Campimetry with two Variables and a New Projection Campimeter* *From the Eye Clinic of the...
11
ENUCLEATIONS AND EVISCERATIONS 839 REFERENCES 1. Stone, W . : In Fasanella, R. M.: Management of Complications in Eye Surgery, Philadelphia, Saunders, 1957, chap. 6. 2. Hughes, W. L.: Evisceration. A M A Arch. Ophth., 63 :36 (Jan.) 1960. 3. Culler, .: Enucleation and cosmetic rehabilitation. A M A Arch. Ophth., 45:445 (Apr.) 1955. 4. Moore, T.: A screw-type implant. Am. J. Ophth., 35:399-404 (Mar.) 1952. 5. Allen, J. H., and Allen, I.: A buried muscle cone implant. A M A Arch. Ophth., 43:879 (May) 1950. 6. Ellis, O. H.: A new orbital implant. Am. J. Ophth., 32:990 (May) 1950. CAMPIMETRY WITH TWO VARIABLES A N D A NEW PROJECTION CAMPIMETER* ANTONIO GRIGNOLO, M.D., MARIO ZINGIRIAN, M.D., AND ALFREDO RIVARA, M.D. Genova, Italy The purpose of perimetry with two vari- ables is to vary the brightness and surface area of the test object while the background illumination remains unchanged. This type of perimetry has become widespread since the introduction of the Goldmann projection perimeter, which utilizes a uniform and ad- justable illumination of the background bowl and several targets with different areas and brightness. The same source of light is used for illumination of the targets and of the background. The field is exacdy recorded at the time of measurement and the fixation is well-controlled. The most important property of Gold- mann's instrument is that it allows for standardization of the photometric variables, namely, brightness, contrast and surface area of the target. It is possible therefore to re- produce exactly the conditions of the exami- nation and to compare subsequent findings. Similar refinements have not, as yet, been in- troduced in campimetry, whose main advan- tage over perimetry is the easier and more detailed plotting of defects in the central and paracentral field. The usual technique of the tangent screen examination, however, has many drawbacks: mainly the difficulty of producing exactly a uniform illumination of screen and target; the inconstancy of the reflectivity of the tar- * From the Eye Clinic of the University of Ge- nova. Director: Prof. A. Grignolo. get and of the background due to their con- tinous u.se; and the distraction of the patient by the movements of the examiner and of the target handle. Therefore, some attempts to improve the campimetric technique have been made. Conover and Spaeth' and Spence" pro- posed a magnetic campimeter, allowing the targets to be moved without a handle. Targets produced by a projector either held in the hand (Juler,^ Lauber") or moved through a cardan joint (Hagedoorn and Van den Bosch") have been suggested. The main dis- advantage of such methods is that they do not consider the illumination of the background, so that its variation may cause marked changes in the contrast. Some authors (Berk,^ Weckers and Hum- blet,** Berens and Luckiesh* and Jayle and Mossé^) devised tangent screen illuminators of a constant intensity which may be regu- lated. These attempts, however, have not introduced the use of a single source of light for target and background, a uniform illumination of the tangent screen which can be modified at will and may be calibrated and targets with standardized surface areas and brightness. We" have constructed an instrument which can produce on a tangent screen at two m. the same conditions which are at- tained with the Goldmann projection perim- eter, obviously over a more restricted field.
Transcript of Campimetry with two Variables and a New Projection Campimeter* *From the Eye Clinic of the...

E N U C L E A T I O N S A N D E V I S C E R A T I O N S 839
REFERENCES
1. Stone, W . : In Fasanella, R. M . : Management of Complications in Eye Surgery, Philadelphia, Saunders, 1957, chap. 6.
2. Hughes, W . L.: Evisceration. A M A Arch. Ophth., 63:36 (Jan.) 1960. 3. Culler, Α . : Enucleation and cosmetic rehabilitation. A M A Arch. Ophth., 45:445 (Apr.) 1955. 4. Moore, T.: A screw-type implant. Am. J. Ophth., 35:399-404 (Mar.) 1952. 5. Allen, J. H., and Allen, I.: A buried muscle cone implant. A M A Arch. Ophth., 43:879 (May) 1950. 6. Ellis, O. H . : A new orbital implant. Am. J. Ophth., 32:990 (May) 1950.
