Chronic Total Occlusions Antegrade Approach...CTO Revascularization Evidence Considerations from a...
42
Chronic Total Occlusions Sceptical Considerations and Technical Approach Α-Δ. ΜΑΥΡΟΓΙΑΝΝΗ ΚΑΡΔΙΟΛΟΓΟΣ AIMOΔΥΝΑΜIΚΟ ΕΡΓΑΣΤΗΡΙΟ Γ.Ν.Θ. «Γ.ΠΑΠΑΝΙΚΟΛΑΟΥ» ΘΕΣΣΑΛΟΝΙΚΗ
Transcript of Chronic Total Occlusions Antegrade Approach...CTO Revascularization Evidence Considerations from a...

Chronic Total Occlusions Sceptical Considerations and Technical Approach
Α-Δ. ΜΑΥΡΟΓΙΑΝΝΗΚΑΡΔΙΟΛΟΓΟΣ
AIMOΔΥΝΑΜIΚΟ ΕΡΓΑΣΤΗΡΙΟΓ.Ν.Θ. «Γ.ΠΑΠΑΝΙΚΟΛΑΟΥ»
ΘΕΣΣΑΛΟΝΙΚΗ

Disclosure Statement of Financial Interest
none whatsoever…

The Late Open Artery Hypothesis: Rationale and Dilemmas of CTO PCI
• Reduction in ischemic burden
• Enable completeness of revascularization
• Improvement of symptoms
• Improvement in LV function
• Reduced predisposition to arrhythmic
events and ischemic events
• Avoidance of procedures and reduced
medications
• Survival benefit
• Technical and procedural challenges
• Misperceptions regarding viability,
collateral flow
• Uncertainty regarding which patients may
benefit balanced by
• Concern for complications in patients who
may not derive clinical benefit
Disclaimer: Capability to perform CTO PCI imparts clinical wisdom to decide when it is and is not indicated

CTO Revascularization Evidence Considerations From A Patient Perspective
In what Clinical Settings might CTO PCI Improve my Outcome?
Objective In Favor Against
Symptom Improvement 7 trials (1 RCT,6 single-arm)
demonstrating benefit relative to
procedural failure or medical therapy
alone and comparable to non-CTO PCI
1 RCT showing no symptom benefit or
reduction in medicines
Event Free Survival 16 observational studies (~32,500 pts)
reporting improved survival;
4-5 yr TLR 9%
1 RCT showing no difference in MACCE
compared with medical therapy
Improvement in LV Function Meta-analysis of 34 studies and at least
9 additional studies demonstrate
improvement in LV function and/or LV
dimensions
Outcome may depend on viability and
extent of baseline impairment;
EXPLORE RCT no difference; REVASC
no difference in regional or global LV
function but improved MACE
Other Avoidance of need for CABG (>80%);
Reduction in ventricular arrhythmic
events (VACTO)
Limited alternative evidence

CTO Revascularization Evidence: Evolution of CTO PCI - What is Known
• Several observational studies: improved
survival with CTO PCI
• Improvement in LV function: suggestive
but inconsistent
• Most but not all CTO trials examining
health status have associated a benefit
with CTO PCI
• Debate exists regarding what evidence,
trial design and endpoints and study
conduct needed to advance CTO PCI
CTO revascularization remains uncommon in the interventional community despite its prevalence in ~20% of patients with coronary
artery disease

