition of 25-OH-D3 to la-OH-D3
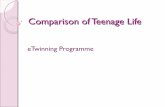
Fig. 2. Regression of the changes in calcifi cation front versus thchanges in PCA x Patients treated with la-OH-D3 are denoted by triangles (A), and patients treated with 25-OH-D3, bcircles (S). A horizontal line was drawn at 8% of calcificatiorfront increase to show that all patients treated with 25-OH-D3 artabove this line, whereas all patients treated with 1cs-OH-D artbelow it. N = 12 refers to ten patients, one patient being considered three times: twice while on lis-OH-D3 alone ® and onctwhen 25-OH-Da was added to lu-OH-D3 0
8.0
500
4000
30
20ci
> 1000 40
200
///LIJJJJJ4/LI-I.I1'1'-I-o-[! 111_I
'I \ \ \\ \\\ \\\ \\ \ ' \ S S \S \ \ .0..
040 r
0,0=F-a- \\x
2.0E
1.0U0a,
UU- —-- cr
Before After 2 mo. After 9 mo. After addition oflo-OH-D3 lo-OH-D lo-OHD3 25-OHD3 X 6 mo.
(2 pg/day (2 pg-i pg/day) (100-50 pg/day)
Fig. 1. Variations of the different biochemical and histomorpho-metric parameters in the patient who was evaluated once beforeany treatment, twice while on Ici-OH-D3 alone (after 2 and 9months), and again after 6 additional months of a combinationof lu-OH-D3 and 25-OH-D3. The hatched area represents thelimits of normal for the parameters indicated along the verticalaxis, on which the hatched area is connected. The closed circlesrepresent the parameters of the left vertical axis (Pca), and theopen circles represent the parameters of the right vertical axis.
25
a, •
20 10 10 20 3C
Pc X Pp4
r = —0.63N = 12P < 0.05

I ca-OH-D3 and 25-OH-D3 in renal osteodystrophy 201
Regression studies. Changes in PIPTH showed nosignificant correlation to PCa changes nor to changesof P04 in either group. A significant positive corre-lation was observed between the changes in PIPTHand those observed in osteoclast count (r = +0.88,N = 5, P < 0.05) or in the osteoclastic resorptionsurface (r = 0.80, N = 5, P = 0.05) in the la-OH-D3-treated group but not in the group treated with25-OH-D3. No significant correlation was found be-tween the changes of the mineralization front andthe changes of the calcium phosphate product whenthe two groups were considered separately, but asignificant negative one was found when the groupswere considered together (r = —0.63, N = 12, P <0.05) (Fig. 2). This latter figure shows furthermorethat all patients treated with 25-OH-D3 have an in-crease in their mineralization front greater than 8%,whereas those treated with la-OH-D3 have an in-crease in their mineralization front smaller than 8%.On the other hand, the PCa X P04 product increaseis greater than 20 in all patients treated with la-OH-D3 except one and is equal or below 20 in all pa-tients treated with 25-OH-D3.
Longitudinal survey of the hypercalcemic effect.Figure 3 shows the mean weekly variations Of Pca inthe patients receiving 2 tg/day of la-OH-D3 or 100gIday of 25-OH-D3. After starting the treatment, asignificant increase was noted (greater than 2 SEM ofpretreatment values) after 2 weeks with la-OH-D3and 8 weeks with 25-OH-D3. When the drug wasdiscontinued, mean PCa returned to pretreatmentlevels within a week with la-OH-D3, but not before4 weeks with 25-OH-D3. In the patient taking 50 .tgof 25-OH-D3 daily, PCa increased significantly onlyafter 2 months, and no hypercalcemia was observedafter 6 months. In the patient treated for 9 monthswith la-OH-D3, the initial dosage of 2 pg/day had tobe reduced by half after 4 months of treatment toprevent recurrence of hypercalcemia.
Discussion
The available results indicate that at the dosagesused both vitamin D compounds are equally ca-pable of raising serum calcium, even in anephric pa-tients. la-OH-D3 appears 50 times as effective as25-OH-D3 in this regard. Moreover, this calcemiceffect develops more quickly with la-OH-D3 than itdoes with 25-OH-D3, and following cessation oftreatment, hypercalcemia regresses much earlier inthe lct-OH-D3-treated group. The hypercalcemic ef-fect of both these vitamin D sterols is of shorter du-ration than it is with either vitamin D2 or D3, amarked therapeutic advantage.