C A M P I M E T R Y W I T H T W O V A R I A B L E S A N D A N E W
P R O J E C T I O N C A M P I M E T E R *
A N T O N I O GRIGNOLO, M . D . , M A R I O ZINGIRIAN, M . D . , A N D ALFREDO RIVARA, M . D . Genova, Italy
The purpose of perimetry with two variables is to vary the brightness and surface area of the test object while the background illumination remains unchanged. This type of perimetry has become widespread since the introduction of the Goldmann projection perimeter, which utilizes a uniform and adjustable illumination of the background bowl and several targets with different areas and brightness. The same source of light is used for illumination of the targets and of the background. The field is exacdy recorded at the time of measurement and the fixation is well-controlled.
The most important property of Goldmann's instrument is that it allows for standardization of the photometric variables, namely, brightness, contrast and surface area of the target. It is possible therefore to reproduce exactly the conditions of the examination and to compare subsequent findings. Similar refinements have not, as yet, been introduced in campimetry, whose main advantage over perimetry is the easier and more detailed plotting of defects in the central and paracentral field.
The usual technique of the tangent screen examination, however, has many drawbacks: mainly the difficulty of producing exactly a uniform illumination of screen and target; the inconstancy of the reflectivity of the tar-
* From the Eye Clinic of the University of Genova. Director: Prof. A. Grignolo.
get and of the background due to their con-tinous u.se; and the distraction of the patient by the movements of the examiner and of the target handle. Therefore, some attempts to improve the campimetric technique have been made.
Conover and Spaeth' and Spence" proposed a magnetic campimeter, allowing the targets to be moved without a handle. Targets produced by a projector either held in the hand (Juler,^ Lauber") or moved through a cardan joint (Hagedoorn and Van den Bosch") have been suggested. The main disadvantage of such methods is that they do not consider the illumination of the background, so that its variation may cause marked changes in the contrast.
Some authors (Berk,^ Weckers and Hum-blet,** Berens and Luckiesh* and Jayle and Mossé^) devised tangent screen illuminators of a constant intensity which may be regulated. These attempts, however, have not introduced the use of a single source of light for target and background, a uniform illumination of the tangent screen which can be modified at will and may be calibrated and targets with standardized surface areas and brightness.
W e " have constructed an instrument which can produce on a tangent screen at two m. the same conditions which are attained with the Goldmann projection perimeter, obviously over a more restricted field.

840 A N T O N I O GRIGNOLO, M A R I O ZINGIRIAN A N D ALFREDO R I V A R A
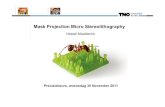
Fig. 1 (Grignolo, et al.). The projection campimeter unit and the tangent screen.
26 degrees, 30 iriinutes from the fixation point.
APPARATU-S AND METHOD
The instrument ( f ig . 1) projects two separate luminous beams originating from the saine light source onto an opaque white tangent screen (2.0 by 2.0 m . ) . One beam uniformly illuminates the background; the other projects the luminous targets onto the
screen. A mechanical linkage allows the examiner to move the luminous target on the screen, and the handle moves a stylus over a campimetry chart, allowing the field to be plotted directly.
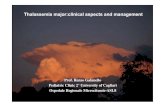
The patient is seated on an adjustable stool with his head immobilized by a strap around the forehead (fig. 2 ) . The projector is located on a stand behind the patient's head. A side extension of this stand holds the recording chart and the control handle which moves the targets.
Details of the instrument are as follows: Optical system. Figure 3 shows schemati
cally the optical components of the instrument. A fan-cooled 500 w. lamp provides the source of illumination for the screen and the target. A n optical system located in front of the lamp provides the background illumination.
The optical system is composed of two condensing lenses (fig. 3-1 and 2 ) . These pass the light from the lamp (Γ.) by means of a tilted mirror ( A ) through a third lens ( 3 )
Fig. 2 (Grignolo, et al.). Position of the patient and the observer during the campinietric examination.
Fig. 3 (Grignolo, et al.). Schematic drawing of the optical .system for the simultaneous projection of the target and illumination of the screen. (A, B, C) reflecting mirrors; (D) diaphragm; (E) switching device; (F) projection device for the fixation spot; (L) lamp; (S) diffusing surface; (1, 2, 3, 4) condensing lenses; (5, 6) projecting lenses.

C A M P I M E T R Y W I T H T W O V A R I A B L E S 841
which condenses it onto a convex diffusing surface ( S ) . This surface uniformly illuminates the tangent screen. The iris diaphragm regulates the intensity of the light. Behind the lamp, a mirror ( B ) reflects the light through a biconvex condensing lens to the target projection system which consists of the objective [a negative lens ( 5 ) and a positive lens ( 6 ) ] . A rotating mirror ( C ) reflects the projected target onto the screen. The light beam which projects the target may be turned off by a push button.
Mechanical system for moving the targets. T o produce vertical and horizontal movements of the targets, two independent rotations are transmitted to the mirror which projects the one target around a vertical axis and the other around a horizontal axis—both in the plane of the mirror's surface.
The recording device consists of an opalescent glass screen, illuminated from the back and holding a campimetry chart (figs. 4 and 5 ) . A stylus is integrated with the handle which controls the movements of the reflecting mirror and thereby the position of the target on the screen. In this way the visual field may be plotted exactly and at the same time that the tests are performed.
The tangent screen (fig. 1) on which the targets are projected is a 2.0-m. square frame covered by a white opaque cloth with a reflection coefficient of 0.8. It is illuminated by the light emitted by the diffusing surface (fig. 3 - S ) . A photometric check showed negligible differences between the center and the periphery of the screen.
Fig. 4 (Grignolo, et al.). Recording device.
Fig. 5 (Grignolo, et al.). Campimetric chart.
The illumination of the tangent screen may be modified with a diaphragm (fig. 3 -D) from darkness to 20 apostilb ( a s b ) . It is possible therefore to examine the visual field under scotopic, as well as mescopic and photopic, conditions. The distance between the subject's eye and the center of the tangent screen is 2.0 m. Small differences in the distance between the eye and the fixation point do not modify the extent of the visual field, providing they are within five percent of the distance (Goldmann*). This means that in our instrument such A'ariations have to be kept within 10 cm. Variations due to individual differences of the eye-occiput distance fall well within this range.
Fixation. The fixation point is a round luminous target projected on the center of the screen by the small projector located in front of the instrument. Its illuminations and optical system are independent of those of the main projector (fig. 3 - F ) .
The diameter of the fixation target can be varied from 1.87 to 30 mm. Its intensity may be modified with a rheostat. A red filter can be interposed in order to obtain a fixation spot suitable for visual field examination under mesopic and scotopic conditions.
The exammer's position allows him to observe the subject's eye directly and check its fixation. It is felt that such direct obser-

842 A N T O N I O GRIGNOLO, M A R I O ZINGIRIAN A N D ALFREDO RIVARA
Fig. 6 (Grignolo, et al.). Device for photometric standardization of background luminance, (a) Contiguous illuminated areas, (b) Identical luminance of both areas.
vation of the fixing eye is accurate enough for the purposes of campimetry. Very seldom will a patient steadily fix a point different from the fixation spot. More frequently the patient's eye shows a tendency to follow the moving target, which is easily detected by inspection. On the other hand, a small degree of eccentric fixation also escapes notice in an apparently more accurate device such as that on the Goldmann perimeter.
Targets. A s previously mentioned, the targets projected by the instrument can be guided by a very sensitive mechanism to every point of the tangent screen. Their surface area and brightness can be modified at will.
Suitable diaphragms of progressively increasing aperture can be interposed in order to modify the area of the targets. The size of the diaphragms, held in a revolving drum, can be easily changed. In this way targets
with areas of 2.75, 11, 44, 176 and 704 mm.^—indicated by the Roman numerals 0, I, II, III and IV—-can be projected.