CTO Revascularization Evidence Considerations from a Patient Perspective
What is the Procedural Success and Safety Following Contemporary CTO PCI?
Event Estimate Context
Death0.2-0.9%
Source: OPENCTO¹, PERSPECTIVE²,
RECHARGE³
1.5%
ACC NCDR SVG PCI
Procedural MI 1.8% to2.8%
Source: OPENCTO¹, PERSPECTIVE²,
RECHARGE³
EXPERT CTO4
3.6%
LM PCI EXCEL Trial 6
Technical Success86% to90%
Source: OPENCTO1, PERSPECTIVE2,
RECHARGE3, EXPERT CTO4, PROGRESS5
74%
Mayo Clinic 2003-20057
Clinical Success 86% to 96%
Source: PERSPECTIVE2, EXPERT CTO4 85,9%
ACC NCDR
1Sapontis. JACC Intv2017; 2 Kandzari. TCT 2017; 3 Maeremans. JACC 2016; 4 Kandzari. JACC Intv2015; 5 Karmpaliotis. CCI 2016; 6 Stone. NEJM 2016; 7 Prasad JACC 2007; 8 Brilakis JACC Interventions 2015

CTO Revascularization Evidence
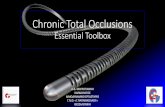
Patient Reported Health Status: PERSPECTIVE Trial
0%
25%
50%
75%
100%
Baseline N 243 1 Year N 210
34
8226
15
40
3
84,1
% A
ppro
pri
ate
by A
UC
SAQ Angina Frequency Scale
None Monthly Daily
Kandzari D.
Procedural, clinical and health status outcomes in chronic total coronary occlusion revascularization with zotarolimus-eluting stents:
results from the PERSPECTIVE trial.
Presented at: SCAI 2018. April 26, 2018. San Diego, CA.

CTO PCI: at the Intersection of Evidence and Experience in Clinical Practice
The Basics
• CLINICAL INDICATION
• DUAL ACCESS AND DUAL INJECTIONS
• STUDYING THE LESION
• GUIDE SUPPORT
• EQUIPMENT KNOWLEDGE AND USE
• COMPLICATION MANAGEMENT KNOWLEDGE

Predictors of Anterograde Procedural Failure
Univariate Predictors Multivariate Predictors
OR 95% CI p OR 95% CI p
Dyslipidemia 0.5 0.375-1.456 0.52
Diabetes 0.2 0.186-2.356 0.71
Hypertension 0.7 0.452-1.856 0.36
Smoking 0.6 0.532-1.156 0.44
Previous MI 0.8 0.620-1.030 0.08
Previous CABG 0.7 0.569-1.050 0.16
In stent CTO 0.7 0.345-1.756 0.54
Severe tortuosity 0.4 0.332-1.876 0.45
Severe calcification 0.43 0.348-0.686 <0.001 0.35 0.241-0.515 <0.001
CTO length >20mm 0.49 0.301-0.619 <0.001 0.52 0.352-0.790 0.002
CTO diameter <3mm 1.1 0.850-1.775 0.32
Blunt stump 0.63 0.490-0.816 <0.001 0.59 0.435-0.807 0.001
Galassi AR. et al.
In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion:
insights from the ERCTO (European Registry of Chronic Total Occlusion) registry.
EuroIntervention. 2011 Aug;7(4):472-9

Final Strategy per J CTO Score
AWE antegrade wire escalation ADR antegrade dissection reentry RW retrograde wiring RDR retrograde dissection reentry
Luo C. et al.
Predictors of Interventional Success of Antegrade PCI for CTO.
JACC Cardiovasc Imaging. 2015 Jul;8(7):804-13

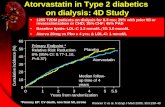
Angiographic Assessment for CTO-PCI
Procedure Planning
Dual Catheter Angiography
Antegrade Retrograde
1.Ambiguous proximal cap
2. Poor distal target
3. Interventional collaterals
Wire
Escalation
Dissection Reentry
( Cross Boss Stingray )
Wire
Escalation
Dissection Reentry
( Reverse CART )
Yes
Yes Yes
No
No No
fail fail fail fail
fail fail
Brilakis ES. et al.
A percutaneous treatment algorithm for crossing coronary chronic total occlusions.
JACC Cardiovasc Interv. 2012 Apr;5(4):367-79
4. Length < 20mm

