
Association of Plasma γ′ Fibrinogen With Incident...
16
2700 P lasma fibrinogen is a coagulation factor and an acute- phase inflammatory marker that has been implicated in the pathophysiology of cardiovascular disease (CVD). 1 Several epidemiological studies have shown an independent, positive association between elevated levels of fibrinogen and CVD, with hypothesized mechanisms relating to increased plasma viscosity or the size and strength of thrombi. 1–4 However, a study using Mendelian randomization suggests that the epi- demiological association may not be causal. 5 Fibrinogen is also associated positively with several established CVD risk factors, so elevated fibrinogen may be one pathway by which these CVD risk factors exert their influence on the cardiovas- cular system. 4,6,7 Fibrinogen is a 6-chain molecule containing 2 copies each of the Aα, Bβ, and γ chains, with the latter having 2 isoforms γA and γ′ arising from alternative mRNA processing. 8,9 γ′ fibrinogen constitutes ≈7% of plasma fibrinogen with higher levels found among individuals with pathological condi- tions.. 9 Recent evidence suggests that higher plasma concen- trations of γ′ fibrinogen yield thrombi that are resistant to fibrinolysis, 8,9 which provides novel hypotheses to explain the relationship between fibrinogen and CVD events. 10 Accordingly, some studies have observed a positive associa- tion between γ′ fibrinogen and atherothrombotic events inde- pendent of total plasma fibrinogen levels. 11–15 However, the retrospective or cross-sectional design of these studies that were conducted among individuals already diagnosed with CVD events hampers the determination of the temporality of this association, and a prospective design could reveal new perspectives on the association of γ′ fibrinogen with CVD events. Therefore, the aim of this study was to prospectively inves- tigate the association of plasma γ′ fibrinogen with the inci- dence of multiple CVD end points, independent of established CVD risk factors, total fibrinogen, and other inflammatory markers, among participants enrolled in the Atherosclerosis Risk in Communities (ARIC) study, a biracial cohort of white and black men and women. Materials and Methods Materials and Methods are available in the online-only Data Supplement. © 2015 American Heart Association, Inc. Arterioscler Thromb Vasc Biol is available at http://atvb.ahajournals.org DOI: 10.1161/ATVBAHA.115.306284 Objectives—To prospectively examine the association of plasma γ′ fibrinogen with the incidence of multiple cardiovascular disease (CVD) end points, independent of established CVD risk factors, total fibrinogen, and other inflammatory markers. Approach and Results—The Atherosclerosis Risk in Communities (ARIC) study measured γ′ fibrinogen by enzyme-linked immunosorbent assay in stored plasma samples from 1993 to 1995 and related levels in 10 601 adults to incident CVD end points (coronary heart disease [n=1603], ischemic stroke [n=548], peripheral artery disease [n=599], heart failure [n=1411], and CVD mortality [n=705]) through 2012 (median follow-up, 18 years). In Cox models accounting for established CVD risk factors and total fibrinogen levels, γ′ fibrinogen was associated positively with peripheral artery disease (hazard ratio [HR] per 1-SD [8.80 mg/dL] increment, 1.14 [1.04–1.24]), heart failure (HR, 1.06 [1.01–1.13]), and CVD deaths (HR, 1.12 [1.04–1.21]) but not with incident coronary heart disease (HR, 1.01 [0.96–1.07]) or ischemic stroke (HR, 0.98 [0.89–1.07]). Additional adjustment for C-reactive protein, however, eliminated the associations with peripheral artery disease and heart failure. Conclusions—These findings do not lend support to the hypothesis that γ′ fibrinogen influences CVD events through its prothrombotic properties. Rather, γ′ fibrinogen concentrations seem to reflect general inflammation that accompanies and may contribute to atherosclerotic CVD, instead of γ′ fibrinogen being a causal risk factor. (Arterioscler Thromb Vasc Biol. 2015;35:2700-2706. DOI: 10.1161/ATVBAHA.115.306284.) Key Words: cardiovascular ◼ coronary disease diseases ◼ epidemiology ◼ fibrinogen ◼ thrombosis Received on: July 24, 2015; final version accepted on: October 12, 2015. From the Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis. The online-only Data Supplement is available with this article at http://atvb.ahajournals.org/lookup/suppl/doi:10.1161/ATVBAHA.115.306284/-/DC1. Correspondence to Duke Appiah, PhD, Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, 1300 South 2nd St, Suite 300, Minneapolis, MN 55454. E-mail [email protected] Association of Plasma γ′ Fibrinogen With Incident Cardiovascular Disease The Atherosclerosis Risk in Communities (ARIC) Study Duke Appiah, Pamela J. Schreiner, Richard F. MacLehose, Aaron R. Folsom by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from by guest on May 29, 2018 http://atvb.ahajournals.org/ Downloaded from
Transcript of Association of Plasma γ′ Fibrinogen With Incident...
2700
Plasma fibrinogen is a coagulation factor and an acute-phase inflammatory marker that has been implicated in the
pathophysiology of cardiovascular disease (CVD).1 Several epidemiological studies have shown an independent, positive association between elevated levels of fibrinogen and CVD, with hypothesized mechanisms relating to increased plasma viscosity or the size and strength of thrombi.1–4 However, a study using Mendelian randomization suggests that the epi-demiological association may not be causal.5 Fibrinogen is also associated positively with several established CVD risk factors, so elevated fibrinogen may be one pathway by which these CVD risk factors exert their influence on the cardiovas-cular system.4,6,7
Fibrinogen is a 6-chain molecule containing 2 copies each of the Aα, Bβ, and γ chains, with the latter having 2 isoforms γA and γ′ arising from alternative mRNA processing.8,9 γ′ fibrinogen constitutes ≈7% of plasma fibrinogen with higher levels found among individuals with pathological condi-tions..9 Recent evidence suggests that higher plasma concen-trations of γ′ fibrinogen yield thrombi that are resistant to fibrinolysis,8,9 which provides novel hypotheses to explain
the relationship between fibrinogen and CVD events.10 Accordingly, some studies have observed a positive associa-tion between γ′ fibrinogen and atherothrombotic events inde-pendent of total plasma fibrinogen levels.11–15 However, the retrospective or cross-sectional design of these studies that were conducted among individuals already diagnosed with CVD events hampers the determination of the temporality of this association, and a prospective design could reveal new perspectives on the association of γ′ fibrinogen with CVD events.
Therefore, the aim of this study was to prospectively inves-tigate the association of plasma γ′ fibrinogen with the inci-dence of multiple CVD end points, independent of established CVD risk factors, total fibrinogen, and other inflammatory markers, among participants enrolled in the Atherosclerosis Risk in Communities (ARIC) study, a biracial cohort of white and black men and women.
Materials and MethodsMaterials and Methods are available in the online-only Data Supplement.
© 2015 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol is available at http://atvb.ahajournals.org DOI: 10.1161/ATVBAHA.115.306284
Objectives—To prospectively examine the association of plasma γ′ fibrinogen with the incidence of multiple cardiovascular disease (CVD) end points, independent of established CVD risk factors, total fibrinogen, and other inflammatory markers.
Approach and Results—The Atherosclerosis Risk in Communities (ARIC) study measured γ′ fibrinogen by enzyme-linked immunosorbent assay in stored plasma samples from 1993 to 1995 and related levels in 10 601 adults to incident CVD end points (coronary heart disease [n=1603], ischemic stroke [n=548], peripheral artery disease [n=599], heart failure [n=1411], and CVD mortality [n=705]) through 2012 (median follow-up, 18 years). In Cox models accounting for established CVD risk factors and total fibrinogen levels, γ′ fibrinogen was associated positively with peripheral artery disease (hazard ratio [HR] per 1-SD [8.80 mg/dL] increment, 1.14 [1.04–1.24]), heart failure (HR, 1.06 [1.01–1.13]), and CVD deaths (HR, 1.12 [1.04–1.21]) but not with incident coronary heart disease (HR, 1.01 [0.96–1.07]) or ischemic stroke (HR, 0.98 [0.89–1.07]). Additional adjustment for C-reactive protein, however, eliminated the associations with peripheral artery disease and heart failure.
Conclusions—These findings do not lend support to the hypothesis that γ′ fibrinogen influences CVD events through its prothrombotic properties. Rather, γ′ fibrinogen concentrations seem to reflect general inflammation that accompanies and may contribute to atherosclerotic CVD, instead of γ′ fibrinogen being a causal risk factor. (Arterioscler Thromb Vasc Biol. 2015;35:2700-2706. DOI: 10.1161/ATVBAHA.115.306284.)
