Autoantibodies vex the vasculature
2
NEWS AND VIEWS Future investigations will undoubtedly dig deeper into questions raised by this study. It would be helpful to know which component of the virus triggers the TLRs. Examining the IRF-7 pathway in other natural SIV hosts might help clarify the impact of IFN-α, but researchers should also consider whether other inflammatory cytokines such as TNF-α and IL-12 might be altered in different hosts. If the finding that IFN-α signaling under- lies immune activation in sooty mangabeys also holds true in people, as some research suggests 13 , there may be therapeutic implica- tions. Considering the ability of current anti- retroviral drug regimens to eliminate the viral replication that drives immune activation, it seems unlikely that agents blocking IFN-α induction or action would find their way into a drug regimen. However, by interrupting the fundamental pathogenic process, approaches focused on IFN-α could reduce or delay the need to start lifelong antiretroviral therapy. In addition, research into how HIV-1 causes chronic immune activation may provide valu- able tools and concepts for understanding other viral infections and diseases in which there is abnormal immune activation. 1. Gao, F. et al. Nature 397, 436–441 (1999). 2. Mandl, J.N. et al. Nat. Med. 14, 1077–1087 (2008). 3. Mellors, J.W. et al. Science 272, 1167–1170 (1996). 4. Giorgi, J.V. et al. J. Infect. Dis. 179, 859–870 (1999). 5. Silvestri, G., Paiardini, M., Pandrea, I., Lederman, M.M. & Sodora, D.L. J. Clin. Invest. 117, 3148–3154 (2007). 6. Pandrea, I. et al. J. Virol. 82, 3713–3724 (2008). 7. Milush, J.M. et al. J. Immunol. 179, 3047–3056 (2007). 8. Boasso, A. & Shearer, G.M. Clin. Immunol. 126, 235–242 (2008). 9. Brenchley, J.M. et al. Nat. Med. 12, 1365–1371 (2006). 10. Somma, F. et al. J. Immunol. 164, 5078–5087 (2000). 11. Takaoka, A. et al. Nature 424, 516–523 (2003). 12. Rogge, L. et al. J. Immunol. 161, 6567–6574 (1998). 13. Sedaghat, A.R. et al. J. Virol. 82, 1870–1883 (2008). 14. Herbeuval, J.P. et al. Proc. Natl. Acad. Sci. USA 102, 13974–13979 (2005). 1018 VOLUME 14 | NUMBER 10 | OCTOBER 2008 NATURE MEDICINE Autoantibodies vex the vasculature Cees GM Kallenberg, Coen A Stegeman & Peter Heeringa Infections with fimbriated bacteria may trigger autoimmunity and cause a form of severe vasculitis that affects capillaries in the kidney and that can destroy the organ (pages 1088–1096). Cees G.M. Kallenberg is in the Department of Rheumatology and Clinical Immunology, Coen A. Stegeman is in the Department of Nephrology and Peter Heeringa is in the Department of Medical Biology, University Medical Center Groningen, University of Groningen, Hanzeplein, P.O. Box 30.001, Groningen 9700RB, The Netherlands. e-mail: [email protected] Systemic vasculitides comprise a group of idiopathic disorders characterized by inflam- mation of vessel walls 1 . In many small-vessel vasculitides, such as Henoch Schönlein pur- pura and cryoglobulinemic vasculitis, immune complexes underlie the vascular inflammation. In other cases, however, immune deposits are not detected or are detected at low levels in the lesion tissue. In this issue of Nature Medicine, Kain et al. 2 begin to uncover a mechanism behind these harder-to-crack pauci-immune small-vessel vasculitides. The findings suggest that infection with a Gram-negative bacterium such as E. coli may trigger disease in susceptible individuals by inducing the production of antibodies to a human protein expressed on neutrophils, lyso- somal membrane protein-2 (LAMP-2). These antibodies activate neutrophils that, in turn, may erode the vasculature. New insights and therapeutic approaches are needed for the relatively rare but deadly pauci-immune small-vessel vasculitides, which include Wegener’s granulomatosis, microscopic polyangiitis, renal limited vasculitis and Churg- Strauss syndrome 3 . The kidneys are frequently affected in these conditions. Without immedi- ate and strong immunosuppressive treatment, mortality is extremely high, and, even with treatment, mortality goes up to 35% within five years. As relapses frequently occur, long- term treatment is necessary, which