When There' s a Will There' s a WayThe BUSHI DO (Bipoint Unilateral Sheathless catheter Insertion via Distal & prOximal radial artery)
Technique
Yoshimachi F., Takagava Y., Sakai K., Ikari Y.
EuroPCR 2018

Antegrade Wire Escalation: Step By Step
• Select a microcatheter
• Getting to the CTO with a workhorse wire &
microcatheter
• Advance the microcatheter to the proximal
cap
• Selecting a Guidewire for CTO Crossing
Pearls of Wisdom
The best way to prolong ( or fail) a case is by taking shortcuts…
W. Lombardi
CTO Expert
E. Brilakis
Manual of Chronic Total Occlusion Interventions: A Step-by-Step Approach
2nd Edition, Academic Press 2017

Support: Guide Catheter Extension
E.Brilakis
Manual of Coronary Chronic Total Occlusion Interventions. A Step-by-Step Approach.
Academic Press 2014, 1st Edition

Support: Microcatheter & OTW Balloon
Microcatheters & OTW Balloons:
• enhance the wire-penetrating capacity
• improve wire torque response
• allow wire tip reshaping without losing
wire position
• facilitate wire exchanges
Microcatheter vs OTW Balloon:
• more flexible and track better
• less kinking upon wire removal
• less likely to cause proximal vessel injury
• better assessment of the tip location
• better penetration of the CTO once a wire is through
• ↑↑↑ cost

Support: Microcatheter
Ron Waksman, Shigeru Saito Chronic Total Occlusions: A Guide to Recanalization
2nd Edition, Apr 2013 Wiley-Blackwell

CTO Toolbox-Wires
❖ Tapered, soft (~1) plastic jacketed GW (XT/XT-A/XTR)
➢ Antegrade/Retrograde microchannel/soft plaque probing
➢ Facilitation of quick wiring Dissection Re-entry in abmbigous vessel anatomy/soft plaque (Knuckle wire technique)
➢ Very small and tortuous collateral chanel crossing epicardial and septal(retrograde access)
❖ Non-tapered, soft plastic jacketed GW (Fielder FC/Pilot 50/Whisper)
➢ Multi-tasking (Mainly work in the body of the occlusion-getting less fashionable)
❖ Non tapered, medium gram force plastic jacketed wire (Pilot 150/200)
➢ Body of the occlusion
➢ Facilitation of quick wiring in complex lesions and/or dissection-reentry in ambiguous vessel anatomy
❖ Non-tapered, soft, composite core, hydrophilic coated GW (SION)
➢ Multitasking
➢ Access to difficult take-off collaterals
➢ Crossing of non challenging collaterals channels
➢ Subintinal spaces connection and GC engagment in retrograde technigues (CART/XCART)
❖ Non-tapered, medium gram force (<6g), non coated, sliding wires (Miracle 3/4.5/6)
➢ Used to be workhorse wires for lesion crossing-tend to be abandoned
❖ Non-tapered, medium gram force (<6g), hydrophilic coated, sliding wires (Miracle Ultimate)
➢ For lesion crossing (body of the occlusion) in hard but not severely calcified plaques and non tortuous anatomy
❖ Tapered, medium gram (<6g), composite core, hydrophilic coated GW (GAIA family)
➢ Are becoming the workhorse wires for lesion crossing (body of the occlusion) in hard but not severely calcified plaques even in tourtous anatomy
➢ Subintima space connection in Retrograde techniques
❖ Tapered and not tapered w-w/o hydrophilic coating, high gram(>9) GW penetration wires (Confianza fm, PROGRESS 200T)
➢ Crossing of severely calcified spots, exchanged to other categories afterwards

Wire Options For Antegrade Wire Escalation
Polymer jacketed tapered
Fielder XT Fighter
Course of occluded
vessel known?
Stiff tapered
Gaia 2nd Confianza Pro 12
Stiff polymer jacketed
Pilot 200
Yes No
E. Brilakis
Manual of Chronic Total Occlusion Interventions: A Step-by-Step Approach
2nd Edition, Academic Press 2017