Key Words: cardiovascular ◼ coronary disease diseases ◼ epidemiology ◼ fibrinogen ◼ thrombosis
Received on: July 24, 2015; final version accepted on: October 12, 2015.From the Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis.The online-only Data Supplement is available with this article at http://atvb.ahajournals.org/lookup/suppl/doi:10.1161/ATVBAHA.115.306284/-/DC1.Correspondence to Duke Appiah, PhD, Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, 1300 South
2nd St, Suite 300, Minneapolis, MN 55454. E-mail [email protected]
Association of Plasma γ′ Fibrinogen With Incident Cardiovascular Disease
The Atherosclerosis Risk in Communities (ARIC) Study
Duke Appiah, Pamela J. Schreiner, Richard F. MacLehose, Aaron R. Folsom
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
by guest on M
ay 29, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
by guest on M
ay 29, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
by guest on M
ay 29, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
by guest on M
ay 29, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
by guest on M
ay 29, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
Appiah et al γ′ Fibrinogen and Incident CVD 2701
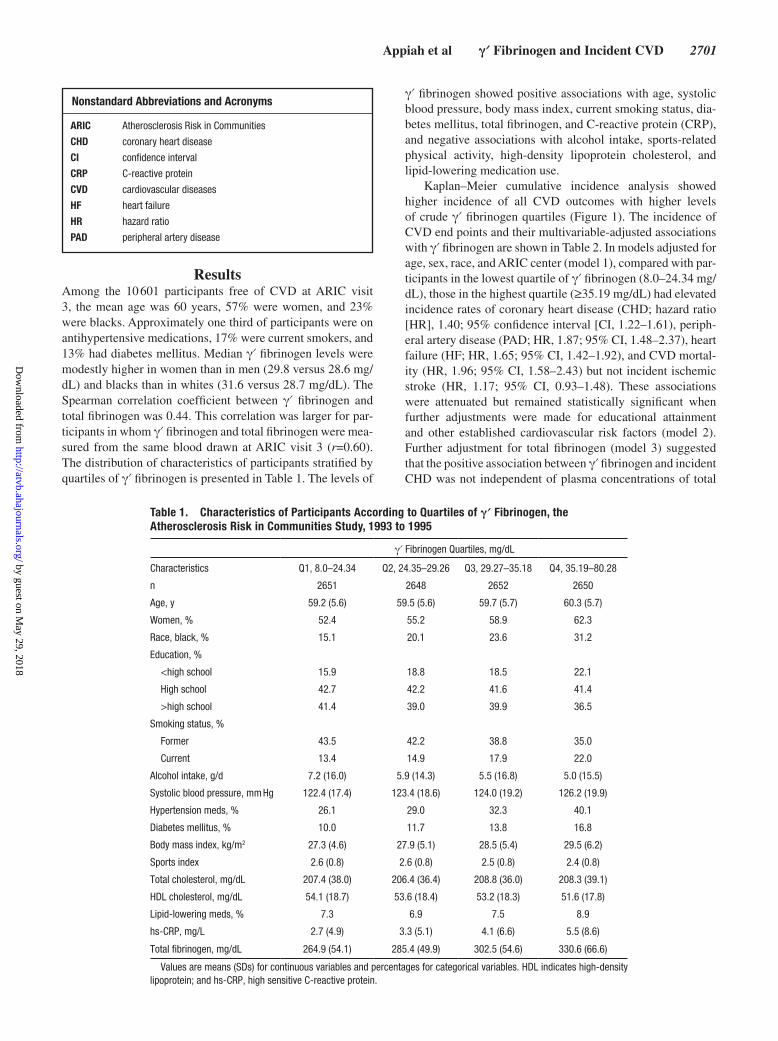
ResultsAmong the 10 601 participants free of CVD at ARIC visit 3, the mean age was 60 years, 57% were women, and 23% were blacks. Approximately one third of participants were on antihypertensive medications, 17% were current smokers, and 13% had diabetes mellitus. Median γ′ fibrinogen levels were modestly higher in women than in men (29.8 versus 28.6 mg/dL) and blacks than in whites (31.6 versus 28.7 mg/dL). The Spearman correlation coefficient between γ′ fibrinogen and total fibrinogen was 0.44. This correlation was larger for par-ticipants in whom γ′ fibrinogen and total fibrinogen were mea-sured from the same blood drawn at ARIC visit 3 (r=0.60). The distribution of characteristics of participants stratified by quartiles of γ′ fibrinogen is presented in Table 1. The levels of
γ′ fibrinogen showed positive associations with age, systolic blood pressure, body mass index, current smoking status, dia-betes mellitus, total fibrinogen, and C-reactive protein (CRP), and negative associations with alcohol intake, sports-related physical activity, high-density lipoprotein cholesterol, and lipid-lowering medication use.
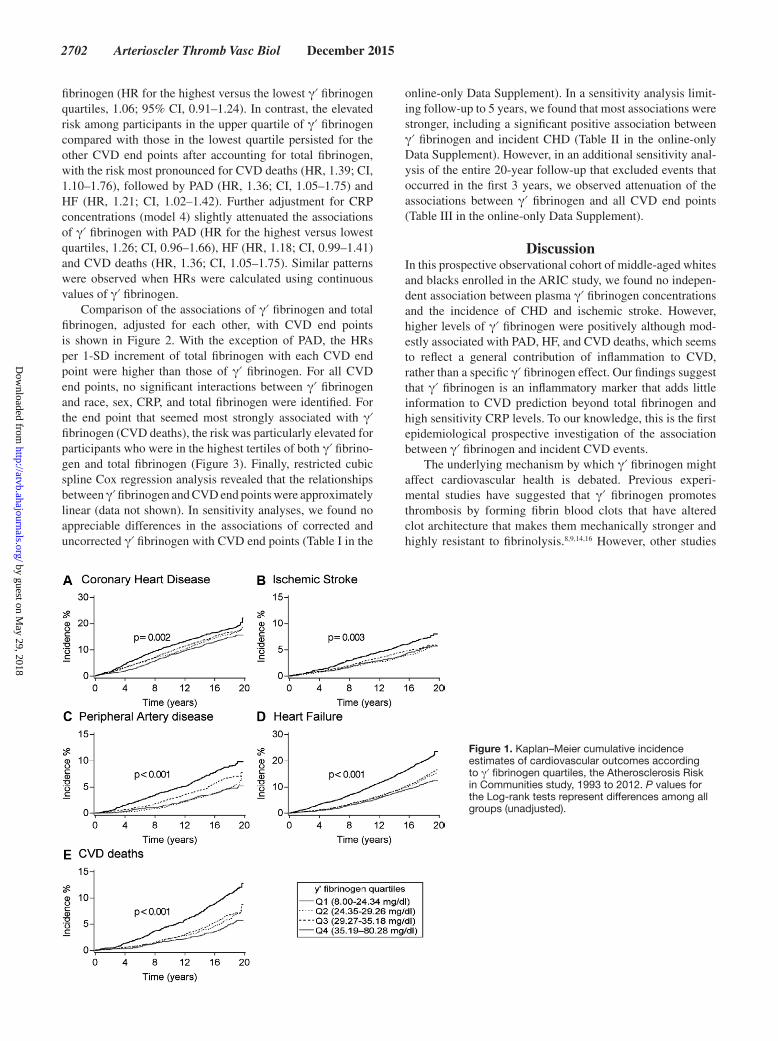
Kaplan–Meier cumulative incidence analysis showed higher incidence of all CVD outcomes with higher levels of crude γ′ fibrinogen quartiles (Figure 1). The incidence of CVD end points and their multivariable-adjusted associations with γ′ fibrinogen are shown in Table 2. In models adjusted for age, sex, race, and ARIC center (model 1), compared with par-ticipants in the lowest quartile of γ′ fibrinogen (8.0–24.34 mg/dL), those in the highest quartile (≥35.19 mg/dL) had elevated incidence rates of coronary heart disease (CHD; hazard ratio [HR], 1.40; 95% confidence interval [CI, 1.22–1.61), periph-eral artery disease (PAD; HR, 1.87; 95% CI, 1.48–2.37), heart failure (HF; HR, 1.65; 95% CI, 1.42–1.92), and CVD mortal-ity (HR, 1.96; 95% CI, 1.58–2.43) but not incident ischemic stroke (HR, 1.17; 95% CI, 0.93–1.48). These associations were attenuated but remained statistically significant when further adjustments were made for educational attainment and other established cardiovascular risk factors (model 2). Further adjustment for total fibrinogen (model 3) suggested that the positive association between γ′ fibrinogen and incident CHD was not independent of plasma concentrations of total
Nonstandard Abbreviations and Acronyms
ARIC Atherosclerosis Risk in Communities
CHD coronary heart disease
CI confidence interval
CRP C-reactive protein
CVD cardiovascular diseases
HF heart failure
HR hazard ratio
PAD peripheral artery disease
Table 1. Characteristics of Participants According to Quartiles of γ′ Fibrinogen, the Atherosclerosis Risk in Communities Study, 1993 to 1995
γ′ Fibrinogen Quartiles, mg/dL
Characteristics Q1, 8.0–24.34 Q2, 24.35–29.26 Q3, 29.27–35.18 Q4, 35.19–80.28
n 2651 2648 2652 2650
Age, y 59.2 (5.6) 59.5 (5.6) 59.7 (5.7) 60.3 (5.7)
Women, % 52.4 55.2 58.9 62.3
Race, black, % 15.1 20.1 23.6 31.2
Education, %
<high school 15.9 18.8 18.5 22.1
High school 42.7 42.2 41.6 41.4
>high school 41.4 39.0 39.9 36.5
Smoking status, %
Former 43.5 42.2 38.8 35.0
Current 13.4 14.9 17.9 22.0
Alcohol intake, g/d 7.2 (16.0) 5.9 (14.3) 5.5 (16.8) 5.0 (15.5)
Systolic blood pressure, mm Hg 122.4 (17.4) 123.4 (18.6) 124.0 (19.2) 126.2 (19.9)
Hypertension meds, % 26.1 29.0 32.3 40.1
Diabetes mellitus, % 10.0 11.7 13.8 16.8
Body mass index, kg/m2 27.3 (4.6) 27.9 (5.1) 28.5 (5.4) 29.5 (6.2)
Sports index 2.6 (0.8) 2.6 (0.8) 2.5 (0.8) 2.4 (0.8)
Total cholesterol, mg/dL 207.4 (38.0) 206.4 (36.4) 208.8 (36.0) 208.3 (39.1)
HDL cholesterol, mg/dL 54.1 (18.7) 53.6 (18.4) 53.2 (18.3) 51.6 (17.8)
Lipid-lowering meds, % 7.3 6.9 7.5 8.9
hs-CRP, mg/L 2.7 (4.9) 3.3 (5.1) 4.1 (6.6) 5.5 (8.6)
Total fibrinogen, mg/dL 264.9 (54.1) 285.4 (49.9) 302.5 (54.6) 330.6 (66.6)
Values are means (SDs) for continuous variables and percentages for categorical variables. HDL indicates high-density lipoprotein; and hs-CRP, high sensitive C-reactive protein.