Drug administration Drug discontinuationweeks weeks
0 2 4 8 12 16 240 —2 —4 —6 —8
1c-OH-D3
rIW
Evaluation of the effect of vitamin D on P04 inpatients on chronic hemodialysis can be difficult be-cause predialysis Pp04 mainly depend on diet andpatient's adherence to the prescribed aluminum hy-droxide therapy. Furthermore, phosphate removalby dialysis is mainly dependent on dialysis durationand frequency. Therefore, to compare the effect ofthe two vitamin D sterols on predialysis P04, weselected the patients for whom dialysis durationwas kept constant and for whom the dosage of theprescribed aluminum hydroxide was not changed.In these conditions, it appears that lct-OH-D3 tend-ed to have a greater hyperphosphatemic effect than25-OH-D3 did, although the difference was not sta-tistically significant. The PCa x P04 product showeda greater increase with la-OH-D3 than it did with25-OH-D3.
The two treatments were equally effective in re-ducing P!PTH. A significant positive correlation be-tween the changes of PIpTU and those of osteoclastcount or active resorption surface was observed on-ly in the la-OH-D3 group. This difference, how-ever, does not permit the conclusion that la-OH-D3would be more appropriate than 25-OH-D3 wouldbe to treat osteitis fibrosa, as the lack of correlationfound in the 25-OH-D3-treated group may be ex-plained by the fact that the initial values of osteo-clast count and osteoclastic resorption surface werein the normal range in four out of six patients in thisgroup.
- 11.0
:: 10.0 _______________________ ___________________
9.0 A/N 8.0
25-OH-D311.0
Co
1100 *AMA/8.0
Fig. 3. Effect of lcs-OH-D3 and 25-OH-D3 on plasma calcium(P4). Mean Pca with la-OH-D3 at 2 p.glday is represented byclosed triangle (A). Mean Pa with 25-OH-D at 100 1sglday isrepresented by closed circle (. Pca of the patient treated with50 g/day is represented by open circle (0). The hatched areasrepresents the mean 2 SEM of the control values.

202 Fournier et at
Osteoblastic surface and SAlk Pase increased with25-OH-D.1 and decreased with lcx-OH-D3. In nutri-tional osteomalacia, this initial increase of theosteoblastic surface was also observed with 25-OH-D3 but not with la,25(OH)2D3, la-OH-D3, nor with24,25(OH)2D3. This led to the suggestion that 25-OH-D3 itself could stimulate the osteoblasts eitherdirectly or indirectly through the increase of P04 in-duced by 25-OH-D3 in vitamin-D-deficient nonure-mic man [271. Since, in our patients, the increase intheir osteoblastic surface was observed without in-crease in P04, we suggest that 25-OH-D3 may havea direct stimulating effect on the osteoblasts. Thisincrease in the osteoblastic surface and SAlk Pasewith 25-OH-Da seems transient, however, since it isnot observed in the patient treated for 6 monthswith 25-OH-D3 alone nor in the patient of Fig. 1, 6months after addition of 25-OH-D3.