Composite Core technology
• Anti kinking structure
• Higher torque performance with W core
Tip load
XT-A = 1.0g XT-R = 0.6gW-Coil structure
SLIP-COAT® Coating 170mm0.36mm
(0.014”)30mm20mm
straight taper
“Composite core”0.26mm
(0.010”) PTFE Coating
Compatible for retrograde approach ; Length 190cm
Soft Polymeric Tappering Jacket Guide Wires
FIELDER XT-R, FIELDER XT-A
Introduced in 2012-Fusion of Technology

Description of the Deflection
In compliant lesions, stress is applied to the shaped portion of the wire;
thus, the direction in which the tip advances changes.
Sianos G.
New Wires; What we have, What is essential, What is in the horizon.
EUROCTO CLUB
The Experts Live Workshop, 2017

• Softer guide wire tends to have more deflection.
• Much easier to use deflection in order to cross the lesion.
Softer tip guide wire
Parameters Influencing the Deflection
Sianos G.
New Wires; What we have, What is essential, What is in the horizon.
EUROCTO CLUB
The Experts Live Workshop, 2017

Parameters Influencing the Deflection
• Stiffer guide wire possess a lot of straight direction force
→ less deflection.
Stiffer tip guide wire
Sianos G.
New Wires; What we have, What is essential, What is in the horizon.
EUROCTO CLUB
The Experts Live Workshop, 2017

Gaia Concept
Deflection And Rotational (Directional-torque) Control
Deflection
Rotation
Intentional control through deflection to stay true lumen
Sianos G.
New Wires; What we have, What is essential, What is in the horizon.
EUROCTO CLUB
The Experts Live Workshop, 2017

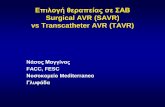
The Gaia Series: Anti Trapping Technology
6.
4.5
4.
3.5
2.
1.7
0. 1.5 3. 4.5 6. 7.5
ASAHI Gaia Next 3
ASAHI Gaia Third
ASAHI Gaia Next 2
ASAHI Gaia Second
ASAHI Gaia Next 1
ASAHI Gaia First
Tip Load Line Up
ACT ONE High torque performance while ensuring tip flexibility
Gaia micro-cone tip High penetration ability
XTRAND coil Anti trapping feature to avoid coil damage

Asahi Gaia Third? Or Confianza Pro?
Plaque=intima
Lumen
Tough tissue…
Asahi Gaia ⇒ Pass by GW control <Deflection & Rotation>Confianza Pro ⇒ Pass by penetration force
Ca++
Confianza Pro
Gaia
Sianos G.
New Wires; What we have, What is essential, What is in the horizon.
EUROCTO CLUB
The Experts Live Workshop, 2017

UB3/Pilot 150-200
Hard plaque Severe calcification
Stiffer tip
XT-A
ASAHI Gaia First
ASAHI Gaia Second
Miracle6-9
ASAHI Gaia Third
Confianza Pro12
Progress 200T
Confianza Pro
XT-R
Current Algorithm: What to Use When?

CTO (Single) Guide wire Advancement
• Sliding
• Drilling
• Penetration
• Advance - deflect - rotate - advance
CROSSING THE CTO
• Crossing the proximal cap
• Navigating through the occlusion
• Distal entry into the lumen
ACCESS WIRE POSITION
• True lumen
• Subintimal space
• Outside the vessel architecture

• controlled rotation of the GW in both directions.
• small tip bend (to avoid the creation of a large subintimal space).
• GW:• moderate tip stiffness
• escalation to stiffer wires
• forward GW advancement intentionally steering (directing)
• Indications:
- lesions with a calcified, hard-to-penetrate, proximal cap
- short occlusions with well understood vessel courses
• GW:• Miracle 12
• Confianza Pro 12
• Gaia 3
• support by a micro-catheter
• gently advancement and rotation to find micro-channels
• check for the wire position in 2 orthogonal planes
• avoid entry into sub-intimal space
GW:• tapered polymer coated GW (Fielder XT, Gaia 1)
• tapered hydrophilic GW (Runthrough NS)