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
2702 Arterioscler Thromb Vasc Biol December 2015
fibrinogen (HR for the highest versus the lowest γ′ fibrinogen quartiles, 1.06; 95% CI, 0.91–1.24). In contrast, the elevated risk among participants in the upper quartile of γ′ fibrinogen compared with those in the lowest quartile persisted for the other CVD end points after accounting for total fibrinogen, with the risk most pronounced for CVD deaths (HR, 1.39; CI, 1.10–1.76), followed by PAD (HR, 1.36; CI, 1.05–1.75) and HF (HR, 1.21; CI, 1.02–1.42). Further adjustment for CRP concentrations (model 4) slightly attenuated the associations of γ′ fibrinogen with PAD (HR for the highest versus lowest quartiles, 1.26; CI, 0.96–1.66), HF (HR, 1.18; CI, 0.99–1.41) and CVD deaths (HR, 1.36; CI, 1.05–1.75). Similar patterns were observed when HRs were calculated using continuous values of γ′ fibrinogen.
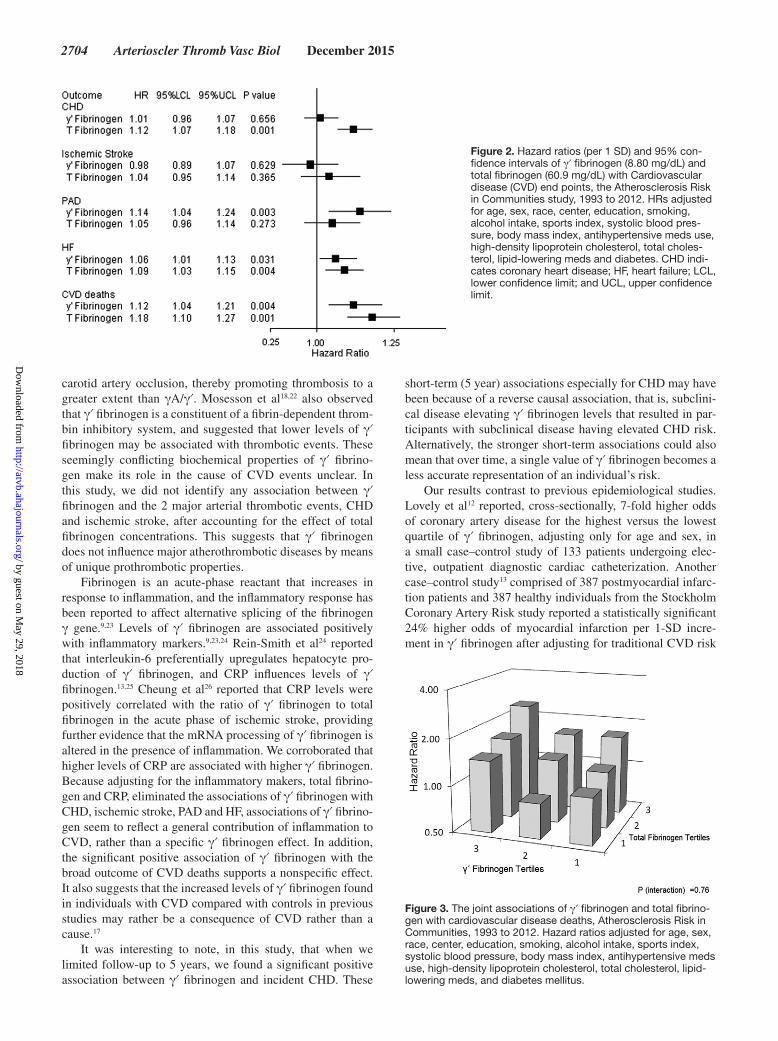
Comparison of the associations of γ′ fibrinogen and total fibrinogen, adjusted for each other, with CVD end points is shown in Figure 2. With the exception of PAD, the HRs per 1-SD increment of total fibrinogen with each CVD end point were higher than those of γ′ fibrinogen. For all CVD end points, no significant interactions between γ′ fibrinogen and race, sex, CRP, and total fibrinogen were identified. For the end point that seemed most strongly associated with γ′ fibrinogen (CVD deaths), the risk was particularly elevated for participants who were in the highest tertiles of both γ′ fibrino-gen and total fibrinogen (Figure 3). Finally, restricted cubic spline Cox regression analysis revealed that the relationships between γ′ fibrinogen and CVD end points were approximately linear (data not shown). In sensitivity analyses, we found no appreciable differences in the associations of corrected and uncorrected γ′ fibrinogen with CVD end points (Table I in the
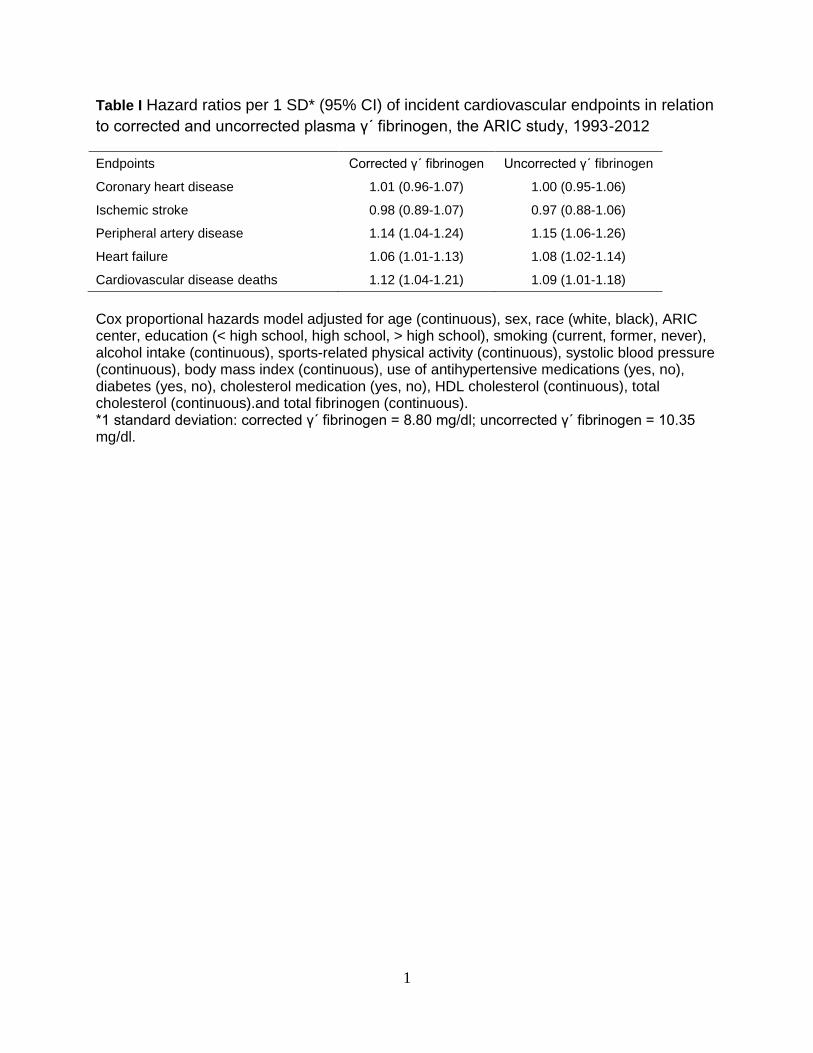
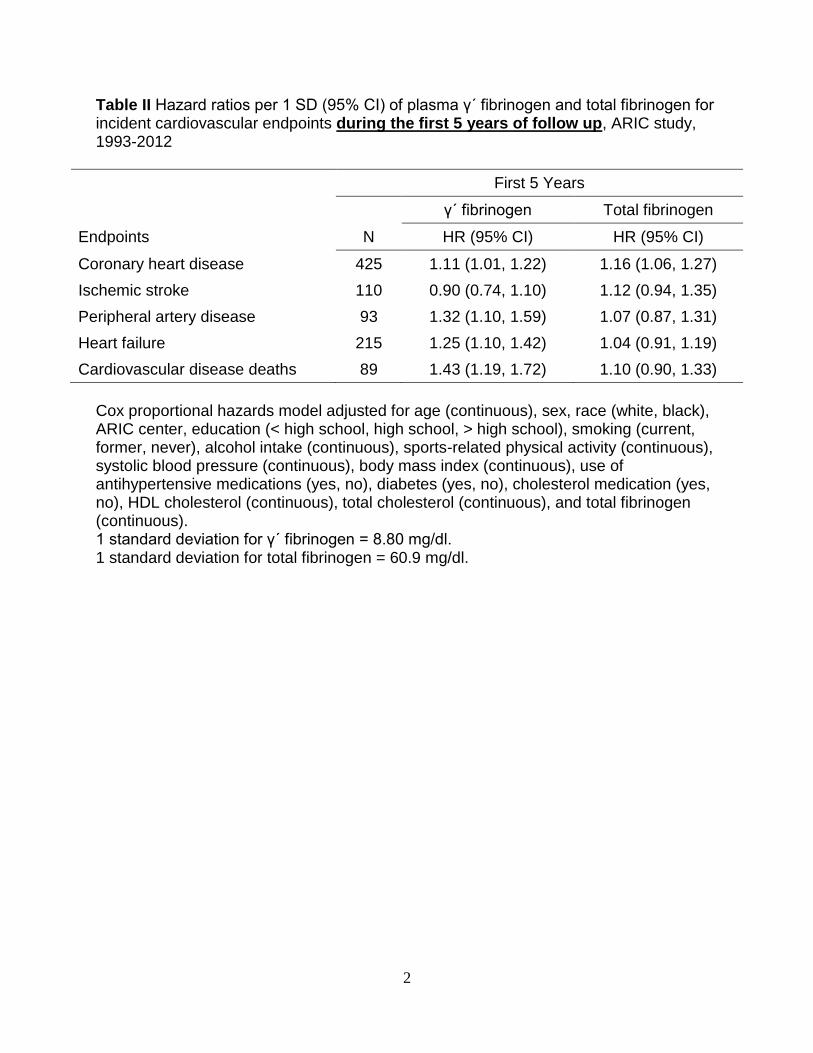
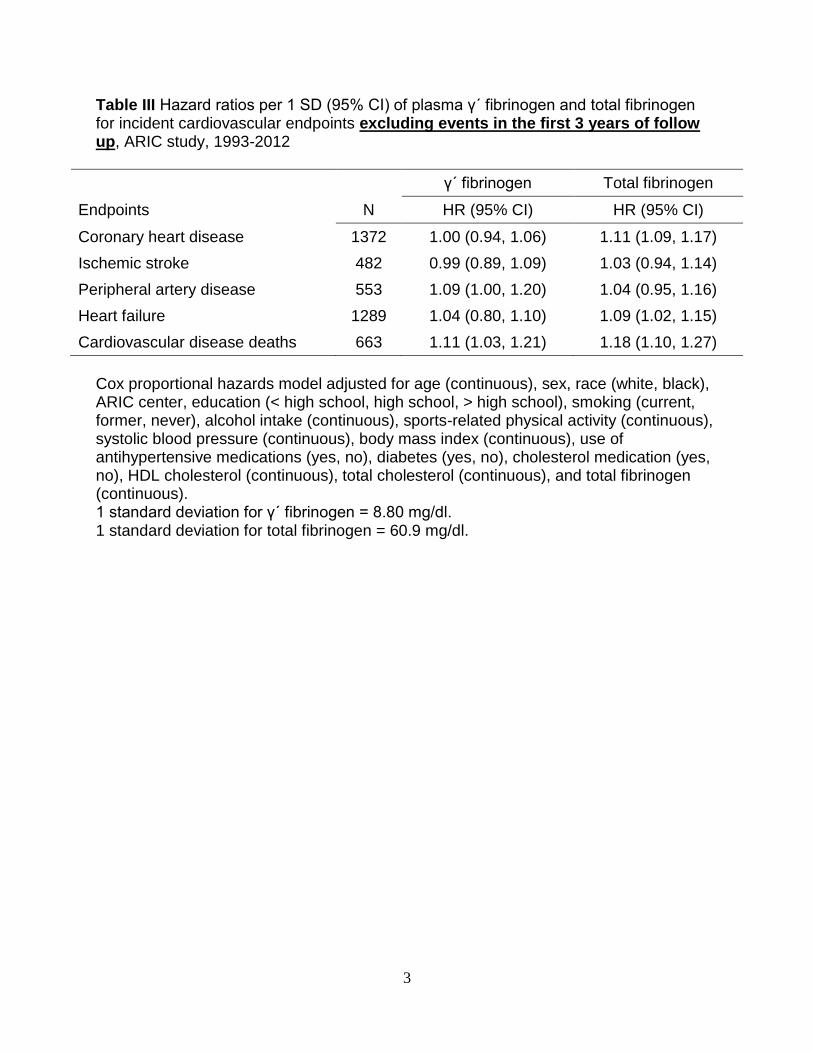
online-only Data Supplement). In a sensitivity analysis limit-ing follow-up to 5 years, we found that most associations were stronger, including a significant positive association between γ′ fibrinogen and incident CHD (Table II in the online-only Data Supplement). However, in an additional sensitivity anal-ysis of the entire 20-year follow-up that excluded events that occurred in the first 3 years, we observed attenuation of the associations between γ′ fibrinogen and all CVD end points (Table III in the online-only Data Supplement).
DiscussionIn this prospective observational cohort of middle-aged whites and blacks enrolled in the ARIC study, we found no indepen-dent association between plasma γ′ fibrinogen concentrations and the incidence of CHD and ischemic stroke. However, higher levels of γ′ fibrinogen were positively although mod-estly associated with PAD, HF, and CVD deaths, which seems to reflect a general contribution of inflammation to CVD, rather than a specific γ′ fibrinogen effect. Our findings suggest that γ′ fibrinogen is an inflammatory marker that adds little information to CVD prediction beyond total fibrinogen and high sensitivity CRP levels. To our knowledge, this is the first epidemiological prospective investigation of the association between γ′ fibrinogen and incident CVD events.
The underlying mechanism by which γ′ fibrinogen might affect cardiovascular health is debated. Previous experi-mental studies have suggested that γ′ fibrinogen promotes thrombosis by forming fibrin blood clots that have altered clot architecture that makes them mechanically stronger and highly resistant to fibrinolysis.8,9,14,16 However, other studies
Figure 1. Kaplan–Meier cumulative incidence estimates of cardiovascular outcomes according to γ′ fibrinogen quartiles, the Atherosclerosis Risk in Communities study, 1993 to 2012. P values for the Log-rank tests represent differences among all groups (unadjusted).
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
Appiah et al γ′ Fibrinogen and Incident CVD 2703
suggest that γ′ fibrinogen is antithrombotic and exhibits anticoagulant properties because of its ability to sequester thrombin.17 Recent studies observed that that γ′ fibrinogen has high-affinity binding sites for thrombin exosite II, which inhibits thrombin-mediated platelet activation and reduces
fibrinopeptide B cleavage and factor VIII activation.17–21 Accordingly, Walton et al17 reported that γ′ fibrinogen did not promote acute arterial thrombosis in mice and revealed that the more dominant isoform of the fibrinogen γ chain, γA/γA, increased fibrin formation rates and shortened the time to
Table 2. Hazard Ratios (95% Confidence Interval) of Incident Cardiovascular Outcomes in Relationship With Plasma γ′ Fibrinogen, the Atherosclerosis Risk in Communities Study, 1993 to 2012
γ′ Fibrinogen Quartiles, mg/dL
Ptrend
Continuous
Q1, 8.0–24.34 Q2, 24.35–29.26 Q3, 29.27–35.18 Q4, 35.19–80.28 1-SD Increment*
CHD
Events, n 359 393 407 444 1603
Incidence rate† 8.6 (7.8–9.6) 9.6 (8.7–10.6) 9.9 (9.0–10.9) 11.3 (10.3–12.4) 9.8 (9.4–10.3)
Model 1 1 (referent) 1.12 (0.97–1.30) 1.20 (1.04–1.38) 1.40 (1.22–1.61) 0.001 1.14 (1.08–1.19)
Model 2 1 (referent) 1.11 (0.96–1.28) 1.08 (0.93–1.25) 1.18 (1.02–1.37) 0.040 1.05 (1.00–1.11)
Model 3 1 (referent) 1.07 (0.93–1.24) 1.01 (0.87–1.17) 1.06 (0.91–1.24) 0.816 1.01 (0.96–1.07)
Model 4 1 (referent) 1.10 (0.94–1.28) 1.02 (0.88–1.20) 1.04 (0.89–1.23) 0.847 1.00 (0.94–1.06)
Ischemic stroke
Events, n 127 120 132 169 548
Incidence rate† 2.9 (2.5–3.5) 2.8 (2.3–3.3) 3.1 (2.6–3.6) 4.1 (3.5–4.7) 3.2 (2.9–3.5)
Model 1 1 (referent) 0.90 (0.70–1.16) 0.95 (0.75–1.22) 1.17 (0.93–1.48) 0.049 1.11 (1.02–1.20)
Model 2 1 (referent) 0.89 (0.69–1.15) 0.86 (0.69–1.10) 0.96 (0.76–1.22) 0.884 1.00 (0.92–1.09)
Model 3 1 (referent) 0.86 (0.67–1.11) 0.84 (0.65–1.08) 0.89 (0.69–1.16) 0.397 0.98 (0.89–1.07)
Model 4 1 (referent) 0.90 (0.69–1.17) 0.82 (0.63–1.08) 0.87 (0.66–1.15) 0.352 0.97 (0.87–1.07)
PAD
Events, n 111 117 160 211 599
Incidence rate† 2.5 (2.1–3.1) 2.7 (2.2–3.2) 3.7 (3.2–4.3) 5.1 (4.5–5.8) 3.5 (3.2–3.8)
Model 1 1 (referent) 1.02 (0.79–1.33) 1.40 (1.10–1.78) 1.87 (1.48–2.37) 0.001 1.30 (1.20–1.40)
Model 2 1 (referent) 0.97 (0.74–1.26) 1.20 (0.94–1.54) 1.43 (1.13–1.82) 0.001 1.16 (1.07–1.25)
Model 3 1 (referent) 0.95 (0.73–1.25) 1.17 (0.91–1.50) 1.36 (1.05–1.75) 0.042 1.14 (1.04–1.24)
Model 4 1 (referent) 1.00 (0.76–1.32) 1.16 (0.89–1.51) 1.26 (0.96–1.66) 0.050 1.09 (0.99–1.19)
Heart failure
Events, n 272 317 336 486 1411
Incidence rate† 6.3 (5.6–7.1) 7.4 (6.7–8.3) 7.9 (7.1–8.8) 12.1 (11.0–13.2) 8.4 (7.9–8.8)
Model 1 1 (referent) 1.12 (0.95–1.32) 1.14 (0.97–1.34) 1.65 (1.42–1.92) 0.001 1.23 (1.17–1.30)
Model 2 1 (referent) 1.06 (0.90–1.25) 0.99 (0.84–1.16) 1.30 (1.11–1.52) 0.001 1.10 (1.04–1.15)
Model 3 1 (referent) 1.04 (0.88–1.23) 0.93 (0.79–1.11) 1.21 (1.02–1.42) 0.066 1.06 (1.01–1.13)
Model 4 1 (referent) 1.08 (0.91–1.28) 0.91 (0.76–1.09) 1.18 (0.99–1.41) 0.080 1.05 (0.99–1.12)
CVD deaths
Events, n 123 151 166 265 705
Incidence rate† 2.7 (2.3–3.3) 3.4 (2.9–4.0) 3.7 (3.2–4.3) 6.2 (5.5–7.0) 4.0 (3.7–4.3)
Model 1 1 (referent) 1.19 (0.94–1.51) 1.27 (1.00–1.60) 1.96 (1.58–2.43) 0.001 1.30 (1.21–1.39)
Model 2 1 (referent) 1.16 (0.91–1.46) 1.17 (0.92–1.48) 1.66 (1.33–2.08) 0.001 1.19 (1.11–1.28)
Model 3 1 (referent) 1.10 (0.86–1.40) 1.04 (0.81–1.32) 1.39 (1.10–1.76) 0.014 1.12 (1.04–1.21)
Model 4 1 (referent) 1.12 (0.87–1.45) 1.00 (0.77–1.30) 1.36 (1.05–1.75) 0.015 1.10 (1.01–1.20)
Model 1: Cox proportional hazards model adjusted for age (continuous), sex, race (white and black), and ARIC center. Model 2: model 1 additionally adjusted for education (<high school, high school, and >high school), smoking (current, former, and never), alcohol intake (continuous), sports index (continuous), systolic blood pressure (continuous), body mass index (continuous), use of antihypertensive medications (yes and no), diabetes mellitus (yes and no), cholesterol medication (yes and no), high-density cholesterol (continuous), and total cholesterol (continuous). Model 3: model 2 additionally adjusted for total fibrinogen (continuous). Model 4: model 3 additionally adjusted for high sensitivity C-reactive protein (continuous). CHD indicates coronary heart disease; CVD, cardiovascular disease; and PAD, peripheral artery disease.
*1 SD=8.80 mg/dL.†Unadjusted incidence rate per 1000 person-years with 95% confidence intervals.
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
2704 Arterioscler Thromb Vasc Biol December 2015
carotid artery occlusion, thereby promoting thrombosis to a greater extent than γA/γ′. Mosesson et al18,22 also observed that γ′ fibrinogen is a constituent of a fibrin-dependent throm-bin inhibitory system, and suggested that lower levels of γ′ fibrinogen may be associated with thrombotic events. These seemingly conflicting biochemical properties of γ′ fibrino-gen make its role in the cause of CVD events unclear. In this study, we did not identify any association between γ′ fibrinogen and the 2 major arterial thrombotic events, CHD and ischemic stroke, after accounting for the effect of total fibrinogen concentrations. This suggests that γ′ fibrinogen does not influence major atherothrombotic diseases by means of unique prothrombotic properties.
Fibrinogen is an acute-phase reactant that increases in response to inflammation, and the inflammatory response has been reported to affect alternative splicing of the fibrinogen γ gene.9,23 Levels of γ′ fibrinogen are associated positively with inflammatory markers.9,23,24 Rein-Smith et al24 reported that interleukin-6 preferentially upregulates hepatocyte pro-duction of γ′ fibrinogen, and CRP influences levels of γ′ fibrinogen.13,25 Cheung et al26 reported that CRP levels were positively correlated with the ratio of γ′ fibrinogen to total fibrinogen in the acute phase of ischemic stroke, providing further evidence that the mRNA processing of γ′ fibrinogen is altered in the presence of inflammation. We corroborated that higher levels of CRP are associated with higher γ′ fibrinogen. Because adjusting for the inflammatory makers, total fibrino-gen and CRP, eliminated the associations of γ′ fibrinogen with CHD, ischemic stroke, PAD and HF, associations of γ′ fibrino-gen seem to reflect a general contribution of inflammation to CVD, rather than a specific γ′ fibrinogen effect. In addition, the significant positive association of γ′ fibrinogen with the broad outcome of CVD deaths supports a nonspecific effect. It also suggests that the increased levels of γ′ fibrinogen found in individuals with CVD compared with controls in previous studies may rather be a consequence of CVD rather than a cause.17
It was interesting to note, in this study, that when we limited follow-up to 5 years, we found a significant positive association between γ′ fibrinogen and incident CHD. These
short-term (5 year) associations especially for CHD may have been because of a reverse causal association, that is, subclini-cal disease elevating γ′ fibrinogen levels that resulted in par-ticipants with subclinical disease having elevated CHD risk. Alternatively, the stronger short-term associations could also mean that over time, a single value of γ′ fibrinogen becomes a less accurate representation of an individual’s risk.
Our results contrast to previous epidemiological studies. Lovely et al12 reported, cross-sectionally, 7-fold higher odds of coronary artery disease for the highest versus the lowest quartile of γ′ fibrinogen, adjusting only for age and sex, in a small case–control study of 133 patients undergoing elec-tive, outpatient diagnostic cardiac catheterization. Another case–control study13 comprised of 387 postmyocardial infarc-tion patients and 387 healthy individuals from the Stockholm Coronary Artery Risk study reported a statistically significant 24% higher odds of myocardial infarction per 1-SD incre-ment in γ′ fibrinogen after adjusting for traditional CVD risk
Figure 2. Hazard ratios (per 1 SD) and 95% con-fidence intervals of γ′ fibrinogen (8.80 mg/dL) and total fibrinogen (60.9 mg/dL) with Cardiovascular disease (CVD) end points, the Atherosclerosis Risk in Communities study, 1993 to 2012. HRs adjusted for age, sex, race, center, education, smoking, alcohol intake, sports index, systolic blood pres-sure, body mass index, antihypertensive meds use, high-density lipoprotein cholesterol, total choles-terol, lipid-lowering meds and diabetes. CHD indi-cates coronary heart disease; HF, heart failure; LCL, lower confidence limit; and UCL, upper confidence limit.
Figure 3. The joint associations of γ′ fibrinogen and total fibrino-gen with cardiovascular disease deaths, Atherosclerosis Risk in Communities, 1993 to 2012. Hazard ratios adjusted for age, sex, race, center, education, smoking, alcohol intake, sports index, systolic blood pressure, body mass index, antihypertensive meds use, high-density lipoprotein cholesterol, total cholesterol, lipid-lowering meds, and diabetes mellitus.
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from

Appiah et al γ′ Fibrinogen and Incident CVD 2705
factors and total fibrinogen. Similarly, cross-sectional results from the Framingham Heart Study Offspring Cohort14 showed a statistically significant 76% higher odds of prevalent myo-cardial infarction among participants in the highest tertile of γ′ fibrinogen compared with the lowest tertile after adjusting for established CVD risk factors. Data on the relationship between γ′ fibrinogen and ischemic stroke are sparse and con-flicting. van den Herik et al27 observed that individuals with ischemic stroke had elevated levels of γ′ fibrinogen than age- and sex-matched stroke-free controls, and each unit increase in γ′ fibrinogen was associated with 48% higher odds for unfavorable stroke outcome. Cheung et al15 identified elevated levels of γ′ fibrinogen in the acute phase of ischemic stroke that reduced to prestroke levels after 3 months. However, the Framingham Heart Study Offspring Cohort14 found no asso-ciation between γ′ fibrinogen and prevalent stroke (odds ratio, 1.42; CI, 0.68–2.95).
Possible explanations for these disparate results may be related to their study designs and inadequate control of the influence of total fibrinogen and other inflammatory mark-ers. For instance, in the Framingham Heart Study Offspring Cohort,14 γ′ fibrinogen was positively associated with preva-lent CVD in models adjusted for established CVD risk factors, but additional control for total fibrinogen levels rendered the association nonsignificant. Furthermore, the cross-sectional or retrospective designs used by previous studies have greater likelihood of selection bias, as people who died of disease before the inception of such studies may have had different γ′ fibrinogen concentrations compared with survivors who were enrolled. Moreover, cross-sectional/retrospective studies lack the ability to determine whether elevated γ′ fibrinogen pre-ceded or followed the CVD event, as it was measured among cases who already had CVD.
This study has several notable strengths, including the use of a large population-based biracial sample, extensive assess-ment of CVD risk factors, physician-adjudicated CHD, and stroke events using standardized criteria, and 20 years of fol-low-up with low attrition. In addition, validated procedures to measure γ′ fibrinogen levels were used.
Limitations of this study should be considered when inter-preting our results. First, analyses were based on a single mea-sure of γ′ fibrinogen. Second, our quality control data showed that our γ′ fibrinogen measurements for whites had some down-ward drift, requiring us to adjust those γ′ fibrinogen values to be comparable with the stable and precise levels observed for blacks. Our corrections in γ′ fibrinogen were an attempt to adjust for the drift seen in the normal data. Sensitivity analy-ses revealed that corrected and uncorrected results were simi-lar. Because the ARIC study had only a single measure of γ′ fibrinogen on participants and there is no published long-term reliability coefficient in the literature, we could not address γ′ fibrinogen variation over time. Any misclassification of γ′ fibrinogen levels is likely to have been nondifferential with respect to our outcomes. Such errors would have biased our effect estimates toward the null (regression dilution), in expec-tation, and is one possible explanation for our findings. Third, we measured total fibrinogen and CRP from blood samples obtained 6 and 3 years, respectively, before the assessment
of γ′ fibrinogen, and these may not represent actual levels at visit 3. Because γ′ fibrinogen is moderately correlated with total fibrinogen and CRP, we deemed it necessarily to adjust for these inflammatory markers in our models to enhance our understanding of any potential underlying mechanisms for the association of γ′ fibrinogen with CVD end points. Fourth, the statistically nonsignificant findings of CHD and ischemic stroke may be because of inadequate power to detect a small effect. However, our study had high power (>0.8) for HRs of 1.2 for CHD and 1.4 for stroke. Finally, some CVD end points (eg, HF, PAD, and CVD mortality) relied on International Classification of Disease codes. However, in ARIC, a high validity for International Classification of Disease codes in identifying these CVD end points has been demonstrated.28
In summary, γ′ fibrinogen was associated positively with PAD, HF, and CVD deaths but not independently with incident CHD and ischemic stroke, after accounting for total fibrino-gen levels. With the exception of CVD deaths, these associa-tions were attenuated to marginal statistical significance when high sensitivity CRP was added to the model. Our findings are consistent with γ′ fibrinogen concentration reflecting the inflammation that accompanies and may contribute to athero-sclerotic CVD, rather than γ′ fibrinogen being a risk factor for CVD events.
AcknowledgmentsWe thank the staff and participants of the Atherosclerosis Risk in Communities (ARIC) study for their important contributions and Elaine Cornell for supervising γ′ fibrinogen measurements.
Sources of FundingThe Atherosclerosis Risk in Communities (ARIC) study is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute contracts (HHSN268201100005C, HHSN268201100006C, HHSN268201100007C, HHSN268201100008C, HHSN268-201100009C, HHSN268201100010C, HHSN268201100011C, and HHSN268201100012C). Dr Appiah was supported by National Heart, Lung, and Blood Institute training grant T32HL007779.
DisclosuresNone.
References 1. Danesh J, Lewington S, Thompson SG, et al; Fibrinogen Studies
Collaboration. Plasma fibrinogen level and the risk of major cardiovas-cular diseases and nonvascular mortality: an individual participant meta-analysis. JAMA. 2005;294:1799–1809.
2. Folsom AR, Wu KK, Rosamond WD, Sharrett AR, Chambless LE. Prospective study of hemostatic factors and incidence of coronary heart disease: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 1997;96:1102–1108.
3. Folsom AR, Rosamond WD, Shahar E, Cooper LS, Aleksic N, Nieto FJ, Rasmussen ML, Wu KK. Prospective study of markers of hemostatic func-tion with risk of ischemic stroke. The Atherosclerosis Risk in Communities (ARIC) study investigators. Circulation. 1999;100:736–742.
4. Stec JJ, Silbershatz H, Tofler GH, Matheney TH, Sutherland P, Lipinska I, Massaro JM, Wilson PF, Muller JE, D’Agostino RB Sr. Association of fibrinogen with cardiovascular risk factors and cardiovascular disease in the Framingham Offspring Population. Circulation. 2000;102:1634–1638.
5. Keavney B, Danesh J, Parish S, Palmer A, Clark S, Youngman L, Delépine M, Lathrop M, Peto R, Collins R. Fibrinogen and coronary heart dis-ease: test of causality by ‘Mendelian randomization’. Int J Epidemiol. 2006;35:935–943. doi: 10.1093/ije/dyl114.
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from

2706 Arterioscler Thromb Vasc Biol December 2015
6. Krobot K, Hense HW, Cremer P, Eberle E, Keil U. Determinants of plasma fibrinogen: relation to body weight, waist-to-hip ratio, smoking, alcohol, age, and sex. Results from the second MONICA Augsburg survey 1989–1990. Arterioscler Thromb. 1992;12:780–788.
7. Folsom AR, Wu KK, Davis CE, Conlan MG, Sorlie PD, Szklo M. Population correlates of plasma fibrinogen and factor VII, putative cardio-vascular risk factors. Atherosclerosis. 1991;91:191–205.
8. Lovely RS, Kazmierczak SC, Massaro JM, D’Agostino RB Sr, O’Donnell CJ, Farrell DH. Gamma’ fibrinogen: evaluation of a new assay for study of associations with cardiovascular disease. Clin Chem. 2010;56:781–788. doi: 10.1373/clinchem.2009.138347.
9. Farrell DH. γ’ fibrinogen as a novel marker of thrombotic disease. Clin Chem Lab Med. 2012;50:1903–1909. doi: 10.1515/cclm-2012-0005.
10. Kim PY, Stewart RJ, Lipson SM, Nesheim ME. The relative kinetics of clotting and lysis provide a biochemical rationale for the correla-tion between elevated fibrinogen and cardiovascular disease. J Thromb Haemost. 2007;5:1250–1256. doi: 10.1111/j.1538-7836.2007.02426.x.
11. Drouet L, Paolucci F, Pasqualini N, Laprade M, Ripoll L, Mazoyer E, Bal dit Sollier C, Vanhove N. Plasma gamma’/gamma fibrinogen ratio, a marker of arterial thrombotic activity: a new potential cardiovascular risk factor? Blood Coagul Fibrinolysis. 1999;10(suppl 1):S35–S39.
12. Lovely RS, Falls LA, Al-Mondhiry HA, Chambers CE, Sexton GJ, Ni H, Farrell DH. Association of gammaA/gamma’ fibrinogen levels and coro-nary artery disease. Thromb Haemost. 2002;88:26–31.
13. Mannila MN, Lovely RS, Kazmierczak SC, Eriksson P, Samnegård A, Farrell DH, Hamsten A, Silveira A. Elevated plasma fibrinogen gamma’ concentration is associated with myocardial infarction: effects of varia-tion in fibrinogen genes and environmental factors. J Thromb Haemost. 2007;5:766–773. doi: 10.1111/j.1538-7836.2007.02406.x.
14. Lovely RS, Yang Q, Massaro JM, Wang J, D’Agostino RB Sr, O’Donnell CJ, Shannon J, Farrell DH. Assessment of genetic determinants of the association of γ’ fibrinogen in relation to cardiovascular disease. Arterioscler Thromb Vasc Biol. 2011;31:2345–2352. doi: 10.1161/ATVBAHA.111.232710.
15. Cheung EY, Uitte de Willige S, Vos HL, Leebeek FW, Dippel DW, Bertina RM, de Maat MP. Fibrinogen gamma’ in ischemic stroke: a case-control study. Stroke. 2008;39:1033–1035. doi: 10.1161/STROKEAHA.107.495499.
16. Uitte de Willige S, Standeven KF, Philippou H, Ariens RA. The pleio-tropic role of the fibrinogen gamma’ chain in hemostasis. Blood. 2009;114:3994–4001.
17. Walton BL, Getz TM, Bergmeier W, Lin FC, Uitte de Willige S, Wolberg AS. The fibrinogen γA/γ’ isoform does not promote acute arterial
thrombosis in mice. J Thromb Haemost. 2014;12:680–689. doi: 10.1111/jth.12534.
18. Mosesson MW. Update on antithrombin I (fibrin). Thromb Haemost. 2007;98:105–108.
19. Cooper AV, Standeven KF, Ariëns RA. Fibrinogen gamma-chain splice variant gamma’ alters fibrin formation and structure. Blood. 2003;102:535–540. doi: 10.1182/blood-2002-10-3150.
20. Lovely RS, Rein CM, White TC, Jouihan SA, Boshkov LK, Bakke AC, McCarty OJ, Farrell DH. gammaA/gamma’ fibrinogen inhibits thrombin-induced platelet aggregation. Thromb Haemost. 2008;100:837–846.
21. Lovely RS, Boshkov LK, Marzec UM, Hanson SR, Farrell DH. Fibrinogen gamma’ chain carboxy terminal peptide selectively inhibits the intrinsic coagulation pathway. Br J Haematol. 2007;139:494–503. doi: 10.1111/j.1365-2141.2007.06825.x.
22. Mosesson MW, Hernandez I, Raife TJ, Medved L, Yakovlev S, Simpson-Haidaris PJ, Uitte de Willige S, Bertina RM. Plasma fibrinogen gamma’ chain content in the thrombotic microangiopathy syndrome. J Thromb Haemost. 2007;5:62–69. doi: 10.1111/j.1538-7836.2006.02270.x.
23. Alexander KS, Madden TE, Farrell DH. Association between γ’ fibrino-gen levels and inflammation. Thromb Haemost. 2011;105:605–609. doi: 10.1160/TH10-09-0626.
24. Rein-Smith CM, Anderson NW, Farrell DH. Differential regulation of fibrinogen γ chain splice isoforms by interleukin-6. Thromb Res. 2013;131:89–93. doi: 10.1016/j.thromres.2012.09.017.
25. Kotzé RC, Ariëns RA, de Lange Z, Pieters M. CVD risk factors are related to plasma fibrin clot properties independent of total and or γ’ fibrinogen concentration. Thromb Res. 2014;134:963–969. doi: 10.1016/j.thromres.2014.08.018.
26. Cheung EY, Vos HL, Kruip MJ, den Hertog HM, Jukema JW, de Maat MP. Elevated fibrinogen gamma’ ratio is associated with cardiovascular diseases and acute phase reaction but not with clinical outcome. Blood. 2009;114:4603–4604. doi: 10.1182/blood-2009-08-236240.
27. van den Herik EG, Cheung EY, de Lau LM, den Hertog HM, Leebeek FW, Dippel DW, Koudstaal PJ, de Maat MP. γ’/total fibrinogen ratio is asso-ciated with short-term outcome in ischaemic stroke. Thromb Haemost. 2011;105:430–434. doi: 10.1160/TH10-09-0569.
28. Rosamond WD, Chang PP, Baggett C, Johnson A, Bertoni AG, Shahar E, Deswal A, Heiss G, Chambless LE. Classification of heart failure in the atherosclerosis risk in communities (ARIC) study: a comparison of diagnostic criteria. Circ Heart Fail. 2012;5:152–159. doi: 10.1161/CIRCHEARTFAILURE.111.963199.
Cross-sectional and retrospective investigations have suggested that γ′ fibrinogen, a fibrinogen γ chain variant generated via alternative mRNA processing, is positively associated with atherothrombotic events. However, results from the Atherosclerosis Risk in Communities (ARIC) study, the first prospective study to assess this association, do not lend support to the hypothesis that γ′ fibrinogen influences cardio-vascular disease events through its prothrombotic properties. Rather, γ′ fibrinogen concentrations seem to reflect general inflammation that accompanies and may contribute to atherosclerotic cardiovascular disease, instead of γ′ fibrinogen being a causal risk factor.
Significance
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from
Duke Appiah, Pamela J. Schreiner, Richard F. MacLehose and Aaron R. FolsomAtherosclerosis Risk in Communities (ARIC) Study
Fibrinogen With Incident Cardiovascular Disease: The′γAssociation of Plasma
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2015 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/ATVBAHA.115.3062842015;
2015;35:2700-2706; originally published online October 22,Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/35/12/2700World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org/content/suppl/2015/10/22/ATVBAHA.115.306284.DC1Data Supplement (unedited) at:
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 29, 2018
http://atvb.ahajournals.org/D
ownloaded from

ONLINE SUPPLEMENTAL MATERIALS
Association of plasma gamma prime (γ´) fibrinogen with incident cardiovascular disease: the Atherosclerosis Risk in Communities (ARIC) study.
Duke Appiah, PhD; Pamela J. Schreiner, PhD; Richard F. MacLehose, PhD; Aaron R. Folsom, MD
1
Table I Hazard ratios per 1 SD* (95% CI) of incident cardiovascular endpoints in relation
to corrected and uncorrected plasma γ´ fibrinogen, the ARIC study, 1993-2012
Endpoints Corrected γ´ fibrinogen Uncorrected γ´ fibrinogen
Coronary heart disease 1.01 (0.96-1.07) 1.00 (0.95-1.06)
Ischemic stroke 0.98 (0.89-1.07) 0.97 (0.88-1.06)
Peripheral artery disease 1.14 (1.04-1.24) 1.15 (1.06-1.26)
Heart failure 1.06 (1.01-1.13) 1.08 (1.02-1.14)
Cardiovascular disease deaths 1.12 (1.04-1.21) 1.09 (1.01-1.18)
Cox proportional hazards model adjusted for age (continuous), sex, race (white, black), ARIC center, education (< high school, high school, > high school), smoking (current, former, never), alcohol intake (continuous), sports-related physical activity (continuous), systolic blood pressure (continuous), body mass index (continuous), use of antihypertensive medications (yes, no), diabetes (yes, no), cholesterol medication (yes, no), HDL cholesterol (continuous), total cholesterol (continuous).and total fibrinogen (continuous). *1 standard deviation: corrected γ´ fibrinogen = 8.80 mg/dl; uncorrected γ´ fibrinogen = 10.35 mg/dl.
2
Table II Hazard ratios per 1 SD (95% CI) of plasma γ´ fibrinogen and total fibrinogen for incident cardiovascular endpoints during the first 5 years of follow up, ARIC study, 1993-2012
First 5 Years
γ´ fibrinogen Total fibrinogen
Endpoints N HR (95% CI) HR (95% CI)
Coronary heart disease 425 1.11 (1.01, 1.22) 1.16 (1.06, 1.27)
Ischemic stroke 110 0.90 (0.74, 1.10) 1.12 (0.94, 1.35)
Peripheral artery disease 93 1.32 (1.10, 1.59) 1.07 (0.87, 1.31)
Heart failure 215 1.25 (1.10, 1.42) 1.04 (0.91, 1.19)
Cardiovascular disease deaths 89 1.43 (1.19, 1.72) 1.10 (0.90, 1.33)
Cox proportional hazards model adjusted for age (continuous), sex, race (white, black), ARIC center, education (< high school, high school, > high school), smoking (current, former, never), alcohol intake (continuous), sports-related physical activity (continuous), systolic blood pressure (continuous), body mass index (continuous), use of antihypertensive medications (yes, no), diabetes (yes, no), cholesterol medication (yes, no), HDL cholesterol (continuous), total cholesterol (continuous), and total fibrinogen (continuous). 1 standard deviation for γ´ fibrinogen = 8.80 mg/dl. 1 standard deviation for total fibrinogen = 60.9 mg/dl.
3
Table III Hazard ratios per 1 SD (95% CI) of plasma γ´ fibrinogen and total fibrinogen for incident cardiovascular endpoints excluding events in the first 3 years of follow up, ARIC study, 1993-2012
γ´ fibrinogen Total fibrinogen
Endpoints N HR (95% CI) HR (95% CI)
Coronary heart disease 1372 1.00 (0.94, 1.06) 1.11 (1.09, 1.17)
Ischemic stroke 482 0.99 (0.89, 1.09) 1.03 (0.94, 1.14)
Peripheral artery disease 553 1.09 (1.00, 1.20) 1.04 (0.95, 1.16)
Heart failure 1289 1.04 (0.80, 1.10) 1.09 (1.02, 1.15)
Cardiovascular disease deaths 663 1.11 (1.03, 1.21) 1.18 (1.10, 1.27)
Cox proportional hazards model adjusted for age (continuous), sex, race (white, black), ARIC center, education (< high school, high school, > high school), smoking (current, former, never), alcohol intake (continuous), sports-related physical activity (continuous), systolic blood pressure (continuous), body mass index (continuous), use of antihypertensive medications (yes, no), diabetes (yes, no), cholesterol medication (yes, no), HDL cholesterol (continuous), total cholesterol (continuous), and total fibrinogen (continuous). 1 standard deviation for γ´ fibrinogen = 8.80 mg/dl. 1 standard deviation for total fibrinogen = 60.9 mg/dl.
1
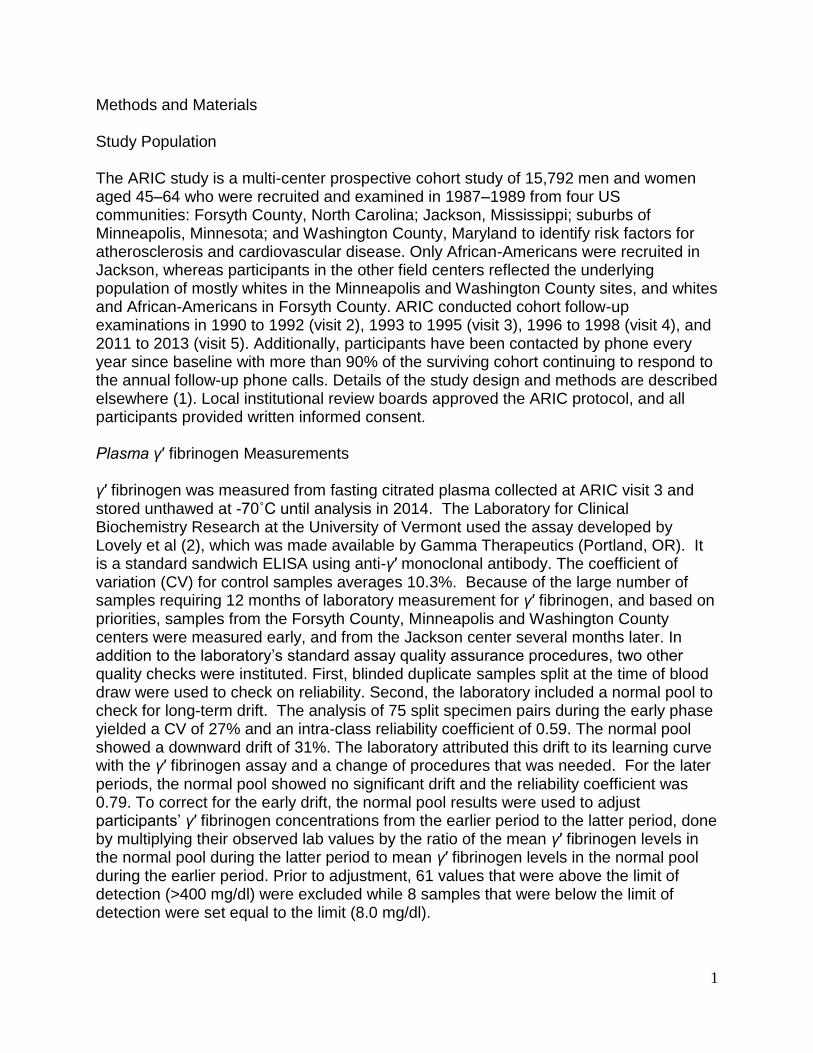
Methods and Materials Study Population The ARIC study is a multi-center prospective cohort study of 15,792 men and women aged 45–64 who were recruited and examined in 1987–1989 from four US communities: Forsyth County, North Carolina; Jackson, Mississippi; suburbs of Minneapolis, Minnesota; and Washington County, Maryland to identify risk factors for atherosclerosis and cardiovascular disease. Only African-Americans were recruited in Jackson, whereas participants in the other field centers reflected the underlying population of mostly whites in the Minneapolis and Washington County sites, and whites and African-Americans in Forsyth County. ARIC conducted cohort follow-up examinations in 1990 to 1992 (visit 2), 1993 to 1995 (visit 3), 1996 to 1998 (visit 4), and 2011 to 2013 (visit 5). Additionally, participants have been contacted by phone every year since baseline with more than 90% of the surviving cohort continuing to respond to the annual follow-up phone calls. Details of the study design and methods are described elsewhere (1). Local institutional review boards approved the ARIC protocol, and all participants provided written informed consent. Plasma γ′ fibrinogen Measurements γ′ fibrinogen was measured from fasting citrated plasma collected at ARIC visit 3 and stored unthawed at -70˚C until analysis in 2014. The Laboratory for Clinical Biochemistry Research at the University of Vermont used the assay developed by Lovely et al (2), which was made available by Gamma Therapeutics (Portland, OR). It is a standard sandwich ELISA using anti-γ′ monoclonal antibody. The coefficient of variation (CV) for control samples averages 10.3%. Because of the large number of samples requiring 12 months of laboratory measurement for γ′ fibrinogen, and based on priorities, samples from the Forsyth County, Minneapolis and Washington County centers were measured early, and from the Jackson center several months later. In addition to the laboratory’s standard assay quality assurance procedures, two other quality checks were instituted. First, blinded duplicate samples split at the time of blood draw were used to check on reliability. Second, the laboratory included a normal pool to check for long-term drift. The analysis of 75 split specimen pairs during the early phase yielded a CV of 27% and an intra-class reliability coefficient of 0.59. The normal pool showed a downward drift of 31%. The laboratory attributed this drift to its learning curve with the γ′ fibrinogen assay and a change of procedures that was needed. For the later periods, the normal pool showed no significant drift and the reliability coefficient was 0.79. To correct for the early drift, the normal pool results were used to adjust participants’ γ′ fibrinogen concentrations from the earlier period to the latter period, done by multiplying their observed lab values by the ratio of the mean γ′ fibrinogen levels in the normal pool during the latter period to mean γ′ fibrinogen levels in the normal pool during the earlier period. Prior to adjustment, 61 values that were above the limit of detection (>400 mg/dl) were excluded while 8 samples that were below the limit of detection were set equal to the limit (8.0 mg/dl).
2
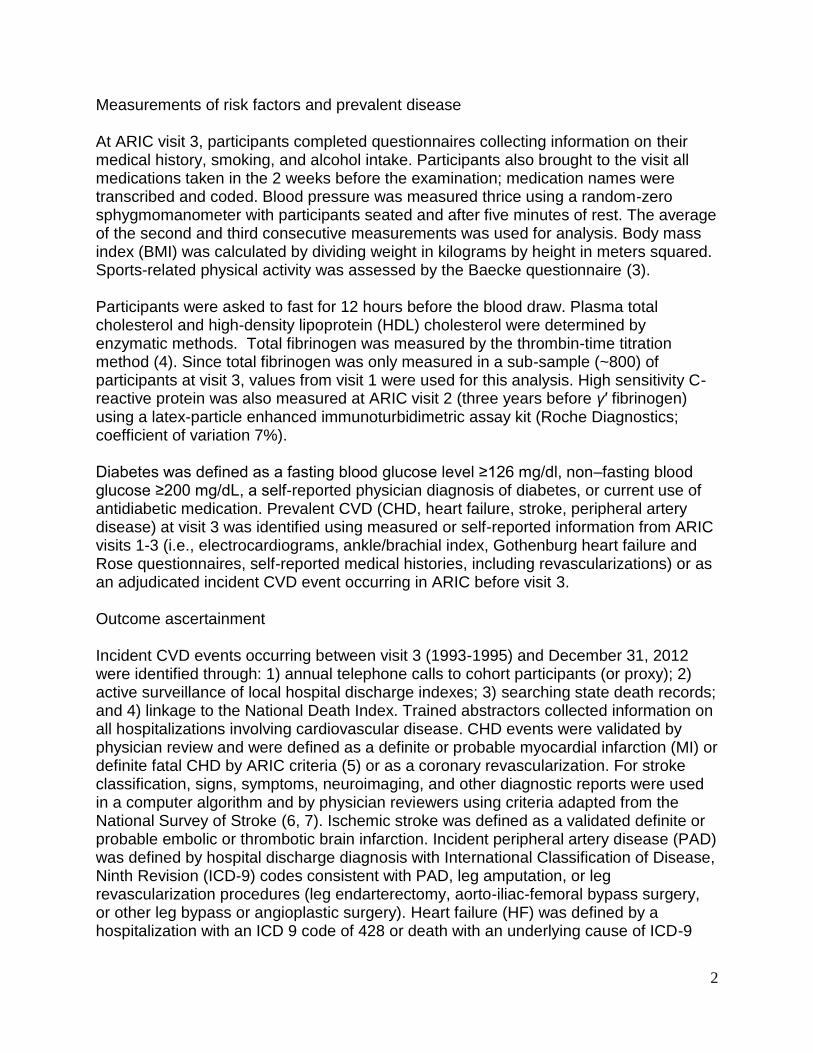
Measurements of risk factors and prevalent disease At ARIC visit 3, participants completed questionnaires collecting information on their medical history, smoking, and alcohol intake. Participants also brought to the visit all medications taken in the 2 weeks before the examination; medication names were transcribed and coded. Blood pressure was measured thrice using a random-zero sphygmomanometer with participants seated and after five minutes of rest. The average of the second and third consecutive measurements was used for analysis. Body mass index (BMI) was calculated by dividing weight in kilograms by height in meters squared. Sports-related physical activity was assessed by the Baecke questionnaire (3). Participants were asked to fast for 12 hours before the blood draw. Plasma total cholesterol and high-density lipoprotein (HDL) cholesterol were determined by enzymatic methods. Total fibrinogen was measured by the thrombin-time titration method (4). Since total fibrinogen was only measured in a sub-sample (~800) of participants at visit 3, values from visit 1 were used for this analysis. High sensitivity C-reactive protein was also measured at ARIC visit 2 (three years before γ′ fibrinogen) using a latex-particle enhanced immunoturbidimetric assay kit (Roche Diagnostics; coefficient of variation 7%). Diabetes was defined as a fasting blood glucose level ≥126 mg/dl, non–fasting blood glucose ≥200 mg/dL, a self-reported physician diagnosis of diabetes, or current use of antidiabetic medication. Prevalent CVD (CHD, heart failure, stroke, peripheral artery disease) at visit 3 was identified using measured or self-reported information from ARIC visits 1-3 (i.e., electrocardiograms, ankle/brachial index, Gothenburg heart failure and Rose questionnaires, self-reported medical histories, including revascularizations) or as an adjudicated incident CVD event occurring in ARIC before visit 3. Outcome ascertainment Incident CVD events occurring between visit 3 (1993-1995) and December 31, 2012 were identified through: 1) annual telephone calls to cohort participants (or proxy); 2) active surveillance of local hospital discharge indexes; 3) searching state death records; and 4) linkage to the National Death Index. Trained abstractors collected information on all hospitalizations involving cardiovascular disease. CHD events were validated by physician review and were defined as a definite or probable myocardial infarction (MI) or definite fatal CHD by ARIC criteria (5) or as a coronary revascularization. For stroke classification, signs, symptoms, neuroimaging, and other diagnostic reports were used in a computer algorithm and by physician reviewers using criteria adapted from the National Survey of Stroke (6, 7). Ischemic stroke was defined as a validated definite or probable embolic or thrombotic brain infarction. Incident peripheral artery disease (PAD) was defined by hospital discharge diagnosis with International Classification of Disease, Ninth Revision (ICD-9) codes consistent with PAD, leg amputation, or leg revascularization procedures (leg endarterectomy, aorto-iliac-femoral bypass surgery, or other leg bypass or angioplastic surgery). Heart failure (HF) was defined by a hospitalization with an ICD 9 code of 428 or death with an underlying cause of ICD-9
3
code 428 or ICD-10 code I50 (8). Total CVD mortality was defined as deaths with
underlying causes of ICD‐9 codes 390‐459 or ICD‐10 codes I00‐I99. Statistical analysis Of the 12,887 participants who attended ARIC visit 3 (1993 to 1995), we excluded individuals with prevalent CVD (CHD, HF, PAD or stroke) (n=1,848), those taking anticoagulant therapy (n= 62), and those with missing information on γ´ fibrinogen (n= 296). Additionally, we excluded, due to small numbers, participants in Minnesota and Washington County who were not white as well as participants in any field center who were not white or African American (n =80), resulting in an analytic sample of 10,601 participants. Characteristics of the study participants at visit 3 were described using means (standard deviations) and proportions stratified by quartiles of γ´ fibrinogen concentration. Person-time was accrued from the date of the participants’ visit 3 examinations until CVD event, loss-to follow-up, death, or December 31, 2012, whichever came first. Participants contributed information for one or more endpoints. The Kaplan–Meier method was used to estimate cumulative incidence of CHD, ischemic stroke, PAD, HF and CVD deaths by quartiles of γ´ fibrinogen, and the Log-Rank test was used to test for differences between survival curves. Cox proportional hazards regression was used to estimate the hazard ratio (HR) for the association of γ′ fibrinogen with each CVD outcome. The main exposure, γ′ fibrinogen, was modeled as quartiles of the distribution and as a continuous standardized measure (per 1 standard deviation; 8.80 mg/dl). Linear trends in HRs across quartiles of γ′ fibrinogen were tested by modeling the median of each quartile as an ordinal variable in the Cox models for each CVD endpoint. Four models with progressive degree of adjustment were employed. Model 1 adjusted for demographics. Model 2 additionally adjusted for educational attainment and established cardiovascular risk factors. Model 3 further adjusted for total fibrinogen levels. In model 4, we evaluated whether any γ’ fibrinogen association is specific, versus reflecting a general inflammatory association, by further adjusting for CRP. Potential nonlinear relations between γ´ fibrinogen and CVD outcomes were evaluated by using restricted cubic splines with knots set at the 5th, 35th, 65th and 95th percentiles of γ´ fibrinogen. The proportional hazards assumption was tested quantitatively using interaction terms between γ′ fibrinogen quartiles and the log of time as well as qualitatively by visually inspecting plots of Schoenfeld residuals versus time, and the assumption was found to be satisfied for all CVD endpoints. Wald tests were used to formally test for multiplicative interactions of γ′ fibrinogen quartiles with race, sex, CRP and total fibrinogen in relation to incident CVD outcomes. We conducted three sensitivity analyses. To verify if differences existed in the association of corrected and uncorrected γ′ fibrinogen concentrations with CVD endpoints, we repeated the analyses using uncorrected γ′ fibrinogen concentrations. We also assessed the short-term (first 5 years of follow-up) association between γ′ fibrinogen and all the CVD endpoints. Finally, to limit effects of subclinical disease on γ′
4
fibrinogen levels leading to elevated short-term risk, we repeated all analyses after excluding participants who had CVD events during the first three years of follow-up. Statistical analyses were performed using SAS version 9.3 (SAS Institute, Inc., Cary, NC).
References
1. The Atherosclerosis Risk in Communities (ARIC) Study: design and objectives. The
ARIC investigators. American journal of epidemiology 1989;129(4):687-702.
2. Lovely RS, Kazmierczak SC, Massaro JM, et al. Gamma' fibrinogen: evaluation of a new
assay for study of associations with cardiovascular disease. Clinical chemistry
2010;56(5):781-8.
3. Baecke JA, Burema J, Frijters JE. A short questionnaire for the measurement of habitual
physical activity in epidemiological studies. The American journal of clinical nutrition
1982;36(5):936-42.
4. Papp AC, Hatzakis H, Bracey A, et al. ARIC hemostasis study--I. Development of a
blood collection and processing system suitable for multicenter hemostatic studies.
Thrombosis and haemostasis 1989;61(1):15-9.
5. White AD, Folsom AR, Chambless LE, et al. Community surveillance of coronary heart
disease in the Atherosclerosis Risk in Communities (ARIC) Study: methods and initial
two years' experience. Journal of clinical epidemiology 1996;49(2):223-33.
6. Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among
middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC)
cohort. Stroke; a journal of cerebral circulation 1999;30(4):736-43.
7. The National Survey of Stroke. National Institute of Neurological and Communicative
Disorders and Stroke. Stroke; a journal of cerebral circulation 1981;12(2 Pt 2 Suppl
1):I1-91.
8. Loehr LR, Rosamond WD, Chang PP, et al. Heart failure incidence and survival (from
the Atherosclerosis Risk in Communities study). The American journal of cardiology
2008;101(7):1016-22.














![ACUTE SYSTEMIC INFLAMMATION · 5 parameter of inflammation. Increased levels of the acute phase protein fibrinogen are a main determinant of an elevated ESR [10]. A large number of](https://static.fdocument.org/doc/165x107/6147c476a830d0442101a684/acute-systemic-inflammation-5-parameter-of-inflammation-increased-levels-of-the.jpg)