The angle subtended at 2.0 m. by these targets is the same as that subtended at 30 cm. by the corresponding targets of the Gold-mann perimeter (0 , I, II, III and I V ) .
It must be noted that the targets, when projected on the periphery of the screen, undergo a small increase in area and an elliptical deformation of shape. The increase in the area at 26 degrees is about five percent o f that of the same target at 0 degrees.
After several tests, we were able to establish that the greatest enlargement of a target at the periphery induces a negligible change (less than one degree) in the isopter and may therefore be disregarded.
The greatest luminance of the targets is of 200 asb. It can be reduced by interposing neutral filters of decreasing transmission as follows: 1, 0.31, 0.1, 0.031, which give respectively, the following luminances of the targets; 200, 62, 20 and 6.2 asb., indicated by the following Arabic numerals: 3, 2, 1, 0. A second set of filters with transmissions of 1, 0.8, 0.63, 0.5 and 0.4 can be added to the first filters to obtain finer variations of the luminance. This set is indicated by the following letters: e, d, c, b and a. The range of the target luminance of our instrument corresponds exactly to that of Goldmann's perimeter.
Photometric standardization of the instrument. In order to standardize the luminance of the screen with that of the target, a photometric device was constructed. It is composed (fig. 6 ) of a small photometric screen (6 .0 by 5.0 cm.) held 13 cm. in front of the surface of the tangent screen by a suitable stand at a point five degrees below the fixation spot. A small fraction of the light beam forming the target (surface I V ) as well as some of the light which illuminates the background passes through a rectangular window (10 by 22 mm.) in the center of the small screen.

C A M P I M E T R Y W I T H T W O V A R I A B L E S 843
The two beams, coming from two apparently different sources of light, have different angles of incidence, hence, they illuminate two different areas of the tangent screen, each of which reproduces the shape of the window.
The distance of the photometric screen from the background makes the two illuminated rectangular areas contiguous (fig. 6-a) . They may be observed by the examiner, standing at the side of the projector. The largest area of the target ( I V ) is used, and the filter of 0.1 transmission ( 1 ) is inserted in order to obtain a luminance of 20 ash. over the photometric area of the screen corresponding to the target beam. The examiner can easily compare its brightness with that of the area corresponding to the background illumination. The latter can be adjusted by regulating the diaphragm until an identical luminance of both areas is obtained (fig. 6 -b) .
Contrast index. The contrast index is the ratio of brightness of the target (without the background illumination) to that of the tangent screen. It is represented by Δ I / I . The greatest luminance of the target is 200 ash, the background luminance is standardized at 20 ash., hence the greatest contrast index in our instrument is 200/20 = 10.
The contrast indexes corresponding to the lower luminances of the target are, respectively, 62/20 = 3.1; 20/20 = 1; and 6.2/20 = 0.31. In Table 1 are compared the contrast indexes of our instrument and those of Goldmann's perimeter; it can be noted that they are equivalent at three levels.
The highest contrast index (31.5) of the Goldmann perimeter is not available in our instrument. Such a high contrast is, in fact, useless in a campimetric examination which disregards the peripheral field beyond 26 degrees, 30 minutes. However, our instrument provides a low contrast index (0.31) lacking in Goldmann's perimeter, which is very useful for detecting very slight defects in the central visual field.
TABLE 1
CONTRAST INDEXES
Target No.
Goldmann Projection Perimeter
( t )
Our Projection Campimeter
( t ) 4 3 1 . 5
( 1 0 0 0 / 3 1 . 5 ) —
3 1 0 ( 3 1 5 / 3 1 . 5 )
1 0 ( 2 0 0 / 2 0 )
2 3 . 1 5 ( 1 0 0 / 3 1 . 5 )
3 . 1 5 ( 6 2 / 2 0 )
1 1 ( 3 1 . 5 / 3 1 . 5 )
1 ( 2 0 / 2 0 )
0 — 0 . 3 1 ( 6 . 2 / 2 0 )
PRESENT STUDY
Kinetic and static examinations have been performed in a series of 20 normal emmetropic subjects between 25 and 35 years of age to determine the normal visual field. All of them were co-operative and good observers.