Dual-wire Antegrade CTO Techniques: Parallel-Wire
guidewire in subintimal space
microcatheter
initial wire left in place
crossing attempted with second guidewire
successful entry into
distal true lumenE. Brilakis
Manual of Chronic Total Occlusion Interventions: A Step-by-Step Approach
2nd Edition, Academic Press 2017

Dual-Wire Antegrade CTO Techniques: Dual Lumen Catheter
guidewire in subintimal space
microcatheterDual lumen microcatheter
second guidewire
second wire into
distal true lumenE. Brilakis
Manual of Chronic Total Occlusion Interventions: A Step-by-Step Approach
2nd Edition, Academic Press 2017

Complex Antegrade CTO Techniques: ADR
Dissection & re-entry strategies:
▪ dissection:
• Knuckle wire
• CrossBoss catheter
▪ re-entry:
• wire-based re-entry:
- STAR technique
- contrast enhanced
- mini-STAR & LAST technique
• device-based re-entry:
- Stingray balloon and guidewire
- IVUS guided
well defined proximal cap
>20 mm long CTO
good distal vessel with no side branches
at distal cap (visible via contralateral)
E.Brilakis
Manual of Coronary Chronic Total Occlusion Interventions. A Step-by-Step Approach.
Academic Press 2014, 1st Edition

How To Use The Cross Boss Catheter
Step1. deliver Cross Boss to th proximal cap
Step 2. Cross Boss torque attachment
Step 3. Fast spin
Step 4. Assess
Cross Boss in side
branch
Cross Boss partially
crosses occlusion
but does not reach
distal cap
Cross Boss crosses
CTO into distal
subintimal
space
Cross Boss partially
crosses CTO into
distal true lumem
Modify proximal cap
Increase support Redirect Advance guidewire Stingray reentryInsert workhorse
guidewire
Cross Boss does
not advance

How To Use Knuckle Wire Step by Step
Step1. decision to proceed with knuckle wire
Step 2. knuckle formation
Step 3. knuckle advancement
Step 4. Assess
Knuckle partially
reaches occlusion
but not distal cap
Knuckle crosses
CTO into distal
subintimal space
Knuckle crosses CTO
into distal true lumen
*Knukle advancement
distal to the distal cap
should be avoided as it
may create large
hematoma
Redirect • CrossBoss
• different wire
• guide support
• #microcatheter
Stingray reentry Stingray reentry if
distally
PTCA/ Stent if close
to distal cap
Knuckle in
sidebranch

Contemporary ADR vs Classic ADR
Classic ADR 2011 Contemporary ADR 2018
Set Up 8Fr. Femoral with supportive guides
AL 0.75 EBU 3.5
8 Fr. Femoral with Trapliner or 6 Fr.
Radial without guide extension
Initial Microcatheter CrossBoss Corsair/ Turnpike family 135 cm but
still end with CrossBoss to limit
dissection
Re entry Catheter Stingray Stingray
Re entry Wire Stingray wire More flexible approach: Stingray wire/
CP12/ Hornet 14/ Gaia 3/ Astato
Re entry Technique Stick and Go Stick and Swap with Pilot 200
Hematoma Management STRAW if loss of visualization of
distal vessel
Active management with Trapliner
upfront and preemptive STRAW
Pershad A.
Chronic Total Occlusion Summit 2018

Use CrossBoss to Prepare Re-entry Zone
Following knuckle Wire Following CrossBoss

Deal With Your Complications!

Φυριπλάκα Μήλος 30/ 06/ 2020


MILESTONES IN CTO WIRE TECHNOLOGIESSianos et al. BMC Cardiovascular Disorders (2016) 16:33