can result in therapy-related illness and death. Major advances in the understanding and diagnosis of these pauci-immune vasculitides came from the detection of autoantibodies directed against neutrophil constituents in the majority of individuals with Wegener’s granu- lomatosis and microscopic polyangiitis 3,4 . These antineutrophil cytoplasmic autoantibodies (ANCA) are directed either to proteinase-3 in most individuals with Wegener’s granuloma- tosis or to myeloperoxidase in the majority of individuals with other forms 4 . Levels of ANCA follow disease activity, but this relationship is far from perfect 5 . In vitro, ANCA are able to activate primed neutrophils, which, when they contact endothelial cells, can induce endothe- lial damage 4 . The most convincing argument for a pathogenetic role of ANCA comes from in vivo experimental work. Xiao et al. 6 have shown that mice injected with mouse antibod- ies to myeloperoxidase developed (focal) pauci- immune vasculitis, particularly in kidneys. However, passive transfer of mouse or rat anti- bodies to proteinase-3 in mice did not result in a relevant animal model of proteinase-3–specific ANCA–associated Wegener’s granulomatosis 7,8 . So, many questions regarding the etiopathogen- esis of the ANCA-associated vasculitides (AAVs) are still open. In the current work, Kain et al. 2 confirmed an observation previously reported by the same group 9 . They found that individuals with AAVs and renal involvement produce ANCA directed against LAMP-2 (ref. 9)—a heavily glycosylated type 1 membrane protein expressed by many cell types, including neutrophils and endothelial cells, that is involved in cellular adhesion and homeostasis. They went on to provide evidence that anti- bodies to human LAMP-2 have pathogenetic potential 2 . They showed that these antibodies activate neutrophils and cause apoptosis of endothelial cells in vitro 2 . When injected into rats, the antibodies induced pauci-immune necrotizing crescentic glomerulonephritis, the renal histological hallmark of pauci-immune small-vessel vasculitides. More importantly, the authors showed that a major epitope of human LAMP-2 recognized by the autoantibodies has strong homology with FimH, a bacterial adhesin of common Gram- negative bacteria. When rats were immunized with FimH, most developed both cross-reac- tive antibodies to LAMP-2 and pauci-immune NCGN (Fig. 1). The data collectively suggest that bacterial infection, in a susceptible person, may induce autoantibodies that will result in pauci-immune vasculitis in the kidney. How should these results be interpreted? The data suggest that antibodies to human LAMP-2 should be included as a diagnostic test when © 2008 Nature Publishing Group http://www.nature.com/naturemedicine
Transcript of Autoantibodies vex the vasculature

n e w s a n d v i e w s
Future investigations will undoubtedly dig deeper into questions raised by this study. It would be helpful to know which component of the virus triggers the TLRs. Examining the IRF-7 pathway in other natural SIV hosts might help clarify the impact of IFN-α, but researchers should also consider whether other inflammatory cytokines such as TNF-α and IL-12 might be altered in different hosts.
If the finding that IFN-α signaling under-lies immune activation in sooty mangabeys also holds true in people, as some research suggests13, there may be therapeutic implica-tions. Considering the ability of current anti-retroviral drug regimens to eliminate the viral replication that drives immune activation, it
seems unlikely that agents blocking IFN-α induction or action would find their way into a drug regimen. However, by interrupting the fundamental pathogenic process, approaches focused on IFN-α could reduce or delay the need to start lifelong antiretroviral therapy.
In addition, research into how HIV-1 causes chronic immune activation may provide valu-able tools and concepts for understanding other viral infections and diseases in which there is abnormal immune activation.
1. Gao, F. et al. Nature 397, 436–441 (1999). 2. Mandl, J.N. et al. Nat. Med. 14, 1077–1087
(2008).3. Mellors, J.W. et al. Science 272, 1167–1170
(1996).