Mineralization of the osteoid tissue, as assessedby the increase in the mineralization front, appearsto be more effectively produced by 25-OH-D3 thanit is by la-OH-D3, whereas the concomitant in-crease in the Pca x P04 product is smaller. Thisgreater effect of 25-OH-D3 on the mineralizationfront cannot be explained by a longer duration oftreatment or by initial lower values of the mineral-ization front or by initial lower values of P25_OH_D.The greater effect of 25-OH--D3 on mineralization canneither be explained by smaller phosphate depletionnor by smaller aluminum intoxication. These lastfactors have been pointed out because lack of re-sponsiveness of osteomalacia to la,25-OH-D3 orla-OH-D3 has been attributed to phosphate deple-tion [23] and to intoxication by aluminum in the wa-ter used for the dialysate preparation [35], or toboth. In our patients, the initial P04 was com-parable in both groups, and the exposure to alumi-num was also comparable since all were dialyzedwith the same source of softened water and weretaking comparable amounts of aluminum hydrox-ide. The greater effect of 25-OH-D itself in increas-ing the mineralization front is furthermore illus-trated by the patient of Fig. 1, whose mineralizationfront did not change after 9 months of la-OH-Da butincreased by 30% when small doses of 25-OH-Dawere added. This greater effect of 25-OH-D3 com-parative to la-OH-D3, in mineralizing bone, hasbeen observed also in nutritional osteomalacia byBordier et al [27] but was associated with a greaterincrease in P04 because of a greater and a more sus-tained reabsorption of phosphate by the kidneys.The increase of P04 was not, however, the wholeexplanation of the cure of nutritional osteomalacia,
since increasing P04 by phosphate administrationalone, without vitamin D, did not increase the min-eralization front. A direct action of vitamin D onbone was therefore implied with a greater efficiencyfor 25-OH-D3. Our data support this hypothesis,since we found a negative correlation between thechanges in the mineralization front and the changesof Pca x P04 product. These findings and similarones reported by Eastwood et al [36] suggest thatvitamin D increases the mineralization front not pri-marily by increasing the PCa X P04 product but by adirect action on the bone. Since deposition of cal-cium and phosphate in the bone should lead to adecrease in the PCa x P04 product, this explainswhy the greater the mineralization front, the lowerthe PCa x P04 product and why 25-OH-D3 increasesless PCa X P04 product than it does la-OH-D3. As amatter of fact, the smaller increase of PCa X Pp04product with 25-OH-D3 cannot be explained by agreater suppression of osteoclastic resorption norby a smaller increase of renal tubular reabsorptionof calcium and phosphate, which may be presumedto be negligible in end-stage renal failure. A smallerincrease of calcium and phosphate intestinal ab-sorption is another possibility, but no data are avail-able to support it.
The fact that la,25(OH)2D3 is the metabolite intowhich la-OH-D3 is transformed before any meta-bolic effect can be observed [371 and that la-OH-D3is less effective than 25-OH-D3 is in increasing themineralization front, in spite of a greater increase inPCa x product, suggests that la,25(OH)2D3may not be the specific metabolite for bone mineral-ization. It can be argued, however, that because ofthe short half-life of la,25(OH)2D3 (less than 24hours according to Holick et a! [37]), administrationof 4 g of la-OH-D3 3 times per week would notreproduce the physiologic variations of plasmala,25(OH)D3 which is secreted at low but constantrate, whereas pharmacologic dosages of 25-OH-D3would induce, at least in nonanephric men, plasmalevels of lc,25(OH)2D3 that are closer to physiologicones because of its longer half life (12 days accord-ing to Hadad [38]). If this hypothesis is acceptedand our data is considered, that would imply thatla,25(OH)2D3 would promote bone mineralizationat plasma levels different from those which increaseintestinal absorption. Another possibility is that the25-OH-D3 at the dosage used acts directly withoutconversion to la,25(OH)2D3. This is supported bythe calcemic effect in anephric man. It is possiblethat at low dosages, la-OH-D3 does not reach thebone site, whereas 25-OH-D3 at large dosages

/ c-OH-D3 and 25-OH-D3 in renal osteodystrophy 203
would, thus producing the increased mineralizationfront. Thus, a conclusion that 25-OH-D3, at physio-logic dosages, is more efficient at inducing mineral-ization front cannot be made, but it does demon-strate that whatever the mechanism, large dosagesof 25-OH-D3 may be therapeutically superior tosmall dosages of la-OH-D3 in mineralizing bone.
Acknowledgments
This study was supported by the INSERM "Con-trat libre n°76.l20.75." We acknowledge the nurs-ing staff of the hemodialysis unit, who collected theblood samples, Mrs. Jacqueline Fournier, whotyped the manuscript, and Dr. A. Pierides, whogave editorial help.