K I N E T I C CAMPIMETRY
The visual field was examined using all the possible combinations of surface area and contrast of the test object. The differential light threshold was determined by the kinetic method along each of the following hemi-meridians: 0, 45, 90, 135, 180, 225, 270 and 315 degrees. The threshold values were obtained by averaging several determinations made with centripetal as well as centrifugal movements of the target. The target was moved continuously at a rate of five degrees per second. The 0 /0 target with the smallest surface area (2.75 mm.^) and contrast ( 0 . 3 1 / I ) was not perceived by the subjects in our series.
Isopters were obtained which lay up to 26 degrees, 30 minutes from the center of the field, using the following targets: 0/3, 0 /2 , 0 /1 , 1/2, I / l , and II/O. For normal subjects, targets with wider surface area and higher contrast produced isopters which appeared

844 A N T O N I O GRIGNOLO, M A R I O ZINGIRIAN A N D ALFREDO R I V A R A
Fig. 7 (Grignolo, et al.). Kinetic campimetry: isopteric bands (standard deviation) for 0/3, 0/2, 0/1 targets in normal eyes.
to be off the campimetric screen. They can be used for eyes with a pathologic reduction of the differential light threshold.
For each isopter the average and its standard deviation were calculated from the findings in the series. The shaded areas on the diagrams (figs. 7, 8 and 9 ) show seven isopteric bands, each of which indicates the variability (the standard deviation) for each combination of surface area and luminance of the test object. Such a variability is lower for the more central isopters than for the peripheral ones.
Relationship between area and contrast of the target: Spatial summation. Perimetry and campimetry with two variables are based on the fact that the extent of the visual field is directly proportional to the surface area of the target and to its contrast.
A spatial summation of the stimuli is produced when test objects of a certain size and brightness are used. It follows that two targets of different surface area may produce the same isopter provided their contrast and surface areas are proportionately related.
According to Goldmann,*' the law of spatial summation is given by the equation Φ = ( F o V F ) when Φ is the filter transinis-sion needed to obtain the same extent of the visual field with the area F as with the area Fo.
The summation coefficient k is 1 when there is a complete summation, and is less than 1 when the summation is incomplete.
A s stated by Goldmann,* the value of k which best fits the equation is 0.84. It follows that when the progression ratio of the area is 4, that of the transmittivities is 0.31.
Such a condition has been realized in our campimeter, so that the use of the same suiu-mation coefficient (k = 0.84) is implicit. T o indicate how far the Goldmann equation is reliable in our campiineter, a comparison be-
Fig. 8 (Grignolo, et al.). Kinetic campimetry: isopteric bands (standard deviation) for 1/2, I / l , I/O targets in normal eyes.
Fig. 9 (Grignolo, et al.). Kinetic campimetry: isopteric bands (standard deviation) for II/O target in normal eyes.

C A M P I M E T R Y W I T H T W O V A R I A B L E S 845
tween the isopters of photometrically equivalent targets has been made. Geometric superposition, an approximate method of comparison, was used.
A s shown in Figures 10, 11 and 12, the superposition of the theoretically equivalent isopteric bands is more complete for targets with a small surface area and high contrast.
In fact, the area of superj)Osition given by the 0 /1 , 0 /2 and 0/3 targets and that by the I/O, I / l and 1/2 targets is very large, but is larger for the peripheral than for the central isopters. N o superposition is possible between the bands given by the I / l and I I/O targets.
The results of the comparison show that with the coefficient k = 0.84, the smaller the surface area of the target and the farther the retinal point which is investigated is from the macula, the more perfectly the law of spatial summation is realized.
T o this extent is appears that the results of campimetry with two variables performed with our instrument are in good agreement with those obtained with the Goldmann perimeter.
Physiologic scotomas. Physiologic scoto-matous areas, namely the spatial projection of
Fig. 11 (Grignolo, et al.). Kinetic campimetry. comparison between isopteric bands obtained with photometrically equivalent targets (0/2, 0/1) in normal eyes. The black band indicates the area where they are superimposed.
the optic disc (blindspot) and the retinal vessels (angioscotomas) have been detected with the projection campimeter in our series of normal subjects.
The blindspot appears as an oval-shaped scotoma with a central area of total blindness and a peripheral halo of relative blindness. This arises from the fact that the differential retinal sensitivity does not drop
Fig. 10 (Grignolo, et al.). Kinetic campimetry: comparison between isopteric bands obtained with photometrically equivalent targets (0/3, 1/2) in norma! eyes. The black band indicates the area wliere they are superimposed.
Fig. 12 (Grignolo, et a!.). Kinetic campimetry: comparison between isopteric bands obtained witli pliotometrically equivalent targets (0/1, I/O) in normal eyes. The black band indicates the area where they are superimposed.

846 A N T O N I O GRIGNOLO, M A R I O ZLNGIRIAN A N D A L F R E D O R I V A R A
Fig. 13 (Grignolo, et al.). Kinetic campimetry: average limit of the blindspot in normal eyes and its variability (standard deviation).
abruptly at the disc edge but decreases smoothly, as has also been shown by static perimetry.
The vertical and horizontal diameters of the blindspot have been measured. The 1/3 target was used because it is a stiinulus intense enough to detect the area of total blindness and to exclude that of relative blindness. The average horizontal diaineter was 6.15° ± 0.33°, and that of the vertical meridian 8.35° ± 0.37°. The average distance of the blindspot from the fixation point, irieas-ured from its nasal edge, was 12.20° ± 0.51°. The horizontal meridian cuts the vertical diameter of the blindspot into two unequal segments. The average length of the superior segment appeared to be 3.30° ± 0.75°. The average diameters of the blind-spot are shown with the standard deviation in Figure 13.
Physiologic angioscotoma are fairly easily detected with the projection campimeter. The projection targets are particularly suitable for detecting reduced sensitivity in small areas of the visual field. Campimetry at a distance of 2.0 in. produces a magnified projection of the retinal vessels on the tangent screen, which makes it easier to detect small defects such as angioscotomas.
STATIC CAMPIMETRY
The static examination of the visual field has been performed so far only with the projection perimeter. Our projection campimeter enabled us to perform .static campimetry on the tangent screen at a distance of 2.0 m. The advantage of such a method is the easy detection of fine details and of the smallest defects of the central and paracentral visual field.
Twenty normal subjects were examined with static campimetry. For each subject the horizontal meridian (0-180 degrees) was investigated. A test object was presented at
Fig. 14 (Grignolo, et al.). Projection campimetry : angioscotomas from the right eye of a normal subject aged 31 years (1/3 target).
In order to locate these accurately the following conditions are required: (1) the use of a target with a small surface and a contrast high enough to be easily perceived up to 20-25 degrees (the best results were obtained with the 1/3 target) ; (2) a slow smooth movement of the target at a speed of 2.5 degrees per second directed, as much as possible, perpendicular to the longitudinal axis of the angioscotomas; and (3) close co-operation of the subject.
Figure 14 shows an example of angiosco-tometry performed with the projection campimeter in a 31-year-old normal emmetrope.

C A M P I M E T R Y W I T H T W O V A R I A B L E S 847
different angles from the fixation point. The target with 11 mm.^ surface ( I ) was preferred because it is the smallest target which is easily perceived in the peripheral parts of the screen.
The brightness of the target was proges-sively increased, starting from subliminal values, until the threshold of the stimulus was attained. Each stimulus was shown three times to the subject for one second at two-second intervals. The brightness of the stimulus which was perceived at least twice was considered to be liminal.
The results of such an investigation are presented in the form of a graph (fig. 15) in which the threshold luminance (in asb.) is shown on the ordinate and the angular distance (in degrees) from the fixation point on the abscissa. A curve was obtained connecting the points on the graph corresponding to the luminance thresholds for every degree of a meridian.
The averages of the differential threshold and its standard deviation were calculated for each degree near the center and the blindspot, and for every five degrees in the other portions of the curve. The averages and their standard deviations ( ± 2σ) are indicated by the curves on the graph in Figure 16.
The curve shows a peak corresponding to the fixation point, which indicates the sensi-
Fig. 15 (Grignolo, et al.). Static campimetry: differential threshold along the 0-180-degree meridian in a normal eye (target surface 2.0 mm.').
Fig. 16 (Grignolo, et al.). Static campimetry: average differential threshold along 0-180-degree meridian and its variability ( ± 2 ) in normal eyes.
tivity of the fovea, the point of highest sensitivity and its height decreasing progressively from the central point toward the periphery. The nasal part appears more smooth than the temporal. The temporal portion of the curve is interrupted by the blindspot which appears in the graph as a funnel-shaped pit, where the sensitivity is zero, corresponding to the area of total blindness which is wider on the nasal than on the temporal side.
The area of total blindness lines between 13.8° ± 0 . 6 1 ° and 18.6° ± 0.50° from the center. The average brightness threshold of stimulus is 3.58 asb. at the fixation point, 121.04 asb. at 25 degrees on the nasal side and 48.58 asb. at 25 degrees on the temporal side.
The variations of the threshold appear to be smaller near the central part than on the periphery of the curves. The largest variability is located temporally near the medial edge of the blindspot.
The graph in Figure 16 indicates the average threshold value and its standard deviation. Obviously the curves are not so smooth in individual cases when the threshold is determined every half degree from the center (fig. 15 ) .
In the graph used for static campimetry the luminance values are indicated by a

848 A N T O N I O GRIGNOLO, MARIO ZINGIRIAN A N D ALFREDO R I V A R A
Fig. 17 (Grignolo, et al.)- Static perimetry (Goldmann perimeter) : differential threshold along the 0-180-degree meridian in a normal eye. Dotted line indicates the portion which can be better explored with the projection campimeter.
logarithmic scale. In this way the curves also clearly indicate very small variations of the retinal sensitivity, particularly of the macular area. A comparison between the curves of differential thresholds obtained with static campimetry (fig. 15) and static perimetry (fig. 17) show the following advantages and disadvantages of both methods:
1. Much more detail of the differential threshold curves is obtained with static campimetry. This is due to the fact that with our campimeter it is possible to investigate the retinal sensitivity every half degree and at even smaller intervals. With the Gold-mann perimeter the retinal sensitivity cannot be determined at intervals of less than one degree.
2. Retinal sensitivity cannot be determined farther out than 26 degrees, 30 minutes with our campimeter. This prevents it from being used in cases with changes involving the periphery of the retina, which can be better investigated with the Goldmann perimeter.
3. On the other hand, static campimetry gives more detailed information on the sensitivity of the central part of retina, particularly of the macular region, which cannot be attained with perimetry or any other method.
S U M M A R Y
A new projection campimeter is described. Campimetry with two variables can be performed with the instrument on a white opaque tangent screen at a distance of 2.0 m. The same light source is used for illuminating the screen and projecting the targets. The brightness of the background and targets is regulated with a photometric device. Surface areas and contrasts of the targets are equivalent to those of the Gold-mann perimeter. Findings are plotted on a campimetry chart with a recording device.
Campimetry has been performed with the projection campimeter in a series of 20 normal emmetropic subjects using kinetic and static techniques. Results concerning the variability of the isopters, differential threshold curves and physiologic scotomas are reported. The instrument gives more detailed information on the retinal sensitivity in the central and paracentral visual field up to 26.5 degrees from the fixation point which cannot be attained with perimetry or any other method.
Vialc Bcnedetfo XV, No. 5.
REFERENCES
1 Berens, C., and Luckiesh, M . : A tangent screen illuminator. Arch. Ophth., 39:176, 1948 2. Berk, M. M . : A lighting system for a two-meter tangent screen. Am. I. Ophth., 42:486, ]9.·>6.