4. Giorgi, J.V. et al. J. Infect. Dis. 179, 859–870 (1999).
5. Silvestri, G., Paiardini, M., Pandrea, I., Lederman, M.M. & Sodora, D.L. J. Clin. Invest. 117, 3148–3154 (2007).
6. Pandrea, I. et al. J. Virol. 82, 3713–3724 (2008). 7. Milush, J.M. et al. J. Immunol. 179, 3047–3056
(2007).8. Boasso, A. & Shearer, G.M. Clin. Immunol. 126,
235–242 (2008). 9. Brenchley, J.M. et al. Nat. Med. 12, 1365–1371
(2006). 10. Somma, F. et al. J. Immunol. 164, 5078–5087
(2000).11. Takaoka, A. et al. Nature 424, 516–523 (2003). 12. Rogge, L. et al. J. Immunol. 161, 6567–6574
(1998).13. Sedaghat, A.R. et al. J. Virol. 82, 1870–1883
(2008). 14. Herbeuval, J.P. et al. Proc. Natl. Acad. Sci. USA 102,
13974–13979 (2005).
1018 volume 14 | number 10 | october 2008 nature medicine
Autoantibodies vex the vasculatureCees GM Kallenberg, Coen A Stegeman & Peter Heeringa
Infections with fimbriated bacteria may trigger autoimmunity and cause a form of severe vasculitis that affects capillaries in the kidney and that can destroy the organ (pages 1088–1096).
Cees G.M. Kallenberg is in the Department of
Rheumatology and Clinical Immunology, Coen A.
Stegeman is in the Department of Nephrology and
Peter Heeringa is in the Department of Medical
Biology, University Medical Center Groningen,
University of Groningen, Hanzeplein, P.O. Box
30.001, Groningen 9700RB, The Netherlands.
e-mail: [email protected]
Systemic vasculitides comprise a group of idiopathic disorders characterized by inflam-mation of vessel walls1. In many small-vessel vasculitides, such as Henoch Schönlein pur-pura and cryoglobulinemic vasculitis, immune complexes underlie the vascular inflammation. In other cases, however, immune deposits are not detected or are detected at low levels in the lesion tissue. In this issue of Nature Medicine, Kain et al.2 begin to uncover a mechanism behind these harder-to-crack pauci-immune small-vessel vasculitides.
The findings suggest that infection with a Gram-negative bacterium such as E. coli may trigger disease in susceptible individuals by inducing the production of antibodies to a human protein expressed on neutrophils, lyso-somal membrane protein-2 (LAMP-2). These antibodies activate neutrophils that, in turn, may erode the vasculature.
New insights and therapeutic approaches are needed for the relatively rare but deadly pauci-immune small-vessel vasculitides, which include Wegener’s granulomatosis, microscopic polyangiitis, renal limited vasculitis and Churg-
Strauss syndrome3. The kidneys are frequently affected in these conditions. Without immedi-ate and strong immunosuppressive treatment, mortality is extremely high, and, even with treatment, mortality goes up to 35% within five years. As relapses frequently occur, long-term treatment is necessary, which can result in therapy-related illness and death.
Major advances in the understanding and diagnosis of these pauci-immune vasculitides came from the detection of autoantibodies directed against neutrophil constituents in the majority of individuals with Wegener’s granu-lomatosis and microscopic polyangiitis3,4. These antineutrophil cytoplasmic autoantibodies (ANCA) are directed either to proteinase-3 in most individuals with Wegener’s granuloma-tosis or to myeloperoxidase in the majority of individuals with other forms4. Levels of ANCA follow disease activity, but this relationship is far from perfect5. In vitro, ANCA are able to activate primed neutrophils, which, when they contact endothelial cells, can induce endothe-lial damage4. The most convincing argument for a pathogenetic role of ANCA comes from in vivo experimental work. Xiao et al.6 have shown that mice injected with mouse antibod-ies to myeloperoxidase developed (focal) pauci- immune vasculitis, particularly in kidneys. However, passive transfer of mouse or rat anti-bodies to proteinase-3 in mice did not result in a relevant animal model of proteinase-3–specific ANCA–associated Wegener’s granulomatosis7,8. So, many questions regarding the etiopathogen-
esis of the ANCA-associated vasculitides (AAVs) are still open.