Reprint requests to Dr. A. Fournier, Centre Hospitalier Re-gional d'Amiens, Service de Nephrologie, Amiens, 8000 France
References
I. FOURNIER AE, ARNAUD CD. JOHNSON WJ, TAYLOR WF,GOLDSMITH RS: Etiology of hyperparathyroidism and bonedisease during chronic hemodialysis: II. Factors affectingserum immunoreactive parathyroid hormone. J C/in Invest50:599.605, 1971
2. JOHNSON WJ, GOLDSMITH RS, BEABOUT JW, JOWSEY J,KELLY PJ, ARNAUD CD: Prevention and reversal of progres-sive secondary hyperparathyroidism in patients maintainedby hemodialysis. Am J Med 56:827-832, 1974
3. BORDIER PJ, TUN CHOT S, EASTWOOD JB, FOURNIER AE.DE WARDENER HE: Lack of histological evidence of vitaminD abnormality in the bones of anephric patients. C/in Sci
44:33—41, 1973
4. BORDIER P1, MARIE PJ, ARNAUD CD: Evolution of renalosteodystrophy: correlation of bone histomorphometry andserum mineral and immunoreactive parathyroid hormonevalues before and after treatment with calcium carbonate or25 OH calciferol. Kidney mt 7 (suppl 2):S102—S112, 1975
S. HILL LF, STANBURY SW: Vitamin D and the kidney. Neph-ron 15:369—386, 1975
6. BOUILLON R, VERBERCKMOES R. DE MOOR P: Influence ofdialyzate calcium concentration and vitamin D on serumparathyroid hormone during repetitive dialysis. Kidney mt7:422—432, 1975
7. COUNTS Si, BAYLINK DJ, SHEN FH, SHERRARD DJ, HICK-MAN RO: Vitamin D intoxication in an anephric child. AnnIntern Med 82:196—200, 1975
8. RUTHERFORD WE, BLONDIN J, HRUSKA K, KOPELMAN R,KLAHR 5, SLATOPOLSKY E: Effect of 25 hydroxy-cholecalciferol on calcium absorption in chronic renal dis-ease. Kidney in! 8:320—324. 1975
9. TEITELBAUM SI., BONE M, STEIN PM, GILDEN JJ, BATESM, BOISSEAU VC, AvI0IJ LV: Calcifediol in chronic renalinsufficiency: Skeletal response. JAMA 235:164—167, 1976
10. WITMER G, MARGOLIS A, FONTAINE 0, FRITSC'H J, LENOIRG. BROYER M, BALSAN S: Effects of 25 hydroxy-cholecalciferol on bone lesions of children with terminal re-nal failure. Kidney In! 10:396—408, 1976
11. BRICKMAN AS, SHERRARD Di. JOWSEYJ. MASSRY SG, NOR-MAN AW, COBURN JW: 1a,25 dihydroxycholecalciferol: ef-
fect on skeletal lesions and plasma parathyroid hormone lev-els in uremic osteodystrophy. Arch intern Med 134:883—888,1974
12. PIERIDES AM, WARD MK, ALVARES-UDE F, ELLIS HA,PEART EM, SIMPSON W, KERR DNS, NORMAN AW: Longterm therapy with l,25(OH)2D3 in dialysis bone disease.Proc EDTA 12:237—243, 1976
13. HENDERSON RG, RUSSEL RG, LEDINGHAM DG. SMITH R,OLIVER DO, WALTON Ri, SMALL DG, PRESTON C, WARNERGT, NORMAN AW: Effects of la,25(OH)2D on calcium ab-sorption, muscles weakness and bone disease in chronic re-nal failure. Lancet 1:379—384, 1974
14. COBURN 1W, BRICKMAN AS, SHERRARD Di. SINGER FR,WONG EGG, BAYLINK Di, NORMAN AW: Use ofla,25(OH)2 vitamin D3 to separate types of renal osteo-dystrophy. Proc EDTA 14:442—450, 1977
15. AHMED KY, WILLS MR, VARGHESE Z. MEINHARDE A,MOORHEAD iF: The long term effects of small doses of la,25dihydroxycholecalciferol in renal osteodystrophy. Lancet1:629, 1978
16. CHALMERS TM, DAVIE MV, HUNTER JO, SZAZK F, PELC B,KODICECK E: 1-alpha-hydroxycholecalciferol as a substitutefor the kidney hormone lu,25 dihydroxycholecalciferol inchronic renal failure. Lance! 2:696—699, 1973
17. BORDIER P. ZINGRAFF J, GUERIS J, JUNGERS P. MARIE P,PECHET M, RASMUSSEN M: The effect of la(OH)D3 and1cs,25(OH)2D on the bone in patients with renal osteo-dystrophy. Am J Med 64:101—107, 1978
18. CATTO GRD, MACLEOD M: The investigation and treatmentof renal bone disease. Am J Med 61:61—73, 1976
19. TOUGAARD DL, SORENSEN F, BROCHNER-MORTENSEN J,CHRISTENSEN MS. RODBRO P. SORENSEN AWS: Controlledtrial of 1 alpha OH D in chronic renal failure. Lancet1:1044-1047, 1976
20. PORS NILSEN S. BINDERUP E, GODTFREDSEN WO, JENSENH, LADEFOGED J: lu hydroxycholecalciferol: long termtreatment of patients with uremic osteodystrophy. Nephron16:359—370, 1976
21. MADSEN 5, OLGAARD K: l-alpha-Hydroxycholecalciferoltreatment of adults with chronic renal failure. Acta MedScand 200:1-5, 1976
22. DAVIE MWJ, CHALMERS TM, HUNTER JO, PELC B, Kool-CEK K: 1-alpha-Hydroxycholecalciferol in chronic renal fail-ure: studies of the effect of oral doses. Ann Intern Med
84:281—285, 197623. PIERIDES AM, SIMPSON W, WARD MK, ELLIS HA, DEWAR
JH, KERR DNS: Variable response to long term I alpha-hydroxycholecalciferol in hemodialysis osteodystrophy.Lancet 1:1092—1095, 1976
24. KANIS JA, ADAMS ND, EARNSI-IAW H, HEYNEN G, LEDING-I-lAM JG, OLIVER DO, RUSSEL RGG, WOODS CG: VitaminD, osteomalacia and chronic renal failure, in Vitamin D Bio-chemical, Chemical, and Clinical Aspects Related to Ca/-
cia/n Metabolism, edited by NORMAN AW. SCHAEFFER K,COBURN JW, Di LUCA HF, De Gruyter, Berlin, New York,1977, pp. 67 1—673
25. DE LUCA HF: Vitamin D metabolism. C/in Endocrinol(suppl 7):15—l7, 1977
26. HAUSSLER MR. MCCAIN TA: Basic and clinical concepts re-lated to vitamin D metabolism and action. N EngI J Med297:974—983; 1041—1050, 1977
27. BORDIER P. RASMUSSEN H, MARIE P. MIRAVET L, GUERISJ, RYCKEWAERT A: Vitamin D metabolites and bone miner-alization in man. J C/in Endocrinol Metab 46:284—294, 1978

204 Fournier et a!
28. GuERIs J, FERRIERE C: Heterogeneite de Ia parathormoneplasmatique chez l'homme. Pathol Biol 23:821—826, 1975
29. ARNAUD CD, TSAO HS, LITTLEDIKE T: Radio-immunoassayof human parathyroid hormone in serum. J Clin Invest50:21—34, 1971
30. FERRIERE CH, GUERIS J, MIRA VET L: Le dosage par radio-competition du 25 hydroxycholecalciferol. Nelle Presse Med4:2472, 1975
31. BELSEY R, DE LUCA HF, POTTS iT Jit: Competitive bindingassay for vitamin D and 25 hydroxyvitamin D. J Clin Endo-crinol Metab 33:172—175, 1971
32. HADDAD JG, MIN C, WALGATEJ, HAHN T: Competition by24,25 dihydroxycholecalcilerol in the competitive proteinbinding radio-assay of 25 hydroxycholecalciferol. J ClinEndocrinol Metab 43:712—715, 1976
33. BORDIER PJ, TuN CI-IOT S: Quantitative histology of meta-bolic bone disease. Clin Endocrinol Metab 1:197—215,1972
34. FERMANIAN J, SALMON D: Mathématiques: Statistiques.Armand-Colin Ed., Paris, 1974
35. WARD MK, ELLIS HA, FEEST TG, PARKINSON IS, KERRDNS, HERRINGTON J, GOODE GL: Osteomalacia dialysisosteodystrophy: Evidence for a water borne aetiologicalagent, probably aluminum. Lance: 1:841-845, 1978
36. EASTW000 JB, BORDIER Pi, CLARKSON EM, TUN CHOT S,DE WARDENER HE: The contrasting effects on bone histolo-gy of vitamin D and of calcium carbonate in the osteomalaciaof chronic renal failure. C/in Sci Mol Med 47:23—42, 1974
37. HOLICK MF, DE BLANCO M, CLARK MB, HENLEY JW,NEER RM, DE LUCA HF, POTTS JT: The metabolism of [6-3H]-laOH cholecalciferol to [6-Hj-1a,25 dihydroxychole-calciferol in a patient with renal insufficiency. J C/in Endo-cr/no! Metab 44:595—598, 1977
38. HADDAD JG, ROJANASATHIT S: Acute administration of 25OH cholecalciferol in man. J C/in Endocrinol Metab 42:284—290, 1975