C A M P I M E T R Y W I T H T W O V A R I A B L E S 849
3. Conover, W. G., and Spaeth, E. B.: Conover-Spaeth magnetic campimeter. A M A Arch. Ophth., 52:12.1, 1954.
4. Goldmann, H.: Grundlagen exakter Perimetrie. Ophthalmologica, 109 :5, 1945. 5. — : Ein selbstregistrierendes Projectionskugelcampimeter. Ophthalmologica, 109:71, 1945. 6. Hagedoorn, Α., and Van den Bosch, C.: A double-projection campimeter. Am. J. Ophth., 40:891,
1955. 7. Jayle, G. E., and Mossé, P. (Quoted by Ourgaud, A. G., and Étienne, R.) : L'Exploration Fonctio-
nelle de I'Oeil Glaucomateux. Paris, Masson, 1961, p. 1078. 8. Juler, F.: A modification of Elliot's scotometer. Proc. Roy. Soc. Med., 18:2, 1924. 9. Lauber, H. : Ein Lichtpunktwerfer für Perimetrie und Kampimetrie. Ztschr. Augenh., 81:299, 1933. 10. Spence, G. D. : Magnetic tangent screen. Tr. Am. Acad. Ophth., 60:605, 1956. 11. Weekers, R., and Humblet, M . : L'angioscotome phisiologique. Ophthalmologica, 109:43, 1945. 12. Zingirian, M . : Nuovo strumento a proiezione per la campimetria a due variabili su schermo tangente.
Atti Soc. Oft. Ital., in press.
T E M P O R A L I S M U S C L E T R A N S P L A N T F O R T I S S U E D E F E C T S A B O U T T H E O R B I T
ROBERT D . DEITCH , M.D. , AND ALSTON C A L L A H A N , M . D . Birmingham, Alabama
Part or all of the origin of the temporalis muscle has been transplanted for repair of major defects of the upper face. It has not been used for minor defects—congenital, traumatic, or surgical—as frequently as it should have been. Its location and size make it well suited for repairing defects about the lateral aspect of the orbit. It is autogenous living tissue and, therefore, is superior to foreign implantation material. It has been used in a variety of ways around the upper face, as we shall mention.
Our opportunity to utilize the temporalis muscle for a soft tissue defect of the infero-lateral orbital quadrant came when a sftvtn-year-old boy, a physician's son, was brought to us with congenital hypoplasia of the left orbit and agenesis of the left globe. He had 10 surgical procedures prior to consulting us.
At the time of the first examination the right palpebral fissure was 30-mm. long, the left 18-mm. long. The left medial canthus was in good condition and was well attached. There was no movement of the left prosthesis when the right eye was moved. The left upper lid needed much more skin. The orbicularis muscle was working well in it but levator action was questionable. The lateral aspect of the left upper face, espe-
Fig. 1 (Deitch and Callahan). Appearance before transplantation of part of the temporalis. Note the flat appearance of the lateral aspect of the left orbit.
daily in the lower temporal quadrant, was flat and it was planned that strips of silicone rubber would be inserted subcutaneously for the necessary thickness and tied down with Supramyd extra sutures. The socket was deepest in the lower temporal quadrant and shallowest in the upper nasal quadrant.
On July 12, 1962, reconstructive surgery was performed with silicone rubber strips, but infection subsequently developed which resulted in their extrusion. The strips were replaced on January 24, 1963. There was still some flatness around the lateral aspect of the left orbit, as illustrated in Figure 1.
On August 8, 1963, the anterior one third of the left temporalis muscle was rotated forward subcutaneously, as indicated in Fig-













![arXiv:2006.01058v1 [hep-ph] 1 Jun 2020 · 2020. 6. 2. · iINFN Sezione di Genova, Genova, I-16146, Italy E-mail: albalade@jlab.org, danilkin@uni-mainz.de, sgonzal@iu.edu, dwinney@iu.edu](https://static.fdocument.org/doc/165x107/606f77e1e447835a86468f1b/arxiv200601058v1-hep-ph-1-jun-2020-2020-6-2-iinfn-sezione-di-genova-genova.jpg)