In the current work, Kain et al.2 confirmed an observation previously reported by the same group9. They found that individuals with AAVs and renal involvement produce ANCA directed against LAMP-2 (ref. 9)—a heavily glycosylated type 1 membrane protein expressed by many cell types, including neutrophils and endothelial cells, that is involved in cellular adhesion and homeostasis.
They went on to provide evidence that anti-bodies to human LAMP-2 have pathogenetic potential2. They showed that these antibodies activate neutrophils and cause apoptosis of endothelial cells in vitro2. When injected into rats, the antibodies induced pauci-immune necrotizing crescentic glomerulonephritis, the renal histological hallmark of pauci-immune small-vessel vasculitides.
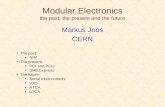
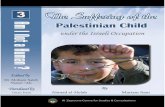
More importantly, the authors showed that a major epitope of human LAMP-2 recognized by the autoantibodies has strong homology with FimH, a bacterial adhesin of common Gram-negative bacteria. When rats were immunized with FimH, most developed both cross-reac-tive antibodies to LAMP-2 and pauci-immune NCGN (Fig. 1). The data collectively suggest that bacterial infection, in a susceptible person, may induce autoantibodies that will result in pauci-immune vasculitis in the kidney.
How should these results be interpreted? The data suggest that antibodies to human LAMP-2 should be included as a diagnostic test when
©20
08 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine

n e w s a n d v i e w s
renal pauci-immune vasculitis is suspected. The sensitivity of the autoantibodies for detect-ing pauci-immune glomerulonephritis seems at least as good as proteinase-3–specific ANCA and myeloperoxidase-specific ANCA. But ques-tions remain concerning the antibodies’ speci-ficity: antibodies to human LAMP-2 were also detected in some individuals with systemic lupus erythematosus or Goodpasture’s syndrome who were concomitantly positive for ANCA. Larger groups of patients with a variety of diseases that could be considered as part of the differential diagnosis of vasculitis, as well as patients with nonrenal AAVs, should be tested for antibodies to human LAMP-2. Furthermore, longitudi-nal studies should be performed to assess the relation between levels of antibodies to human LAMP-2 and disease activity in individuals with vasculitis to establish pathogenetic role in human disease.
The findings suggest that antibodies to human LAMP-2 may contribute to disease expression, but the reality is probably more complex. As the authors showed, antibodies to human LAMP-2 caused neutrophil activation and endothelial apoptosis in vitro, whereas pas-sive transfer of antibodies to human LAMP-2 into rats induced renal pathology similar to that seen in human pauci-immune small-vessel vasculitides2. However, in both experimental settings, either mouse or rabbit antibodies to human LAMP2 were used, and no data were provided on the pathogenic potential of human-derived antibodies to human LAMP-2. In addition, Wegener’s granulomatosis, as a paradigm of AAVs, is characterized not only by pauci-immune small-vessel vasculitis but also by granulomatous inflammation in vari-ous organs, particularly in the respiratory tract. Whether granulomatous inflammation was present in the experimental models using antibodies to human LAMP-2 is not clear.
So, the presence of antibody to human LAMP-2 alone cannot explain the full clinical expression of Wegener’s granulomatosis and microscopic polyangiitis. Given the obser-vation that in the majority of patients both ANCA and antibodies to humanLAMP-2 can be detected, the possibility exists that these autoantibodies act synergistically to cause full-blown vasculitis.
Perhaps the most intriguing implication of the new study is that it suggests that Gram-negative bacteria are involved in the etio-pathogenesis of AAVs2. Previous studies have also suggested that other bacterial agents are involved in AAVs, particularly in Wegener’s granulomatosis. Stegeman et al.10 showed that 63% of individuals with Wegener’s granulomatosis were chronic nasal carriers of Staphyloccous aureus, and carriage was
associated with a 7.16-fold increased risk for relapsing disease. Furthermore, maintenance treatment with the antibiotic co-trimoxazole reduces relapses of Wegener’s granulomato-sis11. Although it is not clear how S. aureus carriage might lead to Wegener’s granulo-matosis12, there is some suggestion that S. aureus–derived antigens could be involved in the development of ANCA for proteinase-3 via a complicated mechanism of protein complementarity13. In addition, the presence of certain superantigens from S. aureus is associated with disease activity in individu-als with AAV and positive for ANCA specific for proteinase-3 (ref. 14). So, S. aureus could be involved in induction of ANCA directed to specific proteinase-3 and expression of the associated disease.
Although Kain et al.2 present some data that infection with FimH-expressing Gram-negative bacteria preceded the clinical pre-sentation of pauci-immune small-vessel vasculitis, more data are needed to further establish this relationship. These vasculitides are rare conditions, whereas infections with Gram-negative bacteria are very common. So, additional, probably host-derived, factors are required for disease induction.
Despite these caveats, the study of Kain et al.2 provides major insight into the pathogen-esis of AAVs. The work shows that, besides
ANCA specific for proteinase-3 and ANCA specific for myeloperoxidase, autoantibodies to human LAMP-2 are present in individuals with these diseases. In addition, it strongly suggests a pathogenetic role for these latter antibodies. Most importantly, it suggests that, aside from S. aureus, Gram-negative bacteria may also be involved in autoantibody induc-tion. If confirmed and extended in future studies, these data could hopefully result in more specific and less toxic therapeutic regi-mens focusing on the elimination of one or more bacterial triggers.
1. Jennette, J.C. et al. Arthritis Rheum. 37, 187–192 (1994).
2. Kain, R. et al. Nat. Med. 14, 1088–1096 (2008)3. Jennette, J.C. & Falk, R.J. N. Engl. J. Med. 337, 1512–
1523 (1997).4. Kallenberg, C.G.M., Heeringa, P. & Stegeman, C.A. Nat.
Clin. Pract. Rheumatol. 2, 661–670 (2006).5. Boomsma, M.M. et al. Arthritis Rheum. 43, 2025–
2033 (2000).6. Xiao, H. et al. J. Clin. Invest. 110, 955–963 (2002).7. Pfister, H. et al. Blood 104, 1411–1418 (2004).8. van der Geld, Y.M., et al. Ann. Rheum. Dis. 66, 1679–
1682 (2007).9. Kain, R. et al. J. Exp. Med. 181, 585–597 (1995).10. Stegeman, C.A. et al. Ann. Intern. Med. 120, 12–17
(1994).11. Stegeman, C.A. et al. N. Engl. J. Med. 335, 16–20
(1996).12. Popa, E.R. & Cohen Tervaert, J.W. Intern. Med. 42,
771–780 (2003).13. Pendergraft, W.F., III et al. Nat. Med. 10, 72–79
(2004).14. Popa, E.R. et al. Rheumatology (Oxford) 46, 1029–
1033 (2007).
nature medicine volume 14 | number 10 | october 2008 1019
Infection with fimbriatedbacteria (e.g. Klebsiella pneumoniae, E. coli)
FimHaa 72–80
LAMP-2, P41–49 epitope
Anti–LAMP-2
Glomerularendothelium
E-selectinApoptosis Vasculitis
Neutrophil
ROS productionDegranulation
LAMP-2
Molecularmimicry
Figure 1 Human LAMP-2 induces glomerular endothelial injury. Infection with fimbriated bacteria induces generation of antibodies to an epitope shared by the bacterial adhesion FimH and human LAMP-2. Autoantibodies to LAMP-2 bind neutrophils and activate these cells, causing shape changes and degranulation. In addition, autoantibodies to LAMP-2 bind glomerular endothelial cells, resulting in upregulation of E-selectin and eventually causing endothelial cell apoptosis. Ultimately, these processes lead to glomerular capillary injury progressing to focal necrotizing glomerulonephritis.
Kim
Cae
sar
©20
08 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine